
Contents
What is pneumoperitoneum
Pneumoperitoneum means the presence of air within the peritoneal cavity and can be divided into 2 subgroups, surgical pneumoperitoneum (90%) and nonsurgical pneumoperitoneum (10%) 1. The most common cause of pneumoperitoneum is a perforation of the abdominal organ, most commonly, a perforated peptic ulcer (gastric and duodenal ulcers), although a pneumoperitoneum may occur as a result of perforation of any part of the bowel; other causes include a benign ulcer, a tumor, or trauma. The exception is a perforated appendix, which seldom causes a pneumoperitoneum.
The presence of a pneumoperitoneum does not, however, always imply a perforation, because a number of other (mostly nonsurgical) conditions are associated with pneumoperitoneum. For example, the most common cause of a spontaneous pneumoperitoneum is the introduction of air through the female genital tract. Likewise, not every bowel perforation results in a pneumoperitoneum; some perforations seal over, allowing little gas to escape. A pneumoperitoneum is common after abdominal surgery; it usually resolves 3-6 days after surgery, although it may persist for as long as 24 days after surgery.
Peritoneal cavity
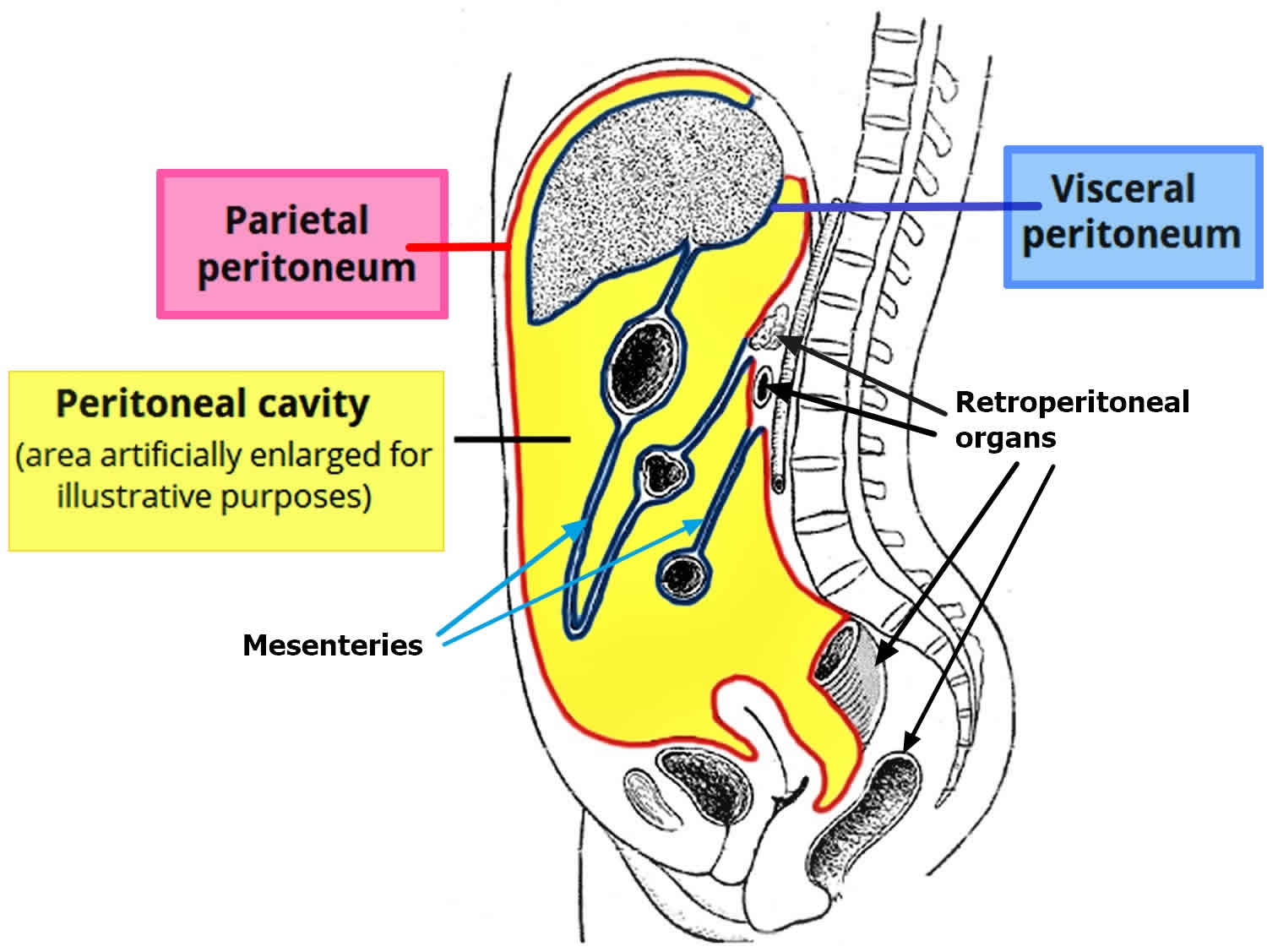
The peritoneal cavity is a potential space between the parietal and visceral peritoneum. The peritoneum is a thin, serous membrane that lines the abdominal cavity that is embryologically derived from mesoderm 2. The peritoneum is composed of mesothelial cells that are supported by a thin layer of fibrous tissue. The outer layer also known as the parietal peritoneum attaches to the abdominal and pelvic walls. The inner or visceral layer wraps around the internal organs located inside the intraperitoneal space. The structures bound by the peritoneal cavity may be intraperitoneal or retroperitoneal.
