Contents
- Cerebral venous thrombosis
- Venous Drainage of the Central Nervous System
- Cerebral venous thrombosis causes
- Cerebral venous thrombosis pathophysiology
- Cerebral venous thrombosis symptoms
- Cerebral venous thrombosis diagnosis
- Cerebral venous thrombosis differential diagnosis
- Cerebral venous thrombosis treatment
- Cerebral venous thrombosis prognosis
Cerebral venous thrombosis
Cerebral venous thrombosis also called cerebral venous sinus thrombosis (CVST) is a condition where blood clot (thrombus) occurs in the cerebral veins and the dural sinuses in your brain (Figures 1 to 4) 1. Blood clots are tangles of molecules and blood cells that clump together that occur when blood hardens from a liquid to a solid. Normally the venous sinuses drain blood from your brain. Cerebral venous sinus thrombosis blocks the blood from draining and can cause a hemorrhagic stroke in young and middle-aged adults, with a sex ratio heavily skewed towards women 2. Cerebral venous sinus thrombosis generally occurs in children and young adults and accounts for less than 1% of all strokes 3. Cerebral venous thrombosis peak incidence rate in adults occurs in the third decade of life with the incidence rate being higher in women compared to men 4.
Cerebral venous thrombosis can present with variable signs and symptoms that range from a patient seen at the clinic with a 1-month history of headache, benign intracranial hypertension, subarachnoid hemorrhage (SAH), focal neurological deficit, stroke, seizures, unexplained changes in brain function such as confusion, loss of memory, loss of alertness, disorientation, poor judgment or thinking, meningoencephalitis (a rare and life-threatening condition in which you have meningitis and encephalitis at the same time) to a comatose patient admitted to the emergency room 2, 3, 5, 6. Headache is the most common symptoms and presents as thunder clap headache. Patients can also present with focal or generalized seizures, focal central nervous system (CNS) deficits (hemianopsia, aphasia, motor or sensory defects), and coma. Consequently, the diagnosis of cerebral venous thrombosis is often delayed or overlooked. Results of the International Study on Cerebral Vein and Dural Sinus Thrombosis demonstrated that the median delay from onset of the symptoms to admission was 4 days and from onset of symptoms to diagnosis was 7 days 7. Therefore, having a high index of suspicion for cerebral venous thrombosis is crucial to ensure timely diagnosis and treatment 8, 9.
A variety of therapies for cerebral venous thrombosis are available, and each should be used in the appropriate setting, preferably guided by data from randomized trials and well-designed cohort studies. Treatment of cerebral venous thrombosis includes: (1) treatment of the underlying cause or removal of the identified risk factors, (2) antithrombotic treatment and (3) symptomatic treatment of intracranial hypertension, seizures and other complications. Treatment of sinus thrombosis with heparin is safe and is likely to improve its outcome 10, 11, 12. Local endovascular thrombolysis may improve outcome in selected cases but has only been tried in small uncontrolled case series 13. Despite improvements in diagnosis and treatment in the past few decades, cerebral venous thrombosis may still cause permanent disability or death with mortality remains about 5 to 10% 2, 14, 15, 16, 17, 18, 19, 10.
Approximately 57% to 86% of patients have functional recovery 20, 11, 15; the mortality rate is 5.5% to 18% 21, 20, 11. The risk factors associated with poor outcomes include age greater than 37 years, male sex, altered mental status on presentation, coma, cerebral hemorrhage, cancer, central nervous system infection, and deep venous thrombosis (DVT) 7.
