Contents
- Photocontact dermatitis
Photocontact dermatitis
Photocontact dermatitis is an inflammatory skin reaction that occurs when ultraviolet (UV) or visible light interacts with a topically applied or systemically taken photoreactive substance on or in the skin 1. Anyone, male or female, can get photocontact dermatitis. Photocontact dermatitis signs and symptoms are similar to other forms of allergic contact dermatitis, but eczematous lesions (small, round or oval bumps on the skin that can be itchy or burning) predominantly affect sun-exposed sites, with sparing of anatomically shaded areas 2, 3. In severe reactions, there can be spreading to non-exposed sites, which can further complicate the clinical picture 4
Photocontact dermatitis results from the interaction of two factors:
- A photoreactive substance (a substance with the potential to induce photocontact dermatitis), either applied topically or taken systemically before reaching the skin through the circulation.
- Exposure to ultraviolet rays, mainly ultraviolet A radiation (UVA), or visible light.
Risk factors for photocontact dermatitis include sunscreen, fragrances and perfumes, medications, cosmetics, and other substances use. Additional risk factors include occupational risk factors such as working outside (e.g., gardeners, farmers, builders, carpenters, roofers, and road workers) and working with plants that contain psoralens (e.g., celery harvesters and canners) 5, 6.
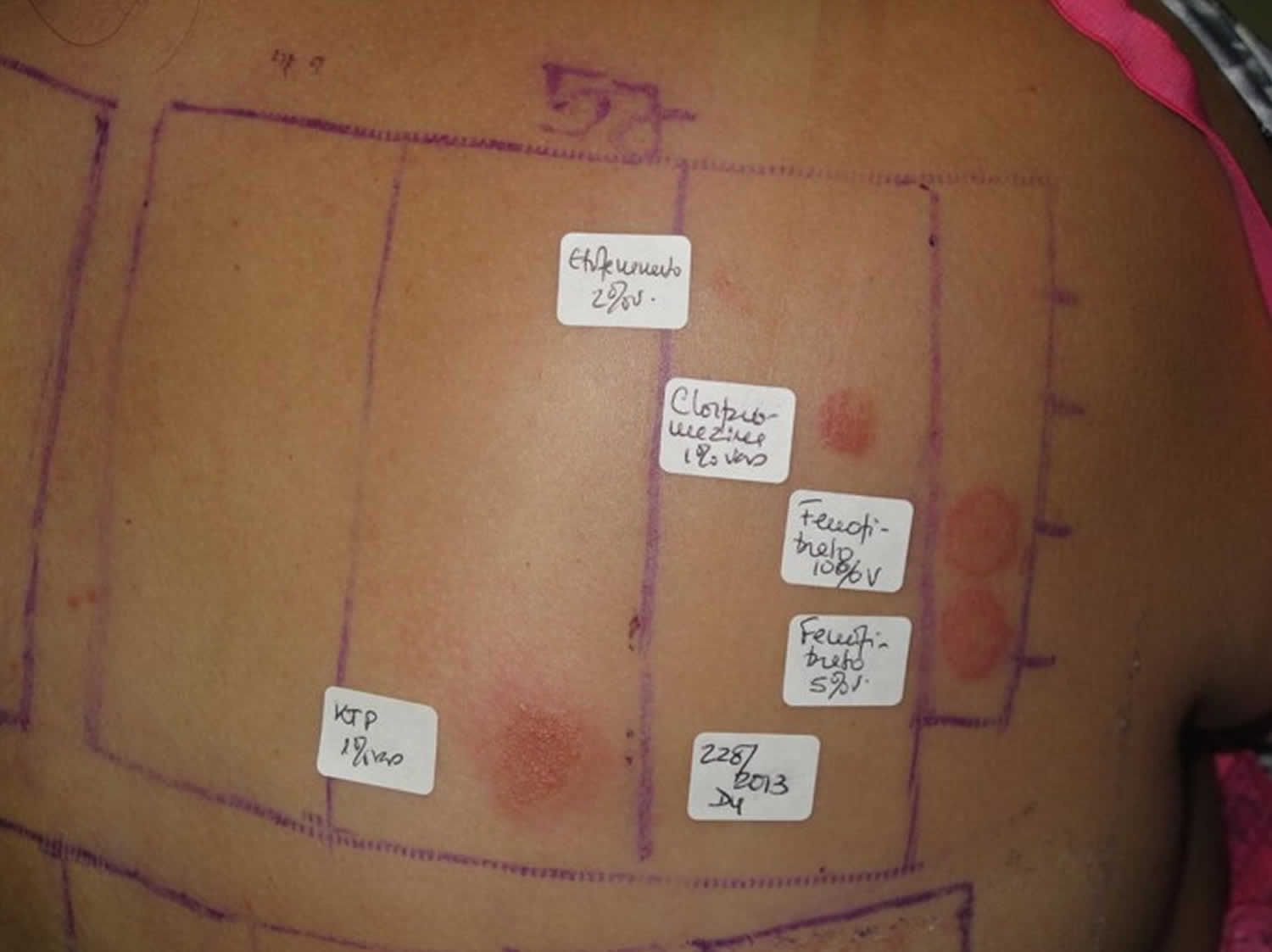
Photocontact dermatitis can be classified into 2 types (see Table 1 below) 1:
- Phototoxic contact dermatitis also known as photo-irritant contact dermatitis affects 5 to 6% of the population is a non-immunological reaction, thought to develop as a result of free radicals produced by phototoxic reactions directly harming the skin 7
- Photoallergic contact dermatitis affects 2 to 8% of the population is a delayed-type 4 hypersensitivity reaction that occurs in a person who is sensitized to a photoallergen and then exposed to UV light 8. Photoallergic contact dermatitis reactions are commonly caused by topical sunscreens or non-steroidal anti-inflammatories 6.
