Contents
- Allergic conjunctivitis
- Allergic conjunctivitis causes
- Allergic conjunctivitis signs and symptoms
- Allergic conjunctivitis diagnosis
- Allergic conjunctivitis treatment
- Table 1. Allergic conjunctivitis treatment options
- Eye drops for allergic conjunctivitis
- Antihistamine eye drops
- Mast cell stabilizers
- Antihistamine and mast cell stabilizer eye drops
- Dual-Acting Antihistamine–Mast Cell Stabilizing Agents
- Leukotriene Receptor Antagonists
- Topical Vasoconstrictors (Decongestants)
- Combination eye drops including decongestant (Antihistamine-Vasoconstrictor Combinations)
- Other eye drops, to prevent allergy symptoms
- Oral antihistamines (tablets and syrups)
- Topical nonsteroidal anti-inflammatory drugs (NSAIDS)
- Corticosteroids
- Topical Calcineurin inhibitors
- Biologicals
- Immunotherapy
- Surgery
- Allergic conjunctivitis home remedies
- Allergic conjunctivitis prognosis
Allergic conjunctivitis
Allergic conjunctivitis is caused by an allergic reaction, with the majority of cases (90–95%) attributed to seasonal (certain times of the year) allergic conjunctivitis or perennial (all year round) allergic conjunctivitis 1, 2. Allergic conjunctivitis is a common conjunctivitis that is caused by immunoglobulin E (IgE) immune responses affecting more than 40% of the general population and is estimated to occur in up to 30% of children, either alone or in association with allergic rhinitis 3, 4, 5, 6. Allergic conjunctivitis is a reaction of the outer lining of the eyeball (conjunctiva) to things in the environment to which a person is allergic (allergens). Dust, pollen, animal dander, and sometimes even medications can all be allergens. When your eyes are in contact with these allergens, the eyes get red, inflamed, watery, itchy or swollen eyelid 7, 8. Although these symptoms can look like the signs of an infection, allergic conjunctivitis is not an infection and is not contagious. However, these signs and symptoms can be sufficiently bothersome that people with allergic conjunctivitis often experience decreased work productivity, increased work or school absenteeism, limitation of everyday activities, and reduced quality of life 7.
Unlike conjunctivitis that is caused by bacterial or viral infection, allergic conjunctivitis is not contagious, so it cannot be transferred from one person to another.
Allergic conjunctivitis is often accompanied with other signs of hay fever. Allergic conjunctivitis signs can include an itchy, runny nose and sneezing or a history of other allergic conditions. The eyes are itchy and watery.
Allergic conjunctivitis other symptoms can include:
- redness behind the eyelid, spreading up the white of the eye
- swelling of the eye/s making them appear puffy
- excessive tears
- a discharge, yellow or green in color, causing crusting around the eyelids
- a dislike of bright lights (photophobia).
Allergic conjunctivitis symptoms may be:
- Perennial (all year round) due to constant exposure to dust mites, animal dander, indoor and outdoor mould spores and, in some cases, foods or food additives.
- Seasonal (certain times of the year) due to airborne allergens such as mould spores and pollen from grasses, trees, and weeds. The amount of airborne pollen varies from day to day and is dependent on the weather. People with pollen allergies often find their symptoms improve in wet weather and become worse on hot windy days or after thunderstorms.
If allergic conjunctivitis is suspected, allergy testing can help identify the allergen responsible, or “trigger”.
Avoiding or minimizing exposure to known allergens is an important first step in managing allergic conjunctivitis.
Allergic conjunctivitis may be helped by treatments used in conditions such as hay fever e.g. antihistamines. Cool compresses and lubricating eye drops may soothe the eyes.
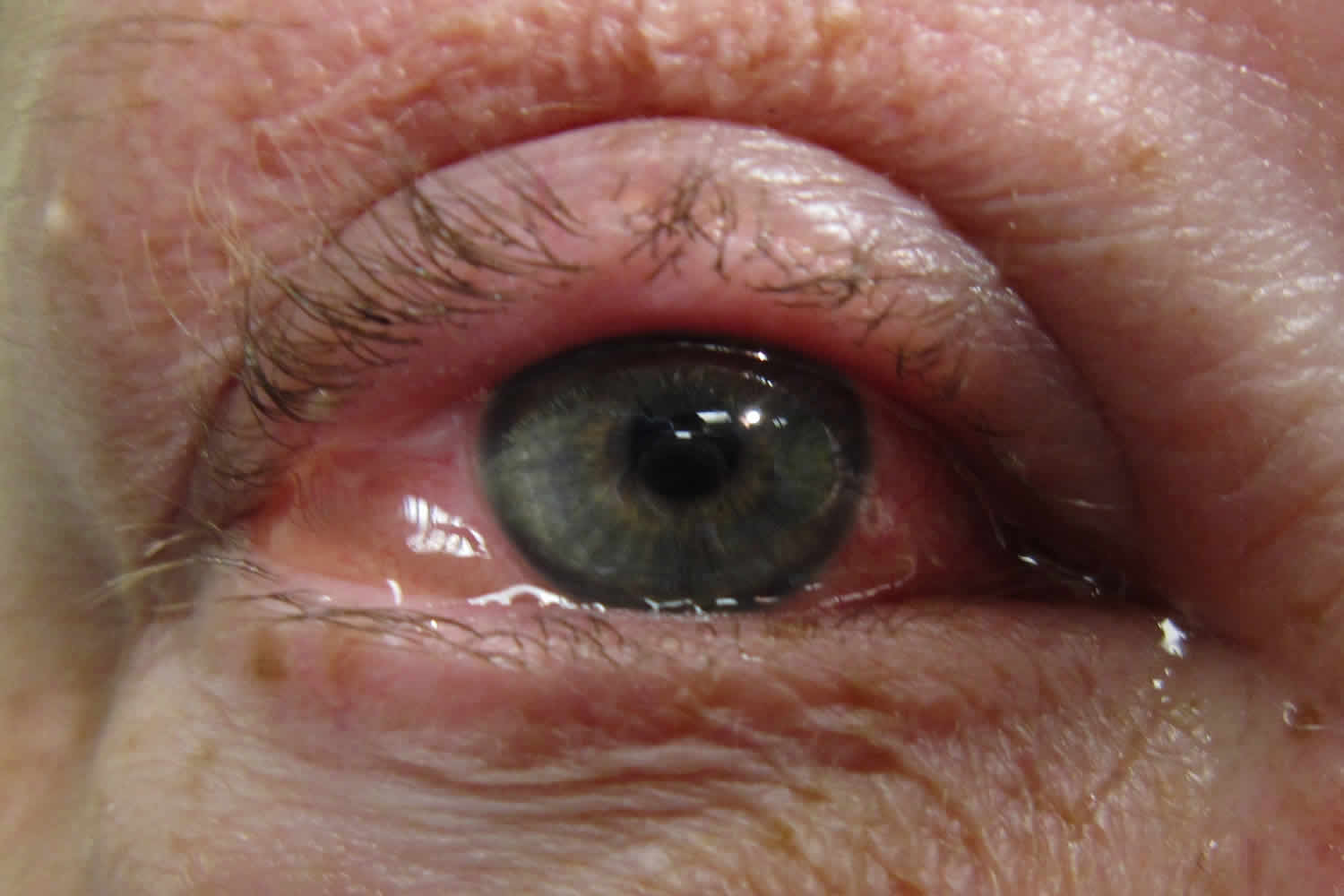
Figure 1. Allergic conjunctivitis
Allergic conjunctivitis causes
Allergic conjunctivitis is caused by contact with something to which a person may be sensitive or allergic to (allergens), air pollution, atopy, pollen exposure, inflammation, and pet hair 9. Examples of common allergens to the conjunctival surface include tree/grass pollen, house dust mites, animal/pest dander, and mold spores 9, 10. Spring, summer and fall allergies tend to be caused by trees weed, grass, and flower pollen. Some people can have allergies all year round due to other household allergens, including dust, mold and animal dander/hair/fur. Some children may have an underlying medical problem making them more at risk for an allergic eye condition.
