Contents
Spiradenoma
Spiradenoma also called eccrine spiradenoma is a rare, benign sweat glands tumor that originates in the skin 1. Spiradenomas or eccrine spiradenomas arise from the eccrine sweat glands that form small, solitary nodules that can grow to several centimeters in size (0.3 to 5 cm) 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12. Usually, there is no connection to the overlying epidermis 13. However, some authors indicate spiradenoma arising from apocrine gland origin 14, 15.
Eccrine spiradenomas form firm nodules that show up on your scalp, neck and upper body, but can also occur in other areas like the breast. Although rare, multiple eccrine spiradenomas on the trunk and extremities have been described 16, 17. Typically, eccrine spiradenomas are often blue or flesh-colored, but may also be grey, pink, purple, red or yellow slow growing and solitary nodule on the head or upper trunk in adult patients and can be very painful 18, 19, 20, 21, 22. Spiradenoma skin tumors range from under 1 cm to several centimeters. Spiradenomas are sometimes painful.
Eccrine spiradenoma can occur at any age, but most often affects young adults in the 2nd to 4th decades of life with no difference between males or females 23, 24, 25, 18.
While eccrine spiradenomas are usually benign, long-standing lesions can sometimes develop into malignant spiradenocarcinomas, especially in people over 50 26, 27, 28, 29, 30, 31. Spiradenocarcinomas (malignant spiradenomas) are aggressive and have high metastasis rates and low survival rates.
Ultrasound evaluation of the tumor generally reveals a smooth, lobulated mass in the superficial subcutaneous tissue 32. The mass appears hypoechoic and often has increased vascularity. The classic MRI appearance is a T1-hypointense, T2-hyperintense mass, with homogeneous enhancement after contrast administration 33.
Clinically, it is difficult to differentiate eccrine spiradenoma from other skin tumors, therefore biopsy is vital for accurate diagnosis. It is important to find out epithelial cells, myoepithelial cells and lymphocytes along with void spaces between blood vessels under the microscopes for diagnostic confirmations 6. Characteristic histological findings on hematoxylin and eosin (H&E) staining are two distinct cell types: a basaloid cell population with hyperchromatic nuclei and scant cytoplasm and a larger cell type with abundant, pale cytoplasm 34, 13. The cells are arranged into sheets, cords, or trabeculae, with cells with large nucleus and pale cytoplasm are located in the center and cells with smaller dense nucleus are located in the periphery 6. The lumen of this contains an acidic substance which is being arranged around a smaller lumen. Some tumors are markedly vascular with cystic dilation of their vascular channels, likely accounting for their increased vascularity seen on ultrasound 32, 13.
Eccrine spiradenoma may accompany similar tumors of apocrine origin, such as trichoblastoma and cylindroma. Histologically, the eccrine glands have relatively clear cytoplasm and occasionally squamous epithelium whereas the apocrine glands have eosinophilic cytoplasm and nuclei located at the base bottom (off centered) 35.
The standard treatment for spiradenoma is surgical excision, but with no clear consensus regarding the width of surgical margins 36. Imaging techniques like CT scans, MRIs, and ultrasounds can also be used to help with treatment.
Figure 1. Eccrine sweat glands
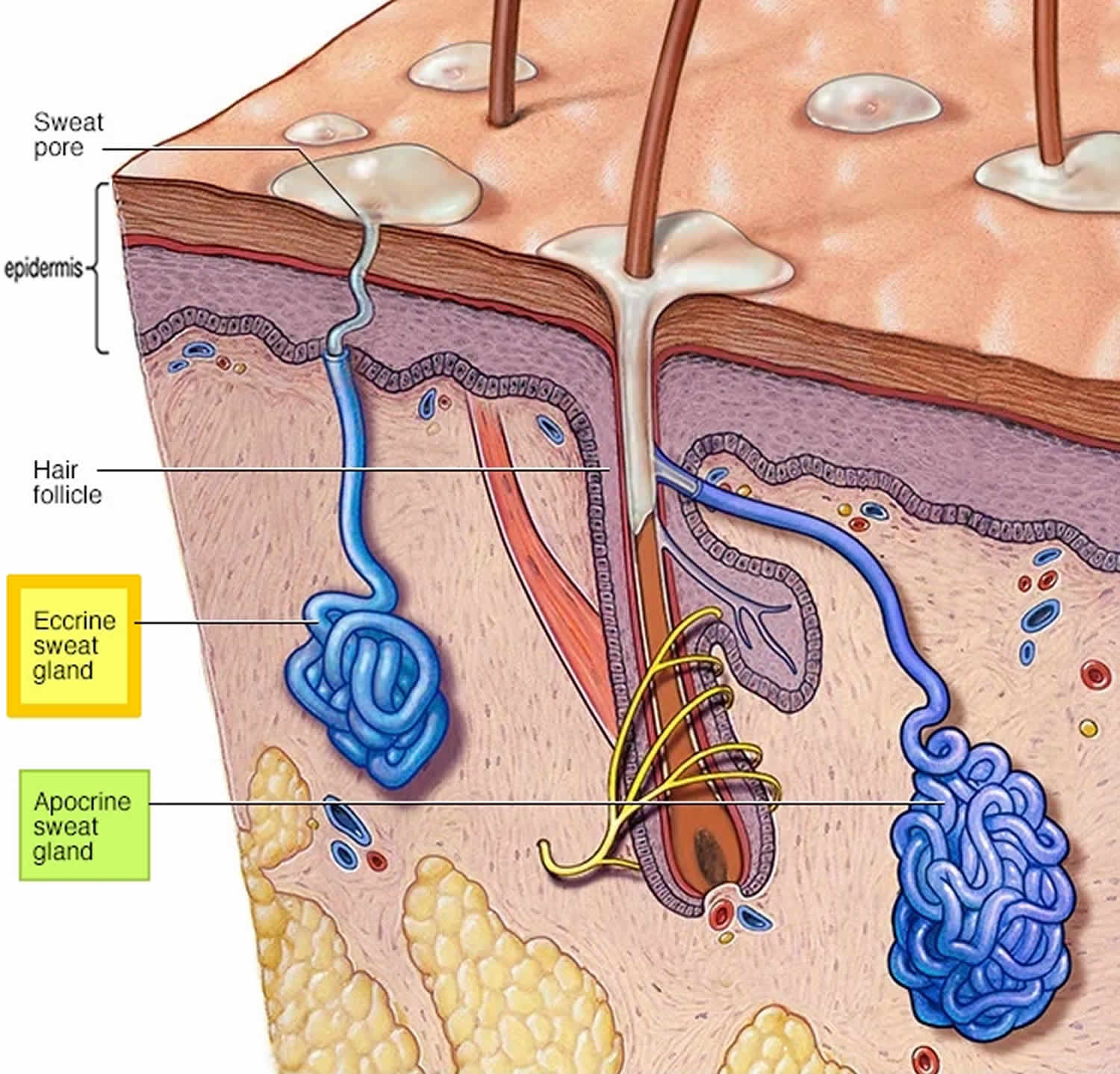
Figure 2. Eccrine spiradenoma

Footnotes: A 49-year-old woman presented with a solitary deep mass of 10-year duration on the right upper arm. The lesion was asymptomatic, firm, and 2.5×2.5 cm in size, with a bluish color in the overlying intact skin (arrow) on her right upper arm.
