Contents
- Polycystic kidney disease
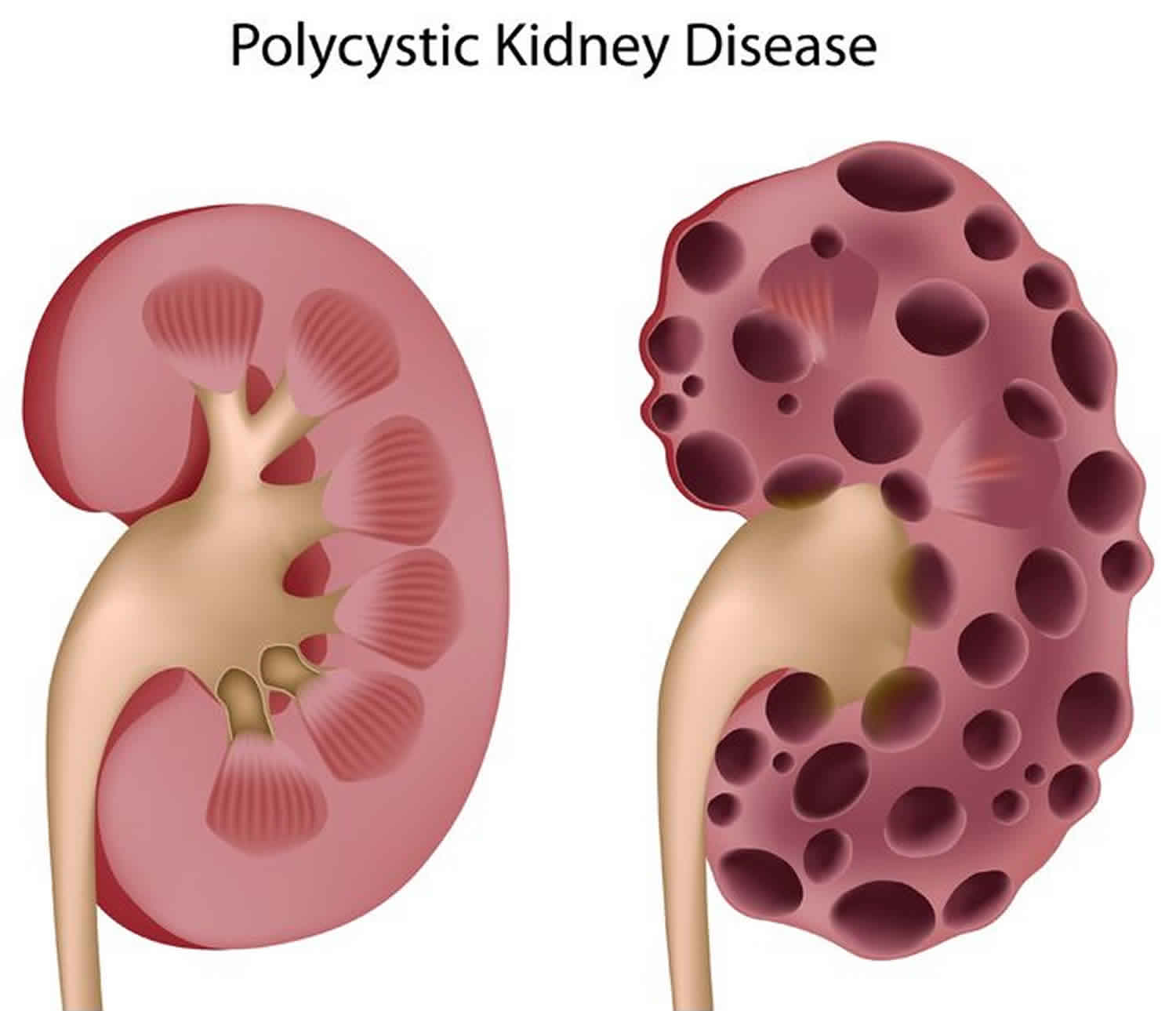
Polycystic kidney disease
Polycystic kidney disease is a disorder that causes numerous cysts to grow in the kidneys and other organs. Clusters of fluid-filled sacs, called cysts, develop in the kidneys and interfere with their ability to filter waste products from the blood. The growth of these cysts can slowly replace much of the kidneys, causing the kidneys to become enlarged, reducing kidney function and and can lead to kidney failure. People with polycystic kidney disease may also have cysts in their liver, pancreas, spleen, ovaries, and large bowel. Cysts in these organs usually do not cause serious problems, but can in some people. Polycystic kidney disease can also affect the brain or heart. People with polycystic kidney disease have an increased risk of an abnormal bulging (an aneurysm) in a large blood vessel called the aorta or in blood vessels at the base of the brain. An aneurysm is a bulging blood vessel that can burst, resulting in a stroke or even death. If polycystic kidney disease affects the heart, the valves can become floppy, resulting in a heart murmur in some patients.