The peritoneum serves to support the organs of the abdomen and acts as a conduit for passage of nerves, blood vessels, and lymphatics. Although the peritoneum is thin, it is made of 2 layers, parietal and visceral peritoneum, with a potential space between them. The potential space between the 2 layers (parietal and visceral peritoneum) contains about 50 to 100 ml of serous fluid, which consists of water, electrolytes, leukocytes and antibodies, that functions to prevent friction and allows the parietal and visceral peritoneum and organs to glide freely and the antibodies in the fluid fight infection 2. While the peritoneal cavity is ordinarily filled with only a thin film of serous fluid, it is referred to as a potential space because excess fluid can accumulate in it, resulting in the clinical condition of ascites or the presence of air within the peritoneal cavity known as pneumoperitoneum.
The boundaries of the peritoneal cavity include:
- Anterior abdominal muscles
- Vertebrae
- Pelvic floor
- Diaphragm
The peritoneal cavity contains omentum, ligaments, and mesentery. These structures connect the abdominal organs or the abdominal wall or to each other. Knowing an organ’s relationship to the peritoneum has surgical significance. Organs that are considered intraperitoneal are the stomach, spleen, liver, the first and fourth parts of the duodenum, jejunum, ileum, transverse and sigmoid colon. The list of retroperitoneal organs includes the aorta, esophagus, second and third parts of the duodenum, ascending and descending colon, pancreas, kidneys, ureters, and adrenal glands.
A key space in the peritoneal cavity is the epiploic foramen, also known as the foramen of Winslow. This foramen allows communication between the greater and lesser sacs. It is bordered by the hepatoduodenal ligament anteriorly, the inferior vena cava (IVC) posteriorly, duodenum inferiorly, and caudate lobe of the liver superiorly. The foramen provides access to a surgeon, should they need to clamp the hepatoduodenal ligament to stop a hemorrhage or gain anatomical access to the lesser sac. The foramen can also serve as a location for a lesser sac hernia.
The greater omentum loosely hangs from the greater curvature of the stomach and folds over the anterior of the intestine before curving back superiority to attach to the transverse colon. It acts as a protective or insulating layer. The mesentery helps attach the abdominal organs to the abdominal wall and contains many blood vessels, nerves, and lymphatics. Abdominal organs that are intraperitoneal are usually mobile while those in the retroperitoneum are usually fixed to the posterior abdominal wall. The dorsal mesentery also gives off the transverse and sigmoid mesocolons, which are important due to them containing the blood, nerve, and lymphatic supply for related structures.
