Contents
- Niacin
- What does Niacin (vitamin B3) do?
- How much Niacin (vitamin B3) do I need?
- What foods provide Niacin (vitamin B3)?
- What kinds of Niacin supplements are available?
- What happens if I don’t get enough Niacin?
- Niacin (vitamin B3) health benefits
- Niacin (vitamin B3) uses
- Niacin (vitamin B3) side effects
- Niacin deficiency
Niacin
Niacin also known as vitamin B3, nicotinamide (pyridine-3-carboxamide), nicotinamide adenine dinucleotide (NAD), nicotinic acid (pyridine-3-carboxylic acid) or nicotinamide riboside is one of the water-soluble B vitamins that occurs in many animal and plant tissues 1, 2, 3, 4. Niacin is the generic name for nicotinic acid (pyridine-3-carboxylic acid), nicotinamide (niacinamide or pyridine-3-carboxamide), and related derivatives, such as nicotinamide riboside 5, 6, 7. Niacin is naturally present in many foods, added to some food products, and available as a dietary supplement. Food such as bran, yeast, eggs, peanuts, poultry, red meat, fish, whole-grain cereals, legumes, and seeds are rich sources of niacin or vitamin B3 8. The essential amino acid tryptophan can also be converted into nicotinamide adenine dinucleotide (NAD) via the kynurenine pathway, so tryptophan (an amino acid in protein) is considered a dietary source of niacin 3, 4. Note that none of the Niacin vitamers are related to the nicotine found in tobacco, although their names are similar. Likewise, nicotine — but not nicotinic acid — is an agonist of the nicotinic receptors that respond to the neurotransmitter, acetylcholine 3.
Essential to all forms of life, the coenzyme nicotinamide adenine dinucleotide (NAD) is synthesized in all tissues in your body from four precursors that are provided in the diet: nicotinic acid, nicotinamide, nicotinamide riboside, and tryptophan (Figure 1) 4. More than 400 enzymes require nicotinamide adenine dinucleotide (NAD) to catalyze reactions in your body, which is more than for any other vitamin-derived coenzyme 5. Nicotinamide adenine dinucleotide (NAD) is also converted into another active form, the coenzyme nicotinamide adenine dinucleotide phosphate (NADP), in all tissues except skeletal muscle 9.
Most dietary niacin is in the form of nicotinic acid and nicotinamide, but some foods contain small amounts of NAD and NADP.
Humans are able to synthesize nicotinic acid from tryptophan – the liver can synthesize niacin from the essential amino acid tryptophan, but the synthesis is extremely slow and requires vitamin B6 (Pyridoxine); 60 mg of tryptophan are required to make one milligram of niacin 10. Bacteria in the gut may also perform the conversion but are inefficient. Another source for nicotinic acid is the gut flora. In humans there is no deamidation of nicotinamide to nicotinic acid in the gut. Nicotinamide is rapidly absorbed in stomach and small intestine. In plasma both the acid and the amide form are found. Red blood cells take up the nicotinic acid by a sodium dependent saturable transport system. Both the nicotinic acid and nicotinamide are able to pass the blood-brain barrier, however separate systems for uptake have been identified. Brain cells have a high affinity for nicotinamide, but not for nicotinic acid. Nicotinamide is the main substance that is transported between the different tissues as a precursor of NAD synthesis. The liver, kidneys, brain and red blood cells prefer nicotinic acid as a precursor for NAD synthesis, but testes and ovaries prefer nicotinamide. NAD nucleosidase cleaves NAD with nicotinamide as one of the products. This can be deamidated to form nicotinic acid (and re-converted to NAD) or methylated and released via urine. Excretion of the amide (and its metabolites) tends to be more extensive compared to the acid 11.