Frequent complications of polycystic kidney disease include dangerously high blood pressure (hypertension), pain in the back or sides, blood in the urine (hematuria), recurrent urinary tract infections, kidney stones, and heart valve abnormalities.
The two major forms of polycystic kidney disease are distinguished by the usual age of onset and the pattern in which it is passed through families. The autosomal dominant polycystic kidney disease (sometimes called ADPKD) has signs and symptoms that typically begin in adulthood, although cysts in the kidney are often present from birth or childhood. Autosomal dominant polycystic kidney disease can be further divided into type 1 and type 2, depending on the genetic cause. The autosomal recessive form of polycystic kidney disease (sometimes called ARPKD) is much rarer and is often lethal early in life. The signs and symptoms of this condition are usually apparent at birth or in early infancy.
Polycystic kidney disease is a fairly common genetic disorder. In the United States about 600,000 people have polycystic kidney disease. It is the fourth leading cause of kidney failure. It is found in all races and occurs equally in men and women. It causes about 5% of all kidney failure. The autosomal dominant form of polycystic kidney disease is much more common than the autosomal recessive form. Autosomal dominant polycystic kidney disease affects 1 in 500 to 1,000 people, while the autosomal recessive polycystic kidney disease occurs in an estimated 1 in 20,000 to 40,000 people 1.
Does everyone with polycystic kidney disease develop kidney failure?
No. About 50 percent of people with polycystic kidney disease will have kidney failure by age 60, and about 60 percent will have kidney failure by age 70. People with kidney failure will need dialysis or a kidney transplant. Certain people have an increased risk of kidney failure including:
- men
- patients with high blood pressure
- patients with protein or blood in their urine
- women with high blood pressure who have had more than three pregnancies
Should women with polycystic kidney disease get pregnant?
Most of the women with polycystic kidney disease (80 percent) have successful and uneventful pregnancies. However, some women with polycystic kidney disease have an increased risk for serious complications for themselves and their babies. This includes women with polycystic kidney disease who also have:
- high blood pressure
- decreased kidney function
Women who have polycystic kidney disease with high blood pressure develop pre-eclampsia (or toxemia) in 40 percent of pregnancies. This is a life-threatening disorder for both the mother and baby, and it can develop suddenly and without warning. Therefore, all women with polycystic kidney disease, particularly those who also have high blood pressure, should be followed closely during their pregnancy by their doctor.
Polycystic kidney disease types
There are three main types of polycystic kidney disease:
Autosomal dominant polycystic kidney disease (ADPKD)
Autosomal dominant polycystic kidney disease is passed from parent to child by dominant inheritance. In other words, only one copy of the abnormal gene is needed to cause the disease. Symptoms usually begin between the ages of 30 and 40, but they can begin earlier, even in childhood. ADpolycystic kidney disease is the most common form of polycystic kidney disease. In fact, about 90 percent of all polycystic kidney disease cases are ADpolycystic kidney disease.
Autosomal recessive polycystic kidney disease (ARPKD)
Infantile or autosomal recessive polycystic kidney disease is passed from parent to child by recessive inheritance. Symptoms can begin in the earliest months of life, even in the womb. It tends to be very serious, progresses rapidly, and is often fatal in the first few months of life. Autosomal recessive polycystic kidney disease is extremely rare. It occurs in 1 out of 20,000 to 40,000 people.
Acquired cystic kidney disease
Acquired cystic kidney disease can happen in kidneys with long-term damage and severe scarring, so it is often associated with kidney failure and dialysis. About 90 percent of people on dialysis for 5 years develop acquired cystic kidney disease. People with acquired cystic kidney disease usually seek help because they notice blood in their urine. This is because the cysts bleed into the urinary system, which discolors urine.
Polycystic kidney disease causes
Mutations in the PKD1, PKD2, and PKHD1 genes cause polycystic kidney disease 2.
