
Contents
What is sebaceous hyperplasia
Sebaceous hyperplasia is the term used for enlarged sebaceous glands (skin oil glands) seen on the forehead or cheeks of the middle-aged and elderly usually in fifth or sixth decade of life and continue to appear into later life and is seen in about 1% of the US population 1, 2, 3, 4, 5, 6, 7, 8. Sebaceous hyperplasia is also common in newborns, but in this case, it is transient as a result of the neonate exposure to maternal hormones 9, 10, 7, 11. Of 1000 consecutive newborns examined in an Iranian prospective cohort study, 43.7% had sebaceous hyperplasia 8, 12. Rarer variants of sebaceous hyperplasia affect your chest 13, mouth 14, scrotum 15, foreskin 16, penile shaft 17, vulva 18 and areola 19. Sebaceous glands are microscopic glands found in your hair follicles that secrete sebum. Sebum is an oily substance that protects your skin from drying out. Sebaceous hyperplasia is a form of benign hair follicle tumor, but they may be associated with non-melanoma skin cancer in transplantation patients 20. Sebaceous hyperplasia may be more prevalent in immunosuppressed patients: for example, in a patient following organ transplantation. About 10–16% of people on long-term cyclosporin A for organ transplants also develop sebaceous hyperplasia. There are a few families where multiple lesions begin to occur during puberty. It is also frequently prominent in the rare Torre-Muir syndrome. Sebaceous hyperplasia lesions are sometimes confused with basal cell carcinoma. Sebaceous hyperplasia appears as small yellow bumps up to 3 mm in diameter. Close inspection reveals a central hair follicle surrounded by yellowish lobules. There are often prominent blood vessels, best seen using dermoscopy.
Sebaceous hyperplasia can be single or multiple and manifest as yellowish, soft, small bumps (papules) on your face (particularly nose, cheeks, and forehead). Sebaceous hyperplasia occasionally also occurs on your chest, areola (nipple), mouth, scrotum, foreskin, shaft of penis, and vulva 21. Rarely reported variants have included a giant form 22, a linear 23 or zosteriform arrangement, a diffuse form, a nevoid form 24 and a familial form.
