Contents
- Acute intermittent porphyria
- Acute intermittent porphyria cause
- Acute intermittent porphyria pathophysiology
- Acute intermittent porphyria types
- Acute intermittent porphyria signs and symptoms
- Acute intermittent porphyria complications
- Acute intermittent porphyria diagnosis
- Acute intermittent porphyria differential diagnosis
- Acute intermittent porphyria treatment
- Acute intermittent porphyria prognosis
Acute intermittent porphyria
Acute intermittent porphyria also called “AIP” or Swedish Porphyria is one of the acute porphyrias, which are a group of rare inherited metabolic disorders that involve defects in heme or ‘haem’ metabolism (a component of hemoglobin [Hb]) and result in excessive secretion of porphyrins and porphyrin precursors 1, 2, 3, 4, 5, 6, 7, 8, 9 , 10, 11. Heme or haem is a ring-shaped iron (Fe) containing molecule (organic compound containing an iron atom between the structure of the porphyrin ring) that commonly serves as a ligand of various proteins, more notably as a component of hemoglobin (the protein that carries oxygen in the blood), which is necessary to bind oxygen in the bloodstream and transport of oxygen in your body. Heme molecule also helps in respiration, detoxification of drugs, and other different biological functions. In hemoglobin, iron exists as ferrous (Fe2+) iron ion that is located at the center of the porphyrin ring, held in place by the four nitrogen atoms of the pyrrole rings (see Figures 1 to 3 below). Normally, your body makes heme (haem) in a multi-step process. Porphyrins are made during several steps of this process. People with porphyria are lacking certain enzymes needed for this process. This causes abnormal amounts of porphyrins or related chemicals to build up in the body. Porphyria occurs when the body cannot convert naturally occurring compounds called ‘porphyrins’ into heme. Porphyrins are substances that are required for the production of red blood cells. A common feature in all porphyrias is the accumulation in the body of porphyrins or porphyrin precursors. Although these are normal body chemicals, they normally do not accumulate. Precisely which of these chemicals builds up depends on the type of porphyria you have. There are 8 enzymes in the pathway for making heme and at least seven major forms of porphyria 12. The symptoms associated with the various forms of porphyria differ. It is important to note that people who have one type of porphyria do not develop any of the other types.
Porphyrias are generally classified into 2 groups: the “hepatic” (liver) and “erythropoietic” (red blood cell) types 12. Porphyrins and porphyrin precursors and related substances originate in excess amounts predominantly from the liver in the hepatic type porphyrias and mostly from the bone marrow in the erythropoietic type porphyrias. Porphyrias with skin manifestations are often referred to as “cutaneous porphyrias”. The term “acute porphyria” is used to describe porphyrias that can be associated with sudden attacks of pain and other neurological symptoms. The “hepatic” (liver) and “erythropoietic” (red blood cell) porphyrias can have cutaneous and acute symptoms, sometimes together. Most forms of porphyria are genetic inborn errors of metabolism.Acute intermittent porphyria (AIP) is an acute, hepatic or liver form of porphyria 12.
Acute intermittent porphyria (AIP) is caused by a deficiency in the enzyme porphobilinogen deaminase (PBGD) also known as hydroxymethylbilane synthase (HMBS). The porphobilinogen deaminase or hydroxymethylbilane synthase enzyme deficiency leads to a buildup of harmful substances called porphyrin precursors in your body, particularly in your liver. This enzyme deficiency is caused by a mutation in the HMBS gene which is inherited as an autosomal dominant trait (only one HMBS gene copy is affected). However, the enzyme deficiency by itself is not sufficient to produce symptoms of the disease and most individuals with a HMBS gene mutation do not develop symptoms of acute intermittent porphyria (AIP) 12. Additional factors such hormonal changes associated with puberty, the use of certain prescribed or recreational drugs, excess alcohol consumption, infections, and fasting or dietary changes are required to trigger the appearance of symptoms 12. Acute intermittent porphyria (AIP) symptoms include attacks of severe abdominal pain, constipation, a rapid heartbeat and increased blood pressure (tachycardia and hypertension), behavioral changes, seizures, and damage of the nerves to muscles (peripheral neuropathy) which can lead to complications like muscle weakness and paralysis. Moreover, unlike some other acute porphyrias, acute intermittent porphyria (AIP) does not manifest as sun sensitivity and skin rashes.
In Europe the prevalence of symptomatic acute intermittent porphyria (AIP) is reported to be 5.9 per million people in the general population 12. It is likely to be similar elsewhere in the world apart from Sweden where it is higher due to a founder effect. The founder effect is a type of genetic defect that occurs when a small group of individuals establishes a new population, leading to reduced genetic diversity compared to the original population 13. This can happen when a few individuals migrate from a larger population or when a population experiences a significant reduction in size. Over time, the resulting new subpopulation will have genetic and physical traits resembling the initial small, separated group, and these may be very different from the original larger population. Recent population based genetic studies have shown that approximately 1 in 2000 of the population inherit a disease causing (pathogenic) mutation in the HMBS gene. This suggests that only 1% of those who inherit the HMBS gene mutation will ever experience porphyria symptoms. Acute intermittent porphyria (AIP) can occur in individuals of all ethnic backgrounds, although it may be less frequently reported in African-American individuals. Women are affected by symptomatic acute intermittent porphyria (AIP) more often than men. The disorder is most common in young or middle-aged women. A study conducted in Sweden demonstrated an increased risk of schizophrenia or bipolar disorder in patients with acute intermittent porphyria (AIP), as well as in their relatives 14.
Clinical findings of an acute porphyria attack 2:
- Presence of otherwise unexplained severe, acute abdominal pain (without physical signs) in the vast majority (90%) of acute attacks 15. The pain, which occasionally may be more severe in the back or thighs, is usually only relieved with opiate analgesia. Atypical presentations are rare.
- During attacks nausea, vomiting, constipation, tachycardia, and hypertension are common.
- Muscle weakness, seizures, mental changes, and hyponatremia are features that alone or in combination increase the probability of acute porphyria.
- The urine may be reddish brown or red; however, this should not be used as a diagnostic criterion as it is not a constant finding, especially if the sample is fresh. The color is enhanced by exposure to air and light and reflects increased urinary concentrations of porphyrins and porphobilins formed from the porphyrin precursor porphobilinogen (PBG).
A diagnosis of acute intermittent porphyria (AIP) can be difficult because most symptoms are nonspecific and occur episodically. A diagnosis is usually based upon identification of characteristic symptoms from a detailed patient history, a thorough clinical evaluation and certain specialized tests. Acute intermittent porphyria (AIP) should be suspected in individuals with unexplained abdominal pain, especially repeated episodes and when occurring along with psychological symptoms, neurological findings with muscle weakness or unexplained hyponatraemia. Dark or reddish urine in such individuals is also suggestive of acute intermittent porphyria (AIP). However, absence of this feature does not exclude acute intermittent porphyria (AIP). The diagnosis of acute intermittent porphyria (AIP) can be confirmed by finding an elevated level of porphobilinogen (PBG) (> 6 mg/L) on a spot urine test during an acute attack 16. If the urinary concentration of porphobilinogen (PBG) is increased, molecular genetic testing is performed to confirm the diagnosis and/or to facilitate screening of family members. When a multigene panel or genomic testing has identified an HMBS gene mutation, the diagnosis of an intermittent porphyria (AIP) attack is confirmed when the urinary concentration of PBG is increased.
Acute intermittent porphyria (AIP) treatment is focused on preventing attacks by educating patients to avoid potential triggers (e.g, fasting, unsafe drugs). Acute attacks usually require hospital care and can be effectively treated with intravenous hematin.
Treatment options in acute intermittent porphyria (AIP) may include the following 16:
- Avoidance of precipitating factors (e.g, fasting, low caloric intake, high-risk porphyrogenic drugs, alcohol, infections and reproductive hormones change)
- High doses of glucose for mild attacks. Intravenous glucose (300 g/d in adults) is used in early acute attacks or when hemin is unavailable, but hemin infusion is more effective 17, 18.
- Hematin for severe attacks, especially those with severe neurologic symptoms. For sporadic acute neurovisceral attacks (i.e., when an individual has experienced one to ≤3 acute porphyria attacks in any 12-month period in the last two years): IV human hemin is the most effective treatment and may be lifesaving if employed early when neuronal damage is reversible. Hemin infusion rapidly downregulates delta-aminolevulinic acid synthase 1 (ALAS1) expression, decreases aminolevulinic acid (ALA) and porphobilinogen (PBG) accumulation, and resolves symptoms in 48–72 hour, although its effectiveness in preventing recurrent attacks is unclear 19, 20. If the criteria for recurrent attacks are met, Givlaari® (givosiran) should be considered, as long-term complications of hemin such as iron overload, phlebitis, and loss of venous access can be avoided. Alternative medical therapies to reduce frequency and/or severity of acute attacks when givosiran is not available include suppression of ovulation and prophylactic hemin infusion.
- During attacks, which generally last for several days, symptomatic treatment for pain and other manifestations (eg, tachycardia, nausea and vomiting, seizures)
- Gonadotropin-releasing hormone analogues for women with attacks related to their menstrual cycles
- Prophylactic hematin infusions
- Givosiran, in patients with acute hepatic porphyria, to decrease the rate of acute attacks 21
- Liver transplantation, as a last resort for patients with intractable recurrent attacks that are life-threatening or severely affect quality of life. Liver transplantation, as reported from several centers, is curative. Indications include repeated life-threatening acute porphyria attacks and poor quality of life when givosiran is not available or has shown insufficient medical efficacy.
Figure 1. Porphyrin molecular structure
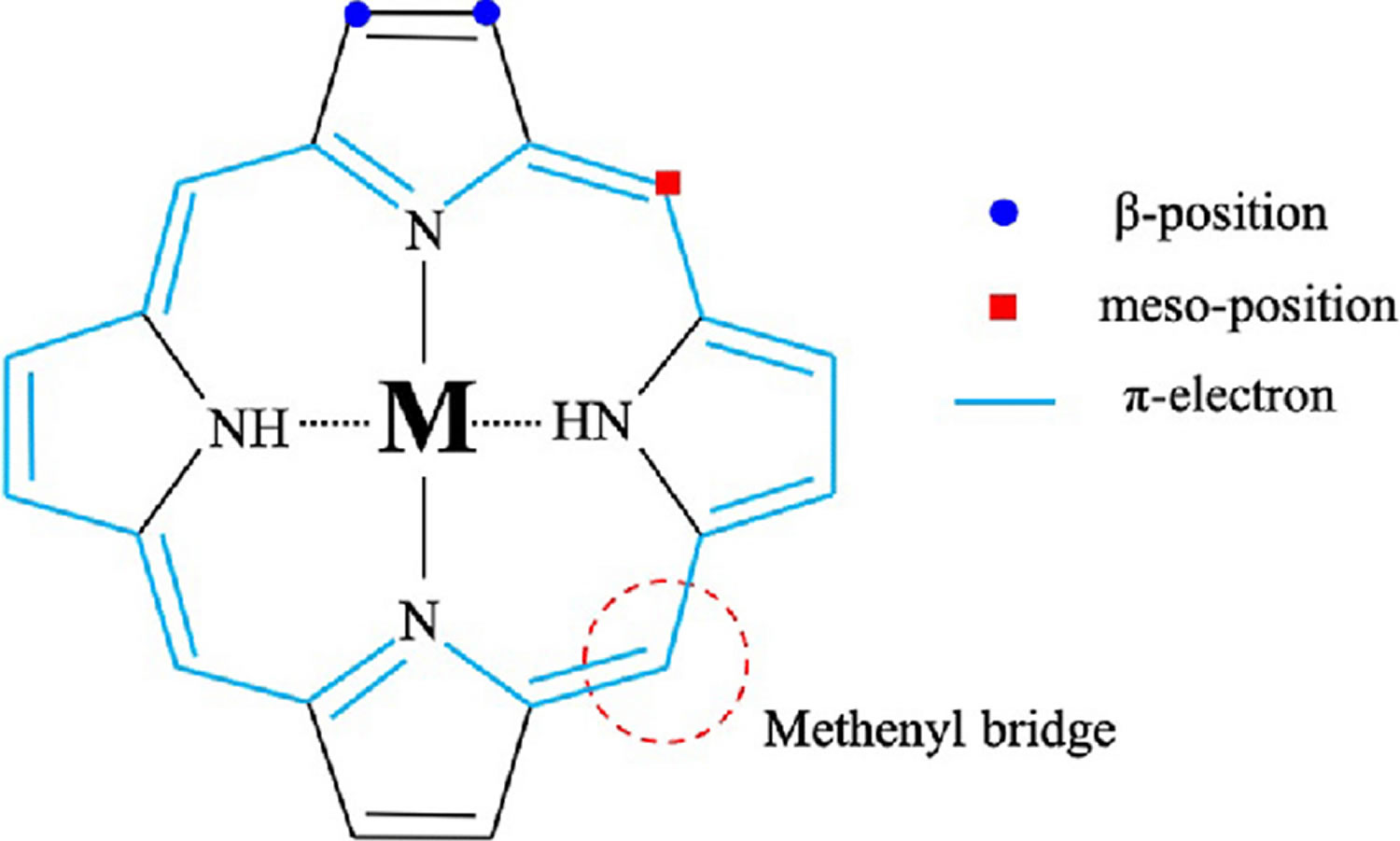
Footnote: Molecular structure of porphyrin (M represent metal ions, such as Mg, Cu, Fe, Zn, etc.).