It is important to distinguish photoallergic contact dermatitis from phototoxic contact dermatitis or photoirritant contact dermatitis. Asking about the onset and timing of the skin eruption may be critical for distinction, as phototoxic contact dermatitis (photoirritant contact dermatitis) can occur within minutes to hours of the first exposure to a chemical and UV radiation, while there is a sensitization delay in photoallergic contact dermatitis 9. Phytophotodermatitis is a well-known type of phototoxic contact dermatitis (photoirritant contact dermatitis) caused by exposure to furocoumarin-containing plants, most commonly limes 10. Other causes of phototoxic contact dermatitis (photoirritant contact dermatitis) include tar products and certain medications 11. Importantly, photopatch testing to a known phototoxic chemical should never be performed because it will cause a strong reaction in anyone tested, regardless of exposure history 12.
Other diagnoses to consider include photoaggravated dermatoses (eg, atopic dermatitis, lupus erythematosus, dermatomyositis) and idiopathic photodermatoses (eg, chronic actinic dermatitis, actinic prurigo, polymorphous light eruption) 12. Although atopic dermatitis usually improves with UV light exposure, photoaggravated atopic dermatitis is suggested in eczema patients who flare with sun exposure, in a seasonal pattern, or after phototherapy; this condition is challenging to differentiate from photoallergic contact dermatitis if photopatch testing is not performed 13. The diagnosis of idiopathic photodermatoses is nuanced; however, asking about the timeline of the reaction including onset, duration, and persistence, as well as characterization of unique clinical features, can help in differentiation 14. In certain scenarios, a biopsy may be helpful. A thorough review of systems will help to assess for autoimmune connective tissue disorders, and relevant serologies should be checked as indicated.
Table 1. Photocontact dermatitis types
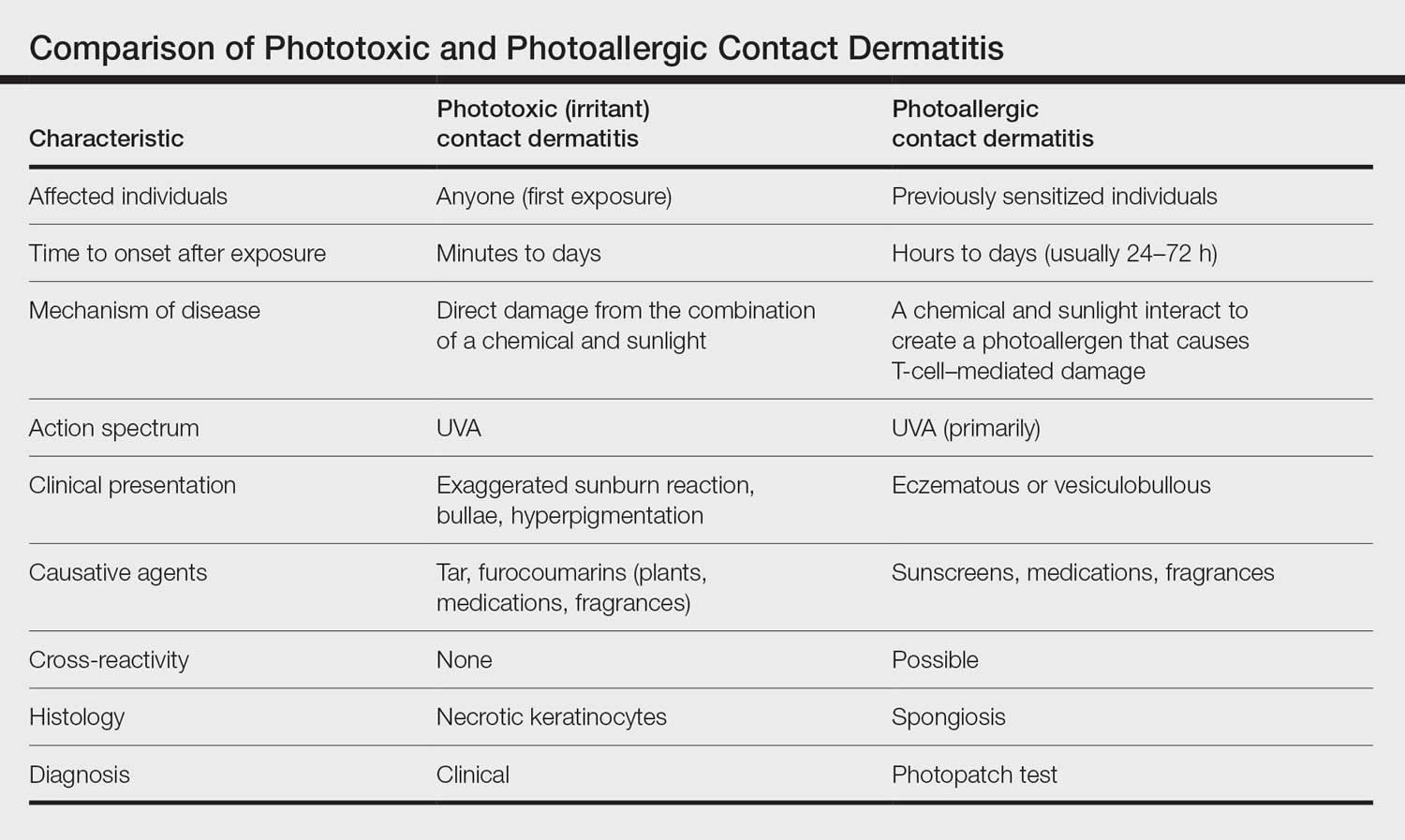
Figure 1. Photoallergic contact dermatitis after application of a sunscreen
Footnote: Photoallergic contact dermatitis after application of a sunscreen, especially in the neckline (a) and back of neck area (b).
[Source 15 ]Figure 2. Photoallergic contact dermatitis

