
Sezary syndrome
Sezary syndrome also called Sézary syndrome, is an aggressive form (grows faster) of a type of blood cancer called cutaneous T-cell lymphoma (CTCL), a term that collectively includes all skin (cutaneous) lymphomas arising from T lymphocytes (T cells) 1, 2, 3. T cells also called T lymphocytes are a type of white blood cell that are a crucial part of your adaptive immune system, protecting your body from pathogens like bacteria and viruses, and from cancer. T cells develop from stem cells in your bone marrow and mature in your thymus, which is why they are called “T” cells. Key functions of T cells include directly killing infected cells, helping B cells fight pathogens, and regulating the overall immune response. Sezary syndrome is named after Albert Sézary, a French dermatologist born in 1880 4. Cutaneous T-cell lymphomas occur when certain white blood cells, called T cells, become cancerous; these cancers characteristically affect the skin, causing different types of skin lesions. In Sezary syndrome, the cancerous T cells, called Sezary cells, are present in the blood, skin, and lymph nodes 5, 6. Sézary cells are cancerous T-cells (T lymphocytes) with an abnormally folded nucleus that looks like a brain described as cerebriform 7. Sézary cells are the hallmark of Sézary syndrome, an aggressive form of cutaneous T-cell lymphoma, and can be found in the blood, skin, and lymph nodes of affected individuals. Sézary cells can lead to a widespread, red, and severely itchy rash (erythroderma).
Characteristics of Sézary cells 7:
- Nucleus: Prominently folded or convoluted, often described as cerebriform (brain-like).
- Size: Intermediate to large, larger than normal T-cells.
- Cytoplasm: Variable amounts of agranular (nongranular) cytoplasm, sometimes containing vacuoles.
- Chromatin: Mildly condensed
Sézary cells have a variable amount of nongranular cytoplasm and show the characteristic convoluted to cerebriform (looks like a brain) nucleus with mildly condensed chromatin and inconspicuous nucleoli (see Figure 3). Sézary cellsmay vary in size, with the smaller forms referred to as Lutzner cells.
Most people with Sezary syndrome develop a red, severely itchy skin rash called erythroderma that covers large portions of their body (at least 80 percent of their body). Sézary cells are found in the skin rash. However, the skin cells themselves are not cancerous; the skin problems result when Sezary cells (cancerous T-cells) move from the blood into the skin. People with Sezary syndrome also have enlarged lymph nodes (lymphadenopathy). Other common signs and symptoms of Sezary syndrome include hair loss (alopecia), skin swelling (edema), thickened skin on the palms of the hands and soles of the feet (palmoplantar keratoderma), abnormalities of the fingernails and toenails, and lower eyelids that turn outward (ectropion). Some people with Sezary syndrome are less able to control their body temperature than people without the condition.
The cancerous T cells can spread to other organs in the body, including the lymph nodes, liver, spleen, and bone marrow. In addition, affected individuals have an increased risk of developing another lymphoma or other type of cancer.
Although Sézary syndrome is sometimes referred to as a variant of another cutaneous T-cell lymphoma (CTCL) called mycosis fungoides, these two cancers are generally considered separate conditions. Sezary syndrome is the second most common form of cutaneous T-cell lymphoma (CTCL) after mycosis fungoides, accounting for approximately 3 to 5 percent of cases of cutaneous T-cell lymphoma (CTCL).
There are about 3,000 new cases of cutaneous T-cell lymphoma (CTCL) each year in the U.S. and approximately 15 percent of those are diagnosed as Sézary syndrome 8. Although Sézary syndrome can affect people of any age, Sézary syndrome is most common in adults ages 50 and over, and is slightly more common in men than women. Sezary syndrome worldwide incidence appears to be 0.8 to 0.9 per million with a male to female ratio of 2:1. Sezary syndrome is not an inherited disease. There are no known risk factors for Sézary syndrome 8.
Sézary syndrome usually progresses rapidly and historically, affected individuals survived an average of 2 to 4 years after development of the condition, although survival has improved with newer treatments.
Because Sézary syndrome is chronic and systemic (affecting the entire body), Sézary syndrome is usually not treated with skin-directed therapies alone. The specific treatment for individual patients is based on a variety of factors, including the patient’s general health and stage of the disease.
Sézary syndrome common treatments include 8:
- Extracorporeal photopheresis (ECP), a procedure used to expose the blood to ultraviolet light.
- Targeted therapy which can bind directly to cancer cells that express specific markers or impact specific internal signaling pathways used by cancer cells to grow or survive.
- Biologic, or immunotherapy, is a cancer treatment that uses the body’s own immune system to fight cancer cells. It works by making it easier for immune cells to recognize and attack cancer, by boosting the immune system’s activity, or by removing the brakes that prevent the immune system from attacking cancer cells. Key types of immunotherapy include checkpoint inhibitors, CAR T-cell therapy, and oncolytic virus therapy.
- Chemotherapy, a drug given either orally or through an infusion in a vein, to stop the growth of rapidly dividing cancer cells.
- Skin-directed therapy such as phototherapy (using light, most commonly ultraviolet (UV) light) or radiation therapy (uses high-energy radiation, such as X-rays, to destroy cancer cells or damage them so they cannot grow, multiply, or spread ) may be used in combination with other systemic therapies.
Figure 1. Sezary syndrome rash

Figure 2. Plantar keratoderma in Sézary syndrome

Footnote: Plantar Keratoderma at the time of diagnosis (A) and after 1 month of treatment (B). A 65‐year‐old woman presented with a 4‐year history of progressive refractory diffuse itch (pruritus). She had been diagnosed 4 months earlier with cutaneous T‐cell lymphoma (CTCL) stage I (mycosis fungoides). After being treated unsuccessfully with psoralen plus ultraviolet A (PUVA) radiation therapy for 31 sessions, she was eventually diagnosed with CTCL stage IVA2 (Sézary syndrome) on the basis of severe worsening itch (pruritus), erythroderma (intense and usually widespread reddening of the skin), palmoplantar keratoderma with skin ulcerations causing cellulitis (A), left eye ectropion, lymphanedopathy, positive skin biopsy and left inguinal lymph node biopsy, raised lactate dehydrogenase (LDH), Sézary cells over 1000/μL with positive clonality, CD4/CD8 ratio: 12.5, and CT chest, abdomen and pelvis showing inguinal and axillary lymphadenopathy with no visceral involvement. With bexarotene, interferon‐alfa, and extracorporeal photopheresis (ECP), her keratoderma stabilized (B), and after 2 months of treatment with keratolytics (6% salicylic acid in 70% propylene glycol and clobetasol), it largely cleared.