Allergic conjunctivitis signs and symptoms
Allergic conjunctivitis symptoms may vary from person to person. Allergic conjunctivitis symptoms can be very mild or very severe. Itching is the most common symptom and eye allergy
is unlikely to be present if itching is not present. Other symptoms may include stinging, tearing, and burning. The conjunctiva is usually pink and/or bloodshot. The white area immediately around the colored part of the eyes can also swell, causing tiny bumps visible on the surface of the eye. Eyelid skin can also be affected, becoming thick, swollen, itchy, or red. Children may frequently rub or roll their eyes if they have allergies. They may even tightly squeeze or blink frequently to help with the itchiness. Symptoms are often worse in the spring and/or summer months, but may stick around throughout the year.
Typical signs and symptoms of allergic conjunctivitis include:
- Redness in both eyes.
- Itching and burning of both the eye and surrounding tissues.
- Watery discharge, often accompanied by acute discomfort in bright light (photophobia).
- Swollen eyelids which may become ‘heavy’ or ‘droopy’. In some severe cases, the eyelids are so swollen that they cannot completely open.
- Swollen conjunctiva which may look light purple and affect vision. Blurred vision or any change in the appearance of the cornea (clear part of the eye that covers the pupil) requires urgent referral to an eye specialist. Speak to your doctor or optometrist for a referral.
Allergic conjunctivitis diagnosis
A diagnosis of allergic conjunctivitis is made by history and examination. Although allergy testing may help pinpoint the specific allergens, it is usually not necessary since the types of allergens that usually cause conjunctivitis are very common, like grass, weed, and tree pollens. Eye drop treatments are the same no matter what allergen is causing the reaction.
If further investigation is needed, even if no identifiable allergens have been found, the second step is skin prick or patch tests 11. Patch tests are preferred in contact blepharoconjunctivitis, while skin prick tests are used in the other diseases 11. These tests are carried out with a standard battery of allergens and sometimes with others that are not normally tested but suspected as the cause of the allergy. If skin testing is indicated but not recommended (e.g., the patient is taking antihistaminic systemic medications), or if results are ambiguous (e.g., presence of dermatographism), or simply to complement the results of previous skin prick test, serum specific IgE measurements for the aeroallergens can be considered 12, 13.
In case of doubt after systemic allergy evaluation tests, a conjunctival allergen provocation test (CAPT) also known as conjunctival allergen challenge or ocular challenge test may be of use to identify the cause 13. In the conjunctival allergen provocation test (CAPT) an allergen is applied to the conjunctival mucosa to evaluate the patients’ immunoreactivity to the allergen. The conjunctival allergen provocation test (CAPT) is used to confirm which allergens the patient is sensitive to and has the same scientific background as other provocation tests used extensively in other mucosae such as nasal or digestive 13, 14. Non-specific or irritant challenges evaluate the hyperreactivity of the ocular mucosa, whilst direct mucosal challenges contain higher concentrations of the allergen encountered in environmental exposure and evaluate patients’ immunoreactivity to the allergen, following the guidelines for standard practice of the European Academy of Allergy and Clinical Immunology 13, 14, 15. A positive test will trigger the same signs and symptoms as those occurring when the allergen is encountered in real life, an IgE-mast cell-dependent immunoreactivity 16, 14. The conjunctival allergen provocation test (CAPT) is also useful to assess the relationship between symptoms and exposure in polysensitized patients and to assess response to therapy 12.
Allergic conjunctivitis treatment
Allergen avoidance is the first line of treatment for allergic conjunctivitis. In the case of pollen allergies, symptoms are often made worse by outdoor activities. Wearing glasses or goggles outdoors can limit contact with allergens. Minimization measures for house dust mites may include removing carpet, using dust mite covers for pillows and mattresses, and washing bedding in hot water are enough to reduce symptoms. Frequent washing of pillowcases and mattress covers as well as vacuuming the carpeting in your room help remove allergens from your surroundings. Regular washing your hair and face can help remove these allergens from the surface of your eyes, hair, and skin. Using artificial tear drops to rinse the eye and remove allergens from the eye can help with symptoms and help calm down the eye inflammation. These drops can provide even more relief when used cold (refrigerated) instead of at room temperature. It is also important to avoid rubbing the eyes, as this can make allergic conjunctivitis worse.
If you have allergic conjunctivitis, both prescription and over-the-counter allergy eye drops can treat allergic conjunctivitis 17. These may include medicines that help control allergic reactions, such as antihistamines and mast cell stabilizers. Or your doctor may recommend medicines to help control inflammation, such as decongestants, steroids and anti-inflammatory drops. Nonprescription versions of these medicines also may be effective. Most of the easily available allergy eye drops work best when used daily for at least a few weeks, and it may take up to a week to get full symptom relief. Some eye drops can be used only on an as needed basis. Allergy eye drops may work better for some than pill or liquid medications as eye drops do not cause any drowsiness or changes in appetite. However, pill or liquid medications may be more helpful if allergies cause a lot of eyelid swelling or affect more than just the eyes. Please speak with your ophthalmologist if you have questions about allergy medications.
Given the different types of over-the-counter eye drops, sometimes what works well for one person may not work as well for another person. You may need to try different types of eye drops before you find one that works for you. If there are still allergic conjunctivitis symptoms even after trying different kinds of allergy eye drops, adding a short-term liquid or pill allergy medication by mouth may help relieve symptoms. Pills and liquid medications by mouth may also a good treatment for people who don’t do well eye drops, or who have other allergy symptoms like a runny nose.
In some cases, steroid eye drops may be needed along with allergy eye drops if the allergic reaction is very severe. However, steroid use needs to be monitored closely by your ophthalmologist and used only as directed to prevent serious eye problems. Use of steroid drops for a long time or at a large amount can cause serious vision problems, including glaucoma, cataracts and eye infections (keratitis). Only ophthalmologists (eye specialists) who can monitor for side effects should prescribe steroids for allergic conjunctivitis. Talk with your ophthalmologist if you have questions about steroid drops.