[Source 22 ]Figure 2. Hemoglobin molecular structure
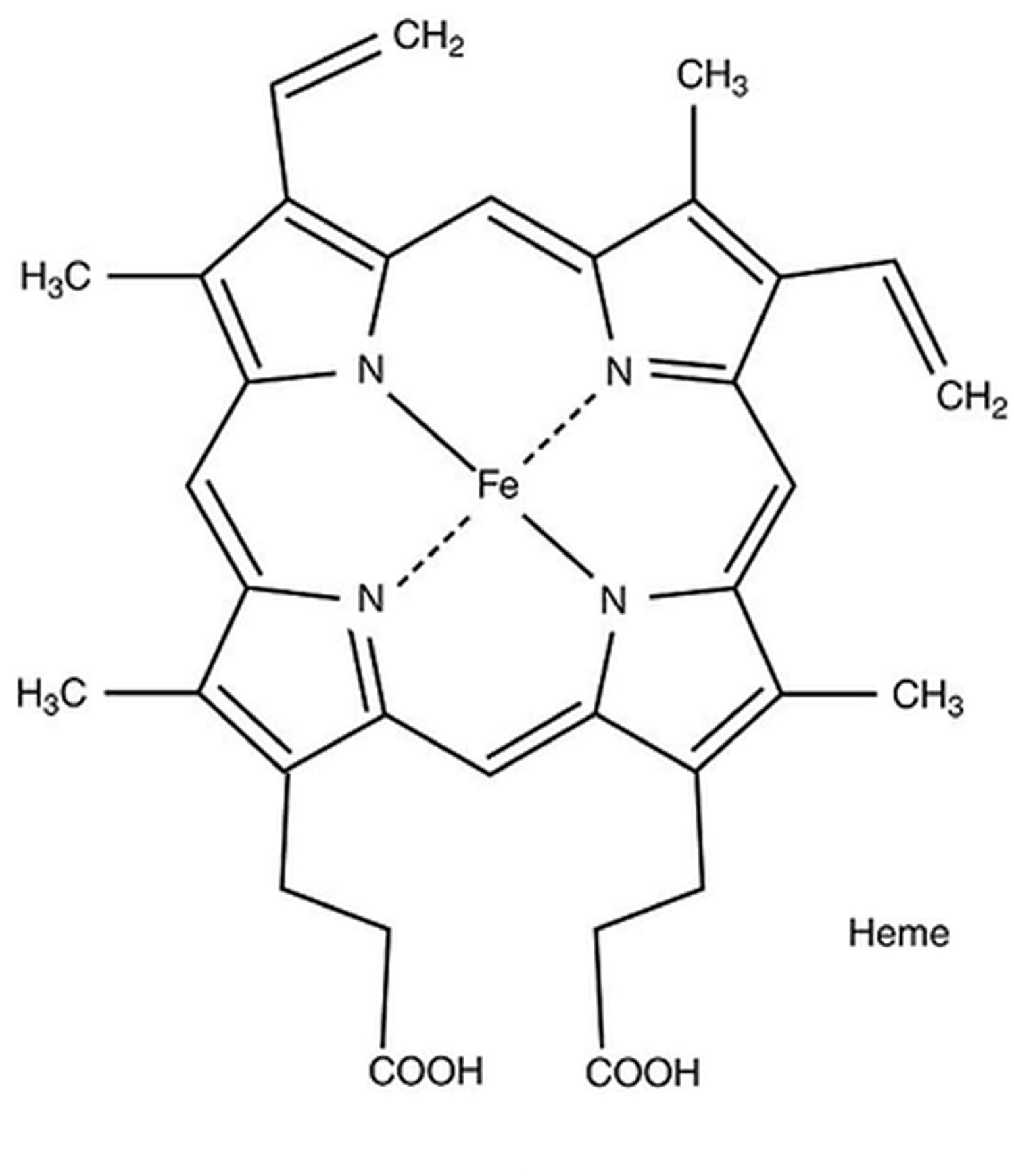
Figure 3. Heme (haem) molecular structure
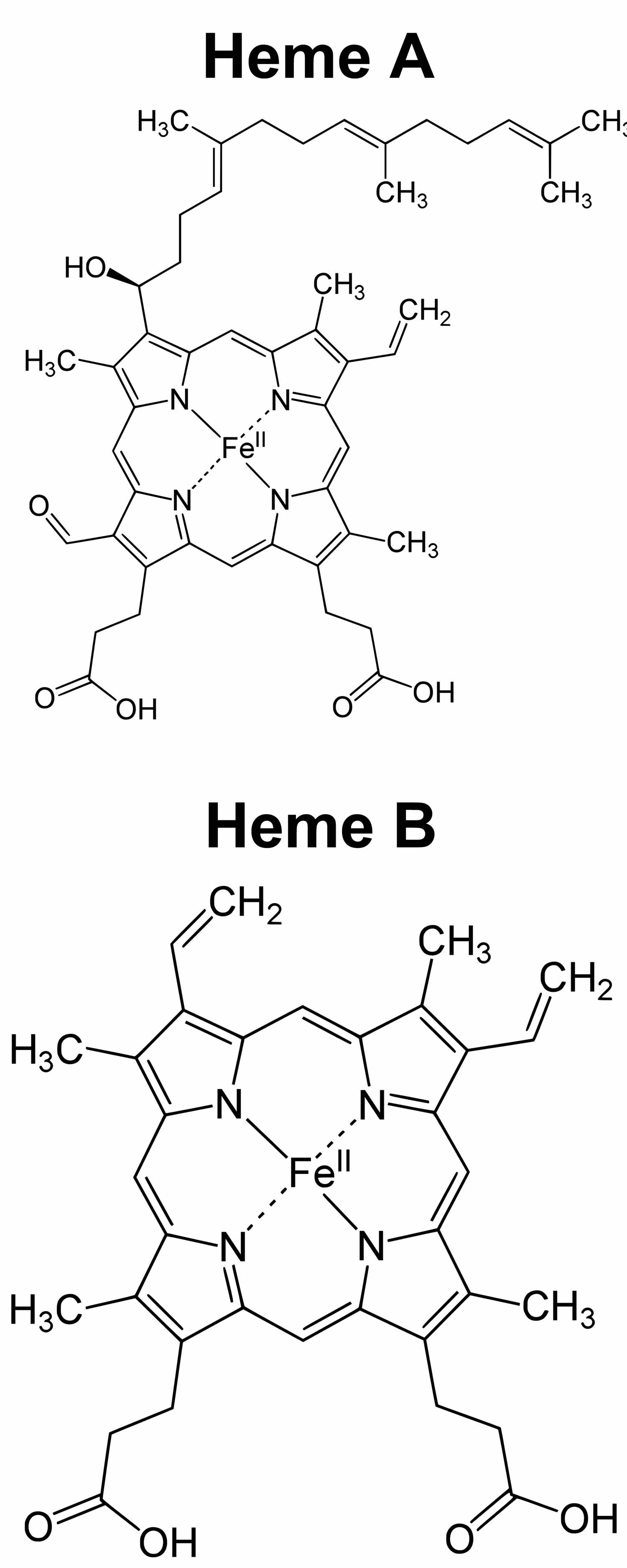
Footnote: Heme A and heme B molecular structures
[Source 24 ]Figure 4. Heme biosynthesis pathway
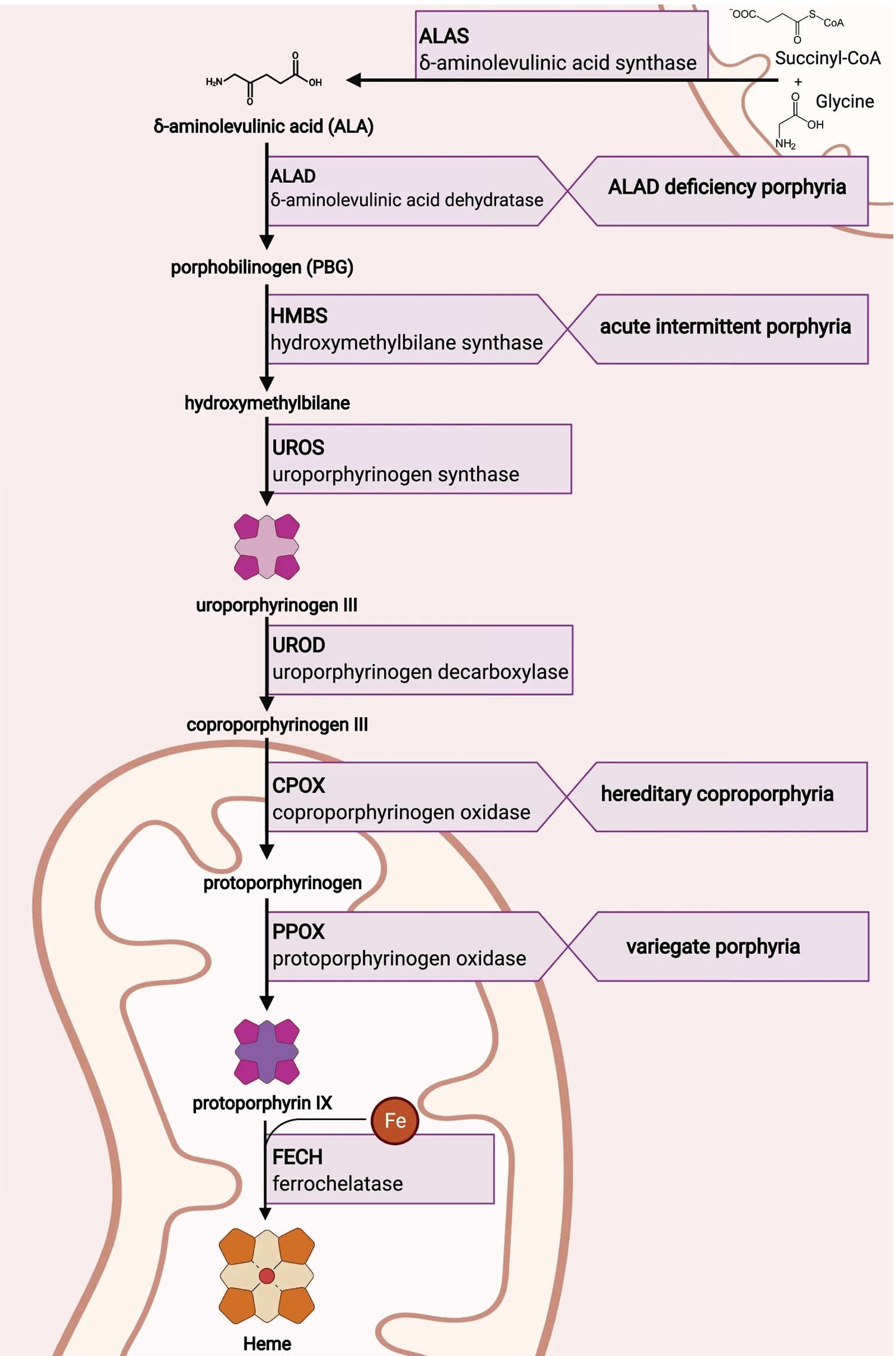
Figure 5. Acute intermittent porphyria attack triggers
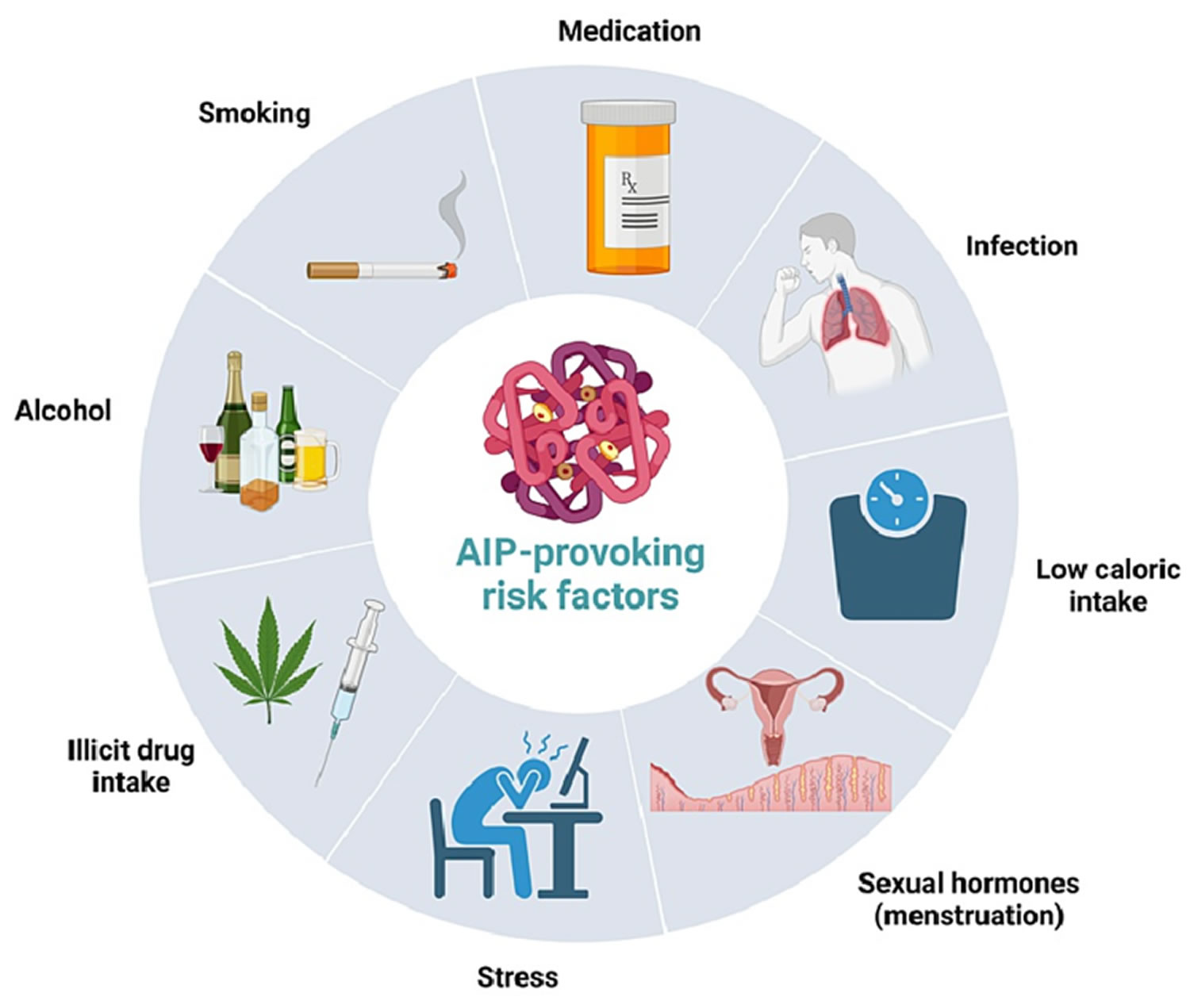
Figure 6. Acute intermittent porphyria signs and symptoms
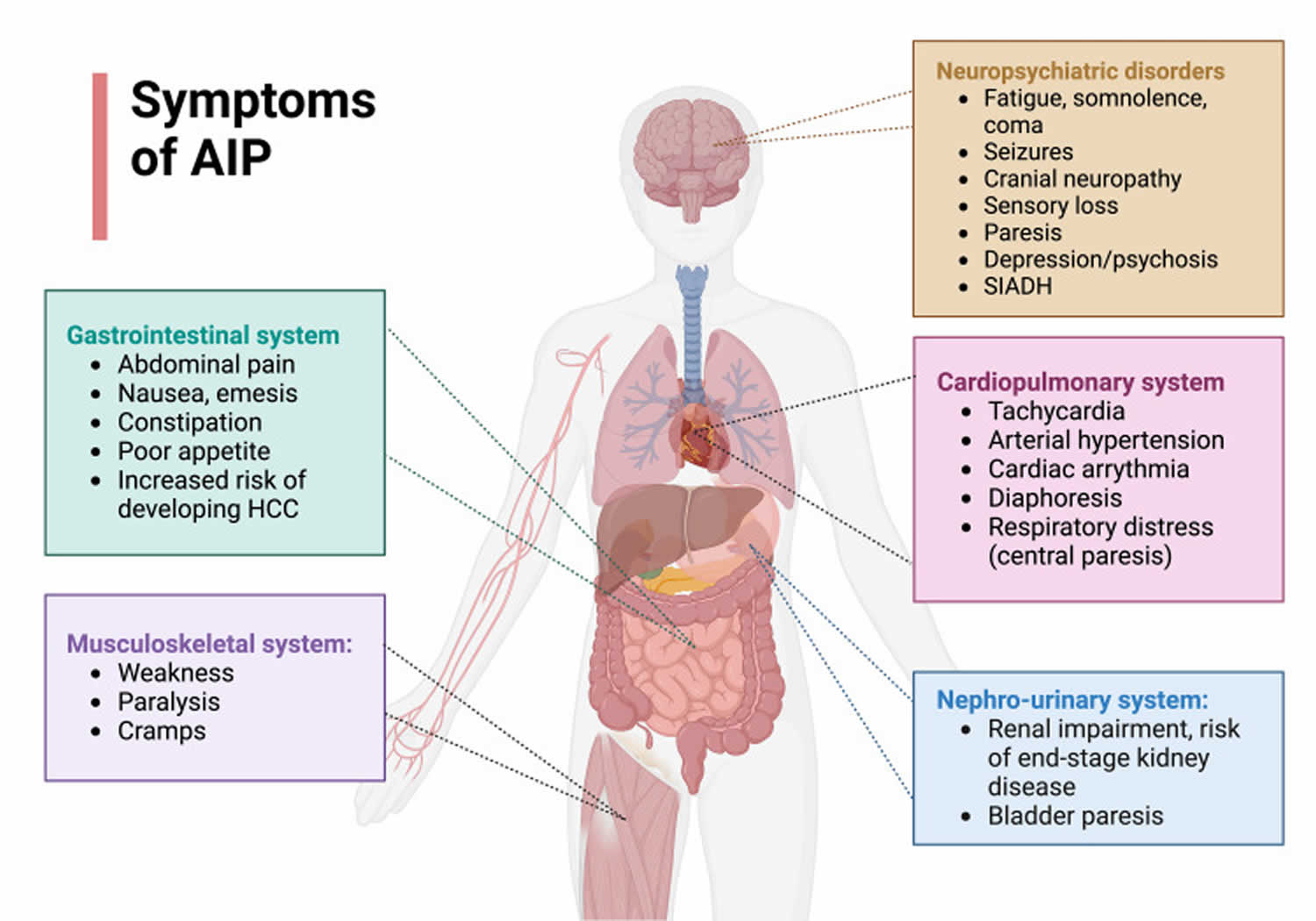
Abbreviations: AIP = acute intermittent porphyria; HCC = hepatocellular carcinoma; SIADH = syndrome of inappropriate antidiuretic hormone secretion
[Source 27 ]Acute intermittent porphyria cause
Acute intermittent porphyria (AIP) is a multifactorial disorder, which means that several different factors such as genetic and environmental factors occurring in combination are necessary for developing symptoms of the disorder 12. Individuals with acute intermittent porphyria (AIP) have a mutation in the HMBS gene located on the 11q24.1-q24.2 chromosome 28, 1. There are more than 500 mutations of the HMBS gene have been identified in the worldwide 8, 29. The HMBS gene provides instructions for making an enzyme known as hydroxymethylbilane synthase (HMBS) also known as porphobilinogen deaminase (PBGD) 30. The porphobilinogen deaminase (PBGD) or hydroxymethylbilane synthase (HMBS) enzyme is involved in the production of a molecule called heme. Heme is vital for all of your body’s organs, although it is most abundant in your blood, bone marrow, and liver. Heme is an essential component of iron-containing proteins called hemoproteins, including hemoglobin (the protein that carries oxygen in the blood). The production of heme is a multi-step process that requires 8 different enzymes. Hydroxymethylbilane synthase (porphobilinogen deaminase) is responsible for the third step in this process, which combines four molecules of porphobilinogen (the product of the second step) to form a compound called hydroxymethylbilane. In subsequent steps, five other enzymes produce and modify compounds that ultimately lead to heme.
Mutations in the HMBS gene lead to deficient levels of hydroxymethylbilane synthase (HMBS) or porphobilinogen deaminase (PBGD) in your body, which in turn can lead to the accumulation and release of porphyrin precursors, delta-aminolevulinic acid (ALA) and porphobilinogen (PBG) from the liver 31, 17.
However, the majority of people with a mutation in this gene do not develop symptoms of acute intermittent porphyria (AIP). Additional endogenous or exogenous factors, often called “triggers” are also required to cause symptomatic acute porphyria 12. These factors are not necessarily the same for each individual, and susceptibility to specific triggers may vary during a patient’s lifetime. Most of these triggers are believed to stimulate increased heme production (synthesis) in the liver and they include certain porphyrinogenic drugs, alcohol consumption, fasting or dieting (e.g. caloric restriction or low caloric intake), stress, infections or certain hormonal (endocrine) factors, female sex hormones, often in combination 12.