Figure 3. Photoallergic contact dermatitis due to diclofenac gel

Figure 4. Phototoxic contact dermatitis due to eating celery seeds

Footnote: Phototoxic contact dermatitis due to eating celery seeds.
[Source 1 ]Figure 5. Phototoxic contact dermatitis due accidental lime juice contact on a sunny day

Footnote: Phototoxic contact dermatitis due accidental lime juice contact on a sunny day
[Source 1 ]See your doctor if:
- The rash is so itchy that you can’t sleep or go about your day
- The rash is severe or widespread
- You’re worried about how your rash looks
- The rash doesn’t get better within three weeks
- The rash involves the eyes, mouth, face or genitals
Seek immediate medical care in the following situations:
- You think your skin is infected. Clues include fever and pus oozing from blisters.
- It’s hard to breathe after inhaling burning weeds.
- Your eyes or nasal passages hurt after inhaling smoke from burning poison ivy.
- You think an ingested substance has damaged the lining of your mouth or digestive tract.
Photocontact dermatitis causes
Photocontact dermatitis results from the interaction of two factors:
- A photoreactive substance (a substance with the potential to induce photocontact dermatitis), either applied topically or taken systemically before reaching the skin through the circulation.
- Exposure to ultraviolet rays, mainly ultraviolet A radiation (UVA), or visible light.
A photoallergic reaction may develop when ultraviolet (UV) light interacts with chemical agents (i.e. fragrances, para-aminobenzoic acid [PABA], plants, parsnips, figs, or certain oral medications), inducing various forms of photosensitization. For example, phototoxic and photoallergic lesions can develop on sun-exposed skin with systemically administered agents (i.e. medications). Contrastingly, when the sensitizing agent is applied directly to the skin (i.e. fragrances), lesions will develop at the site of application following exposure to sunlight.
Risk factors for photocontact dermatitis include sunscreen, fragrances and perfumes, medications, cosmetics, and other substances use. Additional risk factors include occupational risk factors such as working outside (e.g., gardeners, farmers, builders, carpenters, roofers, and road workers) and working with plants that contain psoralens (e.g., celery harvesters and canners).
