Contents
- What is hyperbilirubinemia
- What is bilirubin?
- Hyperbilirubinemia in newborn
- Risk factors for developing neonatal hyperbilirubinemia
- Hyperbilirubinemia in a newborn symptoms
- Hyperbilirubinemia in newborn complications
- Hyperbilirubinemia in newborn prevention
- How is neonatal hyperbilirubinemia diagnosed?
- Neonatal Hyperbilirubinemia Treatment
- Table 1. Bilirubin threshold table for the management of babies of 38 weeks or more gestational age with hyperbilirubinemia
- Phototherapy
- Fiber optic blanket
- Exchange transfusion
- Intravenous immunoglobulin (IVIg)
- Feeding with breastmilk
- Supplemental feedings
- Treating any underlying cause of the hyperbilirubinemia
- Neonatal Hyperbilirubinemia Prognosis
- Hyperbilirubinemia causes
- Hyperbilirubinemia signs and symptoms
- Hyperbilirubinemia diagnosis
- Hyperbilirubinemia treatment
- Hyperbilirubinemia prognosis
What is hyperbilirubinemia
Hyperbilirubinemia is a medical condition characterized by elevated levels of bilirubin (an orange-yellow pigment formed in the liver by the breakdown of hemoglobin) in the blood, which can cause jaundice, a yellowing of the skin, eyes, and mucous membranes 1, 2, 3, 4, 5, 6, 7, 8, 9. Hyperbilirubinemia occurs when the body produces too much bilirubin or the liver cannot process it efficiently, leading to its accumulation. Jaundice is evident when the serum bilirubin level exceeds 3mg/dL. More than 80% of newborn infants experience jaundice or neonatal hyperbilirubinemia as a result of elevated bilirubin during the first few weeks after birth. In most cases, hyperbilirubinemia in newborn is physiologic and temporary, but persistent and extreme elevations can lead to serious long-term complications, such as kernicterus. The irreversible outcome of brain damage from kernicterus is rare (1 out of 100,000 infants) in high-income countries such as the United States 4. In adults, hyperbilirubinemia can indicate underlying liver, gallbladder, or blood cell diseases.
Hyperbilirubinemia causes
- Hyperbilirubinemia in newborn also called neonatal hyperbilirubinemia: The most common cause is physiological jaundice, as a newborn’s immature liver cannot process bilirubin quickly enough. Increased red blood cell breakdown in newborns also contributes.
- Pathologic causes of unconjugated hyperbilirubinemia include metabolic conditions (e.g., hypothyroidism), conditions that increase bilirubin production (e.g., cephalohematoma), and conditions that increase enterohepatic circulation (e.g., pyloric stenosis) 10.
- Conjugated hyperbilirubinemia is uncommon, occurring in about one in 2,500 infants 11, 12. Conjugated or direct bilirubin levels of 5 mg per dL (85.5 micromol/L) or greater are likely due to cholestatic causes including biliary atresia, while lesser elevations are seen in the setting of metabolic causes, hemolysis, and infections 11, 13, 14.
- Hyperbilirubinemia in adults:
- Liver disorders: Viral hepatitis, alcoholic hepatitis, cirrhosis, or liver damage can prevent the liver from processing bilirubin.
- Gallbladder disease: Gallstones obstructing the bile ducts can prevent bilirubin from being eliminated from the body.
- Blood cell breakdown: Conditions like hemolytic anemia cause excessive red blood cells to break down.
- Other factors: Certain medications or high alcohol intake can temporarily stress the liver.
Hyperbilirubinemia caused jaundice, which is yellowing of the skin, whites of the eyes (sclera), and mucous membranes. In newborns, jaundice usually appears within a few days after birth. To check for infant jaundice, press gently on your baby’s forehead or nose. If the skin looks yellow where you pressed, it’s likely your baby has mild jaundice. If your baby doesn’t have jaundice, the skin color should simply look slightly lighter than its usual color for a moment.
Most hospitals have a policy of examining babies for jaundice before discharge. The American Academy of Pediatrics recommends that 15, 10:
- Newborns be examined for jaundice during routine medical checks and at least every 12 hours while in the hospital.
- A newborn’s bilirubin levels should be checked between 24 and 48 hours after birth.
The following symptoms may suggest complications from too much bilirubin 16, 4:
- Your baby’s skin becomes more yellow.
- The skin on your baby’s belly, arms or legs looks yellow.
- The whites of your baby’s eyes look yellow.
- Your baby seems listless or sick or is hard to wake up.
- Your baby isn’t gaining weight or is feeding poorly.
- Your baby makes high-pitched cries.
- Your baby develops any other symptoms that concern you.
- In rare cases, your baby develop seizures.
The initial assessment of the patient presenting with hyperbilirubinemia (jaundice) depends on whether the hyperbilirubinemia is the result of unconjugated or conjugated bilirubin.
Two forms of bilirubin can be measured or estimated by laboratory tests:
- Unconjugated bilirubin—when heme is released from hemoglobin, it is converted to unconjugated bilirubin. It is carried by proteins to the liver. Small amounts may be present in the blood.
- Conjugated bilirubin—formed in the liver when sugars are attached (conjugated) to bilirubin. It enters the bile and passes from the liver to the small intestines and is eventually eliminated in the stool. Normally, no conjugated bilirubin is present in the blood.
Usually, a chemical test is used to first measure the total bilirubin level (unconjugated plus conjugated bilirubin). If the total bilirubin level is increased, the laboratory can use a second chemical test to detect water-soluble forms of bilirubin, called “direct” bilirubin. The direct bilirubin test provides an estimate of the amount of conjugated bilirubin present. Subtracting direct bilirubin level from the total bilirubin level helps estimate the “indirect” level of unconjugated bilirubin. The pattern of bilirubin test results can give your doctor information regarding the condition that may be present.
A urine test positive for bilirubin indicates conjugated hyperbilirubinemia. Conjugated bilirubin is soluble in water; therefore, it can be excreted via urine but not unconjugated bilirubin due to water insolubility. Furthermore, other laboratory testing should include measurement of the serum aspartate transaminase (AST), alanine transaminase (ALT), alkaline phosphatase (ALP), and gamma-glutamyl transpeptidase (GGT) levels, complete blood count (CBC) with an examination of the smear, a reticulocyte count, a direct Coombs test, lactate dehydrogenase (LDH) and haptoglobin levels 17. Jaundice, with a toxic appearance, fever, or abnormal count of white blood cells indicates sepsis that requires prompt evaluation and adequate treatment. The increased levels of aspartate transaminase (AST) and alanine transaminase (ALT) are markers of liver damage/injury. However, increased levels of alkaline phosphatase (ALP) and gamma-glutamyl transpeptidase (GGT) suggest cholestasis (a condition characterized by a reduced or stopped flow of bile from the liver, leading to a buildup of bile components like bilirubin and bile acids in the bloodstream).
A complete blood count (CBC) is a beneficial test for the determination of hemolysis, which is characterized by the presence of damaged red blood cells and increased reticulocytes on the smear. In patients, when the serum total bilirubin levels exceed 3.0 mg/dL, jaundice becomes clinically apparent. Hyperbilirubinemia is unconjugated bilirubin when the conjugated bilirubin level is less than 15% of the total bilirubin. While in conjugated hyperbilirubinemia, conjugated bilirubin level is high and more than 20% of the total bilirubin. Generally, patients with carotenemia (a harmless condition that causes a yellow-orange discoloration of the skin, most often due to excessive consumption of carotene-rich foods like carrots) also present yellow skin but have no elevation in serum bilirubin levels. During the physical examination, carotenemia due to excess carotene intake, e.g., carrots, peaches, etc., can be distinguished from jaundice due to the absence of scleral icterus in carotenemia and with the pigmentation of soles and palms and other areas. Computerized axial tomography (CT) and ultrasonography scanning are useful tools in differentiating cholestasis (intra-hepatic and extra-hepatic) from hepatocellular disease in the assessment of a patient with conjugated hyperbilirubinemia.
Noninvasive imaging modalities in persons with jaundice include ultrasound, computed tomography (CT), and magnetic resonance cholangiopancreatography (MRCP). Ultrasound or computed tomography (CT) is usually the first-line option to evaluate for obstruction, cirrhosis, and vessel patency, with ultrasonography being the least invasive and least expensive modality 18, 17. Visualization of the intra- and extrahepatic biliary tree can be further evaluated using magnetic resonance cholangiopancreatography (MRCP) or endoscopic retrograde cholangiopancreatography (ERCP), with the latter allowing for therapeutic options, such as biliary stent placement to relieve obstruction 17. Endoscopic ultrasonography can be used in addition to endoscopic retrograde cholangiopancreatography (ERCP) for evaluation of common bile duct obstructions and can help determine if the obstruction is from a mass or stone.
Liver biopsy should is reserved for cases of jaundice in which the diagnosis is unclear after the initial history and physical examination, laboratory studies, and imaging. It should be performed only if biopsy results are required to determine treatment and prognosis. Biopsy may alter care in only about one-third of cases 17.
Hyperbilirubinemia treatment depends on many factors, including treating the underlying cause of the hyperbilirubinemia, the level of bilirubin, your age and general health. The goal is to keep the level of bilirubin from increasing to dangerous levels while minimizing any negative effects of the treatment.
Hyperbilirubinemia treatment may include:
- Phototherapy. During phototherapy, the baby is placed under ultraviolet light. Phototherapy may take several hours to begin working and is used throughout the day and night. The baby’s eyes must be protected and the temperature monitored during phototherapy. Blood levels of bilirubin are checked every 6-12 hours to ensure that the phototherapy is working.
- Under special circumstances, an exchange transfusion may be needed to replace the baby’s blood with fresh blood in an attempt to rapidly decrease the bilirubin level. This is done in consultation with the neonatologist.
- Adequate hydration with breastfeeding or pumped breast milk. The American Academy of Pediatrics recommends that, if possible, breastfeeding be continued. Breastfed babies receiving phototherapy who are dehydrated or have excessive weight loss can have supplementation with expressed breast milk or formula.
- Treating any underlying cause of hyperbilirubinemia, such as infection
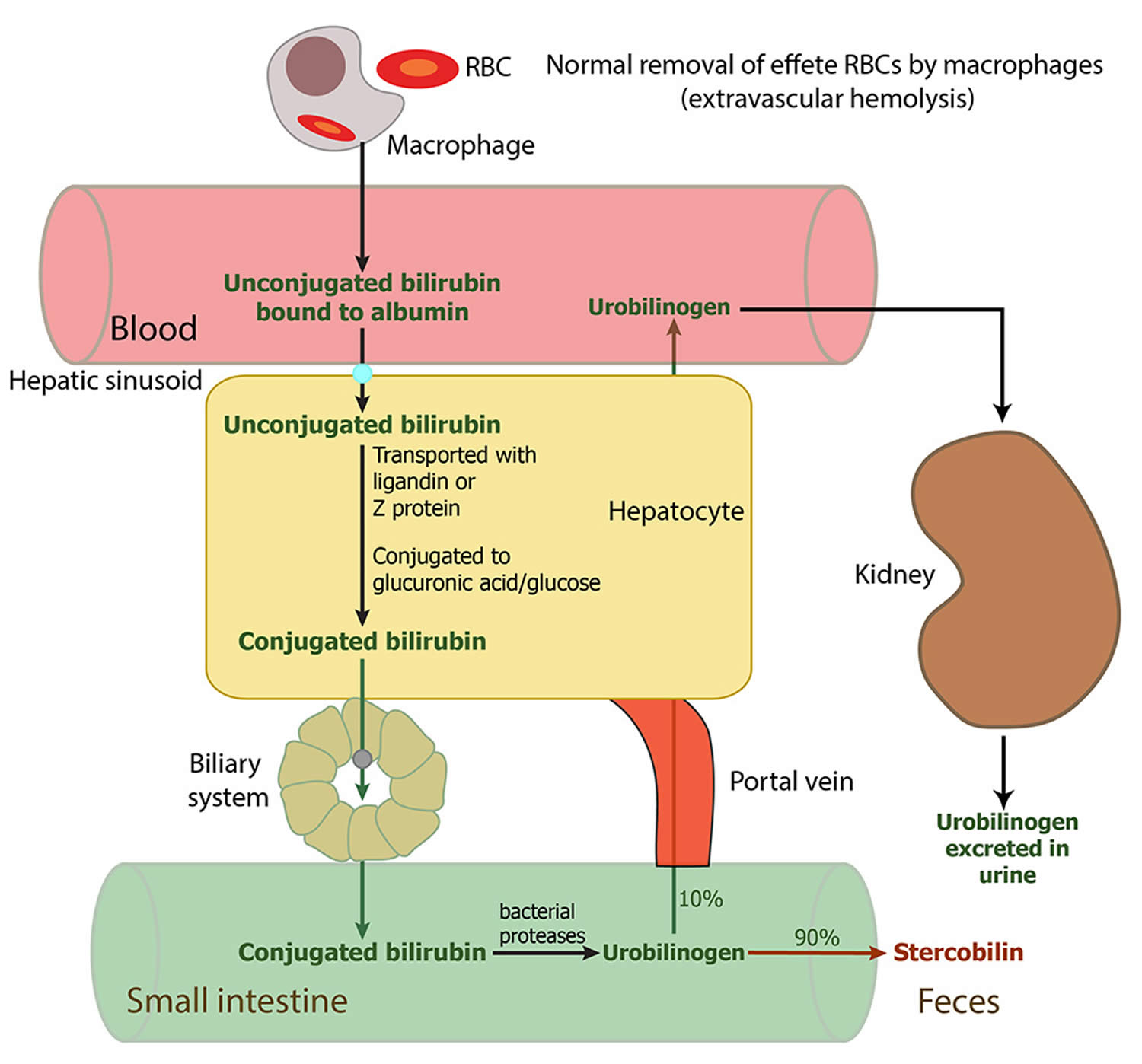
Figure 1. Hyperbilirubinemia in newborn

Figure 2. Hyperbilirubinemia in adults

What is bilirubin?
Bilirubin is an orange-yellow pigment, a waste product primarily produced by the normal breakdown of heme (ferroprotoporphyrin IX) 19, 2, 20, 21, 22. Approximately 85 percent of the heme is from the hemoglobin (Hb; an iron-containing protein in red blood cells that transports oxygen from the lungs to the body’s tissues) following the degradation of red blood cells (RBCs), while the remaining heme derives from the ineffective erythropoiesis and the breakdown of other hemoproteins such as cytochromes, myoglobin, and catalase 23.
There are 2 forms of bilirubin in the body: a toxic form called unconjugated bilirubin and a nontoxic form called conjugated bilirubin. Both forms can be measured or estimated by laboratory tests, and a total bilirubin result (a sum of these) may also be reported. Bilirubin is ultimately processed by the liver to allow its elimination from the body.
Red blood cells normally degrade after about 120 days in the blood circulation. As heme is released from hemoglobin, it is converted to bilirubin. The conversion of heme to bilirubin is a 2-step reaction, in the first step the microsomal heme oxygenase enzyme of the reticuloendothelial system (a network of phagocytic cells, including monocytes and macrophages, that is part of the immune system whose function is to engulf and destroy foreign particles, such as bacteria and toxins, and cellular debris, a process known as phagocytosis), converts heme to biliverdin, which in turn is reduced to unconjugated bilirubin (toxic form of bilirubin) by a second enzyme biliverdin reductase 24. The unconjugated bilirubin (toxic form of bilirubin) is lipophilic (dissolves readily in fats). Unconjugated bilirubin (toxic form of bilirubin) tightly bound to albumin is transported to the liver. The entry of unconjugated bilirubin into the liver has not been elucidated, and the best candidate appears to be a bilirubin transporter 2. In liver cells, unconjugated bilirubin dissociates from albumin and binds to proteins of the glutathione-S-transferases family that present it for conjugation and prevent it from effluxing from the liver 2. Next, unconjugated bilirubin gets conjugated (attached) with one or two molecules of glucuronic acid by the enzyme uridine diphospho-glucuronate glucuronosyltransferase (UGT1A1), which forms bilirubin monoglucuronide and bilirubin diglucuronide respectively 24, 25. Conjugation increases the solubility of bilirubin in plasma and thereby enhances its elimination from the body. The conjugated bilirubin (nontoxic bilirubin) is then pumped into bile via an energy-requiring process requiring the multidrug resistance-associated protein 2 (MRP2) 26. This process also reduces the ability of bilirubin to diffuse across the blood-brain barrier. Therefore, unconjugated hyperbilirubinemia can result from dysfunction of any of these conjugation steps. Conjugated bilirubin enters the bile and passes from the liver to the small intestines; there, it is further broken down by bacteria and eventually eliminated in the stool. Therefore, the breakdown products of bilirubin give stool its characteristic brown color. In newborns, inefficient conjugation of bilirubin leads to unconjugated hyperbilirubinemia (physiologic neonatal jaundice).
A small amount (approximately 250 to 350 milligrams) of bilirubin is produced daily in a normal, healthy adult. Most (85%) of bilirubin is derived from damaged or degraded red blood cells, with the remaining amount derived from the bone marrow or liver. Normally, small amounts of unconjugated bilirubin are released into the blood, but virtually no conjugated bilirubin is present.
Bilirubin concentrations tend to be slightly higher in males than females. African Americans routinely show lower bilirubin concentrations than non-African Americans. Strenuous exercise may increase bilirubin levels.
Drugs that can decrease total bilirubin include barbiturates, caffeine, penicillin, and high doses of salicylates. The drug atazanavir increases unconjugated (indirect) bilirubin.
If the bilirubin level increases in the blood, a person may appear jaundiced, with a yellowing of the skin and/or whites of the eyes. The pattern of bilirubin test results can give your doctor information regarding the condition that may be present. For example, unconjugated bilirubin may be increased when there is an unusual amount of red blood cell destruction (hemolysis) or when the liver is unable to process bilirubin (i.e., with liver diseases such as cirrhosis or inherited problems). Conversely, conjugated bilirubin can increase when the liver is able to process bilirubin but is not able to pass the conjugated bilirubin to the bile for removal; when this happens, the cause is often acute hepatitis or blockage of the bile ducts.
Increased total and unconjugated bilirubin levels are relatively common in newborns in the first few days after birth. This finding is called “physiologic jaundice of the newborn” and occurs because the newborn’s liver is not mature enough to process bilirubin yet. Usually, physiologic jaundice of the newborn resolves itself within a few days. However, in hemolytic disease of the newborn, red blood cells may be destroyed because of blood incompatibilities between the baby and the mother; in these cases, treatment may be required because high levels of unconjugated bilirubin can damage the newborn’s brain.
A rare (about 1 in 10,000 births) but life-threatening congenital condition called biliary atresia can cause increased total and conjugated bilirubin levels in newborns. This condition must be quickly detected and treated, usually with surgery, to prevent serious liver damage that may require liver transplantation within the first few years of life. Some children may require liver transplantation despite early surgical treatment.
Rare inherited disorders that cause abnormal bilirubin metabolism such as Rotor, Dubin-Johnson, and Crigler-Najjar syndromes, may also cause increased levels of bilirubin.