Mutations in either the PKD1 or PKD2 gene can cause autosomal dominant polycystic kidney disease; PKD1 gene mutations cause autosomal dominant polycystic kidney disease type 1, and PKD2 gene mutations cause autosomal dominant polycystic kidney disease type 2. These genes provide instructions for making proteins whose functions are not fully understood. Researchers believe that they are involved in transmitting chemical signals from outside the cell to the cell’s nucleus. The two proteins work together to promote normal kidney development, organization, and function. Mutations in the PKD1 or PKD2 gene lead to the formation of thousands of cysts, which disrupt the normal functions of the kidneys and other organs. People with mutations in the PKD2 gene, particularly women, typically have a less severe form of the disease than people with PKD1 mutations. The signs and symptoms, including a decline in kidney function, tend to appear later in adulthood in people with a PKD2 mutation.
Mutations in the PKHD1 gene cause autosomal recessive polycystic kidney disease. This gene provides instructions for making a protein whose exact function is unknown; however, the protein likely transmits chemical signals from outside the cell to the cell nucleus. Researchers have not determined how mutations in the PKHD1 gene lead to the formation of numerous cysts characteristic of polycystic kidney disease.
Although polycystic kidney disease is usually a genetic disorder, a small percentage of cases are not caused by gene mutations. These cases are called acquired polycystic kidney disease. This form of the disorder occurs most often in people with other types of kidney disease who have been treated for several years with hemodialysis (a procedure that filters waste products from the blood).
Polycystic kidney disease inheritance pattern
Most cases of polycystic kidney disease have an autosomal dominant pattern of inheritance. People with this condition are born with one mutated copy of the PKD1 or PKD2 gene in each cell. In about 90 percent of these cases, an affected person inherits the mutation from one affected parent. The other 10 percent of cases result from a new mutation in one of the genes and occur in people with no history of the disorder in their family.
In cases where the autosomal dominant polycystic kidney disease does run in the family, the chance for an affected person to have a child with the same condition is 50% regardless of whether it is a boy or a girl. These possible outcomes occur randomly. The chance remains the same in every pregnancy and is the same for boys and girls.