In 2013, Greenspoon et al 2 published photopatch testing results for 160 patients undergoing photopatch testing to 26 allergens in Toronto from 2001 to 2010. Test positivity was the highest for chlorpromazine hydrochloride (13.1%) and promethazine hydrochloride (13.1%), and among clinically relevant photoallergens, the highest positive rates were seen with sunscreen ingredients, especially benzophenone-3 (12.1%) and octyldimethyl PABA in 5% alcohol (5.1%). Only one patient reacted to thiourea, with photoaggravated allergic contact dermatitis 2. In 2016, Hu et al 5 published photopatch testing results for 6153 Chinese patients who underwent photopatch testing between 2005 and 2014. The highest positive rates were seen with chlorpromazine (51.82%), para-aminobenzoic acid (11.94%), thimerosal (9.81%), potassium dichromate (6.37%), sulfanilamide (5.38), and formaldehyde (4.7%). Thiourea had a patch test positivity rate of 2.97%, photopatch 1.78%, and photoaggravation 0.07% 5.
Phototoxic contact dermatitis
Phototoxic contact dermatitis also known as photo-irritant contact dermatitis is a non-immunological reaction, thought to develop as a result of free radicals produced by phototoxic reactions directly harming the skin. Anyone exposed to sufficient phototoxic agents and light of an appropriate wavelength can develop phototoxic dermatitis.
Common phototoxic agents include:
- Plants that contain furocoumarins (psoralens) eg, citrus fruits (lemons and limes), figs, yarrow, celery, parsley, cow parsnip/hogweed, beans, and carrots
- Coal tar and its products
- Dyes
- Wood preservatives
- Drugs such as:
- Tetracyclines (doxycycline)
- Thiazides
- Sulfa drugs (eg, sulfonamides, sulfonylureas)
- Phenothiazines
- Amiodarone
- Non-steroidal anti-inflammatory agents (NSAIDs).
Photoallergic contact dermatitis
Photoallergic contact dermatitis is thought to represent a delayed-type 4 hypersensitivity reaction that occurs against a light-activated photosensitizing agent also known as a photosensitizer combines with some component of the skin in the presence of ultraviolet (UV) usually in the UVA range (315–400 nm) and/or visible light 18, 19, 20. When photosensitizing agent (photosensitizer) is applied to the skin and then exposed to UV rays, in some individuals a small portion of the substance (hapten) binds to a protein in the skin to form a photoantigen. This photoantigen is then taken up by an antigen-presenting cells in the epidermis and transported to the nearby lymphocytes where specific T-cells are activated 21. If the sensitized patient uses the same chemical again, sun exposure can cause an eczematous reaction 20.
Development of photoallergic contact dermatitis does not necessarily depend on the dose of the chemical or the amount of UV radiation 9. Why certain individuals may be more susceptible is unknown, though major histocompatibility complex haplotypes could be influential 22, 23.
More than 300 common medications are known to be photosensitizing agents. Many antibiotics, diuretics, antihypertensives, botanicals (St. John’s wort), psoralens, and other agents increase the sensitivity of lens protein to UV damage 24.
Commonly encountered photoallergic agents (photoallergens) include:
- Chemical sunscreen components such as benzophenone-3 and cinnamates (eg, octocrylene)
- Fragrances and perfumes
- Non-steroidal anti-inflammatory agents (NSAIDs) eg, topical ketoprofen, topical etofenamate, piroxicam gel.
Currently, organic UV sunscreen absorbers and topical nonsteroidal anti-inflammatory drugs (NSAIDs) are the commonest photohaptens encountered by patients.
Photocontact dermatitis prevention
Photocontact dermatitis prevention involves identifying what’s causing your rash and avoiding the causative photoreactive agents. Your skin doctor may give you a list of products that typically contain the substance that affects you. Also ask for a list of products that are free of the substance that affects you.
Photocontact dermatitis signs and symptoms
Skin lesions in photocontact dermatitis are generally confined to sun-exposed areas such as your face, neck, V-shaped area of the chest (‘‘V’’ of the anterior neck), dorsal hands, and forearms. The following areas are usually spared: the upper eyelids, upper lip, the area below the chin, the area behind your ears, and the skin folds of your neck.
Phototoxic contact dermatitis
Phototoxic contact dermatitis looks like an exaggerated sunburn and is limited to sun-exposed sites. Patients may report pain and a burning sensation. Blisters and distal onycholysis (fingernails or toenails to separate from the nail bed) are sometimes seen. Postinflammatory hyperpigmentation frequently follows phototoxic contact dermatitis.
Phytophotodermatitis, a type of plant dermatitis, is a phototoxic reaction that develops after psoralen-containing plant sap comes in contact with the skin, which is subsequently exposed to ultraviolet A radiation (UVA). The rash manifests as painful non-itchy reddish linear streaks and blisters. Phytophotodermatitis usually resolves leaving postinflammatory hyperpigmentation. Patients with darker skin types are more likely to have postinflammatory hyperpigmentation.