- Rotor syndrome is a rare, inherited genetic disorder characterized by elevated levels of bilirubin in the blood (hyperbilirubinemia). People with Rotor syndrome have a buildup of both unconjugated and conjugated bilirubin in their blood, but the majority is conjugated bilirubin 27, 28. Rotor syndrome is caused by SLCO1B1 and SLCO1B3 genes. Mutations in both SLCO1B1 and SLCO1B3 genes are required for Rotor syndrome to occur. The SLCO1B1 and SLCO1B3 genes provide instructions for making similar proteins, called organic anion transporting polypeptide 1B1 (OATP1B1) and organic anion transporting polypeptide 1B3 (OATP1B3), respectively. Both proteins are found in liver cells; they transport bilirubin and other compounds from the blood into the liver so that they can be cleared from the body. In the liver, bilirubin is dissolved in a digestive fluid called bile and then excreted from the body. In people with Rotor syndrome, jaundice is usually evident shortly after birth or in childhood and may come and go; yellowing of the whites of the eyes also called conjunctival icterus is often the only symptom. Rotor syndrome is a benign and harmless condition that typically does not require treatment and does not affect life expectancy. Jaundice may be noticeable shortly after birth or in childhood, but often it’s an incidental finding.
- Crigler–Najjar syndrome is a very rare inherited disorder in which bilirubin cannot be broken down. Mutations in the UGT1A1 gene cause Crigler-Najjar syndrome. The UGT1A1 gene provides instructions for making the bilirubin uridine diphosphate glucuronosyl transferase (bilirubin-UGT) enzyme, which is found primarily in liver cells and is necessary for the removal of bilirubin from the body. Mutations in the UGT1A1 gene that cause Crigler-Najjar syndrome result in reduced or absent function of the bilirubin-UGT enzyme. People with Crigler–Najjar Type 1 have no bilirubin uridine diphosphate glucuronosyl transferase (bilirubin-UGT) enzyme function, while people with Crigler–Najjar Type 2 have less than 20 percent of normal function. The loss of bilirubin-UGT function decreases glucuronidation of unconjugated bilirubin. Glucuronidation makes bilirubin dissolvable in water so that it can be removed from the body. This toxic unconjugated bilirubin then builds up in the body, causing unconjugated hyperbilirubinemia and jaundice. Crigler–Najjar Type 1 (CN1) is very severe, and affected individuals can die in childhood due to kernicterus, although with proper treatment, they may survive longer. Crigler–Najjar Type 2 (CN2) is less severe. People with Crigler–Najjar Type 2 are less likely to develop kernicterus, and most affected individuals survive into adulthood.
- Dubin-Johnson syndrome is a rare, inherited liver disorder characterized by an increase in conjugated bilirubin, leading to mild, chronic jaundice. Dubin-Johnson syndrome is caused by mutation in ABCC2 gene affecting the liver’s ability to excrete bilirubin, resulting in pigment deposits that make the liver appear black on medical imaging. The ABCC2 gene provides instructions for making a protein that transports certain substances out of cells so they can be released (excreted) from the body. For example, this protein transports bilirubin out of liver cells and into bile (a digestive fluid produced by the liver). Bilirubin is produced during the breakdown of old red blood cells and has an orange-yellow tint. As a result, bilirubin accumulates in the body, causing a condition called hyperbilirubinemia. The buildup of bilirubin in the body causes the yellowing of the skin and whites of the eyes in people with Dubin-Johnson syndrome. Dubin-Johnson syndrome is most often seen in Middle Eastern Jewish and Japanese people. In the Jewish population, about 60% of affected individuals also have an associated blood clotting abnormality, a prolonged prothrombin time (PT), caused by a decrease in factor VII (factor 7). In most affected people jaundice appears during adolescence or early adulthood. Infants with Dubin-Johnson syndrome typically also have enlarged livers (hepatomegaly) and a severely reduced ability to produce and release a digestive fluid called bile (cholestasis). As these children get older, their liver problems go away and they usually do not have any related health problems later in life. Jaundice is typically the only feature of Dubin-Johnson syndrome, but some people can experience weakness, mild abdominal pain, nausea, or vomiting. In most people with Dubin-Johnson syndrome, certain deposits build up in the liver but do not seem to impair liver function. The deposits make the liver appear black when viewed with medical imaging. Dubin-Johnson syndrome is benign, has a normal life expectancy, and usually requires no specific treatment, though precautions like avoiding birth control pills, alcohol, environmental factors that affect the liver, infection, pregnancy, fasting or dehydration and fatigue are recommended.
Figure 3. Bilirubin metabolism
Unconjugated bilirubin
Unconjugated bilirubin is a fat-soluble form of bilirubin that is formed during the initial chemical breakdown of hemoglobin and while being transported in the blood, is mostly bound to albumin.
Though unconjugated bilirubin may be toxic to brain development in newborns (up to 2-4 weeks of age), it does not pose the same threat to older children and adults. In older children and adults, the “blood-brain barrier” is more developed and prevents bilirubin from gaining access to brain cells. Nevertheless, elevated bilirubin strongly suggests that a medical condition is present that must be evaluated and treated.
Conjugated bilirubin
Conjugated bilirubin is a water-soluble form of bilirubin formed in the liver by the chemical addition of sugar molecules to unconjugated bilirubin; when present in the blood, conjugated bilirubin can become chemically bound to albumin, forming delta-bilirubin also known as biliprotein.
Bilirubin in urine
Bilirubin is not normally present in the urine. However, conjugated bilirubin is water-soluble and may be eliminated from the body through the urine if it cannot pass into the bile. Measurable bilirubin in the urine usually indicates blockage of liver or bile ducts, hepatitis, or some other form of liver damage and may be detectable early in disease; for this reason, bilirubin testing is integrated into common dipstick testing used for routine urinalysis.
Are some people more at genetic risk of abnormal bilirubin levels?
Several inherited chronic conditions increase bilirubin levels in the blood and include Gilbert syndrome, Dubin-Johnson syndrome, Rotor syndrome, and Crigler-Najjar syndrome. The first three are usually mild, chronic conditions that can be aggravated under certain conditions but in general cause no significant health problems. For example, Gilbert syndrome is very common; about 1 in every 6 people has this genetic abnormality, but usually people with Gilbert syndrome do not have elevated bilirubin. Crigler-Najjar syndrome is the most serious inherited condition listed; this disorder is relatively rare, and some people with it may die. Dubin-Johnson syndrome is a rare, inherited liver disorder characterized by an increase in conjugated bilirubin, leading to mild, chronic jaundice. Jaundice is typically the only feature of Dubin-Johnson syndrome, but some people can experience weakness, mild abdominal pain, nausea, or vomiting. In most people with Dubin-Johnson syndrome, certain deposits build up in the liver but do not seem to impair liver function. The deposits make the liver appear black when viewed with medical imaging. Dubin-Johnson syndrome is benign, has a normal life expectancy, and usually requires no specific treatment, though precautions like avoiding oral contraceptives are recommended.
How do you treat abnormal bilirubin levels and/or jaundice?
Treatment depends on the cause of the jaundice. In newborns, phototherapy (special light therapy), blood exchange transfusion, and/or certain drugs may be used to reduce the bilirubin level. In Gilbert, Rotor, and Dubin-Johnson syndromes, no treatment is usually necessary. Crigler-Najjar syndrome may respond to certain enzyme drug therapy or may require a liver transplant. Jaundice caused by an obstruction is often resolved by surgery. Jaundice due to cirrhosis is a result of long-term liver damage and does not respond well to any type of therapy other than liver transplantation.
When is bilirubin test ordered?
A healthcare practitioner usually orders a bilirubin test in conjunction with other liver function tests (alkaline phosphatase [ALP], aspartate aminotransferase [AST], alanine aminotransferase [ALT]) when someone shows signs of abnormal liver function.
A bilirubin level may be ordered when a person:
- Shows evidence of jaundice
- Has a history of drinking excessive amounts of alcohol
- Has suspected drug toxicity
- Has been exposed to hepatitis-causing viruses
Other symptoms that may be present include:
- Dark, amber-colored urine
- Nausea/vomiting
- Abdominal pain and/or swelling
- Fatigue and general malaise that often accompany chronic liver disease
Measuring and monitoring bilirubin in newborns with jaundice is considered standard medical care.
Tests for bilirubin may also be ordered when someone is suspected of having (or known to have) hemolytic anemia as a cause of anemia. In this case, it is often ordered along with other tests used to evaluate hemolysis, such as complete blood count, reticulocyte count, haptoglobin, and lactate dehydrogenase (LDH).
Normal bilirubin levels
Direct (conjugated) Bilirubin
- > or =12 months: 0.0-0.3 mg/dL (less than 5.1 µmol/L)
Reference values have not been established for patients who are <12 months of age.
Total Bilirubin
- 0-6 days: Refer to www.bilitool.org for information on age-specific (postnatal hour of life) serum bilirubin values.
- 7-14 days: <15.0 mg/dL
- 15 days to 17 years: < or =1.0 mg/dL
- > or =18 years: 0.1 to 1.2 mg/dL (1.71 to 20.5 µmol/L)
Normal value ranges may vary slightly among different laboratories. Some labs use different measurements or may test different samples. Talk to your provider about the meaning of your specific test results.
What does high bilirubin levels mean?
Unconjugated hyperbilirubinemia arises in one of the 3 major pathophysiologic conditions or a combination of them 18, 29, 30 31:
- Increased bilirubin production. Increased bilirubin production and consequential unconjugated hyperbilirubinemia can result from increased catabolic degradation of hemoglobin and other heme proteins, typically due to accelerated hemolysis, a large hematoma, dyserythropoiesis (e.g., megaloblastic and sideroblastic anemias), or sometimes due to destruction of transfused erythrocytes. In these conditions, patients with normal liver function efficiently conjugate and excrete the excess bilirubin. As a result, the serum levels of unconjugated bilirubin remain modest (1 to 4 mg/dL) and rarely exceed 4 mg/dL. Prolonged hemolysis can lead to severe unconjugated hyperbilirubinemia in patients with concurrent hepatic dysfunction.
- Impaired bilirubin uptake. The impaired hepatic uptake of bilirubin can be the result of decreased bilirubin delivery to the liver and inefficient uptake of bilirubin by hepatocytes, usually resulting from reduced hepatic blood flow (congestive heart failure and portosystemic shunts) and drugs/contrast administration. The unconjugated hyperbilirubinemia induced by several drugs (rifampin, flavaspidic acid, novobiocin, and various cholecystographic contrast agents), generally resolves within 48 hours of drug discontinuation 32.
- Impaired bilirubin conjugation. Impaired bilirubin conjugation can result from hereditary defects, including Gilbert syndrome and the Crigler-Najjar syndrome type 1 and 2, that cause a decrease or loss of UDP-glucuronosyltransferase (UGT1A1) activity, an enzyme responsible for conjugation of bilirubin with glucuronic acid 33. Lucy-Driscoll syndrome, also known as maternal serum jaundice, a form of transient familial neonatal unconjugated hyperbilirubinemia, is a rare metabolic disorder caused by a UGT1A1 inhibitor usually present in the maternal serum 34. Most newborns develop unconjugated hyperbilirubinemia (neonatal jaundice) because of hepatic immaturity and low activity of UGT1A1 during days 2 to 5. Breast milk feeding increases bilirubin levels in infants which results in maternal milk jaundice 35, 36. Lactation failure also results in hyperbilirubinemia due to insufficient caloric intake, which results in decreased bilirubin clearance, and increased enterohepatic circulation 37. Drugs such as novobiocin, pregnanediol, chloramphenicol, gentamycin, and several HIV protease inhibitors can induce hyperbilirubinemia by inhibiting the UGT1A1 enzyme 38. In newborns, ABO incompatibility or Rh incompatibility may lead to hyperbilirubinemia and consequently, neonatal jaundice 31.
Adults and children
Increased total bilirubin that is mainly unconjugated (indirect) bilirubin may be a result of:
- Hemolytic or pernicious anemia
- Megaloblastic anemia
- A blood disorder called erythroblastosis fetalis
- Transfusion reaction in which red blood cells that were given in a transfusion are destroyed by the person’s immune system
- Cirrhosis (scarring of the liver)
- A relatively common inherited condition called Gilbert syndrome, due to low levels of the enzyme that produces conjugated bilirubin
If conjugated (direct) bilirubin is elevated more than unconjugated (indirect) bilirubin, there typically is a problem associated with decreased elimination of bilirubin by the liver cells. Some conditions that may cause this include:
- Viral hepatitis
- Drug reactions
- Alcoholic liver disease
Conjugated (direct) bilirubin is also elevated more than unconjugated (indirect) bilirubin when there is blockage of the bile ducts. This may occur, for example, with:
- Gallstones present in the bile ducts
- Tumors
- Scarring of the bile ducts or aAbnormal narrowing of the common bile duct (biliary stricture)
- Cancer of the pancreas or gallbladder
In hepatobiliary diseases of various causes, bilirubin uptake, storage, and excretion are impaired to varying degrees. Thus, both conjugated and unconjugated bilirubin are retained and a wide range of abnormal serum concentrations of each form of bilirubin may be observed. Both conjugated and unconjugated bilirubins are increased in hepatitis and space-occupying lesions of the liver; and obstructive lesions such as carcinoma of the head of the pancreas, common bile duct, or ampulla of Vater.
Newborns
An elevated bilirubin level in a newborn may be temporary and resolve itself within a few days to two weeks. However, if the bilirubin level is above a critical threshold or increases rapidly, an investigation of the cause is needed so appropriate treatment can be initiated. Increased bilirubin concentrations may result from the accelerated breakdown of red blood cells due to:
- Blood type incompatibility between the mother and her newborn
- Certain congenital infections
- Lack of oxygen (hypoxia)
- Diseases that can affect the liver
In most of these conditions, only unconjugated (indirect) bilirubin is increased. An elevated conjugated (direct) bilirubin is seen in the rare conditions of biliary atresia and neonatal hepatitis. Biliary atresia requires surgical intervention to prevent liver damage.
Physiologic jaundice should resolve in 5 to 10 days in full-term infants and by 14 days in preterm infants.
Hyperbilirubinemia in newborn
Hyperbilirubinemia in newborn also called neonatal hyperbilirubinemia, is a medical condition in which there is a build up of bilirubin in the blood, defined as a total serum bilirubin level above 5 mg per dL (86 μmol per L), causing yellow discoloration of the eyes and skin, called jaundice. Jaundice typically results from the deposition of unconjugated bilirubin pigment in the skin and mucus membranes. Depending on the underlying cause, this condition may present throughout the neonatal period. Approximately 60% of term babies and 80% of preterm newborns develop jaundice in the first week of life, and about 10% of breastfed babies are still jaundiced at 1 month of age 39, 15, 10, 40, 41. In most babies with jaundice there is no underlying disease, and this early jaundice termed ‘physiological jaundice’ is generally harmless and does not cause any trouble and will resolve on its own in the first week of life 42. However, there are pathological causes of hyperbilirubinemia in the newborn period, which, although rare, need to be detected. Such pathological jaundice may co-exist with physiological jaundice. Hyperbilirubinemia in the newborn period can be associated with severe illnesses such as premature infants (babies born before 37 weeks’ gestation), certain blood disorders, metabolic and endocrine disorders, anatomic abnormalities of the liver, and infections 43. Although low levels of bilirubin are not usually a concern, large amounts of bilirubin can circulate to tissues in the brain and may cause seizures and brain damage. This condition is called kernicterus or bilirubin encephalopathy, which refers to the ‘yellow staining of the basal nuclei of the brain’ caused by bilirubin 44. This is seen in parts of the brain on autopsy. Poor-quality studies have shown a link between kernicterus (acute and chronic brain effects of severe hyperbilirubinemia) and both high serum bilirubin levels and free bilirubin levels in all babies.
Physiological jaundice is mild, unconjugated bilirubinemia, and affects nearly all newborns. Physiological jaundice levels typically peak at 5 to 6 mg/dL (86 to 103 micromol/L) at 72 to 96 hours of age, and do not exceed 17 to 18 mg/dL (291 to 308 micromol/L) 45. The level of bilirubinemia that results in kernicterus in a given infant is unknown. The level of bilirubinemia that causes kernicterus varies by infant, but risk increases significantly when unconjugated bilirubin levels exceed 25 to 30 mg/dL (428 to 513 micromol/L) in term or near-term infants 46, 47, 44, 48. Factors like prematurity, hypoxia, acidosis, and certain infections can lower this threshold, making some infants more vulnerable at lower bilirubin levels
Depending on the cause of the hyperbilirubinemia, jaundice may appear at birth or at any time afterward. Factors significantly associated with hyperbilirubinemia are gestational age < 38 weeks, visible jaundice within 24 hours of birth, mother’s intention to breastfeed exclusively and family history of neonatal jaundice requiring treatment with phototherapy.
Bilirubin is a natural byproduct produced when red blood cells breakdown. The adult liver converts unconjugated bilirubin into a conjugated form, that be excreted. During pregnancy, the placenta excretes bilirubin but when the baby is born, the baby’s immature liver must assume that role. There are several causes of hyperbilirubinemia and jaundice in newborn, including the following:
- Physiologic jaundice. During pregnancy, the placenta removes bilirubin from your baby’s blood. When a baby is born, the baby’s liver takes over this job. Physiologic jaundice occurs as a “normal” response to the baby’s limited ability to excrete bilirubin in the first days of life due to the immaturity of the liver. This will usually resolve by the first week of life.
- Breastfeeding failure jaundice. During the first few days of breastfeeding when the maternal breast milk supply is low and the baby is having trouble latching and feeding, the baby may become dehydrated. Since bilirubin is eliminated in the urine and stool, decreased urination and infrequent stools result in a buildup of bilirubin. While common in full term infants, premature infants and late preterm infants are more susceptible to breastfeeding failure jaundice because they may have uncoordinated suck as well as easy fatigability. Once effective breastfeeding is established, this problem will resolve.
- Breast milk jaundice. About 2 percent of breastfed babies develop jaundice after the first week. It peaks about two weeks of age and can persist up to three to twelve weeks. Breast milk jaundice is thought to be caused by glucuronidase enzyme in the breast milk that deconjugates bilirubin into unconjugated bilirubin 49. Breastfeeding can usually continue or only be interrupted briefly.
- Jaundice from breakdown of red blood cells (hemolysis). Jaundice may occur if there is an increase of red blood cell breakdown (hemolysis) such as that seen when there is a mismatch of maternal and fetal blood type, resulting in ABO incompatibility (a condition where a mother’s antibodies attack a baby’s red blood cells due to a difference in blood type, with most common type when a mother is blood type O and her baby is blood type A or B), hemolytic disease of the newborn (Rh disease) or abnormalities of the red cell itself such as hereditary spherocytosis, elliptocytosis, glucose-6-phosphate dehydrogenase deficiency (G6PD deficiency), pyruvate kinase deficiency; and hemoglobinopathies, such as alpha and beta thalassemias 50. Increased hemolysis (red blood cell breakdown) can also occur if the baby is bruised or develops a hematoma during delivery.
