Contents
Slipped disc
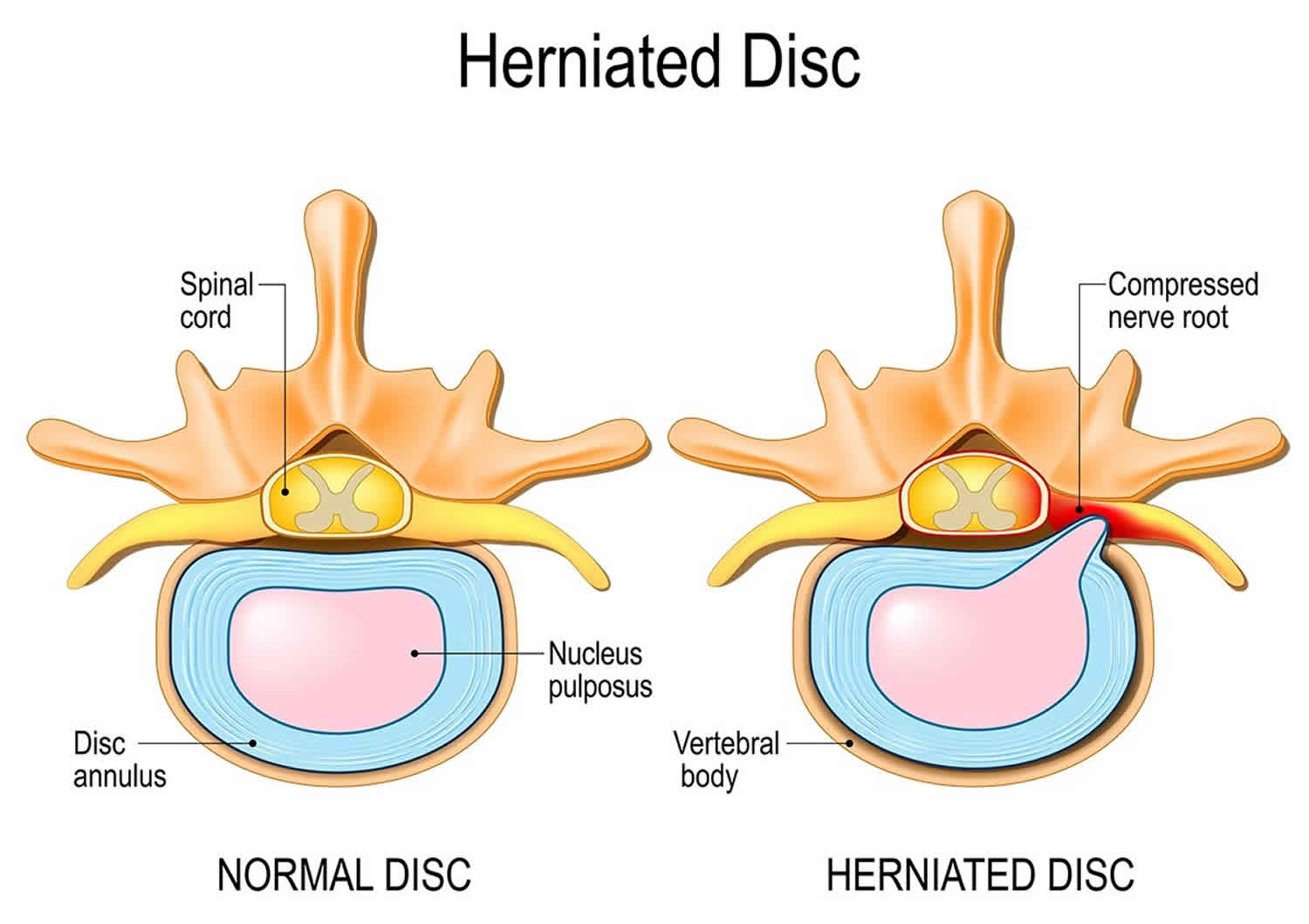
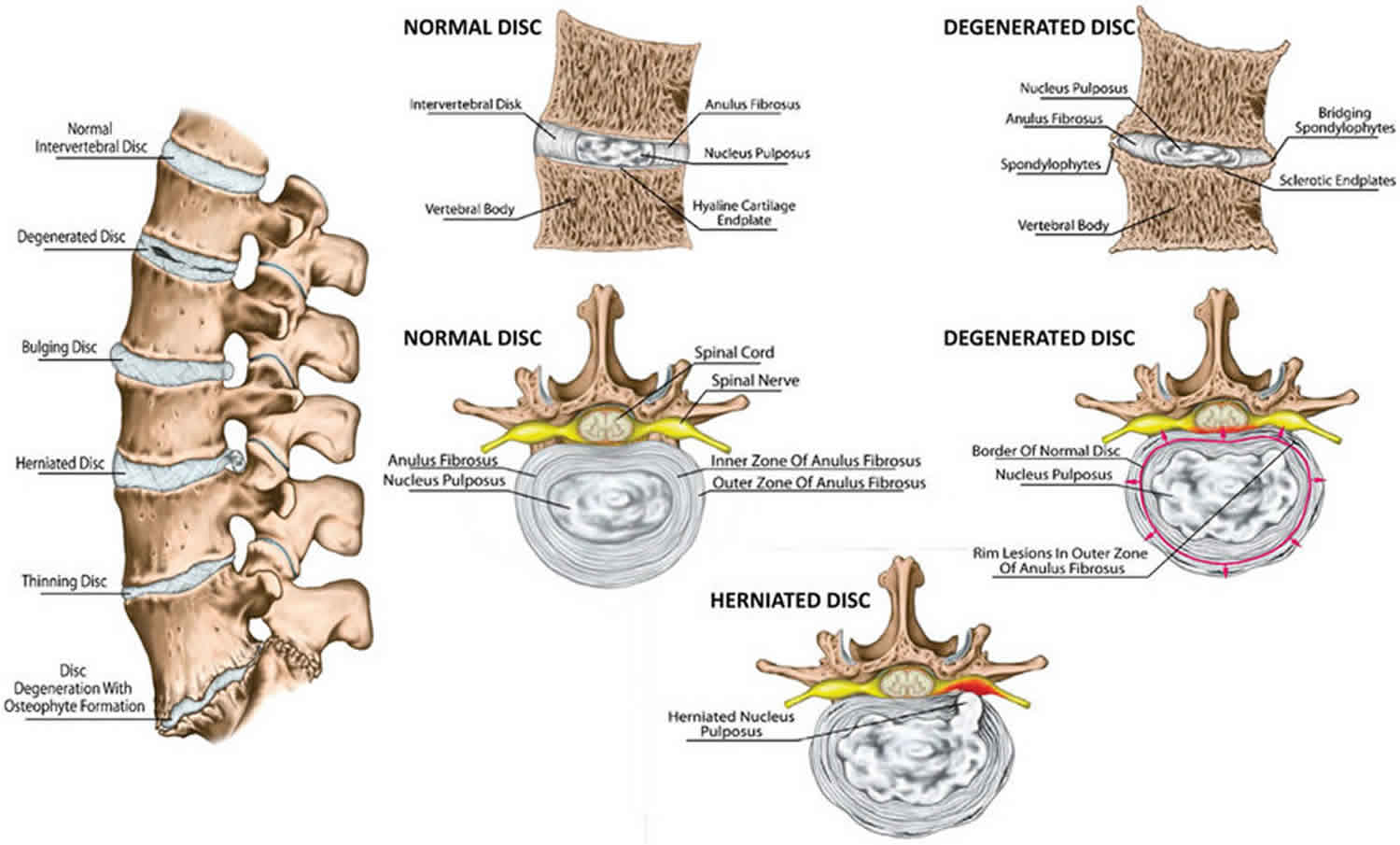
Slipped disc is also called herniated disc, spinal disc herniation, ruptured disc, bulging disc or protruding disc, is a painful medical condition that occurs in your spine (backbone) when some of the nucleus pulposus that fills the center of your intervertebral disc pushes out through a tear in the annulus (ring-shaped disc of fibrous connective tissue that surrounds the nucleus pulposus) (see Figure 1 c). The word “herniate” means to bulge or to stick out. This allows the jelly-like center of the disc to leak, irritating the nearby spinal nerves. These discs become a problem when the center of the disc pushes against a nerve or the spinal cord. Spinal nerves are very sensitive to even slight amounts of pressure, which can result in pain that can vary from mild to severe, numbness, or weakness in one or both legs. This can cause sciatica or back pain and other problems.
- Although a slipped disc (herniated disc) can sometimes be very painful, most people feel much better with just a few months of simple, nonsurgical treatments.
- Not all slipped discs (herniated discs) cause symptoms. Many people will never know they have slipped a disc.
Slipped discs (herniated discs) are most common in the lumbar spine — the lower part of your backbone, between the bottom of your ribs and your hips. They can also happen cervical area (your neck). The discs in your upper-to-mid back (thoracic area) are rarely involved.