Sebaceous hyperplasia bumps are harmless (benign) and does not require any treatment but can create a cosmetic concern. For cosmetic reasons or if they are bothersome if irritated, individual lesions may be removed by light electrocautery or laser vaporisation.
When the lesions are severe, extensive or disfiguring, oral isotretinoin is effective in clearing lesions but these may recur when treatment is stopped. In females, antiandrogens may help improve the appearance.
Figure 1. Sebaceous glands
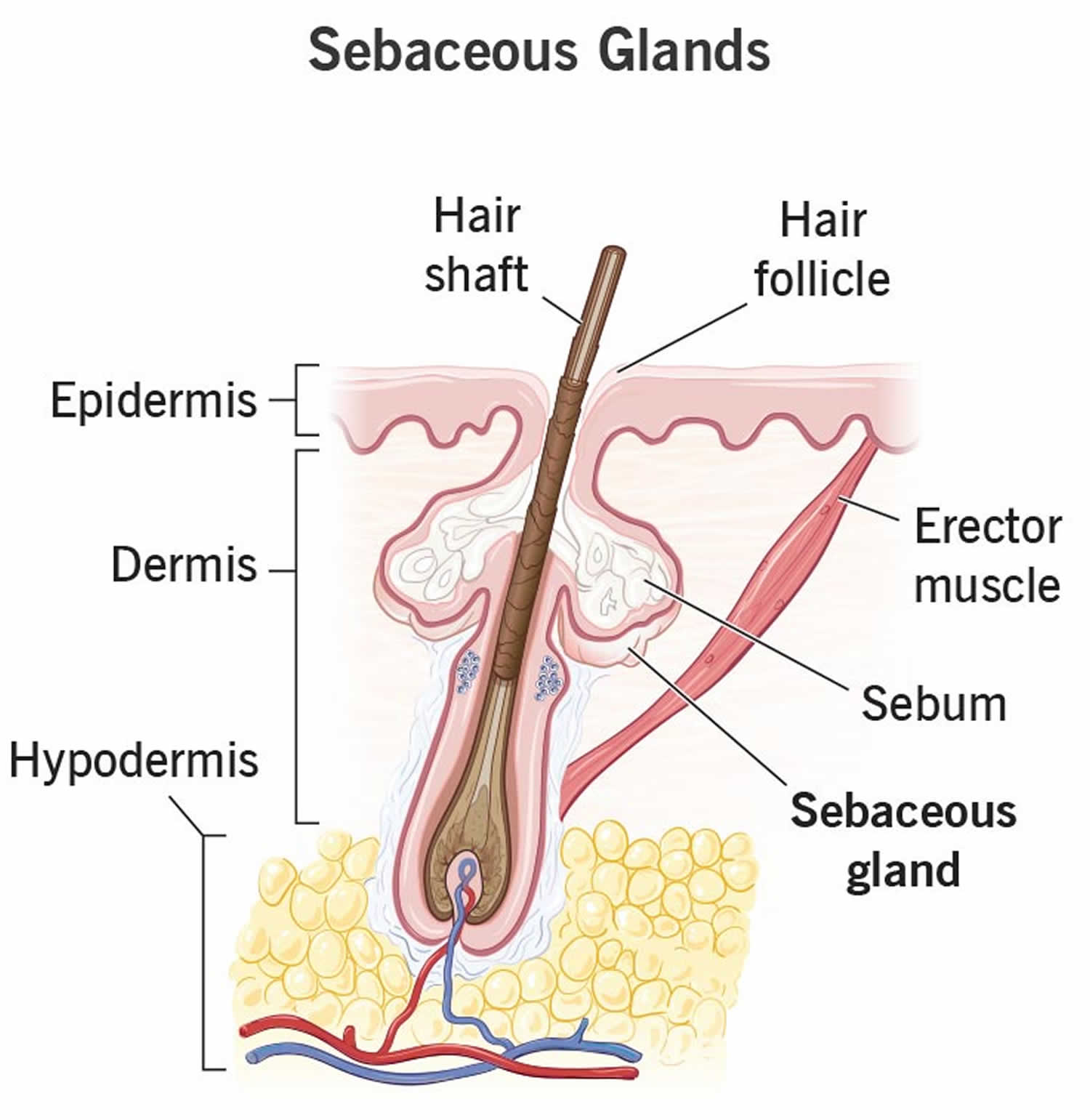
Figure 2. Sebaceous hyperplasia

Footnotes: Sebaceous hyperplasia with solitary small skin-colored, umbilicated papule arising in the region of zygomatic bone
[Source 5 ]Figure 3. Sebaceous hyperplasia dermoscopic image

Footnotes: The dermoscopic features of sebaceous hyperplasia are the white–yellowish globules—in the form of cumulous clouds surrounded by small crown vessels. The follicular ostia is commonly visible as a central umbellic.
[Source 5 ]Figure 4. Sebaceous hyperplasia before and after treatment
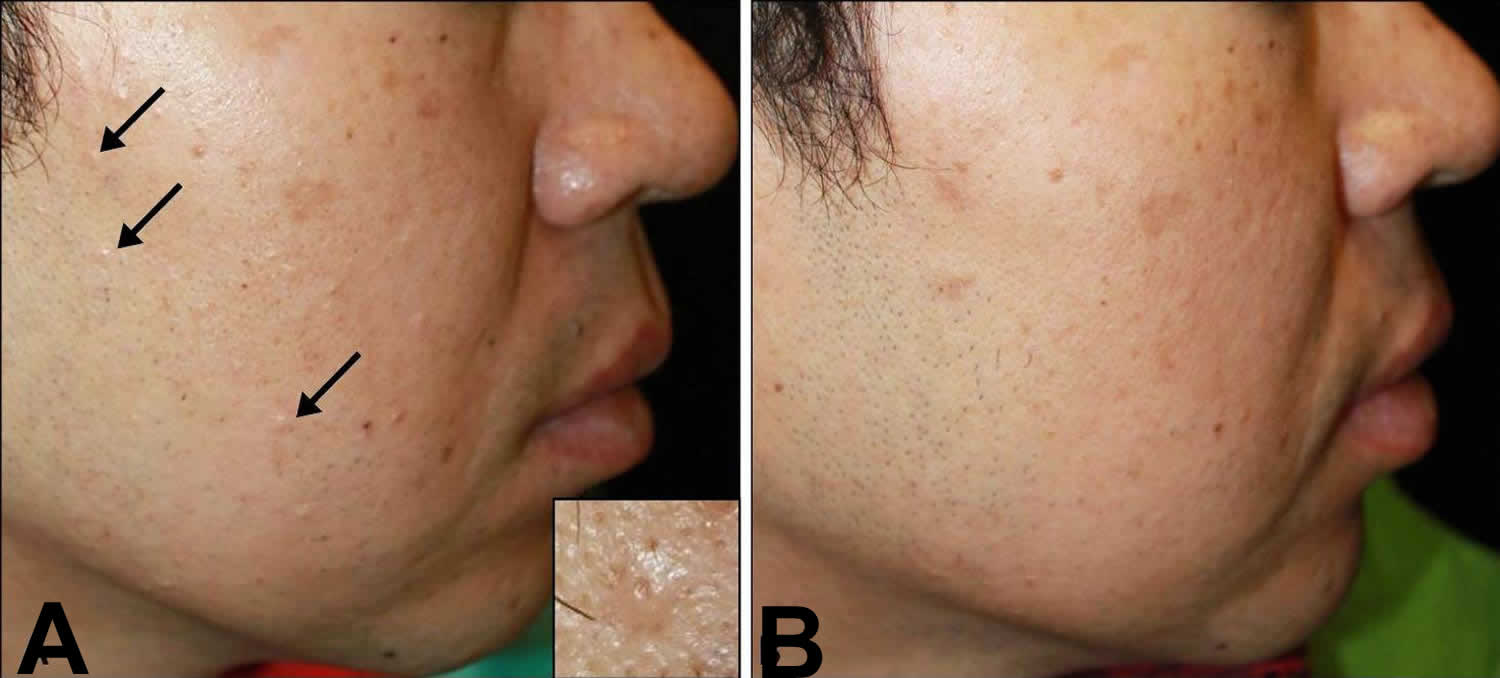
Footnotes: A 40-year old Korean man presented with multiple skin-colored papules on his face. He had undergone kidney transplantation surgery, following which, he was immunosuppressed with oral cyclosporine and prednisolone for 11 years. He started to notice the facial lesions during this period. (A) Prominent multiple hyperplastic sebaceous glands seen as skin-colored papules (arrows) scattered on the right side of the face after treatment of cyclosporine for 11 years and tacrolimus for 4 years. (B) Sebaceous hyperplasia almost completely cleared after 2 months of oral isotretinoin.
[Source 2 ]Figure 5. Sebaceous hyperplasia
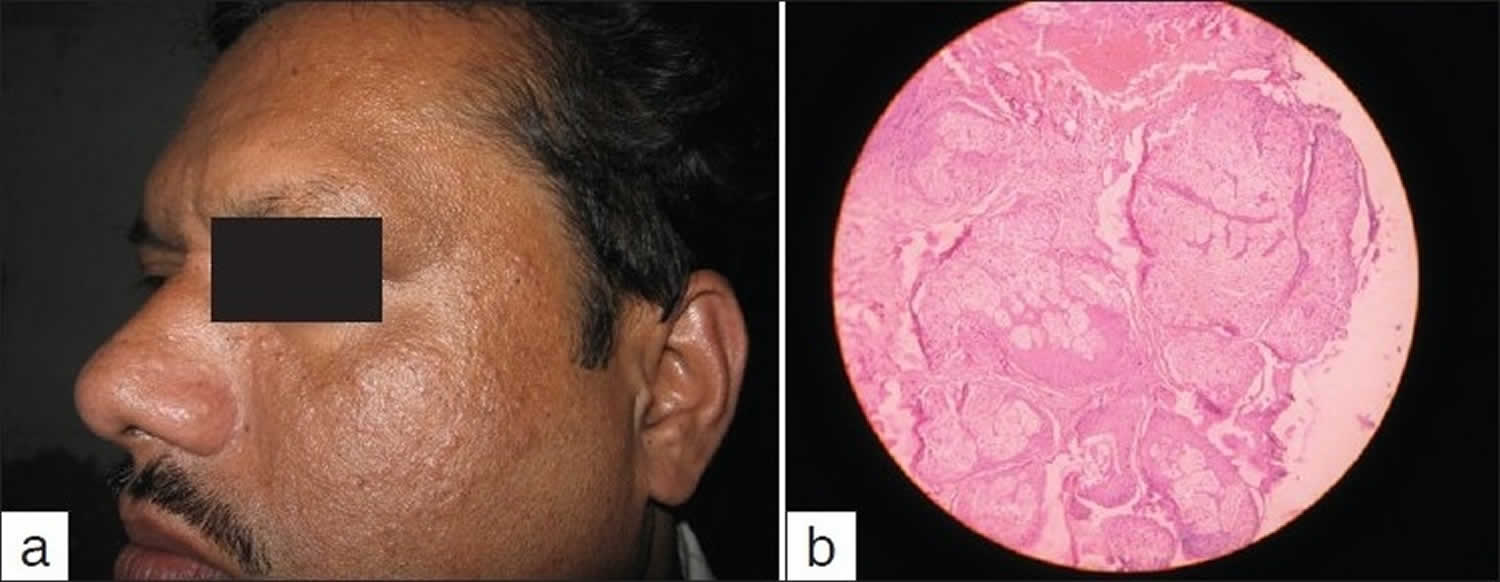
Footnotes: (a) Sebaceous hyperplasia in a 28-year-old male; (b) Histopathology of sebaceous hyperplasia large mature sebaceous lobules (H & E stain, 400×)
[Source 3 ]Figure 6. Sebaceous hyperplasia over the nose

Sebaceous hyperplasia causes