Topical medications (eye drops) treat the symptoms of allergic conjunctivitis directly. Small drops of medication are delivered straight to the surface of the eye and are available in many different types.
- Antihistamine eye drops – effective but should not be used for longer than 6 weeks without medical advice.
- Antihistamine eye drops containing a vasoconstrictor (substances that cause the walls of blood vessels to narrow, or constrict) – minimize itch and remove redness by narrowing the swollen blood vessels in the eye. They should not be used for longer than 14 days without medical advice.
- Mast cell stabilizer eye drops – best used to prevent symptoms from occurring as they can take three to seven days to work. These can be used as long as necessary.
- Mast cell stabilizer eye drops with antihistamines – fast acting, effective and generally well tolerated.
- Steroid eye drops – effective in relieving symptoms quickly, but are associated with cataract formation, glaucoma and bacterial and viral infections of the cornea and conjunctiva. They should only be used under medical supervision as a short-term treatment and should never be used in the presence of herpes infections.
Antihistamine tablets or syrups help some people when it is difficult to avoid the allergen. Some side effects may include dryness of the eyes, nose, and mouth, and blurred vision. Antihistamines are usually contraindicated for people with glaucoma, advice should be sought from an eye specialist.
Allergen immunotherapy for specific allergens may benefit people with persistent, severe allergic conjunctivitis. However, relief of allergic conjunctivitis symptoms will not happen straight away.
Table 1. Allergic conjunctivitis treatment options
| Drug Class | Mechanism of Action | Target Symptom; Response Phase | Dosing Frequency |
|---|---|---|---|
| Antihistamines | Block histamine H1 receptors | Itching; acute action | 4 times daily |
| Vasoconstrictors (decongestants) | Activation of α-adrenergic receptors | Redness; acute action | 4 times daily |
| Mast cell stabilizers | Prevention of mast cell degranulation | Itching; early and late-phase responses | 2–6 times daily |
| Leukotriene receptor antagonists | Competitive binding to leukotriene receptors | Multiple allergic conjunctivitis signs and symptoms; late-phase responses | 1 time daily |
| Nonsteroidal anti-inflammatory drug (NSAIDs) | Prevention of prostaglandin production | Itching; late-phase response | 4 times daily |
| Corticosteroids | Broad anti-inflammatory action through prevention of proinflammatory mediator synthesis | Multiple allergic conjunctivitis signs and symptoms; early- and late-phase responses | 4 times daily |
| Single-agent antihistamine–mast cell stabilizers | Inverse histamine H1-receptor agonism plus prevention of mast cell degranulation | Itching; acute action and early- and late-phase responses | 1–2 times daily |
Eye drops for allergic conjunctivitis
When you have an allergic reaction your body releases histamine from mast cells, which leads to hay fever. Antihistamines block this reaction. Antihistamines act via histamine receptor antagonism to block the inflammatory effects of histamine and relieve any associated signs and symptoms. Most antihistamines used in the treatment of eye allergy are histamine-1 (H1) receptor antagonists, although some agents have affinity for other subtypes. Histamine-2 (H2) antagonists have been shown to modulate both cell growth and migration. Animal model studies have shown that antihistamines may even reduce infiltration of eosinophils and thus reduce the clinical aspects of the late-phase reaction 18.
First-generation antihistamines are well tolerated and associated with a favorable long-term safety record, but are associated with instillation pain, short duration of action, and limited potency 19. First-generation antihistamines remain available in over-the-counter products, particularly in combination with vasoconstrictors (substances that cause the walls of blood vessels to narrow, or constrict). While newer antihistamines are also H1 antagonists, they have a longer duration of action (4–6 hours) and are better tolerated than their predecessors 18.
Topical antihistamines are widely available without a prescription. Antihistamines competitively block histamine receptors (e.g., H1 or H4) on nerve endings and blood vessels of the mucosal surface, thereby reducing itchiness and conjunctival redness 20. First-generation antihistamines were associated with a range of systemic side effects (e.g., sedation, dizziness, cognitive impairment, blurred vision) caused by anticholinergic actions and nonspecific binding to histamine H2 receptors in addition to drying of the ocular surface. Newer oral, intranasal, and topical ocular antihistamines demonstrate improved H1 receptor selectivity, with fewer adverse effects; however, eye side effects, such as burning and dryness, remain a concern. Topical antihistamines (e.g., levocabastine, emedastine difumarate) are useful for providing rapid relief of allergic conjunctivitis symptoms, but their duration of action is limited; most topical antihistamines require dosing four times.
Antihistamine eye drops
Antihistamines are competitive antagonists of histamine receptors that are present in the conjunctiva and eyelids. Once stimulated, histamine receptors lead to capillary dilation and increased vascular permeability, which leads to common allergic symptoms of itching and edema. Therefore, antihistamines work by preventing the binding of histamine to histamine-1 (H1) receptors and preventing the cascade of inflammatory events. In the eye, only H1 receptors are available 21. Examples include azelastine (Eyezep Eye Drops), levocabastine (Livostin Eye Drops, Zyrtec Levocabastine Eye Drops) and emedastine.
Mast cell stabilizers
Mast cell stabilizers work by preventing the degranulation of sensitized mast cells, thus stopping the release of histamine and other inflammatory mediators 22, 23. Since mast cell stabilizers act before the mast cell is degranulated, they rarely have an impact on the inflammatory mediators once they are already released 24, 23. In other words, mast cell stabilizers are not effective once the patient is symptomatic, and clinical trials have had a difficult time showing their efficacy 24. Since there are other quicker and more effective treatment agents available on the market, mast cell stabilizers are rarely used as monotherapy. The most common mast cell stabilizers used for allergic conjunctivitis are sodium lodoxamide 0.1% (Alomide), cromoglycate 2%, and nedocromil 2% 22, 25. Mast cell stabilizers can be used as a prophylactic measure to prevent mast cell degranulation for repeated exposures to the allergen 26.
Antihistamine and mast cell stabilizer eye drops
When you have an allergic reaction your body releases histamine from mast cells, which leads to hay fever. Mast cell stabilizer medicines help reduce this histamine release after allergen exposure and reduce allergic reactions and hayfever 27. Topical mast cell stabilizers act to prevent mast cell degranulation and subsequent release of proinflammatory molecules triggered by IgE binding to sensitized conjunctival mast cells. Topical mast cell stabilizers (e.g., cromolyn sodium, lodoxamide tromethamine, nedocromil sodium, pemirolast potassium) effectively prevent activation of the early phase response by preventing release of histamine, cytokines, and other inflammatory and chemotactic mediators. Preventing the early phase response blocks downstream inflammation events, including production of prostaglandins and leukotrienes, eosinophil infiltration, chemokine and adhesion molecule expression, and chronic mast cell activation that perpetuate the late-phase response in allergic conjunctivitis. Most mast cell stabilizers require administration four to six times daily; nedocromil sodium can be given twice daily. Because of the required loading time for maximal efficacy of mast cell stabilizers, these medications are most effective when treatment is initiated before symptoms manifest; their effectiveness is limited when allergic conjunctivitis cascades have been activated and mast cell degranulation and histamine release have already occurred.