[Source 37 ]Figure 3. Spiradenoma scalp

Figure 4. Giant vascular eccrine spiradenoma

Footnotes: A 47-year-old woman with a 5-year history of a right shin lump. It has been enlarging gradually and has been asymptomatic at rest. However, it has become exquisitely tender to light touch in the preceding months. She was otherwise well, with a history of bipolar affective disorder. She did not have a history of varicose veins or any skin lesions. On examination, there was a tender 3- × 4-cm ovoid mass on the anteromedial aspect of the right leg with surrounding pink discoloration. It was firm to palpation with a rubbery consistency. It was mobile over the anterior surface of the tibia. She did not have any other skin lesions or varicosities. Cardiovascular examination findings were otherwise unremarkable. Surgical excision was performed through a longitudinal incision directly over the mass. A 3- × 2-cm rubbery gray-blue mass was identified in the subcutaneous tissue with multiple feeding veins. The mass was dissected from the surrounding tissue, and the feeding veins were ligated. Histologic examination of the mass confirmed features consistent with a vascular eccrine spiradenoma, including multinodular structure with focal cystic change, intracystic altered blood, pericystic cholesterol clefts, and hemosiderin. Giant vascular eccrine spiradenoma is a rare variant of eccrine spiradenoma first described by Cotton et al. in 1986 39. They reported two cases of large eccrine spiradenoma with a marked degree of vascularity. The giant vascular variant is different from eccrine spiradenoma by its larger size (diameter of > 2 cm) and high vascularity. Bleeding and internal hemorrhage are common presentations and give rise to the frequent misdiagnosis of giant vascular eccrine spiradenoma as angiomatous lesions 40, 41.
[Source 42 ]Figure 5. Spiradenoma pathology
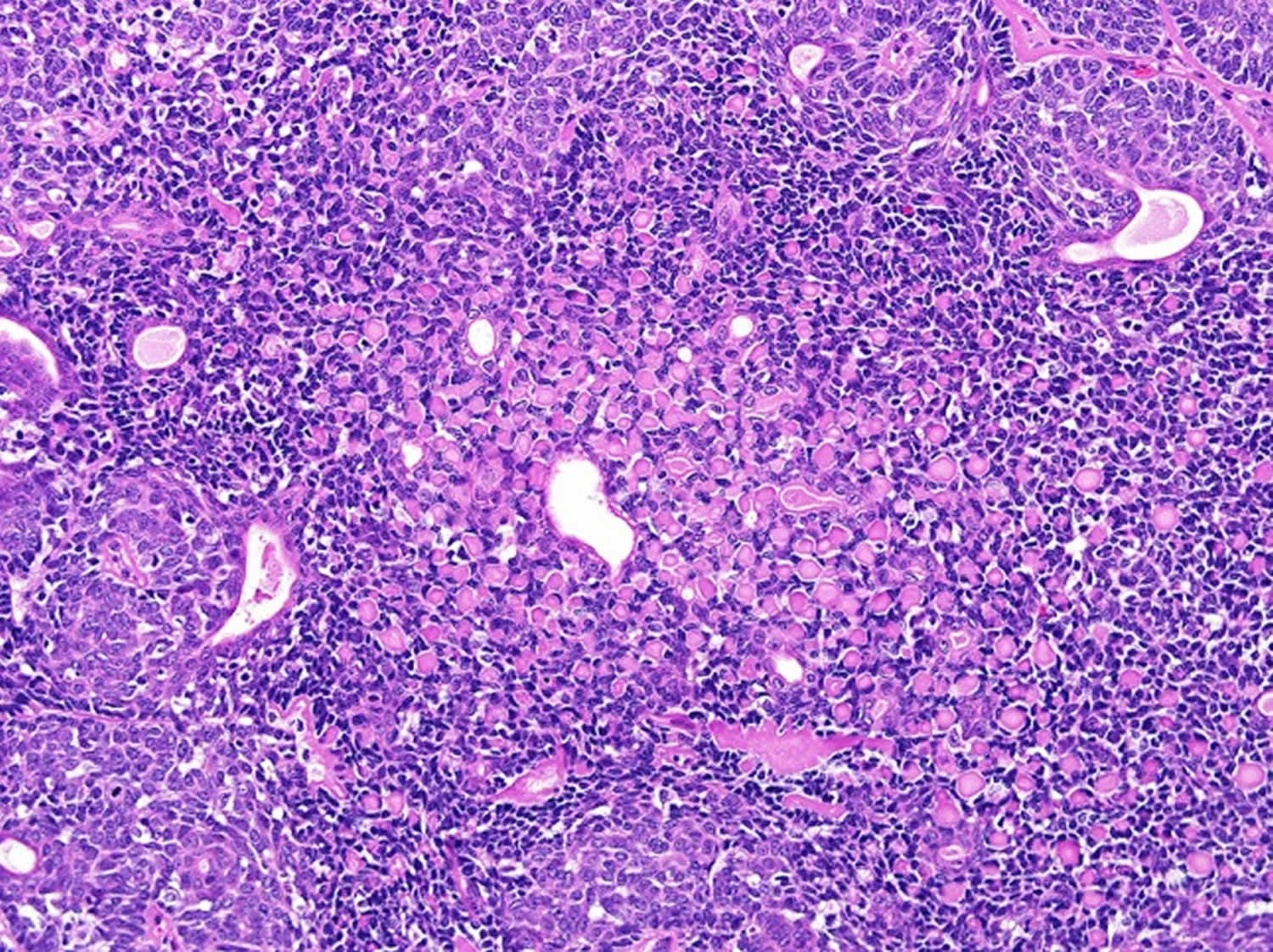
Footnotes: Bland basaloid cells admixed with lymphocytes and droplets of basal membrane material. Focal ductal differentiation can be recognized.