Facial papular sebaceous hyperplasia is thought to be caused by a decrease in the circulating levels of androgen associated with aging 21. Sebum production, together with sweat production, is highly androgen-sensitive; the activity and size of sebaceous glands are different according to age and circulating hormone levels 7. The number of sebaceous gland units remains approximately the same throughout life, but their metabolic rate differs during different life stages. Sebocytes contain androgen-metabolizing enzymes (5-alpha-reductase type 1, 3-beta-hydroxysteroid dehydrogenase, 17-beta-hydroxysteroid dehydrogenase type 2) which metabolize weak circulating androgens into potent androgens; a typical conversion is dehydroepiandrosterone-sulfate into dihydrotestosterone (DHT) 7. Dihydrotestosterone (DHT) binding to androgen-specific receptors of the sebocytes increases their size and metabolic rate. Scalp and face are areas where the 5-alpha-reductase has the highest activity in conversion towards testosterone and dihydrotestosterone (DHT), stimulating sebaceous gland proliferation. The opposite effect occurred for estrogens, which decrease sebaceous gland activity 7.
A decrease in circulating androgen results in smaller sebocytes with larger nuclei and lower lipid content, which migrate slowly through the sebaceous gland. As migration and disintegration of the sebocytes slows, the gland becomes enlarged, with a widened sebaceous duct and an increased number of basal cells.
Ultraviolet radiation is considered only a cofactor, because sebaceous hyperplasia occasionally occurs on areas of the body where sunlight is not a relevant issue, including the buccal mucosa, nipples, and vulva 14, 25, 26.
Sebaceous hyperplasia has also been linked to long-term immunosuppression in post-transplantation patients taking cyclosporin A and antiretroviral drugs 9. Although the mechanism for this reaction is poorly understood, it is thought to be specific to the lipophilic cyclosporin A, considering that other immunosuppressants have not been strongly associated with an increased prevalence of sebaceous hyperplasia. Occasionally, presentation is delayed for months after completion of cyclosporin therapy 27. In 2017, a case of eruptive sebaceous hyperplasia was reported in a renal transplant patient treated with the immunosuppressant tacrolimus 28.
