Contents
Talus fracture
Talus fracture is a break in the talus bone that forms the ankle. Talus fracture often occurs during a high-energy event, such as a car collision or a high-velocity fall. Because the talus is important for ankle movement, a fracture often results in significant loss of motion and function. In addition, a talus fracture that does not heal properly can lead to serious complications, including chronic pain. For this reason, many talus fractures require surgery.
Usually a great deal of force is required to cause fractures or a dislocation of the talus. This can include falls and car accidents, as well as sports like snow-boarding. However, sometimes talus fractures occur with only small injuries when the bones are weak, as in osteoporosis.
Talar fractures will often require both X-Rays and CT scans to confirm the fracture and assess the degree of injury to the surrounding tissues.
Subtle fractures in the talus can be very difficult to see immediately after the fracture has occurred. In later weeks, the healing reaction of the bone can be more easily seen on X-Ray. For this reason, you may require x-rays a few weeks apart to diagnose the fracture.
Fractures of the talus are often difficult to manage. Most of the bone surfaces are covered by a protective smooth substance called cartilage. Cartilage does not allow blood vessels to enter the bone, and this means that the talus has a vulnerable blood supply. For this reason, talar fractures are frequently associated with death of the bone, or ‘avascular necrosis’.
Talus fractures will often require surgery and long rehabilitation. Severe fracture-dislocations of the talus sometimes require removal of the bone fragments and ankle fusion (arthrodesis) to achieve recovery.
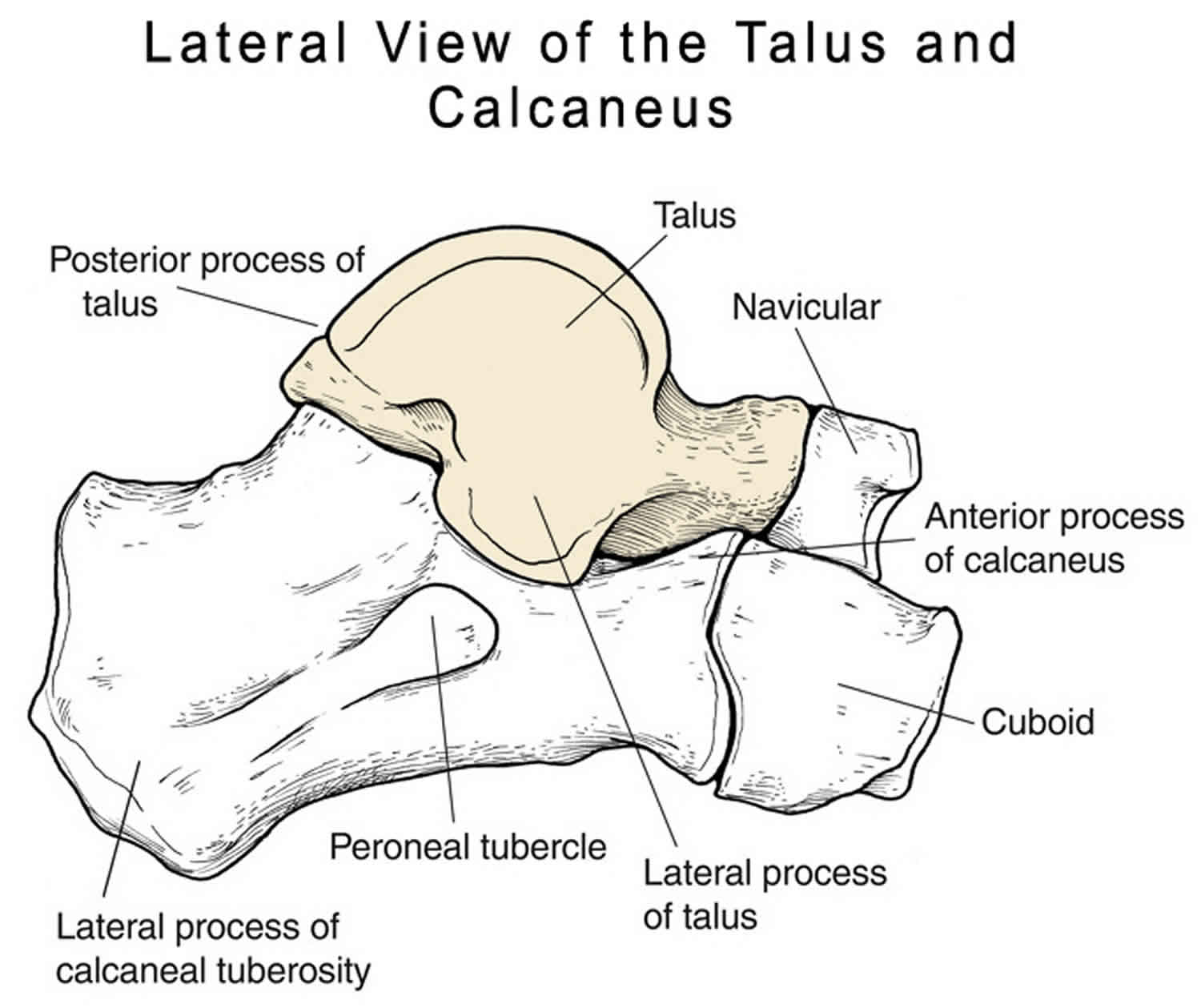
Talus anatomy
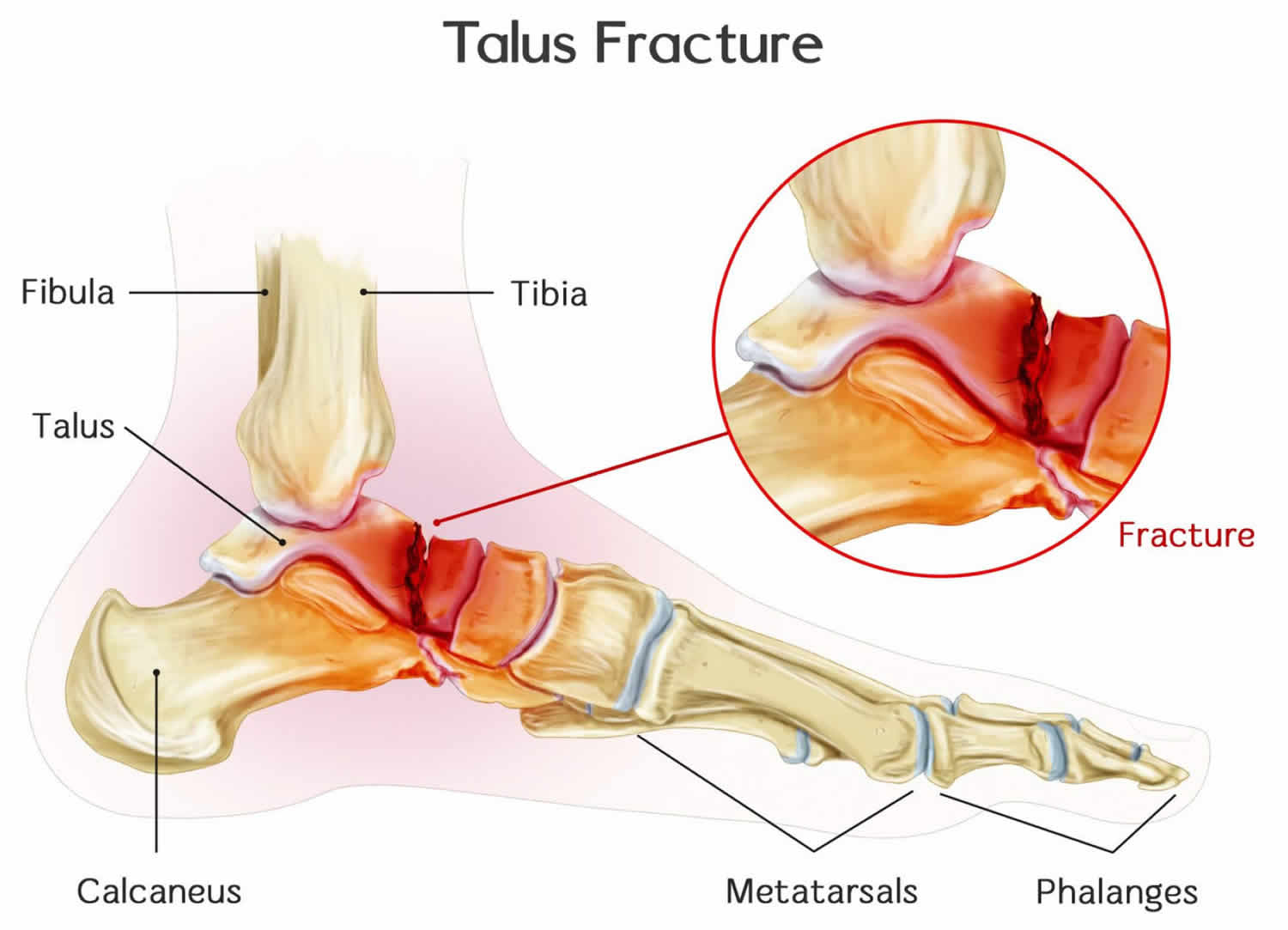
The talus is the bone that makes up the lower part of the ankle joint (the tibia and fibula bones of the lower leg make up the upper part of the ankle joint). The talus sits above the heel bone (calcaneus). Together, the talus and calcaneus form the subtalar joint, which is important for walking, especially on uneven ground.
The talus is the main connector between the foot and leg, helping to transfer weight and pressure forces across the ankle joint. It is largely covered by articular cartilage, the white slippery material that covers all joint surfaces. This cartilage allows the talus to move smoothly against its neighbor bones.
Figure 1. Talus anatomy
Talus fracture classification
Fractures occur in all parts of the talus bone. Most commonly, the talus breaks in its mid-portion, called the “neck.” The neck is between the “body” of the talus, located under the tibia, and the “head,” located further down the foot.