[Source 43 ]Figure 6. Eccrine spiradenoma pathology
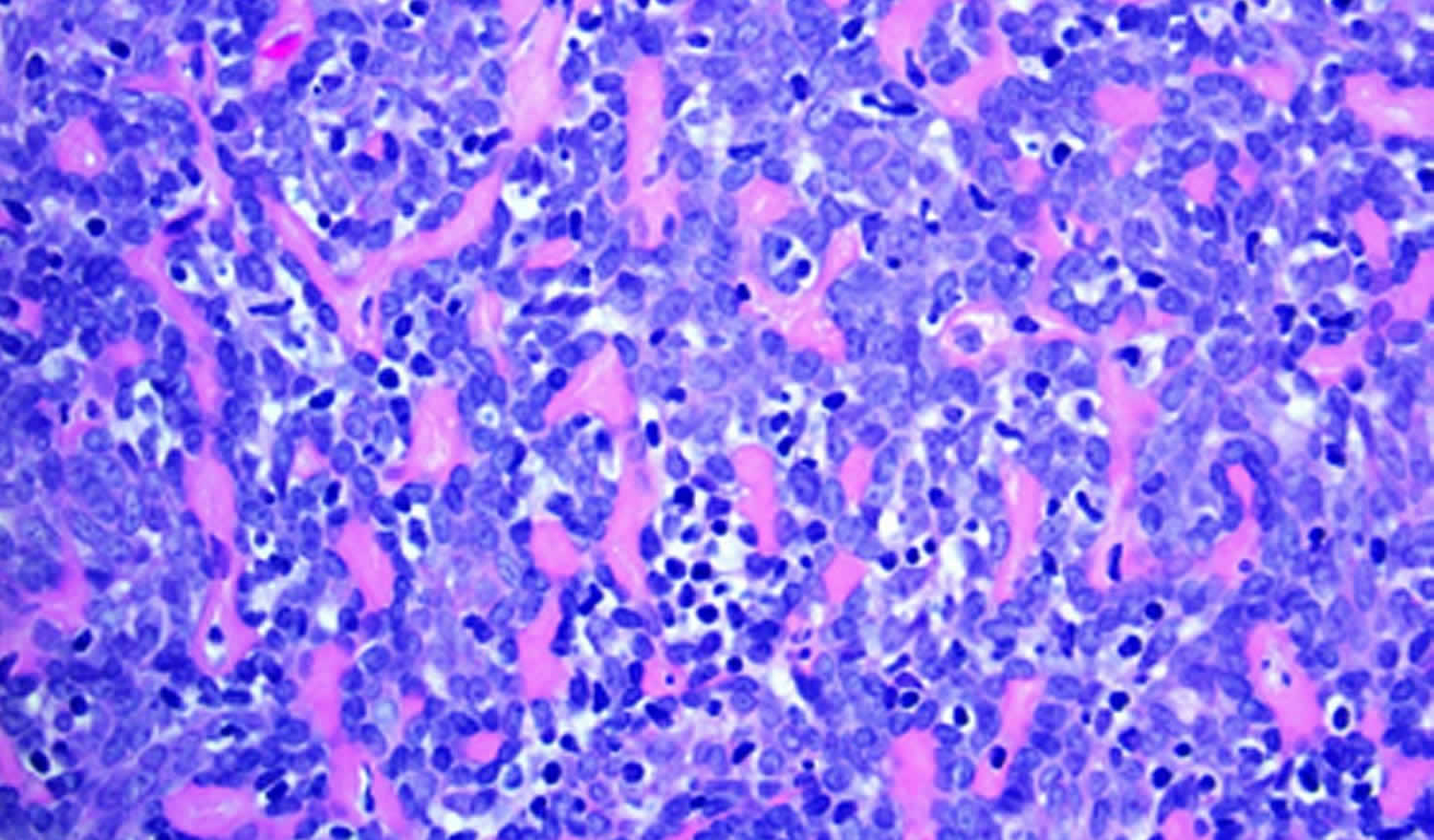
Footnotes: High-powered view demonstrating small, dark, basaloid cells with hyperchromatic nuclei, larger cells with pale nuclei in the center of the clusters, and numerous scattered lymphocytes seen throughout (H&E, magnification 100x)
[Source 14 ]Spiradenoma causes
The exact cause of eccrine spiradenoma is still unknown and remains controversial. Some authors found spiradenoma arising from eccrine sweat glands in the dermis and superficial subcutaneous tissue. However, some authors indicate spiradenoma arising from apocrine gland origin 14, 15. Multiple spiradenomas may be a sign of a familial spiradenoma syndrome or Brooke-Spiegler syndrome. To diagnose Brooke-Spiegler syndrome, in addition to spiradenomas, trichoepitheliomas and cylindromas must be present. Brooke-Spiegler syndrome is an uncommon autosomal dominant disorder characterized by a high affinity to form multiple skin tumors, especially trichoepitheliomas, cylindromas, and spiradenomas 44. The mutations in the CYLD gene on chromosome 16q12 have been described in families with cylindromas, trichoepitheliomas, and spiradenomas 45. Recently, the CYLD gene has been recognized as an important tumor suppressor gene with a prominent role in the regulation of nuclear factor kappa-beta (NF-κβ), a transcription factor that promotes cell survival and oncogenesis 46, 47. Thus, defective tumor suppression genes seem to be important in the development of spiradenomas 14. The CYLD gene provides instructions for making CYLD enzyme called CYLD lysine 63 deubiquitinase that helps regulate numerous signaling pathways, many of which are involved in cell growth 48. These pathways include nuclear factor-kappa-B (NF-KB), Wnt, c-Jun N-terminal kinase (JNK), transforming growth factor beta-1 (TGFB1), and Notch signaling pathways 48. By regulating these signaling pathways, the CYLD lysine 63 deubiquitinase enzyme helps cells respond properly to signals that promote cell growth and division (proliferation) or self-destruction (apoptosis), as necessary. By regulating signals that control cell growth, the CYLD lysine 63 deubiquitinase (CYLD) enzyme acts as a tumor suppressor, which means that it helps prevent cells from growing and dividing too fast or in an uncontrolled way.