Although more commonly found in the older population, premature or familial cases have been reported in which younger individuals are affected with multiple lesions, suggesting a genetic predisposition. In these cases of premature familial sebaceous hyperplasia, extensive eruptions appear at puberty and tend to progress with age 29.
Leopold et al 30 support the hypothesis that mutations in the EGFR-RASMAPK pathway play an important role in the pathogenesis of sebaceous hyperplasia.
Muir–Torre syndrome (MTS), described by Muir et al. in 1967 and Torre in 1968, is characterized by the presence of both sebaceous neoplasms and visceral malignancies 31, 32. Muir–Torre syndrome is a rare autosomal dominant disorder, defined by the presence of multiple skin neoplasms mainly with sebaceous differentiation and the presence of visceral malignancies, mainly colorectal, endometrial, ovarian, and renal/pelvis/ureter carcinomas 5. The skin tumors that have been related to Muir–Torre syndrome are the sebaceous adenomas; sebaceous epitheliomas; sebaceous carcinomas; cystic sebaceous tumors; basal cell carcinomas with sebaceous differentiation; and keratoacanthomas 5. Muir–Torre syndrome (MTS) is caused by microsatellite instability due to mutations in DNA mismatch repair proteins. The association with sebaceous hyperplasia is controversial, but research has demonstrated it in some cases; Muir–Torre syndrome should be a consideration in the appropriate clinical setting 33, 34, 35, 36, 37. The transmission is typically autosomal dominant, so the identification of one patient can potentially aid in the identification of multiple cases in the entire family. Muir–Torre syndrome (MTS) is considered a variant of hereditary non-polyposis colorectal cancer (HNPCC) syndrome or Lynch syndrome 31, 38.
Sebaceous hyperplasia pathophysiology
Sebaceous glands are found throughout the skin except on the palms and soles. They exist as a component of the pilosebaceous unit or, less frequently, open directly to the epithelial surface in areas of modified skin, including the lips and buccal mucosa (as Fordyce spots), glans penis or clitoris (as Tyson glands), areolae (as Montgomery glands), and eyelids (as meibomian glands). The largest and greatest numbers of sebaceous glands are found on the face, chest, back, and the upper outer arms.