Dual-Acting Antihistamine–Mast Cell Stabilizing Agents
Agents with dual antihistamine and mast cell stabilizing actions are more suitable for extant allergic conjunctivitis than single-action medications because they block binding of free histamine to receptors and inhibit further release of proinflammatory mediators from mast cells. This dual action rapidly alleviates multiple signs and symptoms of allergic conjunctivitis in the short term and blocks the feed-forward cycle of persistent inflammation caused by continuous mast cell activation in the long term to promote regression of allergic conjunctivitis. Antihistamine–mast cell stabilizing agents (e.g., olopatadine, alcaftadine, epinastine, bepotastine besilate) are currently considered first-line therapeutics for allergic conjunctivitis because they offer acute symptomatic relief and control inflammation, and can be used chronically without long-term safety concerns. Most dual-acting agents require twice-daily dosing. Olopatadine 0.2% and alcaftadine are indicated for once-daily dosing and maintain effectiveness through 16 hours after administration in conjunctival allergen challenge studies 28, 29, 30.
Olopatadine 0.1% (Pataday Twice Daily Relief) was the first topical anti-allergy medication that was approved for twice-daily usage 22. These agents are all preserved with a surfactant called benzalkonium chloride that may cause ocular surface toxicity 31. These are now considered the first line of treatment for allergic eye disease and are the most common ophthalmic agents recommended by eye care practitioners and allergists 22. These agents can be used to prevent mast cell degranulation and acutely following the onset of symptoms 32.
Compared to placebo, olopatadine has been found to improve symptoms of eyelid swelling, eye redness, chemosis (a condition where the conjunctiva, or the outer surface of the eye, swells due to fluid build-up), itch, and overall quality of life. Multiple randomized control trials have compared ketotifen and olopatadine. One meta-analysis found improvement in symptoms of itching after 14 days in favor of olopatadine 0.1% when compared to ketotifen 0.025% 33. Before 2020, olopatadine was only available as a prescription medication, and ketotifen, in the form of Zaditor or Alaway, was clinically commonly prescribed as the first line of relief as an OTC medication. Within the last 4 years, olopatadine became available OTC and has gained popularity to become clinically superior to ketotifen in terms of efficacy.
Leukotriene Receptor Antagonists
Leukotriene receptor antagonists (e.g., montelukast), which are currently available for oral dosing, prevent leukotrienes from binding to their conjunctival receptors to decrease inflammatory signaling and improve multiple ocular symptoms of allergic conjunctivitis. Leukotriene receptor antagonists have a slower onset of action, are less effective than topical antihistamines, and are not used as first-line therapy or monotherapy for allergic conjunctivitis 20.
Topical Vasoconstrictors (Decongestants)
Topical vasoconstrictors (decongestants) were the first ocular medication approved for the treatment of allergic conjunctivitis. Over-the-counter (OTC) topical vasoconstrictors are effective at temporarily decreasing conjunctival hyperemia by stimulating alpha-adrenergic receptors 24. Alpha-adrenergic agonists cause vasoconstriction of conjunctival blood vessels, resulting in decongestion and whitening of the eye 34, 24. However, the use of these agonists can lead to side effects such as rebound hyperemia and tachyphylaxis and, chronically, can lead to conjunctivitis medicamentosa 26, 24. Commonly used topical vasoconstrictors are oxymetazoline, naphazoline, tetrahydrozoline, and phenylephrine. These are best utilized as short-term solutions and should be avoided in narrow-angle glaucoma and cardiovascular issues 34, 24. These should not be recommended as a standalone treatment and used in combination with antihistamines for the treatment of allergic conjunctivitis 34, 35.
Combination eye drops including decongestant (Antihistamine-Vasoconstrictor Combinations)
Some eye drops contain an antihistamine such as pheniramine or antazoline to stop itching, and a vasoconstrictor (substances that cause the walls of blood vessels to narrow, or constrict) such as naphazoline to take away redness through stimulation of vascular alpha-adrenergic receptors e.g. naphazoline + antazoline (Antistine-Privine, Albalon-A), pheniramine + naphazoline (Visine Allergy with Antihistamine, Naphcon-A). Vasoconstrictors are commonly available in nonprescription combination formulations that contain an antihistamine (e.g., naphazoline-antazoline, naphazoline-pheniramine). These formulations exhibit a rapid onset of action and relieve redness and itchiness associated with allergic conjunctivitis. However, they are not recommended for long-term use because of reduced effectiveness over time and a potential rebound effect that can produce persistent red eye on discontinuation 27. As with topical antihistamines, combination antihistamine–vasoconstrictor formulations have a relatively short duration of action and are administered four times daily 8, 17. Limit use of combination eye drops to no more than 5 to 7 days to avoid a ‘rebound’ redness from overuse.
Other eye drops, to prevent allergy symptoms
These eye drops prevent allergic reactions in the eyes and need to be used 4 to 6 times per day, depending on the ingredient, for the entire time you are exposed to triggers, such as during spring e.g. cromoglycate (Cromolux Eye Drops, Opticrom), lodoxamide (Lomide Eye Drops 0.1%)
Oral antihistamines (tablets and syrups)
There are two types of oral antihistamines: newer, less sedating antihistamines, which do not typically cause drowsiness and older sedating antihistamines that cause drowsiness.
Oral antihistamines are good for treating hay fever symptoms, especially if you have a lot of different symptoms. You can also take oral antihistamines in advance if you know you are going to be exposed to allergens or triggers
Newer, less-sedating antihistamines
Newer antihistamines may rarely cause drowsiness; do not drive or operate machinery if you are affected e.g. cetirizine (Zilarex, Zyrtec), desloratadine (Aerius), fexofenadine (Fexotabs, Telfast), loratadine (Claratyne, Lorano).