Acute intermittent porphyria is a low-penetrant genetic metabolic disease with penetrance considered to be around 10% to 20% 32. The penetrance of acute intermittent porphyria (AIP) in the general population has been estimated to be less than 1% 33. Manifest acute intermittent porphyria (MAIP) is considered when carriers develop typical acute neurovisceral attacks with an elevation of porphyrin precursors. In the absence of clinical episodes, it is referred to as latent acute intermittent porphyria (LAIP). Although higher penetrance has links to specific mutations, the overall genetic susceptibility factors underlying penetrance remain unknown.
Acute intermittent porphyria affects women to a greater degree than men, with a ratio of between 1.5 and 2 to 1. Attacks are rare before puberty. The typical age for the appearance of symptoms is between 18 to 40 years.
Symptomatic acute intermittent porphyria (AIP) is always accompanied by increased production and excretion of porphyrin precursors. However, for reasons that are unknown, some affected individuals have elevated porphyrin precursors without symptoms of acute intermittent porphyria (AIP). As discussed above, triggering factors are required for symptom development. The exact, underlying reasons why symptoms develop in some individuals with acute intermittent porphyria (AIP) are not fully understood. There are several theories as to the underlying pathogenesis of acute intermittent porphyria (AIP). One theory states that a specific porphyrin precursor (most likely 5-aminolevulinic acid [ALA]) is a neurotoxin that damages nerve tissue 12. This theory is supported by the information obtained from patients who have had liver transplant, which corrects both the clinical and biochemical features of the condition 12. A second theory suggests that heme deficiency in nerve cells (neurons) contributes to the development of symptoms 12. More research is necessary to determine the exact underlying mechanisms that are involved in the development of symptomatic episodes in individuals with acute intermittent porphyria (AIP).
Acute intermittent porphyria inheritance pattern
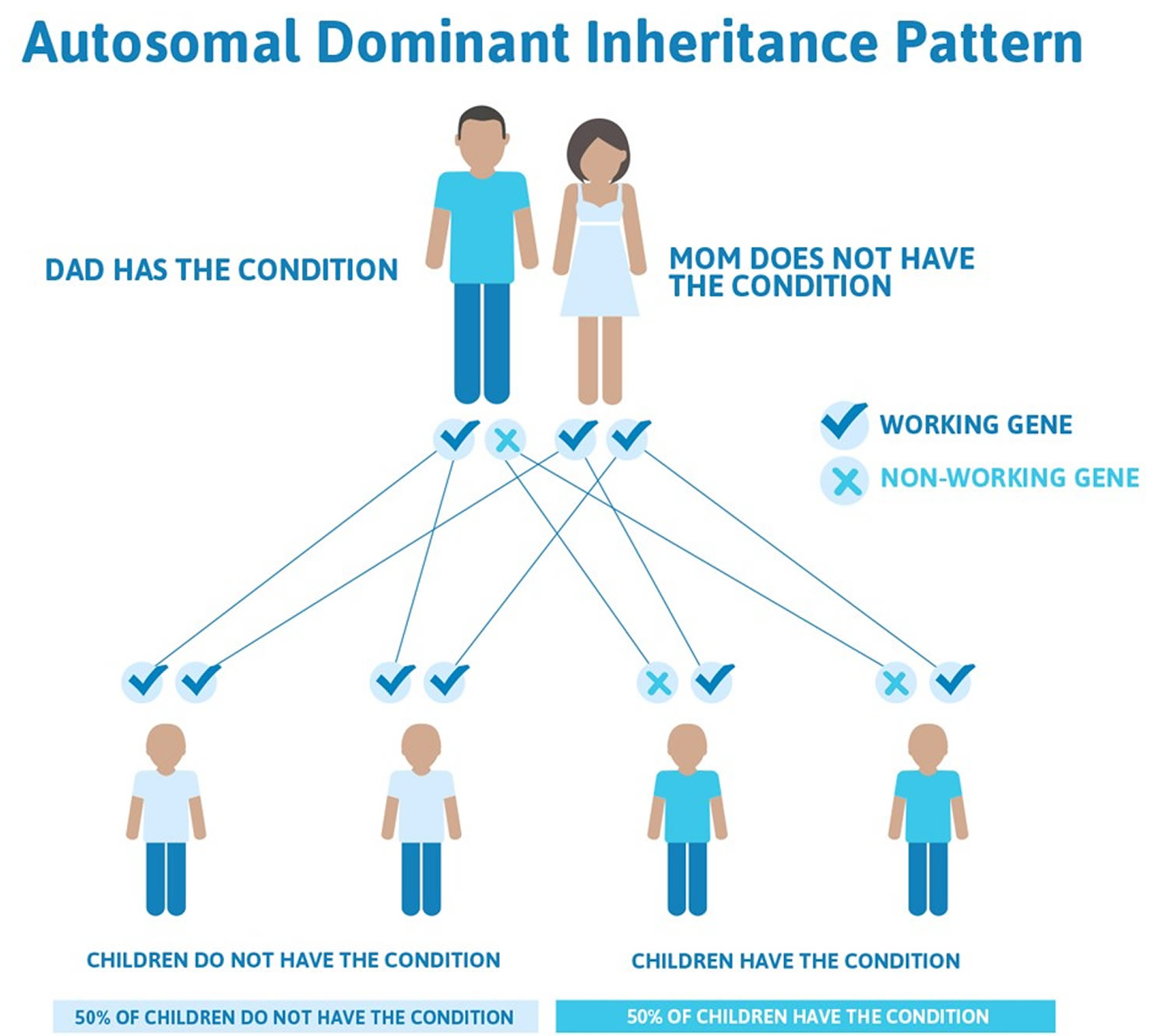
The HMBS gene mutation that predisposes individuals to developing acute intermittent porphyria (AIP) is inherited in an autosomal dominant pattern. Genetic diseases are determined by the combination of genes for a particular trait that are on the chromosomes received from the father and the mother. Dominant genetic disorders occur when only a single copy of an abnormal gene is sufficient for the appearance of the disease. The abnormal gene can be inherited from either parent, or can be the result of a new mutation (gene change) in the affected individual. The risk of passing the abnormal gene from affected parent to offspring is 50% for each pregnancy. The risk is the same for males and females.
People with specific questions about genetic risks or genetic testing for themselves or family members should speak with a genetics professional.