Photoallergic contact dermatitis
Photoallergic contact dermatitis looks like allergic contact dermatitis. The skin lesions are itchy and confined mainly to sun-exposed skin areas, although sometimes may involve non-exposed sites. With frequent exposure to the allergen, the skin lesions may become lichenified (thickened, leathery, and hardened skin that’s often caused by chronic scratching or rubbing).
Photocontact dermatitis complications
Photocontact dermatitis complications may include:
- Postinflammatory hyperpigmentation.
- Blister formation.
- Superimposed bacterial skin infection. Photocontact dermatitis can lead to an infection if you repeatedly scratch the affected area, causing it to become wet and oozing. This creates a good place for bacteria or fungi to grow and may cause an infection.
- Persistent light reactivity might develop into chronic actinic dermatitis (a skin condition that causes inflammation and eczema due to exposure to sunlight or artificial light).
Photocontact dermatitis diagnosis
Your doctor may be able to diagnose photocontact dermatitis by talking to you about your signs and symptoms. You might be asked questions to help identify the cause of your condition and uncover clues about the trigger substance. And you’ll likely undergo a skin exam to assess the rash.
A patient’s history may reveal exposure to irritants or allergens that will guide further investigations and management. The timing, distribution of skin rash, clinical course, triggers, response to treatment and history of atopy are all important.
- The temporal association between exposure to a photoreactive substance and the sun and developing symptoms should raise suspicion for photocontact dermatitis (PCD).
- Photopatch testing (UVA-irradiated patch test) can be done to confirm the diagnosis of photoallergic contact dermatitis (PACD). The purpose of patch testing is to determine if your skin rash is caused by an allergy to certain chemicals that come in contact with your skin, an allergy to UV light, or a chemical that is activated by sunlight. Photo patch testing is done by placing small amounts of chemicals on your back and exposing them to UV light. Your skin doctor will also test your skin by shining small amounts of UV light on your skin. This is a weeklong procedure. But the redness indicating a reaction can be hard to see on brown or Black skin, which may lead to a missed diagnosis.
Photopatch testing
Photopatch testing also called UVA-irradiated patch test aids the diagnosis of suspected contact and/or photocontact sunscreen allergies that may be contributing to photosensitivity 25, 26, 27. Photopatch testing may also help to guide sunscreen choice for the patient.
As most of the relevant contact allergens are activated by ultraviolet A (UVA) rather than ultraviolet B (UVB), UVA irradiation is used in photopatch testing. Photopatch test series may include sunscreens, chemical UV filters, and the patient’s own products. Nonsteroidal anti-inflammatory drugs (NSAIDs) are also commonly tested as they can be implicated in photoallergic reactions.
- Patients have two identical sets of the photocontact allergens applied in parallel to the left and right sides of the back. These are removed after two days.
- One side is then covered with a UV-opaque sheet, while the other side is exposed to 5 J/cm² of UVA. The UVA dose is reduced in patients with significant photosensitivity.
- The patient attends for three consecutive days for reading of the photopatch testing.
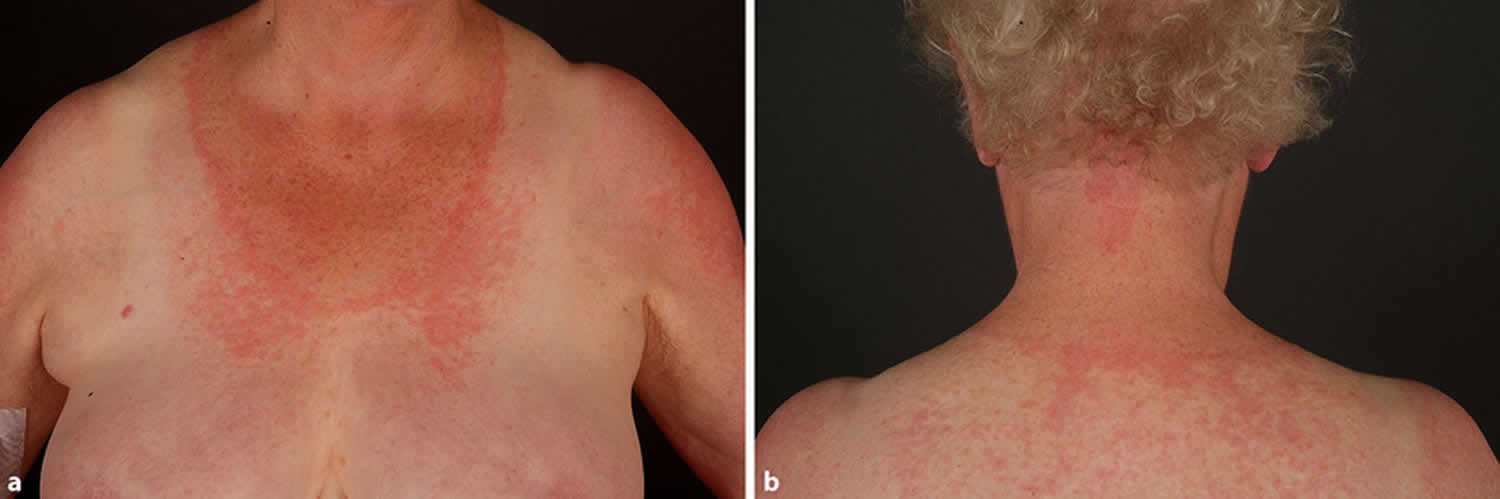
A positive photoallergic response is characterized by a positive response on the irradiated series, with a negative response to the same allergen on the non-irradiated side 25. A positive response on both sides indicates a contact allergy alone. If there is a stronger response on the UV-irradiated side, this would suggest both contact and photocontact allergy 25.