- Birth Trauma such as cephalohematoma (a collection of blood under the scalp that forms on a newborn’s skull, usually caused by ruptured blood vessels during childbirth), subgaleal hemorrhage (a serious, potentially life-threatening condition in newborns caused by bleeding into the space between the skull’s periosteum and the galea aponeurosis [the scalp’s tough, fibrous tissue layer]), or peripheral bruises from birth trauma 51.
- Jaundice related to inadequate liver function. Jaundice may be related to prolonged liver dysfunction due to infection and other factors.
- Disruption or Obstruction in the Biliary System.
- Hereditary Bilirubin Conjugation Defects – Crigler-Najjar syndrome and Gilbert syndrome are due to the deficiency of the enzyme uridine 5′-diphospho-glucuronosyltransferase (UDGPT), which conjugates the bilirubin in the liver cells 52.
- Rotor syndrome is a rare, inherited genetic disorder characterized by elevated levels of bilirubin in the blood (hyperbilirubinemia). People with Rotor syndrome have a buildup of both unconjugated and conjugated bilirubin in their blood, but the majority is conjugated bilirubin 27, 28. Rotor syndrome is caused by SLCO1B1 and SLCO1B3 genes. Mutations in both SLCO1B1 and SLCO1B3 genes are required for Rotor syndrome to occur. The SLCO1B1 and SLCO1B3 genes provide instructions for making similar proteins, called organic anion transporting polypeptide 1B1 (OATP1B1) and organic anion transporting polypeptide 1B3 (OATP1B3), respectively. Both proteins are found in liver cells; they transport bilirubin and other compounds from the blood into the liver so that they can be cleared from the body. In the liver, bilirubin is dissolved in a digestive fluid called bile and then excreted from the body. In people with Rotor syndrome, jaundice is usually evident shortly after birth or in childhood and may come and go; yellowing of the whites of the eyes also called conjunctival icterus is often the only symptom. Rotor syndrome is a benign and harmless condition that typically does not require treatment and does not affect life expectancy. Jaundice may be noticeable shortly after birth or in childhood, but often it’s an incidental finding.
- Crigler–Najjar syndrome is a very rare inherited disorder in which bilirubin cannot be broken down. Mutations in the UGT1A1 gene cause Crigler-Najjar syndrome. The UGT1A1 gene provides instructions for making the bilirubin uridine diphosphate glucuronosyl transferase (bilirubin-UGT) enzyme, which is found primarily in liver cells and is necessary for the removal of bilirubin from the body. Mutations in the UGT1A1 gene that cause Crigler-Najjar syndrome result in reduced or absent function of the bilirubin-UGT enzyme. People with Crigler–Najjar Type 1 have no bilirubin uridine diphosphate glucuronosyl transferase (bilirubin-UGT) enzyme function, while people with Crigler–Najjar Type 2 have less than 20 percent of normal function. The loss of bilirubin-UGT function decreases glucuronidation of unconjugated bilirubin. Glucuronidation makes bilirubin dissolvable in water so that it can be removed from the body. This toxic unconjugated bilirubin then builds up in the body, causing unconjugated hyperbilirubinemia and jaundice. Crigler–Najjar Type 1 (CN1) is very severe, and affected individuals can die in childhood due to kernicterus, although with proper treatment, they may survive longer. Crigler–Najjar Type 2 (CN2) is less severe. People with Crigler–Najjar Type 2 are less likely to develop kernicterus, and most affected individuals survive into adulthood.
- Dubin-Johnson syndrome is a rare, inherited liver disorder characterized by an increase in conjugated bilirubin, leading to mild, chronic jaundice. Dubin-Johnson syndrome is caused by mutation in ABCC2 gene affecting the liver’s ability to excrete bilirubin, resulting in pigment deposits that make the liver appear black on medical imaging. The ABCC2 gene provides instructions for making a protein that transports certain substances out of cells so they can be released (excreted) from the body. For example, this protein transports bilirubin out of liver cells and into bile (a digestive fluid produced by the liver). Bilirubin is produced during the breakdown of old red blood cells and has an orange-yellow tint. As a result, bilirubin accumulates in the body, causing a condition called hyperbilirubinemia. The buildup of bilirubin in the body causes the yellowing of the skin and whites of the eyes in people with Dubin-Johnson syndrome. Dubin-Johnson syndrome is most often seen in Middle Eastern Jewish and Japanese people. In the Jewish population, about 60% of affected individuals also have an associated blood clotting abnormality, a prolonged prothrombin time (PT), caused by a decrease in factor VII (factor 7). In most affected people jaundice appears during adolescence or early adulthood. Infants with Dubin-Johnson syndrome typically also have enlarged livers (hepatomegaly) and a severely reduced ability to produce and release a digestive fluid called bile (cholestasis). As these children get older, their liver problems go away and they usually do not have any related health problems later in life. Jaundice is typically the only feature of Dubin-Johnson syndrome, but some people can experience weakness, mild abdominal pain, nausea, or vomiting. In most people with Dubin-Johnson syndrome, certain deposits build up in the liver but do not seem to impair liver function. The deposits make the liver appear black when viewed with medical imaging. Dubin-Johnson syndrome is benign, has a normal life expectancy, and usually requires no specific treatment, though precautions like avoiding birth control pills, alcohol, environmental factors that affect the liver, infection, pregnancy, fasting or dehydration and fatigue are recommended.
- Neonatal polycythemia also called polycythemia in newborns is a condition where there are too many red blood cells, defined by a venous hematocrit greater than 65% 53, 54, 55. Polycythemia means there are too many red blood cells (RBCs) in an infant’s blood. Polycythemia in newborn can lead to increased blood viscosity and decreased blood flow, causing symptoms like lethargy, poor feeding, and respiratory distress. Causes of polycythemia in newborn include delayed cord clamping, twin-to-twin transfusion, and intrauterine hypoxia. Treatment may involve fluid administration for mild cases or a partial exchange transfusion for more severe cases.
- Hypoalbuminemia is a condition where the level of albumin, a protein in the blood, is abnormally low. Unconjugated bilirubin is lipid-soluble and is normally bound to albumin; a decrease in the albumin level leads to an increase in free unconjugated bilirubin level 56.
- Infection: Congenital infections (eg, syphilis, toxoplasmosis, HIV, herpes virus, and rubella) should be included in the differential diagnosis of neonatal cholestasis, especially when stigmata of congenital infection, including growth restriction, coagulopathy, skin rash, or thrombocytopenia, are present. Cytomegalovirus (CMV) is also a common congenital infection with many manifestations. Most infected newborns are asymptomatic, but hepatomegaly and conjugated hyperbilirubinemia may indicate liver involvement 57. Carefully reviewing maternal history, specific serologies, and viral culture results aid diagnosis. Urine and blood cultures are also a component of the diagnostic evaluation, as urinary tract infections and septicemia can cause conjugated hyperbilirubinemia in neonates. Additionally, microcirculatory changes in the liver, a direct effect of bacterial products, and toxins released by bacteria are thought to be the possible mechanisms of cholestasis in patients with urinary tract infection (UTI) 58.
Prematurity, hemolytic disease of the newborn and glucose-6-phosphate dehydrogenase (G6PD) deficiency are the most common risk factors 48, 59. Newborns who develop neurological complications of hyperbilirubinemia usually have at least two neurotoxicity risk factors 60. There is no clear correlation between bilirubin level alone and the risk of developing brain toxicity 61, 50.
The timing of when your child’s jaundice first starts matters. It may help their your baby’s doctor make a diagnosis.
- First 24 hours. This type of jaundice is often serious. Your child will likely need treatment right away.
- Second or third day. This is often physiologic jaundice. Sometimes it can be a more serious type of jaundice. It’s important to be sure the baby is getting enough milk at this point.
- Toward the end of the first week. This type of jaundice may be from breastmilk jaundice but may be due to an infection or other rare, serious problems.
- In the second week. This is often caused by breastmilk jaundice but may be caused by rare liver problems.
In the United States Kernicterus Registry, 56% had abnormalities known to increase the bilirubin concentration in the blood. Glucose-6-phosphate dehydrogenase deficiency (G6PD deficiency) was diagnosed in 21.3%, severe hemolytic processes were recognized in 20.5%, birth trauma was identified in 15%, and other causes such as galactosemia, Crigler-Najjar syndrome, and sepsis were diagnosed in 7% 44. However, no cause was identified in 43.4% of the infants 62.
Severe jaundice requiring exchange transfusion (bilirubin > 340 micromol/liter) and early onset of jaundice (within 24 hours) are statistically significant risk factors for hearing loss 39, 63. Hemolytic disorders such as G6PD deficiency and ABO incompatibility (ABO incompatible blood) may cause a rapid increase in bilirubin level, and these disorders have been over-represented in international kernicterus registries and population studies of significant hyperbilirubinemia. A study of low-birthweight babies found a weak association between high serum bilirubin levels (> 340 micromol/L) and neurodevelopmental impairment, hearing impairment and psychomotor impairment.
Rarely, bilirubin crosses the blood-brain barrier (BBB) and can cause serious consequences 4. One study performed in Canada found that acute bilirubin encephalopathy occurs in approximately 1 out of 10,000 infants 64. Symptoms include lethargy, hypotonia or hypertonia, back and neck arching, irritability, and high-pitched crying 64, 65. Acute bilirubin encephalopathy fully resolves in most cases but can progress to kernicterus 50, 11.
Complications of kernicterus include 67, 68, 69:
- Hearing loss – most common abnormality
- Extrapyramidal symptoms like athetosis and chorea
- Visual abnormalities including gaze palsies
- Abnormalities in dentition
Because of the serious and irreversible complications of kernicterus, it is important to be aware of risk factors for neurotoxicity and routinely examine newborns for jaundice.
Risk factors for developing neonatal hyperbilirubinemia
Major risk factors for jaundice, particularly severe jaundice that can cause complications, include the following 70:
- Premature birth. A baby born before 37 weeks of gestation may not be able to process bilirubin as quickly as full-term babies do. Premature babies also may feed less and have fewer bowel movements, resulting in less bilirubin removed through stool.
- Jaundice at less than 24 hours of life.
- Significant bruising or scalp hematoma during birth. Newborns who become bruised during delivery may have higher levels of bilirubin from the breakdown of more red blood cells.
- Blood type. If the mother’s blood type is different from her baby’s, the baby may have received antibodies through the placenta that cause rapid breakdown of red blood cells.
- Exclusive breastfeeding with suboptimal intake. Babies who are breastfed, particularly those who have difficulty nursing or getting enough nutrition from breastfeeding, are at higher risk of jaundice. Dehydration or a low caloric intake may contribute to the onset of jaundice. However, because of the benefits of breastfeeding, experts still recommend it. It’s important to make sure your baby gets enough to eat and is adequately hydrated.
- A family history of certain blood disorders. Having a family member with certain blood conditions, such as glucose-6-phosphate dehydrogenase [G6PD] deficiency, increases a baby’s risk of having jaundice.
- A parent or sibling who was treated for jaundice. If a family member had jaundice, your baby’s risk of jaundice is higher.
- Family history of a sibling or parent who required phototherapy or exchange transfusion.
- Down syndrome. Newborns with Down syndrome have a higher risk of developing serious jaundice.
- Being a larger-than-average baby with a mother who has diabetes. Larger babies are commonly associated with diabetic pregnancies. Jaundice happens in 10% to 30% of babies of mothers with diabetes. The risk is even higher in babies born before 37 weeks’ gestation.
- Predischarge total serum bilirubin close to the phototherapy threshold.
- Evidence of hemolysis or rapidly rising total serum bilirubin.
- Phototherapy before hospital discharge.
Hyperbilirubinemia in a newborn symptoms
Yellowing of the skin and the whites of the eyes, the main sign of infant jaundice, usually appears within a few days after birth. To check for infant jaundice, press gently on your baby’s forehead or nose. If the skin looks yellow where you pressed, it’s likely your baby has mild jaundice. If your baby doesn’t have jaundice, the skin color should simply look slightly lighter than its usual color for a moment. Examine your baby in good lighting conditions, preferably in natural daylight.
Hyperbilirubinemia symptoms can occur a bit differently in each child. They can include:
- Yellowing of your baby’s skin and the whites of their eyes (jaundice). This often starts on a baby’s face and moves down their body.
- Poor feeding
- Lack of energy
The symptoms of hyperbilirubinemia may be similar to symptoms of other conditions. Make sure your child sees a doctor for a diagnosis.
Most hospitals have a policy of examining babies for jaundice before discharge. The American Academy of Pediatrics recommends that 15, 10:
- Newborns be examined for jaundice during routine medical checks and at least every 12 hours while in the hospital.
- A newborn’s bilirubin levels should be checked between 24 and 48 hours after birth.
The following symptoms may suggest complications from too much bilirubin 16, 4:
- Your baby’s skin becomes more yellow.
- The skin on your baby’s belly, arms or legs looks yellow.
- The whites of your baby’s eyes look yellow.
- Your baby seems listless or sick or is hard to wake up.
- Your baby isn’t gaining weight or is feeding poorly.
- Your baby makes high-pitched cries.
- Your baby develops any other symptoms that concern you.
- In rare cases, your baby develop seizures.
Hyperbilirubinemia in newborn complications
High levels of bilirubin that cause severe jaundice can cause serious complications if not treated.
Acute bilirubin encephalopathy
Bilirubin is toxic to cells of the brain. If a baby has severe jaundice, there’s a risk of bilirubin passing into the brain, a condition called acute bilirubin encephalopathy 5. Prompt treatment may prevent significant lasting damage.
Bilirubin encephalopathy is a rare neurological condition that occurs in some newborns with severe jaundice due to severe unconjugated hyperbilirubinemia 5. Bilirubin encephalopathy is a serious condition. Many infants with late-stage nervous system complications die.
Bilirubin encephalopathy most often develops in the first week of life, but may be seen up until the third week. Some newborns with Rh hemolytic disease are at high risk for severe jaundice that can lead to this condition. Rarely, bilirubin encephalopathy can develop in seemingly healthy babies.
Signs of acute bilirubin encephalopathy in a baby with jaundice include:
- Listlessness.
- Difficulty waking.
- High-pitched crying.
- Poor sucking or feeding.
- Backward arching of the neck and body.
- Fever.
The signs and symptoms of bilirubin encephalopathy in neonates with severe unconjugated hyperbilirubinemia depend on when the symptoms appear. The level at which unconjugated bilirubin becomes neurotoxic is unclear, and kernicterus has been reported in infants without markedly elevated bilirubin levels on autopsy. There are 3 phases of acute bilirubin encephalopathy, including:
Phase 1: The symptoms of phase 1 appear during the first 1 to 2 days of illness and are notable for poor feeding, lethargy, hypotonia, irritability, or frank seizures.
Early stage symptoms:
- Extreme jaundice
- Absent startle reflex
- Poor feeding or sucking
- Extreme sleepiness (lethargy) and low muscle tone (hypotonia)
Phase 2: If infants continue to deteriorate, they progress to phase 2, characterized by increased extensor muscle tone, exhibiting opisthotonus and retrocollis. This typically occurs during the middle of the first week of illness.
Middle stage:
- High-pitched cry
- Irritability
- May have arched back with neck hyperextended backwards, high muscle tone (hypertonia)
- Poor feeding
Phase 3: After the first week, muscle rigidity, stupor or coma, apnea, or seizures may occur.
Late stage:
- Stupor or coma
- No feeding
- Shrill cry
- Muscle rigidity, markedly arched back with neck hyperextended backwards
- Seizures.
Kernicterus
Kernicterus is the syndrome that happens if acute bilirubin encephalopathy causes permanent damage to the brain 71. Extreme hyperbilirubinemia (total bilirubin of 25 to 30 mg/dL) can cause kernicterus. Kernicterus is usually characterized by the deposition of unconjugated bilirubin (yellow stain) in brain cells. Neuronal necrosis or damage occurs in the basal ganglia, hippocampus, hypothalamic nuclei, diencephalon, midbrain responsible for neurohumoral and electrolyte control, brainstem nuclei accounting for oculomotor and auditory function, and in the cerebellum depositing as a bilirubin-phosphatidylcholine precipitate. Vision, hearing, speech, cognition, gait, and language are typically affected 72, 73, 74, 75. Kernicterus clinical features include cerebral palsy, deafness, seizures, abnormalities of the gaze, and hypoplasia of the dental enamel 71.
The symptoms depend on the stage of bilirubin encephalopathy. Not all babies with kernicterus on autopsy have had definite symptoms.
Kernicterus usually present in 2 forms, depending on the timing of symptoms 31:
- In the first year: These patients present with hypotonia, exaggerated deep tendon reflexes, obligatory tonic neck reflexes, and delayed motor milestones.
- Beyond the first year: Patients exhibit movement disorders, most commonly choreo-athetoid cerebral palsy, dental enamel hypoplasia, upward gaze abnormality, and sensorineural hearing loss.
Kernicterus may result in:
- Permanent brain damage
- Movements that are not controlled or intended, known as athetoid cerebral palsy.
- Permanent upward gaze.
- Hearing loss.
- Improper development of tooth enamel.
- Death.
Hyperbilirubinemia in newborn prevention
Pregnant women should be screened with Rhesus factor (Rh factor) and treated appropriately. Rhesus factor (Rh factor) is a type of protein on the outside or surface of your red blood cells. You inherit the Rh protein, which means you get your Rh factor from your biological parents. If you have the Rh protein, you’re Rh-positive (Rh+). If you don’t have the Rh protein, you’re Rh-negative. The majority of people, about 85%, are Rh-positive (Rh+). During pregnancy, complications may occur if a mother is Rh-negative and the fetus is Rh-positive (Rh+). This is called Rh factor incompatibility. With Rh incompatibility, a mother who is Rh-negative reacts to this difference known as incompatibility and creates antibodies. These antibodies drive an immune system attack against the fetus’s red blood cells that are Rh-positive (Rh+), which a mother who is Rh-negative thinks are foreign objects. This is called Rh sensitization. Obstetricians (physicians who specialize in delivering babies) can prevent this from happening by giving you a shot (injection) of immune globulin called Rh immune globulin (RhIg or RhoGAM®). Rh immune globulin (RhIg or RhoGAM®) is a medication that stops a mother who is Rh-negative from making Rh antibodies. It’s only helpful if your body hasn’t already made Rh antibodies. You receive it as a shot (injection). Rh immunoglobulin shots are usually very successful in treating Rh-incompatibility during pregnancy. Detecting Rh incompatibility early in pregnancy is the best way to prevent serious complications.
If a mother who is Rh-negative already has Rh antibodies, the fetus is at risk for Rh disease. Since Rh immune globulin won’t be helpful, the best treatment is close monitoring for the remainder of your pregnancy. There’s a small chance your obstetrician will want to deliver early, but this depends on how severe the fetus’s Rh disease is.
During pregnancy, a mother don’t share blood with the fetus she’s carrying. However, a small amount of blood from the fetus can mix with a mother’s blood during labor and delivery (either vaginal or cesarean). It can also happen during:
- Tests like amniocentesis and chorionic villus sampling (CVS).