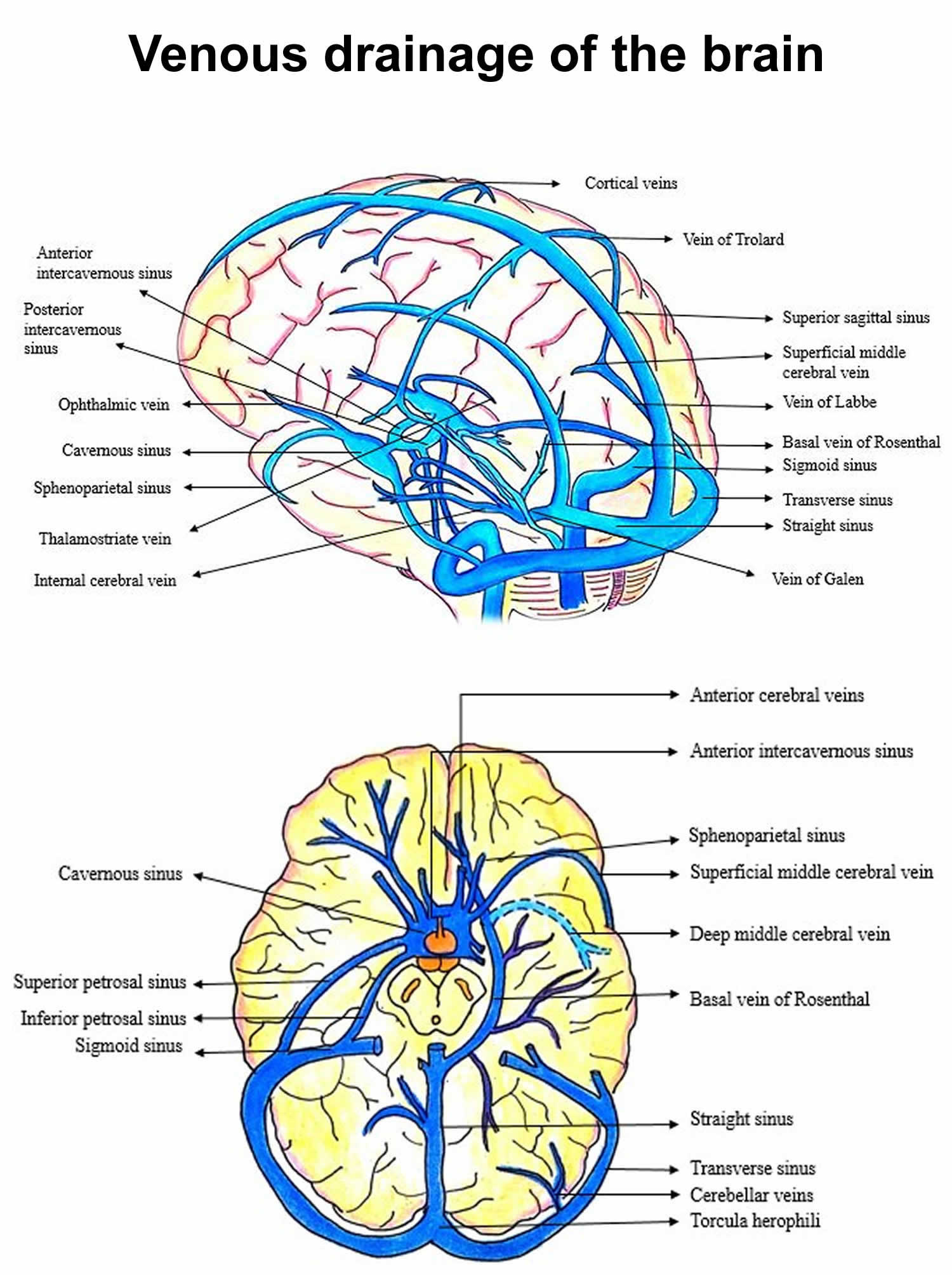
Figure 1. Venous drainage of the brain
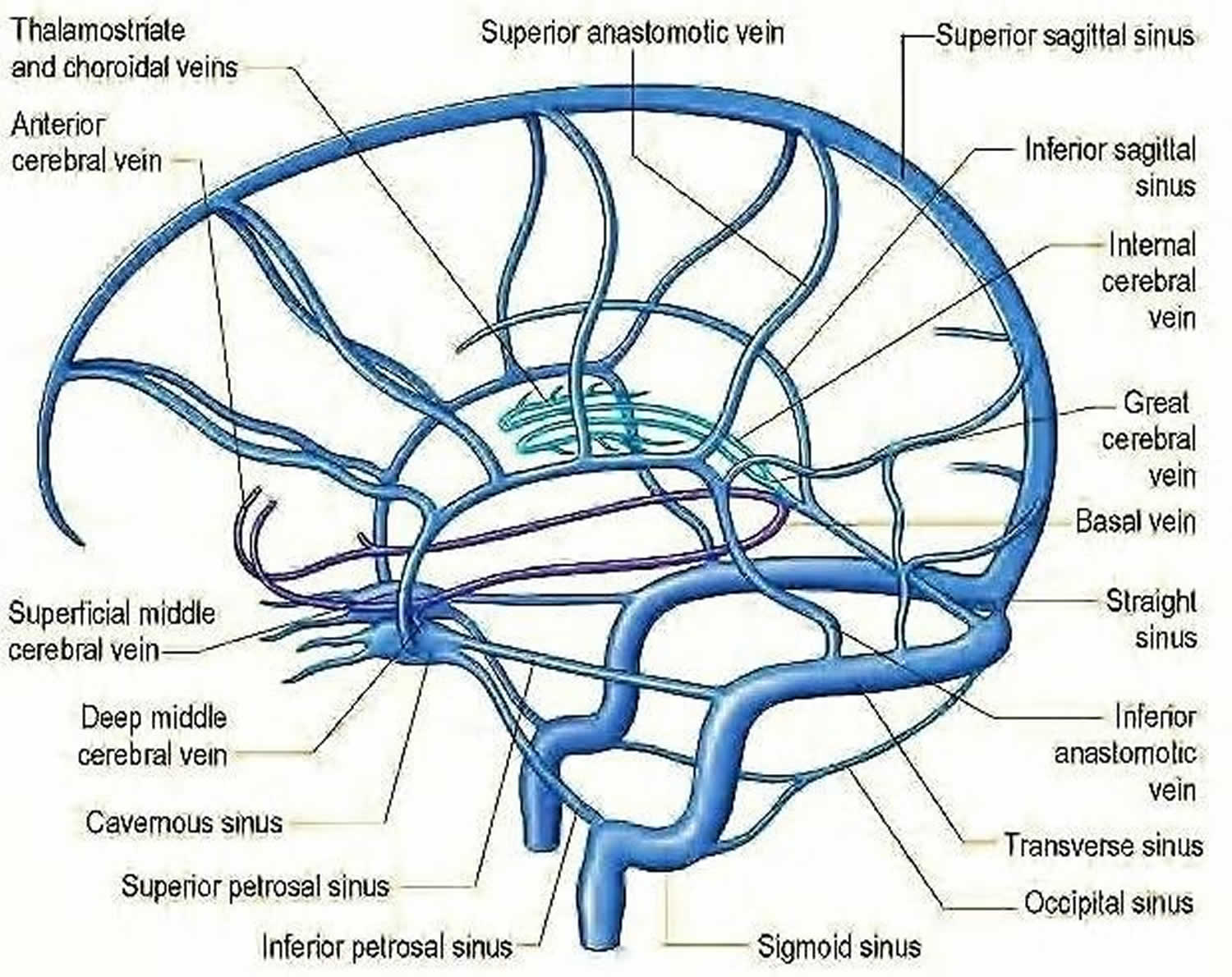
Figure 2. Dural venous sinuses
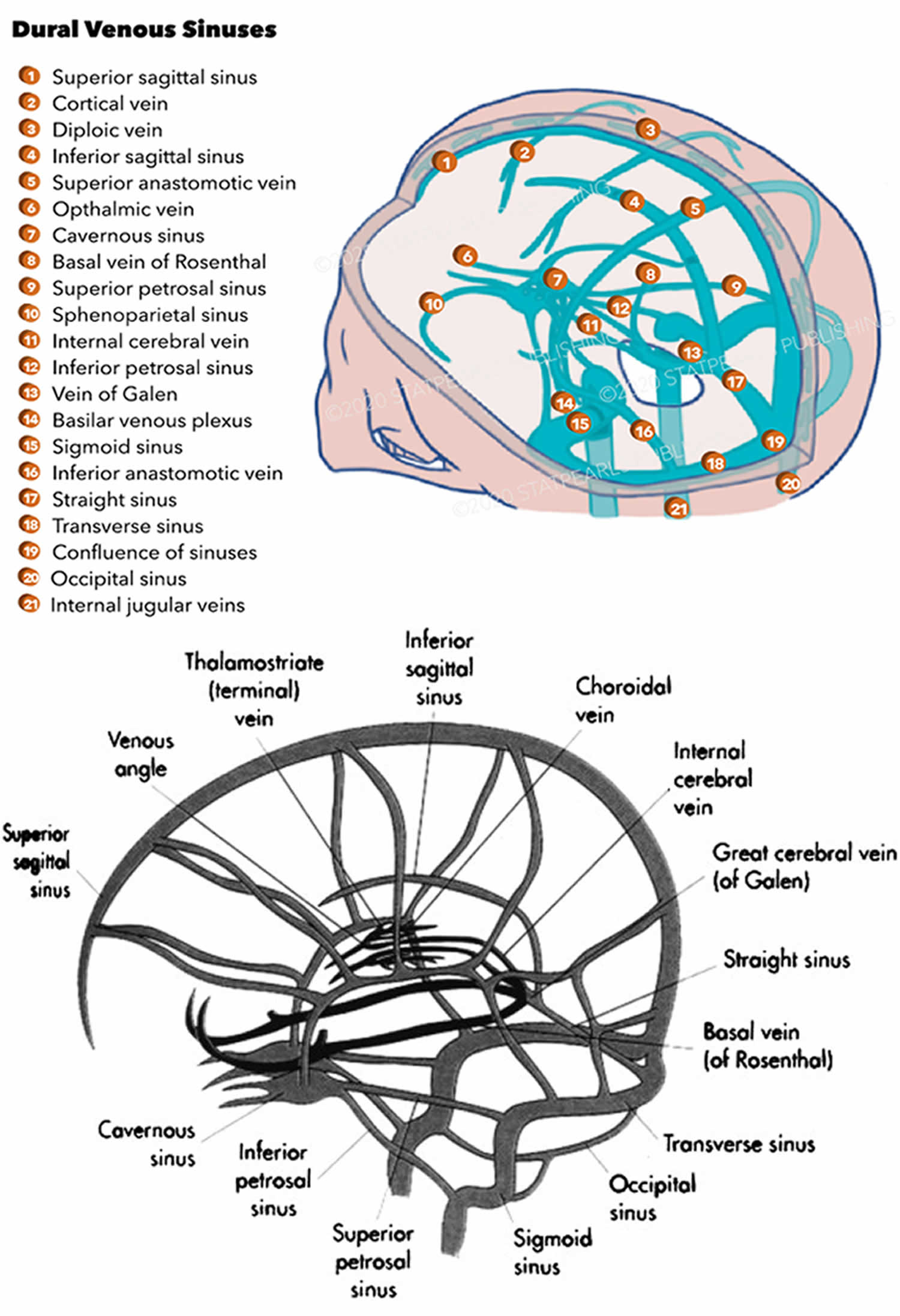
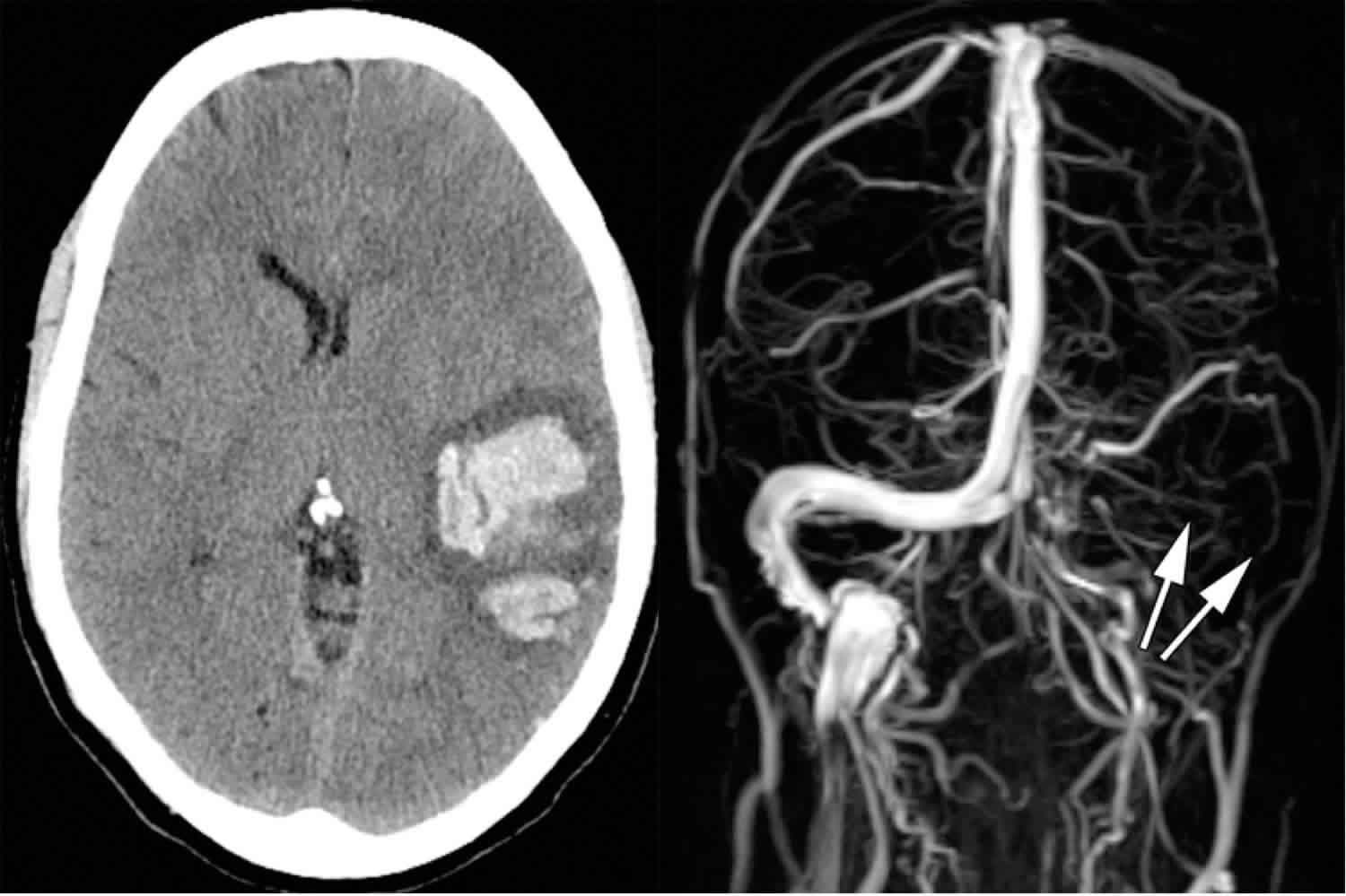
Figure 3. Cerebral venous sinus thrombosis
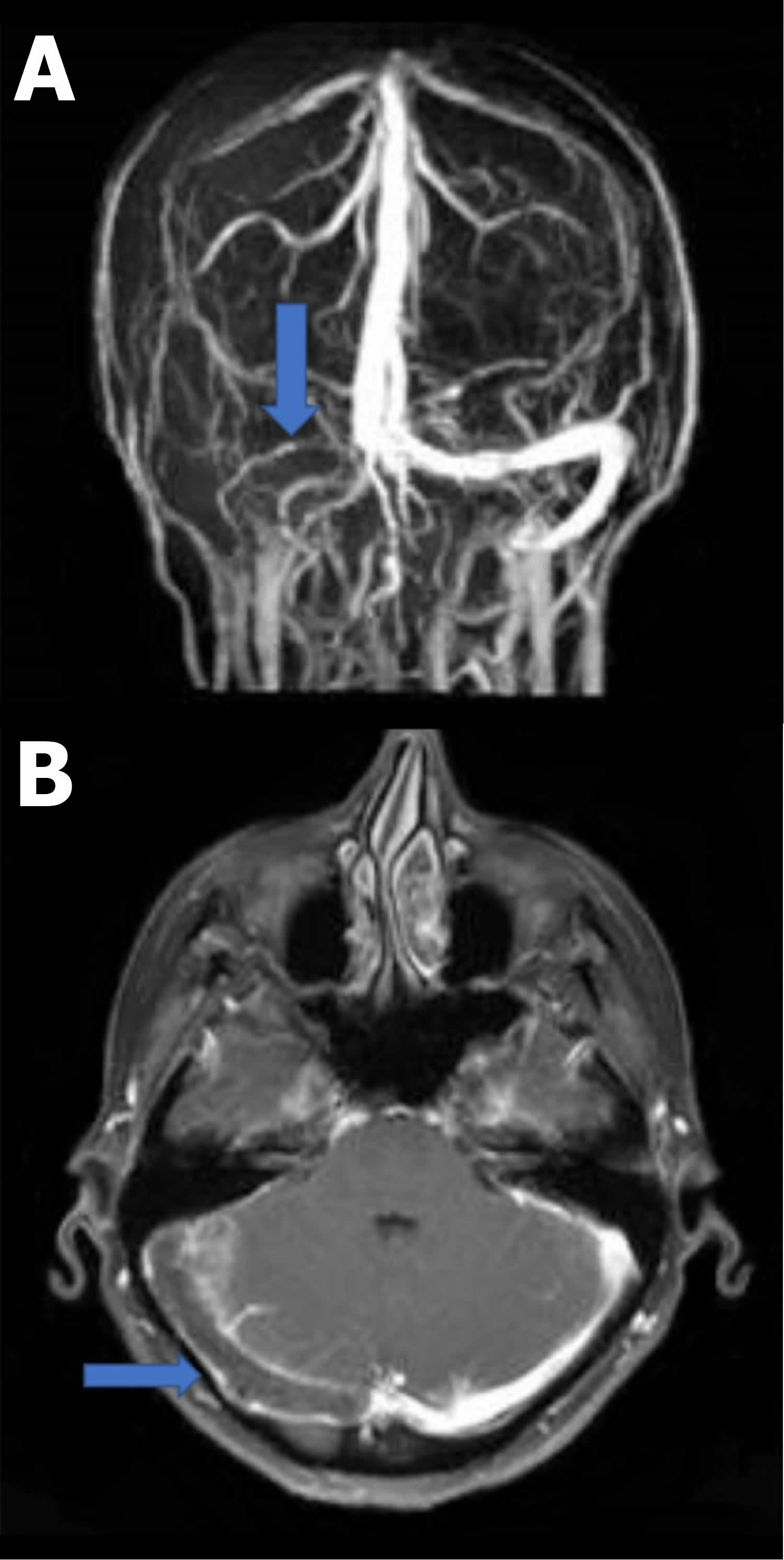
Footnotes: (A) Coronal view of magnetic resonance venogram (MRV) demonstrating no contrast within the right transverse sinus (blue arrow) compatible with thrombosis. (B) Axial view of contrast-enhanced magnetic resonance imaging (MRI) identifying no contrast within the transverse sinus (blue arrow) compatible with occlusion or thrombus.
[Source 3 ]How common is cerebral venous thrombosis?
Cerebral venous thrombosis is a rare disorder with an annual incidence estimated to be 3 to 4 cases per 1,000,000 1. The frequency of peripartum and post-partum cerebral venous thrombosis is about 12 cases per 100,000 deliveries in pregnant women, which is only slightly lower than that of peripartum and post-partum arterial stroke 1. Cerebral venous thrombosis occurs three times more frequently in women than in men 1. This is thought to be due to gender-specific risk factors, for example, oral contraceptive use and, less frequently, pregnancy, puerperium, and hormone replacement therapy 1. More recently, there has been a significant female predominance among young adults, with the majority of cases (70% to 80%) being in women of childbearing age, but not among children or elderly persons.
Venous Drainage of the Central Nervous System
The venous drainage of the brain is complex, and the intracranial veins, unlike the systemic veins, do not follow their arterial counterparts and thus differ in their drainage territory from the arteries. There is also considerable variability in the venous drainage of the brain and skull 24, 25, 26, 23. There are also numerous interconnections between venous drainage systems. Variations in cerebral venous anatomy is a rule rather than an exception 27. These variations must be kept in mind while evaluating a scan for pathologies like cerebral venous sinus thrombosis or assessment of their patency in tumors encasing the venous sinuses 28, 29.
The cerebrum, cerebellum and brainstem are drained by numerous veins, which empty into the dural venous sinuses. The spinal cord is supplied by anterior and posterior spinal veins, which drain into the internal and external vertebral plexuses.
Figure 4. Cerebral venous system
Dural Venous Sinuses
The dural venous sinuses lie between the periosteal and meningeal layers of the dura mater. The dural venous sinuses are best thought of as collecting pools of blood, which drain all of the venous blood from the cerebral hemispheres, the face, and the scalp 30. All the dural venous sinuses ultimately drain into the internal jugular vein. Unlike most veins of the body, the dural venous sinuses do not have valves; therefore, dural venous sinuses can promote a forward or backflow of blood to other associated structures, allowing pathogens and neoplastic cells to travel to different parts of the brain 23.
There are eleven venous sinuses in total 31. There are 7 major dural venous sinuses located within the cranial cavity, specifically between the periosteal and meningeal layer of the dura mater: superior sagittal, inferior sagittal, straight, transverse, sigmoid, cavernous, and superior petrosal sinuses 23. Most of these sinuses are found adjacent to the falx cerebri and tentorium cerebelli. The cavernous sinus is clinically the most important dural venous sinus 23.