- When one parent has the abnormal gene, they will pass on either their normal gene or their abnormal gene to their child. Each of their children therefore has a 50% (1 in 2) chance of inheriting the changed gene and being affected by the condition.
- There is also a 50% (1 in 2) chance that a child will inherit the normal copy of the gene. If this happens the child will not be affected by the disorder and cannot pass it on to any of his or her children.
Although one altered copy of a gene in each cell is sufficient to cause the disorder, an additional mutation in the second copy of the PKD1 or PKD2 gene may make cysts grow faster and increase the severity of the disease. The rate at which cysts enlarge and cause a loss of kidney function varies widely, and may be influenced by mutations in other genes that have not been identified.
Polycystic kidney disease also can be inherited in an autosomal recessive pattern. People with this form of the condition have two altered copies of the PKHD1 gene in each cell. The parents of a child with an autosomal recessive disorder are not affected but are carriers of one copy of the altered gene.
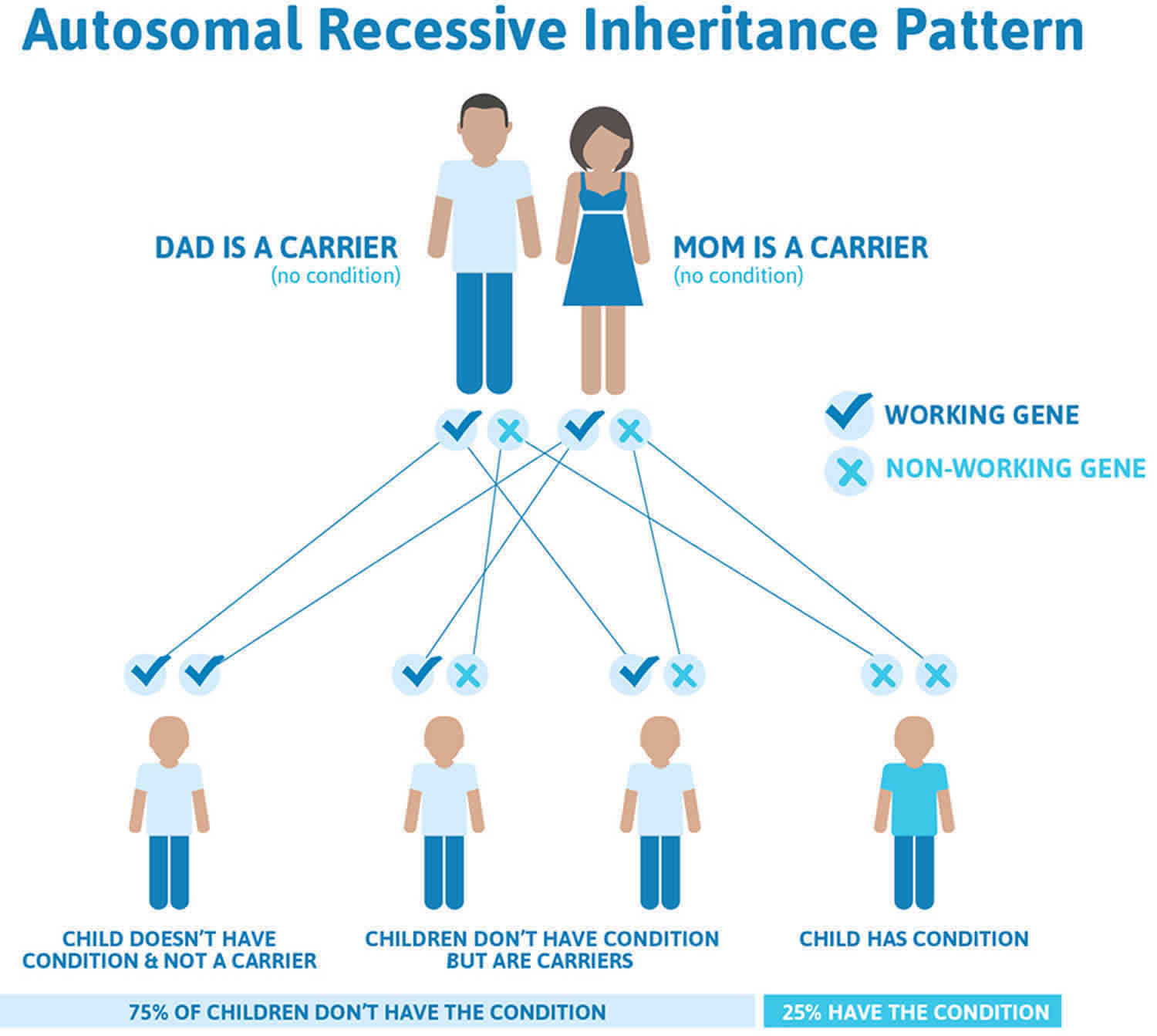
Autosomal recessive conditions are individually pretty rare, so the chance that you and your partner are carriers for the same recessive genetic condition are likely low. Even if both partners are a carrier for the same condition, there is only a 25% chance that they will both pass down the non-working copy of the gene to the baby, thus causing a genetic condition. This chance is the same with each pregnancy, no matter how many children they have with or without the condition.
- If both partners are carriers of the same abnormal gene, they may pass on either their normal gene or their abnormal gene to their child. This occurs randomly.
- Each child of parents who both carry the same abnormal gene therefore has a 25% (1 in 4) chance of inheriting a abnormal gene from both parents and being affected by the condition.
- This also means that there is a 75% ( 3 in 4) chance that a child will not be affected by the condition. This chance remains the same in every pregnancy and is the same for boys or girls.
- There is also a 50% (2 in 4) chance that the child will inherit just one copy of the abnormal gene from a parent. If this happens, then they will be healthy carriers like their parents.
- Lastly, there is a 25% (1 in 4) chance that the child will inherit both normal copies of the gene. In this case the child will not have the condition, and will not be a carrier.