Another common site for talus fractures is along the outside of the bone where it juts out slightly. This area of the bone is called the “lateral process.” Fractures of the lateral process often occur when the ankle is forced out to the side and are commonly seen in snowboarders.
Talus fractures are often classified according to the severity of the displacement — how much the pieces of bone have moved out of their normal position.
- Minimally displaced or stable fractures: This type of fracture is barely out of place. The broken ends of the bones line up almost correctly. In a minimally displaced fracture, the bones usually stay in place during healing, and surgery to fix the bones into position is not usually required.
- Displaced fracture: When a bone breaks and the pieces move out of their anatomic position, it is called a displaced fracture. The amount of displacement relates to the amount of energy that caused the fracture. Fractures that are highly displaced are more likely to be unstable. Unstable displaced fractures of the talus often require surgery to restore correct alignment and to give the best chance for the return to normal movement of the foot and ankle.
- Open fracture: When broken bones break through the skin, they are called open or compound fractures. Open fractures often involve much more damage to the surrounding muscles, tendons and ligaments. In addition, open fractures expose the fracture site to the environment. They have a higher risk for complications and infection and take a longer time to heal.
Talus fracture Hawkins classification 1:
- Type 1: Non-displaced fracture
- Type 2: Displaced fracture with subluxation or dislocation of the subtalar joint and a normal ankle joint
- Type 3: Displaced fracture with body of talus dislocated from both subtalar and ankle joint
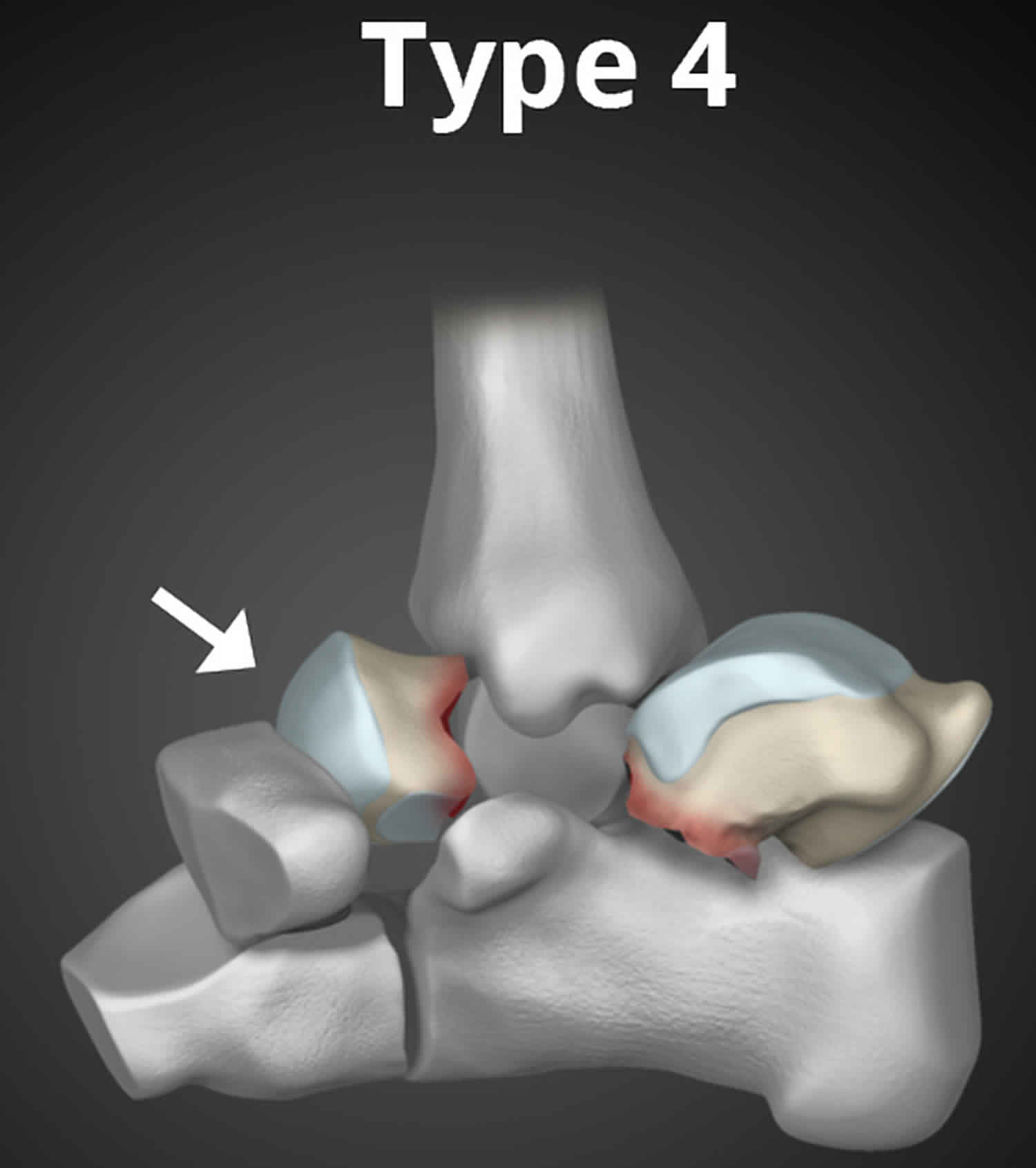
Canale and Kelly 2 described a rare type 4 category which in addition to features described for type 3 there is dislocation or subluxation of the head of the talus at the talonavicular joint.