The straight, superior, and inferior sagittal sinuses are found in the falx cerebri of the dura mater. They converge at the confluence of sinuses (overlying the internal occipital protuberance). The straight sinus is a continuation of the great cerebral vein and the inferior sagittal sinus.
From the confluence, the transverse sinus continues bilaterally and curves into the sigmoid sinus to meet the opening of the internal jugular vein.
The cavernous sinus drains the ophthalmic veins and can be found on either side of the sella turcica. From here, the blood returns to the internal jugular vein via the superior or inferior petrosal sinuses.
The dangerous triangle of the face is a triangular area bounded by the medial angle of the eyes, sides of the nose and the upper lip as its boundaries. This anatomy is important because it serves as the passageway of pathogens from the face into the brain via the cavernous sinuses. Infection coming from the superficial and deep layers of the face can easily travel into the cavernous sinuses leading to the development of a thrombus, a condition termed as cavernous sinus thrombosis. Cavernous sinus thrombosis may result in the swelling of the affected sinuses and pertinent damage to the associated cranial nerves. Patients may develop internal strabismus caused by the lesion in the cranial nerve 6, which is usually the first cranial nerve affected, which is then followed by damage to further movement and sensation of the eyes and skin of the face as well as the scalp, respectively. Ophthalmoplegia or paralysis of the eye muscles can also be manifestations of other damaged cranial nerves. Pulsatile proptosis characterized by a combination of pulsation and protrusion of the eyeball can also present in patients with affected venous sinuses 32, 33, 34, 35.
Veins of the Cerebrum
The veins of cerebrum are responsible for carrying blood from the brain tissue, and depositing it in the dural venous sinuses 31.
The veins of cerebrum can be divided into superficial and deep groups, which are arranged around the gyri and sulci of the brain. Upon exiting the cerebral parenchyma, the veins run in the subarachnoid space and pierce the meninges to drain into the dural venous sinuses.
Superficial veins of cerebrum
The superficial veins of cerebrum is largely responsible for draining the cerebral cortex:
- Superior cerebral veins: Drain the superior surface, carrying blood to the superior sagittal sinus.
- Superficial middle cerebral vein: Drains the lateral surface of each hemisphere, carrying blood to the cavernous or sphenopalatine sinuses.
- Inferior cerebral veins: Drain the inferior aspect of each cerebral hemisphere, depositing blood into cavernous and transverse sinuses.
- Superior anastamotic vein (Trolard): Connects the superficial middle cerebral vein to the superior sagittal sinus.
- Inferior anastamotic vein (Labbé): Connects the superficial middle cerebral vein to the transverse sinus.
Deep veins of cerebrum
- Subependymal veins: There are numerous subependymal veins, which will not be described here in detail. These receive blood from the medullary veins and carry it to the dural venous sinuses. The great cerebral vein (vein of Galen) is worthy of a mention; it is formed by the union of two of the deep veins, and drains into the straight sinus.
- Medullary veins: Originate 1 to 2cm below the cortical grey matter, and drain into subependymal veins. These drain the deep areas of the brain.