Figure 1. Peritoneal cavity
Subdivisions of the peritoneal cavity
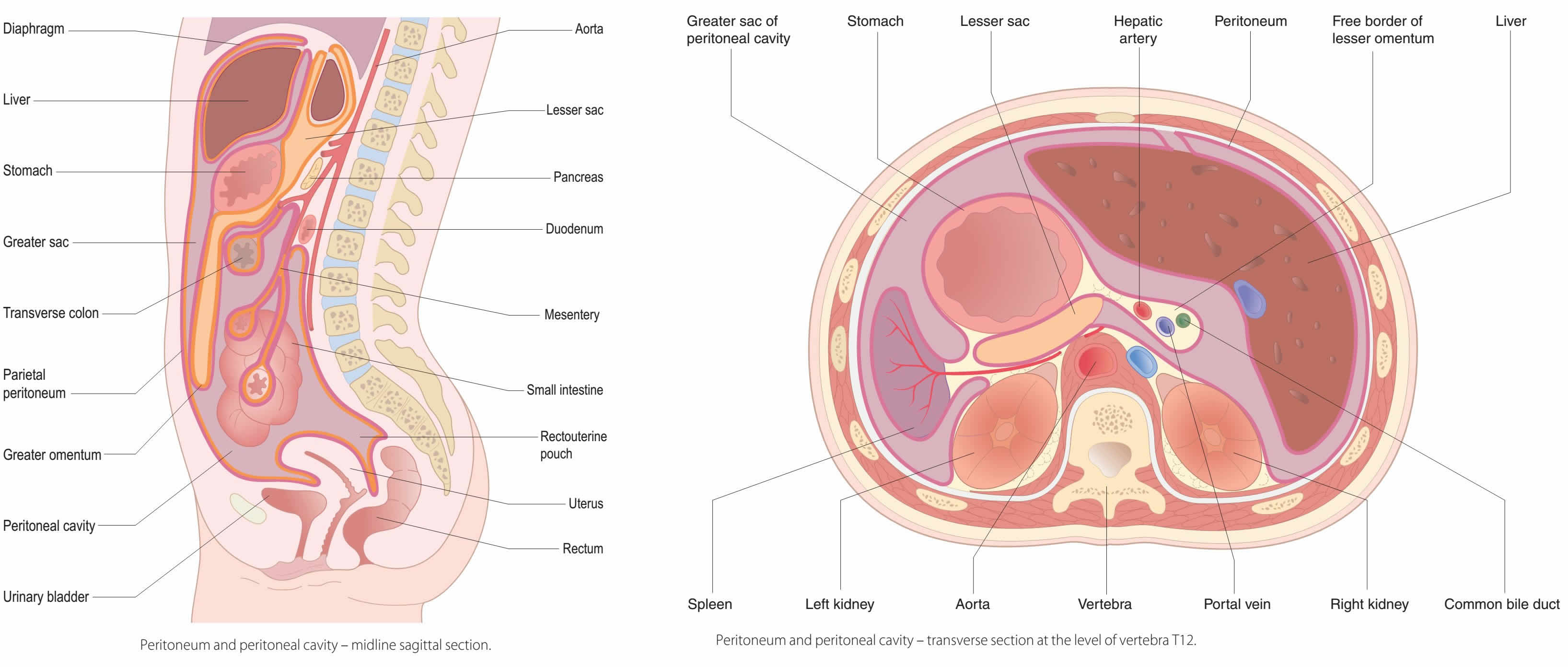
The peritoneal cavity can be divided into the greater and lesser peritoneal sacs. The greater sac comprises the majority of the peritoneal cavity. The lesser sac (also known as the omental bursa) is smaller and lies posterior to the stomach and lesser omentum.
Greater Sac
The greater sac is the larger portion of the peritoneal cavity. It is further divided into two compartments by the mesentery of the transverse colon (known as the transverse mesocolon):
- Supracolic compartment – lies above the transverse mesocolon and contains the stomach, liver and spleen.
- Infracolic compartment – lies below the transverse mesocolon and contains the small intestine, ascending and descending colon. The infracolic compartment is further divided into left and right infracolic spaces by the mesentery of the small intestine.
The supracolic and infracolic compartments are connected by the paracolic gutters which lie between the posterolateral abdominal wall and the lateral aspect of the ascending or descending colon.
Lesser Sac (Omental Bursa)
The lesser sac lies posteriory to the stomach and lesser omentum. It allows the stomach to move freely against the structures posterior and inferior to it.
The omental bursa is connected with the greater sac through an opening in the omental bursa – the epiploic foramen (of Winslow).
The epiploic foramen is situated posterior to the free edge of the lesser omentum (the hepatoduodenal ligament).
Figure 2. Peritoneal cavity subdivision
Structure of the peritoneal cavity in the pelvis
Due to the presence of different pelvic organs, the peritoneal cavity differs in structure between the sexes. The primary difference in structure is the location of the most distal portion of the cavity.