Figure 2. Talus fracture type 1
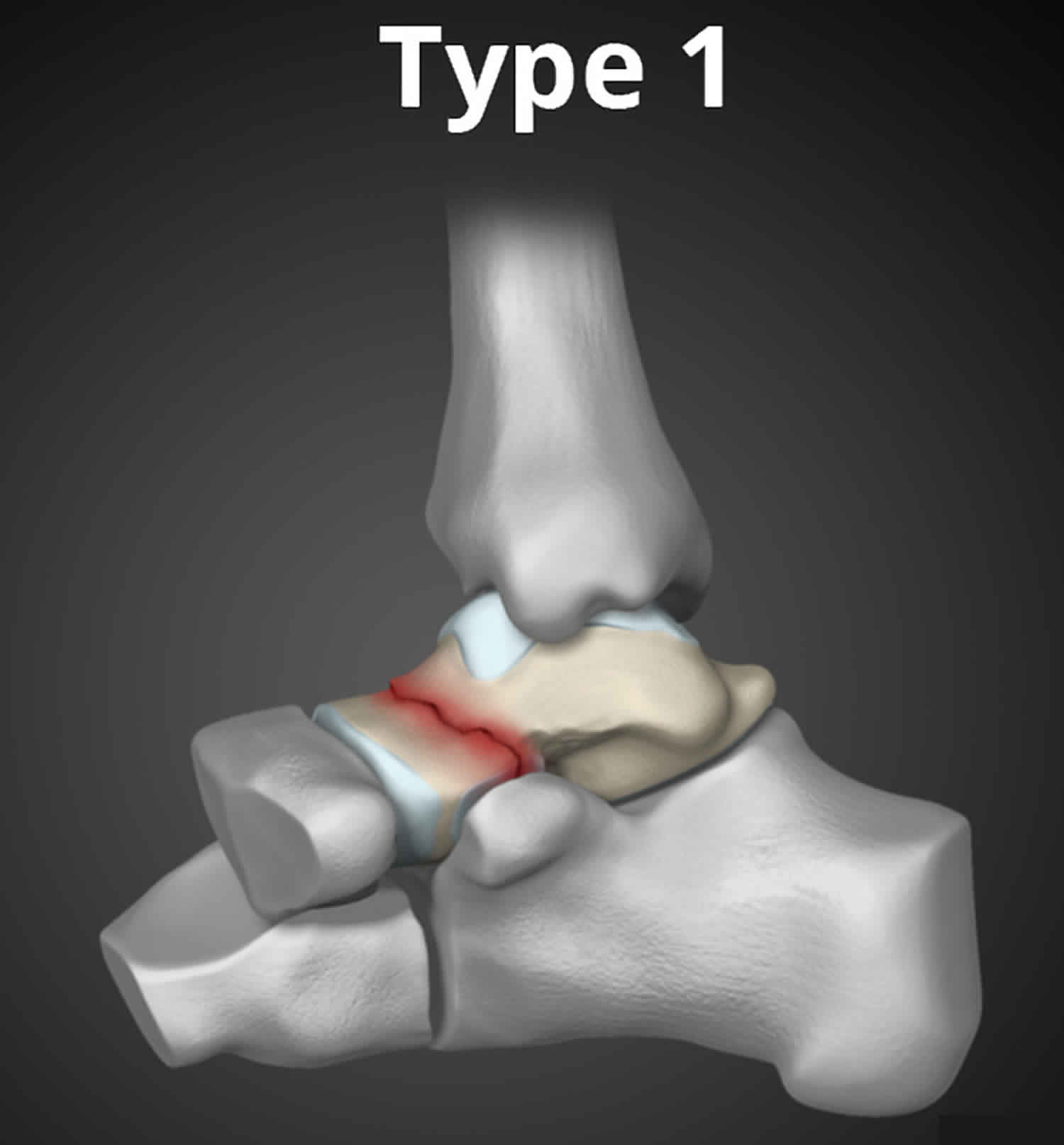
Figure 3. Talus fracture type 2
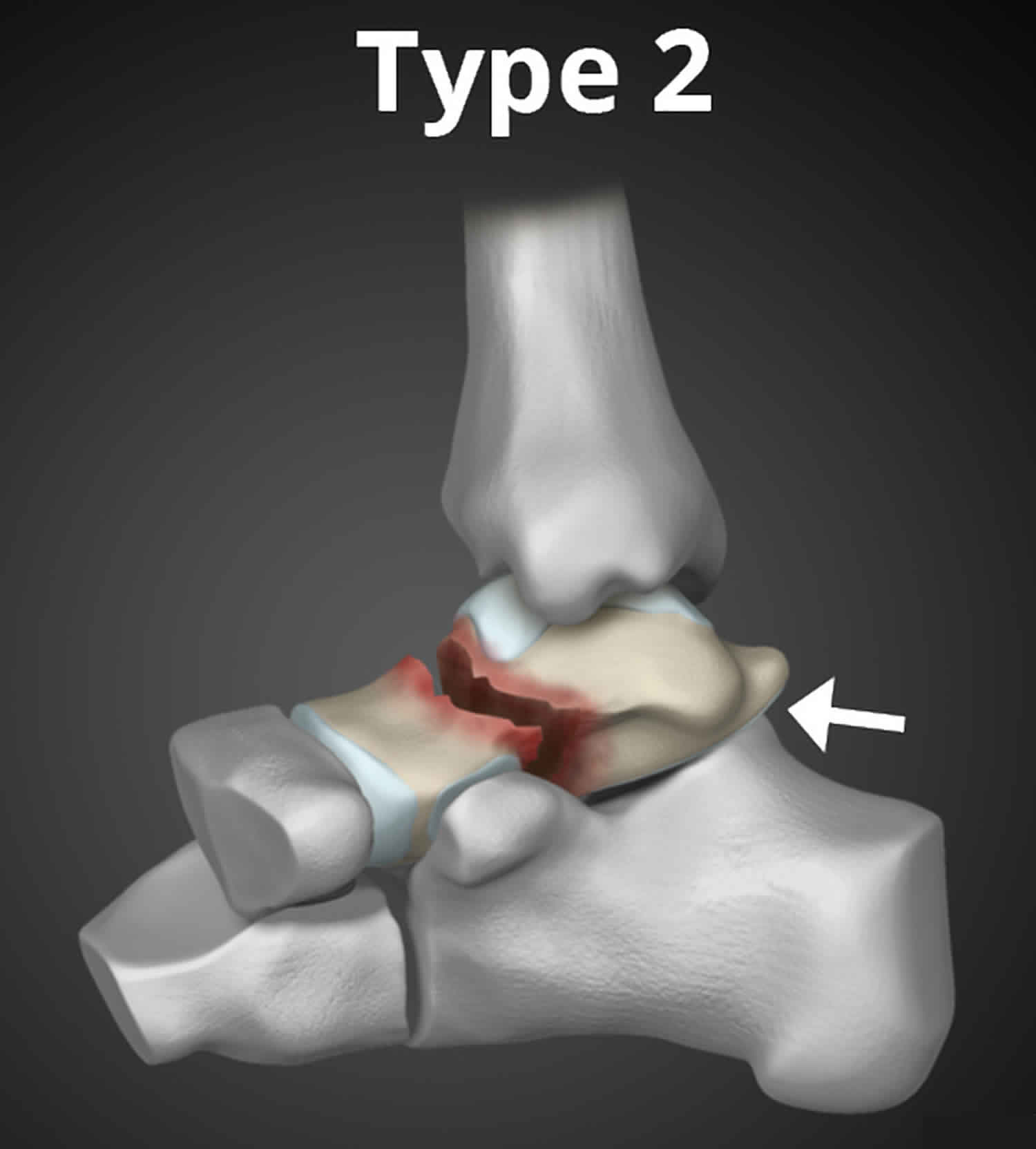
Figure 4. Talus fracture type 3
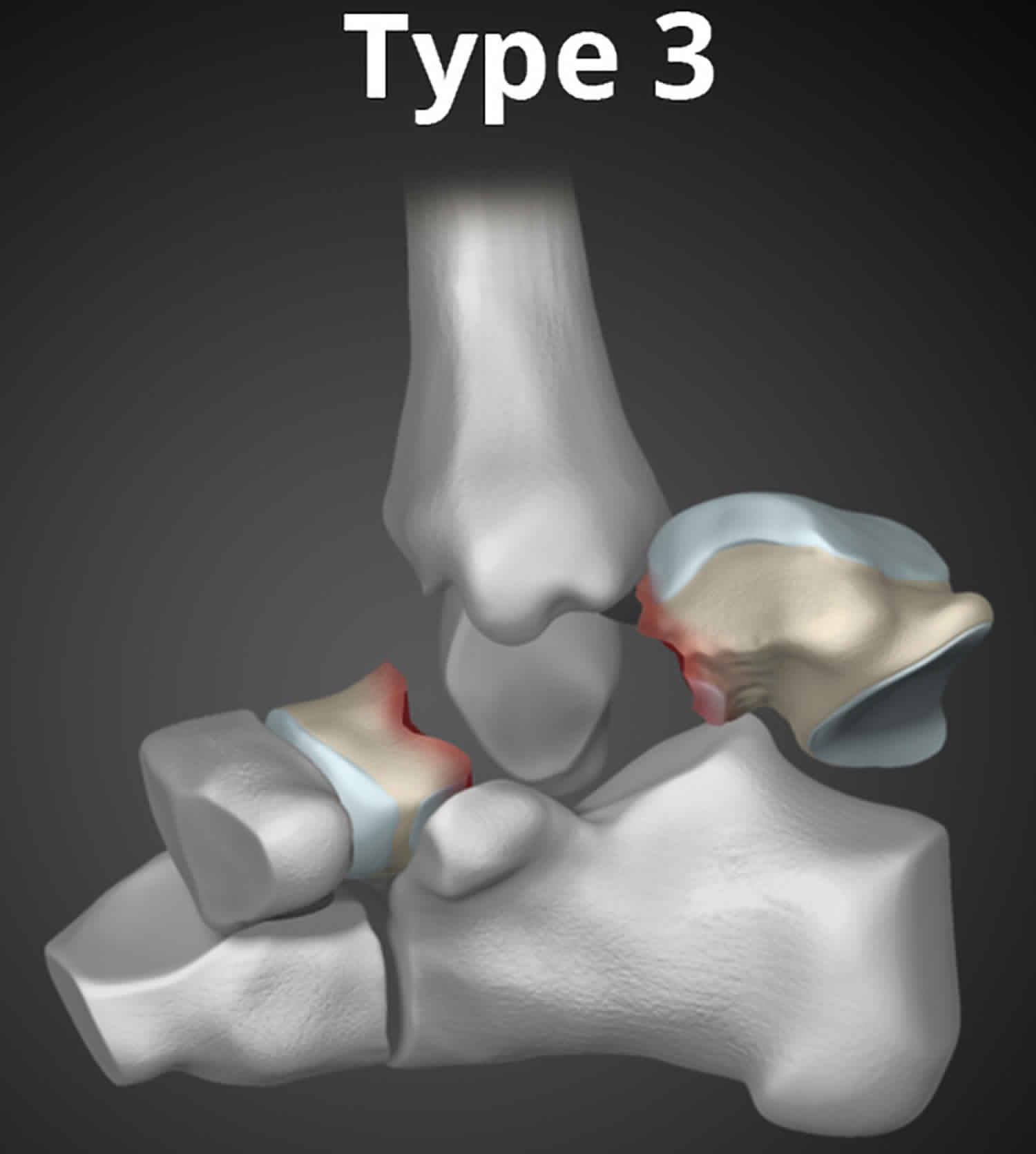
Figure 5. Talus fracture type 4
Talus fracture causes
Most talus fractures are the result of high-energy trauma such as a car collision or a fall from height. Injuries from sports, particularly from snowboarding, are another, less common, cause of talar injuries.
As with many types of fractures, the causes and risk factors can be divided into two types:
- Large forces on strong bones
- Talar fractures are common among sports people who sustain high impact falls and trauma. The sport commonly associated with talar fractures is snow-boarding.
- Other common causes are car accidents and falls onto the feet.
- Small forces on weak bones
- Osteoporosis and advanced age
- Medications and other drugs; most commonly, people who need to take high doses of steroids for long periods of time are at risk of developing weak bones
Risk factors for talus fracture
Risk factors for talus fractures include:
- Playing high impact, high speed sports, like snow-boarding
- Weak bones – usually due to osteoporosis
Talus fracture symptoms
Patients with talus fractures usually experience:
- Acute pain
- Inability to walk or bear weight on the foot
- Considerable swelling, bruising, and tenderness when the foot is touched
- Deformity – the foot might appear as though it is shaped differently to the uninjured foot due to the fracture
Talus fracture complications
Talus fracture complications vary depending on the type and site of the fracture. Some relatively common complications at the time of injury include:
- Infection. This is especially likely to occur if the skin around the ankle has been broken during the accident. Your surgeon will give you antibiotics to help prevent infection.
- Stiffness in the foot and ankle. The talus is a key bone in the ankle and foot, and while it is healing you may have to keep it still for weeks at a time. This unfortunately makes stiffness in the foot and ankle increasingly likely.
- Injury to other components of the foot. The accident that causes the talus fracutre may also cause sprains and tears in the tendons, muscles and other tissues around the talus.
There are a number of possible problems or complications related to any surgery – more information on these can be found here.
Some long-term complications include:
- Long-term pain, deformity and/or stiffness in the foot. The talus plays a key role in both the ankle and foot and consequently, damage to this bone is likely to affect both these areas. It is not always possible to predict who will develop these symptoms or how severe they will be. When pain is significantly affecting daily activities, a ‘salvage’ surgery can be used to relieve pain. This is most often arthrodesis, or fusion, of the joints.
- Posttraumatic arthritis is a type of arthritis that develops after an injury. Even when your bones heal normally, the cartilage protecting the bones can be damaged, leading to pain and stiffness over time. The majority of talus fractures result in some degree of posttraumatic arthritis. In cases of extreme arthritis that limits activity, additional surgery, such as a joint fusion or ankle replacement, may be the best option to relieve symptoms.