Cetirizine and loratadine are available as syrups for children; check correct doses for different age groups. Cetirizine is more likely to cause drowsiness than other less sedating antihistamines
Older, sedating antihistamines
Older sedating antihistamines can cause drowsiness, sometimes the next day; it is important you do not drive or operate machinery e.g. chlorpheniramine + pseudoephedrine (Demazin 6 Hour Relief Tablets), dexchlorpheniramine (Polaramine), loratadine + pseudoephedrine (Claratyne-D with Decongestant Repetabs), promethazine (Phenergan, Sandoz Fenezal)
Older antihistamines are not available without a prescription for children under 2 years old. Do not drink alcohol with antihistamines that make you drowsy
If you have other medical conditions, such as glaucoma, epilepsy or prostate problems, or you take antidepressants, check with your doctor before taking these medicines
Topical nonsteroidal anti-inflammatory drugs (NSAIDS)
Topical nonsteroidal anti-inflammatory drugs (NSAIDS) act by blocking the cyclooxygenase enzymes (COX-1 and COX-2) within the cyclooxygenase pathway, resulting in the inhibition of inflammatory mediators such as prostaglandins and leukotrienes 24, 23. These drugs have proven efficacy against conjunctival hyperemia, pruritus, pain, and irritation 24. Topical NSAID agents commonly associated with the relief of ocular allergy symptoms include ketorolac, diclofenac, indomethacin, and flurbiprofen 24, 23. Although ketorolac has been approved for treating allergic conjunctivitis, studies have indicated that it is less effective compared to topical antihistamine agents 24, 23, 36. Moreover, these agents can cause burning and stinging sensations upon instillation, so long-term compliance is an issue. Thus, NSAIDs may be used for temporary relief of itching and hyperemia compared to no treatment; however, they do not aid with symptoms of mucous discharge, chemosis (a condition where the conjunctiva, or the outer surface of the eye, swells due to fluid build-up), and corneal damage, so alternative methods should be considered 24, 23, 36, 37.
Corticosteroids
Corticosteroids prevent production of multiple classes of late-phase response mediators, including prostaglandins, leukotrienes, histamine, and some cytokines. The numerous points of intervention in the inflammatory cascade make glucocorticoids an effective pharmacologic therapy for allergic conjunctivitis, but long-term topical use can lead to serious adverse effects, including increased intraocular pressure and corneal abnormalities 27. Long-term systemic corticosteroid use increases the risk of posterior subcapsular cataract formation 38. For this reason, patients at risk (e.g., those with glaucoma or diabetic retinopathy) or patients who receive higher doses or longer treatment courses of corticosteroids should be monitored by an ophthalmologist.
Corticosteroids (e.g., loteprednol etabonate, given four times daily) are generally not used as primary therapy for allergic conjunctivitis unless there is persistent or moderate-to-severe inflammation that the eye doctor does not feel will respond sufficiently to antihistamine–mast cell stabilizer medications alone 8. When corticosteroids are prescribed, they typically are used for short durations in the early stages of allergic conjunctivitis or during flare-ups until allergic conjunctivitis can be controlled with safer medications such as antihistamines, mast cell stabilizers, or dual-acting, single-molecule antihistamine–mast cell stabilizer agents 39. Topical corticosteroids are important in severe cases of allergic eye disease to break the cycle of inflammation and can be discontinued once the condition is under control. Most cases of seasonal allergic conjunctivitis or perennial allergic conjunctivitis do not often require corticosteroid intervention. For patients who require long-term use of corticosteroids, close observation by an ophthalmologist is warranted.
Supratarsal steroids
Supratarsal steroids are required in patients with the severe palpebral form of the disease who are unresponsive to topical steroids or are non-compliant. The conjunctiva is everted, and injection is given in the supratarsal conjunctiva. An injection of 0.1 ml betamethasone 4 mg/mL, dexamethasone 4 mg/mL, or triamcinolone can be provided 40.
Topical Calcineurin inhibitors
The topical calcineurin inhibitors cyclosporine A and tacrolimus are very effective in the treatment of giant papillary conjunctivitis (GPC), atopic keratocongiuntivitis (AKC), and vernal keratoconjunctivitis (VKC) and may serve as steroid-sparing agents when these forms of chronic allergic conjunctivitis become steroid-dependent 41, 13.
Cyclosporine A (CsA) is also used worldwide for the treatment of dry eye. Suspensions of cyclosporine A may be prepared in pharmacies, although some countries also have commercialized forms 42. The concentrations of cyclosporine A in the different ophthalmic formulations range between 0.01% and 2% and therefore the administration varies between 1 and 6 times per day 15. Tacrolimus may also be prepared as suspension by pharmacies and exists as an ointment for dermatological purposes in most countries at a concentration of 0.03-0.1%. Recent research shows that tacrolimus may have similar if not superior effectivity than cyclosporine A for the treatment of vernal keratoconjunctivitis (VKC). Moreover, dermatologic ointment containing tacrolimus is effective for the treatment of lid eczema in atopic keratocongiuntivitis (AKC) 41, 13. Topical treatment with calcineurin inhibitors has side effects such as stinging/burning sensation and the possibility of molluscum contagiosum virus, papillomavirus, or herpesvirus infection, although there is evidence from studies on dry eye syndrome that treatment with cyclosporine A can be topically administered long term and without systemic absorption 13, 15, 43, 42. At present, tacrolimus is generally administered topically in cases that do not respond to cyclosporine A.1 Finally, in very severe cases, allergic conjunctivitis such as VKC and atopic keratocongiuntivitis (AKC) may require systemic immunosuppression that is usually achieved with cyclosporine A, tacrolimus, or mycophenolate mofetil 41, 13, 44.
Biologicals
In theory, biological treatments could have superior results because they block the underlying inflammation pathways by bonding with specific biological molecules to decrease conjunctival inflammation 45. A few trials have reported the systemic use of the biologicals omalizumab, indicated for severe asthma, and dupilumab, indicated for atopic dermatitis, in vernal keratoconjunctivitis (VKC) and atopic keratocongiuntivitis (AKC). Omalizumab shows generally good results, though it has not yet been approved for allergic conjunctivitis, while dupilumab may increase the risk of blepharoconjunctivitis, which is tacrolimus-responsive in patients with severe atopic disease or previous atopic keratocongiuntivitis (AKC) 41, 46, 47, 48. Benralizumab, mepolizumab, and reslizumab, which are anti IL-5 biologic agents have not been studied in the context of allergic conjunctivitis 12.
Insunakinra (EBI-005) is the first inmunophilin synthesized for topical ophthalmologic use. It is an antagonist of the IL-1 receptor and binds to it, blocking the rest of the pathway. It has been documented to diminish ocular surface symptoms such as itching, inflammation, and discomfort 49.
Another molecule called liftitegrast (Shire Pharmaceuticals) has both activity as an antagonist of the IL-1 receptor and as antagonist of the lymphocyte functional antigen-1 and has proven effective for treatment of ocular surface symptoms 50.