Veins of the Cerebellum
There are two main veins responsible for the venous drainage of the cerebellum – the superior and inferior cerebellar veins. They empty into the superior petrosal, transverse and straight dural venous sinuses.
Veins of the Brainstem
Venous drainage of the brainstem is carried out by numerous vessels – many of which are beyond the scope of this article. Examples of veins that drain the brainstem include the transverse pontine vein, anteromedian medullary vein, and the anterior and posterior spinal veins.
Veins of the Spinal Cord
The spinal cord is supplied by three anterior and three posterior spinal veins. These veins are valveless, and form an anastamotic network along the surface of the spinal cord. They also receive venous blood from the radicular veins.
The spinal veins drain into the internal and external vertebral plexuses, which in turn empty into the systemic segmental veins. The internal vertebral plexus also empties into the dural venous sinuses superiorly.
Cerebral venous thrombosis causes
Cerebral venous sinus thrombosis patients usually have at least one of these risk factors:
- Thrombophilia, a tendency to develop blood clots due to abnormalities in coagulation, e.g. factor V Leiden, deficiency of protein C, protein S or antithrombin, or related problems
- Nephrotic syndrome, a kidney problem causing protein loss in the urine (proteinuria)
- Chronic inflammatory diseases, such as inflammatory bowel disease (Crohn’s disease and ulcerative colitis), systemic lupus erythematosus (autoimmune disease that occurs when your body’s immune system attacks your own tissues and organs) and Behçet’s disease (inflammation in blood vessels of unknown cause)
- Pregnancy and puerperium (the period after giving birth)
- Particular blood disorders, especially polycythemia vera (a rare blood disorder in which there is an increase in all blood cells, particularly red blood cells) and paroxysmal nocturnal hemoglobinuria (is a rare disease in which red blood cells break apart prematurely that presents clinically with a variety of symptoms, the most prevalent of which are hemolytic anemia, hemoglobinuria, and somatic symptoms including fatigue and shortness of breath)
- Use of estrogen-containing forms of hormonal contraception
- Meningitis and infections of the ear, nose and throat area such as mastoiditis and sinusitis
- Direct injury to the venous sinuses
- Medical procedures in the head and neck area
- Sickle cell anemia
- Dehydration, primarily in infants and children
- Homocystinuria
In general, cerebral venous thrombosis is common in any condition that leads to a hypercoagulable state (prothrombotic state or thrombophilia, which is the tendency to venous thrombosis due to an abnormality in the coagulation system), including pregnancy, the post-partum state, or those on oral contraceptives. In the International Study on Cerebral Vein and Dural Sinus Thrombosis (ICSVT), genetic and acquired thrombophilia were present in 34% of patients with cerebral venous thrombosis. Inherited thrombophilia includes protein C and protein S deficiencies, antithrombin deficiency, factor V Leiden mutation, prothrombin gene mutation 20210, as well as hyperhomocysteinemia 36, 37.
At least one risk factor was identified in more than 85% of patients with cerebral venous thrombosis, and multiple risk factors are found in more than 50% of patients with cerebral venous thrombosis 38.
Acquired thrombophilia should be suspected in patients with a history of nephrotic syndrome (due to loss of antithrombin) or antiphospholipid antibodies 1. Additional causes and risk factors associated with cerebral venous thrombosis include chronic inflammatory disease states such as systemic lupus erythematosus (SLE), inflammatory bowel disease (Crohn’s disease and ulcerative colitis), cancer, and inflammation in blood vessels such as Wegener’s granulomatosis 1. Local infections such as otitis and mastoiditis, which can lead to thrombosis of the adjacent sigmoid and transverse sinuses, have also been implicated in developing cerebral venous thrombosis. Cerebral venous thrombosis may also be seen in a patient with a head injury, after certain neurosurgical procedures, direct injury to the sinuses or jugular veins, such as jugular vein catheterization, and even after a lumbar puncture 39, 40.
Cerebral venous thrombosis risk factors
Cerebral venous thrombosis has multiple risk factors, which can be grouped into:
- Transient risk factors:
- Oral contraceptive pills very common cause in female patients <50 years of age and other medications with prothrombotic effects e.g., steroids,
- Pregnancy and puerperium (the period after giving birth),
- Infections, especially those involving the central nervous system or the paranasal sinus, the ear and the mastoid sinus (dural sinus occlusive disease)
- Skull abnormalities or trauma
- Compressing mass: e.g. meningioma
- Systemic illness
- Dehydration: e.g. gastroenteritis
- Sepsis
- Cancer
- Connective tissue disorders
- Iatrogenic
- COVID-19 vaccine, especially AstraZeneca 41
- Permanent risk factors:
- Prothrombotic medical conditions, including genetic thrombophilic diseases, antiphospholipid syndrome, myeloproliferative disorders and cancers.
In around 13% of adult cerebral venous thrombosis no risk factors are identified (idiopathic) 7.
Cerebral venous thrombosis pathophysiology
Cerebral venous thrombosis pathogenesis remains poorly understood 42. There are two pathophysiologic mechanisms thought to contribute to the clinical signs and symptoms of cerebral venous thrombosis 1.
First, thrombosis of the cerebral veins leads to increased venous and capillary pressure, which leads to a decrease in cerebral perfusion 1. Decreased cerebral perfusion results in ischemic injury, manifested by cytotoxic edema, which damages the energy-dependent cellular membrane pumps and leads to intracellular swelling. Disrupting the blood-brain barrier leads to vasogenic edema and leakage into the interstitial space. The increased pressure in the venous system can lead to an intraparenchymal hemorrhage 1.
The second pathophysiologic mechanism resulting in cerebral venous thrombosis is obstruction of the cerebral sinuses, particularly when the blood clot (thrombus) does not resolve 1. Normally, the cerebrospinal fluid (CSF) found in the cerebral ventricles is transported through the subarachnoid space to the arachnoid granulations and absorbed into the venous sinuses. Thrombosis of the venous sinuses results in impaired cerebrospinal fluid absorption, ultimately leading to increased intracranial pressure. Increased intracranial pressure leads to cytotoxic and vasogenic edema and may result in parenchymal hemorrhage also called hemorrhagic stroke 1. In a healthy brain, neurons (brain cells) do not come into direct contact with blood. In hemorrhagic stroke, when an artery in the brain bursts, blood gushes into or around the brain, damaging the surrounding tissue.
Cerebral venous thrombosis symptoms
Cerebral venous thrombosis can present with variable signs and symptoms that range from a patient seen at the clinic with a 1-month history of headache, benign intracranial hypertension, subarachnoid hemorrhage (SAH), focal neurological deficit, stroke, seizures, unexplained changes in brain function such as confusion, loss of memory, loss of alertness, disorientation, poor judgment or thinking, meningoencephalitis (a rare and life-threatening condition in which you have meningitis and encephalitis at the same time) to a comatose patient admitted to the emergency room 2, 3, 5, 6. Headache is the most common symptoms and presents as thunder clap headache. Patients can also present with focal or generalized seizures, focal central nervous system (CNS) deficits (hemianopsia, aphasia, motor or sensory defects), and coma. Consequently, the diagnosis of cerebral venous thrombosis is often delayed or overlooked. Results of the International Study on Cerebral Vein and Dural Sinus Thrombosis demonstrated that the median delay from onset of the symptoms to admission was 4 days and from onset of symptoms to diagnosis was 7 days 7.
Cerebral venous thrombosis symptoms include the following:
- headaches (89-91%) 43
- decreased or altered conscious state
- decreased or altered vision
- nausea and vomiting
Cerebral venous thrombosis signs include the following:
Signs and symptoms may be acute, subacute, or chronic, with the most common symptom in cerebral venous thrombosis being a headache. A subacute pattern of the clinical presentation was observed in almost 60% of cases compared to acute (<48 hours in 37%) and chronic (>30 days in 7%) 38. A headache presents in up to 90% of patients 38. Headaches may be generalized or diffuse and tend to mimic migraines but may increase in severity slowly over days and weeks and are not relieved with sleep 1. In some instances, the headache may be thunderclap in nature, starting suddenly and maximal in intensity at onset, thereby mimicking the presentation of subarachnoid hemorrhage 1.
A headache is often worsened with Valsalva or coughing, indicative of increased intracranial pressure 1. Papilledema and visual symptoms, such as diplopia caused by a sixth cranial nerve palsy when the intracranial pressure is too high, may accompany a headache. The funduscopic examination will reveal papilledema, which, depending on the severity, can cause visual impairment and even permanent blindness if left untreated. However, an isolated headache without any other focal neurologic deficits or papilledema has been reported in up to a fourth of patients with cerebral venous thrombosis and further complicates the diagnostic picture.
Focal neurologic signs are common and are seen in up to 44% of patients 1. Motor weakness, including hemiparesis, is the most common focal finding. However, unlike arterial thrombosis in the setting of cerebrovascular accidents, localization to one vascular territory is often absent. Hemispheric symptoms, such as aphasia and hemiparesis, are a characteristic but rare finding. Seizures are seen in about 40% of patients with cerebral venous thrombosis, the most common of which are focal seizures. Focal seizures account for 50% of those who experience a seizure in the setting of cerebral venous thrombosis but have the potential to generalize to a status epilepticus. Therefore, cerebral venous thrombosis should be considered in any patient who presents with a headache and some combination of either focal neurologic deficit or new-onset seizures 1. Thrombosis of the straight sinus, or in severe cases of venous infarction with hemorrhagic transformation, can lead to compression of the diencephalon and brainstem, resulting in coma or death due to cerebral herniation 44.
Cerebral venous thrombosis diagnosis
Doctors should highly suspect cerebral venous thrombosis given the variable signs and symptoms and low annual incidence.