- Any type of vaginal bleeding during pregnancy.
- Injury or trauma to your abdomen.
- Early pregnancy complications like miscarriage or ectopic pregnancy.
- After external cephalic version, a maneuver to turn a breech baby.
Rh incompatibility doesn’t affect the pregnant woman. In a fetus, Rh disease can cause hemolytic anemia. Hemolytic anemia destroys the fetus’s red blood cells faster than it can replace them.
The effects of Rh incompatibility can range from mild to severe. These effects may also include:
- Jaundice.
- Liver failure.
- Heart failure.
- Stillbirth.
For mild Rh disease, the fetus may not need any treatment. Most fetuses recover fully if they have a mild case of Rh disease.
For severe Rh disease cases, the fetus may receive a blood transfusion. This procedure helps replace its red blood cells. Doctors can use special lights to help reduce bilirubin levels in fetuses that have jaundice. You may need to give birth early to avoid serious complications of hemolytic anemia.
Since the development of Rh immune globulin injections, Rh disease occurs infrequently.
Because suboptimal feeding plays a role in developing hyperbilirubinemia, all breastfeeding mothers should receive support to promote adequate feeding. Breastfeeding within the first hour of life is recommended, followed by on-demand nursing at least 8 times daily. Furthermore, staff should visually assess all hospitalized neonates for jaundice at least every 12 hours. The AAP guidelines recommend universal bilirubin screening before discharge with total serum bilirubin 70.
For all babies, diagnosing jaundice early and getting treatment right away are key. This can stop your baby’s bilirubin levels from rising to dangerous levels.
Treating jaundice or conditions that may lead to it can help prevent neonatal hyperbilirubinemia. Infants with the first signs of jaundice have bilirubin level measured within 24 hours. If the level is high, the infant should be screened for diseases that involve the destruction of red blood cells (hemolysis).
The best preventive of infant jaundice is adequate feeding. Feedings should start within the first hour of life and continue at least every 2 or 3 hours, or sooner if the baby shows signs of wanting to eat. The more premature the baby, the more likely they are to need supplements of expressed milk or formula at first. Make sure you feed your baby early and often. Breastfed infants should have 8 to 12 feedings a day for the first several days of life.
All newborns have a follow-up appointment within 2 to 3 days after leaving the hospital. This is very important for late preterm or early term babies (born more than 2 to 3 weeks before their due date).
How is neonatal hyperbilirubinemia diagnosed?
A doctor will likely diagnose infant jaundice by checking your baby’s appearance. However, clinical assessment is unreliable, especially if a newborn has received phototherapy or has dark skin 76. Therefore, clinically significant jaundice should always be confirmed by measuring the level of bilirubin in your baby’s blood 5. The level of bilirubin can show how serious the jaundice is and help decide the course of treatment.
The timing of the appearance of jaundice helps with the diagnosis. Jaundice appearing in the first 12 to 24 hours can be serious and may require early treatment. When jaundice appears on the second or third day, it is usually “physiologic” or related to dehydration. Your baby’s doctor will usually rely on a bilirubin tool or graph to decide when the level of bilirubin becomes dangerous as infants who are a few days old can tolerate higher levels of bilirubin compared to an infant who is less than 48 hours old. When jaundice appears toward the end of the first week, it may be due to an infection. Later appearance of jaundice in the second week, is often related to breast milk feedings, but may have other causes.
Diagnostic procedures for neonatal hyperbilirubinemia may include:
- Direct and indirect bilirubin levels. A blood test can determine if the bilirubin is bound with other substances by the liver so that it can be excreted (direct), or is circulating in the blood circulation (indirect). Normal physiologic jaundice has indirect bilirubin. Jaundice due to more serious problems can have high levels of either type of bilirubin.
- Red blood cell count may be used to determine if the baby has too many or too few red blood cells.
- Reticulocyte count determines the number of young red blood cells, which is an indication of red blood cell production.
- Blood type and testing for ABO or Rh incompatibility (Coombs test).
Figure 4. Hyperbilirubinemia threshold graph for babies
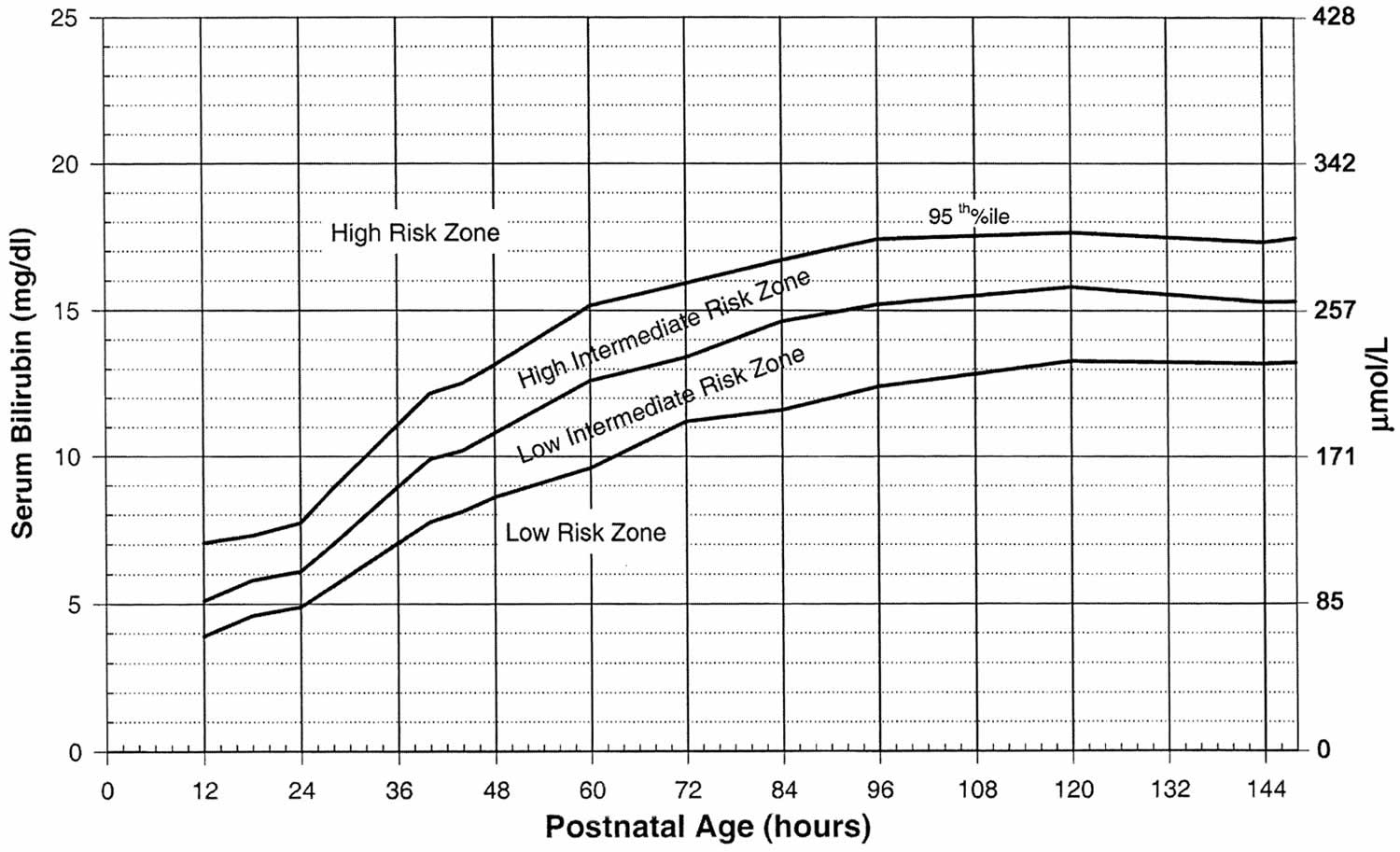 [Source 77 ]
[Source 77 ]
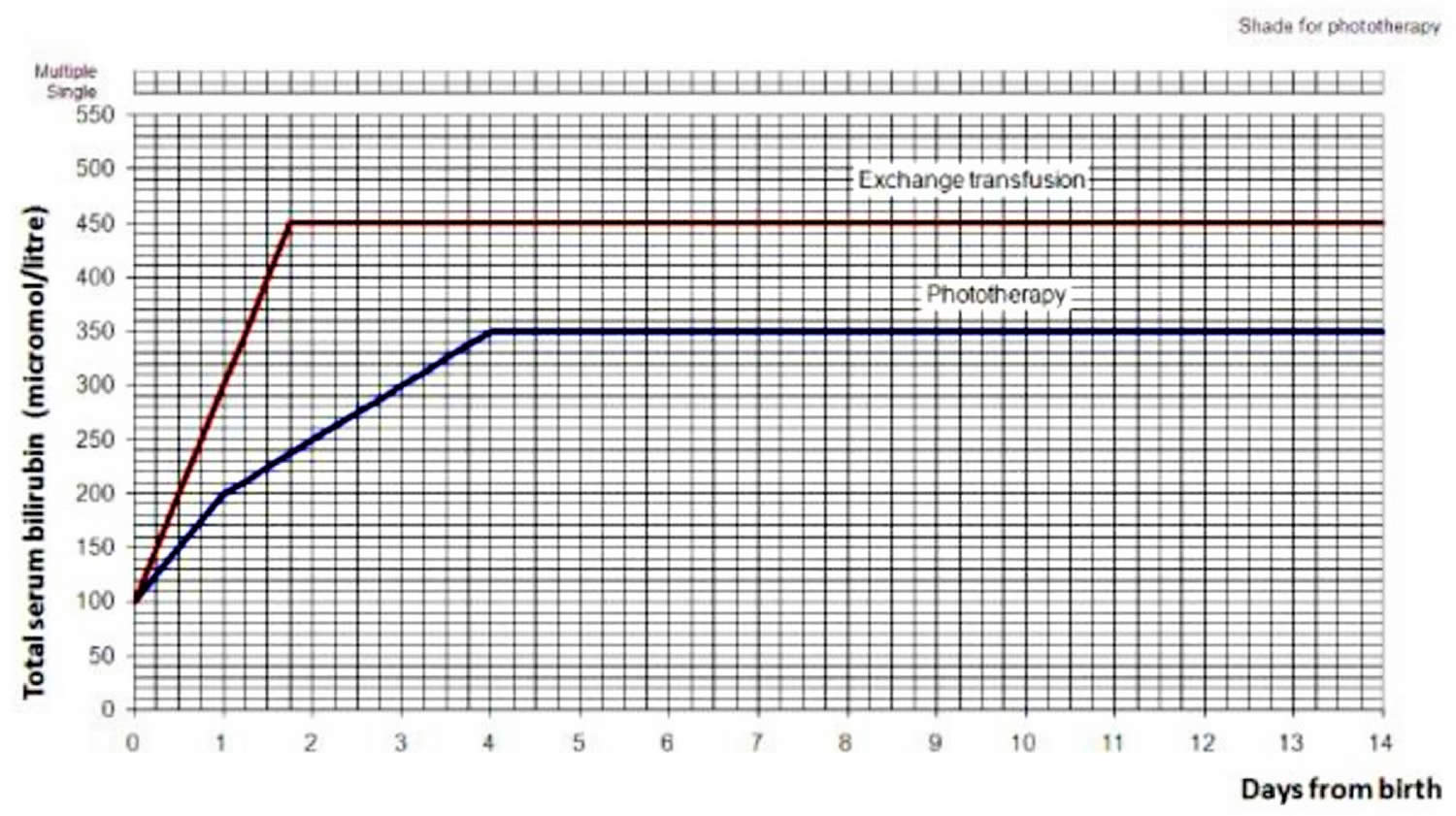
Figure 5. Hyperbilirubinemia treatment threshold graph for babies with neonatal jaundice: >=38 weeks gestation
Neonatal Hyperbilirubinemia Treatment
Treatment will depend on your child’s symptoms, age, and general health. It will also depend on how bad the condition is. Mild infant jaundice often disappears on its own within two or three weeks. For moderate or severe jaundice, a baby may need to stay longer in the newborn nursery or be readmitted to the hospital. Use the bilirubin level to determine the management of hyperbilirubinemia in all babies, see threshold table (see Table 1) and treatment threshold graphs (Figures 4 and 5).
Treatment depends on how old the baby is (in hours) and whether the baby has any risk factors (such as prematurity). It may include:
- Light therapy also called phototherapy. Your baby may be placed under a special lamp that emits light in the blue-green spectrum. The light changes the shape and structure of bilirubin molecules in such a way that they can be excreted in both the urine and stool. During treatment, your baby will wear only a diaper and protective eye patches. Light therapy may be supplemented with the use of a light-emitting pad or mattress.
- Fiber optic blanket is another form of phototherapy. The blanket is usually put under your baby. It may be used alone or with regular phototherapy.
- Exchange transfusions (removing the child’s blood and replacing it with fresh donor blood or plasma). Rarely, when severe jaundice doesn’t respond to other treatments, a baby may need an exchange transfusion of blood. This involves repeatedly withdrawing small amounts of blood and replacing it with donor blood. The procedure dilutes the bilirubin and maternal antibodies and is done in a newborn intensive care unit.
- Enhanced nutrition. To prevent weight loss, your baby’s doctor may recommend more-frequent feeding or supplementation to ensure that your baby receives enough nutrition.
- Intravenous immunoglobulin (IVIg). Jaundice may be related to blood type differences between mother and baby. This condition results in the baby carrying antibodies from the mother that contribute to the rapid breakdown of the baby’s red blood cells. Intravenous transfusion of an immunoglobulin (IVIg), a blood protein that can reduce levels of antibodies, may decrease jaundice and lessen the need for an exchange transfusion, although results are not conclusive.
- Treating any underlying cause of the hyperbilirubinemia.
In preterm infants, the risk of a handicap increases by 30% for each 2.9 mg/dL increase of maximal total bilirubin concentration. While central nervous system damage is rare when total serum bilirubin is less than 20 mg/dL, premature infants may be affected at lower levels. The decision to institute therapy is based on a number of factors including total serum bilirubin, age, clinical history, physical examination, and coexisting conditions. Phototherapy typically is discontinued when total serum bilirubin level reaches 14 to 15 mg/dL.
Table 1. Bilirubin threshold table for the management of babies of 38 weeks or more gestational age with hyperbilirubinemia
| Age (hours) | Bilirubin measurement (micromol/liter) | |
|---|---|---|
| 0 | >100 | >100 |
| 6 | >125 | >150 |
| 12 | >150 | >200 |
| 18 | >175 | >250 |
| 24 | >200 | >300 |
| 30 | >212 | >350 |
| 36 | >225 | >400 |
| 42 | >237 | >450 |
| 48 | >250 | >450 |
| 54 | >262 | >450 |
| 60 | >275 | >450 |
| 66 | >287 | >450 |
| 72 | >300 | >450 |
| 78 | >312 | >450 |
| 84 | >325 | >450 |
| 90 | >337 | >450 |
| 96 | >350 | >450 |
| Action | Start phototherapy | Perform an exchange transfusion unless the bilirubin level falls below threshold while the treatment is being prepared |
Footnotes: Note that there is variability between assays from different manufacturers in reported bilirubin measurement. Healthcare professionals should consult their local pathology laboratory when interpreting threshold tables.
[Source 78 ]Phototherapy
Bilirubin absorbs light. High bilirubin levels often decrease when a baby is put under special blue spectrum lights. This is called phototherapy 7, 5, 6. Your child may get this treatment in the day and night. It may take several hours for it to start working. During light treatment, your baby’s eyes will be protected. Your baby’s doctor will check your baby’s temperature. They will also test your baby’s bilirubin levels. This will tell if phototherapy is working.
Bilirubin optimally absorbs light in the blue-green range (ie, 460-490 nm). The underlying mechanism of phototherapy involves inducing photoisomerization and converting bilirubin into lumirubin, which is readily excreted into bile and urine 79. During phototherapy, the neonate’s maximum body surface area should be exposed to the light source while keeping the eyes covered to avoid retinal injury, and interruptions should be minimized. The maintenance of hydration is necessary to ensure adequate urine output, as most bilirubin is excreted in the urine as lumirubin, a structural isomer of bilirubin formed during phototherapy. Therefore, breastfeeding support should be offered to all nursing mothers as early initiation of breastfeeding and frequent, on-demand feeding decreases the likelihood of dehydration. Although supplemental oral water and dextrose water are not recommended, supplemental pumped breastmilk or infant formula can be considered for feeding issues, including infants with ineffective sucking or latching or inadequate maternal milk production 70.
After phototherapy is discontinued, there may be an increase in the total serum bilirubin level, known as the rebound bilirubin. This level is usually lower than the pretreatment level and rarely requires reinitiation of phototherapy 80. Phototherapy is considered safe, but recent evidence suggests a possible association with long-term complications, including a small risk of childhood seizures. However, no studies have proven causation 81. A few studies also have reported a possible association between solid organ tumors and nonlymphocytic leukemias and children treated with phototherapy 82, 83. Adverse effects of phototherapy include rashes, dehydration, hypocalcemia, retinal damage, hemolysis due to oxidative damage, delay in patent ductus arteriosis closure in preterm infants, and allergic reactions 84. Bronze baby syndrome is a self-limited condition associated with elevated levels of conjugated bilirubin that rarely occurs with phototherapy, resulting in irregular, bronze-gray pigmentation of the skin, mucous membranes, and urine. The Bronze baby syndrome’s mechanism is unclear but appears to be related to the accumulation of bilirubin and biliverdin photoisomers. Bronze baby syndrome usually resolves within a few days of discontinuing phototherapy; however, the prognosis depends upon the underlying cause of the conjugated hyperbilirubinemia 85, 86.
Fiber optic blanket
A fiber optic blanket is another form of phototherapy. The blanket is usually put under your baby. It may be used alone or with regular phototherapy.
Exchange transfusion
Exchange transfusion is the treatment that involves removing your baby’s blood that has a high bilirubin level and replacing it with fresh donor blood or plasma 87. This raises your baby’s red blood cell count. It also lowers their bilirubin level. During the procedure, your baby will switch between giving and getting small amounts of blood. This will be done through a vein or artery in the baby’s umbilical cord. It is only done in an intensive care nursery when bilirubin levels are extremely high. Your baby may need to have this procedure again if their bilirubin levels stay high.