A slipped disc (herniated disc) can cause:
- lower back pain – the most common symptom
- numbness or tingling in your shoulders, back, arms, hands, legs or feet
- neck pain
- problems bending or straightening your back
- muscle weakness
- pain in the buttocks, hips or legs if the disc is pressing on the sciatic nerve (sciatica)
Your doctor will diagnose a slipped disc (herniated disc) with a physical exam and, sometimes, imaging tests. With treatment, most people recover. Treatments include rest, pain and anti-inflammatory medicines, physical therapy, and sometimes surgery.
Risk Factors for slipped disc (herniated disc)
In children and young adults, discs have high water content. As people age, the water content in the discs decreases and the discs become less flexible. The discs begin to shrink and the spaces between the vertebrae get narrower. Conditions that can weaken the disc include:
- Improper lifting
- Smoking
- Excessive body weight that places added stress on the discs (in the lower back)
- Sudden pressure (which may be slight)
- Repetitive strenuous activities
Other types of spinal disc problems include:
- degenerative disc disease, which is the natural change that happen to your discs as you age, and is not really a disease
- injury from falls or accidents
- infection
- cancers that affect the spine.
Other causes of back pain
Sometimes the pain may be a result of an injury such as a sprain or strain but often there’s no obvious reason. Back pain is rarely caused by anything serious.
Nonsurgical treatment is effective in treating the symptoms of slipped discs (herniated discs) in the majority of patients. Most neck or back pain will resolve gradually with simple measures.
- Rest and over-the-counter pain relievers may be all that is needed.
- Muscle relaxers, analgesics, and anti-inflammatory medications are also helpful.
- Cold compresses or ice can also be applied several times a day for no more than 20 minutes at a time.
- After any spasms settle, gentle heat applications may be used.
See your doctor right away if you have any of the following symptoms:
- have numbness around your bottom or genitals
- can’t urinate
- lose feeling in one or both feet or legs
- loss of bowel or bladder function
- ave a very high temperature or you feel hot and shivery
- have unexplained weight loss
- have a swelling in your back
- notice the pain is worse at night
- got it after a serious accident, such as a car accident
- more pain or weakness than usual in your backbone.
These could be signs of complications or a more serious problem.
What is intervertebral disc
Intervertebral discs (inter- = between) are found between the bodies of adjacent vertebrae from the second cervical (C2) vertebra to the sacrum (see Figures 1 to 4) and collectively, the intervertebral discs account for about 25% to 33% of the height of the vertebral column. There are 25 intervertebral discs (7 cervical, 12 thoracic, 5 lumbar, and 1 sacral). There is no intervertebral disc between C1 and C2, which is unique in the spine 1. Together the vertebrae and the discs surround and protect your spinal cord, the bundle of nerves that connects your brain to the nerves in your body (see Figures 1 and 2). Each intervertebral disc is a cushionlike pad composed of an inner soft, pulpy, highly elastic substance, the nucleus pulposus (pulposus = pulplike) and an outer fibrous ring of about 12 concentric rings consisting of fibrocartilage called the anulus fibrosus (“fibrous ring”) (annulus = ringlike). The main function of these fibrous rings (anulus fibrosus) is to contain the nucleus pulposus (the inner soft, pulpy, highly elastic substance), limiting its expansion when the spine is compressed. However, the fibrocartilage rings (anulus fibrosus) also function like a woven strap, binding the successive vertebrae together, resisting tension on the spine, and absorbing compressive forces.
- The anulus fibrosus is a ring-shaped disc of fibrous connective tissue that surrounds the nucleus pulposus. This structure is highly organized, consisting of 15 to 25 stacked sheets, or “lamellae,” of predominantly collagen, with interspersed proteoglycans, glycoproteins, elastic fibers, and the connective tissue cells that secrete these extracellular matrix products. Each lamella contains collagen uniformly oriented in a plane that differs in orientation to adjacent lamella by about 60 degrees. This alignment leads to the parallel orientation of alternate lamella. This “radial-ply” formation provides exceptional strength compared to an entirely longitudinal setup and has been mimicked in the construction of products such as car tires. The lamellae are interconnected through translamellar bridges. The number of translamellar bridges per unit area is set to achieve a balance between strength and flexibility. A greater number of bridges would provide greater resistance to compressive forces, but would limit flexibility, and vice-versa. The anulus fibrosus contains an inner and an outer portion. They differ primarily in their collagen composition. While both are primarily collagen, the outer annulus contains mostly type I collagen, while the inner has predominantly type II. The inner annulus also contains more proteoglycans than the inner. The ratio of type I to type II changes gradually; as the distance from the nucleus pulposus increases, the amount of type II collagen decreases, while the amount of type I increases. Another major difference between the two segments is the morphology of the connective tissue cells that secrete extracellular matrix. The cells of the inner annulus are described as round, while the outer annulus has a more oblong, fibroblast-like appearance 2.
- The nucleus pulposus fills the center of the intervertebral disc, is gelatinous, and absorbs compression forces between vertebrae. The nucleus pulposus is a gel-like structure that sits at the center of the intervertebral disc and accounts for much of the strength and flexibility of the spine. It is made of 66% to 86% water with the remainder consisting of primarily type II collagen (it may also contain type VI, IX, and XI) and proteoglycans. The proteoglycans include the larger aggrecan and versican that bind to hyaluronic acid, as well as several small leucine-rich proteoglycans. Aggrecan is largely responsible for retaining water within the nucleus pulposus. This structure also contains a low density of cells. While sparse, these cells produce the extracellular matrix (ECM) products (aggrecan, type II collagen, etc.) and maintain the integrity of the nucleus pulposus.
The superior (top) and inferior (bottom) surfaces of the intervertebral disc consist of a thin plate of hyaline cartilage endplates that anchor the discs to adjacent vertebrae 3. Collagen fibers in adjacent rings in the anulus cross like an X, allowing the spine to withstand twisting. This arrangement creates the same antitwisting design provided by bone lamellae in osteons (see Figure 3). Each nucleus pulposus is gelatinous and acts like a rubber ball, enabling the spine to absorb compressive stress.
The intervertebral discs form strong joints, permit various movements of the vertebral column, and absorb vertical shock. Under compression, they flatten and broaden. Degenerative changes in the anulus fibrosus can lead to herniation of the nucleus pulposus. Posterolateral herniation can impinge on the roots of a spinal nerve in the intervertebral foramen.
The intervertebral discs act as shock absorbers during walking, jumping, and running. At points of compression, the discs flatten and bulge out a bit between the vertebrae. The discs are thickest in the lumbar (lower back) and cervical (neck) regions of the vertebral column. As a result of compression and loss of fluid from the gelatinous nucleus pulposus, they flatten somewhat by the end of each day. So, you are probably 1 to 2 centimeters shorter at night than when you awake in the morning.
During the course of a day the discs compress and lose water from their cartilage so that we are a bit shorter at night. While you are sleeping there is less compression and rehydration occurs, so that you are taller when you awaken in the morning. With age, the nucleus pulposus hardens and becomes less elastic. Decrease in vertebral height with age results from bone loss in the vertebral bodies and not a decrease in thickness of the intervertebral discs.
Since intervertebral discs are avascular, the annulus fibrosus and nucleus pulposus rely on blood vessels from the bodies of vertebrae to obtain oxygen and nutrients and remove wastes. Certain stretching exercises, such as yoga, decompress discs and increase general blood circulation, both of which speed up the uptake of oxygen and nutrients by discs and the removal of wastes.
The vertebral column, or spine (see Figure 4), physically supports the skull and trunk, allows for their movement, protects the spinal cord and absorbs stresses produced by walking, running, and lifting. It also provides attachment for the limbs, thoracic cage, and postural muscles. Although commonly called the backbone, it consists of not a single bone but a flexible chain of 33 vertebrae with intervertebral discs of fibrocartilage between most of them. The adult vertebral column averages about 71 cm (28 in.) long, with the intervertebral discs accounting for about one-quarter of the length.
During the course of a day the discs compress and lose water from their cartilage so that we are a bit shorter at night. While you are sleeping there is less compression and rehydration occurs, so that you are taller when you awaken in the morning. With age, the nucleus pulposus hardens and becomes less elastic. Decrease in vertebral height with age results from bone loss in the vertebral bodies and not a decrease in thickness of the intervertebral discs.
Intervertebral disc thickness generally increases from rostral to caudal, except for a nadir at T3-T4. The thickness of the intervertebral discs relative to the size of the vertebral bodies is highest in the cervical and lumbar regions. This reflects the increased range of motion found in those regions.
In the cervical and lumbar regions, the intervertebral discs are thicker anteriorly. This creates the secondary curvature of the spine – the cervical and lumbar lordoses.
Since intervertebral discs are avascular, the annulus fibrosus and nucleus pulposus rely on blood vessels from the bodies of vertebrae to obtain oxygen and nutrients and remove wastes. Certain stretching exercises, such as yoga, decompress discs and increase general blood circulation, both of which speed up the uptake of oxygen and nutrients by discs and the removal of wastes.