Resources for locating a genetics professional in your community are available online:
- The National Society of Genetic Counselors (https://www.findageneticcounselor.com/) offers a searchable directory of genetic counselors in the United States and Canada. You can search by location, name, area of practice/specialization, and/or ZIP Code.
- The American Board of Genetic Counseling (https://abgc.learningbuilder.com/Search/Public/MemberRole/Verification) provides a searchable directory of certified genetic counselors worldwide. You can search by practice area, name, organization, or location.
- The Canadian Association of Genetic Counselors (https://www.cagc-accg.ca/index.php?page=225) has a searchable directory of genetic counselors in Canada. You can search by name, distance from an address, province, or services.
- The American College of Medical Genetics and Genomics (https://clinics.acmg.net/) has a searchable database of medical genetics clinic services in the United States.
Figure 7. Acute intermittent porphyria autosomal dominant inheritance pattern
Acute intermittent porphyria pathophysiology
Acute intermittent porphyria (AIP) results from defects in the enzyme porphobilinogen deaminase (PBGD) also known as hydroxymethylbilane synthase (HMBS), which catalyzes the conversion of porphobilinogen (PBG) to hydroxymethylbilane. Impaired function of porphobilinogen deaminase (PBGD) leads to the accumulation of the porphyrin precursors porphobilinogen (PBG) and amino-levulinic acid (ALA). The predominant clinical problem appears to be neurologic damage that leads to peripheral and autonomic neuropathies and psychiatric manifestations 34.
Although levels of porphobilinogen (PBG) and amino-levulinic acid (ALA) are always elevated during acute attacks, how this leads to symptomatic acute intermittent porphyria is still unclear because most patients with the HMBS genetic defect have excessive porphyrin secretion but no symptoms.
In patients with acute intermittent porphyria (AIP), the function of porphobilinogen deaminase (PBGD) is only 40-60% of normal 1. With the advent of molecular technique, it has become clear that carriage of the HMBS genetic defect is much more common than symptomatic acute intermittent porphyria (AIP) 1. On average, out of 100 patients with the HMBS genetic defect, perhaps 10-20 secrete excess porphyrin precursors and only 1 to 2 have symptoms 1.
In acute intermittent porphyria (AIP), the neurologic damage occurs due to the accumulation of the porphyrin precursors, porphobilinogen (PBG) and aminolevulinic acid (ALA). The acute intermittent porphyria (AIP)-associated neurological damage manifests as peripheral and autonomic neuropathies and psychiatric manifestations.
A 2017 case-control study in 50 patients reported the association of acute intermittent porphyria (AIP) with systemic inflammation. Storjord et al. 35 found that the levels of insulin, C-peptide, prealbumin, and markers of kidney function, were decreased in symptomatic patients only, but not in asymptomatic ones. They postulated that in symptomatic patients of acute intermittent porphyria (AIP), the decrease in C-peptide levels in symptomatic acute intermittent porphyria (AIP) cases indicates that reduced insulin release is associated with enhanced disease activity and compromised kidney function 35.
Acute intermittent porphyria types
There 5 types of acute intermittent porphyria (AIP), caused by a heterozygous HMBS gene mutation and are based on the urine porphobilinogen (PBG)-to-creatinine ratio and occurrence of acute attacks 2, 36:
- Active (symptomatic) acute intermittent porphyria: An individual who has experienced at least one acute attack within the last two years.
- Sporadic AIP: 1-3 acute porphyria attacks in any 12-month period within the last 2 years
- Recurrent AIP: ≥4 acute porphyria attacks in a maximum period of 12 months within the last 2 years
- Symptomatic high excreter: Urine porphobilinogen (PBG)-to-creatinine ratio ≥4 times upper limit of normal (ULN) and no acute attacks in the last 2 years but has chronic long-standing manifestations of acute porphyria (e.g., pain or other porphyria-related manifestations in the absence of other likely explanations).
- Asymptomatic high excreter: Urine porphobilinogen (PBG)-to-creatinine ratio ≥4 times upper limit of normal (ULN) and no acute attacks in the last 2 years and no porphyria-related manifestations.
- Asymptomatic acute intermittent porphyria: Urine porphobilinogen (PBG)-to-creatinine ratio <4 times upper limit of normal (ULN) and no acute attacks in the last 2 years but has had ≥1 acute attack in the past.
- Latent (inactive) acute intermittent porphyria: Urine porphobilinogen (PBG)-to-creatinine ratio <4 times upper limit of normal (ULN) and no acute porphyria-related manifestations to date.
- Latent at-risk individual: An asymptomatic individual with a positive family history of acute intermittent porphyria (AIP) in whom an HMBS pathogenic variant was identified during screening of family members
- Latent low-risk individual: An asymptomatic individual with no known family history of acute intermittent porphyria (AIP) in whom the identification of an HMBS pathogenic variant was an incidental finding (the identification of a pathogenic variant in a gene that does not account for the phenotype that prompted the diagnostic testing).
Active (Symptomatic) acute intermittent porphyria
Active symptomatic acute intermittent porphyria, which are more common in women than men, are very rare before puberty 2. Onset typically occurs in the second or third decade 37.
The visceral, peripheral, autonomic, and/or central nervous systems (brain and spinal cord) may be affected, leading to a range of findings that are usually intermittent and sometimes life-threatening 2. The course of acute porphyria attacks is highly variable in an individual and between individuals 2.
Affected individuals may recover from acute porphyria attacks within days, but recovery from severe attacks that are not promptly recognized and treated may take weeks or months 2. Although attacks in most individuals are typically caused by exposure to certain endogenous or exogenous factors, it is not uncommon for individuals to have acute attacks in which no precipitating factor can be identified 2.
Acute porphyria attacks
An acute porphyria attack is defined as an episode that includes significantly increased urinary porphobilinogen (PBG) concentration and two or more of the clinical manifestations of an acute porphyria attack that typically persist for more than 24 hours in the absence of other likely explanations 38.
Severe abdominal pain, which may be generalized or localized and not accompanied by muscle guarding, is the most common symptom and is often the initial sign of an acute attack. Back, buttock, or limb pain may be a feature. Gastrointestinal features including nausea, vomiting, constipation or diarrhea, and abdominal distention are common, and ileus can occur. Tachycardia and hypertension are frequent, while fever, sweating, restlessness, and tremor are seen less frequently. Urinary retention, incontinence, and dysuria may be present.
Approximately 3%-8% of individuals with acute intermittent porphyria (AIP), mainly women, experience recurrent acute intermittent porphyria (AIP) (defined as ≥4 attacks in one year) for a prolonged period, often many years 38, 15.
Acute porphyria triggers
Acute porphyria attacks may be precipitated or triggered by endogenous or exogenous factors. These include the following 39:
- Prescribed and recreational drugs that are detoxified in the liver by cytochrome P450 and/or result in induction of 5-aminolevulinic acid (ALA) synthase and heme biosynthesis. Prescription drugs that can precipitate an attack include, for example, barbiturates, sulfa-containing antibiotics and antibiotics for urinary tract infections, some anti-seizure medications, progestogens, and synthetic estrogens (see a list of medications that clinicians must avoid using in porphyria patients (https://drugsporphyria.net/).
- Endocrine factors. Reproductive hormones play an important role in the clinical expression of acute intermittent porphyria (AIP). In women, acute neurovisceral attacks related to the menstrual cycle, usually the luteal phase, are common 39. Pregnancy in women with acute intermittent porphyria (AIP) is usually uncomplicated, and although urinary PBG concentration may increase during pregnancy, this does not lead to a higher frequency of clinical porphyria manifestations 40. However, there is a higher risk for pregnancy-induced hypertensive disorder, gestational diabetes, and infants with intrauterine growth restriction. In general, risk ratios are higher among women with acute intermittent porphyria (AIP) who have high lifetime urinary porphobilinogen (PBG) concentrations 41.
- Fasting. A recognized precipitating factor is inadequate caloric intake in connection with, for example, dieting or heavy exercise schedules 39.
- Stress. Psychosocial and other stresses, including intercurrent illnesses, infections, alcoholic excess, and surgery, can precipitate an attack 42
Peripheral neuropathy
Peripheral neuropathy is predominantly motor and is less common now than in the past, due to the availability of better treatments that reduce the risk of long duration of untreated acute porphyria attacks, the main risk factor for neurologic manifestations and long-term neurologic complications 2. Muscle weakness often begins proximally in the legs but may involve the arms or legs distally and can progress to include respiratory muscles, resulting in complete paralysis with respiratory failure 2. Bilateral axonal motor neuropathy may also involve the distal radial nerves. Motor neuropathy may also affect the cranial nerves or lead to bulbar paralysis.
Patchy sensory neuropathy may also occur 2.
Central nervous system signs
Mild mental changes such as anxiety, insomnia, irritability, and even mild cognitive impairment occur in up to 80% of symptomatic individuals and often in the initial stages of an acute porphyria attack 15.
Severe mental symptoms attributed to acute encephalopathy characterize the severe acute porphyria attack, manifesting as aberrant behavior, hallucinations, confusion, impaired consciousness, or seizures 43, 38.
Brain MRI changes can be detected in 47% of individuals with severe mental changes, usually in the form of posterior reversible encephalopathy syndrome, but normal MRI examination despite acute encephalopathy also occurs 43.
Hyponatremia is present in 25%-61% of acute porphyria attacks due to sodium loss, overhydration, hypothalamic involvement (i.e., syndrome of inappropriate antidiuretic hormone [SIADH]), or a combination of these conditions 43, 44.
Seizures occur in 1%-20% of acute porphyria attacks, with or without hyponatremia. They are transient and only present in severe attacks with acute encephalopathy; they do not occur in remission 43.
High Urine Porphobilinogen (PBG) Excreter
- Symptomatic high excreter. An individual with permanently high urinary porphobilinogen (PBG) concentration is considered symptomatic (i.e., a symptomatic high excreter) when having porphyria-related manifestations, usually pain, peripheral neuropathy, and psychiatric symptoms. Management of these manifestations is based on the need for supportive drugs, all of which should be evaluated for safety in acute intermittent porphyria (AIP). The condition usually occurs after an acute porphyria attack and can persist for many years 45. In a Swedish acute intermittent porphyria (AIP) cohort approximately 10% of adults with acute intermittent porphyria (AIP) are high urinary porphobilinogen (PBG) excreters 46.
- Asymptomatic high excreter. An asymptomatic HMBS heterozygote with permanently high urinary porphobilinogen (PBG) concentration (urine PBG-to-creatinine ratio ≥4 times the upper limit of normal) and has had no porphyria-related manifestations during the last two years.
Asymptomatic acute intermittent porphyria
Asymptomatic acute intermittent porphyria also called acute porphyria in remission refers to a person has had one or more acute porphyria attacks in the past but has had no acute porphyria-related manifestations during the last two years and has a urine porphobilinogen (PBG)-to-creatinine ratio is less than four times the upper limit of normal.
Latent acute intermittent porphyria
Latent acute intermittent porphyria refers to a person who is heterozygous for an HMBS pathogenic variant associated with acute intermittent porphyria who has never experienced acute porphyria-related manifestations and does not have significantly elevated urinary porphobilinogen (PBG) concentration.
The risk of becoming symptomatic depends on age, sex, and exposure to provoking agents, and is higher if the individual belongs to a family with other symptomatic individuals 47.
Acute intermittent porphyria signs and symptoms
Most people who inherit the HMBS gene for acute intermittent porphyria (AIP) never develop symptoms. However, experts recommend that all relatives of someone with acute intermittent porphyria obtain testing, to determine who has the genetic trait and who does not. Those who test positive for the trait should be educated as to measures that will help avoid attacks. Prevention is essential to good management.
It is important to note the highly variable nature of acute intermittent porphyria (AIP) and that affected individuals may not have all of the symptoms discussed below. Acute intermittent porphyria (AIP) can be associated with a range of symptoms and physical findings that can potentially involve multiple organ systems of the body. The course and severity of attacks is highly variable from one person to another. In some cases, particularly those without proper diagnosis and treatment, acute intermittent porphyria (AIP) can potentially cause life-threatening complications. Affected individuals and parents of affected children should talk to their physician and medical team about their specific case, associated symptoms and overall prognosis.
Acute intermittent porphyria (AIP) rarely attacks before puberty, with typical symptoms occurring between the ages of 20 and 40, more in females than males due to female sex hormones 4. Symptoms usually come as discrete attacks that develop over two or more days.
The abdominal pain is typically severe, epigastric, and colicky and can be severe and occurs in most cases. It tends to last for several days. The abdominal pain can be associated with constipation, nausea and vomiting 2.
Other symptoms may include:
- nausea
- vomiting
- constipation
- pain in the back, arms and legs
- muscle weakness (due to effects on nerves supplying the muscles)
- urinary retention
- palpitation (due to a rapid heart rate and often accompanied by increased blood pressure)
- Sometimes red or brown urine due to elevated porphobilinogen (PBG) in urine, which are the immediate precursors proximal to the hydroxymethylbilane synthase (HMBS), may be observed, which darkens on exposure to air, light, and warmth 48.
Central nervous system signs may include delirium, confusion, hallucinations, weakness with progression to quadriplegia and respiratory failure, cortical blindness, and even coma. In 5% of cases, patients can develop seizures, with partial seizures being the most common subtype 49
Sometimes the level of salt (sodium and chloride) in the blood decreases markedly and contributes to some of these symptoms. The skin is not affected.
The symptoms of acute intermittent porphyria (AIP) usually occur as episodes or “attacks” that develop over course of several hours or a few days. Affected individuals usually recover from an attack within days. However, if an acute attack is not diagnosed and treated promptly recovery can take much longer, even weeks or months. Most affected individuals do not exhibit any symptoms in between episodes. Onset of attacks usually occurs in the 20s or 30s, but may rarely occur at or just after puberty. Onset before puberty is extremely rare. Attacks are much more common in women than men, probably because of the menstrual cycle hormones. Approximately 3%-5% of affected individuals, predominately women, experience recurrent attacks, which are defined as more than 4 per year, for a period of many years.