Some rarer complications include:
- Avascular necrosis (AVN) – this literally means death of the bone due to inadequate blood supply (a similar term is osteonecrosis). Avascular necrosis is a significat risk in talar fractures because the blood supply to the talus is relatively vulnerable. With unstable talus fractures, the blood supply to the bone can be disrupted at the time of the injury. Sometimes, the blood supply simply returns to the bone and normal healing begins. In other cases, however, the bone cells die without a blood supply, leading to a gradual and very painful collapse of the bone. Avascular necrosis is a serious complication because in addition to pain and instability, the dead bone is likely to become infected. For this reason, the dead bone needs to be removed. Furthermore, when the bone collapses, the articular cartilage covering the bone also collapses. Without this smooth cartilage, bone rubs against bone, leading to increased pain, arthritis and loss of motion and function. The more severe the talus fracture, the more likely it is that avascular necrosis will occur. Even fractures that are treated appropriately, including those that are treated surgically, may develop avascular necrosis. Some people are at greater risk of developing osteonecrosis in the talus, including those with diabetes, poor blood vessels to their foot, smokers and the elderly.
- Nonunion and malunion. These two occur when the bone fails to heal or heals in an inappropriate position. It sometimes occurs when weight is put on the healing bone too early, but can occur for no apparent reason.
Talus fracture diagnosis
Most people with talus fractures will go to an urgent care center or emergency room for initial treatment because of the severity of their symptoms.
Physical Examination
After discussing your symptoms and medical history, your doctor will do a careful examination. He or she will:
- Examine your foot and ankle carefully to see if there are any cuts from the injury.
- Check to see if you can move your toes, and can feel things on the bottom of your foot. In some cases, nerves may be injured at the same time that the bone is broken.
- Check your pulse at key points of the foot to be sure that there is good blood supply to the foot and toes.
- Check to see that pressure from fluids is not building up in the muscles of the foot, a condition called compartment syndrome. Compartment syndrome can result in loss of sensation and function, and requires emergency surgery once it is diagnosed.
- Determine whether you have received any other injuries by examining the rest of your injured foot and your legs, pelvis and spine.
Imaging Tests
Information from diagnostic imaging tests will help your doctor decide whether surgery is required and will be critical for surgical planning.
- X-rays. X-rays are the most common and widely available diagnostic imaging technique. An x-ray can show if the bone is broken and whether there is displacement (the gap between broken bones). It can also show how many pieces of bone there are.
- Computed tomography (CT) scan. If your doctor still needs more information after viewing your x-rays, a CT scan may also be ordered. A CT scan shows a cross-sectional image of your foot. It can provide valuable information about the severity of the fracture by helping your doctor see the fracture lines more clearly.
Talus fracture treatment
Immediate first aid treatment for a talus fracture, as with any painful ankle injury, is to apply a well-padded splint around the back of the foot and leg from the toe to the upper calf to immobilize the limb and protect it. Elevating the foot above the level of the heart helps to minimize swelling and pain. Specific treatment depends upon the severity and the type of fracture, so it is important to seek immediate medical attention.
In mild talus fractures where the bones remain in place, the foot can be immobilized in a cast without surgery. However, surgery is required in most forms of talar fracture. Following surgery, most people will need to avoid putting any weight on their foot for long periods of time.
Outcomes following talus fracture will depend greatly on whether the bone survives or becomes infected and needs to be removed. Even when the rehabilitation period is complication-free, rates of osteoarthritis following the injury are high.
Nonsurgical treatment
Only fractures that are well-aligned (stable) can be treated without surgery. This is very rare in a talus fracture, however, because of the high-energy force that causes the injury.
- Casting. A cast will hold the bones in your foot in place while they heal. You will have to wear a cast for 6 to 8 weeks. During this time, you will be asked to limit the amount of pressure you put on your foot. The goal is for the bone to heal enough for you to bear weight on it without the risk that it will move out of position.
- Rehabilitation. When the cast is removed, your doctor will give you exercises to help restore the range of motion and strengthen your foot and ankle.
Talus fracture surgery
If the bones have shifted out of place (displaced), surgery to internally set and stabilize the broken pieces results in the best outcome and reduces the risk of future complications.
The type of fracture and severity of injury to the surrounding tendons will influence the type of surgery chosen. Your surgeon will be able to discuss this with you in more detail, however some aspects that may come up include:
- Open reduction and internal fixation. During this operation, the bone fragments are first repositioned (reduced) into their normal alignment. They are then held together with special screws or metal plates and screws. While there a number of different techniques used to fix talar fractures, a common approach is to fuse the bones together.
- Bone grafts – if the talus is so damaged that fragments of bone need to be removed, your surgeon may ‘harvest’ extra bone from a thin bone in you leg called the fibula.
What happens in the first week after surgery?