Immunotherapy
The goal of immunotherapy is to diminish the symptoms and signs of rhinitis and conjunctivitis triggered by known allergens and to prevent their recurrence. Allergen-specific immunotherapy may be considered in cases of failure of first line treatments, or as a modifier of the natural course of the disease 41, 51, 52. Changes involve downregulation of Th2 response and upregulation of regulatory T-cells 12. It is carried out by administering gradually increasing amounts of the allergen to induce an immunological tolerance. According to the European Academy of Allergy and Clinical Immunology guidelines, it is indicated in patients with a documented IgE-mediated hypersensitivity to airborne agents, with severe forms of rhinoconjunctivitis that affect their quality of life in spite of allergen avoidance and pharmacotherapy 53, 54, 55. Immunotherapy can also be applied in children, but because it requires a strict regimen of desensitization, it may be difficult to treat children below 6 years of age 56, 52. There are commercial forms of many recognized allergens and the allergist determines the allergen to be prescribed based on previous hypersensitivity tests. Desensitization consists of two phases, an induction phase that lasts 5-8 months and a maintenance phase that last 3-5 years 52, 55. The standard method of administering the antigen has been subcutaneous injection, but recently other less invasive methods have been developed, such as sublingual or epicutaneous administration, with good results 43, 52. Adherence to sublingual is deemed better because it does not involve injections but has not been studied as exhaustively as subcutaneous injection; more randomized controlled trials are needed. Other forms of immunotherapy such as intralymphatic administration or edible vaccines are still being studied 43, 55.
In isolated allergic conjunctivitis (IgE- and non-IgE-mediated), allergen immunotherapy may be considered on the same premise as in rhinoconjunctivitis. However, there is less evidence of its beneficial effects and a few studies have documented an improvement of the clinical symptoms in vernal keratoconjunctivitis (VKC) but not in atopic keratocongiuntivitis (AKC) 43, 57, 44, 55.
Surgery
In very recalcitrant cases of atopic keratocongiuntivitis (AKC) and vernal keratoconjunctivitis (VKC), eye surgery may be needed. Papillae resection, in some cases with grafting of autologous conjunctiva, amniotic membrane or mucous membrane are effective in the treatment of severe forms of vernal keratoconjunctivitis (VKC) with corneal ulcers 54, 58, 59. Plaque resection may be necessary for subepithelial deposits in vernal keratoconjunctivitis (VKC) 60, 61. In atopic keratocongiuntivitis (AKC), surgery may be needed for eyelid and conjunctival scarring.
Atopic disease and atopic keratocongiuntivitis (AKC) can be complicated by subcapsular cataracts and/or severe ocular surface disease that may require complex surgery such as superficial keratectomy, limbal transplantation, or keratoprosthesis implantation 62.
Allergic conjunctivitis home remedies
If your conjunctivitis is caused by allergies, stopping the source of the allergy is important. Allergic conjunctivitis will continue as long as you’re in contact with whatever is causing it. Allergic conjunctivitis is not contagious. You can still go to work or school with allergic conjunctivitis and no one else will catch it.
To reduce your symptoms of allergic conjunctivitis you can:
- Take allergy medicine or use allergy eye drops.
- Put a cool, damp washcloth over your eyes for a few minutes.
- Use over-the-counter lubricating eye drops (artificial tears).
Allergic conjunctivitis prognosis
Most people with allergic conjunctivitis the prognosis for allergic conjunctivitis is good 63, 9. However, visual impairment can occur related to certain types of severe eye allergies, too much eye rubbing, eye infections, corneal damage or steroid use. Additionally, the medications used to manage allergic conjunctivitis can be associated with the development of cataracts 9.
- Butrus S, Portela R. Ocular allergy: diagnosis and treatment. Ophthalmol Clin North Am. 2005 Dec;18(4):485-92, v. doi: 10.1016/j.ohc.2005.07.007[↩]
- Gomes PJ. Trends in prevalence and treatment of ocular allergy. Curr Opin Allergy Clin Immunol. 2014 Oct;14(5):451-6. doi: 10.1097/ACI.0000000000000100[↩]
- Leonardi A, Castegnaro A, Valerio AL, Lazzarini D. Epidemiology of allergic conjunctivitis: clinical appearance and treatment patterns in a population-based study. Curr Opin Allergy Clin Immunol. 2015 Oct;15(5):482-8. doi: 10.1097/ACI.0000000000000204[↩]
- What is allergic conjunctivitis? https://aapos.org/glossary/allergic-conjunctivitis[↩]
- Carr W, Schaeffer J, Donnenfeld E. Treating Allergic Conjunctivitis: A Once-daily Medication that Provides 24-hour Symptom Relief. Allergy & Rhinology. 2016;7(2). doi:10.2500/ar.2016.7.0158[↩][↩][↩]
- Singh K, Axelrod S, Bielory L. The epidemiology of ocular and nasal allergy in the United States, 1988-1994. J Allergy Clin Immunol. 2010 Oct;126(4):778-783.e6. doi: 10.1016/j.jaci.2010.06.050[↩]
- Chigbu D.I. The pathophysiology of ocular allergy: A review. Cont Lens Anterior Eye 32: 3–15; quiz 43–44, 2009.[↩][↩]
- Bielory L., Meltzer E.O., Nichols K.K.et al. An algorithm for the management of allergic conjunctivitis. Allergy Asthma Proc 34: 408–420, 2013.[↩][↩][↩]
- Baab S, Le PH, Gurnani B, et al. Allergic Conjunctivitis. [Updated 2024 Jan 26]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK448118[↩][↩][↩][↩]
- Wise S.K., Lin S.Y., Toskala E., Orlandi R.R., Akdis C.A., Alt J.A., Azar A., Baroody F.M., Bachert C., Canonica G.W., et al. International consensus statement on allergy and rhinology: Allergic rhinitis—2023. Int. Forum. Allergy Rhinol. 2023;13:293–859. doi: 10.1002/alr.23090[↩]