[Source 9 ]Figure 3. Sézary cells
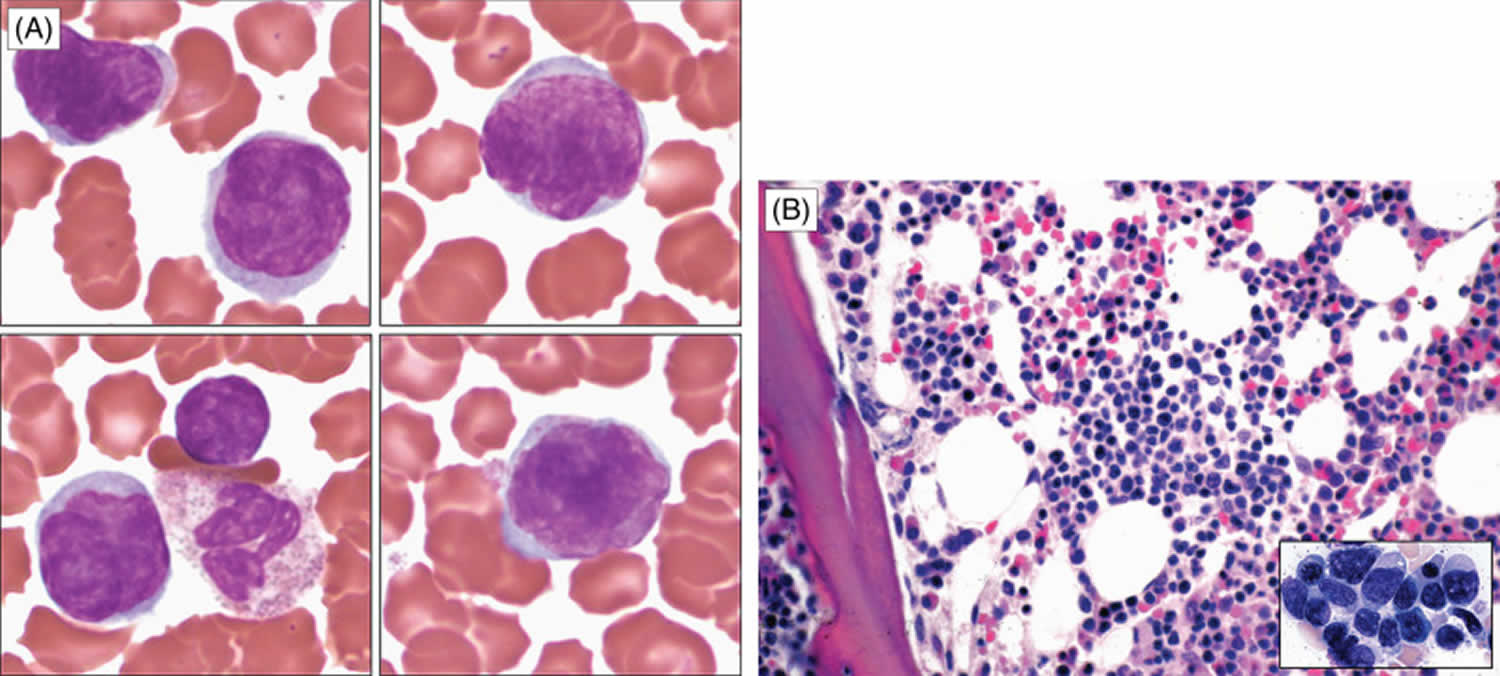
Footnotes: Several Sézary cells with convoluted nuclei are demonstrated in the blood smear (A). Bone marrow biopsy section (B) and smear (B, inset) show an aggregate of atypical lymphocytes with irregular nuclei.
[Source 7 ]Can Sezary syndrome be cured?
Sezary syndrome is difficult to cure. Treatment is usually palliative, with the intention of relief of symptoms and improvement in the quality of life. Patients may live many years with the disease 10.
Sezary syndrome causes
Although a small percentage of cases of Sezary syndrome are associated with human T-lymphotropic viruses type 1 and type 2, the underlying cause of most cases is currently unknown 11. In most affected individuals, the cancerous T-cells also called Sezary cells usually have one or more chromosomal abnormalities, such as the loss or gain of genetic material 6. These abnormalities occur during a person’s lifetime and are found only in the DNA of cancerous cells. Abnormalities have been found on most chromosomes, but some regions are more commonly affected than others. People with Sezary syndrome tend to have losses of DNA from regions of chromosomes 10 and 17 or additions of DNA to regions of chromosomes 8 and 17 6. However, it is unclear whether these alterations play a role in Sezary syndrome, although the tendency to acquire chromosomal abnormalities (chromosomal instability) is a feature of many cancers. It can lead to genetic changes that allow cells to grow and divide uncontrollably.
Rare cases of cancer including Sézary syndrome during treatment with JAK inhibitors have been reported 4. Causality has not been established and requires further investigation 4.
The role of Staphylococcus aureus superantigen or chronic antigen stimulation has been proposed to lead to clonal expansion of T-cell and malignant transformation 4.
The malignant T cells in the skin and blood have the following characteristics:
- CD4 positive: this indicates they are central memory T cells
- A significant percentage exhibit loss of CD26 and CD7
- Abnormal clonal Th2 cells
- Reduced Th1 (T-helper) cells
This contributes to endogenous immunosuppression.
Is Sezary syndrome inherited?
The underlying cause of Sezary syndrome is unknown in most cases. However, it generally occurs sporadically in people with no family history of the condition and is not thought to be inherited in most cases 6.
Sezary syndrome symptoms
Sezary syndrome is an aggressive form of cutaneous T-cell lymphoma (CTCL) which is a group of disorders that occur when T-cells (a type of white blood cell) become cancerous and affect the skin. In Sezary syndrome, specifically, the cancerous T cells are called Sezary cells (large T cells with an abnormal shape) and are found in the skin, lymph nodes, and blood. They can also spread to other organs in the body, including the liver, spleen, and bone marrow 12.
In Sezary syndrome, the skin all over the body is reddened (erythroderma), itchy, peeling, and painful. There may also be patches, plaques, or tumors on the skin. It is not known if Sézary syndrome is an advanced form of mycosis fungoides or a separate disease.
Although Sezary syndrome can affect people of all ages, it is most commonly diagnosed in adults over age 60. The signs and symptoms of Sezary syndrome can vary but may include 12:
- A red, itchy skin rash that covers large portions of the body, often with shedding of the outer layer (exfoliation).
- Feeling cold (loss of temperature control by the skin).
- Enlarged lymph nodes (lymphadenopathy)
- Alopecia (hair loss)
- Thickened skin on the palms of the hands and soles of the feet (palmoplantar keratoderma)
- Abnormalities of the fingernails and toenails commonly paronychia, leukonychia, onycholysis are seen but onychoschizia, onychauxis, distal notching and anonychia seem to be more specific changes 4.
- Frequent skin infections (for instance, with Staphylococcus aureus).
- Ectropion a medical condition where the eyelid, most often the lower one, turns outward away from the eyeball. This causes the inner eyelid to become exposed, leading to symptoms like excessive tearing, dryness, irritation, redness, and mucus discharge.