Figure 1. Polycystic kidney disease autosomal dominant inheritance pattern
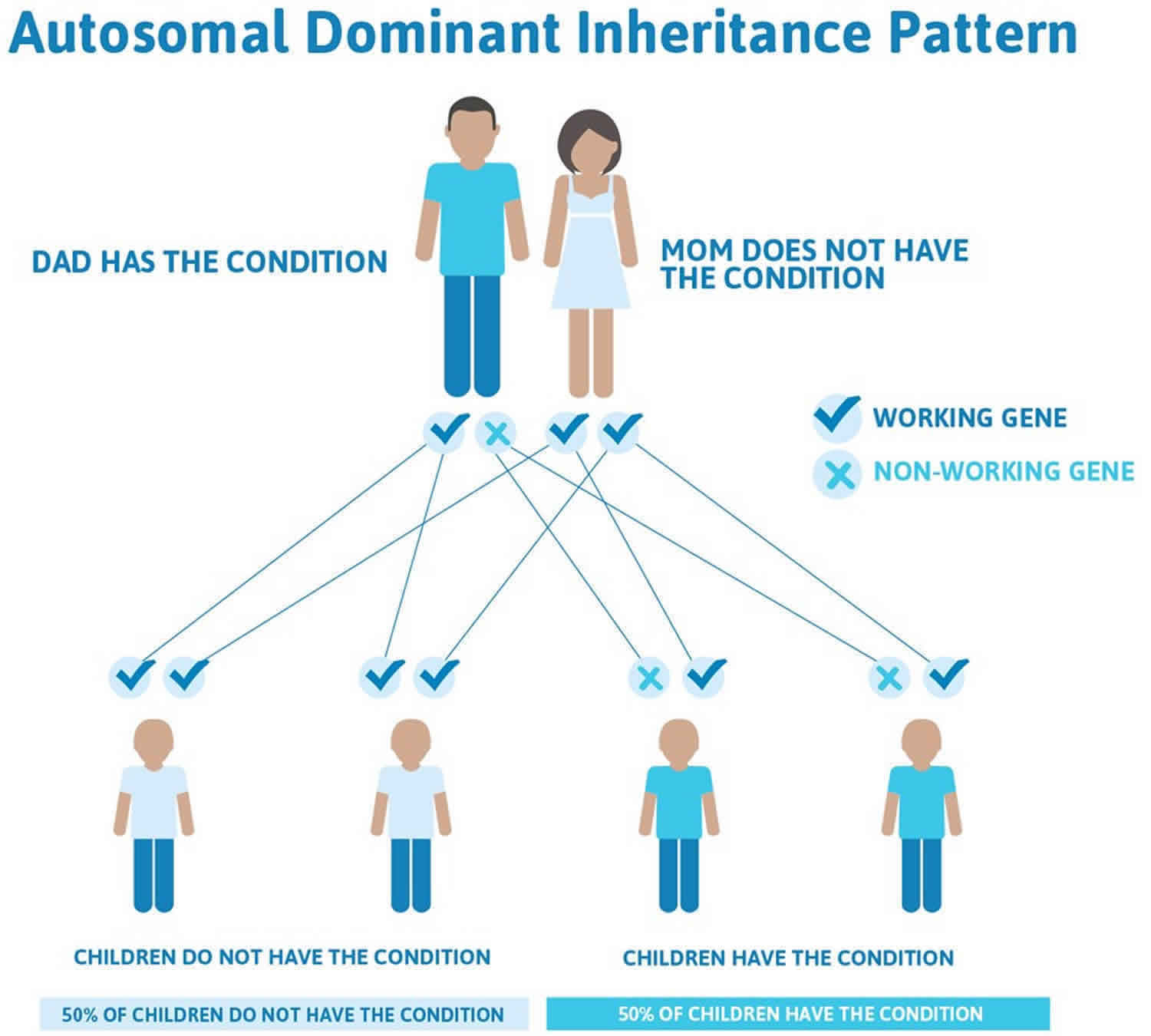
Figure 2. Polycystic kidney disease autosomal recessive inheritance pattern
The sooner you know you or your child has polycystic kidney disease, the sooner you can keep the condition from getting worse. Getting tested if you or your child are at risk for polycystic kidney disease can help you take early action.
People with specific questions about genetic risks or genetic testing for themselves or family members should speak with a genetics professional.
Resources for locating a genetics professional in your community are available online:
- The National Society of Genetic Counselors (https://findageneticcounselor.nsgc.org) offers a searchable directory of genetic counselors in the United States and Canada. You can search by location, name, area of practice/specialization, and/or ZIP Code.
- The American Board of Genetic Counseling (https://abgc.learningbuilder.com/Search/Public/MemberRole/Verification) provides a searchable directory of certified genetic counselors worldwide. You can search by practice area, name, organization, or location.
- The Canadian Association of Genetic Counselors (https://www.cagc-accg.ca/index.php?page=225) has a searchable directory of genetic counselors in Canada. You can search by name, distance from an address, province, or services.
- The American College of Medical Genetics and Genomics (https://www.acmg.net/ACMG/Directories.aspx) has a searchable database of medical genetics clinic services in the United States.
Polycystic kidney disease prevention
Researchers have not yet found a way to prevent polycystic kidney disease. However, you may be able to slow polycystic kidney disease problems caused by high blood pressure, such as kidney damage. Aim for a blood pressure goal of less than 120/80. Work with a health care team to help manage your or your child’s polycystic kidney disease. Your health care team will probably include a general practitioner and a nephrologist, a health care provider specializing in kidney health.
Here are some tips for keeping your blood pressure in check:
- Take the blood pressure medications prescribed by your doctor as directed.