Exchange transfusion is now the second-line treatment for severe unconjugated hyperbilirubinemia since phototherapy was developed in the 1950s 88, 89. Indications for exchange transfusion include neonatal failure to respond to phototherapy or a total serum bilirubin level at the exchange transfusion threshold. The threshold to initiate exchange transfusion is calculated based on several factors, including the total serum bilirubin level and rate of rise, neonatal age (ie, hours or days since birth), and risk factors for neurologic complications 70. Exchange transfusion rapidly removes bilirubin and hemolysis-causing antibodies from the infant’s circulation. A double-volume exchange blood transfusion (160-180 ml/kg) is performed, replacing aliquots of the neonate’s blood with crossed-matched donor blood. Since most of the total body bilirubin is extravascular, the total serum bilirubin level immediately following exchange transfusion is approximately 60% of the pre-exchange level, but that later increases to 70% to 80% of the pretreatment level as a result of equilibrium. During exchange transfusion, the neonate’s vital signs should be monitored closely. Following the procedure, total serum bilirubin, complete blood count, serum calcium, glucose, and electrolytes should be rechecked due to potential complications, including electrolyte abnormalities (eg, hypocalcemia and hyperkalemia), cardiac arrhythmias, thrombocytopenia, blood-borne infections, portal vein thrombosis, graft versus host disease, and necrotizing enterocolitis (NEC) 90, 91. Phototherapy should resume after exchange transfusion until the bilirubin reaches a level where phototherapy can be safely discontinued.
Intravenous immunoglobulin (IVIg)
Jaundice may be related to blood type differences between mother and baby. This condition results in the baby carrying antibodies from the mother that contribute to the rapid breakdown of the baby’s red blood cells. Intravenous transfusion of an immunoglobulin (IVIg), a blood protein that can reduce levels of antibodies, may decrease jaundice and lessen the need for an exchange transfusion, although results are not conclusive. The American Academy of Pediatrics recommends intravenous immunoglobulin (IVIg) infusion in immune-mediated hemolysis if total serum bilirubin remains within 2 to 3 mg/dL of the exchange threshold despite intensive phototherapy 92, 93. However, the evidence that intravenous immunoglobulin (IVIg) reduces the need for exchange transfusion is unclear. Nonetheless, intravenous immunoglobulin (IVIg) is often used in clinical practice to manage severe unconjugated hyperbilirubinemia 5.
Feeding with breastmilk
The American Academy of Pediatrics says that you should keep breastfeeding a baby with jaundice. If your baby has not been getting enough milk at the breast, you may need to supplement with pumped breastmilk or formula.
Feeding more frequently will provide your baby with more milk and cause more bowel movements, increasing the amount of bilirubin eliminated in your baby’s stool. Infants who are breastfed should have 8 to 12 feedings a day for the first several days of life. Formula-fed infants usually should have 1 to 2 ounces (about 30 to 60 milliliters) of formula every 2 to 3 hours for the first week.
Supplemental feedings
If your baby is having trouble breastfeeding, is losing weight or is dehydrated, your baby’s doctor may suggest giving your baby formula or expressed milk to supplement breastfeeding. Depending on the situation, your baby’s doctor may recommend using formula alone for a couple of days and then resuming breastfeeding. Ask your baby’s doctor what feeding options are right for your baby.
Treating any underlying cause of the hyperbilirubinemia
This may include treating an infection.
Neonatal Hyperbilirubinemia Prognosis
With treatment, the prognosis for most cases of unconjugated hyperbilirubinemia is excellent 5. In patients with delayed or inadequate hyperbilirubinemia treatment, bilirubin encephalopathy may ensue. The burden of bilirubin encephalopathy is significantly higher in developing and resource-limited nations 94. Reports suggest a resurgence of kernicterus in countries where this complication had virtually disappeared, primarily attributed to the early hospital discharge of newborns with inadequate follow-up 5. Patients with Crigler-Najjar type I carry a poor prognosis and require liver transplantation for a definitive cure. In the absence of liver transplantation, bilirubin encephalopathy is common.
The prognosis for conjugated hyperbilirubinemia depends on the cause. The prognosis of patients with biliary atresia is significantly improved by early diagnosis and surgery within 60 days of life. Similarly, patients with bile acid synthesis disorder have excellent outcomes and respond well to medical treatment 5. Historically, the outlook for gestational alloimmune liver disease (GALD) was poor, with up to 80% mortality without liver transplantation 5. However, with the advent of intravenous transfusion of an immunoglobulin (IVIg) use and double volume exchange transfusion, the prognosis has significantly improved in recent years 95. Infants with neonatal cholestasis are also at risk of developing liver failure, cirrhosis, and even hepatocellular carcinoma in rare cases 5. Long-standing cholestasis may also lead to failure to thrive and fat-soluble vitamin deficiencies 5. The outlook for most other causes of cholestasis is often unfavorable, and many patients will require multidisciplinary interventions 5.
Hyperbilirubinemia causes
Hyperbilirubinemia or excess bilirubin in the blood is the main cause of jaundice. Bilirubin is a yellow-pigmented substance released into the bloodstream when red blood cells break down.
Newborns produce more bilirubin than adults do. This is due to greater production and faster breakdown of red blood cells in the first few days of life. Typically, the liver filters bilirubin from the bloodstream and releases it into the intestinal tract. A newborn’s immature liver often can’t remove bilirubin quickly enough. This causes a buildup of bilirubin. Jaundice caused by these typical newborn conditions is called physiologic jaundice, and it typically appears on the second or third day of life.
Neonatal Hyperbilirubinemia causes
There are several causes of hyperbilirubinemia and jaundice in newborn, including the following:
- Physiologic jaundice. During pregnancy, the placenta removes bilirubin from your baby’s blood. When a baby is born, the baby’s liver takes over this job. Physiologic jaundice occurs as a “normal” response to the baby’s limited ability to excrete bilirubin in the first days of life due to the immaturity of the liver. This will usually resolve by the first week of life.
- Breastfeeding failure jaundice. During the first few days of breastfeeding when the maternal breast milk supply is low and the baby is having trouble latching and feeding, the baby may become dehydrated. Since bilirubin is eliminated in the urine and stool, decreased urination and infrequent stools result in a buildup of bilirubin. While common in full term infants, premature infants and late preterm infants are more susceptible to breastfeeding failure jaundice because they may have uncoordinated suck as well as easy fatigability. Once effective breastfeeding is established, this problem will resolve.
- Breast milk jaundice. About 2 percent of breastfed babies develop jaundice after the first week. It peaks about two weeks of age and can persist up to three to twelve weeks. Breast milk jaundice is thought to be caused by glucuronidase enzyme in the breast milk that deconjugates bilirubin into unconjugated bilirubin 49. Breastfeeding can usually continue or only be interrupted briefly.
- Jaundice from breakdown of red blood cells (hemolysis). Jaundice may occur if there is an increase of red blood cell breakdown (hemolysis) such as that seen when there is a mismatch of maternal and fetal blood type, resulting in ABO incompatibility (a condition where a mother’s antibodies attack a baby’s red blood cells due to a difference in blood type, with most common type when a mother is blood type O and her baby is blood type A or B), hemolytic disease of the newborn (Rh disease) or abnormalities of the red cell itself such as hereditary spherocytosis, elliptocytosis, glucose-6-phosphate dehydrogenase deficiency (G6PD deficiency), pyruvate kinase deficiency; and hemoglobinopathies, such as alpha and beta thalassemias 50. Increased hemolysis (red blood cell breakdown) can also occur if the baby is bruised or develops a hematoma during delivery.
- Birth Trauma such as cephalohematoma (a collection of blood under the scalp that forms on a newborn’s skull, usually caused by ruptured blood vessels during childbirth), subgaleal hemorrhage (a serious, potentially life-threatening condition in newborns caused by bleeding into the space between the skull’s periosteum and the galea aponeurosis [the scalp’s tough, fibrous tissue layer]), or peripheral bruises from birth trauma 51.
- Jaundice related to inadequate liver function. Jaundice may be related to prolonged liver dysfunction due to infection and other factors.
- Disruption or Obstruction in the Biliary System.
- Hereditary Bilirubin Conjugation Defects – Crigler-Najjar syndrome and Gilbert syndrome are due to the deficiency of the enzyme uridine 5′-diphospho-glucuronosyltransferase (UDGPT), which conjugates the bilirubin in the liver cells 52.
- Rotor syndrome is a rare, inherited genetic disorder characterized by elevated levels of bilirubin in the blood (hyperbilirubinemia). People with Rotor syndrome have a buildup of both unconjugated and conjugated bilirubin in their blood, but the majority is conjugated bilirubin 27, 28. Rotor syndrome is caused by SLCO1B1 and SLCO1B3 genes. Mutations in both SLCO1B1 and SLCO1B3 genes are required for Rotor syndrome to occur. The SLCO1B1 and SLCO1B3 genes provide instructions for making similar proteins, called organic anion transporting polypeptide 1B1 (OATP1B1) and organic anion transporting polypeptide 1B3 (OATP1B3), respectively. Both proteins are found in liver cells; they transport bilirubin and other compounds from the blood into the liver so that they can be cleared from the body. In the liver, bilirubin is dissolved in a digestive fluid called bile and then excreted from the body. In people with Rotor syndrome, jaundice is usually evident shortly after birth or in childhood and may come and go; yellowing of the whites of the eyes also called conjunctival icterus is often the only symptom. Rotor syndrome is a benign and harmless condition that typically does not require treatment and does not affect life expectancy. Jaundice may be noticeable shortly after birth or in childhood, but often it’s an incidental finding.
Crigler–Najjar syndrome is a very rare inherited disorder in which bilirubin cannot be broken down. Mutations in the UGT1A1 gene cause Crigler-Najjar syndrome. The UGT1A1 gene provides instructions for making the bilirubin uridine diphosphate glucuronosyl transferase (bilirubin-UGT) enzyme, which is found primarily in liver cells and is necessary for the removal of bilirubin from the body. Mutations in the UGT1A1 gene that cause Crigler-Najjar syndrome result in reduced or absent function of the bilirubin-UGT enzyme. People with - Crigler–Najjar Type 1 have no bilirubin uridine diphosphate glucuronosyl transferase (bilirubin-UGT) enzyme function, while people with Crigler–Najjar Type 2 have less than 20 percent of normal function. The loss of bilirubin-UGT function decreases glucuronidation of unconjugated bilirubin. Glucuronidation makes bilirubin dissolvable in water so that it can be removed from the body. This toxic unconjugated bilirubin then builds up in the body, causing unconjugated hyperbilirubinemia and jaundice. Crigler–Najjar Type 1 (CN1) is very severe, and affected individuals can die in childhood due to kernicterus, although with proper treatment, they may survive longer. Crigler–Najjar Type 2 (CN2) is less severe. People with Crigler–Najjar Type 2 are less likely to develop kernicterus, and most affected individuals survive into adulthood.
Dubin-Johnson syndrome is a rare, inherited liver disorder characterized by an increase in conjugated bilirubin, leading to mild, chronic jaundice. Dubin-Johnson syndrome is caused by mutation in ABCC2 gene affecting the liver’s ability to excrete bilirubin, resulting in pigment deposits that make the liver appear black on medical imaging. The ABCC2 gene provides instructions for making a protein that transports certain substances out of cells so they can be released (excreted) from the body. For example, this protein transports bilirubin out of liver cells and into bile (a digestive fluid produced by the liver). Bilirubin is produced during the breakdown of old red blood cells and has an orange-yellow tint. As a result, bilirubin accumulates in the body, causing a condition called hyperbilirubinemia. The buildup of bilirubin in the body causes the yellowing of the skin and whites of the eyes in people with Dubin-Johnson syndrome. Dubin-Johnson syndrome is most often seen in Middle Eastern Jewish and Japanese people. In the Jewish population, about 60% of affected individuals also have an associated blood clotting abnormality, a prolonged prothrombin time (PT), caused by a decrease in factor VII (factor 7). In most affected people jaundice appears during adolescence or early adulthood. Infants with Dubin-Johnson syndrome typically also have enlarged livers (hepatomegaly) and a severely reduced ability to produce and release a digestive fluid called bile (cholestasis). As these children get older, their liver problems go away and they usually do not have any related health problems later in life. Jaundice is typically the only feature of - Dubin-Johnson syndrome, but some people can experience weakness, mild abdominal pain, nausea, or vomiting. In most people with Dubin-Johnson syndrome, certain deposits build up in the liver but do not seem to impair liver function. The deposits make the liver appear black when viewed with medical imaging. Dubin-Johnson syndrome is benign, has a normal life expectancy, and usually requires no specific treatment, though precautions like avoiding birth control pills, alcohol, environmental factors that affect the liver, infection, pregnancy, fasting or dehydration and fatigue are recommended.
- Neonatal polycythemia also called polycythemia in newborns is a condition where there are too many red blood cells, defined by a venous hematocrit greater than 65% 53, 54, 55. Polycythemia means there are too many red blood cells (RBCs) in an infant’s blood. Polycythemia in newborn can lead to increased blood viscosity and decreased blood flow, causing symptoms like lethargy, poor feeding, and respiratory distress. Causes of polycythemia in newborn include delayed cord clamping, twin-to-twin transfusion, and intrauterine hypoxia. Treatment may involve fluid administration for mild cases or a partial exchange transfusion for more severe cases.
- Hypoalbuminemia is a condition where the level of albumin, a protein in the blood, is abnormally low. Unconjugated bilirubin is lipid-soluble and is normally bound to albumin; a decrease in the albumin level leads to an increase in free unconjugated bilirubin level 56.
- Infection: Congenital infections (eg, syphilis, toxoplasmosis, HIV, herpes virus, and rubella) should be included in the differential diagnosis of neonatal cholestasis, especially when stigmata of congenital infection, including growth restriction, coagulopathy, skin rash, or thrombocytopenia, are present. Cytomegalovirus (CMV) is also a common congenital infection with many manifestations. Most infected newborns are asymptomatic, but hepatomegaly and conjugated hyperbilirubinemia may indicate liver involvement 57. Carefully reviewing maternal history, specific serologies, and viral culture results aid diagnosis. Urine and blood cultures are also a component of the diagnostic evaluation, as urinary tract infections and septicemia can cause conjugated hyperbilirubinemia in neonates. Additionally, microcirculatory changes in the liver, a direct effect of bacterial products, and toxins released by bacteria are thought to be the possible mechanisms of cholestasis in patients with urinary tract infection (UTI) 58.
Prematurity, hemolytic disease of the newborn and glucose-6-phosphate dehydrogenase (G6PD) deficiency are the most common risk factors 48, 59. Newborns who develop neurological complications of hyperbilirubinemia usually have at least two neurotoxicity risk factors 60. There is no clear correlation between bilirubin level alone and the risk of developing brain toxicity 61, 50.
The timing of when your child’s jaundice first starts matters. It may help their your baby’s doctor make a diagnosis.
- First 24 hours. This type of jaundice is often serious. Your child will likely need treatment right away.
- Second or third day. This is often physiologic jaundice. Sometimes it can be a more serious type of jaundice. It’s important to be sure the baby is getting enough milk at this point.
- Toward the end of the first week. This type of jaundice may be from breastmilk jaundice but may be due to an infection or other rare, serious problems.
- In the second week. This is often caused by breastmilk jaundice but may be caused by rare liver problems.
In the United States Kernicterus Registry, 56% had abnormalities known to increase the bilirubin concentration in the blood. Glucose-6-phosphate dehydrogenase deficiency (G6PD deficiency) was diagnosed in 21.3%, severe hemolytic processes were recognized in 20.5%, birth trauma was identified in 15%, and other causes such as galactosemia, Crigler-Najjar syndrome, and sepsis were diagnosed in 7% 44. However, no cause was identified in 43.4% of the infants 62.
Adults hyperbilirubinemia causes
Approximately 250 mg of bilirubin per day is produced by an average adult through the breakdown of the heme molecule (a porphyrin ring organic compound complexed with ferrous iron and protoporphyrin IX that is present in proteins like hemoglobin and myoglobin, where it performs functions such as oxygen transport, energy production, and antioxidant defense) 96. Heme is released during red blood cell destruction. Heme is first converted to biliverdin and then to unconjugated bilirubin within macrophages in the reticular endothelial system 97. Unconjugated bilirubin is lipid soluble and passes easily through cell membranes to bind to albumin in serum, whereas free (unbound) bilirubin is taken up by liver cells and converted to conjugated bilirubin 98, 96. Conjugated bilirubin is water soluble and is transported from liver cells into the biliary tract system where it passes to the intestines and is excreted into the stool. Some conjugated bilirubin is reabsorbed in the intestines and is excreted by the kidneys as urobilinogen 98, 96. Jaundice occurs when there are disruptions along this metabolic pathway, causing an increase in unconjugated bilirubin (e.g., from increased red blood cell destruction or impaired bilirubin conjugation) or conjugated bilirubin (e.g., from hepatocellular damage or biliary tract obstructions).
Jaundice in adults can result from a problem in any of the three phases of bilirubin 1, 99, 100:
- Before your liver processes bilirubin (prehepatic jaundice). This type of jaundice happens before your body makes bilirubin. Too much red blood cell breakdown takes over your liver’s ability to filter out bilirubin from your blood.
- During the production of bilirubin (hepatic jaundice). This type happens when your liver can’t remove enough bilirubin from your blood. Hepatic jaundice can happen if you have liver failure.
- After production of bilirubin (posthepatic jaundice). Also called obstructive jaundice, this type happens when a blockage stops bilirubin from draining into your bile ducts.
Figure 6. Adults hyperbilirubinemia causes
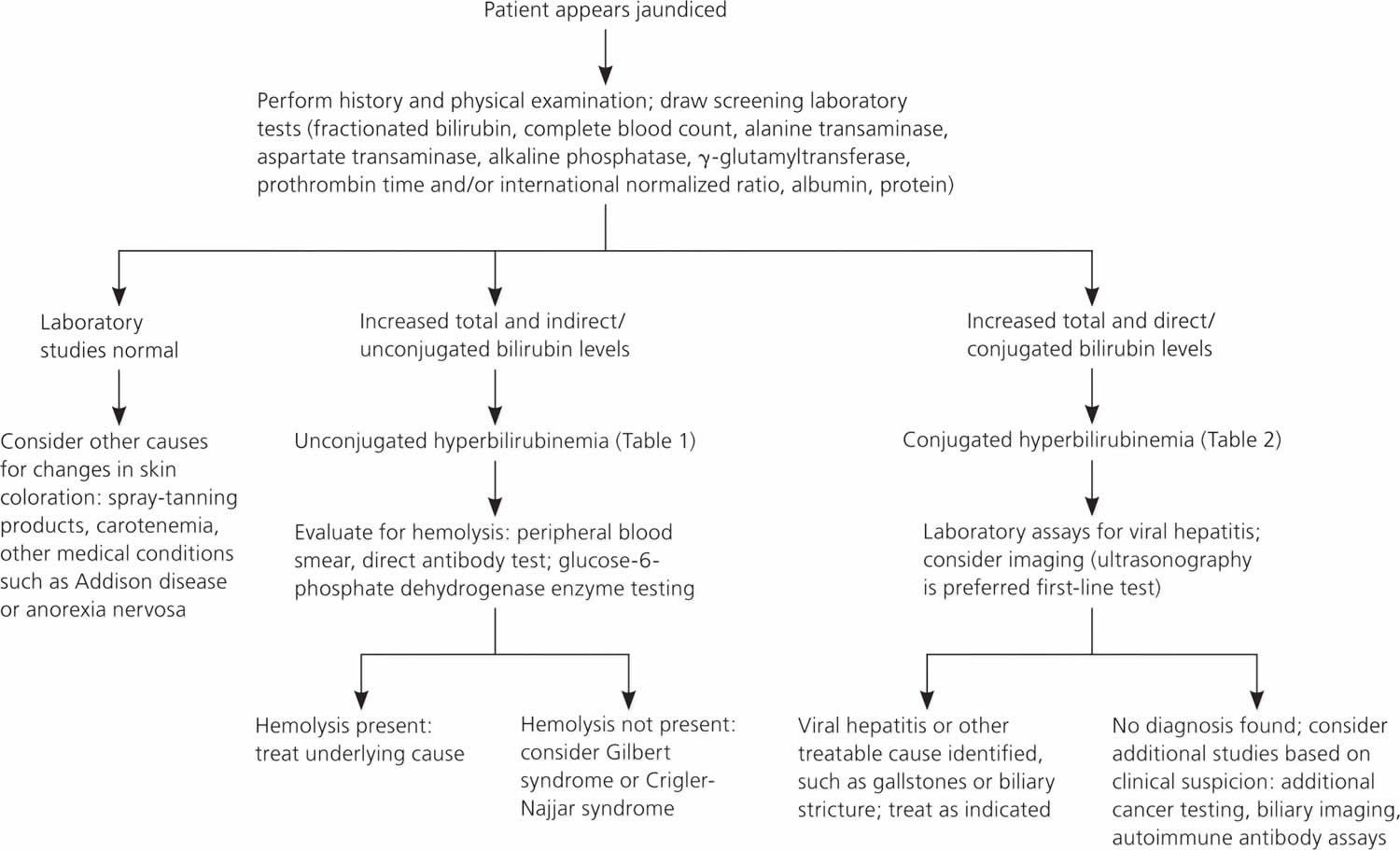
Prehepatic jaundice causes
- Breaking down a large hematoma (bruise) and then reabsorbing it back into your bloodstream.