While only the outer third of the anulus fibrosus is vascular and innervated in a non-pathologic state, in aging and states of inflammation, nerve growth and granulation tissue growth are stimulated. Additionally, the granulation tissue secretes inflammatory cytokines, which further increases sensitivity to pain sensations.
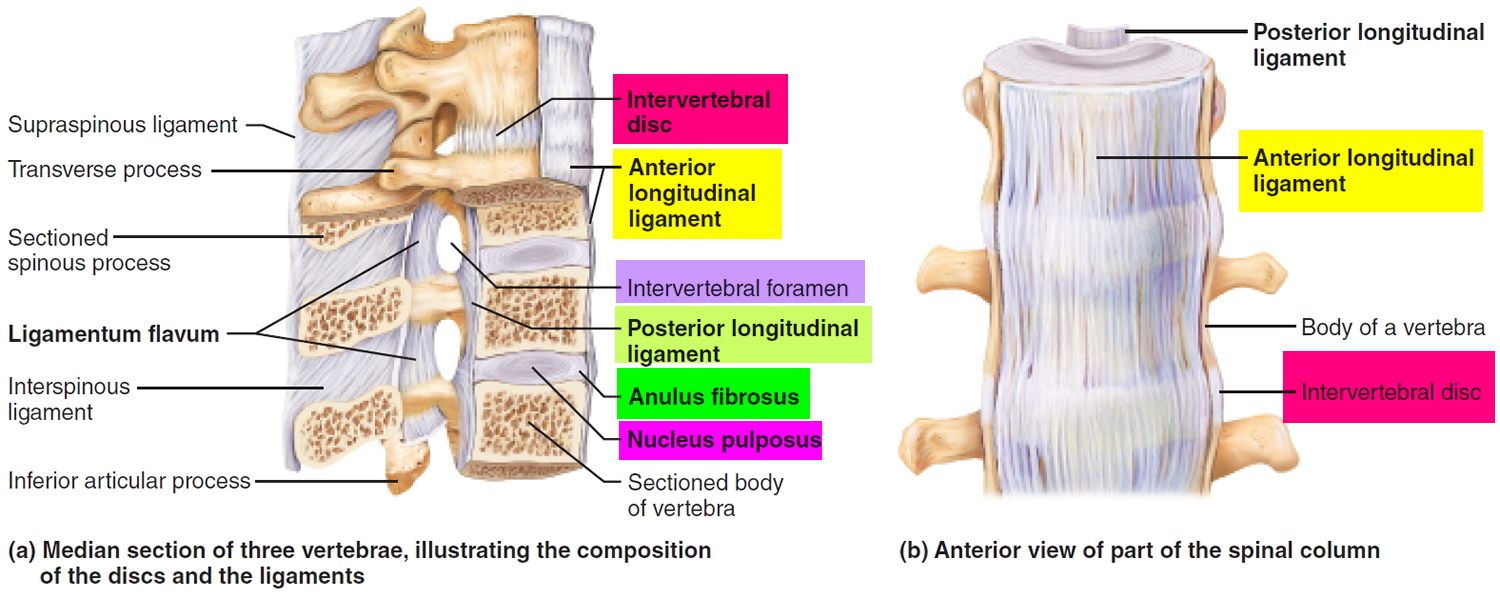
Two major ligaments support the intervertebral discs. The anterior longitudinal ligament is a broadband that covers the anterolateral surface of the spine from the foramen magnum in the skull to the sacrum. This ligament assists the spine in preventing hyperextension and prevents intervertebral disc herniation in the anterolateral direction. The posterior longitudinal ligament covers the posterior aspect of the vertebral bodies, within the vertebral canal, and serves