When humans stand or sit upright, any superfluous fluid (which could be blood, pus, or infected fluid) is likely to collect in the most inferior portion of the peritoneal cavity. Thus, it is clinically important to be aware of the differences between males and females.
Male
In males, the rectovesical pouch is a double folding of peritoneum located between the rectum and the bladder. The peritoneal cavity is completely closed in males.
Females
In females, there are two areas of note:
- Rectouterine pouch of Douglas – double folding of the peritoneum between the rectum and the posterior wall of the uterus.
- Vesicouterine pouch – double folding of peritoneum between the anterior surface of the uterus and the bladder.
The peritoneal cavity is not completely closed in females – the uterine tubes open into the peritoneal cavity, providing a potential pathway between the female genital tract and the abdominal cavity. Clinically, this means that infections of the vagina, uterus, or uterine tubes may result in infection and inflammation of the peritoneum (peritonitis).
Actual passage of infectious material into the peritoneum, however, is rare due to the presence of a mucous plug in the external os (opening) of the uterus which prevents the passage of pathogens but allows sperm to enter the uterus.
Pneumoperitoneum causes
Pneumoperitoneum can be divided into 2 subgroups, surgical pneumoperitoneum (90%) and nonsurgical pneumoperitoneum (10%). In children, the causes are different from the adult population. Surgical pneumoperitoneum involves some of the most common and most urgent causes of pneumoperitoneum including those attributed to a perforated gastrointestinal tract in the abdomen (i.e., perforated peptic ulcer, ruptured diverticulum, trauma, and other things); this group requires prompt diagnosis and intervention 3.
Nonsurgical pneumoperitoneum is usually defined as the presence of free air in the peritoneal cavity that is detectable by an X-ray or a CT scan and is either successfully treated nonoperatively or results in a negative exploratory laparotomy or laparoscopy. It is usually caused by physiologic processes that do not require surgical management, and based on its cause can be further divided into 5 categories, including postoperatively retained air, thoracic, abdominal, gynecologic, and idiopathic. Examples include retained postsurgical air, spontaneous bacterial peritonitis, blunt abdominal trauma, positive-pressure ventilation, gynecologic examination with or without insufflation, coitus, oro-genital sex, and vaginal douching. It is thought that retained postsurgical air is responsible for almost 25% of the cases of nonsurgical pneumoperitoneum 3.
Postoperative pneumoperitoneum is a well-known sequela of abdominal surgery that is defined as the presence of free intraperitoneal air after surgery. In laparotomy, the origin of the air is thought to be room air, and in laparoscopy, the air is from carbon dioxide insufflation. Generally, postoperative pneumoperitoneum is believed to be bilateral and transient, demonstrating resolution within 7 day 4.
The causes of pneumoperitoneum in adults:
- Perforated hollow gastrointestinal tract
- peptic ulcer disease
- ischemic bowel
- bowel obstruction
- necrotizing enterocolitis
- appendicitis
- diverticulitis
- malignancy
- inflammatory bowel disease
- mechanical perforation
- trauma
- colonoscopy
- foreign bodies
- iatrogenic
- Postoperative free intraperitoneal gas
- Peritoneal dialysis
- Vaginal “aspiration” 5
- cunnilingus
- douching
- sudden squatting
- postpartum exercises
- water-skiing 6
- Mechanical ventilation
- Pneumomediastinum
- Pneumothorax
A gastrointestinal perforation constitutes one of the commonest surgical emergencies. The causes of pneumoperitoneum in adults are perforation, peritoneal dialysis, immediate postoperative status, vaginal aspiration, and mechanical ventilation 7. Mechanical perforation may be seen after colonoscopy, endoscopy, etc. Sometimes pneumomediastinum and pneumothorax may also result in pneumoperitoneum. The causes of pneumoperitoneum in children are perforation (necrotizing enterocolitis, Hirschsprung’s disease, and meconium ileus) and iatrogenic effects, such as from use of rectal thermometer, enema, and postintubation or mechanical ventilation 8.
Bali et al. in their study of 400 patients found that the commonest cause of perforation peritonitis in their study was acid peptic disease (45%), followed by appendicitis (18.5%), typhoid fever (12%), tuberculosis (10%), and trauma (9%) 9. Similar results were seen by Jhobta et al. in their study of 504 consecutive cases 10.