- Villegas BV, Benitez-Del-Castillo JM. Current Knowledge in Allergic Conjunctivitis. Turk J Ophthalmol. 2021 Feb 25;51(1):45-54. doi: 10.4274/tjo.galenos.2020.11456[↩][↩]
- Dupuis P, Prokopich CL, Hynes A, Kim H. A contemporary look at allergic conjunctivitis. Allergy Asthma Clin Immunol. 2020;16:5. doi: 10.1186/s13223-020-0403-9[↩][↩][↩][↩]
- Fauquert JL, Jedrzejczak-Czechowicz M, Rondon C, Calder V, Silva D, Kvenshagen BK, Callebaut I, Allegri P, Santos N, Doan S, Perez Formigo D, Chiambaretta F, Delgado L, Leonardi A Interest Group on Ocular Allergy (IGOA) from the European Academy of Allergy and Clinical Immunology. Conjunctival allergen provocation test : guidelines for daily practice. Allergy. 2016;72:43–54. doi: 10.1111/all.12986[↩][↩][↩][↩][↩][↩][↩][↩]
- Pepper AN, Ledford DK. Nasal and ocular challenges. J Allergy Clin Immunol. 2018;141:1570–1577. doi: 10.1016/j.jaci.2017.11.066[↩][↩][↩]
- Leonardi A, Bogacka E, Fauquert JL, Kowalski ML, Groblewska A, Jedrzejczak-Czechowicz M, Doan S, Marmouz F, Demoly P, Delgado L. Ocular allergy: recognizing and diagnosing hypersensitivity disorders of the ocular surface. Allergy. 2012;67:1327–1337. doi: 10.1111/all.12009[↩][↩][↩]
- Bilkhu PS, Wolffsohn JS, Naroo SA, Robertson L, Kennedy R. Effectiveness of nonpharmacologic treatments for acute seasonal allergic conjunctivitis. Ophthalmology. 2014;121:72–78. doi: 10.1016/j.ophtha.2013.08.007[↩]
- Azari AA, Barney NP. Conjunctivitis: a systematic review of diagnosis and treatment. JAMA. 2013 Oct 23;310(16):1721-9. doi: 10.1001/jama.2013.280318. Erratum in: JAMA. 2014 Jan 1;311(1):95. Dosage error in article text.[↩][↩]
- Leonardi A. Management of vernal keratoconjunctivitis. Ophthalmol Ther. (2013) 2:73–88. 10.1007/s40123-013-0019-y[↩][↩]
- Yanni JM, Sharif NA, Gamache DA, Miller ST, Weimer LK, Spellman JM. A current appreciation of sites for pharmacological intervention in allergic conjunctivitis: effects of new topical ocular drugs. Acta Ophthalmol Scand Suppl. (1999) 228:33–7. 10.1111/j.1600-0420.1999.tb01171.x[↩]
- Gane J, Buckley R. Leukotriene receptor antagonists in allergic eye disease: a systematic review and meta-analysis. J Allergy Clin Immunol Pract. 2013 Jan;1(1):65-74. doi: 10.1016/j.jaip.2012.07.001[↩][↩]
- Simons F.E., Simons K.J. Histamine and H1-antihistamines: Celebrating a century of progress. J. Allergy Clin. Immunol. 2011;128:1139–1150.e4. doi: 10.1016/j.jaci.2011.09.005[↩]
- Bielory L. Ocular allergy overview. Immunol. Allergy Clin. N. Am. 2008;28:1–23. doi: 10.1016/j.iac.2007.12.011[↩][↩][↩][↩]
- Sanchez-Hernandez M.C., Campo P., Benitez del Castillo J.M., Merayo-Lloves J., Montero J., Valero A., Antón E., Rondon C., Matheu V., Fernández-Parra B., et al. Consensus document on allergic conjunctivitis (DECA) J. Investig. Allergol. Clin. Immunol. 2015;25:94–106.[↩][↩][↩][↩][↩][↩]
- Abelson M.B., Shetty S., Korchak M., Butrus S.I., Smith L.M. Advances in pharmacotherapy for allergic conjunctivitis. Expert. Opin. Pharmacother. 2015;16:1219–1231. doi: 10.1517/14656566.2015.1040760[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Palmares J., Delgado L., Cidade M., Quadrado M.J., Filipe H.P. Allergic conjunctivitis: A national cross-sectional study of clinical characteristics and quality of life. Eur. J. Ophthalmol. 2010;20:257–264. doi: 10.1177/112067211002000201[↩]
- La Rosa M., Lionetti E., Reibaldi M., Russo A., Longo A., Leonardi S., Tomarchio S., Avitabile T., Reibaldi A. Allergic conjunctivitis: A comprehensive review of the literature. Ital. J. Pediatr. 2013;39:18. doi: 10.1186/1824-7288-39-18[↩][↩]
- Bielory B.P., O’Brien T.P., and Bielory L. Management of seasonal allergic conjunctivitis: Guide to therapy. Acta Ophthalmol 90: 399–407, 2012.[↩][↩][↩]
- Abelson M.B., and Gomes P.J. Olopatadine 0.2% ophthalmic solution: The first ophthalmic antiallergy agent with once-daily dosing. Expert Opin Drug Metab Toxicol 4: 453–461, 2008.[↩]
- Greiner JV, Edwards-Swanson K, Ingerman A. Evaluation of alcaftadine 0.25% ophthalmic solution in acute allergic conjunctivitis at 15 minutes and 16 hours after instillation versus placebo and olopatadine 0.1%. Clin Ophthalmol. 2011 Jan 13;5:87-93. doi: 10.2147/OPTH.S15379[↩]
- Ackerman S, D’Ambrosio F Jr, Greiner JV, Villanueva L, Ciolino JB, Hollander DA. A multicenter evaluation of the efficacy and duration of action of alcaftadine 0.25% and olopatadine 0.2% in the conjunctival allergen challenge model. J Asthma Allergy. 2013 Apr 8;6:43-52. doi: 10.2147/JAA.S38671[↩]
- Kari O., Saari K.M. Updates in the treatment of ocular allergies. J. Asthma Allergy. 2010;3:149–158. doi: 10.2147/JAA.S13705[↩]
- Berger W., Gomes P.J., Beck M., Kimura S., Westbrook T., Storms W., Galant S. Effects of adjuvant therapy with 0.1% olopatadine hydrochloride ophthalmic solution on quality of life in patients with allergic rhinitis using systemic or nasal therapy. Ann. Allergy Asthma Immunol. 2005;95:361–371. doi: 10.1016/S1081-1206(10)61155-6[↩]
- Kam K.W., Chen L.J., Wat N., Young A.L. Topical Olopatadine in the Treatment of Allergic Conjunctivitis: A Systematic Review and Meta-analysis. Ocul. Immunol. Inflamm. 2017;25:663–677. doi: 10.3109/09273948.2016.1158282[↩]
- Dordal M.T., Lluch-Bernal M., Sánchez M.C., Rondón C., Navarro A., Montoro J., Matheu V., Ibáñez M.D., Fernández-Parra B., Dávila I. Allergen-specific nasal provocation testing: Review by the rhinoconjunctivitis committee of the Spanish Society of Allergy and Clinical Immunology. J. Investig. Allergol. Clin. Immunol. 2011;21:1–12. quiz 12.[↩][↩][↩]
- Dupuis P., Prokopich C.L., Hynes A., Kim H. A contemporary look at allergic conjunctivitis. Allergy Asthma Clin. Immunol. 2020;16:5. doi: 10.1186/s13223-020-0403-9[↩]
- Mishra G.P., Tamboli V., Jwala J.K., Mitra A. Recent patents and emerging therapeutics in the treatment of allergic conjunctivitis. Recent Pat. Inflamm. Allergy Drug Discov. 2011;5:26–36. doi: 10.2174/187221311794474883[↩][↩]