mainly to prevent a posterior herniation of the intervertebral discs, and is therefore responsible for the most herniations being in the postero-lateral direction.
Figure 1. Intervertebral disc
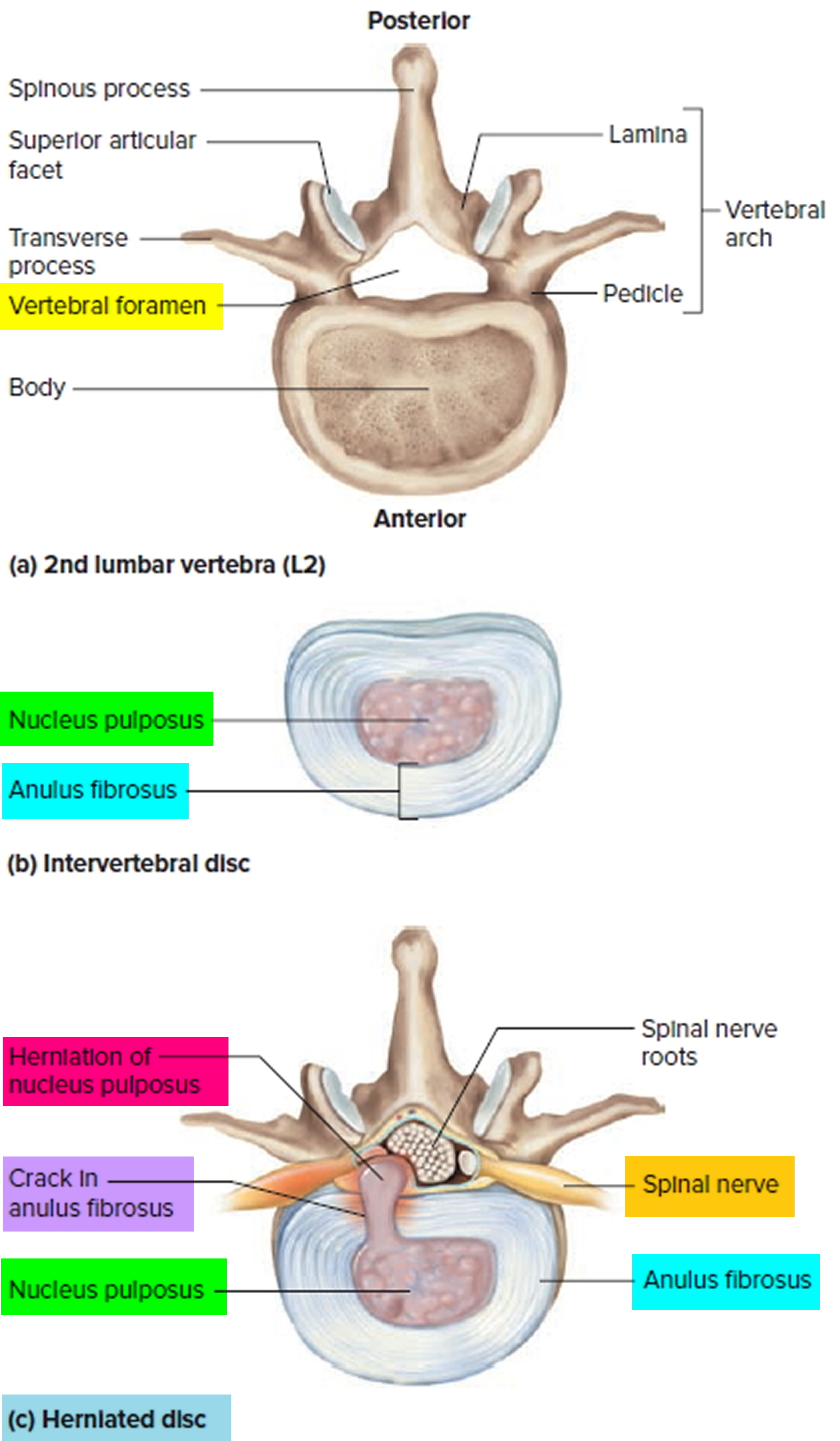
Figure 2. Structure of typical intervertebral disc
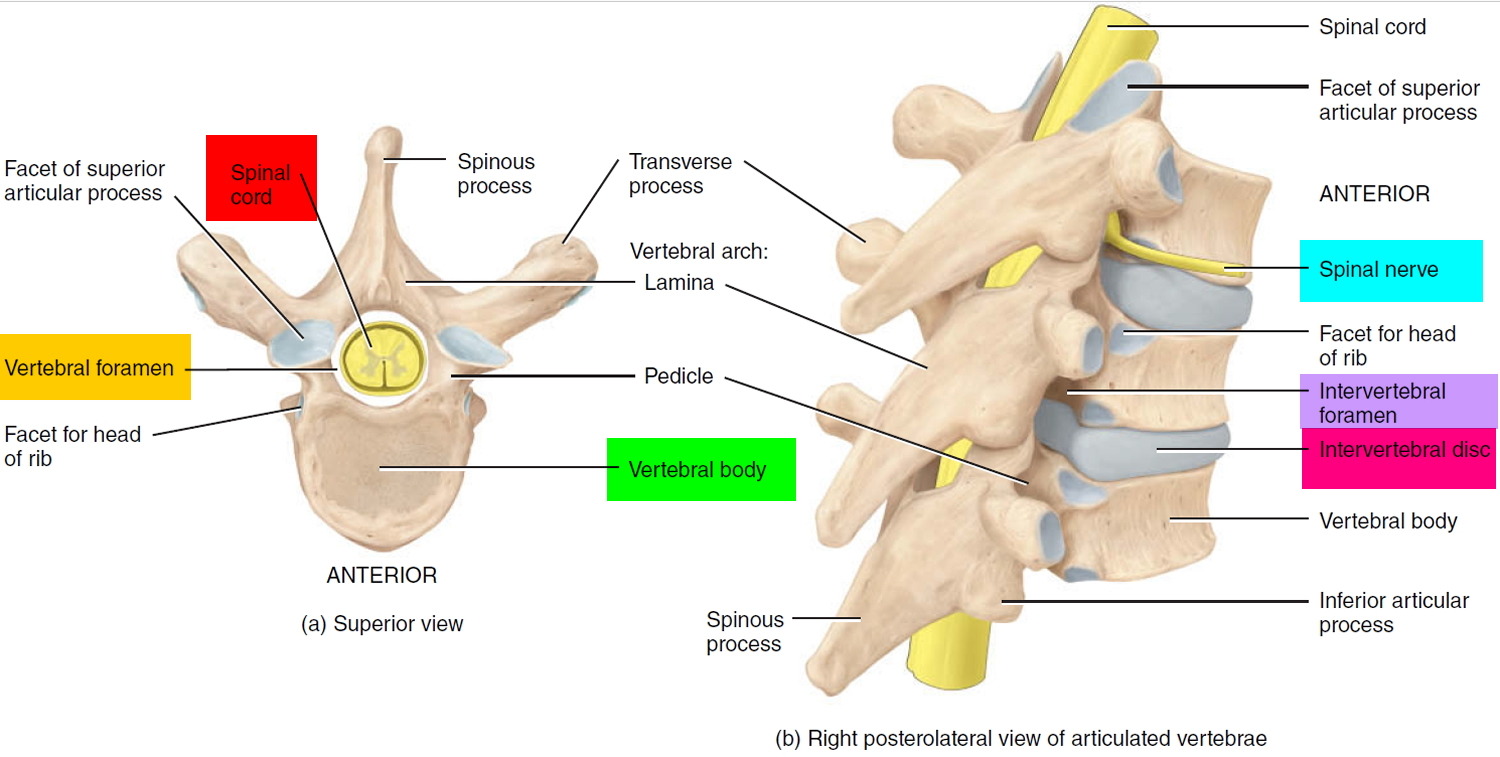
Figure 3. Fibrocartilage of a typical intervertebral disc
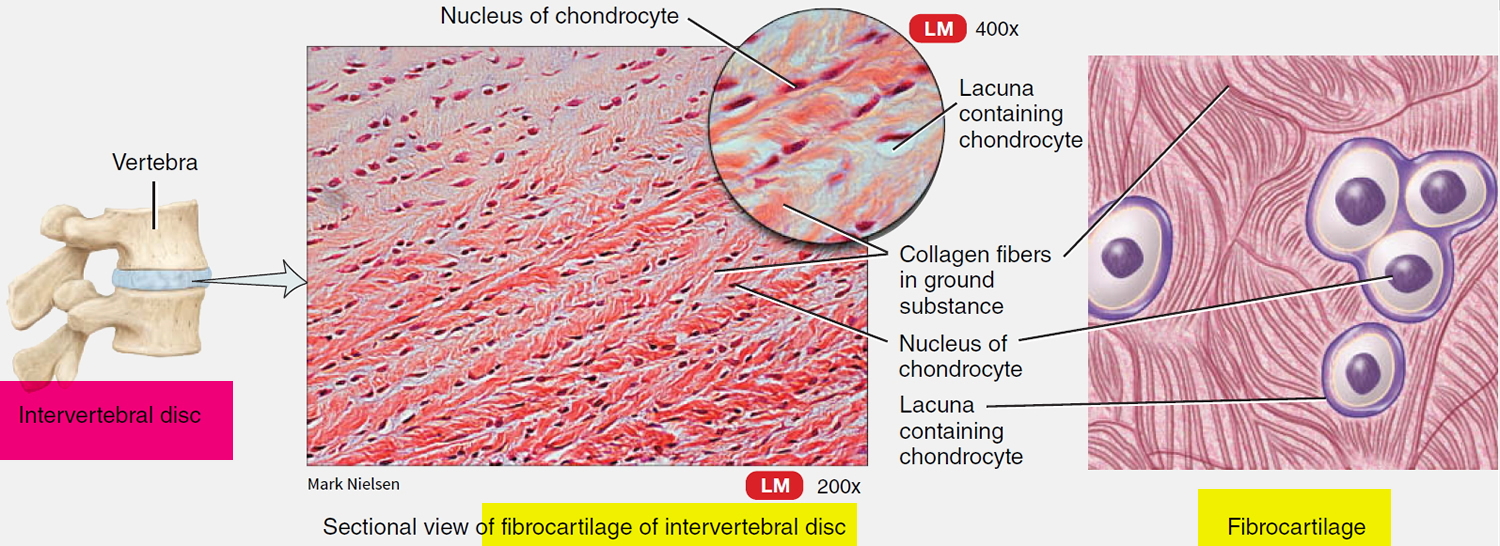
Figure 4. Structure of typical vertebral column
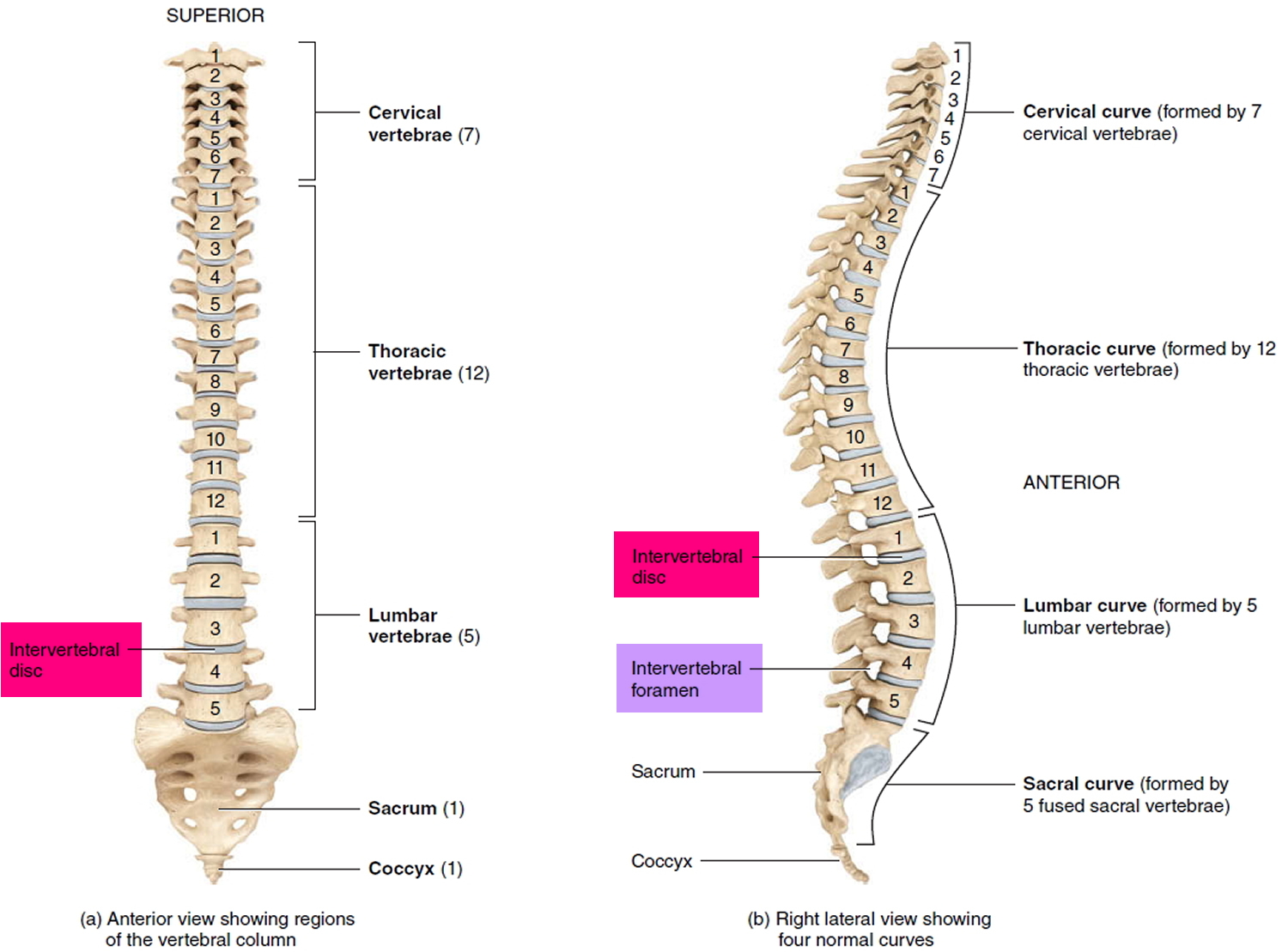
Figure 5. Intervertebral disc disease
Ligaments of the Spine
Like a tremulous telecommunication transmitting tower, the vertebral column cannot stand upright by itself. It must be held in place by an elaborate system of supports. Serving this role are the straplike ligaments of the back and the muscles of the trunk.