Figure 2 illustrates the separate biosynthetic pathways that lead to nicotinamide adenine dinucleotide (NAD) production from the various dietary precursors. Nicotinamide adenine dinucleotide (NAD) is synthesized from nicotinamide and nicotinamide riboside via two enzymatic reactions, while the pathway that yields nicotinamide adenine dinucleotide (NAD) from nicotinic acid – known as the Preiss-Handler pathway — includes three steps 3. The kynurenine pathway is the longest nicotinamide adenine dinucleotide (NAD) biosynthetic pathway: the catabolism of tryptophan through kynurenine produces quinolinic acid, which is then converted to nicotinic acid mononucleotide, an intermediate in nicotinamide adenine dinucleotide (NAD) metabolism. Nicotinamide adenine dinucleotide (NAD) is then synthesized from nicotinic acid mononucleotide in the Preiss-Handler pathway 12.
All pathways generate intermediary mononucleotides — either nicotinic acid mononucleotide or nicotinamide mononucleotide 3. Specific enzymes, known as phosphoribosyltransferases, catalyze the addition of a phosphoribose moiety onto nicotinic acid or quinolinic acid to produce nicotinic acid mononucleotide or onto nicotinamide to generate nicotinamide mononucleotide 3. Nicotinamide mononucleotide is also generated by the phosphorylation of nicotinamide riboside, catalyzed by nicotinamide riboside kinases (NRKs) 3. Furthermore, adenylyltransferases catalyze the adenylation of these mononucleotides to form either nicotinic acid adenine dinucleotide or nicotinamide adenine dinucleotide (NAD). Nicotinic acid adenine dinucleotide is then converted to nicotinamide adenine dinucleotide (NAD) by glutamine-dependent NAD synthetase (NADSYN), which uses glutamine as an amide group donor (Figure 2) 12. Of note, nicotinic acid adenine dinucleotide has been reported to form following the administration of high-dose nicotinamide riboside, suggesting that a potential deamidation could occur to convert nicotinamide adenine dinucleotide (NAD) to nicotinic acid adenine dinucleotide when the pool of nicotinamide adenine dinucleotide (NAD) is high 2.
When NAD and NADP are consumed in foods, they are converted to nicotinamide in the gut and then absorbed 9. Ingested niacin is absorbed primarily in the small intestine, but some is absorbed in the stomach 5, 6, 7.
Niacin or vitamin B3 helps turn the food you eat into the energy you need. Niacin is important for the development and function of the cells in your body 13.
As a drug, Niacin or vitamin B3, has two main indications 8:
- To treat hyperlipidemia (types 2A and 2B or primary hypercholesterolemia) (FDA approved use). Niaspan and generic niacin extended release (ER), available as a prescription medicine, provides 500-1,000 mg extended-release nicotinic acid. It is used to treat high blood cholesterol levels 4. The principal antilipemic effect of niacin appears to result mainly from decreased production of very low density lipoprotein cholesterol (VLDL-cholesterol) and is effective in lowering low density lipoprotein (LDL) cholesterol and raising high density lipoprotein (HDL) cholesterol, which makes this agent of unique value in the therapy of dyslipidemia 14, 15. Decreased production of VLDL-cholesterol by niacin may be related to the partial inhibition of free fatty acid release from adipose tissue, a decreased delivery of free fatty acids to the liver, and a decrease in triglyceride synthesis and VLDL-triglyceride transport. Enhanced clearance of VLDL-cholesterol and chylomicron triglycerides also may occur, possibly as a result of enhanced activity of lipoprotein lipase. Reductions in LDL-cholesterol concentrations may be related to decreased production and enhanced hepatic clearance of LDL-cholesterol precursors (i.e., VLDL-cholesterol). The mechanism by which niacin increases HDL-cholesterol concentrations has not been fully elucidated but may be related to a decreased hepatic clearance of apo A-I-containing particles and decreased synthesis of apo A-II. Niacin has no effect on cholesterol synthesis or fecal excretion of fats, sterols, or bile acids.