- Eat a low-salt diet containing plenty of fruits, vegetables and whole grains.
- Maintain a healthy weight. Ask your doctor what the right weight is for you.
- If you smoke, quit.
- Exercise regularly. Aim for at least 30 minutes of moderate physical activity most days of the week.
- Limit alcohol use.
If you have polycystic kidney disease and you’re considering having children, a genetic counselor can help you assess your risk of passing the disease to your offspring.
Polycystic kidney disease symptoms
Most people do not develop symptoms until they are 30 to 40 years old. The first noticeable signs and symptoms may include:
- Back or side pain
- An increase in the size of the abdomen
- Blood in the urine
- Frequent bladder or kidney infections
- High blood pressure
High blood pressure is the most common sign of polycystic kidney disease. Occasionally, patients may develop headaches related to high blood pressure or their doctors may detect high blood pressure during a routine physical exam. Because high blood pressure can cause kidney damage, it is very important to treat it. In fact, treatment of high blood pressure can help slow or even prevent kidney failure.
Fluttering or pounding in the chest
About 25% of polycystic kidney disease patients have a so-called floppy valve in the heart, and may experience a fluttering or pounding in the chest as well as chest pain. These symptoms almost always disappear on their own but may be the first hint that someone has polycystic kidney disease.
Autosomal recessive polycystic kidney disease symptoms
Early signs of autosomal recessive polycystic kidney disease in the womb are larger-than-normal kidneys and a smaller-than-average size baby, a condition called growth failure. The early signs of autosomal recessive polycystic kidney disease are also complications. However, some people with autosomal recessive polycystic kidney disease do not develop signs or symptoms until later in childhood or even adulthood.
Polycystic kidney disease complications
Complications associated with polycystic kidney disease include:
- High blood pressure. Elevated blood pressure is a common complication of polycystic kidney disease. Untreated, high blood pressure can cause further damage to your kidneys and increase your risk of heart disease and stroke.
- Loss of kidney function. Progressive loss of kidney function is one of the most serious complications of polycystic kidney disease. Nearly half of those with the disease have kidney failure by age 60. Polycystic kidney disease can interfere with the ability of your kidneys to keep wastes from building to toxic levels, a condition called uremia. As the disease worsens, end-stage kidney (renal) failure may result, necessitating ongoing kidney dialysis or a transplant to prolong your life.
- Pregnancy complications. Pregnancy is successful for most women with polycystic kidney disease. In some cases, however, women may develop a life-threatening disorder called preeclampsia. Those most at risk have high blood pressure before they become pregnant.
- Growth of cysts in the liver. The likelihood of developing liver cysts for someone with polycystic kidney disease increases with age. While both men and women develop cysts, women often develop larger cysts. Female hormones might contribute to cyst development.
- Development of an aneurysm in the brain. A balloonlike bulge in a blood vessel (aneurysm) in your brain can cause bleeding (hemorrhage) if it ruptures. People with polycystic kidney disease have a higher risk of aneurysm. People with a family history of aneurysm seem to be at highest risk.
- Heart valve abnormalities. As many as 1 in 4 adults with polycystic kidney disease develops mitral valve prolapse. When this happens, the valve no longer closes properly, which allows blood to leak backward.
- Colon problems. Weaknesses and pouches or sacs in the wall of the colon (diverticulosis) may develop in people with polycystic kidney disease.
- Chronic pain. Pain is a common symptom for people with polycystic kidney disease. It often occurs in your side or back. The pain can also be associated with a urinary tract infection, a kidney stone or a malignancy.
Polycystic kidney disease diagnosis
Ultrasound is the most reliable, inexpensive and non-invasive way to diagnose polycystic kidney disease. If someone at risk for polycystic kidney disease is older than 40 years and has a normal ultrasound of the kidneys, he or she probably does not have polycystic kidney disease. Occasionally, a CT scan (computed tomography scan) and MRI (magnetic resonance imaging) may detect smaller cysts that cannot be found by an ultrasound. MRI is used to measure and monitor volume and growth of kidneys and cysts.
In some situations, genetic testing might also be done. This involves a blood test that checks for abnormal genes that cause the disease. Genetic testing is not recommended for everyone. The test is costly, and it also fails to detect polycystic kidney disease in about 15% of people who have it. However, genetic testing can be useful when a person:
- has an uncertain diagnosis based on imaging tests
- has a family history of polycystic kidney disease and wants to donate a kidney
- is younger than 30-years old with a family history of polycystic kidney disease and a negative ultrasound, and is planning to start a family
Polycystic kidney disease treatment
At present, there is no cure for polycystic kidney disease. However, a lot of research is being done. Recent studies suggest that drinking plain water throughout the day and avoiding caffeine in beverages can slow the growth of cysts. Research is also helping us understand the genetic basis of polycystic kidney disease.