Diagnosis of cerebral venous thrombosis is clinical and confirmed with neuroimaging. Given cerebral venous thrombosis varied presentation and myriad of symptoms, one must have a high index of suspicion to identify and diagnose this rare and potentially life-threatening condition correctly. Cerebral venous thrombosis should be suspected in young and middle-aged patients, especially those with cerebral venous thrombosis risk factors, such as postpartum women, those with genetic or acquired thrombophilia, and patients with focal neurological findings. It should also be suspected in the following 1:
- Under the age of 50
- Who present with atypical headaches or those having multiple repeat evaluations for an unrelenting headaches
- Focal neurological deficit
- Stroke-like symptoms, especially in the absence of vascular risk factors that would predispose to cerebral vascular accidents (carotid atherosclerosis)
- Seizures (focal, generalized, or status-epilepticus)
- Intracranial hypertension or evidence of papilledema on funduscopic exam
- Patients with CT evidence of hemorrhagic infarcts, particularly in the setting of multiple infarcts not confined to a single vascular territory
Some important clinical clues to the diagnosis include slow progression, bilateral involvement, and concurrent seizures 38.
Laboratory tests
Laboratory tests should include a complete blood count, coagulation panel, chemistry panel, as well as inflammatory markers such as a sedimentation rate (ESR) and C-reactive protein (CRP) to evaluate for proinflammatory states 1. Ideally, a screening test that could effectively rule out the diagnosis without subjecting patients to neuroimaging when it is not necessary would be ideal and prove helpful to clinical practice. The D-dimer assay has been evaluated in this regard, and unfortunately, it has been shown to have an unacceptable false-negative rate of up to 26% in one study. This low sensitivity of the D-dimer assay is in contrast to the utility of the D-dimer in ruling out deep venous thrombosis, which may be due to the lower thrombotic burden of cerebral venous thrombosis compared to deep vein thrombosis (DVT) 45, 46.
Based on recent American Heart Associationand the American Stroke Association guidelines, a negative D-dimer does not effectively rule out cerebral venous thrombosis and should not preclude neuroimaging if there is clinical suspicion for cerebral venous thrombosis 47, 48. However, adding D-dimer (≥500 μg/L) to the clinical cerebral venous thrombosis score (comprising of variables such as seizure, known thrombophilia, oral contraceptive use, duration of symptoms for >6 days, worst headache ever, and focal neurologic deficits) has shown to improve its predictive value 49
Neuroimaging
- Non-contrast computed tomography (CT): The speed and accessibility with which this test can be obtained make it the first test that should be obtained in any patient presenting with an atypical headache, focal neurologic deficit, seizures, altered mental status, or coma. A direct sign of cerebral venous thrombosis is the cord sign, a curvilinear hyperdensity within a cortical vein in the presence of thrombosis that can be seen for up two weeks following thrombus formation. Other direct signs include hyperdensity with a triangular shape in the superior sagittal sinus, also known as the dense triangle sign. Intraparenchymal hemorrhages or infarcts may be seen on non-contrast head CT and may cross vascular boundaries. In a multicentric study, brain infarction was observed in 36.4%, hemorrhagic transformation in 17.3%, and intraparenchymal hemorrhage in 3.8% of cohorts 38. Hyperdensity within a cortical vein or dural sinus in plain CT is observed in only one-third of the cases 38.
- CT Venography (CTV): While MRI does have a better sensitivity and specificity when compared to computed tomography, diagnostic and confirmatory venography is required to exclude cerebral venous thrombosis. The presence of new, helical CT scanners has led to evidence that CT venography is superior in the identification of cerebral veins when compared to MR venography (MRV) and that the two methods are equivocal in the identification and diagnosis of cerebral venous thrombosis. The fact that CT venography can rapidly be performed following a non-contrast head CT while the patient is still in the CT scanner makes CT venography (CTV) a viable option in the emergency setting when access to MRI imaging and venography may otherwise be limited or unavailable. Contrast-enhanced computed tomography illustrates the empty delta sign, representing contrast enhancement flowing around the comparatively hypodense region of the thrombosed superior sagittal sinus.
- Magnetic resonance imaging (MRI) and magnetic resonance venography (MRV) are considered the gold standard in diagnosing cerebral venous thrombosis as they have a higher sensitivity than computed tomography 1. MRI is superior to CT when evaluating for parenchymal edema as a result of cerebral venous thrombosis. MRI findings are dependent on the age of the thrombus, as signal intensities change depending on thrombus age. Thus, MRI interpretation requires a detailed understanding of the evolutionary changes seen radiographically. An acutely formed thrombus (0 to 7 days) is harder to detect, but by week 2, abnormalities are easier to detect, with both T1 and T2-weighted images showing a hyperdense signal. The combination of an abnormal signal in a venous sinus combined with the absence of flow on MRV confirms the diagnosis of cerebral venous thrombosis. 2-dimensional lumen-based TOF showing the absence of a flow void in the dural sinus is the most sensitive imaging modality. Multiscale entropy (MSE) of hemoglobin products within the thrombus is of high diagnostic value 50. The presence of DWI abnormality within the involved veins or sinus indicates low chances of recanalization. The differentials include arachnoid granulations and fenestrations 42.
- Cerebral angiography: If the diagnosis is still in question after using MRI and MRV, then intra-arterial angiography is indicated. Angiography allows for superior visualization of the cerebral veins and helps identify anatomical variants of normal venous anatomy that mimic cerebral venous thrombosis. It is useful in rare cases of isolated cortical vein thrombosis without sinus thrombosis and may show indirect signs such as dilated and tortuous “corkscrew” collateral veins, evidence that there may be thrombosis further downstream of the sinuses. Superior sagittal sinus is most frequently involved, followed by transverse sinus 38.
Cerebral venous thrombosis differential diagnosis
Cerebral venous thrombosis differential diagnosis include the following 1:
- Abducens nerve palsy (cranial nerve 6 palsy)
- Blood diseases (e.g., hemophilia, clots disorders, and blood cancers such as leukemia, lymphoma, and myeloma)
- Cavernous sinus syndrome
- Head injury
- Intracranial abscess
- Neurosarcoidosis
- Pediatric status epilepticus
- Pseudotumor cerebri (idiopathic intracranial hypertension)
- Staphylococcal meningitis
- Subdural empyema
Cerebral venous thrombosis treatment
Cerebral venous sinus thrombosis treatment initially focuses on identifying and addressing life-threatening complications of cerebral venous thrombosis, including increased intracranial pressure (ICP), seizures, and coma 1. If a patient has seizures and has a lesion such as a hemorrhage or infarction on neuroimaging, then specific anticonvulsant therapy, as well as seizure prophylaxis, should be initiated 1. If a seizure does not occur, then seizure prophylaxis is not indicated. In the case of increased intracranial pressure (ICP), the head of the bed should be elevated, and administration of dexamethasone and mannitol should be done promptly to reduce increased intracranial pressure (ICP). This is followed by admission to the intensive care unit (ICU) or stroke unit for close intracranial pressure (ICP) monitoring, with a neurosurgical consultation if the patient decompensates and requires surgical decompression. Next, attention should be shifted to specific therapy, including anticoagulation and, in certain cases, catheter-directed fibrinolysis and surgical thrombectomy.
Anticoagulation
Anticoagulation medications also known as blood thinners or anticoagulants are medicines that prevent blood clots from forming. Anticoagulation medications do not break up clots that you already have. But they can stop those clots from getting bigger.
There are different types of blood thinners:
- Anticoagulants, such as heparin or warfarin (also called Coumadin), slow down your body’s process of making clots.
- Antiplatelets, such as aspirin and clopidogrel, prevent blood cells called platelets from clumping together to form a clot. Antiplatelets are mainly taken by people who have had a heart attack or stroke.
Anticoagulation has been a controversial topic due to the potential for hemorrhagic transformation of cerebral infarcts before administering anticoagulation. The goal of anticoagulation is to prevent thrombus propagation, help recanalize the lumen of occluded cerebral veins, and to prevent the complications of deep venous thrombosis and pulmonary embolism in patients who already have thrombus burden and are predisposed to forming additional thrombi. The results of two randomized controlled trials, which compared anticoagulation with placebo, although statistically insignificant, showed that anticoagulation had a favorable outcome more often than controls. They also showed that anticoagulation was safe and not contraindicated, even in patients with cerebral hemorrhage.
Based on these randomized controlled trials and other observational studies, anticoagulation is recommended as a safe and effective treatment of cerebral venous thrombosis. It should be initiated immediately upon diagnosis of cerebral venous thrombosis. Anticoagulation with intravenous unfractionated heparin or subcutaneously administered low-molecular-weight heparin is recommended as a bridge to oral anticoagulation with a vitamin K antagonist. There are no outcome differences while comparing unfractionated heparin (UFH) or low molecular weight heparin (LMWH). The European stroke organization guidelines advocate unfractionated heparin in patients with renal insufficiency or the probability of requiring emergent reversal 38.
The target goal of treatment is an international normalized ratio (INR) of 2.0 to 3.0 cerebral venous thrombosis 3 to 6 months in patients with provoked cerebral venous thrombosis and 6 to 12 months in patients with unprovoked cerebral venous thrombosis 38. Indefinite anticoagulation should be considered in patients with recurrent cerebral venous thrombosis, those who develop deep vein thrombosis and pulmonary embolism in addition to cerebral venous thrombosis, or those with first-time cerebral venous thrombosis in the setting of severe thrombophilia.
Thrombolysis (Thrombolytic Therapy)
Thrombolysis also called fibrinolytic therapy is the breakdown of blood clots formed in blood vessels using medications (thrombolytics) or a minimally invasive procedure to break up blood clots and prevent new clots from forming.