- To treat Niacin or vitamin B3 Deficiency, also known as pellagra (Italian for “rough skin”) 16, 17, 18. In the 1700s, pellagra first appeared in Italy, and the name translates into “pella” meaning skin, and “agra” meaning rough 19. Niacin or vitamin B3 deficiency causes pellagra, a disease characterized by the triad of dermatitis, diarrhea, and dementia that is endemic today in parts of India and China, and may result in death in severe cases 20, 21. Other symptoms include irritability, loss of appetite, weakness, and dizziness. Niacin deficiency is rare in the United States but may still be seen in alcoholics, dietary cultists, and patients with malabsorption syndrome 22. Some clinicians prefer niacinamide for the treatment of pellagra because it lacks vasodilating effects 23.
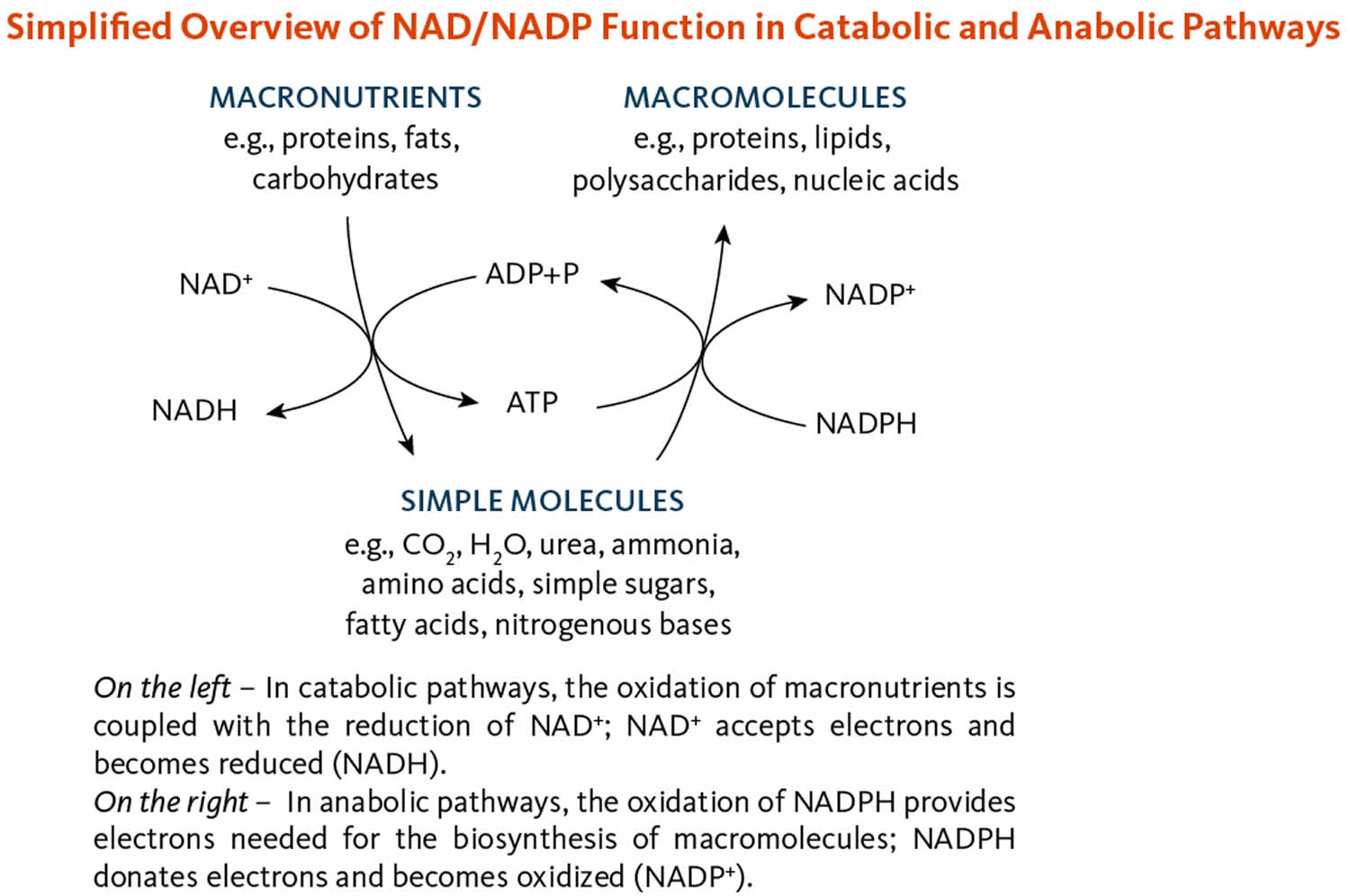
The coenzymes nicotinamide adenine dinucleotide (NAD) and nicotinamide adenine dinucleotide phosphate (NADP) are required in most metabolic oxidation-reduction (redox) processes in cells where NAD and NADP are oxidized or reduced (Figure 3) 4. NAD is primarily involved in catabolic reactions that transfer the potential energy in carbohydrates, fats, and proteins to adenosine triphosphate (ATP), the cell’s primary energy currency 9. Nicotinamide adenine dinucleotide (NAD) is also required for enzymes involved in critical cellular functions, such as the maintenance of genome integrity, control of gene expression, and cellular communication 9, 7. Nicotinamide adenine dinucleotide phosphate (NADP), in contrast, enables anabolic reactions, such as the synthesis of cholesterol and fatty acids, and plays a critical role in maintaining cellular antioxidant function 4.
Even when taken in very high doses of 3–4 g, niacin is almost completely absorbed 4. Once absorbed, physiologic amounts of niacin are metabolized to nicotinamide adenine dinucleotide (NAD). Some excess niacin is taken up by red blood cells to form a circulating reserve pool. The liver methylates any remaining excess to N1-methyl-nicotinamide, N1-methyl-2-pyridone-5-carboxamide, and other pyridone oxidation products, which are then excreted in the urine 4. Unmetabolized nicotinic acid and nicotinamide might be present in the urine as well when niacin intakes are very high 4.