- Hepatosplenomegaly (enlarged liver and spleen)
Affected people may also have an increased risk of developing another lymphoma or other type of cancer.
Skin signs
Patients with Sezary syndrome present with diffusely red, thickened and scaly skin. Pruritus (itch) is common, often severe, and can be difficult to manage. Other features may include:
- Slowly-developing generalised induration (firmness of the skin)
- Lichenification (increased skin markings due to scratching and rubbing)
- Scaly papules due to follicular prominence
- Thickened nails
- Ectropion (drooping of lower eyelid)
- Diffuse or patchy alopecia (hair loss)
These symptoms often lead to lack of sleep, anxiety and depression.
Very rarely, Sezary syndrome has been reported to present with pruritus, Sezary cells on biopsy of normal-looking skin, and no visible rash.
Systemic involvement
Other features of Sezary syndrome include:
- Peripheral lymphadenopathy (enlarged lymph nodes): often generalized, involving neck, armpits, groins
- Enlarged spleen (splenomegaly)
- Less commonly, liver, lungs and gastrointestinal tract can be affected.
The following cancers are associated with Sezary syndrome:
Sezary syndrome diagnosis
A diagnosis of Sezary syndrome is often suspected in people with characteristic signs and symptoms. Additional testing can then be ordered to confirm the diagnosis. This may include 5:
- A skin biopsy
- A complete blood count
- Peripheral blood smear
- Immunophenotyping
- T-cell receptor (TCR) gene rearrangement test
- Flow cytometry
- A series of imaging tests such as CT (computerized axial tomography), MRI (magnetic resonance imaging) and/or PET (positron emission tomography) scans to determine if the cancer has spread to lymph nodes or other organs.
In addition to these diagnostic tests, occasionally a bone marrow biopsy may be necessary to verify complete staging. Because Sézary syndrome is such a rare cancer, it is important to confirm the diagnosis by a dermatopathologist or a hematopathologist, a pathologist who is an expert in diagnosing lymphomas.
Note that many of the same tests and exams used to diagnose and stage other subtypes of cutaneous T-cell lymphoma (CTCL) are used in Sézary syndrome 13. Blood flow cytometry is essential to diagnose and stage Sézary syndrome, and whole-body imaging often is needed to determine if the cancer has spread to the lymph nodes or other organs. These tests may include a CT scan, a PET scan, and/or magnetic resonance imaging (MRI, a procedure that takes detailed pictures of areas inside the body using a powerful magnet and radio waves). Swollen lymph nodes can be positive on a PET scan so a biopsy might be necessary to confirm if cancer cells are present in the lymph node. A bone marrow biopsy (a procedure to collect small samples of the spongy tissue inside the bone) may also be performed but is not always necessary.
Once the diagnosis is made, patients undergo exams to assess the disease stage (how much the cancer has grown, what is the extent and pattern of growth in the skin [patch, plaque or tumor], and if it has spread to other parts of the body). Patients with Sézary syndrome by definition have stage 4 (stage IV) lymphoma. The clinical stages of cutaneous T-cell lymphoma (CTCL) are
detailed in Table 1.
Because Sézary syndrome is a rare disease, patients should be referred to a health care team that specializes in this type of lymphoma. The patients’ clinical stage is important to select the best treatment. The treatment is individually chosen for each patient and may be adjusted frequently depending on how effective the treatment is and how well the patient tolerates it.
The clinical stage is also important to determine the prognosis and treatment options. Keep in mind that no two patients are alike and that statistics can only predict how a large group of patients will
do not what will happen to an individual patient. Your doctor most familiar with your situation is in the best position to interpret these statistics and understand how well they apply to your particular situation.
Skin biopsy
If possible, select an area of indurated skin for biopsy. The removal of cells or tissues so they can be viewed under a microscope to check for signs of cancer. The doctor may remove a growth from the skin, which will be examined by a pathologist. Multiple biopsies are useful especially if morphology varies.
Features on light microscopy may include:
- Atypical lymphocytes infiltrating dermis
- Epidermotropism (cells migrating to epidermis)
- Lymphocytes with a single cerebriform nucleus (not diagnostic)
- Pautrier microabscesses, or intra-epidermal aggregates of atypical cells
- Immunohistochemistry stains positive for CD3+ and CD4+ cells
Other tests that may be done on the cells or tissue sample include the following:
- Immunophenotyping: A laboratory test that uses antibodies to identify cancer cells based on the types of antigens or markers on the surface of the cells. This test is used to help diagnose specific types of lymphoma.
- Flow cytometry: A laboratory test that measures the number of cells in a sample, the percentage of live cells in a sample, and certain characteristics of the cells, such as size, shape, and the presence of tumor (or other) markers on the cell surface. The cells from a sample of a patient’s blood, bone marrow, or other tissue are stained with a fluorescent dye, placed in a fluid, and then passed one at a time through a beam of light. The test results are based on how the cells that were stained with the fluorescent dye react to the beam of light. This test is used to help diagnose and manage certain types of cancers, such as leukemia and lymphoma. Flow cytometry can demonstrate CD4+CD7- and CD4+CD26- T cells, which are characteristic of Sezary syndrome. T-cell antigens may also be absent (CD2, CD3, CD4 and/or CD5). The CD4:CD8 ratio is > 10, but is not diagnostic.
- T-cell receptor (TCR) gene rearrangement test: A laboratory test in which cells in a sample of blood or bone marrow are checked to see if there are certain changes in the genes that make receptors on T cells (white blood cells). Testing for these gene changes can tell whether large numbers of T cells with a certain T-cell receptor are being made.
Blood tests
Sezary cells are large atypical mononuclear cells with a large cerebriform nuclei. They are found in large numbers in the peripheral blood of patients with Sezary syndrome. Smaller numbers may be found in healthy patients or those with other diseases.
- Sezary blood cell count: A procedure in which a sample of blood is viewed under a microscope to count the number of Sezary cells.
- Human immunodeficiency virus (HIV) test: A test to measure the level of HIV antibodies in a sample of blood. Antibodies are made by the body when it is invaded by a foreign substance. A high level of HIV antibodies may mean the body has been infected with HIV.
- Human T-cell lymphotropic virus (HTLV-1).
Lymph node biopsy
Skin lymphomas often spread to lymph nodes, so your doctor may recommend a lymph node biopsy to help confirm the diagnosis or help determine how widespread the lymphoma is.
Excisional biopsy where a surgeon cuts through your skin to remove entire lymph node is required to distinguish between dermatopathic lymph node changes and reactive lymph node changes.
Removing a lymph node almost always provides enough tissue to diagnose the exact type of lymphoma. Most doctors prefer this type of biopsy if it can be done without too much discomfort.
Chromosome and gene tests
Chromosomes are long strands of DNA that contain your genes. Normal human cells have 23 pairs of chromosomes. Each chromosome is usually a certain size and looks a certain way. But in some types of lymphoma, the cells have changes in their chromosomes, such as having too many, too few, or abnormal chromosomes. These changes can often help identify the type of lymphoma.