The major supporting ligaments are the anterior and posterior longitudinal ligaments (Figure 6) that run vertically along the anterior and posterior surfaces of the bodies of the vertebrae, from the neck to the sacrum. The anterior longitudinal ligament is wide and attaches strongly to both the bony vertebrae and the intervertebral discs. Along with its supporting role, this thick anterior ligament prevents hyperextension of the back (bending too far backward). The posterior longitudinal ligament, which is narrow and relatively weak, attaches only to the intervertebral discs. This ligament helps to prevent hyperflexion (bending the vertebral column too sharply forward).
Several other posterior ligaments connect each vertebra to those immediately superior and inferior (Figure 5 a). Among these is the ligamentum flavum (fla vum; “yellow”), which connects the lamina of adjacent vertebrae. It contains elastic connective tissue and is especially strong: It stretches as you bend forward, then recoils as you straighten to an erect position.
Figure 6. Ligaments of the spine
Intervertebral disc function
Intervertebral discs serve a number of vital functions in the form structural support and locomotion. Intervertebral discs allow the spine to be flexible without sacrificing a great deal of strength. Intervertebral discs also provide a shock-absorbing effect within the spine and prevent the vertebrae from grinding together. Within the intervertebral disc, itself, the separate components serve different purposes. The nucleus pulposus serves to distribute hydraulic pressure throughout the intervertebral disc. By virtue of its high water content, the nucleus pulposus can disperse the forces placed on one aspect of a vertebral body to the entire structure. A solid nucleus pulposus, in contrast, would transmit a force placed on one aspect of a vertebral body directly to the corresponding aspect of the inferior vertebral body, thus increasing the risk of trauma. The annulus fibrosus serves, for one, to encircle the nucleus pulposus as a “cage” to provide structure to the gelatinous form. The aforementioned “radial-ply” configuration allows for increased resistance to the compressive forces exerted upon it by the nucleus pulposus. Given the general rostral-caudal direction of the fibers, the annulus fibrosus also resists torsion, flexion and extension movements of the spine.
Holistically, the intervertebral discs first allow for the spine to be both a supportive, yet flexible structure. They provide separation and connectivity between vertebrae and counteract forces that act to lengthen or compress the spine or affect it in a torsional or shear manner. They also sufficiently separate the vertebrae to allow spinal nerves to exit the intervertebral foramina.
In a similar vein to the flexibility created by the intervertebral discs, they also have a protective effect on vertebrae. This “shock-absorbing” feature distributes forces throughout the spine – lessening the load on any one vertebra, thus reducing the risk of fracture and degenerative changes.
Slipped disc causes
The cause of slipped disc will depend on your type of spinal disc problem, such as prolapsed disc or degenerative disc disease.
Slipped disc is most often the result of a gradual, aging-related wear and tear called disc degeneration. As you age, your spinal discs lose some of their water content. That makes them less flexible and more prone to tearing or rupturing with even a minor strain or twist.
Most people can’t pinpoint the exact cause of their slipped disc. Sometimes, using your back muscles instead of your leg and thigh muscles to lift large, heavy objects can lead to a slipped disc, as can twisting and turning while lifting. Rarely, a traumatic event such as a fall or a blow to the back can cause a slipped disc.
The true cause is usually not known, but it is more common in people who:
- are middle-aged or older
- are male
- lift heavy objects
- are overweight or obese. Excess body weight causes extra stress on the discs in your lower back.
- do repetitive actions involving bending or twisting
- Occupation. People with physically demanding jobs have a greater risk of back problems. Repetitive lifting, pulling, pushing, bending sideways and twisting also may increase your risk of a herniated disc.
- sit in the same position for a long time regularly
- live an inactive lifestyle
- smoke
- Genetics. Some people inherit a predisposition to developing a herniated disc.
Causes of degenerative disc disease
This condition is more common as you age. People who have had spinal injuries or infections are also more likely to get degenerative disc disease.
Slipped disc prevention
There’s not much you can do to prevent a slipped disc. It is often caused by natural aging and deterioration. To keep your discs and back in good working order, work on living a healthy lifestyle:
- Keeping your body in the correct posture
- Avoiding heavy lifting
- Maintain a healthy weight.
- Exercise regularly.
- Regularly doing exercises to strengthen your core stomach and back muscles.
- void repetitive movements.
- If you sit all day make sure you have correct sitting position and get up and walk around every hour.
- Practice safe lifting and bending techniques.
If you have undiagnosed back problems, see your doctor.
Slipped disc complications
Your spinal cord doesn’t extend into the lower portion of your spinal canal. Just below your waist, the spinal cord separates into a group of long nerve roots (cauda equina) that resemble a horse’s tail. Rarely, slipped disc can compress the entire cauda equina. Emergency surgery may be required to avoid permanent weakness or paralysis.
Seek emergency medical attention if you have:
- Worsening symptoms. Pain, numbness or weakness may increase to the point that you can’t perform your usual daily activities.
- Bladder or bowel dysfunction. People who have cauda equina syndrome may become incontinent or have difficulty urinating even with a full bladder.
- Saddle anesthesia. This progressive loss of sensation affects the areas that would touch a saddle — the inner thighs, back of legs and the area around the rectum.
Slipped disc signs and symptoms
When part of a disc presses on a nerve, it can cause pain. Often the pain occurs on one side of your body. Where the pain is located depends on where the slipped disc is located.
A slipped disc in the cervical section (neck) of your spine can cause pain in your neck and arms. You could experience:
- Pain when moving your neck
- Pain near the shoulder blade
- Shooting pain down the arm and into the fingers
- Numbness in the shoulder, elbow, forearm, or fingers
- Weakness
A slipped disc in the lumbar part of your spine (lower back) can cause pain in the back and legs. It is often referred to as sciatica. This is because the disc pushes on the sciatic nerve, which runs down your leg. Symptoms include:
- Pain in the leg, hip, or buttocks
- Numbness in these areas
- Pain or numbness in the back of the calf or sole of the foot
- Weakness in one leg
How bad the symptoms are depends on how much of the disc is pressing on the nerve. The pain from a slipped disc is usually worse when you’re active and gets better when you’re resting. Coughing, sneezing, sitting, driving, and bending forward may make the pain worse. These movements put more pressure on the nerve. People who have painful slipped discs often try to change positions to reduce the pain.
Slipped disc diagnosis
Your doctor will ask you questions about your symptoms and give you an exam.
After discussing your symptoms and medical history, your doctor will examine your spine, check you for numbness, weakness, reflexes, and pain. During the physical examination, your doctor may conduct the following tests to help determine the cause of your low back pain.
Neurological examination. A physical examination should include a neurological examination to detect weakness or sensory loss. To test muscle weakness, your doctor will assess how you walk on your heels and toes. Your thigh, ankle, and toe strength may also be tested. Your doctor can detect any loss of sensation by checking whether you are numb to light touch in the leg and foot. In addition, your reflexes at the knee and ankle will be tested, and sometimes may be absent.
Straight leg raise (SLR) test. This test is a very accurate predictor of a disc herniation in patients under the age of 35. In this test, you lie on your back and your doctor lifts your affected leg. Your knee stays straight. If you feel pain down your leg and below the knee, you test positive for a herniated disc.
The straight leg raise (SLR) is positive when it reproduces the patient’s symptoms (pain and paresthesia) at an angle lower than 45 degrees with radiation below the knee (Lasegue sign). It is most helpful in diagnosing L4, L5, and S1 radiculopathies. The patient is asked to dorsiflex the foot while the examiner is raising the leg (Bragaad’s sign) to increase the sensitivity of the test.
L1 nerve root exits at the L1-L2 foramina, assessed with a cremasteric reflex (male). When compressed by a herniated disc, it causes pain, and sensory loss in the inguinal region rarely causes weakness in the hip flexion.
The L2 and L3 nerve roots exit at the L2-L3 and L3-L4 foramina, respectively. Symptoms worsen with sneezing, coughing, or leg straightening.
L4 nerve root exits at the L4-L5 foramina. L4 has a reflex assessed with a patellar reflex. When compressed by a herniated disc, it causes back pain that radiates into the anterior thigh and the medial aspect of the leg, accompanied with sensory loss in the same distribution, weakness in the hip flexion and adduction, weakness in knee extension, and a decreased patellar reflex.
L5 nerve root exits at the L5-S1 foramina. When compressed by a herniated disc, it causes back pain that radiates into the buttock, lateral thigh, lateral calf, the dorsum of the foot, and the great toe. Sensory loss is present on the web space between the big toe and second toe, the dorsum of the foot, and lateral calf. There is a weakness in hip abduction, knee flexion, foot dorsiflexion, big toe dorsiflexion, foot inversion, and eversion. Patients present with decreased semitendinosus/semimembranosus reflex. Weakness in foot dorsiflexion makes it challenging to walk on the heels. Chronic L5 radiculopathy may cause atrophy of the extensor digitorum brevis and the tibialis anterior of the anterior leg.