Spiradenoma signs and symptoms
Eccrine spiradenoma is a rare, benign sweat glands tumor that originates in the skin. Eccrine spiradenomas arise from the eccrine sweat glands that form small, solitary nodules that can grow to several centimeters in size (0.3 to 5 cm) 2, 3, 4, 5, 6, 7, 8, 9, 10. However, some reviews indicate spiradenoma from apocrine gland origin 14, 15. Usually, there is no connection to the overlying epidermis 13. A large majority of patients present with pain or tenderness associated with the lesion, as was seen in 91% of the patients first described by Kersting and Helwig in 1956 34.
Eccrine glands are simple sweat glands that open directly onto your skin’s surface. Eccrine sweat glands occur over most of your body and are made up of coiled ducts and a secretory coil deep in the dermis. Eccrine sweat glands are found in most of your body and help regulate body temperature. Eccrine glands release sweat to the skin’s surface when the body temperature rises. The sweat evaporates, cooling the skin and blood.
Eccrine spiradenomas form firm nodules that show up on your scalp, neck and upper body, but can also occur in other areas like the breast. Although rare, multiple eccrine spiradenomas on the trunk and extremities have been described 16, 17. Typically, eccrine spiradenomas are often blue or flesh-colored, but may also be grey, pink, purple, red or yellow slow growing and solitary nodule on the head or upper trunk in adult patients and can be very painful 18, 19, 20, 21, 22. Spiradenoma skin tumors range from under 1 cm to several centimeters. Spiradenomas are sometimes painful.
Eccrine spiradenoma can occur at any age, but most often affects young adults in the 2nd to 4th decades of life with no difference between males or females 23, 24, 25, 18.
Spiradenoma diagnosis
Ultrasound evaluation of the tumor generally reveals a smooth, lobulated mass in the superficial subcutaneous tissue 32. The mass appears hypoechoic and often has increased vascularity. The classic MRI appearance is a T1-hypointense, T2-hyperintense mass, with homogeneous enhancement after contrast administration 33.
Clinically, it is difficult to differentiate eccrine spiradenoma from other skin tumors, therefore the definitive diagnosis of eccrine spiradenoma consists of a skin biopsy; however, fine needle cytology has also been reported 49.
Spiradenoma pathology
Eccrine spiradenoma comprises large, sharply circumscribed, basophilic nodules (“cannon balls” or “blue balls”) arranged in intertwining cords, islands, or sheets in the dermis or subcutaneous tissue that are surrounded by a fibrous capsule 50. It is important to find out epithelial cells, myoepithelial cells and lymphocytes along with void spaces between blood vessels under the microscopes for diagnostic confirmations 6. Characteristic histological findings on H&E staining are two distinct cell types: a basaloid cell population with hyperchromatic nuclei and scant cytoplasm and a larger cell type with abundant, pale cytoplasm 34, 13. The cells are arranged into sheets, cords, or trabeculae, with cells with large nucleus and pale cytoplasm are located in the center and cells with smaller dense nucleus are located in the periphery 6. The lumen of this contains an acidic substance which is being arranged around a smaller lumen. Some tumors are markedly vascular with cystic dilation of their vascular channels, likely accounting for their increased vascularity seen on ultrasound 32, 13.
Duct-like structures can be present at the center of the lesions, which often have scattered lymphocytes 18. Strands of cells are positive for cytokeratin and the lumina are positive for carcinoembryonic antigen 51. Eccrine spiradenoma may accompany similar tumors of apocrine origin, such as trichoblastoma and cylindroma. Histologically, the eccrine glands have relatively clear cytoplasm and occasionally squamous epithelium whereas the apocrine glands have eosinophilic cytoplasm and nuclei located at the base bottom (off centered) 35. S-100 staining has been noted in eccrine spiradenoma and cylindromas attributed to eccrine differentiation. In cases where eccrine spiradenoma has co-expression of cytokeratin and smooth muscle actin, authors have suggested differentiation toward myoepithelial cells 52.
Malignant eccrine spiradenoma is suspected in patients with rapid enlargement, an increase in number, change in color, or with the development of symptoms, such as pain, ulceration, or pruritus. Histological findings may include atypical cells, elevated mitotic counts, loss of the typical lobular pattern and dual cell population, rare foci of necrosis, and enlarged cells of one cell type on histological evaluation 24, 53. Additionally, tumor cells extending through the capsule into adjacent stroma are also suggestive 54.
Immunohistochemistry can be useful in evaluating for malignant cases of eccrine spiradenoma. In a case of malignant eccrine spiradenoma of the breast, typical histological features were noted along with areas of adenocarcinoma, squamous cell carcinoma, and sarcoma with staining positive for the p53 protein 55. Others have demonstrated that cells may express cytokeratins, epithelial membrane antigen, and p53 56.
Eccrine spiradenoma differential diagnosis
Eccrine spiradenoma should be considered in the differential diagnosis of skin tumors.