The causes of neonatal pneumoperitoneum are different from adult pneumoperitoneum and include:
- Perforated hollow gastrointestinal tract
- necrotizing enterocolitis (NEC): most common
- meconium ileus in cystic fibrosis
- Hirschsprung disease
- intestinal atresia or web
- peptic ulcer disease
- Iatrogenic
- intubation/mechanical ventilation
- rectal thermometer
- enema
Pneumoperitoneum signs and symptoms
Pneumoperitoneum common signs and symptoms are abdominal pain, vomiting, abdominal distension, constipation, fever, diarrhea, tachycardia (pulse >110/min), hypotension (systolic blood pressure <100 mmHg), urine output (<30 mL/hour), and tachypnea (respiratory rate >20/min) 7. The clinical presentation of the patients varies according to the site of perforation. Patients of duodenal ulcer perforation usually have a short history of epigastric pain along with generalized tenderness and guarding. An associated history of nonsteroidal anti-inflammatory drug (NSAID) consumption may be present. Patients with small bowel perforation may present with a prolonged history of fever followed by the appearance of pain in lower abdomen. Appendicular perforations usually have a classical history of pain starting in the periumbilical area or right iliac fossa, along with vomiting and fever. Perforations of the proximal gastrointestinal tract are more common in India, in sharp contrast to findings from studies in developed countries, such as the USA, Greece, and Japan, where distal gastrointestinal tract perforations are more common 11.
Pneumoperitoneum diagnosis
CT scan is regarded as the criterion standard for the detection of a pneumoperitoneum; it provides exquisite scans, and it is theoretically more sensitive than plain abdominal radiography. However, CT is not always required when a pneumoperitoneum is suspected. Despite the contrary consensus, the accuracy of supine abdominal radiography closely approximates CT when the entire abdomen is imaged.
An erect chest x-ray is the most sensitive plain radiograph for the detection of free intraperitoneal gas in an emergency setting. On chest x-ray, any subdiaphragmatic free gas can be seen (Figures 3 and 4) 7. Abdominal radiography is routinely done in cases of acute abdomen. The various relevant signs described in an abdominal radiograph are as follows 12:
- Cupola/saddlebag/mustache sign — Seen on a supine radiograph, refers to air accumulation underneath the central tendon of the diaphragm in the midline.
- Rigler’s sign — Air outlining both sides of the bowel wall.
- Lucent liver sign – Reduction of liver opacity due to air located anterior to the liver.
- Football sign — Seen in massive pneumoperitoneum, where the abdominal cavity is outlined by gas.
- Silver’s sign — Also called a falciform ligament sign, where air outlines the falciform ligament.
- Inverted V sign — Air outlining lateral umbilical ligaments (inferior epigastric vessels).
- Doge’s cap sign — Triangular collection of gas in Morison pouch.
- Telltale triangle sign — Triangular air pocket between three loops of bowel.
- Urachus sign — Outline of middle umbilical ligament.
Ultrasound is usually the first investigation performed in emergency patients. Ultrasound is a noninvasive test that is widely available and is particularly valuable in children, pregnant women, and individuals of reproductive age. Some studies have reported sensitivities greater than that of plain abdominal radiography in the diagnosis of a pneumoperitoneum 13. Compared with plain radiography, ultrasound examination also has the advantage of depicting other changes, such as free abdominal fluid and inflammatory masses 14.