S1 nerve root exits at the S1-S2 foramina, assessed with the Achilles reflex. When compressed with a herniated disc, it presents with sacral or buttock pain that radiates into the posterolateral thigh, the calf, plantar or lateral foot or the perineum. Sensory loss is present on the calf, lateral, or plantar aspect of the foot. There is weakness on foot plantar flexion, hip extension, and flexion of the knee. Weakness in foot plantar flexion causes an inability to tiptoe walk. It could also cause urinary and fecal incontinence and sexual dysfunction 4, 5, 6.
Your doctor will probably order X-rays or imaging tests to see whether you have a herniated disc. These could include a CT scan, an MRI scan or a myelogram. A myelogram is where a dye is injected into the spinal fluid, and then X-rays are taken. This test can show pressure on your spinal cord or nerves due to multiple herniated discs or other conditions. This is to rule out any potential rare causes, including spinal cancer, bone growths (spurs), fracture or narrowing of spinal canal (stenosis). There are also nerve tests your doctor can order. These can determine what nerves are involved, if there is nerve damage, and how well your nerves are conducting feelings.
Slipped disc differential diagnosis
The differential diagnoses for a slipped disc include 4:
- Discal cyst
- Mechanical back pain
- Degenerative spinal stenosis
- Epidural abscess
- Epidural hematoma
- Metastasis
- Diabetic amyotrophy
- Neurinoma
- Osteophytes
- Cauda equina syndrome
- Synovial cyst
Slipped disc treatment
There are a number of steps that can be taken to treat a slipped disc.
Conservative treatment — mainly avoiding painful positions and following a planned exercise and pain-medication regimen — relieves symptoms in most people within a few days or weeks.
Medications
Your doctor may recommend over-the-counter pain medicine like acetaminophen (Tylenol, others), ibuprofen (Advil, Motrin IB, others) or naproxen sodium (Aleve). He or she may prescribe you pain medicine, such as a narcotic, to help with severe pain. They may also give you muscle relaxants to help relieve muscle spasms that can increase pain.
Narcotics (Opioids). If your pain doesn’t improve with over-the-counter medications, your doctor might prescribe opioids (narcotics), such as codeine or an oxycodone-acetaminophen combination (Percocet, OxyContin, others), for a short time. Sedation, nausea, confusion and constipation are possible side effects from these drugs. However, because of the side effects of opioids (narcotics) and the potential for addiction, many health care professionals hesitate to prescribe them for disc herniation.
Neuropathic drugs. These drugs affect nerve impulses to decrease pain. The drugs originally designed to control seizures also may be helpful in the treatment of the radiating nerve pain often associated with a herniated disc. They include gabapentin (Horizant, Neurontin), pregabalin (Lyrica), duloxetine (Cymbalta), or venlafaxine (Effexor XR).
Muscle relaxers. You might be prescribed these if you have muscle spasms. Sedation and dizziness are common side effects.
Cortisone injections (steroid injections). If your pain doesn’t improve with oral medicines, your doctor might recommend a corticosteroid injection or steroid injection. These are shots of steroids that are injected directly into the area around the spinal nerves. Spinal imaging can help guide the needle. The steroids reduce the swelling around the disc and can lessen the pain. Sometimes 1 injection is enough. Often, they are given in a series of shots over a few weeks. These injections can bring relief for weeks or months at a time.
Physical therapy
Certain exercises can be helpful for a slipped disc. The goal of exercise is to make your back and stomach muscles stronger. This will ease the pressure on your disc and make you hurt less. Ask your doctor or physical therapist about exercises for your back. Your doctor may want you to see a physical therapist to learn about safe back exercises.
Physiotherapists usually recommend movement and exercise to help improve your mobility and function. This may include:
- exercises designed to improve movement and strength in a specific part of the body – these usually need to be repeated regularly for a set length of time
- activities that involve moving your whole body, such as walking or swimming – these can help if you’re recovering from an operation or injury that affects your mobility
- exercises carried out in warm, shallow water (hydrotherapy or aquatic therapy) – the water can help relax and support the muscles and joints, while providing resistance to help you gradually strengthen
- advice and exercises to help you increase or maintain your physical activity – advice will be given on the importance of keeping active, and how to do this in a safe, effective way
- providing mobility aids – such as crutches or a walking stick to help you move around
Your physiotherapist may also recommend exercises that you can continue doing to help you manage pain in the long term or reduce your risk of injuring yourself again.
Slipped disc exercises
Exercise is the most important way that you can:
- Ease stiffness and pain build up muscle strength and stamina
- Improve your flexibility and general fitness.
If your back pain lasts a while, lack of movement can cause the muscles to become weak. This makes it more likely that you’ll strain them in future. It’s important that you don’t rest for too long and keep moving.
Your pain should ease within 2 weeks and you should recover over approximately a 4–6 week period. You should carry on with the exercises for at least 6–8 weeks to help prevent another injury. If the pain is severe or not improving after a week or so, see your doctor.
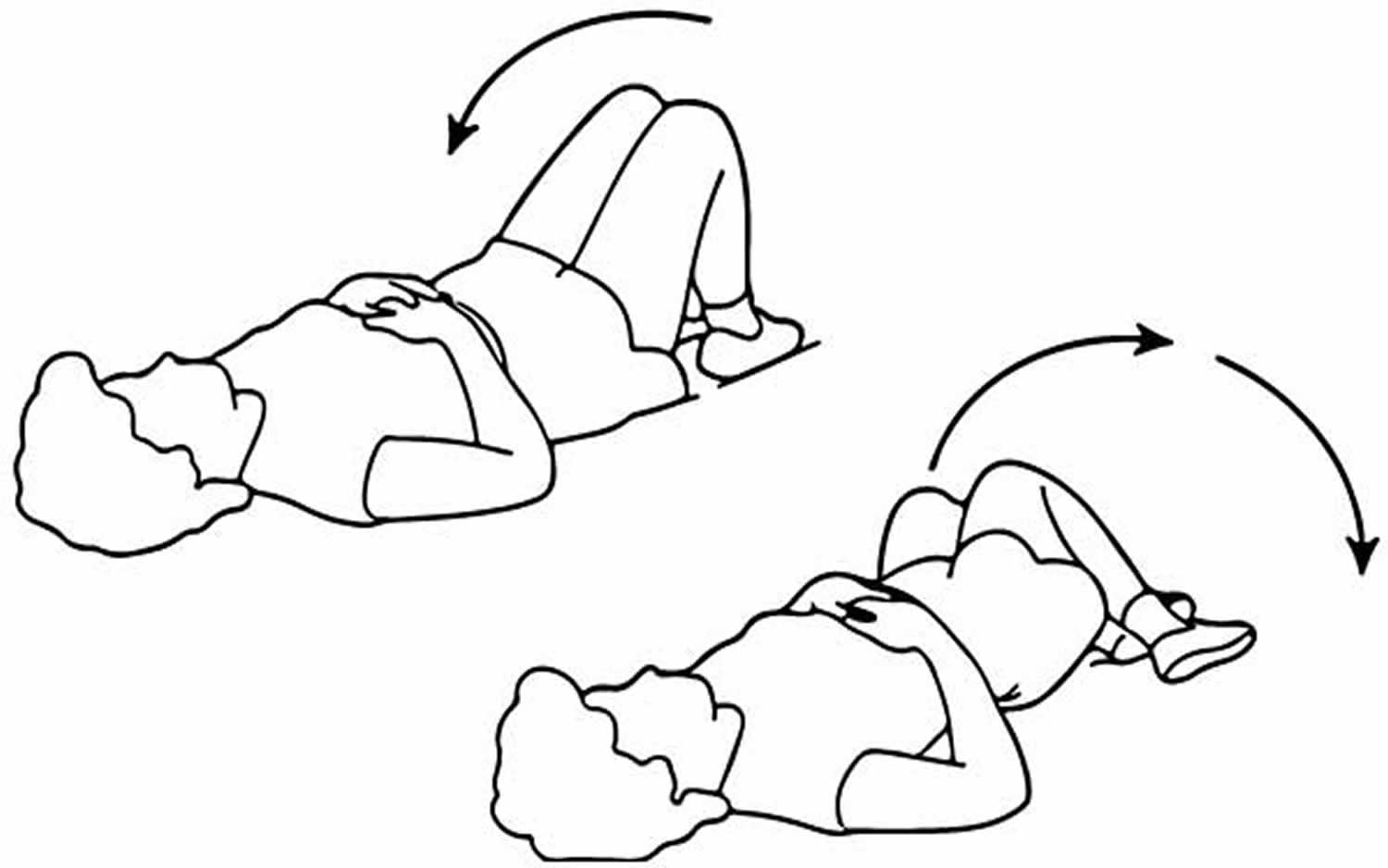
- Back stretch
Lie on your back, hands above your head. Bend your knees and roll them slowly to one side, keeping your feet on the floor. Hold for 10 seconds. Repeat 3 times on each side. Note your upper knee should be directly above lower knee.