- Swamy B.N., Chilov M., McClellan K., Petsoglou C. Topical non-steroidal anti-inflammatory drugs in allergic conjunctivitis: Meta-analysis of randomized trial data. Ophthalmic Epidemiol. 2007;14:311–319. doi: 10.1080/09286580701299411[↩]
- Carnahan MC, Goldstein DA. Ocular complications of topical, peri-ocular, and systemic corticosteroids. Curr Opin Ophthalmol. 2000 Dec;11(6):478-83. doi: 10.1097/00055735-200012000-00016[↩]
- O’Brien TP. Allergic conjunctivitis: an update on diagnosis and management. Curr Opin Allergy Clin Immunol. 2013 Oct;13(5):543-9. doi: 10.1097/ACI.0b013e328364ec3a[↩]
- Singh S, Pal V, Dhull CS. Supratarsal injection of corticosteroids in the treatment of refractory vernal keratoconjunctivitis. Indian J Ophthalmol. 2001 Dec;49(4):241-5.[↩]
- Patel N, Venkateswaran N, Wang Z, Galor A. Ocular involvement in atopic disease: a review. Curr Opin Ophthalmol. 2018;29:576–581. doi: 10.1097/ICU.0000000000000532[↩][↩][↩][↩][↩]
- Hoy SM. Ciclosporin Ophthalmic Emulsion 0.1%: A Review in Severe Dry Eye Disease. Drugs. 2017;77:1909–1916. doi: 10.1007/s40265-017-0834-x[↩][↩]
- Bielory L, Schoenberg D. Emerging therapeutics for ocular surface disease. Curr Allergy Asthma Rep. 2019;28:19–16. doi: 10.1007/s11882-019-0844-8[↩][↩][↩][↩]
- Bielory L, Schoenberg D. Ocular allergy: update on clinical trials. Curr Opin Allergy Clin Immunol. 2010;19:495–502. doi: 10.1097/ACI.0000000000000564[↩][↩]
- De Bosscher K, Haegeman G, Elewaut D. Targeting inflammation using selective glucocorticoid receptor modulators. Curr Opin Pharmacol. 2010;10:497–504. doi: 10.1016/j.coph.2010.04.007[↩]
- Bozkurt MK, Tülek B, Bozkurt B, Akyürek N, Öz M, Kiyici A. Comparison of the efficacy of prednisolone, montelukast, and omalizumab in an experimental allergic rhinitis model. Turk J Med Sci. 2014;44:439–447. doi: 10.3906/sag-1212-23[↩]
- van der Schaft J, Thijs JL, de Bruin-Weller MS, Balak DMW. Dupilumab after the 2017 approval for the treatment of atopic dermatitis: what’s new and what’s next? Curr Opin Allergy Clin Immunol. 2019;19:341–349. doi: 10.1097/ACI.0000000000000551[↩]
- Nahum Y, Mimouni M, Livny E, Bahar I, Hodak E, Leshem YA. Dupilumabinduced ocular surface disease (DIOSD) in patients with atopic dermatitis: clinical presentation, risk factors for development and outcomes of treatment with tacrolimus ointment. Br J Ophthalmol. 2020;104:776–779. doi: 10.1136/bjophthalmol-2019-315010[↩]
- Amparo F, Dastjerdi MH, Okanobo A, Ferrari G, Smaga L, Hamrah P, Jurkunas U, Schaumberg DA, Dana R. Topical interleukin 1 receptor antagonist for treatment of dry eye disease: a randomized clinical trial. JAMA Ophthalmol. 2013;131:715–723. doi: 10.1001/jamaophthalmol.2013.195[↩]
- Tauber J, Karpecki P, Latkany R, Luchs J, Martel J, Sall K, Raychaudhuri A, Smith V, Semba CP; OPUS-2 Investigators. Lifitegrast Ophthalmic Solution 5.0% versus Placebo for Treatment of Dry Eye Disease: Results of the Randomized Phase III OPUS-2 Study. Ophthalmology. 2015;122:2423–2431. doi: 10.1016/j.ophtha.2015.08.001[↩]
- Moote W, Kim H, Ellis AK. Allergen-specific immunotherapy. Allergy Asthma Clin Immunol. 2018;14(Suppl 2):53. doi: 10.1186/s13223-018-0282-5[↩]
- Calderon MA, Penagos M, Sheikh A, Canonica GW, Durham S. Sublingual immunotherapy for treating allergic conjunctivitis. Cochrane Database Syst Rev. 2011;7:CD007685. doi: 10.1002/14651858.CD007685.pub2[↩][↩][↩][↩]
- Roberts G, Pfaar O, Akdis CA, et al. EAACI Guidelines on Allergen Immunotherapy: Allergic rhinoconjunctivitis. Allergy. 2018;73:765–798. doi: 10.1111/all.13317[↩]
- Iyer G, Agarwal S, Srinivasan B. Outcomes and Rationale of Excision and Mucous Membrane Grafting in Palpebral Vernal Keratoconjunctivitis. Cornea. 2018;37:172–176. doi: 10.1097/ICO.0000000000001421[↩][↩]
- Bielory BP, Shah SP, O’Brien TP, Perez VL, Bielory L. Emerging therapeutics for ocular surface disease. Curr Opin Allergy Clin Immunol. 2016;16:477–486. doi: 10.1097/ACI.0000000000000309[↩][↩][↩][↩]
- Berger WE, Granet DB, Kabat AG. Diagnosis and management of allergic conjunctivitis in pediatric patients. Allergy Asthma Proc. 2017;38:16–27. doi: 10.2500/aap.2017.38.4003[↩]
- Addis H, Jeng BH. Vernal Keratoconjunctivitis. Clinical Ophthalmol. 2018;12:119–123. doi: 10.2147/OPTH.S129552[↩]
- Nishiwaki-Dantas MC, Dantas PE, Pezzutti S, Finzi S. Surgical resection of giant papillae and autologous conjunctival graft in patients with severe vernal keratoconjunctivitis and giant papillae. Ophthalmic Plast Reconstr Surg. 2000;16:438–442. doi: 10.1097/00002341-200011000-00007[↩]
- Guo P, Kheirkhah A, Zhou WW, Qin L, Shen XL. Surgical resection and amniotic membrane transplantation for treatment of refractory giant papillae in vernal keratoconjunctivitis. Cornea. 2013;32:816–820. doi: 10.1097/ICO.0b013e31826a1e53[↩]
- La Rosa M, Lionetti E, Reibaldi M, Russo A, Longo A, Leonardi S, Tomarchio S, Avitabile T, Reibaldi A. Allergic conjunctivitis: a comprehensive review of the literature. Ital J Pediatr. 2013;39:18. doi: 10.1186/1824-7288-39-18[↩]
- Irkeç MT, Orhan M, Erdener U. Role of tear inflammatory mediators in contact lens-associated giant papillary conjunctivitis in soft contact lens wearers. Ocul Immunol Inflamm. 1999;7:35–38. doi: 10.1076/ocii.7.1.35.8107[↩]
- Jabbehdari S, Starnes TW, Kurji KH, Eslani M, Cortina MS, Holland EJ, Djalilian AR. Management of advanced ocular surface disease in patients with severe atopic keratoconjunctivitis. Ocul Surf. 2019;17:303–309. doi: 10.1016/j.jtos.2018.12.002[↩]
- La Rosa M, Lionetti E, Reibaldi M, Russo A, Longo A, Leonardi S, Tomarchio S, Avitabile T, Reibaldi A. Allergic conjunctivitis: a comprehensive review of the literature. Ital J Pediatr. 2013 Mar 14;39:18. doi: 10.1186/1824-7288-39-18[↩]





{kind=link}