- Hemolytic anemias (when blood cells are destroyed and removed from the bloodstream before their normal lifespan is over).
- Abnormal development of red blood cells (dyserythropoiesis), leading to their destruction within the bone marrow or release into the bloodstream with abnormalities 101, 102. It can cause anemia, which may result in fatigue, weakness, and jaundice. Dyserythropoiesis can be congenital (inherited) or acquired, and a primary example is congenital dyserythropoietic anemia.
Hepatic jaundice causes
- Viruses, including hepatitis A, chronic hepatitis B and C, hepatitis D, Cytomegalovirus and Epstein-Barr virus infection (infectious mononucleosis).
- Alcohol-induced hepatitis.
- Nonalcoholic steatohepatitis (NASH)
- Autoimmune disorders.
- Rare genetic metabolic defects e.g., Wilson’s disease
- Drugs and Toxins, including penicillin, oral contraceptives, chlorpromazine (Thorazine R), rifampin, probenecid, estrogenic or anabolic steroids, acetaminophen toxicity, herbal medications (e.g., Jamaican bush tea, kava kava) and arsenic.
- Cholestatic liver disease: Primary biliary cholangitis, primary sclerosing cholangitis
- Infiltrative diseases (e.g., amyloidosis, lymphoma, sarcoidosis, tuberculosis)
- Sepsis and hypoperfusion states
- Total parenteral nutrition (TPN)
- Hepatic crisis in sickle cell disease
- Pregnancy.
- Gilbert syndrome is a harmless, inherited liver disorder that causes reduced liver uptake of bilirubin resulting mildly elevated levels of bilirubin in the blood, which can lead to occasional, mild jaundice (yellowing of the skin and eyes). Changes in the UGT1A1 gene cause Gilbert syndrome. The UGT1A1 gene provides instructions for making the bilirubin uridine diphosphate glucuronosyltransferase (bilirubin-UGT) enzyme, which is found primarily in liver cells and is necessary for the removal of bilirubin from the body. Most people with Gilbert syndrome have no symptoms and no treatment is needed. Symptoms that can occur, though they are often mild, include fatigue, nausea, and abdominal pain.
- Crigler–Najjar syndrome is a very rare inherited disorder in which bilirubin cannot be broken down. Mutations in the UGT1A1 gene cause Crigler-Najjar syndrome. The UGT1A1 gene provides instructions for making the bilirubin uridine diphosphate glucuronosyl transferase (bilirubin-UGT) enzyme, which is found primarily in liver cells and is necessary for the removal of bilirubin from the body. Mutations in the UGT1A1 gene that cause Crigler-Najjar syndrome result in reduced or absent function of the bilirubin-UGT enzyme. People with Crigler–Najjar Type 1 have no enzyme function, while people with Crigler–Najjar Type 2 have less than 20 percent of normal function. The loss of bilirubin-UGT function decreases glucuronidation of unconjugated bilirubin. Glucuronidation makes bilirubin dissolvable in water so that it can be removed from the body. This toxic bilirubin then builds up in the body, causing unconjugated hyperbilirubinemia and jaundice. Crigler–Najjar Type 1 (CN1) is very severe, and affected individuals can die in childhood due to kernicterus, although with proper treatment, they may survive longer. Crigler–Najjar Type 2 (CN2) is less severe. People with Crigler–Najjar Type 2 are less likely to develop kernicterus, and most affected individuals survive into adulthood.
Posthepatic jaundice causes
- Gallstones.
- Inflammation (swelling) of your gallbladder.
- Gallbladder cancer.
- Pancreatic tumor (head of pancreas cancer).
- Extrahepatic biliary atresia
- Acute and chronic pancreatitis
- Strictures
- Parasitic infections (e.g., Ascaris lumbricoides, liver flukes).
Hyperbilirubinemia signs and symptoms
Hyperbilirubinemia in babies
Elevated bilirubin or hyperbilirubinemia is evident by yellow discoloration of the baby’s eyes, mucosa and skin, usually starting from the head and moving downward. If your baby doesn’t have jaundice, the skin color should simply look slightly lighter than its usual color for a moment. Examine your baby in good lighting conditions, preferably in natural daylight. Prior to discharge in the hospital, most babies will have their bilirubin level checked, either by a skin (transcutaneous) probe or a blood test. Other symptoms of jaundice may include poor feeding or lethargy. The symptoms of hyperbilirubinemia may resemble other conditions or medical problems. Always consult your baby’s doctor for a diagnosis.
Hyperbilirubinemia symptoms can occur a bit differently in each child. They can include:
- Yellowing of your baby’s skin and the whites of their eyes (jaundice). This often starts on a baby’s face and moves down their body.
- Poor feeding
- Lack of energy
The symptoms of hyperbilirubinemia may be similar to symptoms of other conditions. Make sure your child sees a doctor for a diagnosis.
Most hospitals have a policy of examining babies for jaundice before discharge. The American Academy of Pediatrics recommends that 15, 10:
- Newborns be examined for jaundice during routine medical checks and at least every 12 hours while in the hospital.
- A newborn’s bilirubin levels should be checked between 24 and 48 hours after birth.
The following symptoms may suggest complications from too much bilirubin 16, 4:
- Your baby’s skin becomes more yellow.
- The skin on your baby’s belly, arms or legs looks yellow.
- The whites of your baby’s eyes look yellow.
- Your baby seems listless or sick or is hard to wake up.
- Your baby isn’t gaining weight or is feeding poorly.
- Your baby makes high-pitched cries.
- Your baby develops any other symptoms that concern you.
- In rare cases, your baby develop seizures.
Hyperbilirubinemia in adults
Hyperbilirubinemia in adults will cause jaundice, the yellow discoloration of your skin and sclera from the accumulation of excess bilirubin. How serious your symptoms are depends on what causes them and how quickly or slowly they develop.
Symptoms that can be associated with jaundice in adults include:
- Yellowish tint to your skin and the whites of your eyes.
- Fever.
- Chills.
- Pain in your belly.
- Flu-like symptoms.
- Dark-colored urine.
- Pale-colored poop.
- Being tired or confused.
- Itchy skin.
- Weight loss.
Hyperbilirubinemia diagnosis
Your doctor can tell if you have hyperbilirubinemia or elevated bilirubin in your blood by measuring the bilirubin levels in your blood and seeing whether it’s the type of bilirubin related to red blood cell breakdown (unconjugated) or liver injury (conjugated). Your doctor may also check for other signs of liver disease, including:
- Bruising.
- Spider angiomas (abnormal collection of blood vessels near the surface of your skin).
- Palmar erythema (red palms and fingertips).
Your doctor will also examine you to decide your liver’s size and tenderness. Your doctor may use imaging (ultrasound and CT scanning) and liver biopsy (taking a tissue sample of your liver) to better understand what’s causing your liver injury.
Bilirubin test
Bilirubin test measures the amount of bilirubin in your blood to evaluate your liver function or to help diagnose anemias caused by red blood cell destruction (hemolytic anemia).
A bilirubin test is used to detect an elevated bilirubin level in the blood. Bilirubin test may be used to help determine the cause of jaundice and/or help diagnose conditions such as liver disease, hemolytic anemia, and blockage of the bile ducts.
Bilirubin is an orange-yellow pigment, a waste product primarily produced by the normal breakdown of heme. Heme is a component of hemoglobin, which is found in red blood cells. Bilirubin is ultimately processed by the liver to allow its elimination from the body. Any condition that accelerates the breakdown of red blood cells or affects the processing and elimination of bilirubin may cause an elevated blood level.
Two forms of bilirubin can be measured or estimated by laboratory tests:
- Unconjugated bilirubin—when heme is released from hemoglobin, it is converted to unconjugated bilirubin. It is carried by proteins to the liver. Small amounts may be present in the blood.
- Conjugated bilirubin—formed in the liver when sugars are attached (conjugated) to bilirubin. It enters the bile and passes from the liver to the small intestines and is eventually eliminated in the stool. Normally, no conjugated bilirubin is present in the blood.
Usually, a chemical test is used to first measure the total bilirubin level (unconjugated plus conjugated bilirubin). If the total bilirubin level is increased, the laboratory can use a second chemical test to detect water-soluble forms of bilirubin, called “direct” bilirubin. The direct bilirubin test provides an estimate of the amount of conjugated bilirubin present. Subtracting direct bilirubin level from the total bilirubin level helps estimate the “indirect” level of unconjugated bilirubin. The pattern of bilirubin test results can give your doctor information regarding the condition that may be present.
A urine test positive for bilirubin indicates conjugated hyperbilirubinemia. Conjugated bilirubin is soluble in water; therefore, it can be excreted via urine but not unconjugated bilirubin due to water insolubility. Furthermore, other laboratory testing should include measurement of the serum aspartate transaminase (AST), alanine transaminase (ALT), alkaline phosphatase (ALP), and gamma-glutamyl transpeptidase (GGT) levels, complete blood count (CBC) with an examination of the smear, a reticulocyte count, a direct Coombs test, lactate dehydrogenase (LDH) and haptoglobin levels 17. Jaundice, with a toxic appearance, fever, or abnormal count of white blood cells indicates sepsis that requires prompt evaluation and adequate treatment. The increased levels of aspartate transaminase (AST) and alanine transaminase (ALT) are markers of liver damage/injury. However, increased levels of alkaline phosphatase (ALP) and gamma-glutamyl transpeptidase (GGT) suggest cholestasis (a condition characterized by a reduced or stopped flow of bile from the liver, leading to a buildup of bile components like bilirubin and bile acids in the bloodstream).
A complete blood count (CBC) is a beneficial test for the determination of hemolysis, which is characterized by the presence of damaged red blood cells and increased reticulocytes on the smear. In patients, when the serum total bilirubin levels exceed 3.0 mg/dL, jaundice becomes clinically apparent. Hyperbilirubinemia is unconjugated bilirubin when the conjugated bilirubin level is less than 15% of the total bilirubin. While in conjugated hyperbilirubinemia, conjugated bilirubin level is high and more than 20% of the total bilirubin. Generally, patients with carotenemia (a harmless condition that causes a yellow-orange discoloration of the skin, most often due to excessive consumption of carotene-rich foods like carrots) also present yellow skin but have no elevation in serum bilirubin levels. During the physical examination, carotenemia due to excess carotene intake, e.g., carrots, peaches, etc., can be distinguished from jaundice due to the absence of scleral icterus in carotenemia and with the pigmentation of soles and palms and other areas. Computerized axial tomography (CT) and ultrasonography scanning are useful tools in differentiating cholestasis (intra-hepatic and extra-hepatic) from hepatocellular disease in the assessment of a patient with conjugated hyperbilirubinemia.
In adults and older children, bilirubin is measured to:
- Diagnose and/or monitor diseases of the liver and bile duct (e.g., cirrhosis, hepatitis, or gallstones)
- Evaluate people with sickle cell disease or other causes of hemolytic anemia; these people may have episodes called crises when excessive red blood cell destruction increases bilirubin levels.
In newborns with jaundice, bilirubin is used to distinguish the causes of jaundice.
- In both physiologic jaundice of the newborn and hemolytic disease of the newborn, only unconjugated (indirect) bilirubin is increased.
- In much less common cases, damage to the newborn’s liver from neonatal hepatitis and biliary atresia will increase conjugated (direct) bilirubin concentrations as well, often providing the first evidence that one of these less common conditions is present.
It is important that an elevated level of bilirubin in a newborn be identified and quickly treated because excessive unconjugated bilirubin damages developing brain cells. The consequences of this damage include mental retardation, learning and developmental disabilities, hearing loss, eye movement problems, and death.
Imaging
Noninvasive imaging modalities in persons with jaundice include ultrasound, computed tomography (CT), and magnetic resonance cholangiopancreatography (MRCP). Ultrasound or computed tomography (CT) is usually the first-line option to evaluate for obstruction, cirrhosis, and vessel patency, with ultrasonography being the least invasive and least expensive modality 18, 17. Visualization of the intra- and extrahepatic biliary tree can be further evaluated using magnetic resonance cholangiopancreatography (MRCP) or endoscopic retrograde cholangiopancreatography (ERCP), with the latter allowing for therapeutic options, such as biliary stent placement to relieve obstruction 17. Endoscopic ultrasonography can be used in addition to endoscopic retrograde cholangiopancreatography (ERCP) for evaluation of common bile duct obstructions and can help determine if the obstruction is from a mass or stone.
Liver Biopsy
Liver biopsy should is reserved for cases of jaundice in which the diagnosis is unclear after the initial history and physical examination, laboratory studies, and imaging. It should be performed only if biopsy results are required to determine treatment and prognosis. Biopsy may alter care in only about one-third of cases 17.
Hyperbilirubinemia treatment
Hyperbilirubinemia treatment depends on many factors, including treating the underlying cause of the hyperbilirubinemia, the level of bilirubin, your age and general health. The goal is to keep the level of bilirubin from increasing to dangerous levels while minimizing any negative effects of the treatment.
Hyperbilirubinemia treatment may include:
- Phototherapy. During phototherapy, the baby is placed under ultraviolet light. Phototherapy may take several hours to begin working and is used throughout the day and night. The baby’s eyes must be protected and the temperature monitored during phototherapy. Blood levels of bilirubin are checked every 6-12 hours to ensure that the phototherapy is working.
- Under special circumstances, an exchange transfusion may be needed to replace the baby’s blood with fresh blood in an attempt to rapidly decrease the bilirubin level. This is done in consultation with the neonatologist.
- Adequate hydration with breastfeeding or pumped breast milk. The American Academy of Pediatrics recommends that, if possible, breastfeeding be continued. Breastfed babies receiving phototherapy who are dehydrated or have excessive weight loss can have supplementation with expressed breast milk or formula.
- Treating any underlying cause of hyperbilirubinemia, such as infection
Unconjugated Hyperbilirubinemia Treatment
Phototherapy and exchange transfusion are the mainstays of treatment for newborns with unconjugated hyperbilirubinemia. Other treatment modalities may be utilized based on patient response to these therapies. The approach to treatment is determined by the neurotoxicity risk factors present, neonatal gestational age, and hour-specific total serum bilirubin 15.
Phototherapy
Bilirubin absorbs light. High bilirubin levels often decrease when a baby is put under special blue spectrum lights. This is called phototherapy 7, 5, 6. Your child may get this treatment in the day and night. It may take several hours for it to start working. During light treatment, your baby’s eyes will be protected. Your baby’s doctor will check your baby’s temperature. They will also test your baby’s bilirubin levels. This will tell if phototherapy is working.
Bilirubin optimally absorbs light in the blue-green range (ie, 460-490 nm). The underlying mechanism of phototherapy involves inducing photoisomerization and converting bilirubin into lumirubin, which is readily excreted into bile and urine 79. During phototherapy, the neonate’s maximum body surface area should be exposed to the light source while keeping the eyes covered to avoid retinal injury, and interruptions should be minimized. The maintenance of hydration is necessary to ensure adequate urine output, as most bilirubin is excreted in the urine as lumirubin, a structural isomer of bilirubin formed during phototherapy. Therefore, breastfeeding support should be offered to all nursing mothers as early initiation of breastfeeding and frequent, on-demand feeding decreases the likelihood of dehydration. Although supplemental oral water and dextrose water are not recommended, supplemental pumped breastmilk or infant formula can be considered for feeding issues, including infants with ineffective sucking or latching or inadequate maternal milk production 70.
After phototherapy is discontinued, there may be an increase in the total serum bilirubin level, known as the rebound bilirubin. This level is usually lower than the pretreatment level and rarely requires reinitiation of phototherapy 80. Phototherapy is considered safe, but recent evidence suggests a possible association with long-term complications, including a small risk of childhood seizures. However, no studies have proven causation 81. A few studies also have reported a possible association between solid organ tumors and nonlymphocytic leukemias and children treated with phototherapy 82, 83. Adverse effects of phototherapy include rashes, dehydration, hypocalcemia, retinal damage, hemolysis due to oxidative damage, delay in patent ductus arteriosis closure in preterm infants, and allergic reactions 84. Bronze baby syndrome is a self-limited condition associated with elevated levels of conjugated bilirubin that rarely occurs with phototherapy, resulting in irregular, bronze-gray pigmentation of the skin, mucous membranes, and urine. The Bronze baby syndrome’s mechanism is unclear but appears to be related to the accumulation of bilirubin and biliverdin photoisomers. Bronze baby syndrome usually resolves within a few days of discontinuing phototherapy; however, the prognosis depends upon the underlying cause of the conjugated hyperbilirubinemia 85, 86.
Fiber optic blanket
A fiber optic blanket is another form of phototherapy. The blanket is usually put under your baby. It may be used alone or with regular phototherapy.
Exchange transfusion
Exchange transfusion is the treatment that involves removing your baby’s blood that has a high bilirubin level and replacing it with fresh donor blood or plasma 87. This raises your baby’s red blood cell count. It also lowers their bilirubin level. During the procedure, your baby will switch between giving and getting small amounts of blood. This will be done through a vein or artery in the baby’s umbilical cord. It is only done in an intensive care nursery when bilirubin levels are extremely high. Your baby may need to have this procedure again if their bilirubin levels stay high.