- Cylindroma — In cylindroma the low power view shows discrete polygonal tumor islands. There is frequently a more prominent population of S100 positive dendritic cells while in eccrine spiradenoma there is a lymphocytic infiltrate 7, 57, 58. Dermal cyclindroma can be differentiated histologically from eccrine spiradenoma. Comprised of cords of cells, surrounded by a prominent basement membrane, that exhibit a mosaic pattern, cyclindromas lack pseudoglandular structures and a true capsule, have more hyaline material and are more superficial with a tendency to approach the epidermis which bay be flattened or atrophic 59.
- Spiradenocylindroma — some tumors features of both cylindroma and eccrine spiradenoma can be seen and are designated as overlap tumors 58.
- Cutaneous lymphadenoma — in this tumor there is a lobular tumor of basaloid cells which may show peripheral palisading, and a dense mixed inflammatory cell infiltrate though predominantly lymphocytic 58.
Spiradenoma treatment
Because of eccrine spiradenoma potential for local recurrence or malignant transformation, complete surgical excision is the preferred treatment method but with no clear consensus regarding the width of surgical margins and this tumor does not seem to recur if complete resection had been pursued 36. Although most cases of spiradenoma are benign, they can recur locally with incomplete excision. Imaging techniques like CT scans, MRIs, and ultrasounds can also be used to help with treatment. Routine follow-up to screen for local recurrence or malignant degeneration is also important 60.
Other treatment options may include radiotherapy, carbon dioxide laser ablation, or chemotherapy, are reserved for cases in multiplicity or that are malignant 14. Due to the potential for malignant transformation, wide surgical excision or Mohs micrographic surgery offers the most conservative treatment choice, and lesions treated tend not to recur 14. One author suggests a combination of surgical management (staged surgical resections with reconstruction using complex linear closures and random-pattern cutaneous flaps) and medical management (carbon dioxide laser) for good cosmetic results 61.
For the treatment of eccrine spiradenocarcinoma (malignant eccrine spiradenoma), no treatment has been routinely established as paramount 14. Resection with wide margins (1–3cm) down to the fascia with lymph node dissection has been described as the most accepted treatment 56, 62, 63. Radiation and chemotherapy have also been proposed, but no conclusive studies have substantiated optimal practice 11, 64, 62. Hyperthermic limb perfusion chemotherapy has been tried as some believe that alterations of temperature may target treatment to tumor cells over healthy ones 65. A meta-analysis of eccrine spiradenocarcinoma demonstrated that patients with no metastasis who underwent surgical excision had a disease-free survival rate of 100 percent at 33 months 62. In contrast, patients with distant metastases treated with either surgery alone or surgery and adjuvant chemotherapy had a median survival of 12 and 20 months, respectively. Despite the difference in median survival rates between the two groups, the results were not statistically significant. Resection of lymph node metastasis resulted in patients who were disease free at the final follow-up evaluation (mean 47 months) suggesting that, in the case of positive lymph nodes, surgical resection is certainly warranted. The authors concluded that aggressive surgical removal is necessary in cases of malignant eccrine spiradenoma with or without metastasis 62.
In cases of malignant eccrine spiradenoma, close clinical follow up every three months the first year after resection, every six months the second year after resection, and annually thereafter is important given the possibility of recurrences 14. Due to the high rate of metastasis to the liver and lung, annual chest radiographs, liver function tests, liver ultrasound, chest and abdomen CT, and/or MRI may be useful 53. But again, no consensus has validated these practices. Genetic counseling for cases of familial eccrine spiradenoma is also advised 61.
Spiradenoma prognosis
Eccrine spiradenoma is a rare, benign sweat glands tumor that originates in the skin. Very rarely malignant changes into eccrine spiradenocarcinoma may occur if the eccrine spiradenoma lasts long enough, typical history was one of rapid enlargement of a cutaneous nodule of long standing 66, 29, 56. Malignant transformation occurs more often in cases of multiple benign eccrine spiradenoma than in solitary cases 11. There are just over 100 cases reported of malignant transformation 67. Malignant transformation of eccrine spiradenoma generally occurs 20 to 30 years after initial lesion detection 11. Malignant spiradenomas nearly always arise from a long-standing benign lesion, although they can rarely arise as de novo malignancies 67. Malignant spiradenomas tend to be diagnosed in older patients. They can present with rapid growth, erythema, ulceration, and bleeding and may resemble melanoma 67.
Many mechanisms have been proposed, such as trauma, but none are substantiated in the literature 68, 64, 53. In these rare cases of malignant potential, p53 may be increased even in the presence of a benign-appearing histology 69, 70. Malignant eccrine spiradenoma are aggressive tumors that spread both hematogenously and lymphogenously and have been reported to have a mortality of 39 percent if left untreated 64, 53. Since the rate of metastasis is close to 50 percent and can result in death, these patients must be followed closely. Currently, no guidelines have been developed for surveillance in patients with multiple eccrine spiradenoma, although it seems reasonable that patients with larger-sized, multiple, and/or symptomatic lesions be monitored regularly.
Malignant transformation of eccrine spiradenoma shares many clinical and pathologic features with malignant transformation of dermal cylindroma. Pathology shows anaplastic basaloid cells with areas of highly pleomorphic cells and numerous mitotic figures 60.
In 2000, Granter et al 71, 72 divided malignant eccrine spiradenoma into 2 groups (high and low grade) based on clinical and histological features. High-grade malignant eccrine spiradenoma has more obvious features of malignancy with pleomorphism and increased mitoses (4–32/hpf) 71, 53. Low-grade malignant eccrine spiradenoma has less obvious features of malignancy, such as loss of the typical ductal cells, mild-to-moderate pleomorphism, and lower mitotic rates (2–10/hpf) 71, 53. Malignant eccrine spiradenoma tends to have a high rate of metastasis to regional lymph nodes, lungs, brain, and liver; therefore, radiological studies, such as x-ray, computed tomography (CT), or magnetic resonance imaging (MRI), are useful in assessing for metastatic foci.