These holocrine glands are composed of acini attached to a common excretory duct. The life cycle of a sebocyte, the cells that form the sebaceous gland, begins at the periphery of the gland in the highly mitotic basal cell layer. As sebocytes differentiate and mature, they accumulate increasing amounts of lipid and migrate toward the central excretory duct. The mature sebocytes complete their life cycle at the central duct and disintegrate, releasing their lipid contents as sebum. The turnover time from sebocyte production to disintegration is approximately 1 month.
Sebaceous glands are highly androgen sensitive, and, although the number of sebaceous glands remains approximately the same throughout life, their activity and size vary according to age and circulating hormone levels. Together, sebaceous and sweat glands account for the vast majority of androgen metabolism in the skin.
Sebocytes contain androgen-metabolizing enzymes, including 5-alpha-reductase type I, 3-beta-hydroxysteroid dehydrogenase, and 17-beta-hydroxysteroid dehydrogenase type II. These enzymes metabolize relatively weak circulating androgens, such as dehydroepiandrosterone-sulfate, into the more potent androgens, such as dihydrotestosterone. These, in turn, bind to receptors within the sebocytes, causing an increase in the size and metabolic rate of the sebaceous gland. Studies have shown that the activity of 5-alpha-reductase is higher in the scalp and facial skin than in other areas, so that testosterone and dihydrotestosterone stimulate more sebaceous gland proliferation in these areas. Estrogens, on the other hand, have been found to decrease sebaceous gland secretion.
In the perinatal period, the sebaceous glands are initially large and are likely responsible for the production of vernix caseosa often seen in newborns. The activity and size of the sebaceous glands regress shortly after birth, due to withdrawal of maternal hormones, and remain small throughout infancy and childhood. At puberty, sebaceous glands enlarge and become increasingly active due to increased production of androgens, reaching their maximum by the third decade of life. As androgen levels decrease with advancing age, the sebocyte turnover begins to slow down.
This decrease in cellular turnover results in crowding of primitive sebocytes within the gland, resulting in enlargement. In contrast to normal sebocytes that are engorged with lipid, the hyperplastic sebaceous glands contain small undifferentiated sebocytes with large nuclei and scant cytoplasmic lipid 29.
Sebaceous hyperplasia signs and symptoms
Sebaceous hyperplasia lesions may be single or multiple small (2 to 9 mm), painless, whitish-yellow-to-pink or skin-colored bumps, often with a central depression or dimple corresponding to the follicular infundibular ostium. They are seen in areas where many oil glands are found – the face (nose, cheeks, and forehead), chest, upper arms, mouth lining, vulvar area, and around the nipples.
The severity of sebaceous hyperplasia lesions has been classified as limited if less than ten lesions are recognized, moderate (10 to 50 lesions), frequent (less than 100 lesions), and very frequent (more than 100 lesions) 39.
Sebaceous hyperplasia diagnosis
No laboratory studies are necessary. Biopsy is occasionally indicated to exclude basal cell carcinoma.
Dermoscopically, sebaceous hyperplasia reveals a pattern composed of aggregated white-yellowish nodules corresponding to hyperplastic sebaceous glands. The ostium of the sebaceous gland is sometimes visible as a small crater or umbilication in the center of those yellowish nodules 40. Surrounding the nodules, there is a blood vessel pattern visible with dermoscopy; the most common and specific is the so-called “crown vessels”, which may extend toward the center without crossing it. The dermoscopic findings significantly aid in the diagnosis 41.
Sebaceous hyperplasia histopathology
Histopathological examination of sebaceous hyperplasia lesions reveals enlarged sebaceous glands with normal cellular architecture. Inside each gland, mature sebaceous lobules connect to a dilated principal sebaceous duct, while the presence of at least four lobules per hair follicle is suggested as a diagnostic criterion 9. Another commonly used criterion for distinguishing sebaceous hyperplasia from sebaceous adenoma is the number of germinative cell layers in the periphery of the lobules; when more than two germinative cell layers are present, a sebaceous adenoma should be suspected 42, 43.
Sebaceous hyperplasia treatment
Sebaceous hyperplasia is harmless and does not require any treatment. However, for cosmetic reasons or if they are bothersome if irritated, individual lesions may be removed by light electrocautery or laser vaporization.
Many types of treatment can remove sebaceous hyperplasia, with a small risk of leaving scars:
- Burning (cautery)
- Freezing (cryosurgery)
- Applying topical chemicals
- Applying a drug activated by light (photodynamic therapy)
- Laser treatment
- Cutting out the lesions (excision)
When the lesions are severe, extensive or disfiguring, oral isotretinoin is effective in clearing lesions but the treatment must continue for several months, and there are high relapse rates with discontinuation. Oral isotretinoin is not for use during pregnancy. In females, antiandrogens may help improve the appearance.