Exchange transfusion is now the second-line treatment for severe unconjugated hyperbilirubinemia since phototherapy was developed in the 1950s 88, 89. Indications for exchange transfusion include neonatal failure to respond to phototherapy or a total serum bilirubin level at the exchange transfusion threshold. The threshold to initiate exchange transfusion is calculated based on several factors, including the total serum bilirubin level and rate of rise, neonatal age (ie, hours or days since birth), and risk factors for neurologic complications 70. Exchange transfusion rapidly removes bilirubin and hemolysis-causing antibodies from the infant’s circulation. A double-volume exchange blood transfusion (160-180 ml/kg) is performed, replacing aliquots of the neonate’s blood with crossed-matched donor blood. Since most of the total body bilirubin is extravascular, the total serum bilirubin level immediately following exchange transfusion is approximately 60% of the pre-exchange level, but that later increases to 70% to 80% of the pretreatment level as a result of equilibrium. During exchange transfusion, the neonate’s vital signs should be monitored closely. Following the procedure, total serum bilirubin, complete blood count, serum calcium, glucose, and electrolytes should be rechecked due to potential complications, including electrolyte abnormalities (eg, hypocalcemia and hyperkalemia), cardiac arrhythmias, thrombocytopenia, blood-borne infections, portal vein thrombosis, graft versus host disease, and necrotizing enterocolitis (NEC) 90, 91. Phototherapy should resume after exchange transfusion until the bilirubin reaches a level where phototherapy can be safely discontinued.
Intravenous immunoglobulin (IVIg)
Jaundice may be related to blood type differences between mother and baby. This condition results in the baby carrying antibodies from the mother that contribute to the rapid breakdown of the baby’s red blood cells. Intravenous transfusion of an immunoglobulin (IVIg), a blood protein that can reduce levels of antibodies, may decrease jaundice and lessen the need for an exchange transfusion, although results are not conclusive. The American Academy of Pediatrics recommends intravenous immunoglobulin (IVIg) infusion in immune-mediated hemolysis if total serum bilirubin remains within 2 to 3 mg/dL of the exchange threshold despite intensive phototherapy 92, 93. However, the evidence that intravenous immunoglobulin (IVIg) reduces the need for exchange transfusion is unclear. Nonetheless, intravenous immunoglobulin (IVIg) is often used in clinical practice to manage severe unconjugated hyperbilirubinemia 5.
Feeding with breastmilk
The American Academy of Pediatrics says that you should keep breastfeeding a baby with jaundice. If your baby has not been getting enough milk at the breast, you may need to supplement with pumped breastmilk or formula.
Feeding more frequently will provide your baby with more milk and cause more bowel movements, increasing the amount of bilirubin eliminated in your baby’s stool. Infants who are breastfed should have 8 to 12 feedings a day for the first several days of life. Formula-fed infants usually should have 1 to 2 ounces (about 30 to 60 milliliters) of formula every 2 to 3 hours for the first week.
Supplemental feedings
If your baby is having trouble breastfeeding, is losing weight or is dehydrated, your baby’s doctor may suggest giving your baby formula or expressed milk to supplement breastfeeding. Depending on the situation, your baby’s doctor may recommend using formula alone for a couple of days and then resuming breastfeeding. Ask your baby’s doctor what feeding options are right for your baby.
Conjugated Hyperbilirubinemia Treatment
Treatment of conjugated hyperbilirubinemia is tailored to the specific underlying cause of the jaundice. To achieve the best outcomes, patients diagnosed with biliary atresia require a Kasai operation (hepatic portoenterostomy) within the first 2 months of life to prevent irreversible liver damage 103. The surgery involves the removal of the atretic biliary ducts and fibrous plate and anastomosis of the jejunum with the remaining ducts by a Roux-en-Y procedure to provide an alternative pathway for biliary drainage 104. Infectious causes of cholestasis are treated with specific antimicrobial agents, whereas treatment with cholic acid and chenodeoxycholic acid is often curative for many bile acid synthesis disorders. Patients with gestational alloimmune liver disease (GALD) appear to respond well to intravenous immunoglobulin (IVIg) and double-volume exchange transfusion. Patients with conditions of cholestasis (eg, gestational alloimmune liver disease (GALD) and biliary atresia) and severe hepatic damage may require liver transplantation, which is curative but technically challenging in infants 105. Parenteral nutrition-associated cholestasis (PNAC) is managed with cyclic parenteral nutrition, reducing the duration of exposure and initiating enteral feeds as early as possible. The manganese and copper content of parenteral nutrition should be monitored closely to minimize liver injury.
Adults hyperbilirubinemia treatment
Adult hyperbilirubinemia treatment focuses on addressing the underlying cause. Doctors may use imaging like ultrasound, CT scans, or MRI to identify the cause, and procedures like ERCP to both diagnose and treat the problem. Common treatments include: medication adjustment, surgery to remove gallstones or other blockages, treatments for liver disease, lifestyle changes, and in rare, severe cases, liver transplantation. Mild cases, like Gilbert’s syndrome, usually don’t require treatment.
Adult hyperbilirubinemia treatment by cause:
- Gallstones: Surgery (cholecystectomy) to remove the gallbladder, or procedures like endoscopic retrograde cholangiopancreatography (ERCP) to remove or break up gallstones and relieve the obstruction.
- Liver disease: Treatment depends on the specific liver condition. For viral hepatitis, treatment focuses on antivirals or, in severe cases, a liver transplant. Lifestyle measures like a healthy diet, avoiding alcohol, and staying hydrated may support liver health.
- Medication-induced: If a medication is causing it, a doctor may switch you to a different drug.
- Bile duct obstruction: Procedures like endoscopic retrograde cholangiopancreatography (ERCP) may be used to clear the obstruction.
- Hemolytic anemia: Treatment will target the underlying cause of red blood cell breakdown.
- Mild or benign conditions: Conditions like Gilbert’s syndrome and Rotor syndrome are generally benign and do not require specific treatment. For conditions like Gilbert’s syndrome, lifestyle adjustments can help manage symptoms, including getting adequate sleep, staying hydrated, avoiding excessive exercise or fasting, and managing stress.
Managing complications
Your doctor can treat the complications of hyperbilirubinemia, such as severe itching, by prescribing medication like cholestyramine.
Hyperbilirubinemia prognosis
Most patients with unconjugated hyperbilirubinemia have an excellent prognosis. The prognosis in neonatal jaundice is excellent if the baby receives the recommended standard of care. In most cases, neonatal jaundice gets better within one or two weeks. In some cases, such as breast milk jaundice and maternal serum jaundice, jaundice can persist for several weeks. Therefore, the serum bilirubin levels need to be monitored closely, with adequate adjustments in treatment made accordingly to prevent persistent hyperbilirubinemia and thereby its consequence, kernicterus and bilirubin induced neurologic dysfunction. The prognosis of patients with ineffective erythropoiesis, which causes the overproduction of bilirubin is also excellent and depends on the cause.
Patients with Crigler Najjar syndrome type 1 have a high risk of kernicterus, and thereby present a poor prognosis and need intensive, aggressive management. The common medications used for the treatment of patients with Crigler Najjar syndrome type 1 are phenobarbital, calcium (infusions), ursodeoxycholic acid, metalloporphyrins, chlorpromazine, and cholestyramine. The emergent treatment for bilirubin encephalopathy relies on repeated plasma exchange transfusions followed by long-term phototherapy 106. The process of plasma exchange transfusion flushes out bilirubin-saturated albumin and provides free protein, which lures bilirubin from the tissues. To maintain the levels of unconjugated hyperbilirubinemia below the neurotoxic threshold, patients with Crigler-Najjar syndrome type 1 generally need phototherapy for 10 to 12 hours a day. Phototherapy helps in converting bilirubin to more water-soluble bilirubin isoforms that can get excreted in the urine. The efficacy of phototherapy is dose-dependent and depends on the intensity of light, exposure of the body surface, or reflecting mirrors used. Short-term complications of phototherapy are reduced cardiac output and renal perfusion, hyperthermia, increased cerebral perfusion, oxidative stress, skin rash, breastfeeding interruption, and rarely bronze baby syndrome 88. The bronze baby syndrome is a rare, reversible dark, grayish-brown skin, serum, and urine discoloration, caused by bronze pigmented photoisomers, identified in infants treated with phototherapy 107. Pigments are eliminated slowly after phototherapy discontinuation, and resolution is seen within weeks without any complications 108. Some side effects associated with long-term phototherapy are restriction of activity, delay in normal development, diarrhea, reduced weight gain, problems in maintaining body temperature, and risk of seizures (greater in boys) 81.
The prognosis of Crigler Najjar syndrome type 2 is more favorable and rarely associated with kernicterus. Individuals with Crigler Najjar syndrome type 2 do not require any treatment and can be managed with phenobarbital.
Gilbert syndrome is a benign inherited disorder, and patients with this syndrome have an excellent prognosis. An individual affected with Gilbert syndrome can live a normal life without needing medical therapy and phenobarbital has been effectively shown to decrease bilirubin production. Recent studies have shown that a person with Gilbert syndrome has a low risk of cardiovascular diseases, possibly due to an increase in bilirubin ameliorating oxidative stress 109, 110. Long-term survival is identified in patients that had liver transplantation 111.
Neonates with jaundice from causes with poor prognoses often require multidisciplinary consultations, and parents should be adequately counseled and supported.
- Joseph A, Samant H. Jaundice. [Updated 2023 Aug 8]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK544252[↩][↩]
- Singh A, Koritala T, Jialal I. Unconjugated Hyperbilirubinemia. [Updated 2023 Feb 20]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK549796[↩][↩][↩][↩]
- Chastain AP, Geary AL, Bogenschutz KM. Managing neonatal hyperbilirubinemia: An updated guideline. JAAPA. 2024 Oct 1;37(10):19-25. doi: 10.1097/01.JAA.0000000000000120[↩]
- Par EJ, Hughes CA, DeRico P. Neonatal Hyperbilirubinemia: Evaluation and Treatment. Am Fam Physician. 2023 May;107(5):525-534. https://www.aafp.org/pubs/afp/issues/2023/0500/neonatal-hyperbilirubinemia.html[↩][↩][↩][↩][↩][↩]
- Ansong-Assoku B, Adnan M, Daley SF, et al. Neonatal Jaundice. [Updated 2024 Feb 12]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK532930[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Horn D, Ehret D, Gautham KS, Soll R. Sunlight for the prevention and treatment of hyperbilirubinemia in term and late preterm neonates. Cochrane Database Syst Rev. 2021 Jul 6;7(7):CD013277. doi: 10.1002/14651858.CD013277.pub2[↩][↩][↩]
- Gottimukkala SB, Lobo L, Gautham KS, Bolisetty S, Fiander M, Schindler T. Intermittent phototherapy versus continuous phototherapy for neonatal jaundice. Cochrane Database Syst Rev. 2023 Mar 2;3(3):CD008168. doi: 10.1002/14651858.CD008168.pub2[↩][↩][↩]
- Qian S, Kumar P, Testai FD. Bilirubin Encephalopathy. Curr Neurol Neurosci Rep. 2022 Jul;22(7):343-353. doi: 10.1007/s11910-022-01204-8[↩]
- Hegyi T, Kleinfeld A. Neonatal hyperbilirubinemia and the role of unbound bilirubin. J Matern Fetal Neonatal Med. 2022 Dec;35(25):9201-9207. doi: 10.1080/14767058.2021.2021177[↩]
- Maisels MJ. Neonatal jaundice. Pediatr Rev. 2006 Dec;27(12):443-54. doi: 10.1542/pir.27-12-443[↩][↩][↩][↩][↩]
- Kemper AR, Newman TB, Slaughter JL, et al. Clinical Practice Guideline Revision: Management of Hyperbilirubinemia in the Newborn Infant 35 or More Weeks of Gestation. Pediatrics. 2022 Sep 1;150(3):e2022058859. doi: 10.1542/peds.2022-058859[↩][↩][↩]
- Gottesman LE, Del Vecchio MT, Aronoff SC. Etiologies of conjugated hyperbilirubinemia in infancy: a systematic review of 1692 subjects. BMC Pediatr. 2015 Nov 20;15:192. doi: 10.1186/s12887-015-0506-5[↩]
- Harpavat S, Garcia-Prats JA, Anaya C, Brandt ML, Lupo PJ, Finegold MJ, Obuobi A, ElHennawy AA, Jarriel WS, Shneider BL. Diagnostic Yield of Newborn Screening for Biliary Atresia Using Direct or Conjugated Bilirubin Measurements. JAMA. 2020 Mar 24;323(12):1141-1150. doi: 10.1001/jama.2020.0837[↩]
- Davis AR, Rosenthal P, Escobar GJ, Newman TB. Interpreting conjugated bilirubin levels in newborns. J Pediatr. 2011 Apr;158(4):562-565.e1. doi: 10.1016/j.jpeds.2010.09.061[↩]
- American Academy of Pediatrics Subcommittee on Hyperbilirubinemia. Management of hyperbilirubinemia in the newborn infant 35 or more weeks of gestation. Pediatrics. 2004 Jul;114(1):297-316. doi: 10.1542/peds.114.1.297. Erratum in: Pediatrics. 2004 Oct;114(4):1138.[↩][↩][↩][↩][↩]
- Infant jaundice. https://www.mayoclinic.org/diseases-conditions/infant-jaundice/symptoms-causes/syc-20373865[↩][↩][↩]
- Winger J, Michelfelder A. Diagnostic approach to the patient with jaundice. Prim Care. 2011 Sep;38(3):469-82; viii. doi: 10.1016/j.pop.2011.05.004[↩][↩][↩][↩][↩][↩][↩][↩]
- Roche SP, Kobos R. Jaundice in the adult patient. Am Fam Physician. 2004 Jan 15;69(2):299-304. https://www.aafp.org/pubs/afp/issues/2004/0115/p299.html[↩][↩][↩]
- Kalakonda A, Jenkins BA, John S. Physiology, Bilirubin. [Updated 2022 Sep 12]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK470290[↩]
- Kosmachevskaya OV, Topunov AF. Alternate and Additional Functions of Erythrocyte Hemoglobin. Biochemistry (Mosc). 2018 Dec;83(12):1575-1593. doi: 10.1134/S0006297918120155[↩]
- Dosch AR, Imagawa DK, Jutric Z. Bile Metabolism and Lithogenesis: An Update. Surg Clin North Am. 2019 Apr;99(2):215-229. doi: 10.1016/j.suc.2018.12.003[↩]
- Shen H, Zeng C, Wu X, Liu S, Chen X. Prognostic value of total bilirubin in patients with acute myocardial infarction: A meta-analysis. Medicine (Baltimore). 2019 Jan;98(3):e13920. doi: 10.1097/MD.0000000000013920[↩]
- Franchini M, Targher G, Lippi G. Serum bilirubin levels and cardiovascular disease risk: a Janus Bifrons? Adv Clin Chem. 2010;50:47-63. doi: 10.1016/s0065-2423(10)50003-9[↩]
- Vítek L, Schwertner HA. The heme catabolic pathway and its protective effects on oxidative stress-mediated diseases. Adv Clin Chem. 2007;43:1-57. doi: 10.1016/s0065-2423(06)43001-8[↩][↩]
- Vítek L, Ostrow JD. Bilirubin chemistry and metabolism; harmful and protective aspects. Curr Pharm Des. 2009;15(25):2869-83. doi: 10.2174/138161209789058237[↩]
- Jedlitschky G, Hoffmann U, Kroemer HK. Structure and function of the MRP2 (ABCC2) protein and its role in drug disposition. Expert Opin Drug Metab Toxicol. 2006 Jun;2(3):351-66. doi: 10.1517/17425255.2.3.351[↩]
- Hashmi MF, Mehta D. Rotor Syndrome. [Updated 2023 Feb 19]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK532306[↩][↩][↩]
- Rotor syndrome. https://medlineplus.gov/genetics/condition/rotor-syndrome[↩][↩][↩]
- Fargo MV, Grogan SP, Saguil A. Evaluation of Jaundice in Adults. Am Fam Physician. 2017 Feb 1;95(3):164-168. https://www.aafp.org/pubs/afp/issues/2017/0201/p164.html[↩][↩]
- Nelson M, Mulani SR, Saguil A. Evaluation of Jaundice in Adults. Am Fam Physician. 2025 Jan;111(1):25-30. https://www.aafp.org/pubs/afp/issues/2025/0100/jaundice.html[↩]