- Gupta S, Radotra BD, Kaur I, Handa S, Kumar B. Multiple linear eccrine spiradenomas with eyelid involvement. J Eur Acad Dermatol Venereol. 2001;15:163–6. doi: 10.1046/j.1468-3083.2001.00234.x[↩]
- Opango ADC, Nshimirimana B, Jaifi A, Belmaachi S, Fawzi S, Mansouri-Hattab N. Eccrine spiradenoma of nose: Surgical case report. Int J Surg Case Rep. 2023 Dec;113:109033. doi: 10.1016/j.ijscr.2023.109033[↩][↩]
- Satturwar S, Wakely PE Jr, Lott Limbach A. Fine needle aspiration cytopathology of eccrine spiradenoma. J Am Soc Cytopathol. 2022 Sep-Oct;11(5):274-280. doi: 10.1016/j.jasc.2022.05.002[↩][↩]
- Li Z, Li G, Jiang X, Fu X. Giant vascular eccrine spiradenoma: the first case in the scrotum and review of the literature author. Diagn Pathol. 2021 Apr 30;16(1):37. doi: 10.1186/s13000-021-01073-8[↩][↩]
- Khurana A, Ambastha R, Kaur M. Giant vascular eccrine spiradenoma; A rare entity with review of literature. Indian J Pathol Microbiol. 2022 Jan-Mar;65(1):233-235. doi: 10.4103/IJPM.IJPM_798_20[↩][↩]
- Kim J, Yang HJ, Pyo JS. Eccrine Spiradenoma of the Scalp. Arch Craniofac Surg. 2017 Sep;18(3):211-213. doi: 10.7181/acfs.2017.18.3.211[↩][↩][↩][↩][↩][↩]
- Kersting DW, Helwig EB. Eccrine spiradenoma. AMA Arch Derm. 1956;73:199–227. doi: 10.1001/archderm.1956.01550030001001[↩][↩][↩]
- Wright S, Ryan J. Multiple familial eccrine spiradenoma with cylindroma. Acta Derm Venereol. 1990;70(1):79-82.[↩][↩]
- Dhua S., Sekhar D.R. A rare case of eccrine spiradenoma – treatment and management. Eur. J. Plast. Surg. 2016;39:143–146. doi: 10.1007/s00238-015-1103-4[↩][↩]
- Gordon S, Styron BT, Haggstrom A. Pediatric segmental eccrine spiradenomas: a case report and review of the literature. Pediatr Dermatol. 2013 Nov-Dec;30(6):e285-6. doi: 10.1111/j.1525-1470.2012.01777.x[↩][↩]
- Braun-Falco M, Bonel H, Ring J, Hein R. Linear spiradenoma with focal malignant transformation. J Eur Acad Dermatol Venereol. 2003;17(3):308–312. doi: 10.1046/j.1468-3083.2003.00779.x[↩][↩][↩][↩]
- Cooper PH, Frierson HF, Jr, Morrison AG. Malignant transformation of eccrine spiradenoma. Arch Dermatol. 1985;121(11):1445–1448.[↩]
- Mambo NC. Eccrine spiradenoma: clinical and pathologic study of 49 tumors. J Cutan Pathol. 1983;10(5):312–320. doi: 10.1111/j.1600-0560.1983.tb00333.x[↩][↩][↩][↩][↩][↩]
- Englander L, Emer JJ, McClain D, Amin B, Turner RB. A rare case of multiple segmental eccrine spiradenomas. J Clin Aesthet Dermatol. 2011 Apr;4(4):38-44. https://pmc.ncbi.nlm.nih.gov/articles/PMC3084607[↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Jin W, Kim GY, Lew BL, Yang DM, Kim HC, Ryu JK, Park JS, Ryu KN. Sonographic findings of an eccrine spiradenoma: case report and literature review. J Ultrasound Med. 2008 May;27(5):813-8. doi: 10.7863/jum.2008.27.5.813[↩][↩][↩]
- Revis P., Chyu J., Medenica M. Multiple eccrine spiradenoma: case report and review. J. Cutan. Pathol. 1988;15:226–229. doi: 10.1111/j.1600-0560.1988.tb00549.x[↩][↩]
- Gupta S, Jain VK, Singh U, Gupta S. Multiple eccrine spiradenomas in zosteriform distribution in a child. Pediatr Dermatol. 2000;17:384–6. doi: 10.1046/j.1525-1470.2000.017005384.x[↩][↩]
- Ekmekci TR, Koslu A, Sakiz D. Congenital blaschkoid eccrine spiradenoma on the face. Eur J Dermatol. 2005 Mar-Apr;15(2):73-4.[↩][↩][↩][↩][↩]
- Rodríguez-Martín M, Sánchez González R, Sáez-Rodríguez M, García-Bustínduy M, Martín-Herrera A, Noda-Cabrera A. An unusual case of congenital linear eccrine spiradenoma. Pediatr Dermatol. 2009 Mar-Apr;26(2):180-3. doi: 10.1111/j.1525-1470.2009.00879.x[↩][↩]
- Cooper PH, Frierson HF Jr, Morrison AG. Malignant transformation of eccrine spiradenoma. Arch Dermatol. 1985 Nov;121(11):1445-8. [↩][↩]
- Yoshida A, Takahashi K, Maeda F, Akasaka T. Multiple vascular eccrine spiradenomas: a case report and published work review of multiple eccrine spiradenomas. J Dermatol. 2010 Nov;37(11):990-4. doi: 10.1111/j.1346-8138.2010.00925.x[↩][↩]
- Gupta S, Jain VK, Singh U, Gupta S. Multiple eccrine spiradenomas in zosteriform distribution in a child. Pediatr Dermatol. 2000 Sep-Oct;17(5):384-6. doi: 10.1046/j.1525-1470.2000.017005384.x[↩][↩]
- Bowman Kelsey M., Bennett Daniel D., Hanna Amgad S. Benign eccrine spiradenoma imitating a nerve sheath tumor: illustrative case. J. Neurosurg. Case Lessons. 2022;25:CASE21505. doi: 10.3171/CASE21505[↩][↩]
- Nath AK, Kumari R, Thappa DM. Eccrine spiradenoma with chondroid syringoma in Blaschkoid distribution. Indian J Dermatol Venereol Leprol. 2009;75(6):600–602. doi: 10.4103/0378-6323.57723[↩][↩][↩]