Although most patients see clinical improvement with anticoagulation therapy, a small subset of patients do not, and these individuals clinically deteriorate despite anticoagulation. In these cases, where the prognosis is poor, systemic and catheter-directed thrombolysis is indicated in patients with large and extensive cerebral venous thrombi who clinically deteriorate despite treatment with anticoagulation 1. As is the case, whenever fibrinolytics are used, there is an increased risk of intracranial hemorrhage 1. Based on a systemic review conducted in 2003 38, which looked at 72 studies and 169 patients with cerebral venous thrombosis, there seems to be a possible clinical benefit due to the use of fibrinolytics in patients with a severe presentation. Intracranial hemorrhage occurred in 17% of patients treated with fibrinolytics and was associated with clinical deterioration in 5% of cases. Overall, endovascular thrombolytics should be used at centers with staff experienced in interventional radiology and should be reserved for patients who are clinically deteriorating and despite treatment with anticoagulation. A systematic study has shown local thrombolysis to be beneficial only in patients with severe cerebral venous thrombosis, whereas the results are anecdotal for mechanical thrombectomy 38.
Surgical Intervention
Surgical thrombectomy is reserved for cases of severe neurological deterioration despite maximal medical therapy. In the case of large venous infarcts and hemorrhages causing a mass effect with risk of herniation, decompressive surgery has been thought to improve clinical outcomes, especially if done early. Decompressive surgery is life-saving, with favorable outcomes observed in more than 50% of patients, with a mortality rate of approximately 20% 38.
Supportive Care
It is important to find the underlying contributory factors of cerebral venous thrombosis and devise a treatment strategy to correct them. Women on hormonal contraceptive therapy should seek non-estrogen-based methods of contraception such as levonorgestrel and copper intrauterine devices or progestin-only pills. Further testing to identify the cause of all acquired and reversible thrombophilic states should be conducted and, when possible, corrected. In addition to clinical follow-up, the American Heart Association and American Stroke Association recommend follow-up imaging 3 to 6 months after diagnosis to assess for recanalization.
The risks for intracerebral hemorrhage following anticoagulation therapy ranged from zero to 5.4%. A systematic review has shown that the overall mortality was 9.4%, and dependency of 9.4% and 9.7%, respectively 51, 52.
Post-Stroke Rehabilitation
Stroke rehabilitation is vital to stroke recovery and can help you relearn skills you lost because of the brain damage. The goal is to help you become as independent as possible and to have the best possible quality of life.
- Physical therapy is the main form of rehabilitation for most people with stroke. The aim of physical therapy is to help people relearn simple motor activities such as walking, sitting, standing, lying down, and the process of switching from one type of movement to another. To achieve this, physical therapists use training and exercises to restore movement, balance, and coordination. In one stroke rehabilitation study, researchers compared at home physical therapy to a locomotor training program using treadmill walking with body weight support followed by walking practice. The Locomotor Experience Applied Post-Stroke (LEAPS) trial found that people who had a stroke and had physical therapy at home improved their ability to walk just as well as those who were treated with the locomotor training program. Study investigators also found that patients continued to improve up to one year after stroke, defying conventional wisdom that recovery occurs early and largely ends at six months.
- Occupational therapy helps people relearn the skills needed to perform everyday activities such as eating, drinking and swallowing, dressing, bathing, cooking, reading and writing, and toileting. This type also involves exercise and training. Occupational therapists can recommend home or workplace modifications to better help the person resume living an independent or semi-independent lifestyle.
- Speech therapy helps people with stroke relearn language and speaking skills or learn other forms of communication. Speech therapy is appropriate for people who have no problems with cognition or thinking but have problems understanding speech or written words, or problems forming speech. Speech therapy also helps people develop coping skills to deal with the frustration of not being able to communicate fully. With time and patience, speech therapy can help a stroke survivor regain some, and sometimes all, language and speaking abilities.
- Vocational therapy helps people return to the workforce. Approximately one-fourth of all strokes occur in people between the ages of 45 and 65. For most people in this age group, returning to work is a major concern. It may involve relearning the more complex skills that were performed on the job or learning new skills for a different job. Vocational therapists can help people with lasting disabilities identify job skills and strengths and look for new work opportunities if necessary.
- Psychological or psychiatric therapy can assist many people as they recuperate from stroke. Depression, anxiety, frustration, and anger are common disabilities in people with stroke. Psychological or psychiatric therapy, along with medication, can help ease some of the mental and emotional problems that result from stroke. Sometimes it is useful for family members to seek psychological help for themselves, as well.
- The U.S. Food and Drug Administration (FDA) approved the Neurolutions Upper Extremity Rehabilitation System for individuals age 18 and older with upper arm disability who are undergoing stroke rehabilitation to increase range of motion and grasping. The brain-computer interface uses non-invasive electroencephalography electrodes to record brain activity, which is then wirelessly conveyed to a tablet for the analysis of the intended muscle movement, and a signal is sent to a wireless electronic hand brace, which in turn moves the person’s hand.
- The FDA approved the MicroTransponder Vivistim Paired VNS (vagus nerve stimulation) System, which is to be used along with stroke rehabilitation to help individuals who have moderate to severe impaired upper limb and extremity motor defects caused by a chronic ischemic stroke. The system electrically stimulates the vagus nerve, which runs from the brain down to the abdomen, to improve upper limb and extremity motor function and to improve an individual’s ability to move the arms and hands..
Cerebral venous thrombosis prognosis
The natural history of cerebral venous thrombosis is highly variable, with some patients having minimal or no symptoms and an uneventful recovery (~65%), whereas others have a severe course culminating in extensive venous infarction and dependency or death (~20%) 7. Coma, hemorrhagic venous infarcts and co-existing cancer correlate with poor outcome 7. Deep cerebral venous thrombosis also has a negative impact on prognosis due to the usually bilateral involvement of the thalami 53. Dural arteriovenous fistula, increased CSF pressure and subarachnoid hemorrhage have been reported as possible complications after cerebral venous thrombosis.
In about 50% of cases, cerebral venous thrombosis progresses to venous infarction 54. Unlike arterial infarcts, venous infarcts usually present after some days 54:
- Less than 2 days of symptom onset: 30%
- 2-30 days: 50%
- Greater than 30 days: 20%
Figure 5. Cerebral venous thrombosis risk score
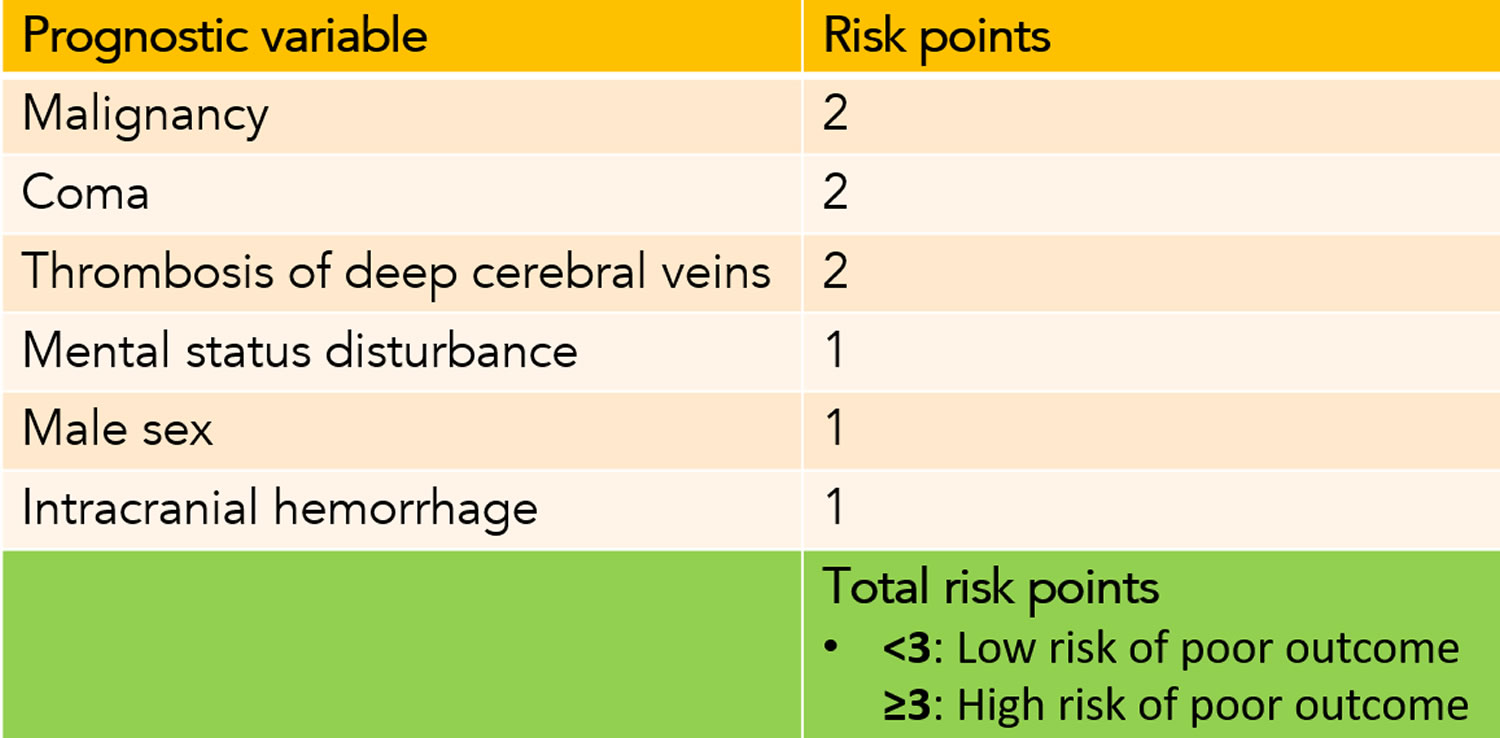
The natural history and prognosis of cerebral venous thrombosis patients has been improving over the last decades, not only due to the increase in diagnosis of milder forms of cerebral venous thrombosis and to improved care, but also due to the substantial decrease of septic cerebral venous thrombosis 14, 15, 16, 17, 18, 19, 56. Mortality in the Western countries is now below 5% and about 80% of the patients make a complete recovery 7. Death is mainly caused by fatal brain herniation, secondary to large hemispheric hemorrhagic strokes 57. Other deaths are related to the underlying condition, status epilepticus, infection and very rarely to pulmonary embolism. Cerebral venous thrombosis risk score can be used to help identifying cerebral venous thrombosis patients with a higher risk of unfavorable outcome 58.