If multiple sunscreen allergies are evident, it is advisable to refer on for full patch testing to investigate for coexisting contact allergies.
Figure 6. Photopatch testing
Monochromator light testing
Monochromator light testing is an essential aspect of phototesting. The light source used is usually a 2500 watt xenon arc lamp 25. These lamps have an output that mimics sunlight.
The monochromator is a precision optical device designed to fractionate the light to allow exposure to a clearly defined waveband 25.
- An area of skin, usually on the patient’s back, is tested to incremental doses of a number of wavelengths.
- Wavelengths tested and dose ranges used vary between different photodermatology units. They may include ultraviolet B (UVB) eg, 300 nm; ultraviolet A (UVA) eg, 320, 330, 350, 370, and 400 nm; and visible wavelengths eg, 500 and 600 nm.
- The skin is then examined 24 hours later to record the minimal erythema dose (MED). The minimal erythema dose (MED) is the lowest dose of the wavelength that produces an identifiable pink response.
Photoprovocation testing
Photoprovocation can induce an eruption in patients with photosensitivity that have normal erythemal thresholds 25. It can be useful in the diagnosis of various photosensitive disorders including polymorphic light eruption (PMLE), photoaggravated atopic dermatitis, and actinic prurigo 25.
- Testing is usually performed by exposure to broadband UVA +/- visible optical radiation sources (solar simulator) on a 5×5 cm square on the patient’s forearm.
- Repeated provocation testing increases the yield for a positive response, and the standard protocol should aim for consecutive challenges over a three-day period.
The morphology of the artificially-provoked rash assists in diagnosis 25. A skin biopsy may be performed with immunofluorescence if indicated to further confirm the diagnosis. A negative test may not exclude these conditions.
Laboratory investigations
Laboratory investigations can help formulate a diagnosis in patients with photosensitivity.
Laboratory investigations may include:
- Porphyrin screen (blood, urine, feces)
- Antinuclear antibodies (ANA), anti-SSA (anti-Ro), anti-SSB (anti-La) and/or antibodies to double-stranded DNA (dsDNA) to investigate for autoimmune conditions eg, lupus
- Serum IgE (elevated in photoaggravated eczema and chronic actinic dermatitis)
- Human leukocyte antigen (HLA) genotyping: (HLA-DRB1*04:07 is present in 60% of cases of actinic prurigo)
- Vitamin D status (often low in photoprotected patients).
Photocontact dermatitis differential diagnosis
Photocontact dermatitis differential diagnosis may include:
- Allergic contact dermatitis
- Irritant contact dermatitis
- Airborne contact dermatitis. Airborne contact dermatitis refers to acute and chronic dermatitis of exposed parts of the body, especially the face, caused by particles suspended in the air. These particles may include fibres, dust, vapors, sprays, gases, and plant materials.
- Polymorphic light eruption
- Actinic prurigo. Actinic prurigo is an intensely itchy skin condition caused by an abnormal reaction to sunlight (photosensitivity). It presents with small, intensely itchy papules (prurigo) on sun-exposed sites.
- Hydroa vacciniforme. Hydroa vacciniforme is one of the rarest forms of photosensitivity dermatoses. It affects sun-exposed skin and is characterized by recurrent fluid-filled blisters (‘hydroa’) that heal with pox-like (‘vacciniform’) scars.
- Solar urticaria
- Cutaneous porphyrias, eg, porphyria cutanea tarda
- Systemic disorders with photosensitivity such as lupus and dermatomyositis (juvenile or adult-onset).