Abdominal pain, which is usually severe, is the most common symptom associated with acute intermittent porphyria (AIP) and often the initial sign of an attack. Abdominal pain is usually severe, steady (unremitting) and widespread (diffuse). Less often, abdominal pain is described as cramping. Pain may also occur in the neck, lower back, buttocks, or arms and legs.
Gastrointestinal symptoms are also common during an attack and can include nausea, vomiting, constipation or diarrhea, and abdominal swelling (distention). A painful blockage or obstruction (ileus) of part of the small intestines may also occur. Difficulty passing urine (urinary retention) can also occur.
Neurological symptoms may also develop including damage to the nerves outside the central nervous system (peripheral neuropathy). Peripheral neuropathy is characterized by numbness or tingling and burning sensations that usually begin in the feet and sometimes the arms. Affected individuals may develop muscle weakness in the legs that may progress to affect the arms and the trunk of the body, eventually causing partial loss or impairment of motor function (motor paralysis). In rare cases, the muscles used to breathe can become involved and potentially cause life-threatening respiratory failure which requires mechanical ventilation.
During attacks some individuals develop psychological symptoms including irritability, depression, anxiety, insomnia, hallucinations, paranoia, disorientation, and altered consciousness ranging from excessive drowsiness (somnolence) to agitation or, in severe cases, coma.
Affected individuals may also experience a faster than normal heart rate (tachycardia) , high blood pressure (hypertension) and irregular heartbeats (cardiac arrhythmias). Seizures have also been reported. Abnormally low sodium levels (hyponatremia) may develop rapidly during an attack and contribute to the onset of seizures.
Patients have been reported to be completely free of symptoms in between the attacks. However, it is also suggested that 20% to 64% of patients may suffer from disabling chronic signs and symptoms such as pain, nausea, fatigue, and neuropathic features, including numbness and tingling sensations 50.
Individuals with chronic acute intermittent porphyria (AIP) may also develop complications that occur after many years (long-term complications) such as high blood pressure (hypertension), kidney damage potentially resulting in kidney failure, and liver cancers such as hepatocellular carcinoma (liver cancer) or cholangiocarcinoma (bile duct cancer).
A study conducted in Sweden demonstrated an increased risk of schizophrenia or bipolar disorder in patients with acute intermittent porphyria (AIP), as well as in their relatives 14.
Acute intermittent porphyria complications
Acute intermittent porphyria complications include:
- Systemic arterial hypertension and chronic kidney disease – Reports exist of the prevalence of up to 30% of these closely linked disorders in patients with acute intermittent porphyria (AIP) 51. End-stage renal disease (ESRD) is a life-threatening complication in acute intermittent porphyria (AIP) patients with chronic active disease 52
- Muscle denervation is another major pathologic complication 53. Some patients after acute attacks have residual deficits such as foot/wrist drop or wasting of the intrinsic muscles of hands 54.
- Hepatocellular carcinoma (liver cancer): This is the most deadly long-term complication of acute intermittent porphyria (AIP). Results of studies performed over the last 3 to 4 decades have shown a remarkably increased incidence of hepatocellular carcinoma (liver cancer) in acute intermittent porphyria (AIP) patients compared with the general population 55. A Swedish study showed that the risk for hepatocellular carcinoma (liver cancer) in AIP is increased 80 times after the age of 50 years 56, 2. It is worthwhile to know that acute intermittent porphyria (AIP) -associated hepatocellular carcinoma (liver cancer) is typically free from the usual preceding comorbidities such as Hepatitis B or C infection.
Acute intermittent porphyria diagnosis
A diagnosis of acute intermittent porphyria (AIP) can be difficult because most symptoms are nonspecific and occur episodically. A diagnosis is usually based upon identification of characteristic symptoms from a detailed patient history, a thorough clinical evaluation and certain specialized tests. Acute intermittent porphyria (AIP) should be suspected in individuals with unexplained abdominal pain, especially repeated episodes and when occurring along with psychological symptoms, neurological findings with muscle weakness or unexplained hyponatraemia. Dark or reddish urine in such individuals is also suggestive of acute intermittent porphyria (AIP). However, absence of this feature does not exclude acute intermittent porphyria (AIP). The diagnosis of acute intermittent porphyria (AIP) can be confirmed by finding an elevated level of porphobilinogen (PBG) (> 6 mg/L) on a spot urine test during an acute attack 16. If the urinary concentration of porphobilinogen (PBG) is increased, molecular genetic testing is performed to confirm the diagnosis and/or to facilitate screening of family members. When a multigene panel or genomic testing has identified an HMBS gene mutation, the diagnosis of an intermittent porphyria (AIP) attack is confirmed when the urinary concentration of PBG is increased.
Clinical Testing and Workup
Screening tests to measure the levels of the porphyrin precursor porphobilinogen (PBG) in urine are essential to confirm a diagnosis of acute porphyria. Acute attacks are always accompanied by increased production and excretion of porphyrin precursor porphobilinogen (PBG) in acute intermittent porphyria (AIP). If urinary porphobilinogen (PBG) excretion is increased, then further testing (fecal and blood porphyrin measurement) is necessary to distinguish acute intermittent porphyria (AIP) from variegate porphyria or hereditary coproporphyria. This should not delay treatment of acutely unwell patients. Delta-aminolevulinic acid (ALA) excretion will also be elevated in urine samples from individuals with acute intermittent porphyria (AIP), but measurement is less widely available and is not essential. These tests can be performed on a random (spot) urine sample that should be protected from light after collection and during transport to the laboratory. There is now good evidence that once urine porphobilinogen (PBG) excretion is increased in acute intermittent porphyria (AIP) it takes many years to return to normal. Increased urine porphobilinogen (PBG) excretion in a known acute intermittent porphyria (AIP) patient does not therefore prove that a patient is having an acute attack.
Family Testing
Molecular genetic testing is not essential to confirm a diagnosis as the porphyrin biochemical findings are characteristic. However molecular genetic testing to detect a mutation in the HMBS gene is usually required so that family members can be offered testing for this mutation. Genetic testing is available mainly from laboratories specializing in porphyria diagnosis.
Patients and family members who have inherited acute intermittent porphyria (AIP) should be advised on how to limit their risk of any future acute attacks. This should include information about acute intermittent porphyria (AIP) and what causes attacks, how to check if a prescribed medication is safe or unsafe and details of relevant patient support groups.
Resources for locating a genetics professional in your community are available online:
- The National Society of Genetic Counselors (https://www.findageneticcounselor.com/) offers a searchable directory of genetic counselors in the United States and Canada. You can search by location, name, area of practice/specialization, and/or ZIP Code.
- The American Board of Genetic Counseling (https://abgc.learningbuilder.com/Search/Public/MemberRole/Verification) provides a searchable directory of certified genetic counselors worldwide. You can search by practice area, name, organization, or location.
- The Canadian Association of Genetic Counselors (https://www.cagc-accg.ca/index.php?page=225) has a searchable directory of genetic counselors in Canada. You can search by name, distance from an address, province, or services.
- The American College of Medical Genetics and Genomics (https://clinics.acmg.net/) has a searchable database of medical genetics clinic services in the United States.
Evaluations Following Initial Diagnosis of Acute Intermittent Porphyria (AIP) Attack
To establish the extent of disease and needs in an individual diagnosed with acute intermittent porphyria (AIP) who is experiencing acute signs and symptoms, the following evaluations (if not performed as part of the evaluation that led to the diagnosis) are recommended:
- Consider other causes of abdominal pain in addition to porphyria.
- Review all medications and discontinue any that can exacerbate acute porphyria 57.
- Initial investigations should include the following:
- Complete blood count
- Measurement of serum/plasma concentrations of urea, creatinine, and electrolytes
- If there is hyponatremia, measure serum and urine osmolality, and urine sodium concentration
- Other blood tests as indicated by the individual’s condition and possible cause of the attack (e.g., C-reactive protein, blood cultures, serum creatine kinase, and plasma magnesium concentration)
- Brain MRI when central nervous system manifestations are present
- Refer individual to a porphyria specialist for more detailed clinical advice on acute intermittent porphyria (AIP).
- Affected individuals should be advised to register with an organization that provides warning jewelry in case of an accident (e.g., MedicAlert® or similar).
- Consultation with a medical geneticist, certified genetic counselor, or certified advanced genetic nurse is recommended to inform affected individuals and their families about the nature, mode of inheritance, and implications of AIP to facilitate medical and personal decision making.
- Assess need for family support and resources including community or online resources and home nursing referral.
Acute intermittent porphyria differential diagnosis
Symptoms of the following disorders can be similar to those of acute intermittent porphyria (AIP). Comparisons may be useful for a differential diagnosis.
The acute attacks that characterize acute intermittent porphyria (AIP) are similar to those seen in 3 other forms of porphyria specifically variegate porphyria, hereditary coproporphyria, and ALA-Dehydratase deficiency porphyria. Collectively, these four forms of the porphyria are classified as the acute porphyrias.
Guillain-Barré syndrome (GBS) is a rare, rapidly progressive autoimmune disorder where the body’s immune system mistakenly attacks the peripheral nerves, causing inflammation of the peripheral nervous system (polyneuritis) and nerve damage resulting in muscle weakness, sometimes progressing to complete paralysis 58, 59. Although the precise cause of Guillain-Barré syndrome is unknown, a viral or respiratory infection precedes the onset of the syndrome in about half of the patients. This has led to the theory that Guillain-Barré syndrome may be an autoimmune disease caused by the body’s own immune system. Damage to the covering (myelin) of nerve axons (the extension of the nerve cell that conducts impulses away from the nerve cell body) results in delayed nerve signal transmission. This causes weakness of the muscles that are supplied by the damaged nerves. Guillain-Barré syndrome begins suddenly and can increase in intensity over a period of hours, days, or weeks until certain muscles cannot be used at all. Some cases of Guillain-Barré syndrome are very mild and only marked by brief weakness. Others cause nearly devastating paralysis, leaving the person unable to breathe on their own. In these cases, the disorder is life-threatening—potentially interfering with breathing, blood pressure, or heart rate. Fortunately, most people eventually recover from even the most severe cases of Guillain-Barré syndrome. After recovery, people may continue to have some weakness. The following variants of Guillain-Barré syndrome are recognized:
- Acute Inflammatory Demyelinating Polyradiculoneuropathy (AIDP) is the most common form of Guillain-Barré Syndrome (GBS), an that affects the peripheral nervous system. Acute Inflammatory Demyelinating Polyradiculoneuropathy (AIDP) occurs when the body’s immune system mistakenly attacks the myelin sheath, the protective covering of the nerves, leading to nerve damage and impaired nerve signaling. It is characterized by rapidly progressive weakness and sensory loss in the limbs due to inflammation and damage to the myelin sheath of peripheral nerves.
- Miller Fisher syndrome (MFS) is a rare neurological disorder considered a variant of Guillain-Barré syndrome (GBS) 60. Miller Fisher syndrome (MFS) is characterized by a triad of symptoms: ataxia (loss of coordination), areflexia (loss of reflexes), and ophthalmoplegia (paralysis of the eye muscles). While MFS is rare, affecting 1-2 people per million each year, it is typically self-limiting, with most individuals recovering within 6 months even without specific treatment
- Acute Motor-Sensory Axonal Neuropathy (AMSAN) is a severe variant of Guillain-Barré syndrome (GBS) characterized by rapidly progressive weakness and sensory loss, often requiring ventilation and having a prolonged recovery period 61. Acute Motor-Sensory Axonal Neuropathy (AMSAN) is an axonal subtype, meaning it primarily affects the nerve fibers (axons) rather than the myelin sheaths that surround them.
- Acute motor axonal neuropathy (AMAN) is a rare variant of Guillain-Barré syndrome (GBS) characterized by acute, predominantly motor paralysis, with minimal or no sensory loss 62. Acute motor axonal neuropathy (AMAN) is an autoimmune disorder where the body’s immune system attacks the motor axons (nerve fibers). Acute motor axonal neuropathy (AMAN) is often associated with prior infection, particularly by Campylobacter jejuni, and can lead to significant motor weakness and, in some cases, respiratory failure.
Causes of acute abdomen – Peritonitis, appendicitis, acute cholecystitis, acute gastritis, acute pancreatitis, intestinal occlusion, strangulated abdominal hernia, acute mesenteric ischemia, ileus, diverticulitis, esophagitis, endometriosis, gastric outlet obstruction, intussusception, pelvic inflammatory disease, ovarian cysts, acute pyelonephritis, aortic dissection.
Tyrosinemia type 1 is a rare autosomal recessive genetic metabolic disorder characterized by lack of the enzyme fumarylacetoacetate hydrolase (FAH), which is needed for the final break down of the amino acid tyrosine. Failure to properly break down tyrosine leads to abnormal accumulation of tyrosine and its metabolites in the liver, including a heme precursor aminolevulinic acid (ALA), potentially resulting in severe liver disease. Tyrosine may also accumulate in the kidneys and central nervous system. Symptoms and physical findings associated with tyrosinemia type 1 appear in the first months of life and include failure to gain weight and grow at the expected rate (failure to thrive), fever, diarrhea, vomiting, an abnormally enlarged liver (hepatomegaly), and yellowing of the skin and the whites of the eyes (jaundice). Tyrosinemia type 1 may progress to more serious complications such as severe liver disease, cirrhosis, and hepatocellular carcinoma if left untreated. Untreated children can also suffer neurological crises similar to those seen in acute porphyria. Treatment with nitisinone and a low-tyrosine diet should begin as soon as possible after the diagnosis is confirmed.