Figure 6. Lower back stretch
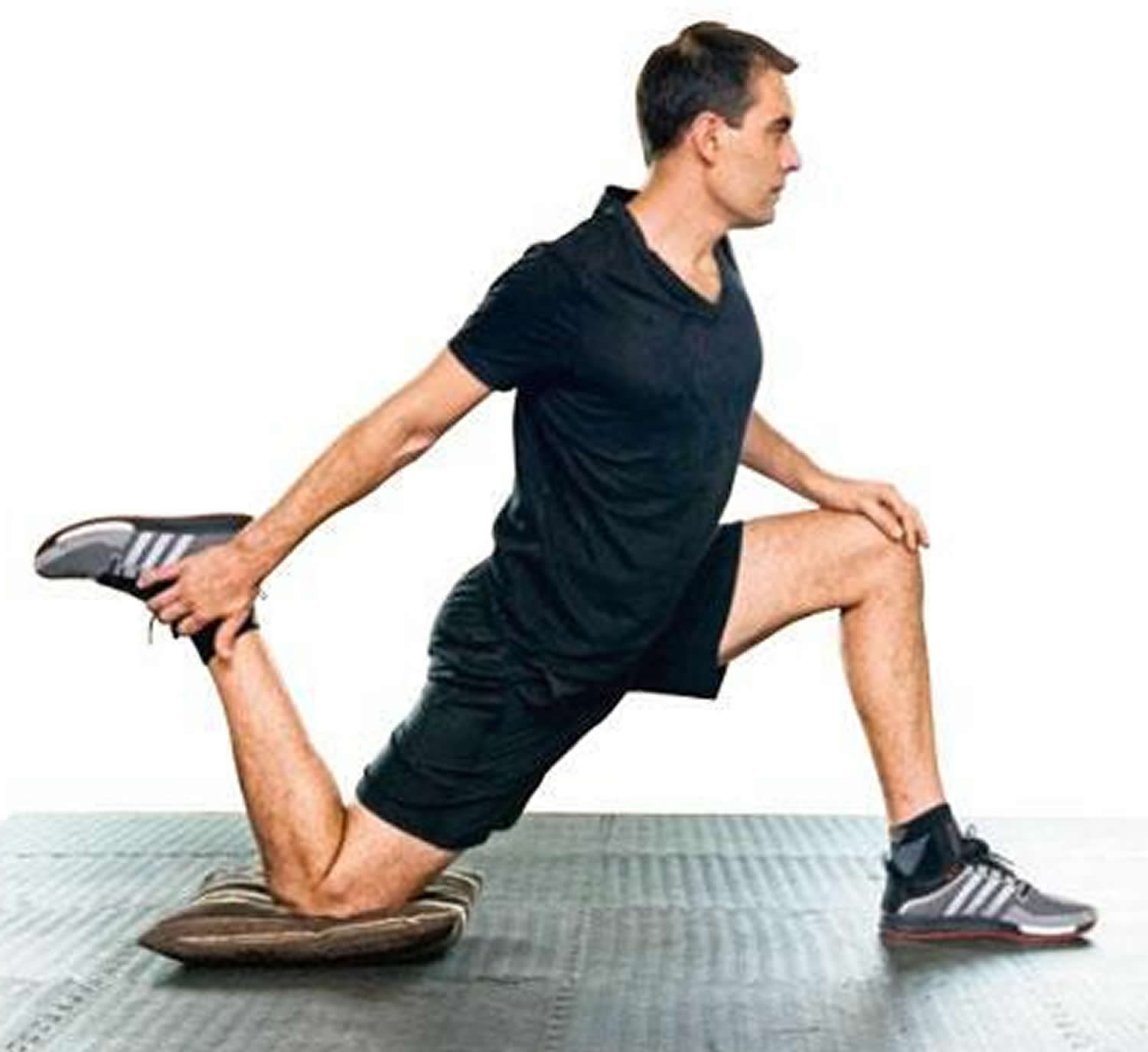
- Deep Lunge
Kneel on one knee, the other foot in front. Facing forwards, lift the back knee up. Hold for 5 seconds. Repeat 3 times on each side.
Figure 7. Deep Lunge
One-leg stand (front)
Holding onto something for support if needed, bend one leg up behind you. Hold for 5 seconds. Repeat 3 times on each side.
Figure 8. One-leg stand (front)

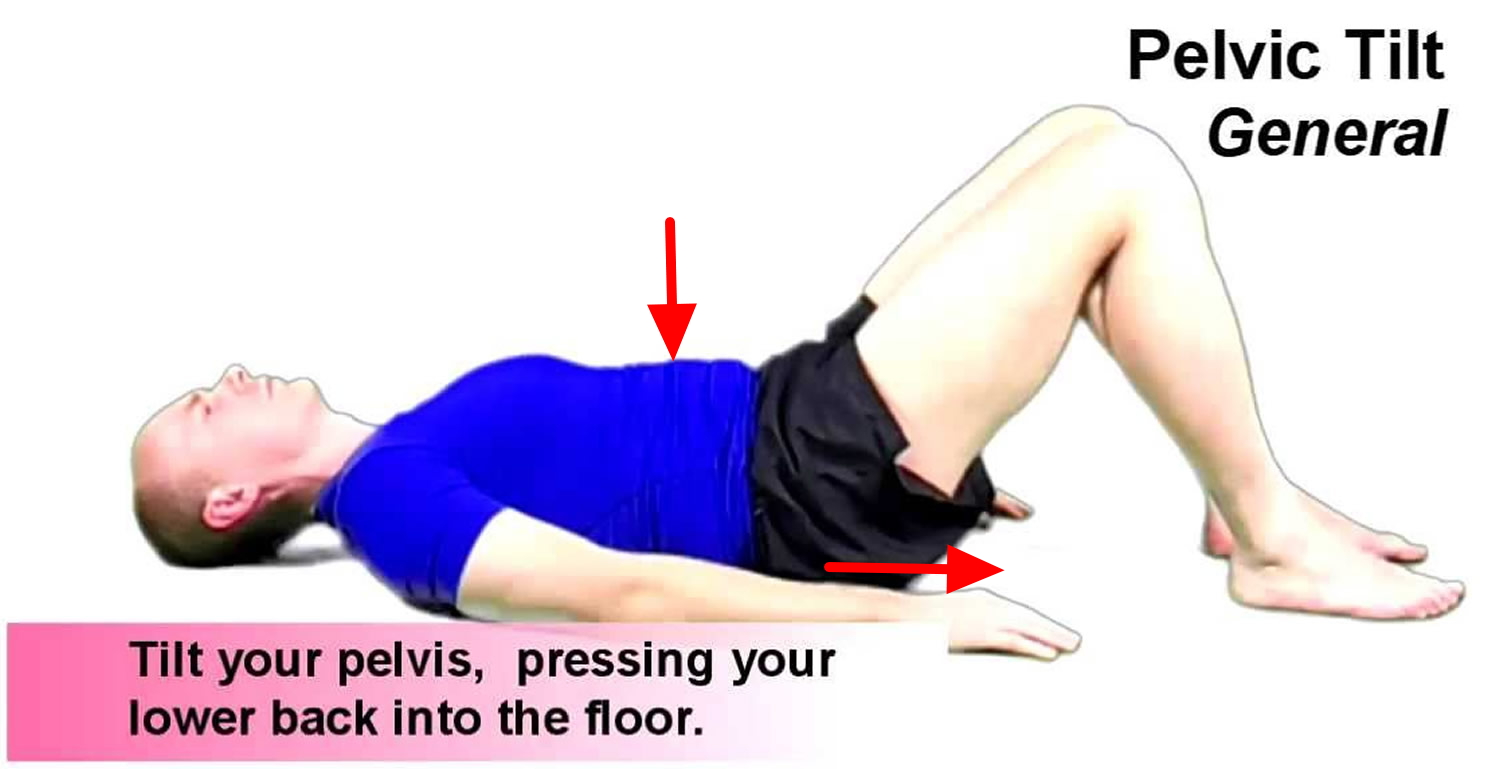
Pelvic tilt
Lie down with your knees bent. Tighten your stomach muscles, flattening your back against the floor. Hold for 5 seconds. Repeat 5 times.
Figure 9. Pelvic tilt
Knees to chest
Lie on your back, knees bent. Bring one knee up and pull it gently into your chest for 5 seconds. Repeat up to 5 times on each side.
Figure 10. Knees to chest

Manual therapy
Manual therapy is a technique where a physiotherapist uses their hands to manipulate, mobilize and massage the body tissues.
This can help:
- relieve pain and stiffness
- improve blood circulation
- help fluid drain more efficiently from parts of the body
- improve the movement of different parts of the body
- promote relaxation
Manual therapy can be used to treat specific problems, such as back pain, but may also be useful for a range of conditions that don’t affect the bones, joints or muscles.