- Cytogenetics (karyotyping): Cells are looked at with a microscope to see if the chromosomes have any abnormalities. The cells need to be grown in the lab first, so results can take a week or more.
- Fluorescent in situ hybridization (FISH): This test looks more closely at lymphoma cell DNA using special fluorescent dyes that only attach to specific genes or parts of chromosomes. FISH can find most chromosome changes that can be seen in standard cytogenetic tests, as well as some gene changes too small to be seen with cytogenetic testing. FISH is very accurate and can usually provide results within a couple of days.
- Other molecular and genetic tests: Other types of lab tests can also be done on the samples to look for specific gene changes or other changes in the lymphoma cells.
Many of these tests are done using next-generation sequencing (NGS), which can look for changes in many different genes at once. This type of testing usually takes a week or longer to get results.
Table 1. Clinical Stages of Cutaneous T-cell lymphoma (CTCL)
| Stage | A | B |
|---|---|---|
| I (disease that is limited to the skin) | Less than 10% of the skin is covered in red patches or plaques | 10% or more of the skin is covered in patches or plaques |
| II (disease that is limited to the skin) | Any amount of the skin surface is covered with patches or plaques and lymph nodes are enlarged and inflamed, but the cancer has not spread to the lymph nodes. | One or more tumors are found on the skin, lymph nodes may be enlarged, but cancer has not spread to the lymph nodes. |
| III (patients with erythroderma but without significant blood involvement) | Non-applicable | Non-applicable |
| IV (disease has spread to the lymph nodes and/or the bloodstream) | Most of the skin is reddened and cancer is found in the blood; cancer may have spread to the lymph nodes but does not involve other internal organs. | Most of the skin is reddened, and cancer is found in the blood; cancer may have spread to the lymph nodes and has spread to other organs such as bone marrow (the spongy tissue inside the bones). |
Lymphoma of the Skin Stages
After you are diagnosed with skin lymphoma, your cancer care team will try to figure out if it has spread, and if so, how far. This process is called staging. The stage of a cancer describes how much cancer is in the body. It helps determine how serious the cancer is and how best to treat it. Knowing the stage of your skin lymphoma may help in deciding the best treatment.
The staging systems for skin lymphomas were developed by the International Society for Cutaneous Lymphomas (ISCL) and the European Organization for Research and Treatment of Cancer (EORTC).
There are 2 different staging systems 14:
- One for mycosis fungoides and Sezary syndrome
- One for other skin lymphomas
These systems can be hard to understand. If you have questions about the stage of your lymphoma, ask your doctor to explain it to you in a way you understand. This can help you make choices about your treatment.
Staging for mycosis fungoides and Sezary syndrome
Mycosis fungoides and Sezary syndrome are staged based on 4 factors:
- T describes how much of the skin is affected by the lymphoma (tumor).
- N describes the extent of the lymphoma in the lymph nodes (bean-sized collections of immune cells).
- M is for metastasis or spread of the lymphoma to other organs.
- B is for lymphoma cells in the blood.
T categories
T describes how much of the skin is affected by the lymphoma (tumor).
- T1: Skin lesions can be small patches (flat lesions), papules (small bumps), and/or plaques (raised or lowered, flat lesions), but the lesions cover less than 10% of the skin surface.
- T2: The patches, papules, and/or plaques cover 10% or more of the skin surface.
- T3: At least one of the skin lesions is a tumor (a lesion growing deeper into the skin) that is at least 1 centimeter (cm) across (a little less than 1/2 an inch).
- T4: The skin lesions have grown together to cover at least 80% of the skin surface.
N categories
N describes the extent of the lymphoma in the lymph nodes (bean-sized collections of immune cells).
- N0: Lymph nodes are not enlarged and a lymph node biopsy is not needed.
- N1: Lymph nodes are enlarged, but when biopsied the patterns of cells look normal or close to normal under the microscope.
- N2: Lymph nodes are enlarged, and when biopsied the patterns of cells look more abnormal under the microscope.
- N3: Lymph nodes are enlarged, and when biopsied the patterns of cells look very abnormal under the microscope.
- NX: Lymph nodes are enlarged but haven’t been removed (biopsied) to be looked at under the microscope.
M categories
M is for metastasis or spread of the lymphoma to other organs.
- M0: The lymphoma cells have not spread to other organs.
- M1: Lymphoma cells have spread to other organs, such as the liver or spleen.
B categories
B is for lymphoma cells in the blood.
- B0: No more than 5% of lymphocytes in the blood are Sezary (lymphoma) cells.
- B1: Low numbers of Sezary cells in the blood (more than in B0 but less than in B2).
- B2: High number of Sezary cells in the blood.
Stage grouping (I-IV)
Once the values for T, N, M, and B are known, they are combined to determine the overall stage of the lymphoma. This process is called stage grouping.
Mycosis fungoides and Sezary syndrome stages range from I (1) through IV (4).
As a rule, the lower the number, the less the cancer has spread.
- A higher number, such as stage IV (stage 4), means cancer has spread more.
- Within each numbered stage (I-IV), an earlier letter means a lower stage.
Although each person’s cancer experience is unique, cancers with similar stages tend to have a similar outlook and are often treated in much the same way.
Stage IA (T1, N0, M0, B0 or B1)
- There are skin lesions but no tumors.
- Skin lesions cover less than 10% of the skin surface (T1).
- The lymph nodes are not enlarged (N0).
- Lymphoma cells have not spread to other organs (M0).
- The number of Sezary cells in the blood is not high (B0 or B1).
Stage IB (T2, N0, M0, B0 or B1)
- There are skin lesions but no tumors.
- Skin lesions cover at least 10% of the skin surface (T2).
- The lymph nodes are not enlarged (N0).
- Lymphoma cells have not spread to other organs (M0).
- The number of Sezary cells in the blood is not high (B0 or B1).
Stage IIA (T1 or T2, N1 or N2, M0, B0 or B1)
- There are skin lesions but no tumors.
- Skin lesions can cover up to 80% of the skin surface (T1 or T2).
- Lymph nodes are enlarged but the patterns of cells do not look very abnormal under the microscope (N1 or N2).
- Lymphoma cells have not spread to other organs (M0).
- The number of Sezary cells in the blood is not high (B0 or B1).
Stage IIB (T3, N0 to N2, M0, B0 or B1)
- At least one of the skin lesions is a tumor that is 1 cm across or larger (T3).
- The lymph nodes are either normal (N0) or are enlarged but the patterns of cells do not look very abnormal under the microscope (N1 or N2).
- Lymphoma cells have not spread to other organs (M0).
- The number of Sezary cells in the blood is not high (B0 or B1).
Stage IIIA (T4, N0 to N2, M0, B0)
- Skin lesions cover at least 80% of the skin surface (T4).