Lead toxicity can cause symptoms that mimic acute porphyria (acute abdominal pain, constipation, neuropathy). Lead inhibits several of the enzymes of heme biosynthesis, which can therefore result in an increase in urine coproporphyrin and 5-aminolevulinic acid excretion, but not porphobilinogen excretion. It can also cause an increase in erythrocyte protoporphyrin concentration, although this is all the zinc-chelate form (zinc-protoporphyrin). The definitive test for lead poisoning is blood lead measurement.
Acute intermittent porphyria treatment
The treatment of acute intermittent porphyria (AIP) is directed toward the specific symptoms that are apparent in each individual. Treatment may require the coordinated efforts of a team of specialists. Pediatricians, neurologists, hematologists, hepatologists, psychiatrists, and other healthcare professionals may need to systematically and comprehensively plan an affected patient’s treatment. Genetic counseling may benefit affected individuals and their families.
The objective of acute intermittent porphyria (AIP) treatment is to manage your symptoms, prevent complications and to suppress heme synthesis in your liver with hematin, which reduces the production of porphyrin precursors. Initial treatment steps also include stopping any medications that can potentially worsen acute intermittent porphyria (AIP) or cause an attack and ensuring proper caloric intake, which can include intravenous infusion of sufficient nutrients (glucose and salt). Carbohydrate loading in conjunction with good pain medication may be sufficient for mild attacks.
Hospitalization is often necessary for acute attacks, particularly if nausea and vomiting have prevented adequate oral intake. Medications for pain, nausea and vomiting, intravenous (IV) hydration, and close observation are generally required.
In the United States, affected individuals may be treated with Panhematin (hemin for injection), an enzyme inhibitor derived from red blood cells that is potent in suppressing acute attacks of porphyria. Panhematin almost always returns porphyrin and porphyrin precursor levels to normal values. The U.S. Food and Drug Administration (FDA) approved Panhematin for the treatment of recurrent attacks of acute intermittent porphyria (AIP) related to the menstrual cycle in susceptible women, after a trial of glucose therapy and should be administered only by physicians experienced in the management of porphyrias in a hospital setting. Based on much experience, it is used for treating and even preventing acute attacks, often without an initial trial of glucose, and has been found to be safe during pregnancy.
Glucose and other carbohydrates can help suppress disease activity, are given by vein or by mouth, and are part of initial treatment. Intravenous heme, however, is both more specific and effective than glucose and should be started if the patient’s symptoms fail to improve within 36 hours. Heme is sold as Panhematin®, from Recordati Rare Diseases (https://recordatirarediseases.com/products). Most hospitals do not stock it. Therefore the pharmacy must be notified at the time the patient’s admission to initiate a request for air-freighting enough medication for 5 days of treatment. Generally, shipping will take at least 24 hours.
Panhematin, is the only commercially available form of heme for treatment and prevention of acute porphyric attacks in the United States. Heme arginate, which is marketed in other countries as Normosang® (Orphan Europe), is another preparation for intravenous administration. The main side-effect of Panhematin® is irritation of the vein used for infusion (phlebitis). This is avoided by slow infusion through a large caliber vein or central line. Adding human albumin to the heme solution also may reduce the risk of phlebitis. (Directions for preparing Panhematin® in this manner can be obtained from porphyria specialist and is included in the Primary Care Physician/Emergency Room Kit.) Heme therapy is indicated only if an acute attack of porphyria is proven by a marked increase in urine porphobilinogen. It may be useful also as preventive therapy for people with frequent recurrent attacks.
In 2019, the FDA approved Givlaari (givosiran) for the treatment of adult patients with acute hepatic porphyria, including acute intermittent porphyria (AIP). Givlaari (givosiran) aims to reduce the number of attacks patients experience.
Normosang (heme arginate) is another heme preparation that can be used to treat individuals with acute intermittent porphyria (AIP). Normosang is not available in the United States, but is used in many other countries where Panhematin is not available.
Treatment for acute intermittent porphyria (AIP) also includes drugs to treat specific symptoms such as certain pain medications (analgesics), anti-anxiety drugs, anti-hypertensive drugs, and drugs to treat nausea and vomiting, tachycardia, or restlessness. The pain is usually very severe and generally requires opiates (e.g. morphine) for adequate relief. Medications to treat any infections that may occur at the same time as an attack (intercurrent infection) may also be necessary. Although many types of drugs are believed to be safe in individuals with acute intermittent porphyria (AIP), recommendations about drugs for treating acute intermittent porphyria (AIP) are based upon experience and clinical study. Since many commonly used drugs have not been tested for their effects on porphyria, they should be avoided if at all possible. If a question of drug safety arises, a physician or medical center specializing in porphyria should be contacted. A list of these institutions may be obtained from the American Porphyria Foundation. The Foundation also maintains an Acute Porphyria Drug Database (https://porphyriafoundation.org/for-healthcare-professionals/ahp-drug-safety-database/). The EPNET/NAPOS Database should also be consulted. The Norwegian Porphyria Centre (NAPOS), with the European Porphyria Network (EPNET), has created a list of medications that clinicians must avoid using in porphyria patients (https://drugsporphyria.net/). These drugs include ketamine, thiopental, chloramphenicol, erythromycin, nitrofurantoin, rifampicin, trimethoprim/sulfamethoxazole, spironolactone, methyldopa, valproic acid, carbamazepine, phenytoin, phenobarbital, primidone, and risperidone 63. For information on prescribing medication in the context of certain conditions (e.g., HIV, epilepsy, malaria), see https://porphyria.uct.ac.za/porphyria-professionals/prescribing-porphyria-treatment-specific-disorders-poprhyria/therapy-epilepsy.
During treatment of an attack, attention should be given to salt and water balance. For example, if individuals develop hyponatremia, which can induce seizures, they should be treated by saline infusion. Harmful drugs should be stopped. These include barbiturates, sulfonamides, and many others (see the full list here: https://porphyriafoundation.org/for-healthcare-professionals/ahp-drug-safety-database/).
In some patients, an attack is precipitated by a low intake of carbohydrates in an attempt to lose weight. Consequently, dietary counseling is very important. Affected individuals who are prone to attacks should eat a normal balanced diet and should not greatly restrict their intake of carbohydrates or calories, even for short periods of time. If weight loss is desired, it is advisable to contact a physician and dietician.
Premenstrual attacks often resolve quickly with the onset of menstruation. Hormone manipulation may be effective in preventing such attacks and some affected women have been treated with gonadotropin-releasing hormone analogues to suppress ovulation and prevent frequent cyclic attacks. Some individuals who experience recurrent attacks may benefit from regular hematin infusion. This is sometimes recommended for women with severe symptoms during the time of their menses.
If a proper diagnosis has not been made, acute intermittent porphyria (AIP) can be particularly dangerous, especially if drugs which aggravate the disorder are administered. The prognosis of acute intermittent porphyria (AIP) is usually good if the disorder is recognized before severe nerve damage has occurred and if treatment and preventive measures are begun. Although symptoms usually resolve after an attack, some individuals may develop chronic pain. Nerve damage and associated muscle weakness from a severe attack improves over time, but such improvement may take many months to resolve fully.
Liver transplantation has been used to treat some individuals with acute intermittent porphyria (AIP), specifically individuals with severe disease who have failed to respond to other treatment options. A liver transplant in individuals with acute intermittent porphyria (AIP) is an option of last resort. Affected individuals who experience kidney failure may require a kidney transplant. Some individuals have required a combined kidney and liver transplant.
Wearing a Medic Alert bracelet is advisable for patients who have had attacks. People who are asymptomatic carriers of the genetic trait may choose not to wear a bracelet but should be prepared in any medical encounter to advise their care-givers of medications that are risky in acute intermittent porphyria. It should be remembered that acute intermittent porphyria patients can develop other diseases, and symptoms will not always be due to porphyria.
Treatment of Sporadic Acute Neurovisceral Attacks
Intravenous human hemin is the most effective treatment for sporadic acute neurovisceral attacks (i.e., when an individual has experienced 1 to ≤3 acute porphyria attacks). Intravenous administration of hemin preparations may be lifesaving if employed early, when neuronal damage is still reversible, and may help to avoid peripheral neuropathy or prevent its progression.
The recommended dose for hemin is 3-4 mg/kg by IV, given once daily for four days. Treatment may be extended, depending on the clinical course. Note: Because 100 mg of hemin contains 8 mg of iron, frequent administration of hemin may increase the risk for iron overload. Periodic monitoring of serum ferritin concentration and/or transferrin saturation is therefore appropriate in individuals treated repeatedly with hemin.
- Panhematin® is approved for treatment of acute attacks in the United States. This product is supplied as a dried powder, which must be reconstituted with sterile water immediately before IV injection and administered over ten to 15 minutes. Because the administration of Panhematin® reconstituted with sterile water is associated with transient, mild coagulopathy, concurrent anticoagulant therapy should be avoided.
- Heme arginate (Normosang®) is an arginine-stabilized form of human hemin available nearly worldwide, including in Europe, Africa, the Middle East, and South America. It is infused over at least 30 minutes. It has the same advantage as hemin in treating an acute neurovisceral attack but has fewer reported side effects 32.
Note: (1) Phlebitis after IV injection can be minimized by reconstituting hematin in 20% human serum albumin solution and/or by using a large vein or a central catheter for infusion. Peripheral cannulas used to administer hematin should be replaced after each use. (2) An infusion set with an in-line filter is recommended to remove any undissolved particulate matter. (3) Rigorous flushing of venous catheters with boluses of saline totaling 200 mL is recommended.
Recurrent acute attacks are best managed with support and advice from a porphyria specialist. See information and contact details of specialist porphyria centers at the International Porphyria Network website.
If the criterion for recurrent attacks is met, Givlaari® (givosiran) should be considered, as long-term complications of hemin such as iron overload, phlebitis, and loss of venous access can be avoided 38.
Prevention of Recurrent Acute Neurovisceral Attacks
Givlaari® (givosiran) is a subcutaneously delivered RNA interference therapeutic specifically targeting ALAS1 mRNA in the liver to reduce urinary excretion of 5-aminolevulinic acid (ALA) and PBG. It is approved for treatment of acute porphyria in adults and adolescents age ≥12 years in the European Union and adults in the United States. Clinical studies have shown an acceptable safety profile and clinical efficacy in reducing attack rates and use of hemin 44.
When available, use of this treatment has meant that older treatment alternatives such as ovulation suppression therapy and preventive hemin can be avoided. For the sporadic acute attack, hemin is still the treatment of primary choice.
Liver Transplantation
Liver transplantation is curative and reported from several centers 64. Indications include repeated life-threatening acute porphyria attacks and poor quality of life where givosiran is not available or has shown insufficient medical efficacy.
Note that ALA toxicity is the major hypothesis proposed for the pathogenesis of the neurologic lesions causing the clinical features of acute porphyria attacks. Support for this hypothesis are (1) the success of liver transplantation as a cure for recurrent acute attacks 64; and (2) the occurrence of acute attacks in persons who do not have acute intermittent porphyria (AIP) who have received a liver transplant from persons who experience recurrent acute attacks, implicating release of a hepatic neurotoxin, probably ALA, as their cause 65.
Supportive Therapy
Other recommendations to reduce the frequency and/or severity of acute attacks include the following:
- Ensure that adequate nutrition is provided by a normal balanced diet. Avoid unsupervised diets that restrict caloric intake, particularly those that exclude carbohydrates completely.
Seek timely treatment of systemic illness or infection. - Pain relief. Effective analgesia should be provided as soon as possible, usually in the form of parenteral opiates (morphine, diamorphine, and fentanyl are safe). Very large quantities may be required in a severe acute attack. Consider patient-controlled analgesia and support from a pain management team.
- Treatment of hypertension. Sixty percent of symptomatic individuals with acute intermittent porphyria (AIP) have hypertension because of development of acute intermittent porphyria (AIP)-related chronic kidney disease 66. Beta-blockers and renin-angiotensin-aldosterone system (RAAS)-blockers are considered safe and should be used to delay the development of end-stage kidney disease.
- Prevention of nausea and vomiting. Prochloperazine, promazine, or ondansetron are considered safe.
- Prompt treatment of seizures can be terminated with intravenous diazepam, clonazepam, or magnesium sulphate.
- Maintenance of fluid and electrolyte balance. Intravenous fluid replacement may be required to correct dehydration or electrolyte imbalance. Dextrose in water solutions should be avoided because of the risk of hyponatremia. Chronic hyponatremia (developing over >48 hours) should be corrected slowly to minimize the risk of central pontine myelinolysis 57.
- Combined liver and kidney transplantation, which has been successful, can be considered in individuals with acute intermittent porphyria (AIP) who have recurrent acute porphyria attacks and end-stage kidney disease 67. Individuals with acute intermittent porphyria (AIP) may require kidney replacement therapy 39.
Alternative Medical Therapies
Alternative medical therapies to reduce the frequency and/or severity of acute porphyria attacks if givosiran is not available include ovulation suppression therapy and prophylactic hemin infusion.
- Ovulation suppression therapy with gonadorelin analogs has been used for women with recurrent menstrual cycle-related acute neurovisceral attacks 68. Long-acting analogs that can be used to prevent ovulation should be administered during the first few days of the menstrual cycle to minimize the early stimulation effect on hormone release that can trigger an attack. Side effects can be minimized by administering estrogen, preferably by patch. Gynecologic review and bone density monitoring are recommended. This treatment should be continuously evaluated in consultation with a porphyria specialist and preferably not last longer than two years.