- Bedlow AJ, Cook MG, Kurwa A. Extensive naevoid eccrine spiradenoma. Br J Dermatol. 1999;140(1):154–157. doi: 10.1046/j.1365-2133.1999.02627.x[↩][↩]
- Engel CJ, Meads GE, Joseph NG, Stavraky W. Eccrine spiradenoma: a report of malignant transformation. Can J Surg. 1991 Oct;34(5):477-80.[↩]
- Chou SC, Lin SL, Tseng HH. Malignant eccrine spiradenoma: a case report with pulmonary metastasis. Pathol Int. 2004 Mar;54(3):208-12. doi: 10.1111/j.1440-1827.2004.01609.x[↩]
- Ishikawa M, Nakanishi Y, Yamazaki N, Yamamoto A. Malignant eccrine spiradenoma: a case report and review of the literature. Dermatol Surg. 2001 Jan;27(1):67-70. https://journals.lww.com/dermatologicsurgery/abstract/2001/01000/malignant_eccrine_spiradenoma__a_case_report_and.20.aspx[↩]
- Cooper PH, Frierson HF, Morrison AG. Malignant Transformation of Eccrine Spiradenoma. Arch Dermatol. 1985;121(11):1445–1448. doi:10.1001/archderm.1985.01660110093023[↩][↩]
- Chen G, Cheuk W, Cheung JS, Chan JK. Carcinosarcoma ex eccrine spiradenoma of the vulva: report of the first case. Int J Gynecol Pathol. 2011 May;30(3):301-5. doi: 10.1097/PGP.0b013e3182055a3d[↩]
- Saboorian MH, Kenny M, Ashfaq R, Albores-Saavedra J. Carcinosarcoma arising in eccrine spiradenoma of the breast. Report of a case and review of the literature. Arch Pathol Lab Med. 1996 May;120(5):501-4.[↩]
- Kwon KE, Kim SJ, Choi HJ, et al. Sonographic appearance of an eccrine spiradenoma: A case report. J Clin Ultrasound. 2018;46(7):494–496. doi: 10.1002/jcu.22572[↩][↩][↩][↩]
- Han YD, Huan Y, Deng JL, Zhang YG, Zhang CH. MRI appearance of multiple eccrine spiradenoma. Br J Radiol. 2007;80(949):e27–e29. doi: 10.1259/bjr/55828940[↩][↩]
- Kersting DW, Helwig EB. Eccrine spiradenoma. AMA Arch Derm. 1956;73(3):199–227. doi: 10.1001/archderm.1956.01550030001001[↩][↩][↩]
- Kim MH, Cho E, Lee JD, Cho SH. Giant vascular eccrine spiradenoma. Ann Dermatol. 2011;23:S197–S200. doi: 10.5021/ad.2011.23.S2.S197[↩][↩]
- Rahim RR, Rajan N, Langtry JA. Infiltrative recurrent eccrine spiradenoma of the anterior neck treated using Mohs micrographic surgery. Dermatol Surg. 2013 Nov;39(11):1711-4. doi: 10.1111/dsu.12328[↩][↩]
- Kim MH, Cho E, Lee JD, Cho SH. Giant vascular eccrine spiradenoma. Ann Dermatol. 2011 Oct;23(Suppl 2):S197-200. doi: 10.5021/ad.2011.23.S2.S197[↩]
- Sweat gland derived (apocrine & eccrine glands). Spiradenoma. https://www.pathologyoutlines.com/topic/skintumornonmelanocyticeccrinespiradenoma.html[↩]
- Cotton DW, Slater DN, Rooney N, Goepel JR, Mills PM. Giant vascular eccrine spiradenomas: a report of two cases with histology, immunohistology and electron microscopy. Histopathology. 1986;10:1093–9. doi: 10.1111/j.1365-2559.1986.tb02546.x[↩]
- Kim M.H., Cho E., Lee J.D., Cho S.H. Giant vascular eccrine spiradenoma. Ann Dermatol. 2011;23(Suppl 2):S197–S200. doi: 10.5021/ad.2011.23.S2.S197[↩]
- Ko J.Y., Lee C.W., Moon S.H., Song K.W., Park C.K. Giant vascular eccrine spiradenoma: report of a case with immunohistochemical study. J Korean Med Sci. 2006;21:172–176. doi: 10.3346/jkms.2006.21.1.172[↩]
- Ho KKF, Kwon L, Wong D, Hagley D. Giant vascular eccrine spiradenoma presenting as a thrombosed varix. J Vasc Surg Cases Innov Tech. 2019 Nov 26;5(4):583-585. doi: 10.1016/j.jvscit.2019.10.007[↩]
- Kazakov DV. Brooke-Spiegler Syndrome and Phenotypic Variants: An Update. Head Neck Pathol. 2016 Jun;10(2):125-30. doi: 10.1007/s12105-016-0705-x[↩]
- Uede K, Yamamoto Y, Furukawa F. Brooke-Spiegler syndrome associated with cylindroma, trichoepithelioma, spiradenoma, and syringoma. J Dermatol. 2004;31(1):32–38. doi: 10.1111/j.1346-8138.2004.tb00501.x[↩]
- Blake PW, Toro JR. Update of cylindromatosis gene (CYLD) mutations in Brooke-Spiegler syndrome: novel insights into the role of deubiquitination in cell signaling. Hum Mutat. 2009;30(7):1025–1036. doi: 10.1002/humu.21024[↩]
- Sun SC. CYLD: a tumor suppressor deubiquitinase regulating NF-kappaB activation and diverse biological processes. Cell Death Differ. 2010;17(1):1725–1734. doi: 10.1038/cdd.2009.43[↩]
- Kazakov DV, Schaller J, Vanecek T, et al. Brooke-Spiegler syndrome: report of a case with a novel mutation in the CYLD gene and different types of somatic mutations in benign and malignant tumors. J Cutan Pathol. 2010;37(8):886–890. doi: 10.1111/j.1600-0560.2010.01511.x[↩]
- CYLD gene. https://medlineplus.gov/genetics/gene/cyld[↩][↩]