- The lymph nodes are either normal (N0) or are enlarged but the patterns of cells do not look very abnormal under the microscope (N1 or N2).
- Lymphoma cells have not spread to other organs or tissues (M0).
- No more than 5% of the lymphocytes in the blood are Sezary cells (B0).
Stage IIIB (T4, N0 to N2, M0, B1)
- Skin lesions cover at least 80% of the skin surface (T4).
- The lymph nodes are either normal (N0) or are enlarged but the patterns of cells do not look very abnormal under the microscope (N1 or N2).
- Lymphoma cells have not spread to other organs (M0).
- The number of Sezary cells in the blood is low (B1).
Stage IVA1 (Any T, N0 to N2, M0, B2)
- Skin lesions can cover any amount of the skin surface (any T).
- The lymph nodes are either normal (N0) or are enlarged but the patterns of cells do not look very abnormal under the microscope (N1 or N2).
- Lymphoma cells have not spread to other organs (M0).
- The number of Sezary cells in the blood is high (B2).
Stage IVA2 (Any T, N3, M0, any B)
- Skin lesions can cover any amount of the skin surface (any T).
- Some lymph nodes are enlarged, and the patterns of cells look very abnormal under the microscope (N3).
- Lymphoma cells have not spread to other organs (M0).
- Sezary cells may or may not be in the blood (any B).
Stage IVB (Any T, any N, M1, any B)
- Skin lesions can cover any amount of the skin surface (any T).
- The lymph nodes may be normal or abnormal (any N).
- Sezary cells may or may not be in the blood (any B).
- Lymphoma cells have spread to other organs, such as the liver or spleen (M1).
Sezary syndrome treatment
Since Sézary syndrome is systemic (cancer has spread to the bloodstream), it is not treated with skin-directed therapies alone. Treatment for Sezary syndrome is determined by the stage of disease and other medical conditions you have. Sezary syndrome treatment is generally systemic and can be given alone or in combination with skin-based therapy. Patients with stage IVA (stage 4A) (no visceral involvement) are usually treated with extracorporeal phototherapy combined with biological response modifiers (retinoids and interferons). Other alternatives include low-dose methotrexate and histone deacetylase inhibitors (vorinostat and romidepsin). Various combinations of the above can be used along with skin-directed therapy.
In general, there are six different treatment options available to people with Sezary syndrome. These include 15:
- Photodynamic therapy
- Radiation therapy
- Chemotherapy
- Other drug therapy (i.e. topical steriods, retinoids)
- Biologic therapy (immunotherapy)
- Targeted therapy
- Stem cell transplantation
There is no standard therapy for Sezary syndrome. Patients are prescribed topical and systemic medications. They may also receive UVB or PUVA phototherapy, and/or radiotherapy (localized superficial rays or total skin electron beam therapy).
Topical therapy for Sezary syndrome
Topical therapies generally are used for earlier-stage Sezary disease and are useful to treat patients who have patches and limited plaques. These therapies include:
- Topical corticosteroids most frequently used topical therapy.
- Potassium permanganate or dilute bleach baths to prevent infection.
- Topical chemotherapy for example, mechlorethamine (Valchlor).
- Topical retinoids like bexarotene (Targretin).
- Topical immunotherapy drugs that use the body’s immune system to fight cancer with imiquimod (Zyclara).
- Local or total skin radiation therapy.
- Phototherapy with ultraviolet (UV) light.
- Emollients.
Corticosteroids are the most commonly used topical treatment for cutaneous T-cell lymphoma (CTCL). Bexarotene gel (Targretin) and mechlorethamine gel (Valchlor) have been approved by the U.S. Food and Drug Administration (FDA) as a topical treatment for Stages 1A and 1B CTCL in patients who have received previous skin treatment.
Photodynamic therapy
- Psoralen and ultraviolet A radiation (PUVA). In psoralen and ultraviolet A (PUVA) therapy, the patient receives a drug called psoralen and then ultraviolet A radiation is directed to the skin. Therapeutic trials with PUVA have shown an 80% to 90% complete remission rate with early cutaneous stages achieving the best responses. PUVA may be used in conjunction with systemic treatment 16. Continued maintenance therapy with PUVA at more protracted intervals is generally required to prolong remission duration 16. PUVA combined with interferon alpha-2a is associated with a high response rate 16.
- Narrowband ultraviolet B radiation. Single-arm and retrospective comparisons confirm narrowband ultraviolet B with 80% to 90% complete remission rates, especially for patients with early cutaneous stages 17.
- Extracorporeal photochemotherapy alone 18 or in combination with total-skin electron-beam radiation 19. Extracorporeal photopheresis is an immune-sparing therapy, the patient is given photosensitizing agent (psoralen/8-methoxsalen) and then some blood cells are taken from the body, put under a special ultraviolet A light, and put back into the body. Extracorporeal photochemotherapy may be used alone or combined with total skin electron beam radiation therapy. It is the preferred first line therapy in early stages. Response rates are improved when combined with biological response modifiers. Side effects include headache, fatigue, itch and transient hypotension (low blood pressure) with possible syncope (collapse).
Systemic treatment
Systemic treatment may be used in more advanced-stage disease and in patients with earlier-stage disease who did not respond to or did not tolerate topical therapies.
Systemic treatments include:
- Chemotherapy drugs that stop the growth of or kill cancer cells, including:
- Methotrexate
- Pegylated liposomal doxorubicin
- Fludarabine
- 2-chlorodeoxyadenosine
- Pentostatin
- Chlorambucil
- Folate analogues, like pralatrexate (Folotyn).
- Immunotherapy (drugs that use the body’s immune system to fight cancer)
- Immunomodulatory agents (drugs that work on the immune system directly by regulating [activating or slowing down] the activity of specific proteins) such as interferon alfa or gamma with or without topical therapies.
- Antibody-drug conjugate (ADC) such as brentuximab vedotin (Adcetris) which is a monoclonal antibody attached to a chemotherapy drug. The monoclonal antibody in the antibody-drug conjugate recognizes and binds to a protein called CD30 on the cancer cell surface. Once the antibody-drug conjugate is inside the cell, the chemotherapy drug separates from the antibody-drug conjugate and kills the cancer cell by targeting cell multiplication.
- Monoclonal antibodies are proteins made in the laboratory that bind to cancer cells and help your immune system destroy them) such as mogamulizumab (Poteligeo).
- Oral retinoids like bexarotene (Targretin).
- Targeted therapy are drugs that target molecules that the cancer cells use to grow and spread with histone deacetylase (HDAC) inhibitors such as vorinostat (Zolinza) or romidepsin (Istodax).
- Extracorporeal photopheresis (ECP) is a procedure that removes your blood and the white blood cells are isolated and exposed to ultraviolet A (UVA) light, and then returns the treated blood to the body.
Patients with more advanced-stage Mycosis fungoides often require systemic therapies, and those with high-risk disease (advanced disease that has failed to adequately respond to multiple forms of systemic therapy) may receive an allogeneic stem cell transplant.