Studies also suggest that some treatments may slow the rate of kidney disease in polycystic kidney disease, but further research is needed before these treatments can be used in patients. In the meantime, many supportive treatments can be done to control symptoms, help slow the growth of cysts, and help prevent or slow down the loss of kidney function in people with polycystic kidney disease. These include:
- Careful control of blood pressure
- Prompt treatment with antibiotics of a bladder or kidney infection
- Lots of fluid when blood in the urine is first noted
- Medication to control pain (talk to your doctor about which over-the-counter medicines are safe to take if you have kidney disease)
- A healthy lifestyle with regard to smoking cessation, exercise, weight control and reduced salt intake
- Drinking lots of plain water throughout the day
- Avoiding caffeine in all beverages
- Kidney failure. If your kidneys lose their ability to remove waste products and extra fluids from your blood, you’ll eventually need either dialysis or a kidney transplant.
- Aneurysms. If you have polycystic kidney disease and a family history of ruptured brain (intracranial) aneurysms, your doctor may recommend regular screening for intracranial aneurysms.
In April 2018, the U.S. Food and Drug Administration (FDA) approved a new drug called tolvaptan for the treatment of autosomal dominant polycystic kidney disease. The drug can be used to help slow kidney function decline in adults at risk for this type of polycystic kidney disease. You can speak with a healthcare professional for more information about this treatment and if it’s right for you.
If lifestyle and diet changes don’t help control your blood pressure, a health care provider may prescribe one or more blood pressure medicines. Two types of blood pressure medicines, angiotensin-converting enzyme (ACE) inhibitors and angiotensin receptor blockers (ARBs), may slow kidney disease and delay kidney failure.
If an aneurysm is discovered, surgical clipping of the aneurysm to reduce the risk of bleeding may be an option, depending on its size. Nonsurgical treatment of small aneurysms may involve controlling high blood pressure and high blood cholesterol, as well as quitting smoking.
Polycystic kidney disease diet
At present, no specific diet is known to prevent cysts from developing in patients with polycystic kidney disease. Reducing salt intake helps control blood pressure in polycystic kidney disease patients who have high blood pressure. A diet low in fat and moderate in calories is recommended to maintain a healthy weight. Speak to your doctor or a dietitian about other changes to your diet, such as avoiding caffeine.
It is important not to become too dehydrated during any physical activity.
Lifestyle changes
You also can take steps to help delay or prevent kidney failure. Healthy lifestyle practices such as being active, reducing stress, and quitting smoking can help.
- Be active for 30 minutes or more on most days. Regular physical activity can help you reduce stress, manage your weight, and control your blood pressure. If you are not active now, ask your health care provider about how much and what type of physical activity is right for you.
- If you play contact sports, such as football or hockey, a health care provider should do a magnetic resonance imaging (MRI) test to see whether these sports are safe for you. Trauma to your body, especially to your back and sides, may cause kidney cysts to burst.
- Lose weight. Being overweight makes your kidneys work harder. Losing weight helps protect your kidneys.
- Aim for 7 to 8 hours of sleep each night. Getting enough sleep is important to your overall physical and mental health and can help you manage your blood pressure and blood glucose, or blood sugar.
- Reduce stress. Long-term stress can raise your blood pressure and even lead to depression. Some of the steps you take to manage your polycystic kidney disease are also healthy ways to cope with stress. For example, getting enough physical activity and sleep helps reduce stress.
- Quit smoking. Cigarette smoking can raise your blood pressure, making your kidney damage worse. Quitting smoking may help you meet your blood pressure goals, which is good for your kidneys and can lower your chances of having a heart attack or stroke. Quitting smoking is even more important for people with polycystic kidney disease who have aneurysms. An aneurysm is a bulge in the wall of a blood vessel.
Polycystic kidney disease prognosis
The prognosis in patients with autosomal dominant polycystic kidney disease covers a wide spectrum. Renal failure has been reported in children; conversely, individuals with autosomal dominant polycystic kidney disease may live a normal lifespan without knowing that they have the disease. More typically, however, autosomal dominant polycystic kidney disease causes progressive renal dysfunction, resulting in grossly enlarged kidneys and kidney failure by the fourth to sixth decade of life. There is an inverse association between the size of polycystic kidneys and the level of glomerular filtration 3.