Photocontact dermatitis treatment
Photocontact dermatitis treatment options may include:
- Identify and avoid the photoreactive substance(s) (awareness of synonyms that may be used in ingredient lists is important).
- Avoid chemicals that may cross-react with the causative agent.
- Sun protection and sun protective clothing (eg, long sleeves, hats).
- Use of a suitable sunscreen. Physical (mineral-based) sunscreens such as zinc oxide and titanium dioxide are an alternative if you have a chemical sunscreen photoallergy.
- Topical steroids or calcineurin inhibitors can be used for limited photocontact dermatitis. Steroid creams or ointments are applied to the skin to help soothe the rash. You might apply prescription topical steroids, such as clobetasol 0.05% or triamcinolone 0.1%. Talk with your skin doctor about how many times a day to apply it and for how many weeks.
- Widespread photocontact dermatitis may be treated with a short course of systemic steroids. In severe cases, your skin doctor may prescribe pills you take by mouth (oral medications) to reduce swelling, relieve itching or fight a bacterial infection.
- Apply an anti-itch cream or ointment. Put on the itchy area 1% hydrocortisone cream or ointment (Cortizone 10, others). This is a nonprescription product that you can buy at a drugstore. Use it 1 to 2 times a day for a few days. Or try calamine lotion. Whatever product you use, try cooling it in the refrigerator before applying.
- Take an anti-itch drug. An oral antihistamine, such as diphenhydramine (Advil PM, Benadryl, others), which may also help you sleep better. A nonprescription antihistamine that won’t make you so drowsy is loratadine (Alavert, Claritin, others).
- Apply cool, wet compresses. Place a cool, wet cloth over the rash for 15 to 30 minutes several times a day.
- Protect your skin. Avoid scratching. Trim your nails. If you can’t keep from scratching an itchy area, cover it with a dressing. Leave blisters alone. While your skin heals, stay out of the sun or use other sun protection measures.
- Soak in a soothing cool bath. Soak the affected area in cool water for 20 minutes. Sprinkle the water an oatmeal-based bath product (Aveeno).
- Protect your hands. Rinse and dry hands well and gently after washing. Use moisturizers throughout the day — on top of any medicated cream you’re using. And choose gloves based on what you’re protecting your hands from. For example, plastic gloves lined with cotton are good if your hands are often wet.
Photocontact dermatitis prognosis
Photocontact dermatitis gradually improves if the photoreactive agent is avoided. While photoallergic reactions can continue up to three weeks, phototoxic reactions often fade within a week.
- Photocontact dermatitis. https://dermnetnz.org/topics/photocontact-dermatitis[↩][↩][↩][↩]
- Greenspoon J, Ahluwalia R, Juma N, Rosen CF. Allergic and photoallergic contact dermatitis: a 10-year experience. Dermatitis. 2013 Jan-Feb;24(1):29-32. doi: 10.1097/DER.0b013e31827edc8b[↩][↩][↩]
- Monteiro AF, Rato M, Martins C. Drug-induced photosensitivity: Photoallergic and phototoxic reactions. Clin Dermatol. 2016 Sep-Oct;34(5):571-81. doi: 10.1016/j.clindermatol.2016.05.006[↩]
- Pratt ME, Pratt MD. Occupational photoallergic contact dermatitis to thiourea in a firefighter. SAGE Open Med Case Rep. 2021 Nov 12;9:2050313X211057931. doi: 10.1177/2050313X211057931[↩]
- Hu Y, Wang D, Shen Y, Tang H. Photopatch Testing in Chinese Patients Over 10 Years. Dermatitis. 2016 May-Jun;27(3):137-42. doi: 10.1097/DER.0000000000000170[↩][↩][↩]
- European Multicentre Photopatch Test Study (EMCPPTS) Taskforce. A European multicentre photopatch test study. Br J Dermatol. 2012 May;166(5):1002-9. doi: 10.1111/j.1365-2133.2012.10857.x[↩][↩]