- Prophylactic hemin infusion is possible. The minimum effective infusion frequency should be employed, usually a weekly dose of hemin infused via an indwelling venous catheter. Problems include those associated with a venous access device (infection, blockage) and iron overload.
Experimental Therapies
- Enzyme Replacement Therapy [ERT] – Based on the experience of administering doses of recombinant human HMBS/PBGD (rhPBGD) protein in a mouse model of acute intermittent porphyria (AIP) that reduced plasma porphobilinogen (PBG) accumulation during an acute attack induced after phenobarbital challenge, in 2002 the European Medicines Agency (EMA) granted recombinant human HMBS/PBGD an orphan designation (EU/3/ 02/103). Researchers conducted clinical trials in healthy subjects, asymptomatic hydroxymethylbilane synthase (HMBS)-deficient subjects with increased porphyrin precursor excretion, and acute intermittent porphyria (AIP) patients with repeated attacks 69, 70. Although the enzyme was able to detoxify porphobilinogen (PBG) metabolites, the treatment approach limitations included its short half-life in circulation and the lack of liver targeting.
- Liver Gene Therapy – Clinical trials using two strategies, HMBS-gene therapy and interference RNA for ALAS1 gene inhibition, are being conducted in patients with acute intermittent porphyria (AIP). The two strategies include – the delivery of the HMBS gene to the liver cells using a viral vector. The other option is a small interfering RNA (siRNA) directed against aminolevulinic acid synthase, with the objective of reducing delta aminolevulinic acid (ALA) production. Both of them are still in the trial phase and await approval, pending larger trials that would hopefully provide consistent efficacy and safety 10, 71.
Acute intermittent porphyria diet
Acute intermittent porphyria patients prone to attacks should eat a normal or high carbohydrate diet and should not greatly restrict their intakes of carbohydrate and calories, even for short periods of time. If weight loss is desired, it is advisable to consult a physician, who may request that a dietitian estimate an individual’s normal caloric intake, which varies greatly from one person to another. It may be appropriate to prescribe a diet that is approximately 10% below the normal level of calories for the patient. This should result in a gradual weight loss and usually will not cause an attack of porphyria.
Acute intermittent porphyria and pregnancy
Pregnancy in women with acute intermittent porphyria (AIP) is usually uncomplicated. Offspring have a 50% chance of inheriting the gene for acute intermittent porphyria, but the great majority of them remain “latent” for all or most of their lifetimes. The minority that eventually have symptoms usually benefit from treatment. Given these considerations, most patients or individuals with “latent” porphyria elect to have children for the same reasons as anyone else.
Although urinary porphobilinogen (PBG) concentration may increase during pregnancy, this does not lead to a higher frequency of clinical manifestations of porphyria 40.
Preconception counseling is recommended to advise women with acute intermittent porphyria (AIP) of the clinical manifestations of porphyria, self-care, and preventative measures to avoid exacerbations (i.e., adequate and regular nutrition, rest, and carbohydrate intake for treating mild-to-moderate symptoms).
There is a higher risk for pregnancy-induced hypertensive disorder, gestational diabetes, and fetuses with intrauterine growth restriction (IUGR). In general, risk ratios are higher among women with acute intermittent porphyria (AIP) who have high lifetime urinary porphobilinogen (PBG) concentrations 41.
Testing for urinary porphobilinogen (PBG) concentration prior to pregnancy may establish the individual’s risk levels.
Women with biochemically active acute hepatic porphyria (AHP) (i.e., urinary porphobilinogen (PBG) concentration greater than four times the upper limit of normal) or a history of active acute hepatic porphyria (AHP) should be offered specialized prenatal care. Hyperemesis, a catabolic risk for precipitating acute attacks, should be treated promptly. Blood pressure should be monitored once monthly during the first and second trimesters, and weekly during the last trimester. Additional monitoring of fetal growth during pregnancy will help identify intrauterine growth restriction (IUGR) 41.
When a woman with acute intermittent porphyria (AIP) experiences abdominal pain, hypertension, and tachycardia during pregnancy, urine porphobilinogen (PBG) concentration should be measured, and complications of pregnancy should be excluded in consultation with an obstetrician before the findings are attributed to an acute attack.
- If an acute porphyria attack is suspected, a urine porphobilinogen (PBG) concentration should be measured before deciding on specific treatment.
- Any symptomatic treatment needed should be chosen after considering the risk of the drug triggering/aggravating an acute porphyria attack in the pregnant woman.
- An obstetrician should be consulted regarding medical treatment and possible effects on the fetus.
- Human hemin is safe to be used during pregnancy 72
- No human pregnancies have been reported during or after treatment with Givlaari® (givosiran); there are no data on the presence of givosiran in human milk.
Note: In an obstetric emergency, no drug should be restricted if it is likely to be of major clinical benefit or is required in a life-threatening situation.
Acute intermittent porphyria prognosis
Prognosis is good if acute intermittent porphyria is recognized early and treated at the time 1. The mortality rate for acute intermittent porphyria has decreased through the past decades to 5% to 20% (on acute attacks) thanks to new methods of diagnosis and treatment (use of human hemin) 1. But if acute intermittent porphyria is resistant to heme therapy and is recurrent, the only currently approved way to reduce mortality is with an orthotopic liver transplant where a diseased liver is removed and replaced with a healthy donor liver in the same anatomical position 39, 73, 54. The overall survival at five years after liver transplantation is 82%, which is consistent with survival data for individuals transplanted for other metabolic diseases 64.
With ongoing trials exploring the efficacy and safety of enzyme replacement therapy (ERT) and liver gene therapy, the prognosis of acute intermittent porphyria (AIP) is expected to become better very soon 1.
Untreated acute intermittent porphyria (AIP) is associated with significant morbidity and can lead to paresis (incomplete paralysis) and death. Long-term complications include chronic hypertension, chronic neuropathy, chronic kidney disease, and risk of hepatocellular carcinoma (liver cancer) 74, 75, 44.
- Gonzalez-Mosquera LF, Sonthalia S. Acute Intermittent Porphyria. [Updated 2023 May 1]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK547665[↩][↩][↩][↩][↩][↩][↩][↩]
- Sardh E, Barbaro M. Acute Intermittent Porphyria. 2005 Sep 27 [Updated 2024 Feb 8]. In: Adam MP, Feldman J, Mirzaa GM, et al., editors. GeneReviews® [Internet]. Seattle (WA): University of Washington, Seattle; 1993-2025. Available from: https://www.ncbi.nlm.nih.gov/books/NBK1193[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Bustad HJ, Kallio JP, Vorland M, Fiorentino V, Sandberg S, Schmitt C, Aarsand AK, Martinez A. Acute Intermittent Porphyria: An Overview of Therapy Developments and Future Perspectives Focusing on Stabilisation of HMBS and Proteostasis Regulators. Int J Mol Sci. 2021 Jan 12;22(2):675. doi: 10.3390/ijms22020675[↩]
- Lei JJ, Li S, Dong BX, Yang J, Ren Y. Acute intermittent porphyria: a disease with low penetrance and high heterogeneity. Front Genet. 2024 Aug 12;15:1374965. doi: 10.3389/fgene.2024.1374965[↩][↩]
- Ren Y, Li S, Lei JJ, Li R, Dong BX, Yang J. Clinical feature and genetic analysis of HMBS gene in Chinese patients with acute intermittent porphyria: a systematic review. Front Genet. 2023 Dec 11;14:1291719. doi: 10.3389/fgene.2023.1291719[↩]
- Longo M, Paolini E, Meroni M, Dongiovanni P. Cutting-Edge Therapies and Novel Strategies for Acute Intermittent Porphyria: Step-by-Step towards the Solution. Biomedicines. 2022 Mar 11;10(3):648. doi: 10.3390/biomedicines10030648[↩]
- Patel P, Midha S, Shukla S, Dhamija D, Bello AO, Khan S. Evaluating the Efficacy of a Small Interfering Ribonucleic Acid Molecule, Givosiran, in Treating Acute Intermittent Porphyria: A Systematic Review. Cureus. 2023 Jun 18;15(6):e40585. doi: 10.7759/cureus.40585[↩]
- Li S, Lei JJ, Dong BX, Ren Y, Yang J. HMBS gene mutations and hydroxymethylbilane synthase activity in acute intermittent porphyria: A systematic review. Medicine (Baltimore). 2023 Sep 29;102(39):e35144. doi: 10.1097/MD.0000000000035144[↩][↩]
- Storjord E, Wahlin S, Karlsen BO, Hardersen RI, Dickey AK, Ludviksen JK, Brekke OL. Potential Biomarkers for the Earlier Diagnosis of Kidney and Liver Damage in Acute Intermittent Porphyria. Life (Basel). 2023 Dec 21;14(1):19. doi: 10.3390/life14010019[↩]
- Bissell DM, Anderson KE, Bonkovsky HL. Porphyria. N Engl J Med. 2017 Aug 31;377(9):862-872. doi: 10.1056/NEJMra1608634[↩][↩]
- Acute Intermittent Porphyria (AIP). https://porphyriafoundation.org/for-patients/types-of-porphyria/aip/[↩]
- Acute Intermittent Porphyria. https://rarediseases.org/rare-diseases/acute-intermittent-porphyria/[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Founder Effect. https://www.genome.gov/genetics-glossary/Founder-Effect[↩]
- Cederlöf M, Bergen SE, Larsson H, Landén M, Lichtenstein P. Acute intermittent porphyria: comorbidity and shared familial risks with schizophrenia and bipolar disorder in Sweden. Br J Psychiatry. 2015 Dec;207(6):556-7. doi: 10.1192/bjp.bp.114.157073[↩][↩]
- Gouya L, Ventura P, Balwani M,, et al. EXPLORE: A Prospective, Multinational, Natural History Study of Patients with Acute Hepatic Porphyria with Recurrent Attacks. Hepatology. 2020 May;71(5):1546-1558. doi: 10.1002/hep.30936[↩][↩][↩]
- Acute Intermittent Porphyria. https://emedicine.medscape.com/article/205220-overview[↩][↩][↩]
- Schulenburg-Brand D., Stewart F., Stein P., Rees D., Badminton M. (2022). Update on the diagnosis and management of the autosomal dominant acute hepatic porphyrias. J. Clin. Pathol. 75, 537–543. 10.1136/jclinpath-2021-207647[↩][↩]
- Wang B., Bonkovsky H. L., Lim J. K., Balwani M. (2023). AGA clinical practice update on diagnosis and management of acute hepatic porphyrias: expert review. Gastroenterology 164, 484–491. 10.1053/j.gastro.2022.11.034[↩]
- Yarra P., Faust D., Bennett M., Rudnick S., Bonkovsky H. L. (2019). Benefits of prophylactic heme therapy in severe acute intermittent porphyria. Mol. Genet. Metab. Rep. 19, 100450. 10.1016/j.ymgmr.2019.01.002[↩]
- Blaylock B., Epstein J., Stickler P. (2020). Real-world annualized healthcare utilization and expenditures among insured US patients with acute intermittent porphyria (AIP) treated with hemin. J. Med. Econ. 23, 537–545. 10.1080/13696998.2020.1724118[↩]
- Poli A, Schmitt C, Moulouel B, et al. Givosiran in acute intermittent porphyria: A personalized medicine approach. Mol Genet Metab. 2022 Mar;135(3):206-214. doi: 10.1016/j.ymgme.2022.01.002[↩]
- Lin, Jou & Shi, Donglu. (2021). Photothermal and photovoltaic properties of transparent thin films of porphyrin compounds for energy applications. Applied Physics Reviews. 8. 011302. https://doi.org/10.1063/5.0036961[↩]
- Panawala, Lakna. (2017). What is the Function of Hemoglobin in the Human Body. https://www.researchgate.net/publication/313841668_What_is_the_Function_of_Hemoglobin_in_the_Human_Body[↩]
- Heme and Bilirubin Metabolism. https://themedicalbiochemistrypage.org/heme-and-bilirubin-metabolism/[↩]