Combination chemotherapy regimens are for those with refractory disease (cancer that does not respond to treatment) or advanced disease or that has spread from the skin to other parts of the body. Some of the systemic therapies can be combined to improve the response. Patients also often use skin-directed treatments together with systemic therapies.
Radiation therapy
Radiation therapy is a cancer treatment that uses high-energy x-rays or other types of radiation to kill cancer cells or keep them from growing. External radiation therapy uses a machine outside the body to send radiation toward the area of the body with cancer. Sometimes, total skin electron beam (TSEB) radiation therapy is used to treat mycosis fungoides and Sézary syndrome. This is a type of external radiation treatment in which a radiation therapy machine aims electrons (tiny, invisible particles) at the skin covering the whole body. External radiation therapy may also be used as palliative therapy to relieve symptoms and improve quality of life.
Ultraviolet A (UVA) radiation therapy or ultraviolet B (UVB) radiation therapy may be given using a special lamp or laser that directs radiation at the skin.
- Total skin electron beam. Electron-beam radiation of appropriate energies will penetrate only to the dermis, and thus the skin alone can be treated without systemic effects. This therapy requires a radiation therapy facility with physics support and considerable technical expertise to deliver precise dosimetry. Total skin electron beam can result in short- and long-term cutaneous toxic effects and is not widely available. This therapy can provide excellent palliation, with complete response rates of as much as 80%, and may be combined with systemic treatment. Based on the long-term survival of these early-stage patients, electron-beam radiation therapy is sometimes used with curative intent 20. Long-term disease-free survival can be achieved in patients with unilesional mycosis fungoides treated with local radiation therapy 21.
- Local electron-beam radiation or orthovoltage radiation therapy may be used to palliate areas of bulky or symptomatic skin disease 22.
Biologic therapy
Biologic therapy also called immunotherapy is a treatment that uses the patient’s immune system to fight cancer. Substances made by the body or made in a laboratory are used to boost, direct, or restore the body’s natural defenses against cancer. This type of cancer treatment is also called biotherapy or biologic therapy.
- Interferon: This treatment interferes with the division of mycosis fungoides and Sézary cells and can slow tumor growth. Interferon alpha or interferon gamma alone or in combination with topical therapy 23. A retrospective review of 198 patients with mycosis fungoides and Sezary syndrome compared time to next treatment between interferon alpha and conventional chemotherapy. Interferon alpha provided a longer time to next treatment of 8.7 months than did chemotherapy, with a time to next treatment of 3.9 months 24.
Chemotherapy
Chemotherapy is a cancer treatment that uses drugs to stop the growth of cancer cells, either by killing the cells or by stopping them from dividing. When chemotherapy is taken by mouth or injected into a vein or muscle, the drugs enter the bloodstream and can reach cancer cells throughout the body (systemic chemotherapy). Sometimes the chemotherapy is topical (put on the skin in a cream, lotion, or ointment).
Chemotherapeutic agents generally demonstrate short durations of response. In a retrospective review of 198 patients with advanced-stage disease, the median time before patients required new therapy was 4 months 24. However, these comparisons may be confounded by the order in which the agents were introduced.
- Topical chemotherapy with mechlorethamine (nitrogen mustard). This form of treatment may be used palliatively or to supplement therapeutic approaches directed against nodal or visceral disease. Topical application of mechlorethamine has produced regression of cutaneous lesions, with particular efficacy in early stages of disease. The overall complete remission rate is related to skin stage; 50% to 80% of TNM classification T1 patients, 25% to 75% of T2 patients, as many as 50% of T3 patients, and 20% to 40% of T4 patients have complete responses. The overall complete remission rate in 243 patients was 64% and was related to stage; as many as 35% of stage IV patients had complete responses. Treatments are usually continued for 2 to 3 years. Continuous 5-year disease free survival may be possible in as many as 33% of T1 patients 25.
- Oral methotrexate (NCT00425555) 26.
- Pegylated liposomal doxorubicin 27.
- Fludarabine, 2-chlorodeoxyadenosine, and pentostatin are active agents for mycosis fungoides and Sezary syndrome 28.
- Single-agent chemotherapy or combination systemic chemotherapy (chlorambucil plus prednisone, mechlorethamine, cyclophosphamide, methotrexate, and combination chemotherapy) are often combined with treatment directed at the skin 24.
- Pralatrexate (folate analog) 29.
Targeted therapy
Targeted therapy is a type of treatment that uses drugs or other substances to attack cancer cells. Targeted therapies usually cause less harm to normal cells than chemotherapy or radiation therapy do.
Monoclonal antibody therapy: This treatment uses antibodies made in the laboratory from a single type of immune system cell. These antibodies can identify substances on cancer cells or normal substances that may help cancer cells grow. The antibodies attach to the substances and kill the cancer cells, block their growth, or keep them from spreading. They may be used alone or to carry drugs, toxins, or radioactive material directly to cancer cells. Monoclonal antibodies are given by infusion.
- Types of monoclonal antibodies include:
- Brentuximab vedotin 30, which contains a monoclonal antibody that binds to a protein, called CD30, found on some types of lymphoma cells. It also contains an anticancer drug that may help kill cancer cells. Two phase II trials of 58 patients with variable CD30 expression showed a 50% to 70% response rate with 50% of patients still in remission after 1 year 31.
- Mogamulizumab 32, which contains a monoclonal antibody that binds to a protein, called CCR4, found on some types of lymphoma cells. It may block this protein and help the immune system kill cancer cells. It is used to treat mycosis fungoides and Sezary syndrome that came back or did not get better after treatment with at least one systemic therapy. In a prospective randomized trial, 372 previously treated patients received either mogamulizumab, a monoclonal antibody directed against C-C chemokine receptor 4, or vorinostat, the HDACi. With a median follow-up of 17 months, the median progression-free survival favored mogamulizumab at 7.7 months versus 3.1 months for vorinostat 32. In a preliminary study such as this, no overall survival (OS) was seen.
Stem cell transplantation
A stem cell transplant is a medical procedure that replaces damaged or diseased blood-forming stem cells with healthy ones. The patient is treated with high-dose chemotherapy or radiation to remove their blood-forming cells or stem cells, and then the new, healthy stem cells are introduced through an intravenous (IV) infusion to restore the immune system and the bone marrow’s ability to make new blood cells. The transplant can use your own stem cells (autologous) or stem cells from a donor (allogeneic). In allogeneic stem cell transplantation you’ll receive stem cells from a family member or unrelated donor 33. Among these highly selected patients, the 5-year overall survival rate ranges from 30% to 50%, with a relapse-free survival rate of 15% to 25% 34.
These types of treatments produce remissions, but long-term remissions are uncommon. Treatment, therefore, is considered palliative for most patients, although major symptomatic improvement is regularly achieved. Survival in excess of 8 years, however, is common for patients with early stages of disease. All patients with mycosis fungoides and Sezary syndrome are candidates for clinical trials evaluating new approaches to treatment.