Photodynamic therapy uses with the wavelength of 1720 nm is said to be specific for the sebaceous gland unit; it provides minimal damage to the surrounding tissues but requires multiple sessions and special equipment 44. The most appropriate lasers used to treat sebaceous hyperplasia are Argon and carbon dioxide (CO2) 7.
Sebaceous hyperplasia prognosis
Sebaceous hyperplasia has no direct association with malignant degeneration and is not a cause of morbidity beyond cosmetic concerns. Sebaceous hyperplasia has been reported in association with internal malignancy in the setting of Muir-Torre syndrome. Muir-Torre syndrome is a rare autosomal dominant disorder in which visceral malignancies, sebaceous neoplasms (eg, sebaceous adenoma, sebaceous carcinoma), and keratoacanthoma coincide. Colon cancer is the leading internal malignancy associated with Muir-Torre syndrome, followed by hematologic malignancies 45. Sebaceous hyperplasia alone does not signify a predisposition to cancer or represent a sign of Muir-Torre syndrome.
One study reported that 29.9% of patients with a renal transplant had sebaceous hyperplasia, and that 45.7% of these patients had a history of nonmelanoma skin cancer, compared with 7.3% of patients without sebaceous hyperplasia. In this population, the association of nonmelanoma skin cancer with sebaceous hyperplasia remained significant after correction of factors such as age, sex, skin type, and duration since transplantation 20. Thus, the presence of sebaceous hyperplasias in the setting of renal transplantation may serve as a marker for an elevated risk of nonmelanoma skin cancer.
- Lester RA, Torgerson RR, Sandhu NP. Rare presentation of sebaceous hyperplasia. BMJ Case Rep. 2014 Apr 23;2014:bcr2014204025. doi: 10.1136/bcr-2014-204025[↩]
- Jung HY, Kim M, Cho BK, Park HJ. A Case of Cyclosporine-Induced Sebaceous Hyperplasia in a Renal Transplant Patient Successfully Treated with Isotretinoin. Ann Dermatol. 2016 Apr;28(2):271-2. doi: 10.5021/ad.2016.28.2.271[↩][↩]
- Saha A, Das NK, Gharami RC, Chowdhury SN, Datta PK. A clinico-histopathological study of appendageal skin tumors, affecting head and neck region in patients attending the dermatology opd of a tertiary care centre in eastern India. Indian J Dermatol. 2011 Jan;56(1):33-6. doi: 10.4103/0019-5154.77548[↩][↩]
- Durai PC, Thappa DM, Kumari R, Malathi M. Aging in elderly: chronological versus photoaging. Indian J Dermatol. 2012 Sep;57(5):343-52. doi: 10.4103/0019-5154.100473[↩][↩]
- Papadimitriou I, Vakirlis E, Sotiriou E, Bakirtzi K, Lallas A, Ioannides D. Sebaceous Neoplasms. Diagnostics (Basel). 2023 May 9;13(10):1676. doi: 10.3390/diagnostics13101676[↩][↩][↩][↩][↩]
- Salim A., Reece S.M., Smith A.G., Harrison D., Ramsay H.M., Harden P.N., Fryer A.A. Sebaceous hyperplasia and skin cancer in patients undergoing renal transplant. J. Am. Acad. Dermatol. 2006;55:878–881. doi: 10.1016/j.jaad.2005.09.041[↩]
- Farci F, Rapini RP. Sebaceous Hyperplasia. [Updated 2023 Sep 4]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK562148[↩][↩][↩][↩][↩][↩]
- Kanada KN, Merin MR, Munden A, Friedlander SF. A prospective study of cutaneous findings in newborns in the United States: correlation with race, ethnicity, and gestational status using updated classification and nomenclature. J Pediatr. 2012 Aug;161(2):240-5. doi: 10.1016/j.jpeds.2012.02.052[↩][↩]
- Iacobelli J., Harvey N.T., Wood B.A. Sebaceous lesions of the skin. Pathology. 2017;49:688–697. doi: 10.1016/j.pathol.2017.08.012[↩][↩][↩]