Figure 3. Pneumoperitoneum X-ray (erect chest X-ray)
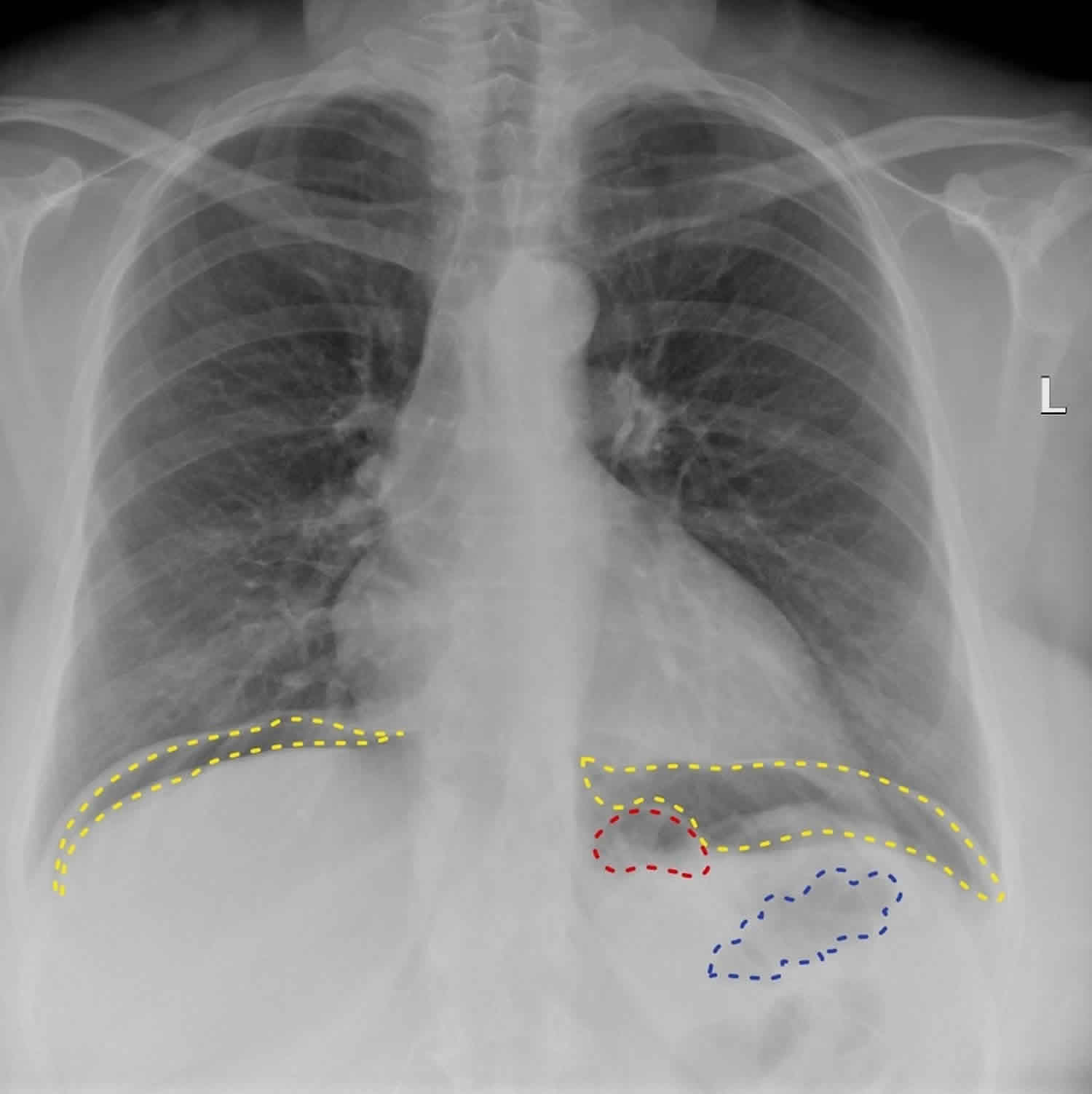
Footnote: A large amount of gas is seen under both diaphragmatic domes (yellow dotted lines). In the left upper quadrant gas is also seen in the stomach (red dotted line) and splenic flexure of the colon (blue dotted line). This patient did have a CT which demonstrated extensive sigmoid diverticular disease with active inflammation and diverticulitis, accounting for the pneumoperitoneum. Conservative treatment was followed by sigmoidoscopy for direct visualiation.