Other drug therapy
- Topical corticosteroids are used to relieve red, swollen, and inflamed skin. They are a type of steroid. Topical corticosteroids may be in a cream, lotion, or ointment.
- Retinoids, such as bexarotene 35, are drugs related to vitamin A that can slow the growth of certain types of cancer cells. The retinoids may be taken by mouth or put on the skin.
- Lenalidomide is a drug that helps the immune system kill abnormal blood cells or cancer cells and may prevent the growth of new blood vessels that tumors need to grow 36.
- Vorinostat and romidepsin are two of the histone deacetylase (HDAC) inhibitors used to treat mycosis fungoides and Sezary syndrome 37. HDAC inhibitors cause a chemical change that stops tumor cells from dividing. A retrospective review of 198 patients with mycosis fungoides and Sézary syndrome compared time to next treatment between HDACi and conventional chemotherapy. HDACi provided a longer time to next treatment of 4.5 months than did chemotherapy, with a time to next treatment of 3.9 months 24.
Sezary syndrome prognosis
The long-term outlook (prognosis) for people with Sezary syndrome is generally poor with median survival of 4 years, with or without the typical generalized erythroderma 38, 39. Sezary syndrome is difficult to cure. Treatment is usually palliative, with the intention of relief of symptoms and improvement in the quality of life. Median survival for patients with Sezary syndrome has been reported to be 2 to 4 years after development of the condition, although survival has improved with newer treatments 40, 41.. The disease-specific 5-year survival rate has been reported to be 24% 10. Patients usually succumb to opportunistic infections due to immune suppression. A common cause of death during the tumor phase is septicemia (an infection that occurs when bacteria enter the bloodstream and spread) caused by chronic skin infection with staph species, herpes simplex, herpes zoster, and fungal skin infections 42, 43. Cytologic transformation from a low-grade lymphoma to a high-grade lymphoma (large cell transformation) occurs rarely (<5%) during the course of these diseases and is associated with a poor prognosis 44, 45, 46. A retrospective analysis of 100 cases with large cell transformation found reduced disease-specific survival with extracutaneous transformation, increased extent of skin lesions, and CD30 negativity 47.
The prognosis and treatment options depend on the following:
- The stage of the cancer.
- The type of lesion (patches, plaques, or tumors).
- The patient’s age and gender.
- Vakiti A, Padala SA, Singh D. Sezary Syndrome. [Updated 2022 Sep 24]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK499874[↩]
- Wilcox RA. Cutaneous T-cell lymphoma: 2017 update on diagnosis, risk-stratification, and management. Am J Hematol. 2017 Oct;92(10):1085-1102. doi: 10.1002/ajh.24876[↩]
- Kamijo H., Miyagaki T. Mycosis fungoides and Sézary syndrome: updates and review of current therapy. Curr Treat Options Oncol. 2021;22(2) doi: 10.1007/s11864-020-00809-w[↩]
- Sézary syndrome. https://dermnetnz.org/topics/sezary-syndrome[↩][↩][↩][↩][↩]
- Mycosis Fungoides (Including Sézary Syndrome) Treatment (PDQ®)–Patient Version. https://www.cancer.gov/types/lymphoma/patient/mycosis-fungoides-treatment-pdq[↩][↩]
- Sézary syndrome. https://medlineplus.gov/genetics/condition/sezary-syndrome[↩][↩][↩][↩]
- Sezary Cell. https://www.sciencedirect.com/topics/medicine-and-dentistry/sezary-cell[↩][↩][↩]
- SÉZARY SYNDROME. https://www.clfoundation.org/sezary-syndrome[↩][↩][↩]
- Fragkos KC. Plantar keratoderma of Sézary syndrome. Clin Case Rep. 2017 Aug 29;5(10):1726-1727. doi: 10.1002/ccr3.1168[↩]
- Mycosis Fungoides (Including Sézary Syndrome) Treatment (PDQ®)–Health Professional Version. https://www.cancer.gov/types/lymphoma/hp/mycosis-fungoides-treatment-pdq[↩][↩]
- Elise A Olsen, MD; Alain H Rook, MD. UpToDate. Clinical presentation, pathologic features, and diagnosis of Sézary syndrome. May 2013[↩]
- Cutaneous T-Cell Lymphoma. https://emedicine.medscape.com/article/2139720-overview[↩][↩]
- https://lymphoma.org/wp-content/uploads/2024/10/Cutaneous_Lymphoma_Fact_Sheet_2024.pdf[↩][↩]
- Lymphoma of the Skin Stages. https://www.cancer.org/cancer/types/skin-lymphoma/detection-diagnosis-staging/staging.html[↩]
- Mycosis Fungoides (Including Sézary Syndrome) Treatment (PDQ®)–Health Professional Version. https://www.cancer.gov/types/lymphoma/hp/mycosis-fungoides-treatment-pdq#_50[↩]
- Olsen EA, Hodak E, Anderson T, et al.: Guidelines for phototherapy of mycosis fungoides and Sézary syndrome: A consensus statement of the United States Cutaneous Lymphoma Consortium. J Am Acad Dermatol 74 (1): 27-58, 2016.[↩][↩][↩]
- Almohideb M, Walsh S, Walsh S, et al.: Bath Psoralen-ultraviolet A and Narrowband Ultraviolet B Phototherapy as Initial Therapy for Early-stage Mycosis Fungoides: A Retrospective Cohort of 267 Cases at the University of Toronto. Clin Lymphoma Myeloma Leuk 17 (9): 604-612, 2017.[↩]
- Scarisbrick JJ, Taylor P, Holtick U, et al.: U.K. consensus statement on the use of extracorporeal photopheresis for treatment of cutaneous T-cell lymphoma and chronic graft-versus-host disease. Br J Dermatol 158 (4): 659-78, 2008.[↩]
- Palareti G, Maccaferri M, Manotti C, et al.: Fibrinogen assays: a collaborative study of six different methods. C.I.S.M.E.L. Comitato Italiano per la Standardizzazione dei Metodi in Ematologia e Laboratorio. Clin Chem 37 (5): 714-9, 1991.[↩]
- Navi D, Riaz N, Levin YS, et al.: The Stanford University experience with conventional-dose, total skin electron-beam therapy in the treatment of generalized patch or plaque (T2) and tumor (T3) mycosis fungoides. Arch Dermatol 147 (5): 561-7, 2011.[↩]