- Yao FL, Chen H, Ma TN, et al. Report of 12 cases of acute phototoxic contact dermatitis caused by Psoralea (with light patch test) Chin J Dermatovenereol. 2000;14:410–411.[↩]
- Kerr A, Ferguson J. Photoallergic contact dermatitis. Photodermatol Photoimmunol Photomed. 2010 Apr;26(2):56-65. doi: 10.1111/j.1600-0781.2010.00494[↩]
- Deleo VA. Photocontact dermatitis. Dermatol Ther. 2004;17(4):279-88. doi: 10.1111/j.1396-0296.2004.04026.x[↩][↩]
- Janusz SC, Schwartz RA. Botanical Briefs: Phytophotodermatitis Is an Occupational and Recreational Dermatosis in the Limelight. Cutis. 2021 Apr;107(4):187-189. doi: 10.12788/cutis.0225[↩]
- Atwal SK, Chen A, Adler BL. Phototoxic Contact Dermatitis From Over-the-counter 8-Methoxypsoralen. Cutis. 2022 Feb;109(2):E2-E3. doi: 10.12788/cutis.0462[↩]
- Guenther J, Johnson H, Yu J, Adler BL. Photoallergic Contact Dermatitis: No Fun in the Sun. Cutis. 2022 Nov;110(5):241-267. doi: 10.12788/cutis.0651[↩][↩][↩]
- Rutter KJ, Farrar MD, Marjanovic EJ, Rhodes LE. Clinicophotobiological Characterization of Photoaggravated Atopic Dermatitis. JAMA Dermatol. 2022 Sep 1;158(9):1022-1030. doi: 10.1001/jamadermatol.2022.2823[↩]
- Lecha M. Idiopathic photodermatoses: clinical, diagnostic and therapeutic aspects. J Eur Acad Dermatol Venereol. 2001 Nov;15(6):499-504; quiz 504-5. doi: 10.1046/j.1468-3083.2001.00344.x[↩]
- Dickel, Heinrich. (2023). Management of contact dermatitis. Allergo Journal International. 32. DOI:10.1007/s40629-023-00246-9[↩]
- Flieger J, Raszewska-Famielec M, Radzikowska-Büchner E, Flieger W. Skin Protection by Carotenoid Pigments. Int J Mol Sci. 2024 Jan 24;25(3):1431. doi: 10.3390/ijms25031431[↩]
- Akat PB. Severe photosensitivity reaction induced by topical diclofenac. Indian J Pharmacol. 2013 Jul-Aug;45(4):408-9. doi: 10.4103/0253-7613.114999[↩]
- Ferguson, J., Kerr, A.C. (2018). Photoallergic Contact Dermatitis. In: John, S., Johansen, J., Rustemeyer, T., Elsner, P., Maibach, H. (eds) Kanerva’s Occupational Dermatology. Springer, Cham. https://doi.org/10.1007/978-3-319-40221-5_16-2[↩]
- Kerr A, Ferguson J. Photoallergic contact dermatitis. Photodermatol Photoimmunol Photomed. 2010 Apr;26(2):56-65. doi: 10.1111/j.1600-0781.2010.00494.x[↩]
- As¸kın Ö, Cesur SK, Engin B, et al. Photoallergic contact dermatitis. Curr Derm Rep. 2019;8:157-163.[↩][↩]
- Wilm A, Berneburg M. Photoallergy. J Dtsch Dermatol Ges. 2015 Jan;13(1):7-12; quiz 13. English, German. doi: 10.1111/ddg.12535[↩]
- Imai S, Atarashi K, Ikesue K, Akiyama K, Tokura Y. Establishment of murine model of allergic photocontact dermatitis to ketoprofen and characterization of pathogenic T cells. J Dermatol Sci. 2006 Feb;41(2):127-36. doi: 10.1016/j.jdermsci.2005.08.006[↩]
- Tokura Y, Yagi H, Satoh T, Takigawa M. Inhibitory effect of melanin pigment on sensitization and elicitation of murine contact photosensitivity: mechanism of low responsiveness in C57BL/10 background mice. J Invest Dermatol. 1993 Nov;101(5):673-8. doi: 10.1111/1523-1747.ep12371674[↩]
- Robert AbelJr. MD, in Integrative Medicine (Fourth Edition), 2018. https://doi.org/10.1016/B978-0-323-35868-2.00084-0[↩]
- Phototesting. https://dermnetnz.org/topics/phototesting[↩][↩][↩][↩][↩][↩][↩][↩]
- Geier J, Bauer A, Becker D, Brehler R, Breit R, Dickel H, Hofmann S, Kapp A, Lehmann P, Mahler V, Molin S. Empfehlungen der Arbeitsgruppe “Photopatchtest” der Deutschen Kontaktallergie-Gruppe (DKG) zur Durchführung des Photopatchtests. J Dtsch Dermatol Ges. 2018 Nov;16(11):1363-1364. doi: 10.1111/ddg.13683_g[↩]
- Gonçalo M. Photopatch testing. In: Johansen JD, Mahler V,
Lepoittevin JP, Frosch PJ, editors. Contact dermatitis.
Cham: Springer Nature;2021. pp. 593–608[↩] - Gonçalo, M. (2021). Photopatch Testing. In: Johansen, J.D., Mahler, V., Lepoittevin, JP., Frosch, P.J. (eds) Contact Dermatitis. Springer, Cham. https://doi.org/10.1007/978-3-030-36335-2_29[↩]





{kind=link}