After your operation, you will wake up with a large cast or bandage on your foot. For the first few days, you will need to keep your foot elevated and leave the cast in place to let the bone heal. After a few days, this cast is removed and a new cast applied. With this cast you will be asked to keep your foot elevated as much as possible (to prevent swelling and avascular necrosis), but also to perform exercises to keep the joints and muscles in you leg supple.
During this time you may be kept in hospital depending on:
- the severity and type of your injury,
- your other medical conditions (for example, if you have heart disease)
- and on your level of support at home.
If you remain in hospital you may be required to wear special thick white stockings and take drugs to prevent clots forming in your leg (see DVT). Once your doctors think you’re safe to return home, you may be reviewed by occupational therapists.
If you notice any of the following symptoms while in hospital inform your doctor immediately:
- Severe pain, or pain that gets worse in the days following the operation
- Tingling and numbness in your toes
- Toes that turn blue
Physiotherapy is vital in rehabilitation after talus fractures, so you will be seen by a physio either during your stay in hospital or very soon after you are discharged. They will advise you on exercises that will facilitate healing and maintain the other muscles and joints in your leg. During your rehabilitation, you will have a series of appointments with your physio who will:
- Review your joint and muscle function
- Assess your walking pattern
- Recommend exercises to promote the healing of your bones and muscles, as well as maintaining strength and flexibility in the other joints in your leg
Talus fracture recovery
Bones have a remarkable capacity to heal. The more severe your injury, however, the longer your recovery may be. After surgery, your foot will be in a splint or cast from 2 to 8 weeks, depending on the nature of the injury and how well your doctor thinks it is healing. As your bones begin to heal, your doctor will likely order x-rays to ensure that everything is in alignment and healing properly.
Pain management
After surgery, you will feel some pain. This is a natural part of the healing process. Your doctor and nurses will work to reduce your pain, which can help you recover from surgery faster.
Medications are often prescribed for short-term pain relief after surgery. Many types of medicines are available to help manage pain, including opioids, non-steroidal anti-inflammatory drugs (NSAIDs), and local anesthetics. Your doctor may use a combination of these medications to improve pain relief, as well as minimize the need for opioids.
Be aware that although opioids help relieve pain after surgery, they are a narcotic and can be addictive. Opioid dependency and overdose has become a critical public health issue in the U.S. It is important to use opioids only as directed by your doctor. As soon as your pain begins to improve, stop taking opioids. Talk to your doctor if your pain has not begun to improve within a few days of your surgery.
Early motion
Many doctors encourage motion of the foot and ankle early in the recovery period, as soon as your pain allows. Patients who have had surgery are instructed to begin moving the affected area as soon as the wound heals. Patients who are treated without surgery will work on regaining motion in the foot and ankle after the cast is removed.
At around two weeks
At around two weeks you will be reviewed by your surgeon who will:
- Remove your cast and check your ankle and foot for signs of skin damage and nerve and blood vessel injury
- Remove any stitches
- Check the joints in your foot are moving and not painful
- If you have not already had a review X-Ray, you will be asked to get one at this point. The review X-Ray lets your surgeon check that your bone is in the correct position and is healing well. (Keep in mind that this X-Ray does not exclude the possibility of avascular necrosis developing later on.)
At this point, you should still be keeping your leg elevated as much as possible. If your foot becomes very swollen the skin and blood supply can be comprimised.
Your surgeon will now suggest that you start putting some weight through your injured foot by placing your toe on the ground. This is called ‘partial weight-bearing’ and it is important that you:
- Only weight bear with assistance – for example, while leaning on a table or chair that can carry your weight. Your physio may recommend using crutches or other gait aids in these exercises.
- Do not put more weight on your leg than you can handle. If weight-bearing causes you significant pain do not force yourself.
Weight-bearing at this point helps to maintain the muscles in your leg and keeps your joints flexible.
After four weeks
You will again be reviewed by your surgeon who will check or change your cast or walking-boot, assess your foot and ankle and get review X-Rays. At this point, your surgeon may be able to tell you if your bone graft is healing into the talus and if the blood supply is good.
Your physio will increased the types of exercises you can do to include strengthening exercises as well as extending your range of motion and flexibility exercises.
If healing is progressing well, you can begin more weight-bearing. This usually involves putting some of your weight on your foot while walking with crutches. Do not, at any time, put your entire weight through your foot.
After six weeks, review X-Rays and an appointment with your surgeon will help to determine if your cast can be removed permanently and if your bones are healing well.
After two to three months
Depending on how well your bones are healing on X-Ray, you may be able to start full weght-bearing. Do not force yourself to take on more than is comfortable. At this point, you may still require walking aids to help you get around.
Physical therapy
Specific physical therapy exercises can improve the range of motion in your foot and ankle, and strengthen supporting muscles.
Weight-bearing
When you begin walking, you may need to use a cane and wear a special boot. You will not be able to put all of your weight on your foot for up to two to three months. If you place too much weight on your foot too soon, the bone pieces may move out of place. Be sure to follow your surgeon’s directions. As your break heals and your pain improves, you will be allowed to put more pressure on your foot.





{kind=link}