- Micaily B, Miyamoto C, Kantor G, et al.: Radiotherapy for unilesional mycosis fungoides. Int J Radiat Oncol Biol Phys 42 (2): 361-4, 1998.[↩]
- Thomas TO, Agrawal P, Guitart J, et al.: Outcome of patients treated with a single-fraction dose of palliative radiation for cutaneous T-cell lymphoma. Int J Radiat Oncol Biol Phys 85 (3): 747-53, 2013.[↩]
- Olsen EA, Bunn PA: Interferon in the treatment of cutaneous T-cell lymphoma. Hematol Oncol Clin North Am 9 (5): 1089-107, 1995.[↩]
- Hughes CF, Khot A, McCormack C, et al.: Lack of durable disease control with chemotherapy for mycosis fungoides and Sézary syndrome: a comparative study of systemic therapy. Blood 125 (1): 71-81, 2015.[↩][↩][↩][↩]
- Lessin SR, Duvic M, Guitart J, et al.: Topical chemotherapy in cutaneous T-cell lymphoma: positive results of a randomized, controlled, multicenter trial testing the efficacy and safety of a novel mechlorethamine, 0.02%, gel in mycosis fungoides. JAMA Dermatol 149 (1): 25-32, 2013.[↩]
- Zackheim HS, Kashani-Sabet M, McMillan A: Low-dose methotrexate to treat mycosis fungoides: a retrospective study in 69 patients. J Am Acad Dermatol 49 (5): 873-8, 2003.[↩]
- Dummer R, Quaglino P, Becker JC, et al.: Prospective international multicenter phase II trial of intravenous pegylated liposomal doxorubicin monochemotherapy in patients with stage IIB, IVA, or IVB advanced mycosis fungoides: final results from EORTC 21012. J Clin Oncol 30 (33): 4091-7, 2012.[↩]
- Kurzrock R, Pilat S, Duvic M: Pentostatin therapy of T-cell lymphomas with cutaneous manifestations. J Clin Oncol 17 (10): 3117-21, 1999.[↩]
- Talpur R, Thompson A, Gangar P, et al.: Pralatrexate alone or in combination with bexarotene: long-term tolerability in relapsed/refractory mycosis fungoides. Clin Lymphoma Myeloma Leuk 14 (4): 297-304, 2014.[↩]
- Kim YH, Tavallaee M, Sundram U, et al.: Phase II Investigator-Initiated Study of Brentuximab Vedotin in Mycosis Fungoides and Sézary Syndrome With Variable CD30 Expression Level: A Multi-Institution Collaborative Project. J Clin Oncol 33 (32): 3750-8, 2015.[↩]
- Duvic M, Tetzlaff MT, Gangar P, et al.: Results of a Phase II Trial of Brentuximab Vedotin for CD30+ Cutaneous T-Cell Lymphoma and Lymphomatoid Papulosis. J Clin Oncol 33 (32): 3759-65, 2015.[↩]
- Kim YH, Bagot M, Pinter-Brown L, et al.: Mogamulizumab versus vorinostat in previously treated cutaneous T-cell lymphoma (MAVORIC): an international, open-label, randomised, controlled phase 3 trial. Lancet Oncol 19 (9): 1192-1204, 2018.[↩][↩]
- Duarte RF, Boumendil A, Onida F, et al.: Long-term outcome of allogeneic hematopoietic cell transplantation for patients with mycosis fungoides and Sézary syndrome: a European society for blood and marrow transplantation lymphoma working party extended analysis. J Clin Oncol 32 (29): 3347-8, 2014.[↩]
- Lechowicz MJ, Lazarus HM, Carreras J, et al.: Allogeneic hematopoietic cell transplantation for mycosis fungoides and Sezary syndrome. Bone Marrow Transplant 49 (11): 1360-5, 2014.[↩]
- Heald P, Mehlmauer M, Martin AG, et al.: Topical bexarotene therapy for patients with refractory or persistent early-stage cutaneous T-cell lymphoma: results of the phase III clinical trial. J Am Acad Dermatol 49 (5): 801-15, 2003.[↩]
- Querfeld C, Rosen ST, Guitart J, et al.: Results of an open-label multicenter phase 2 trial of lenalidomide monotherapy in refractory mycosis fungoides and Sézary syndrome. Blood 123 (8): 1159-66, 2014.[↩]
- Duvic M, Dummer R, Becker JC, et al.: Panobinostat activity in both bexarotene-exposed and -naïve patients with refractory cutaneous T-cell lymphoma: results of a phase II trial. Eur J Cancer 49 (2): 386-94, 2013.[↩]
- Kubica AW, Davis MD, Weaver AL, Killian JM, Pittelkow MR. Sézary syndrome: a study of 176 patients at Mayo Clinic. J Am Acad Dermatol. 2012 Dec;67(6):1189-99. doi: 10.1016/j.jaad.2012.04.043[↩]
- Thompson AK, Killian JM, Weaver AL, Pittelkow MR, Davis MD. Sézary syndrome without erythroderma: A review of 16 cases at Mayo Clinic. J Am Acad Dermatol. 2017 Apr;76(4):683-688. doi: 10.1016/j.jaad.2016.10.029[↩]
- Whittaker S, Hoppe R, Prince HM. How I treat mycosis fungoides and Sézary syndrome. Blood. 2016 Jun 23;127(25):3142-53. doi: 10.1182/blood-2015-12-611830[↩]
- Martin SJ, Duvic M. Prevalence and treatment of palmoplantar keratoderma and tinea pedis in patients with Sézary syndrome. Int J Dermatol. 2012 Oct;51(10):1195-8. doi: 10.1111/j.1365-4632.2011.05204.x[↩]
- Talpur R, Bassett R, Duvic M. Prevalence and treatment of Staphylococcus aureus colonization in patients with mycosis fungoides and Sézary syndrome. Br J Dermatol. 2008 Jul;159(1):105-12. doi: 10.1111/j.1365-2133.2008.08612.x[↩]
- Lebas E, Arrese JE, Nikkels AF. Risk Factors for Skin Infections in Mycosis Fungoides. Dermatology. 2016;232(6):731-737. doi: 10.1159/000455944[↩]
- Kim YH, Bishop K, Varghese A, Hoppe RT. Prognostic Factors in Erythrodermic Mycosis Fungoides and the Sézary Syndrome. Arch Dermatol. 1995;131(9):1003–1008. doi:10.1001/archderm.1995.01690210033005[↩]
- Arulogun SO, Prince HM, Ng J, Lade S, Ryan GF, Blewitt O, McCormack C. Long-term outcomes of patients with advanced-stage cutaneous T-cell lymphoma and large cell transformation. Blood. 2008 Oct 15;112(8):3082-7. doi: 10.1182/blood-2008-05-154609[↩]
- Kadin ME, Hughey LC, Wood GS. Large-cell transformation of mycosis fungoides-differential diagnosis with implications for clinical management: a consensus statement of the US Cutaneous Lymphoma Consortium. J Am Acad Dermatol. 2014 Feb;70(2):374-6. doi: 10.1016/j.jaad.2013.09.007[↩]
- Benner MF, Jansen PM, Vermeer MH, Willemze R. Prognostic factors in transformed mycosis fungoides: a retrospective analysis of 100 cases. Blood. 2012 Feb 16;119(7):1643-9. doi: 10.1182/blood-2011-08-376319[↩]


{kind=link}