- Dennery PA, Seidman DS, Stevenson DK. Neonatal hyperbilirubinemia. N Engl J Med. 2001 Feb 22;344(8):581-90. doi: 10.1056/NEJM200102223440807[↩][↩][↩]
- Kenwright S, Levi AJ. Sites of competition in the selective hepatic uptake of rifamycin-SV, flavaspidic acid, bilirubin, and bromsulphthalein. Gut. 1974 Mar;15(3):220-6. https://pmc.ncbi.nlm.nih.gov/articles/instance/1412884/pdf/gut00616-0068.pdf[↩]
- Radlović N. Hereditary hyperbilirubinemias. Srp Arh Celok Lek. 2014 Mar-Apr;142(3-4):257-60. doi: 10.2298/sarh1404257r[↩]
- ARIAS IM, WOLFSON S, LUCEY JF, MCKAY RJ Jr. TRANSIENT FAMILIAL NEONATAL HYPERBILIRUBINEMIA. J Clin Invest. 1965 Sep;44(9):1442-50. https://pmc.ncbi.nlm.nih.gov/articles/instance/292625/pdf/jcinvest00257-0028.pdf[↩]
- Grunebaum E, Amir J, Merlob P, Mimouni M, Varsano I. Breast mild jaundice: natural history, familial incidence and late neurodevelopmental outcome of the infant. Eur J Pediatr. 1991 Feb;150(4):267-70. doi: 10.1007/BF01955528[↩]
- Maisels MJ, Clune S, Coleman K, Gendelman B, Kendall A, McManus S, Smyth M. The natural history of jaundice in predominantly breastfed infants. Pediatrics. 2014 Aug;134(2):e340-5. doi: 10.1542/peds.2013-4299[↩]
- Maisels MJ, Kring E. Length of stay, jaundice, and hospital readmission. Pediatrics. 1998 Jun;101(6):995-8. doi: 10.1542/peds.101.6.995[↩]
- Zhang D, Chando TJ, Everett DW, Patten CJ, Dehal SS, Humphreys WG. In vitro inhibition of UDP glucuronosyltransferases by atazanavir and other HIV protease inhibitors and the relationship of this property to in vivo bilirubin glucuronidation. Drug Metab Dispos. 2005 Nov;33(11):1729-39. doi: 10.1124/dmd.105.005447[↩]
- National Collaborating Centre for Women’s and Children’s Health (UK). Neonatal Jaundice. London: RCOG Press; 2010 May. (NICE Clinical Guidelines, No. 98.) Available from: https://www.ncbi.nlm.nih.gov/books/NBK65119[↩][↩][↩]
- Practice parameter: management of hyperbilirubinemia in the healthy term newborn. American Academy of Pediatrics. Provisional Committee for Quality Improvement and Subcommittee on Hyperbilirubinemia. Pediatrics. 1994 Oct;94(4 Pt 1):558-65. Erratum in: Pediatrics 1995 Mar;95(3):458-61.[↩]
- Jaundice and hyperbilirubinemia in the newborn. In: Behrman RE, Kliegman RM, Jenson HB, eds. Nelson Textbook of pediatrics. 16th ed. Philadelphia: Saunders, 2000:511–28.[↩]
- Moerschel SK, Cianciaruso LB, Tracy LR. A practical approach to neonatal jaundice. Am Fam Physician. 2008 May 1;77(9):1255-62. https://www.aafp.org/pubs/afp/issues/2008/0501/p1255.html[↩][↩]
- Porter ML, Dennis BL. Hyperbilirubinemia in the term newborn. Am Fam Physician. 2002 Feb 15;65(4):599-606. https://www.aafp.org/pubs/afp/issues/2002/0215/p599.html[↩]
- Reddy DK, Pandey S. Kernicterus. [Updated 2023 Jun 25]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK559120[↩][↩][↩][↩]
- Ali R, Ahmed S, Qadir M, Ahmad K. Icterus Neonatorum in Near-Term and Term Infants: An overview. Sultan Qaboos Univ Med J. 2012 May;12(2):153-60. doi: 10.12816/0003107[↩]
- Ding Y, Wang S, Guo R, Zhang A, Zhu Y. High levels of unbound bilirubin are associated with acute bilirubin encephalopathy in post-exchange transfusion neonates. Ital J Pediatr. 2021 Sep 15;47(1):187. doi: 10.1186/s13052-021-01143-z. Erratum in: Ital J Pediatr. 2023 Feb 15;49(1):22. doi: 10.1186/s13052-023-01432-9[↩]
- Kernicterus. https://emedicine.medscape.com/article/975276-overview[↩]
- Alkén J, Håkansson S, Ekéus C, Gustafson P, Norman M. Rates of Extreme Neonatal Hyperbilirubinemia and Kernicterus in Children and Adherence to National Guidelines for Screening, Diagnosis, and Treatment in Sweden. JAMA Netw Open. 2019 Mar 1;2(3):e190858. doi: 10.1001/jamanetworkopen.2019.0858[↩][↩][↩][↩]
- Leung AK, Sauve RS. Breastfeeding and breast milk jaundice. J R Soc Health. 1989 Dec;109(6):213-7. doi: 10.1177/146642408910900615[↩][↩]
- Gamaleldin R, Iskander I, Seoud I, Aboraya H, Aravkin A, Sampson PD, Wennberg RP. Risk factors for neurotoxicity in newborns with severe neonatal hyperbilirubinemia. Pediatrics. 2011 Oct;128(4):e925-31. doi: 10.1542/peds.2011-0206[↩][↩][↩][↩][↩]
- Raines DA, Krawiec C, Weisbrod LJ, et al. Cephalohematoma. [Updated 2024 Jun 8]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK470192[↩][↩]
- Cichoz-Lach H, Celiński K, Słomka M. Congenital nonhemolytic hyperbilirubinemias. Ann Univ Mariae Curie Sklodowska Med. 2004;59(1):449-52.[↩][↩]
- Bashir BA, Othman SA. Neonatal polycythaemia. Sudan J Paediatr. 2019;19(2):81-83. doi: 10.24911/SJP.106-1566075225[↩][↩]
- Polycythemia – newborn. https://www.mountsinai.org/health-library/diseases-conditions/polycythemia-newborn[↩][↩]
- Wiswell TE, Cornish JD, Northam RS. Neonatal polycythemia: frequency of clinical manifestations and other associated findings. Pediatrics. 1986 Jul;78(1):26-30.[↩][↩]
- Watchko JF, Spitzer AR, Clark RH. Prevalence of Hypoalbuminemia and Elevated Bilirubin/Albumin Ratios in a Large Cohort of Infants in the Neonatal Intensive Care Unit. J Pediatr. 2017 Sep;188:280-286.e4. doi: 10.1016/j.jpeds.2017.06.004[↩][↩]
- Plosa EJ, Esbenshade JC, Fuller MP, Weitkamp JH. Cytomegalovirus infection. Pediatr Rev. 2012 Apr;33(4):156-63; quiz 163. doi: 10.1542/pir.33-4-156[↩][↩]
- Roelofsen H, van der Veere CN, Ottenhoff R, Schoemaker B, Jansen PL, Oude Elferink RP. Decreased bilirubin transport in the perfused liver of endotoxemic rats. Gastroenterology. 1994 Oct;107(4):1075-84. doi: 10.1016/0016-5085(94)90232-1[↩][↩]
- Donneborg ML, Hansen BM, Vandborg PK, Rodrigo-Domingo M, Ebbesen F. Extreme neonatal hyperbilirubinemia and kernicterus spectrum disorder in Denmark during the years 2000-2015. J Perinatol. 2020 Feb;40(2):194-202. doi: 10.1038/s41372-019-0566-8[↩][↩][↩]
- Wu YW, Kuzniewicz MW, Wickremasinghe AC, Walsh EM, Wi S, McCulloch CE, Newman TB. Risk for cerebral palsy in infants with total serum bilirubin levels at or above the exchange transfusion threshold: a population-based study. JAMA Pediatr. 2015 Mar;169(3):239-46. doi: 10.1001/jamapediatrics.2014.3036[↩][↩]
- US Preventive Services Task Force. Screening of infants for hyperbilirubinemia to prevent chronic bilirubin encephalopathy: US Preventive Services Task Force recommendation statement. Pediatrics. 2009 Oct;124(4):1172-7. doi: 10.1542/peds.2009-0128[↩][↩]
- Johnson L, Bhutani VK, Karp K, Sivieri EM, Shapiro SM. Clinical report from the pilot USA Kernicterus Registry (1992 to 2004). J Perinatol. 2009 Feb;29 Suppl 1:S25-45. doi: 10.1038/jp.2008.211[↩][↩]
- Bhutani VK, Johnson LH, Keren R. Treating acute bilirubin encephalopathy—before it’s too late. Contemp Pediatr. 2005;22(5):57-74.[↩]
- Sgro M, Campbell D, Shah V. Incidence and causes of severe neonatal hyperbilirubinemia in Canada. CMAJ. 2006 Sep 12;175(6):587-90. doi: 10.1503/cmaj.060328[↩][↩]
- Usman F, Diala UM, Shapiro SM, et al. Acute bilirubin encephalopathy and its progression to kernicterus: current perspectives. Res Rep Neonatol. 2018;8:33-44. https://www.researchgate.net/publication/323611016_Acute_bilirubin_encephalopathy_and_its_progression_to_kernicterus_current_perspectives[↩]
- Sgro M, Campbell DM, Kandasamy S, Shah V. Incidence of chronic bilirubin encephalopathy in Canada, 2007-2008. Pediatrics. 2012 Oct;130(4):e886-90. doi: 10.1542/peds.2012-0253[↩]
- Shapiro SM. Chronic bilirubin encephalopathy: diagnosis and outcome. Semin Fetal Neonatal Med. 2010 Jun;15(3):157-63. doi: 10.1016/j.siny.2009.12.004[↩]
- Le Pichon JB, Riordan SM, Watchko J, Shapiro SM. The Neurological Sequelae of Neonatal Hyperbilirubinemia: Definitions, Diagnosis and Treatment of the Kernicterus Spectrum Disorders (KSDs). Curr Pediatr Rev. 2017;13(3):199-209. doi: 10.2174/1573396313666170815100214[↩]
- Amin SB, Karp JM, Benzley LP. Unconjugated hyperbilirubinemia and early childhood caries in a diverse group of neonates. Am J Perinatol. 2010 May;27(5):393-7. doi: 10.1055/s-0029-1243314[↩]
- Beal JA. American Academy of Pediatrics’ Updated Clinical Guidelines for Managing Neonatal Hyperbilirubinemia. MCN Am J Matern Child Nurs. 2023 Jan-Feb 01;48(1):49. doi: 10.1097/NMC.0000000000000874[↩][↩][↩][↩][↩][↩]
- Amin SB, Saluja S, Saili A, Orlando M, Wang H, Laroia N, Agarwal A. Chronic Auditory Toxicity in Late Preterm and Term Infants With Significant Hyperbilirubinemia. Pediatrics. 2017 Oct;140(4):e20164009. doi: 10.1542/peds.2016-4009[↩][↩]
- Good WV, Hou C. Visuocortical bilirubin-induced neurological dysfunction. Semin Fetal Neonatal Med. 2015 Feb;20(1):37-41. doi: 10.1016/j.siny.2014.12.007[↩]
- Olds C, Oghalai JS. Audiologic impairment associated with bilirubin-induced neurologic damage. Semin Fetal Neonatal Med. 2015 Feb;20(1):42-46. doi: 10.1016/j.siny.2014.12.006[↩]
- Rose J, Vassar R. Movement disorders due to bilirubin toxicity. Semin Fetal Neonatal Med. 2015 Feb;20(1):20-25. doi: 10.1016/j.siny.2014.11.002[↩]
- Wusthoff CJ, Loe IM. Impact of bilirubin-induced neurologic dysfunction on neurodevelopmental outcomes. Semin Fetal Neonatal Med. 2015 Feb;20(1):52-57. doi: 10.1016/j.siny.2014.12.003[↩]
- Johnson L, Bhutani VK. Guidelines for management of the jaundiced term and near-term infant. Clin Perinatol. 1998 Sep;25(3):555-74, viii. https://doi.org/10.1016/S0095-5108(18)30097-6[↩]
- https://bilitool.org/[↩]
- Jaundice in newborn babies under 28 days. London: National Institute for Health and Care Excellence (NICE); 2023 Oct 31. (NICE Guideline, No. 98.) Available from: https://www.ncbi.nlm.nih.gov/books/NBK553311[↩]
- Bhutani VK; Committee on Fetus and Newborn; American Academy of Pediatrics. Phototherapy to prevent severe neonatal hyperbilirubinemia in the newborn infant 35 or more weeks of gestation. Pediatrics. 2011 Oct;128(4):e1046-52. doi: 10.1542/peds.2011-1494[↩][↩]
- Yetman RJ, Parks DK, Huseby V, Mistry K, Garcia J. Rebound bilirubin levels in infants receiving phototherapy. J Pediatr. 1998 Nov;133(5):705-7. doi: 10.1016/s0022-3476(98)70117-9[↩][↩]
- Newman TB, Wu YW, Kuzniewicz MW, Grimes BA, McCulloch CE. Childhood Seizures After Phototherapy. Pediatrics. 2018 Oct;142(4):e20180648. doi: 10.1542/peds.2018-0648[↩][↩][↩]
- Newman TB, Wickremasinghe AC, Walsh EM, Grimes BA, McCulloch CE, Kuzniewicz MW. Retrospective Cohort Study of Phototherapy and Childhood Cancer in Northern California. Pediatrics. 2016 Jun;137(6):e20151354. doi: 10.1542/peds.2015-1354[↩][↩]
- Auger N, Laverdière C, Ayoub A, Lo E, Luu TM. Neonatal phototherapy and future risk of childhood cancer. Int J Cancer. 2019 Oct 15;145(8):2061-2069. doi: 10.1002/ijc.32158[↩][↩]
- Wang J, Guo G, Li A, Cai WQ, Wang X. Challenges of phototherapy for neonatal hyperbilirubinemia (Review). Exp Ther Med. 2021 Mar;21(3):231. doi: 10.3892/etm.2021.9662[↩][↩]
- Itoh S, Okada H, Kuboi T, Kusaka T. Phototherapy for neonatal hyperbilirubinemia. Pediatr Int. 2017 Sep;59(9):959-966. doi: 10.1111/ped.13332[↩][↩]
- Kar S, Mohankar A, Krishnan A. Bronze baby syndrome. Indian Pediatr. 2013 Jun 8;50(6):624. doi: 10.1007/s13312-013-0161-6[↩][↩]
- Pearson CH. Replacement transfusion as a treatment of erythroblastosis fetalis, by Louis K. Diamond, MD, Pediatrics, 1948;2:520-524. Pediatrics. 1998 Jul;102(1 Pt 2):203-5.[↩][↩]
- Hansen TWR, Maisels MJ, Ebbesen F, Vreman HJ, Stevenson DK, Wong RJ, Bhutani VK. Sixty years of phototherapy for neonatal jaundice – from serendipitous observation to standardized treatment and rescue for millions. J Perinatol. 2020 Feb;40(2):180-193. doi: 10.1038/s41372-019-0439-1[↩][↩][↩]
- DIAMOND LK, ALLEN FH Jr, THOMAS WO Jr. Erythroblastosis fetalis. VII. Treatment with exchange transfusion. N Engl J Med. 1951 Jan 11;244(2):39-49. doi: 10.1056/NEJM195101112440201[↩][↩]
- Jackson JC. Adverse events associated with exchange transfusion in healthy and ill newborns. Pediatrics. 1997 May;99(5):E7. doi: 10.1542/peds.99.5.e7[↩][↩]
- Patra K, Storfer-Isser A, Siner B, Moore J, Hack M. Adverse events associated with neonatal exchange transfusion in the 1990s. J Pediatr. 2004 May;144(5):626-31. doi: 10.1016/j.jpeds.2004.01.054[↩][↩]
- Alpay F, Sarici SU, Okutan V, Erdem G, Ozcan O, Gökçay E. High-dose intravenous immunoglobulin therapy in neonatal immune haemolytic jaundice. Acta Paediatr. 1999 Feb;88(2):216-9. doi: 10.1080/08035259950170420[↩][↩]
- Gottstein R, Cooke RW. Systematic review of intravenous immunoglobulin in haemolytic disease of the newborn. Arch Dis Child Fetal Neonatal Ed. 2003 Jan;88(1):F6-10. doi: 10.1136/fn.88.1.f6[↩][↩]
- Watchko JF, Tiribelli C. Bilirubin-induced neurologic damage–mechanisms and management approaches. N Engl J Med. 2013 Nov 21;369(21):2021-30. doi: 10.1056/NEJMra1308124[↩]
- Rand EB, Karpen SJ, Kelly S, Mack CL, Malatack JJ, Sokol RJ, Whitington PF. Treatment of neonatal hemochromatosis with exchange transfusion and intravenous immunoglobulin. J Pediatr. 2009 Oct;155(4):566-71. doi: 10.1016/j.jpeds.2009.04.012[↩]
- Levitt DG, Levitt MD. Quantitative assessment of the multiple processes responsible for bilirubin homeostasis in health and disease. Clin Exp Gastroenterol. 2014 Sep 2;7:307-28. doi: 10.2147/CEG.S64283[↩][↩][↩]
- Korolnek T, Hamza I. Macrophages and iron trafficking at the birth and death of red cells. Blood. 2015 May 7;125(19):2893-7. doi: 10.1182/blood-2014-12-567776[↩]
- Erlinger S, Arias IM, Dhumeaux D. Inherited disorders of bilirubin transport and conjugation: new insights into molecular mechanisms and consequences. Gastroenterology. 2014 Jun;146(7):1625-38. doi: 10.1053/j.gastro.2014.03.047[↩][↩]
- Nguyen KD, Sundaram V, Ayoub WS. Atypical causes of cholestasis. World J Gastroenterol. 2014 Jul 28;20(28):9418-26. doi: 10.3748/wjg.v20.i28.9418[↩]
- Hucl T. Maligní biliární obstrukce [Malignant biliary obstruction]. Cas Lek Cesk. 2016;155(1):30-7. Czech.[↩]
- Wickramasinghe SN, Looareesuwan S, Nagachinta B, White NJ. Dyserythropoiesis and ineffective erythropoiesis in Plasmodium vivax malaria. Br J Haematol. 1989 May;72(1):91-9. doi: 10.1111/j.1365-2141.1989.tb07658.x[↩]
- Goasguen JE, Bennett JM, Bain BJ, Brunning R, Vallespi MT, Tomonaga M, Zini G, Renault A; (The International Working Group on Morphology of MDS). Dyserythropoiesis in the diagnosis of the myelodysplastic syndromes and other myeloid neoplasms: problem areas. Br J Haematol. 2018 Aug;182(4):526-533. doi: 10.1111/bjh.15435[↩]
- Serinet MO, Wildhaber BE, Broué P, Lachaux A, Sarles J, Jacquemin E, Gauthier F, Chardot C. Impact of age at Kasai operation on its results in late childhood and adolescence: a rational basis for biliary atresia screening. Pediatrics. 2009 May;123(5):1280-6. doi: 10.1542/peds.2008-1949[↩]
- Ohi R. Surgery for biliary atresia. Liver. 2001 Jun;21(3):175-82. doi: 10.1034/j.1600-0676.2001.021003175.x[↩]
- Feldman AG, Whitington PF. Neonatal hemochromatosis. J Clin Exp Hepatol. 2013 Dec;3(4):313-20. doi: 10.1016/j.jceh.2013.10.004[↩]
- Strauss KA, Ahlfors CE, Soltys K, Mazareigos GV, Young M, Bowser LE, Fox MD, Squires JE, McKiernan P, Brigatti KW, Puffenberger EG, Carson VJ, Vreman HJ. Crigler-Najjar Syndrome Type 1: Pathophysiology, Natural History, and Therapeutic Frontier. Hepatology. 2020 Jun;71(6):1923-1939. doi: 10.1002/hep.30959[↩]
- Rubaltelli FF, Da Riol R, D’Amore ES, Jori G. The bronze baby syndrome: evidence of increased tissue concentration of copper porphyrins. Acta Paediatr. 1996 Mar;85(3):381-4. doi: 10.1111/j.1651-2227.1996.tb14040.x[↩]
- Tan KL, Jacob E. The bronze baby syndrome. Acta Paediatr Scand. 1982 May;71(3):409-14. doi: 10.1111/j.1651-2227.1982.tb09443.x[↩]
- Kundur AR, Santhakumar AB, Bulmer AC, Singh I. Mildly elevated unconjugated bilirubin is associated with reduced platelet activation-related thrombogenesis and inflammation in Gilbert’s syndrome. Platelets. 2017 Dec;28(8):779-785. doi: 10.1080/09537104.2017.1280146[↩]
- Lin JP, O’Donnell CJ, Schwaiger JP, Cupples LA, Lingenhel A, Hunt SC, Yang S, Kronenberg F. Association between the UGT1A1*28 allele, bilirubin levels, and coronary heart disease in the Framingham Heart Study. Circulation. 2006 Oct 3;114(14):1476-81. doi: 10.1161/CIRCULATIONAHA.106.633206[↩]
- van der Veere CN, Sinaasappel M, McDonagh AF, et al. Current therapy for Crigler-Najjar syndrome type 1: report of a world registry. Hepatology. 1996 Aug;24(2):311-5. doi: 10.1002/hep.510240205[↩]




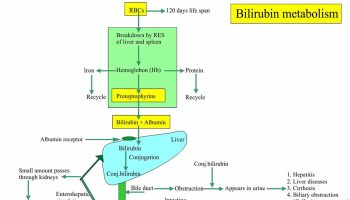
{kind=link}