- Bosch MM, Boon ME. Fine-needle cytology of an eccrine spiradenoma of the breast: diagnosis made by a holistic approach. Diagn Cytopathol. 1992;8(4):366–368. doi: 10.1002/dc.2840080412[↩]
- Park JW, Namkoong S, Chung J, et al. A case of eccrine spiradenoma in a patient with neurofibromatosis. Ann Dermatol. 2010;22(2):191–193. doi: 10.5021/ad.2010.22.2.191[↩]
- Meybehm M, Fischer HP. Spiradenoma and dermal cylindroma: comparative immunohistochemical analysis and histogenetic considerations. Am J Dermatopathol. 1997;19(2):154–161. doi: 10.1097/00000372-199704000-00009[↩]
- Kurokawa I, Nishimura K, Tarumi C, et al. Eccrine spiradenoma: co-expression of cytokeratin and smooth muscle actin suggesting differentiation toward myoepithelial cells. J Eur Acad Dermatol Venereol. 2007;21(1):121–123. doi: 10.1111/j.1468-3083.2006.01809.x[↩]
- Hantash BM, Chan JL, Egbert BM, Gladstone HB. De-novo malignant eccrine spiradenoma: a case report and review of the literature. Dermatol Surg. 2006;32(9):1189–1198. doi: 10.1111/j.1524-4725.2006.32265.x[↩][↩][↩][↩][↩][↩]
- Tanese K, Sato T, Ishiko A. Malignant eccrine spiradenoma: case report and review of the literature, including 15 Japanese cases. Clin Exp Dermatol. 2009;35(1):51–55. doi: 10.1111/j.1365-2230.2008.03072.x[↩]
- Saboorian MH, Kenny M, Ashfaq R, Albores-Saavedra J. Carcinosarcoma arising in eccrine spiradenoma of the breast. Report of a case and review of the literature. Arch Pathol Lab Med. 1996;120(5):501–504.[↩]
- Yildirim S, Akoz T, Akan M, Ege GA. De-novo malignant eccrine spiradenoma with an interesting and unusual location. Dermatol Surg. 2001;27(4):417–420. doi: 10.1046/j.1524-4725.2001.00027.x[↩][↩][↩]
- Mambo NC. Eccrine spiradenoma: clinical and pathologic study of 49 tumors. J Cutan Pathol. 1983;10:312–320. doi: 10.1111/j.1600-0560.1983.tb00333.x[↩]
- Eccrine spiradenoma pathology. https://dermnetnz.org/topics/eccrine-spiradenoma-pathology[↩][↩][↩]
- Crain RC, Helwig EB. Dermal cylindroma (dermal eccrine cylindroma) Am J Clin Pathol. 1961;35:504–515. doi: 10.1093/ajcp/35.6.504[↩]
- Bowman KM, Bennett DD, Hanna AS. Benign eccrine spiradenoma imitating a nerve sheath tumor: illustrative case. J Neurosurg Case Lessons. 2022 Jun 20;3(25):CASE21505. doi: 10.3171/CASE21505[↩][↩]
- Ter Pooten MC, Barrett K, Cook J. Familial eccrine spiradenoma: a case report and review of the literature. Dermatol Surg. 2003;29(4):411–414. doi: 10.1046/j.1524-4725.2003.29096.x[↩][↩]
- Andreoli MT, Itani KM. Malignant eccrine spiradenoma: a meta-analysis of reported cases. Am J Surg. 2010 Sep 17; doi: 10.1016/j.amjsurg.2010.04.015[↩][↩][↩][↩]
- Ben Brahim E, Sfia M, Tangour M, et al. Malignant eccrine spiradenoma: a new case report. J Cutan Pathol. 2010;37(4):478–481. doi: 10.1111/j.1600-0560.2009.01320.x[↩]
- Shaikh-Naidu N, Breitbart A. Eccrine spiradenoma of the upper extremity: case report and an algorithm for management. Eur J Plast Surg. 2003;26(3):160–163.[↩][↩][↩]
- Tay JS, Tapen EM, Solari PG. Malignant eccrine spiradenoma. Case report and review of the literature. Am J Clin Oncol. 1997;20(6):552–557. doi: 10.1097/00000421-199712000-00003[↩]
- Dabska M. Malignant transformation of eccrine spiradenoma. Pol Med J. 1972;11(2):388-96.[↩]
- Andreoli MT, Itani KMF. Malignant eccrine spiradenoma: a meta- analysis of reported cases. Am J Surg. 2011;201(5):695–699. doi: 10.1016/j.amjsurg.2010.04.015[↩][↩][↩]
- Biernat W, Wozniak L. Spiradenocarcinoma: a clinicopathologic and immunohistochemical study of three cases. Am J Dermatopathol. 1994 Aug;16(4):377-82.[↩]
- Dijkhuizen T, van den Berg E, Nikkels PG, et al. Cytogenetics of a case of eccrine spiradenoma. Hum Pathol. 1992;23(9):1085–1087. doi: 10.1016/0046-8177(92)90274-7[↩]
- Kazakov DV, Grossmann P, Spagnolo DV, et al. Expression of p53 and TP53 mutational analysis in malignant neoplasms arising in pre-existing spiradenoma, cylindroma, and spiradenocylindroma, sporadic or associated with Brooke-Spiegler syndrome. Am J Dermatopathol. 2010;32(3):215–321. doi: 10.1097/DAD.0b013e3181b9678c[↩]
- Granter SR, Seeger K, Calonje E, et al. Malignant eccrine spiradenoma (spiradenocarcinoma): a clinicopathologic study of 12 cases. Am J Dermatopathol. 2000;22(2):97–103. doi: 10.1097/00000372-200004000-00002[↩][↩][↩]
- Leonard N, Smith D, McNamara P. Low-grade malignant eccrine spiradenoma with systemic metastases. Am J Dermatopathol. 2003;25(3):253–255. doi: 10.1097/00000372-200306000-00011[↩]





{kind=link}