- Tadi P, Behgam B, Baruffi S. Cerebral Venous Thrombosis. [Updated 2023 Jun 12]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK459315[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Silvis, S., de Sousa, D., Ferro, J. et al. Cerebral venous thrombosis. Nat Rev Neurol 13, 555–565 (2017). https://doi.org/10.1038/nrneurol.2017.104[↩][↩][↩][↩]
- Rawala MS, Noorani MM, Gulati R, Waqas S, Dave D. Elevated Factor VIII Level Associated with Transverse Cerebral Venous Sinus Thrombosis. Am J Case Rep. 2019 Mar 2;20:274-277. doi: 10.12659/AJCR.913917[↩][↩][↩][↩]
- Coutinho JM, Gerritsma JJ, Zuurbier SM, Stam J. Isolated cortical vein thrombosis: systematic review of case reports and case series. Stroke. 2014 Jun;45(6):1836-8. doi: 10.1161/STROKEAHA.113.004414[↩]
- Farooq S, Testai FD. Neurologic Complications of Sickle Cell Disease. Curr Neurol Neurosci Rep. 2019 Feb 28;19(4):17. doi: 10.1007/s11910-019-0932-0[↩][↩]
- Singhal V. Clinical Approach to Acute Decline in Sensorium. Indian J Crit Care Med. 2019 Jun;23(Suppl 2):S120-S123. doi: 10.5005/jp-journals-10071-23188[↩][↩]
- Ferro JM, Canhão P, Stam J, Bousser MG, Barinagarrementeria F; ISCVT Investigators. Prognosis of cerebral vein and dural sinus thrombosis: results of the International Study on Cerebral Vein and Dural Sinus Thrombosis (ISCVT). Stroke. 2004 Mar;35(3):664-70. https://doi.org/10.1161/01.STR.0000117571.76197.26[↩][↩][↩][↩][↩][↩][↩]
- Zhu L, Cheng J, Gu P, Liu Y, Liu J, Wang J, Shen H. Therapeutic strategies of thromboembolic events in patients with inflammatory bowel diseases: Two case reports. Medicine (Baltimore). 2019 Mar;98(9):e14622. doi: 10.1097/MD.0000000000014622[↩]
- Tekesin A, Tunç A. Inflammatory markers are beneficial in the early stages of cerebral venous thrombosis. Arq Neuropsiquiatr. 2019 Feb;77(2):101-105. doi: 10.1590/0004-282X20190001[↩]
- Einhäupl KM, Villringer A, Meister W, Mehraein S, Garner C, Pellkofer M, Haberl RL, Pfister HW, Schmiedek P. Heparin treatment in sinus venous thrombosis. Lancet. 1991 Sep 7;338(8767):597-600. doi: 10.1016/0140-6736(91)90607-q. Erratum in: Lancet 1991 Oct 12;338(8772):958.[↩][↩]
- de Bruijn SF, Stam J. Randomized, placebo-controlled trial of anticoagulant treatment with low-molecular-weight heparin for cerebral sinus thrombosis. Stroke. 1999 Mar;30(3):484-8. doi: 10.1161/01.str.30.3.484[↩][↩][↩]
- Stam J, de Bruijn S, deVeber G. Anticoagulation for cerebral sinus thrombosis. Stroke. 2003 Apr;34(4):1054-5. doi: 10.1161/01.STR.0000062344.87396.72[↩]
- Canhão P, Falcão F, Ferro JM. Thrombolytics for cerebral sinus thrombosis: a systematic review. Cerebrovasc Dis. 2003;15(3):159-66. doi: 10.1159/000068833[↩]
- Rondepierre P, Hamon M, Leys D, Leclerc X, Mounier-Vehier F, Godefroy O, Janssens E, Pruvo JP. Thromboses veineuses cérébrales: étude de l’évolution [Cerebral venous thromboses: study of the course]. Rev Neurol (Paris). 1995 Feb;151(2):100-4. French.[↩][↩]
- Preter M, Tzourio C, Ameri A, Bousser MG. Long-term prognosis in cerebral venous thrombosis. Follow-up of 77 patients. Stroke. 1996 Feb;27(2):243-6. doi: 10.1161/01.str.27.2.243[↩][↩][↩]
- de Bruijn SF, de Haan RJ, Stam J. Clinical features and prognostic factors of cerebral venous sinus thrombosis in a prospective series of 59 patients. For The Cerebral Venous Sinus Thrombosis Study Group. J Neurol Neurosurg Psychiatry. 2001 Jan;70(1):105-8. doi: 10.1136/jnnp.70.1.105[↩][↩]
- Ferro JM, Lopes MG, Rosas MJ, Ferro MA, Fontes J; Cerebral Venous Thrombosis Portugese Collaborative Study Group. Long-term prognosis of cerebral vein and dural sinus thrombosis. results of the VENOPORT study. Cerebrovasc Dis. 2002;13(4):272-8. doi: 10.1159/000057855[↩][↩]
- Breteau G, Mounier-Vehier F, Godefroy O, Gauvrit JY, Mackowiak-Cordoliani MA, Girot M, Bertheloot D, Hénon H, Lucas C, Leclerc X, Fourrier F, Pruvo JP, Leys D. Cerebral venous thrombosis 3-year clinical outcome in 55 consecutive patients. J Neurol. 2003 Jan;250(1):29-35. doi: 10.1007/s00415-003-0932-4[↩][↩]
- Cakmak S, Derex L, Berruyer M, Nighoghossian N, Philippeau F, Adeleine P, Hermier M, Froment JC, Trouillas P. Cerebral venous thrombosis: clinical outcome and systematic screening of prothrombotic factors. Neurology. 2003 Apr 8;60(7):1175-8. doi: 10.1212/01.wnl.0000055811.05743.10[↩][↩]
- Villringer A, Mehraein S, Einhäupl KM. Pathophysiological aspects of cerebral sinus venous thrombosis (SVT). J Neuroradiol. 1994 Apr;21(2):72-80. English, French.[↩][↩]
- Allroggen H, Abbott RJ. Cerebral venous sinus thrombosis. Postgrad Med J. 2000 Jan;76(891):12-5. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1741463/pdf/v076p00012.pdf[↩]
- Nakagawa, Seneka. (2014). Detailed structure of the venous drainage of the brain: relevance to accidental and non-accidental traumatic head injuries. https://eprints.nottingham.ac.uk/14443/1/PhD_Thesis_-_FINAL_-_21.07.14.pdf[↩]
- Bayot ML, Reddy V, Zabel MK. Neuroanatomy, Dural Venous Sinuses. [Updated 2023 Aug 8]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK482257[↩][↩][↩][↩][↩]
- Karakas AB, Govsa F, Ozer MA, Eraslan C. 3D Brain Imaging in Vascular Segmentation of Cerebral Venous Sinuses. J Digit Imaging. 2019 Apr;32(2):314-321. doi: 10.1007/s10278-018-0125-4[↩]
- Ngnitewe Massa R, Minutello K, Mesfin FB. Neuroanatomy, Cavernous Sinus. [Updated 2023 Jul 24]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK459244[↩]
- Graffeo CS, Perry A, Copeland WR 3rd, Raghunathan A, Link MJ. Histology of the distal dural ring. Clin Anat. 2017 Sep;30(6):742-746. doi: 10.1002/ca.22916[↩]
- Looking deep into cerebral venous system: Is that a pathology or just a normal variant? https://epos.myesr.org/poster/esr/ecr2020/C-07764[↩][↩]
- Mattle HP, Wentz KU, Edelman RR, Wallner B, Finn JP, Barnes P, Atkinson DJ, Kleefield J, Hoogewoud HM. Cerebral venography with MR. Radiology. 1991 Feb;178(2):453-8. doi: 10.1148/radiology.178.2.1987608[↩]
- Ayanzen RH, Bird CR, Keller PJ, McCully FJ, Theobald MR, Heiserman JE. Cerebral MR venography: normal anatomy and potential diagnostic pitfalls. AJNR Am J Neuroradiol. 2000 Jan;21(1):74-8. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7976366[↩]
- Balik V, et al. Variability in wall thickness and related structures of major dural sinuses in posterior cranial fossa: a microscopic anatomical study and clinical implications. Operative neurosurgery (Hagerstown, Md.) 2019;17:88–96. doi: 10.1093/ons/opz086[↩]
- The Venous Drainage of the Central Nervous System. https://teachmeanatomy.info/neuroanatomy/vessels/venous-drainage[↩][↩]
- Patel CR, Fernandez-Miranda JC, Wang WH, Wang EW. Skull Base Anatomy. Otolaryngol Clin North Am. 2016 Feb;49(1):9-20. doi: 10.1016/j.otc.2015.09.001[↩]
- Kiyofuji S, Perry A, Graffeo CS, Giannini C, Link MJ. The dangers of the “Head Down” position in patients with untreated pituitary macroadenomas: case series and review of literature. Pituitary. 2018 Jun;21(3):231-237. doi: 10.1007/s11102-017-0851-5[↩]