[Source 15 ]Figure 4. Pneumoperitoneum X-ray
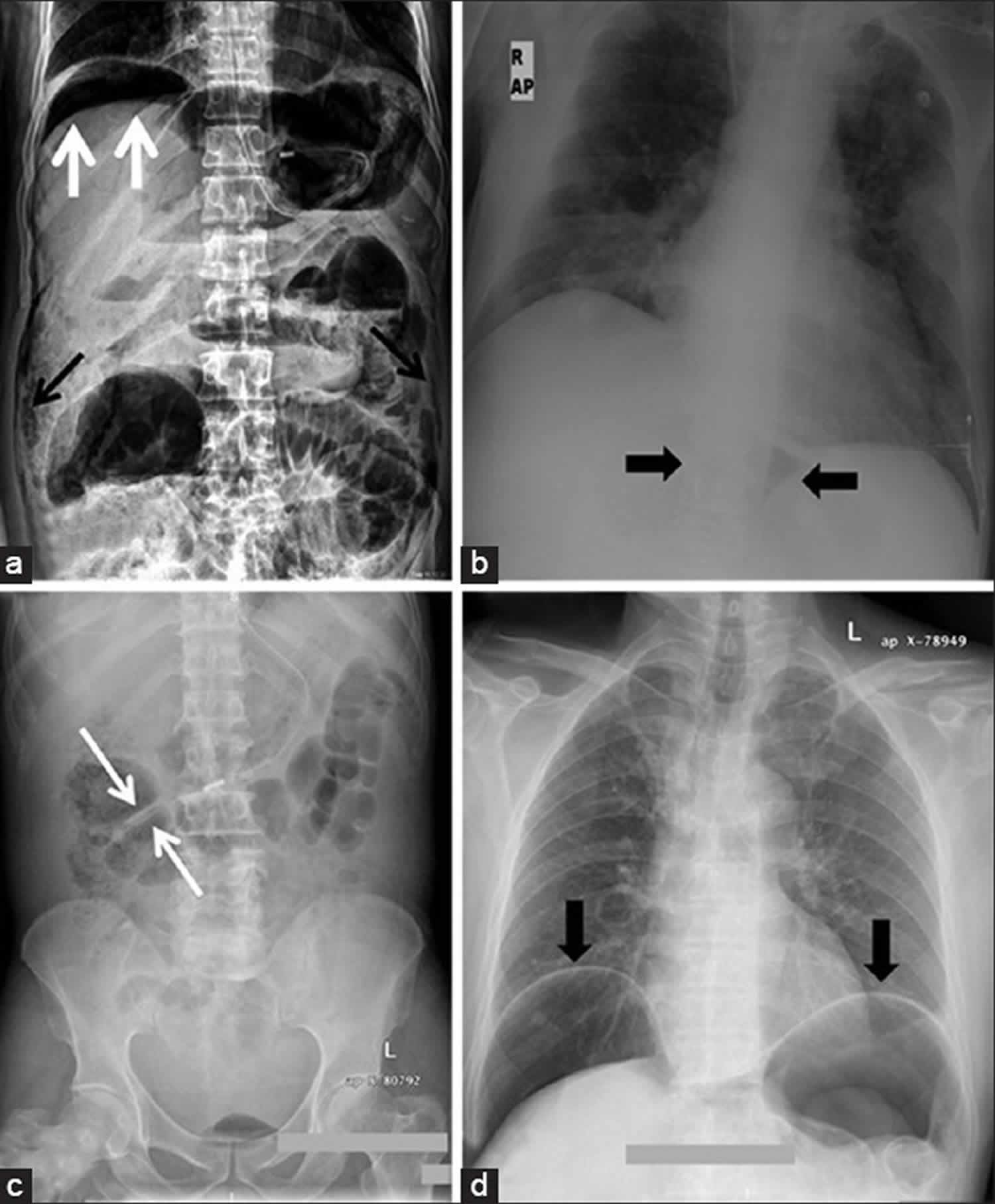
Footnote: (a) X-ray of abdomen, erect view, showing subdiaphragmatic free air (white arrows), air outlining the properitoneal fat stripe (black arrows) (b) Cupola sign (arrowheads) (c) Rigler’s sign (arrow) (d) Chest radiograph showing free air under the diaphragms (arrowhead)
[Source 7 ]Pneumoperitoneum treatment
Pneumoperitoneum treatment involves treating the underlying cause or source of pneumoperitoneum. Surgical pneumoperitoneum involves some of the most common and most urgent causes of pneumoperitoneum including those attributed to a perforated gasttointestinal tract in the abdomen (i.e., perforated peptic ulcer, ruptured diverticulum, trauma, and other things); this group requires prompt diagnosis and intervention.