An early study estimated that approximately 70% of patients with autosomal dominant polycystic kidney disease would develop renal insufficiency if they survived to age 65 years. Currently, half of all patients with autosomal dominant polycystic kidney disease require renal replacement therapy by age 60 years. Risk factors for progression include the following:
- PKD1 genotype
- Large kidneys
- Several episodes of gross hematuria 4
- Severe and frequent kidney infections
- Hypertension
- Multiple pregnancies
- Black racial background 5
- Male sex
The presence of more than one risk factor increases the risk of progression to end-stage renal disease (ESRD).
Although the 2 forms of autosomal dominant polycystic kidney disease, autosomal dominant polycystic kidney disease type 1 and autosomal dominant polycystic kidney disease type 2, share similar clinical features, renal prognosis is strikingly different 6. Autosomal dominant polycystic kidney disease type 2 is a milder disease, based on the age of onset of end-stage renal disease. The median age of renal survival for individuals with autosomal dominant polycystic kidney disease type 1 is 56 years, compared with 68 years in those with autosomal dominant polycystic kidney disease type 2. Although autosomal dominant polycystic kidney disease type 2 is milder than autosomal dominant polycystic kidney disease type 1, it has an overall impact on survival and shortens life expectancy.
Cardiovascular pathology and infections account for approximately 90% of deaths in patients treated with hemodialysis or peritoneal dialysis and after renal transplantation. A rare cause of mortality is in autosomal dominant polycystic kidney disease is subarachnoid hemorrhage from intracranial aneurysms 7.
In a retrospective, observational study of 88 patients with autosomal dominant polycystic kidney disease who died between 1981 and 1999, Rahman et al 8 determined that almost half of the patients died of cardiovascular problems. The median age of death was 60.5 years. Causes of death included the following:
- Cardiovascular problems – 46.6% of patients
- Infection – 15.9% of patients, with 42% of these deaths resulting from septicemia
- Central nervous system disorders – 11.36% of patients, with 60% of these deaths caused by cerebrovascular events
- Uremia – 2.2% of patients
- Other, miscellaneous causes – 11.36%
The Mayo Clinic calculator for autosomal dominant polycystic kidney disease is a useful tool for predicting disease progression (https://www.mayo.edu/research/documents/pkd-center-adpkd-classification/doc-20094754). Recommendations for assessing rapid progression of autosomal dominant polycystic kidney disease have been provided by European experts 9.
- Guay-Woodford LM, Desmond RA. Autosomal recessive polycystic kidney disease: the clinical experience in North America. Pediatrics. 2003;111(5 Pt 1):1072–1080.[↩]
- Polycystic kidney disease. https://ghr.nlm.nih.gov/condition/polycystic-kidney-disease[↩]
- Grantham JJ, Torres VE, Chapman AB, et al. Volume progression in polycystic kidney disease. N Engl J Med. 2006 May 18. 354(20):2122-30.[↩]
- Idrizi A, Barbullushi M, Petrela E, et al. The influence of renal manifestations to the progression of autosomal dominant polycystic kidney disease. Hippokratia. 2009 Jul. 13(3):161-4.[↩]
- Fary Ka E, Seck SM, Niang A, et al. Patterns of autosomal dominant polycystic kidney diseases in black Africans. Saudi J Kidney Dis Transpl. 2010 Jan. 21(1):81-6.[↩]
- Hateboer N, v Dijk MA, Bogdanova N, et al. Comparison of phenotypes of polycystic kidney disease types 1 and 2. European PKD1-PKD2 Study Group. Lancet. 1999 Jan 9. 353(9147):103-7.[↩]
- Chauveau D, Pirson Y, Verellen-Dumoulin C, et al. Intracranial aneurysms in autosomal dominant polycystic kidney disease. Kidney Int. 1994 Apr. 45(4):1140-6.[↩]
- Rahman E, Niaz FA, Al-Suwaida A, et al. Analysis of causes of mortality in patients with autosomal dominant polycystic kidney disease: A single center study. Saudi J Kidney Dis Transpl. 2009 Sep-Oct. 20(5):806-10.[↩]
- Chapman AB, Devuyst O, Eckardt KU, Gansevoort RT, Harris T, Horie S, et al. Autosomal-dominant polycystic kidney disease (ADPKD): executive summary from a Kidney Disease: Improving Global Outcomes (KDIGO) Controversies Conference. Kidney Int. 2015 Jul. 88 (1):17-27.[↩]





{kind=link}