- Hussein L., Perrett C.M. Treatment of sebaceous gland hyperplasia: A review of the literature. J. Dermatol. Treat. 2021;32:866–877. doi: 10.1080/09546634.2020.1720582[↩]
- Kanada KN, Merin MR, Munden A, Friedlander SF. A prospective study of cutaneous findings in newborns in the United States: correlation with race, ethnicity, and gestational status using updated classification and nomenclature. J Pediatr. 2012 Aug. 161(2):240-5.[↩]
- Moosavi Z, Hosseini T. One-year survey of cutaneous lesions in 1000 consecutive Iranian newborns. Pediatr Dermatol. 2006 Jan-Feb;23(1):61-3. doi: 10.1111/j.1525-1470.2006.00172.x[↩]
- Hogan DJ. Sebaceous hyperplasia of the chest. Int J Dermatol. 1991 Apr;30(4):306. doi: 10.1111/j.1365-4362.1991.tb04651.x[↩]
- Daley TD. Intraoral sebaceous hyperplasia. Diagnostic criteria. Oral Surg Oral Med Oral Pathol. 1993 Mar;75(3):343-7. doi: 10.1016/0030-4220(93)90148-w[↩][↩]
- Ma HJ, Zhao G, Wang YX. Sebaceous hyperplasia of the scrotum in an adolescent boy. Pediatr Dermatol. 2007 May-Jun;24(3):340-2. doi: 10.1111/j.1525-1470.2007.00427.x[↩]
- Ena P, Origa D, Massarelli G. Sebaceous gland hyperplasia of the foreskin. Clin Exp Dermatol. 2009 Apr;34(3):372-4. doi: 10.1111/j.1365-2230.2008.02998.x[↩]
- Ju HY, Kim HS, Kim HO, Park YM. Sebaceous hyperplasia of the penile shaft. J Eur Acad Dermatol Venereol. 2009 Apr;23(4):443-4. doi: 10.1111/j.1468-3083.2008.02908.x[↩]
- Bakaris S, Kiran H, Kiran G. Sebaceous gland hyperplasia of the vulva. Aust N Z J Obstet Gynaecol. 2004 Feb;44(1):75-6. doi: 10.1111/j.1479-828X.2004.00165.x[↩]
- Krisp A, Krause W. Areolar sebaceous hyperplasia. Acta Derm Venereol. 2003;83(1):61-2. doi: 10.1080/00015550310002792[↩]
- Salim A, Reece SM, Smith AG, et al. Sebaceous hyperplasia and skin cancer in patients undergoing renal transplant. J Am Acad Dermatol. 2006 Nov. 55(5):878-81.[↩][↩]
- Sebaceous hyperplasia. https://emedicine.medscape.com/article/1059368-overview[↩][↩]
- Kato N, Yasuoka A. “Giant” senile sebaceous hyperplasia. J Dermatol. 1992 Apr. 19(4):238-41.[↩]
- Sato T, Tanaka M. Linear sebaceous hyperplasia on the chest. Dermatol Pract Concept. 2014 Jan. 4 (1):93-5.[↩]
- Mandal RK, Das A, Chakrabarti I, Agarwal P. Nevoid sebaceous hyperplasia mistaken as nevus sebaceous: Report of four cases. Indian J Dermatol Venereol Leprol. 2017 Mar-Apr. 83 (2):213-216.[↩]
- Malliah R, Gilhooly P, Lambert WC, Heller DS. Sebaceous hyperplasia of the vulva: case report and review of the literature. J Low Genit Tract Dis. 2006 Jan;10(1):55-7. doi: 10.1097/01.lgt.0000194825.78244.20[↩]
- Chiriac A, Moldovan C, Coros MF, Podoleanu C, Moncea D, Stolnicu S. Bilateral areolar sebaceous hyperplasia in a post-menopausal woman. Eur J Dermatol. 2016 Jun 1;26(3):299-300. doi: 10.1684/ejd.2016.2739[↩]
- Wilken R, Fung MA, Shi VY, Cheng MY, Patel F, Sultani H, et al. Cyclosporine-induced sebaceous hyperplasia in a hematopoetic stem cell transplant patient: delayed onset of a common adverse event. Dermatol Online J. 2016 Jan 15. 22, 1[↩]
- Levandoski KA, Girardi NA, Loss MJ. Eruptive sebaceous hyperplasia as a side effect of oral tacrolimus in a renal transplant recipient. Dermatol Online J. 2017 May 15. 23, 5[↩]
- Wang Q, Liu JM, Zhang YZ. Premature sebaceous hyperplasia in an adolescent boy. Pediatr Dermatol. 2011 Mar-Apr. 28(2):198-200.[↩][↩]