For example, massage may improve quality of life for some people with serious or long-term conditions by reducing levels of anxiety and improving sleep quality.
Manual techniques are also used to help certain lung conditions.
Alternative medicine
Some alternative and complementary medicine treatments might help ease chronic back pain. Examples include:
- Chiropractic – spinal manipulation has been found to be moderately effective for low back pain that has lasted for at least a month.
- Yoga. A combination of physical activity, breathing exercises and meditation, yoga can improve function and relieve chronic back pain in some people.
- Acupuncture – where fine needles are inserted into specific points of the body, with the aim of reducing pain and promoting recovery.
- Transcutaneous Electrical Nerve Stimulation (TENS) – a small, battery-operated device is used to deliver an electric current to the affected area, with the aim of relieving pain.
- Ultrasound – where high-frequency sound waves are used to treat deep tissue injuries by stimulating blood circulation and cell activity, with the aim of reducing pain and spasms, as well as speeding up healing.
- Massage. This hands-on therapy can provide short-term relief to people dealing with chronic low back pain.
Steroid injections
If medicine and physical therapy aren’t helping, your doctor may suggest steroid injections. Inflammation-suppressing corticosteroids may be given by injection directly into the area around the spinal nerves. Transforaminal epidural steroid injection is recommended to provide short-term (2–4 week) help provide pain relief in patients with lumbar disc herniations with radiculopathy. Spinal imaging can help guide the needle more safely. Occasionally a course of oral steroids may be tried to reduce swelling and inflammation. The steroids reduce the swelling around the disc and can lessen the pain. Sometimes 1 injection is enough. Often they are given in a series of shots over a few weeks. These injections can bring relief for weeks or months at a time.
Slipped disc surgery
If nothing else is helping your pain, your doctor may want to do surgery. He or she will remove all or part of the damaged disc so it no longer presses on the nerve.
Only a small percentage of patients with disc herniations eventually need surgery. Your doctor may suggest surgery if conservative treatments fail to improve your symptoms after six weeks, especially if you continue to experience:
- Numbness or weakness
- Difficulty standing or walking
- Loss of bladder or bowel control
In many cases, surgeons can remove just the protruding portion of the disc. Rarely, however, the entire disc must be removed. In these cases, the vertebrae may need to be fused together with metal hardware to provide spinal stability to allow the process of bone fusion, which takes months. Rarely, your surgeon might suggest the implantation of an artificial disc.
- Lumbar microdiskectomy. This is the most common procedure for a herniated disk in the lower back. Microdiskectomy involves removing the herniated part of the disc and any fragments that are putting pressure on the spinal nerve.
- Cervical diskectomy and fusion. Cervical diskectomy is a procedure for the herniated disc in the neck. To relieve pressure, the entire herniated disc is removed. Bone is placed in the disc space and a metal plate may be used to help support the spine.
Figure 11. Diskectomy

Note: Diskectomy is the surgical removal of the damaged portion of a herniated disc in your spine. A herniated disc occurs when some of the softer material inside the disc pushes out through a crack in the tougher exterior. This can irritate or compress nearby nerves and cause pain, numbness or weakness.
Home treatment
You can practice good home care to treat your disc, as well. Good posture can help your back by reducing the pressure on your disc. Focus on standing up straight, sitting straight, and lifting with your back straight. Follow these tips to do what you can on your own to ease your symptoms.
- Heat or cold treatment, such as placing a heat or cold pack on the affected area. Initially, cold packs can be used to relieve pain and inflammation. After a few days, you may switch to gentle heat to give relief and comfort.
- Bend your knees and hips when you lift something, and keep your back straight.
- Hold an object close to your body when you carry it.
- If you stand for a long time, put one foot on a small stool or box for a while.
- If you sit for a long time, put your feet on a small stool so your knees are higher than your hips.
- Don’t wear high-heeled shoes.
- Don’t sleep on your stomach.
- Avoid too much bed rest. Too much bed rest can lead to stiff joints and weak muscles — which can complicate your recovery. Instead, rest in a position of comfort for 30 minutes, and then go for a short walk or do some work. Try to avoid activities that worsen your pain during the healing process.
- Take pain relievers. Over-the-counter medications — such as ibuprofen (Advil, Motrin IB, others) or naproxen (Aleve, others) — may help reduce the pain associated with a herniated disc.
Most people with acute back pain improve rapidly within a month, often without treatment. Some continue to have pain for longer. Some might have a repeat of the pain at another time, while others won’t.
Living with a slipped disc
Your chances of getting better are good. Most people who have a herniated disc are better in about 4 weeks. Sometimes it takes longer. If you still have pain or numbness after 4 to 6 weeks, or if you feel worse, talk with your doctor. Sometimes it takes surgery to relieve pain.
Slipped disc prognosis
Studies vary on outcomes of slipped disc prognosis, but the majority of cases respond to conservative management 4. One study did show that 30% of patients complain of back pain at one year 7. Many cases of disc herniation are asymptomatic and are found by accident on advanced imaging. Of symptomatic disc herniation cases, 90% of them resolve at six weeks following injury. Surgery may lead to more rapid recovery of the symptomatic herniated disc, but results are also similar to conservative management at one year post-operatively 8, 9, 10, 11. A review of over 600 patients concluded that non-contained disc herniations may respond more successfully to nonsurgical treatment 12. Epidural steroid injections can be used at almost any time; however, the use of steroid injection has been questioned 13.
- Waxenbaum JA, Futterman B. Anatomy, Back, Intervertebral Discs. [Updated 2018 Dec 13]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2019 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK470583[↩]
- van Uden S, Silva-Correia J, Oliveira JM, Reis RL. Current strategies for treatment of intervertebral disc degeneration: substitution and regeneration possibilities. Biomater Res. 2017;21:22[↩]
- Huang YC, Hu Y, Li Z, Luk KDK. Biomaterials for intervertebral disc regeneration: Current status and looming challenges. J Tissue Eng Regen Med. 2018 Nov;12(11):2188-2202[↩]
- Dydyk AM, Ngnitewe Massa R, Mesfin FB. Disc Herniation. [Updated 2023 Jan 16]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK441822[↩][↩][↩]
- De Cicco FL, Camino Willhuber GO. Nucleus Pulposus Herniation. [Updated 2023 Aug 7]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK542307[↩]
- Dydyk AM, Khan MZ, Singh P. Radicular Back Pain. [Updated 2022 Oct 24]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK546593[↩]
- Amlie E, Weber H, Holme I. Treatment of acute low-back pain with piroxicam: results of a double-blind placebo-controlled trial. Spine (Phila Pa 1976). 1987 Jun;12(5):473-6. doi: 10.1097/00007632-198706000-00010[↩]
- Weinstein JN, Tosteson TD, Lurie JD, Tosteson AN, Hanscom B, Skinner JS, Abdu WA, Hilibrand AS, Boden SD, Deyo RA. Surgical vs nonoperative treatment for lumbar disk herniation: the Spine Patient Outcomes Research Trial (SPORT): a randomized trial. JAMA. 2006 Nov 22;296(20):2441-50. doi: 10.1001/jama.296.20.2441[↩]
- Weinstein JN, Lurie JD, Tosteson TD, Skinner JS, Hanscom B, Tosteson AN, Herkowitz H, Fischgrund J, Cammisa FP, Albert T, Deyo RA. Surgical vs nonoperative treatment for lumbar disk herniation: the Spine Patient Outcomes Research Trial (SPORT) observational cohort. JAMA. 2006 Nov 22;296(20):2451-9. doi: 10.1001/jama.296.20.2451[↩]
- Schoenfeld AJ, Weiner BK. Treatment of lumbar disc herniation: Evidence-based practice. Int J Gen Med. 2010 Jul 21;3:209-14. doi: 10.2147/ijgm.s12270[↩]
- Buttermann GR. Treatment of lumbar disc herniation: epidural steroid injection compared with discectomy. A prospective, randomized study. J Bone Joint Surg Am. 2004 Apr;86(4):670-9. https://journals.lww.com/jbjsjournal/abstract/2004/04000/treatment_of_lumbar_disc_herniation__epidural.2.aspx[↩]
- Nakagawa H, Kamimura M, Takahara K, Hashidate H, Kawaguchi A, Uchiyama S, Miyasaka T. Optimal duration of conservative treatment for lumbar disc herniation depending on the type of herniation. J Clin Neurosci. 2007 Feb;14(2):104-9. doi: 10.1016/j.jocn.2006.08.001[↩]
- Iversen T, Solberg TK, Romner B, Wilsgaard T, Twisk J, Anke A, Nygaard O, Hasvold T, Ingebrigtsen T. Effect of caudal epidural steroid or saline injection in chronic lumbar radiculopathy: multicentre, blinded, randomised controlled trial. BMJ. 2011 Sep 13;343:d5278. doi: 10.1136/bmj.d5278[↩]





{kind=link}