- Taniguchi D, Nakajima S, Hayashida A, Kuroki T, Eguchi H, Machida Y, Hattori N, Miwa H. Deep cerebral venous thrombosis mimicking influenza-associated acute necrotizing encephalopathy: a case report. J Med Case Rep. 2017 Sep 26;11(1):281. doi: 10.1186/s13256-017-1444-7[↩]
- Choi KY, Yang CJ. A case report of cavernous sinus thrombosis after trauma. Int J Pediatr Otorhinolaryngol. 2017 Apr;95:101-103. doi: 10.1016/j.ijporl.2017.02.007[↩]
- Leite J, Ribeiro A, Gonçalves D, Sargento-Freitas J, Trindade L, Duque V. Cerebral Venous Thrombosis as Rare Presentation of Herpes Simplex Virus Encephalitis. Case Rep Infect Dis. 2019 Jan 17;2019:7835420. doi: 10.1155/2019/7835420[↩]
- Taneda K, Adachi T, Watanabe Y, Hanajima R. Cerebral Venous Thrombosis due to Nontyphoidal Salmonella Bacteremia. Intern Med. 2019 Jul 1;58(13):1943-1946. doi: 10.2169/internalmedicine.2266-18[↩]
- Ulivi L, Squitieri M, Cohen H, Cowley P, Werring DJ. Cerebral venous thrombosis: a practical guide. Pract Neurol. 2020 Oct;20(5):356-367. doi: 10.1136/practneurol-2019-002415[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Mikulenka P, Peisker T, Vasko P, Stetkarova I. Diagnosis of cerebral venous thrombosis: a single centre experience. Neuro Endocrinol Lett. 2019 Jan;39(6):473-479.[↩]
- Martín-Masot R, Ortiz Pérez P, Serrano Nieto J, Martínez León M, Pascual Martínez A, Blasco-Alonso J, Navas-López VM. Central Venous Sinus Thrombosis in a Boy With Acute Severe Ulcerative Colitis. Front Pediatr. 2019 Feb 1;7:19. doi: 10.3389/fped.2019.00019[↩]
- Rizk JG, Gupta A, Sardar P, et al. Clinical Characteristics and Pharmacological Management of COVID-19 Vaccine–Induced Immune Thrombotic Thrombocytopenia With Cerebral Venous Sinus Thrombosis: A Review. JAMA Cardiol. 2021;6(12):1451–1460. doi:10.1001/jamacardio.2021.3444[↩]
- Poon CS, Chang JK, Swarnkar A, Johnson MH, Wasenko J. Radiologic diagnosis of cerebral venous thrombosis: pictorial review. AJR Am J Roentgenol. 2007 Dec;189(6 Suppl):S64-75. doi: 10.2214/AJR.07.7015[↩][↩]
- Canedo-Antelo M, Baleato-González S, Mosqueira AJ, Casas-Martínez J, Oleaga L, Vilanova JC, Luna-Alcalá A, García-Figueiras R. Radiologic Clues to Cerebral Venous Thrombosis. Radiographics. 2019 Oct;39(6):1611-1628. doi: 10.1148/rg.2019190015[↩][↩][↩]
- Aarju G, Birinder Singh P, Vipin K, Alisha S, Gunchan P. Neurological Predictors of Functional Outcome in Cortical Venous Sinus Thrombosis. J Neurosci Rural Pract. 2022 Mar 10;13(2):290-294. doi: 10.1055/s-0042-1744123[↩]
- Weimar C, Holzhauer S, Knoflach M, Koennecke HC, Masuhr F, Mono ML, Niederstadt T, Nowak-Göttl U, Schellong SM, Kurth T. Zerebrale Venen- und Sinusthrombose : S2k-Leitlinie [Cerebral venous and sinus thrombosis : S2k guidelines]. Nervenarzt. 2019 Apr;90(4):379-387. German. doi: 10.1007/s00115-018-0654-6[↩]
- Monagle P, Newall F. Management of thrombosis in children and neonates: practical use of anticoagulants in children. Hematology Am Soc Hematol Educ Program. 2018 Nov 30;2018(1):399-404. doi: 10.1182/asheducation-2018.1.399[↩]
- Monagle P, Cuello CA, Augustine C, Bonduel M, Brandão LR, Capman T, Chan AKC, Hanson S, Male C, Meerpohl J, Newall F, O’Brien SH, Raffini L, van Ommen H, Wiernikowski J, Williams S, Bhatt M, Riva JJ, Roldan Y, Schwab N, Mustafa RA, Vesely SK. American Society of Hematology 2018 Guidelines for management of venous thromboembolism: treatment of pediatric venous thromboembolism. Blood Adv. 2018 Nov 27;2(22):3292-3316. doi: 10.1182/bloodadvances.2018024786[↩]
- Wangqin R, Laskowitz DT, Wang Y, Li Z, Wang Y, Liu L, Liang L, Matsouaka RA, Saver JL, Fonarow GC, Bhatt DL, Smith EE, Schwamm LH, Prvu Bettger J, Hernandez AF, Peterson ED, Xian Y. International Comparison of Patient Characteristics and Quality of Care for Ischemic Stroke: Analysis of the China National Stroke Registry and the American Heart Association Get With The Guidelines–Stroke Program. J Am Heart Assoc. 2018 Oct 16;7(20):e010623. doi: 10.1161/JAHA.118.010623[↩]
- Heldner MR, Zuurbier SM, Li B, Von Martial R, Meijers JCM, Zimmermann R, Volbers B, Jung S, El-Koussy M, Fischer U, Kohler HP, Schroeder V, Coutinho JM, Arnold M. Prediction of cerebral venous thrombosis with a new clinical score and D-dimer levels. Neurology. 2020 Aug 18;95(7):e898-e909. doi: 10.1212/WNL.0000000000009998[↩]
- Boukobza M, Crassard I, Bousser MG, Chabriat H. MR imaging features of isolated cortical vein thrombosis: diagnosis and follow-up. AJNR Am J Neuroradiol. 2009 Feb;30(2):344-8. doi: 10.3174/ajnr.A1332[↩]
- Ferro JM, Canhão P, Stam J, Bousser MG, Barinagarrementeria F; ISCVT Investigators. Prognosis of cerebral vein and dural sinus thrombosis: results of the International Study on Cerebral Vein and Dural Sinus Thrombosis (ISCVT). Stroke. 2004 Mar;35(3):664-70. doi: 10.1161/01.STR.0000117571.76197.26[↩]
- Saposnik G, Barinagarrementeria F, Brown RD Jr, Bushnell CD, Cucchiara B, Cushman M, deVeber G, Ferro JM, Tsai FY; American Heart Association Stroke Council and the Council on Epidemiology and Prevention. Diagnosis and management of cerebral venous thrombosis: a statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2011 Apr;42(4):1158-92. doi: 10.1161/STR.0b013e31820a8364[↩]
- Herrmann KA, Sporer B, Yousry TA. Thrombosis of the internal cerebral vein associated with transient unilateral thalamic edema: a case report and review of the literature. AJNR Am J Neuroradiol. 2004 Sep;25(8):1351-5. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7975461[↩]
- Rodallec MH, Krainik A, Feydy A, Hélias A, Colombani JM, Jullès MC, Marteau V, Zins M. Cerebral venous thrombosis and multidetector CT angiography: tips and tricks. Radiographics. 2006 Oct;26 Suppl 1:S5-18; discussion S42-3. doi: 10.1148/rg.26si065505[↩][↩]
- José M. Ferro, Helena Bacelar-Nicolau, Teresa Rodrigues, Leonor Bacelar-Nicolau, Patrícia Canhão, Isabelle Crassard, Marie-Germaine Bousser, Aurélio Pimenta Dutra, Ayrton Massaro, Marie-Anne Mackowiack-Cordiolani, Didier Leys, João Fontes, Jan Stam, Fernando Barinagarrementeria; Risk Score to Predict the Outcome of Patients with Cerebral Vein and Dural Sinus Thrombosis. Cerebrovasc Dis 1 June 2009; 28 (1): 39–44. https://doi.org/10.1159/000215942[↩]
- Coutinho JM, Zuurbier SM, Stam J. Declining mortality in cerebral venous thrombosis: a systematic review. Stroke. 2014 May;45(5):1338-41. doi: 10.1161/STROKEAHA.113.004666[↩]
- Canhão P, Ferro JM, Lindgren AG, Bousser MG, Stam J, Barinagarrementeria F; ISCVT Investigators. Causes and predictors of death in cerebral venous thrombosis. Stroke. 2005 Aug;36(8):1720-5. doi: 10.1161/01.STR.0000173152.84438.1c[↩]
- Ferro JM, Bacelar-Nicolau H, Rodrigues T, Bacelar-Nicolau L, Canhão P, Crassard I, Bousser MG, Dutra AP, Massaro A, Mackowiack-Cordiolani MA, Leys D, Fontes J, Stam J, Barinagarrementeria F; ISCVT and VENOPORT investigators. Risk score to predict the outcome of patients with cerebral vein and dural sinus thrombosis. Cerebrovasc Dis. 2009;28(1):39-44. doi: 10.1159/000215942[↩]





{kind=link}