- Marcacci, M., Ricci, A., Cuoghi, C. et al. Challenges in diagnosis and management of acute hepatic porphyrias: from an uncommon pediatric onset to innovative treatments and perspectives. Orphanet J Rare Dis 17, 160 (2022). https://doi.org/10.1186/s13023-022-02314-9[↩]
- Kizilaslan EZ, Ghadge NM, Martinez A, Bass M, Winayak R, Mathew M, Amin R, Khan M, Kizilbash N. Acute Intermittent Porphyria’s Symptoms and Management: A Narrative Review. Cureus. 2023 Mar 13;15(3):e36058. doi: 10.7759/cureus.36058[↩]
- Kizilaslan EZ, Ghadge NM, Martinez A, Bass M, Winayak R, Mathew M, Amin R, Khan M, Kizilbash N. Acute Intermittent Porphyria’s Symptoms and Management: A Narrative Review. Cureus. 2023 Mar 13;15(3):e36058. doi: 10.7759/cureus.36058[↩]
- Namba H, Narahara K, Tsuji K, Yokoyama Y, Seino Y. Assignment of human porphobilinogen deaminase to 11q24.1—-q24.2 by in situ hybridization and gene dosage studies. Cytogenet Cell Genet. 1991;57(2-3):105-8. doi: 10.1159/000133123[↩]
- Szlendak U, Bykowska K, Lipniacka A. Clinical, Biochemical and Molecular Characteristics of the Main Types of Porphyria. Adv Clin Exp Med. 2016 Mar-Apr;25(2):361-8. doi: 10.17219/acem/58955[↩]
- HMBS gene. https://medlineplus.gov/genetics/gene/hmbs/[↩]
- Anderson K. E., Bloomer J. R., Bonkovsky H. L., Kushner J. P., Pierach C. A., Pimstone N. R., et al. (2005). Recommendations for the diagnosis and treatment of the acute porphyrias. Ann. Intern Med. 142, 439–450. 10.7326/0003-4819-142-6-200503150-00010[↩]
- Puy H, Gouya L, Deybach JC. Porphyrias. Lancet. 2010 Mar 13;375(9718):924-37. doi: 10.1016/S0140-6736(09)61925-5[↩][↩]
- Chen B, Solis-Villa C, Hakenberg J, Qiao W, Srinivasan RR, Yasuda M, Balwani M, Doheny D, Peter I, Chen R, Desnick RJ. Acute Intermittent Porphyria: Predicted Pathogenicity of HMBS Variants Indicates Extremely Low Penetrance of the Autosomal Dominant Disease. Hum Mutat. 2016 Nov;37(11):1215-1222. doi: 10.1002/humu.23067[↩]
- Kuo HC, Huang CC, Chu CC, Lee MJ, Chuang WL, Wu CL, Wu T, Ning HC, Liu CY. Neurological complications of acute intermittent porphyria. Eur Neurol. 2011;66(5):247-52. doi: 10.1159/000330683[↩]
- Storjord E, Dahl JA, Landsem A, Fure H, Ludviksen JK, Goldbeck-Wood S, Karlsen BO, Berg KS, Mollnes TE, W Nielsen E, Brekke OL. Systemic inflammation in acute intermittent porphyria: a case-control study. Clin Exp Immunol. 2017 Mar;187(3):466-479. doi: 10.1111/cei.12899[↩][↩]
- Barreda-Sánchez M., Buendía-Martínez J., Glover-López G., Carazo-Díaz C., Ballesta-Martínez M. J., López-González V., et al. (2019). High penetrance of acute intermittent porphyria in a Spanish founder mutation population and CYP2D6 genotype as a susceptibility factor. Orphanet J. Rare Dis. 14, 59. 10.1186/s13023-019-1031-7[↩]
- Wang B, Bonkovsky HL, Lim JK, Balwani M. AGA Clinical Practice Update on Diagnosis and Management of Acute Hepatic Porphyrias: Expert Review. Gastroenterology. 2023 Mar;164(3):484-491. doi: 10.1053/j.gastro.2022.11.034[↩]
- Stein PE, Edel Y, Mansour R, Mustafa RA, Sandberg S; Members of the Acute Porphyria Expert Panel. Key terms and definitions in acute porphyrias: Results of an international Delphi consensus led by the European porphyria network. J Inherit Metab Dis. 2023 Jul;46(4):662-674. doi: 10.1002/jimd.12612[↩][↩][↩][↩]
- Wang B, Rudnick S, Cengia B, Bonkovsky HL. Acute Hepatic Porphyrias: Review and Recent Progress. Hepatol Commun. 2018 Dec 20;3(2):193-206. doi: 10.1002/hep4.1297[↩][↩][↩][↩][↩]
- Vassiliou D, Sardh E. Acute hepatic porphyria and maternal health: Clinical and biochemical follow-up of 44 pregnancies. J Intern Med. 2022 Jan;291(1):81-94. doi: 10.1111/joim.13376[↩][↩]
- Mantel Ä, Vassiliou D, Lissing M, Stephansson O, Wahlin S, Sardh E. Maternal and fetal outcomes in acute hepatic porphyria: A Swedish National Cohort Study. J Inherit Metab Dis. 2023 Jul;46(4):675-686. doi: 10.1002/jimd.12616. Epub 2023 Apr 26. Erratum in: J Inherit Metab Dis. 2024 Jan;47(1):212. doi: 10.1002/jimd.12685[↩][↩][↩]
- Storjord E, Dahl JA, Landsem A, Ludviksen JK, Karlsen MB, Karlsen BO, Brekke OL. Lifestyle factors including diet and biochemical biomarkers in acute intermittent porphyria: Results from a case-control study in northern Norway. Mol Genet Metab. 2019 Nov;128(3):254-270. doi: 10.1016/j.ymgme.2018.12.006[↩]
- Pischik E, Baumann K, Karpenko A, Kauppinen R. Pathogenesis of acute encephalopathy in acute hepatic porphyria. J Neurol. 2023 May;270(5):2613-2630. doi: 10.1007/s00415-023-11586-5[↩][↩][↩][↩]
- Sardh E, Harper P. RNAi therapy with givosiran significantly reduces attack rates in acute intermittent porphyria. J Intern Med. 2022 May;291(5):593-610. doi: 10.1111/joim.13443[↩][↩][↩]
- Marsden JT, Rees DC. Urinary excretion of porphyrins, porphobilinogen and δ-aminolaevulinic acid following an attack of acute intermittent porphyria. J Clin Pathol. 2014 Jan;67(1):60-5. doi: 10.1136/jclinpath-2012-201367[↩]
- Lissing M, Vassiliou D, Floderus Y, Harper P, Bottai M, Kotopouli M, Hagström H, Sardh E, Wahlin S. Risk of primary liver cancer in acute hepatic porphyria patients: A matched cohort study of 1244 individuals. J Intern Med. 2022 Jun;291(6):824-836. doi: 10.1111/joim.13463[↩]
- Baumann K, Kauppinen R. Penetrance and predictive value of genetic screening in acute porphyria. Mol Genet Metab. 2020 May;130(1):87-99. doi: 10.1016/j.ymgme.2020.02.003[↩]
- Fontanellas A, Ávila MA, Berraondo P. Emerging therapies for acute intermittent porphyria. Expert Rev Mol Med. 2016 Nov 2;18:e17. doi: 10.1017/erm.2016.18[↩]
- O’Malley R, Rao G, Stein P, Bandmann O. Porphyria: often discussed but too often missed. Pract Neurol. 2018 Oct;18(5):352-358. doi: 10.1136/practneurol-2017-001878[↩]
- Simon A, Pompilus F, Querbes W, Wei A, Strzok S, Penz C, Howe DL, Hungate JR, Kim JB, Agarwal S, Marquis P. Patient Perspective on Acute Intermittent Porphyria with Frequent Attacks: A Disease with Intermittent and Chronic Manifestations. Patient. 2018 Oct;11(5):527-537. doi: 10.1007/s40271-018-0319-3[↩]
- Pallet N, Mami I, Schmitt C, Karim Z, François A, Rabant M, Nochy D, Gouya L, Deybach JC, Xu-Dubois Y, Thervet E, Puy H, Karras A. High prevalence of and potential mechanisms for chronic kidney disease in patients with acute intermittent porphyria. Kidney Int. 2015 Aug;88(2):386-95. doi: 10.1038/ki.2015.97[↩]
- Sardh E, Andersson DE, Henrichson A, Harper P. Porphyrin precursors and porphyrins in three patients with acute intermittent porphyria and end-stage renal disease under different therapy regimes. Cell Mol Biol (Noisy-le-grand). 2009 Feb 16;55(1):66-71.[↩]
- Ramanujam VS, Anderson KE. Porphyria Diagnostics-Part 1: A Brief Overview of the Porphyrias. Curr Protoc Hum Genet. 2015 Jul 1;86:17.20.1-17.20.26. doi: 10.1002/0471142905.hg1720s86[↩]
- Besur S, Schmeltzer P, Bonkovsky HL. Acute Porphyrias. J Emerg Med. 2015 Sep;49(3):305-12. doi: 10.1016/j.jemermed.2015.04.034[↩][↩]
- Stewart MF. Review of hepatocellular cancer, hypertension and renal impairment as late complications of acute porphyria and recommendations for patient follow-up. J Clin Pathol. 2012 Nov;65(11):976-80. doi: 10.1136/jclinpath-2012-200791[↩]
- Bissell DM, Anderson KE, Bonkovsky HL. Porphyria. N Engl J Med. 2017 Nov 23;377(21):2101. doi: 10.1056/NEJMc1712682[↩]
- Stein PE, Badminton MN, Rees DC. Update review of the acute porphyrias. Br J Haematol. 2017 Feb;176(4):527-538. doi: 10.1111/bjh.14459[↩][↩]
- Nguyen TP, Taylor RS. Guillain-Barre Syndrome. [Updated 2023 Feb 7]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK532254[↩]
- Hadden RD, Cornblath DR, Hughes RA, Zielasek J, Hartung HP, Toyka KV, Swan AV. Electrophysiological classification of Guillain-Barré syndrome: clinical associations and outcome. Plasma Exchange/Sandoglobulin Guillain-Barré Syndrome Trial Group. Ann Neurol. 1998 Nov;44(5):780-8. doi: 10.1002/ana.410440512[↩]
- Rocha Cabrero F, Morrison EH. Miller Fisher Syndrome. [Updated 2023 Jun 26]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK507717[↩]
- McKhann GM, Cornblath DR, Griffin JW, Ho TW, Li CY, Jiang Z, Wu HS, Zhaori G, Liu Y, Jou LP, et al. Acute motor axonal neuropathy: a frequent cause of acute flaccid paralysis in China. Ann Neurol. 1993 Apr;33(4):333-42. doi: 10.1002/ana.410330402[↩]
- Hafer-Macko C, Hsieh ST, Li CY, Ho TW, Sheikh K, Cornblath DR, McKhann GM, Asbury AK, Griffin JW. Acute motor axonal neuropathy: an antibody-mediated attack on axolemma. Ann Neurol. 1996 Oct;40(4):635-44. doi: 10.1002/ana.410400414[↩]
- Roveri G, Nascimbeni F, Rocchi E, Ventura P. Drugs and acute porphyrias: reasons for a hazardous relationship. Postgrad Med. 2014 Nov;126(7):108-20. doi: 10.3810/pgm.2014.11.2839[↩]
- Lissing M, Nowak G, Adam R, Karam V, Boyd A, Gouya L, Meersseman W, Melum E, Ołdakowska-Jedynak U, Reiter FP, Colmenero J, Sanchez R, Herden U, Langendonk J, Ventura P, Isoniemi H, Boillot O, Braun F, Perrodin S, Mowlem E, Wahlin S; European Liver and Intestine Transplant Association. Liver Transplantation for Acute Intermittent Porphyria. Liver Transpl. 2021 Apr;27(4):491-501. doi: 10.1002/lt.25959[↩][↩][↩]
- Dowman JK, Gunson BK, Bramhall S, Badminton MN, Newsome PN. Liver transplantation from donors with acute intermittent porphyria. Ann Intern Med. 2011 Apr 19;154(8):571-2. doi: 10.7326/0003-4819-154-8-201104190-00015. Erratum in: Ann Intern Med. 2011 Apr 19;154(8):572. Erratum in: Ann Intern Med. 2011 Jun 21;154(12):848.[↩]
- Pallet N, Karras A, Thervet E, Gouya L, Karim Z, Puy H. Porphyria and kidney diseases. Clin Kidney J. 2018 Apr;11(2):191-197. doi: 10.1093/ckj/sfx146[↩]
- Wahlin S, Harper P, Sardh E, Andersson C, Andersson DE, Ericzon BG. Combined liver and kidney transplantation in acute intermittent porphyria. Transpl Int. 2010 Jun;23(6):e18-21. doi: 10.1111/j.1432-2277.2009.01035.x[↩]
- Schulenburg-Brand D, Gardiner T, Guppy S, Rees DC, Stein P, Barth J, Felicity Stewart M, Badminton M. An Audit of the Use of Gonadorelin Analogues to Prevent Recurrent Acute Symptoms in Patients with Acute Porphyria in the United Kingdom. JIMD Rep. 2017;36:99-107. doi: 10.1007/8904_2017_2[↩]
- Johansson A, Möller C, Fogh J, Harper P. Biochemical characterization of porphobilinogen deaminase-deficient mice during phenobarbital induction of heme synthesis and the effect of enzyme replacement. Mol Med. 2003 Sep-Dec;9(9-12):193-9. doi: 10.2119/2004-00002.johansson[↩]
- Sardh E, Rejkjaer L, Andersson DE, Harper P. Safety, pharmacokinetics and pharmocodynamics of recombinant human porphobilinogen deaminase in healthy subjects and asymptomatic carriers of the acute intermittent porphyria gene who have increased porphyrin precursor excretion. Clin Pharmacokinet. 2007;46(4):335-49. doi: 10.2165/00003088-200746040-00006[↩]
- Prieto J, Gonzalez-Aseguinolaza G. Acute Intermittent Porphyria: Novel Etiologic and Pathogenic Therapies Based on RNA Transfer to the Liver. Hepatology. 2019 Sep;70(3):1061-1063. doi: 10.1002/hep.30678[↩]
- Vassiliou D, Lempessi C, Harper P, Sardh E. Challenges in the management of acute intermittent porphyria with recurrent attacks during pregnancy: A case report. Clin Case Rep. 2020 Jul 30;8(12):2483-2487. doi: 10.1002/ccr3.3185[↩]
- Pischik E, Kauppinen R. An update of clinical management of acute intermittent porphyria. Appl Clin Genet. 2015 Sep 1;8:201-14. doi: 10.2147/TACG.S48605[↩]
- Lissing M, Vassiliou D, Floderus Y, Harper P, Yan J, Hagström H, Sardh E, Wahlin S. Risk for incident comorbidities, nonhepatic cancer and mortality in acute hepatic porphyria: A matched cohort study in 1244 individuals. J Inherit Metab Dis. 2023 Mar;46(2):286-299. doi: 10.1002/jimd.12583[↩]
- Kauppinen R, Mustajoki P. Prognosis of acute porphyria: occurrence of acute attacks, precipitating factors, and associated diseases. Medicine (Baltimore). 1992 Jan;71(1):1-13.[↩]





{kind=link}