Nonsurgical pneumoperitoneum is usually defined as the presence of free air in the peritoneal cavity that is detectable by an X-ray or a CT scan and is either successfully treated nonoperatively or results in a negative exploratory laparotomy or laparoscopy. It is usually caused by physiologic processes that do not require surgical management, and based on its cause can be further divided into 5 categories, including postoperatively retained air, thoracic, abdominal, gynecologic, and idiopathic. Examples include retained postsurgical air, spontaneous bacterial peritonitis, blunt abdominal trauma, positive-pressure ventilation, gynecologic examination with or without insufflation, coitus, oro-genital sex, and vaginal douching. It is thought that retained postsurgical air is responsible for almost 25% of the cases of nonsurgical pneumoperitoneum 3. Postoperative pneumoperitoneum following laparoscopic surgery is self-limited, typically resolving within days 1. Pneumoperitoneum with carbon dioxide gas is used to facilitate laparoscopic procedures. Generally, postoperative pneumoperitoneum is believed to be bilateral and transient, demonstrating resolution within 7 days 4. Nielsen et al. 16 evaluated the duration of and factors contributing to persistent postoperative pneumoperitoneum. They followed 32 patients for 6 mo after abdominal surgery and concluded that postoperative pneumoperitoneum resolved within 2 d for most of the study population. They further noted that a high body mass index (BMI) and small initial amount of free air were associated with a shorter course of postoperative pneumoperitoneum 16.
- Smith KS, Wilson TC, Luces L, Stevenson AA, Hajhosseini B, Siram SM. Pneumoperitoneum 48 days after laparoscopic hysterectomy. JSLS. 2013;17(4):661–664. doi:10.4293/108680813X13794522666446 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3866076[↩][↩]
- Kalra A, Tuma F. Anatomy, Abdomen and Pelvis, Peritoneum. [Updated 2018 Nov 26]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2019 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK534788[↩][↩]
- Pneumoperitoneum: a review of nonsurgical causes. Mularski RA, Sippel JM, Osborne ML. Crit Care Med. 2000 Jul; 28(7):2638-44.[↩][↩][↩]
- Bannen JE. Post-operative Pneumo-Peritoneum. Br J Radiol. 1944;17:119–121[↩][↩]
- Reeder MM, Felson B. Reeder and Felson’s gamuts in radiology, comprehensive lists of roentgen differential diagnosis. Springer Verlag. (2003) ISBN:0387955887[↩]
- [A case report. Peritonitis after water-skiing]. Lakartidningen. 1993 Jun 23;90(25):2383. https://www.ncbi.nlm.nih.gov/pubmed/8316022[↩]
- Sureka B, Bansal K, Arora A. Pneumoperitoneum: What to look for in a radiograph?. J Family Med Prim Care. 2015;4(3):477–478. doi:10.4103/2249-4863.161369 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4535122[↩][↩][↩][↩]
- Spectrum of perforation peritonitis. Chakma SM, Singh RL, Parmekar MV, Singh KH, Kapa B, Sharatchandra KH, Longkumer AT, Rudrappa S. J Clin Diagn Res. 2013 Nov; 7(11):2518-20.[↩]
- Perforation peritonitis and the developing world. Bali RS, Verma S, Agarwal PN, Singh R, Talwar N. ISRN Surg. 2014; 2014():105492.[↩]
- Spectrum of perforation peritonitis in India–review of 504 consecutive cases. Jhobta RS, Attri AK, Kaushik R, Sharma R, Jhobta A. World J Emerg Surg. 2006 Sep 5; 1():26.[↩]
- A bacteriological study of perforated duodenal ulcers. Shinagawa N, Muramoto M, Sakurai S, Fukui T, Hori K, Taniguchi M, Mashita K, Mizuno A, Yura J. Jpn J Surg. 1991 Jan; 21(1):1-7.[↩]
- Images in clinical medicine. Radiologic signs of pneumoperitoneum. Lee CH. N Engl J Med. 2010 Jun 24; 362(25):2410.[↩]
- Chen SC, Yen ZS, Wang HP. Ultrasonography is superior to plain radiography in the diagnosis of pneumoperitoneum. Br J Surg. 2002 Mar. 89(3):351-4.[↩]
- Ottinger D, Swanson JR. Diagnosing intestinal perforation: a new approach. Am J Perinatol. 2008 May. 25(5):291-3.[↩]
- Pneumoperitoneum. https://radiopaedia.org/cases/pneumoperitoneum-12[↩]
- Duration of postoperative pneumoperitoneum. Nielsen KT, Lund L, Larsen LP, Knudsen P. Eur J Surg. 1997 Jul; 163(7):501-3.[↩][↩]





{kind=link}