- Groesser L, Singer S, Peterhof E, Landthaler M, Heigl U, Schneider-Brachert W, Berneburg M, Hafner C. KRAS, HRAS and EGFR Mutations in Sporadic Sebaceous Gland Hyperplasia. Acta Derm Venereol. 2016 Aug 23;96(6):737-41. doi: 10.2340/00015555-2351[↩]
- Eiger-Moscovich M., Eagle R.C., Jr., Shields C.L., Racher H., Lally S.E., Silkiss R.Z., Shields J.A., Milman T. Muir-Torre Syndrome Associated Periocular Sebaceous Neoplasms: Screening Patterns in the Literature and in Clinical Practice. Ocul. Oncol. Pathol. 2020;6:226–237. doi: 10.1159/000504984[↩][↩]
- Torre D. Multiple sebaceous tumors. Arch Dermatol. 1968 Nov;98(5):549-51. doi: 10.1001/archderm.98.5.549[↩]
- Jakobiec FA, Cortes Barrantes P, Milman T, Lee NG, Fay A. Ocular Adnexal Adenomatoid Sebaceous Gland Hyperplasia: A Clinical and Immunopathologic Analysis in Relation to the Muir-Torre Syndrome. Ophthalmic Plast Reconstr Surg. 2020 Jan/Feb;36(1):e6-e12. doi: 10.1097/IOP.0000000000001497[↩]
- Spraul CW, Jakobczyk-Zmija MJ, Lang GK. Talgdrüsenhyperplasie des Unterlides [Sebaceous hyperplasia of the lower eyelid]. Klin Monbl Augenheilkd. 1999 Nov;215(5):319-20. German. doi: 10.1055/s-2008-1034722[↩]
- Ponti G, Meschieri A, Pollio A, Ruini C, Manfredini M, Longo C, Mandel VD, Ciardo S, Tomasi A, Giannetti L, Pellacani G. Fordyce granules and hyperplastic mucosal sebaceous glands as distinctive stigmata in Muir-Torre syndrome patients: characterization with reflectance confocal microscopy. J Oral Pathol Med. 2015 Aug;44(7):552-7. doi: 10.1111/jop.12256[↩]
- Kruse R, Rütten A, Schweiger N, Jakob E, Mathiak M, Propping P, Mangold E, Bisceglia M, Ruzicka T. Frequency of microsatellite instability in unselected sebaceous gland neoplasias and hyperplasias. J Invest Dermatol. 2003 May;120(5):858-64. doi: 10.1046/j.1523-1747.2003.12125.x[↩]
- Roma AA, Barry J, Pai RK, Billings SD. Sebaceous hyperplasia of the vulva: a series of cases reporting no association with the Muir-Torre syndrome. Int J Gynecol Pathol. 2014 Jul;33(4):437-42. doi: 10.1097/PGP.0b013e31829ff21e[↩]
- John AM, Schwartz RA. Muir-Torre syndrome (MTS): An update and approach to diagnosis and management. J Am Acad Dermatol. 2016 Mar;74(3):558-66. doi: 10.1016/j.jaad.2015.09.074[↩]
- Kavoussi H, Rezaei M, Azimi M, Kavoussi R. Combination of CO2 laser therapy and curettage for sebaceous gland hyperplasia. Acta Dermatovenerol Alp Pannonica Adriat. 2019 Mar;28(1):11-14. https://acta-apa.mf.uni-lj.si/journals/acta-dermatovenerol-apa/papers/10.15570/actaapa.2019.3/actaapa.2019.3.pdf[↩]
- Zaballos P, Gómez-Martín I, Martin JM, Bañuls J. Dermoscopy of Adnexal Tumors. Dermatol Clin. 2018 Oct;36(4):397-412. doi: 10.1016/j.det.2018.05.007[↩]
- Kim NH, Zell DS, Kolm I, Oliviero M, Rabinovitz HS. The dermoscopic differential diagnosis of yellow lobularlike structures. Arch Dermatol. 2008 Jul;144(7):962. doi: 10.1001/archderm.144.7.962[↩]
- Lazar A.J., Lyle S., Calonje E. Sebaceous neoplasia and Torre-Muir syndrome. Curr. Diagn. Pathol. 2007;13:301–319. doi: 10.1016/j.cdip.2007.05.001[↩]
- Böer-Auer A. [Differential diagnostics of sebaceous tumors] Der Pathol. 2014;35:443–455. doi: 10.1007/s00292-014-1934-y[↩]
- Simmons BJ, Griffith RD, Falto-Aizpurua LA, Bray FN, Nouri K; International League of Dermatological Societies; European Dermatology Forum. Light and laser therapies for the treatment of sebaceous gland hyperplasia a review of the literature. J Eur Acad Dermatol Venereol. 2015 Nov;29(11):2080-7. doi: 10.1111/jdv.13066[↩]
- Johnson PJ, Heckler F. Muir-Torre syndrome. Ann Plast Surg. 1998 Jun. 40(6):676-7.[↩]





{kind=link}