Levels of niacin in the blood are not reliable indicators of niacin status 4. The most sensitive and reliable measure of niacin status is the urinary excretion of its two major methylated metabolites, N1-methyl-nicotinamide and N1-methyl-2-pyridone-5-carboxamide 6. Excretion rates in adults of more than 17.5 micromol/day of these two metabolites reflect adequate niacin status, while excretion rates between 5.8 and 17.5 micromol/day reflect low niacin status 4. An adult has niacin deficiency when urinary-excretion rates are less than 5.8 micromol/day 4. Indicators of niacin deficiency such as this and other biochemical signs (e.g., a 2-pyridone oxidation product of N1-methyl-nicotinamide below detection limits in plasma or low red blood cell NAD concentrations) occur well before overt clinical signs of niacin deficiency 6. Another measure of niacin status takes into account the fact that NAD levels decline as niacin status deteriorates, whereas NADP levels remain relatively constant 5, 7, 24. A “niacin number” (the ratio of NAD to NADP concentrations in whole blood x 100) below 130 suggests niacin deficiency 25, 26. A “niacin index” (the ratio of red blood cell NAD to NADP concentrations) below 1 suggests that an individual is at risk of developing niacin deficiency 27. No functional biochemical tests that reflect total body stores of niacin are available 24.
The recommended dietary allowance (RDA) of Niacin or vitamin B3 is 14 to 16 mg daily in adults, and slightly more for pregnant women (18 mg) and less for children (2 to 12 mg). No adverse effects have been reported from the consumption of naturally occurring niacin in foods 6, 15. However, high intakes of both nicotinic acid and nicotinamide taken as a dietary supplement or medication can cause adverse effects, although their toxicity profiles are not the same.
30 mg to 50 mg nicotinic acid or more typically causes flushing; the skin on the patient’s face, arms, and chest turns a reddish color because of vasodilation of small subcutaneous blood vessels 4. The flushing is accompanied by burning, tingling, and itching sensations 28, 29. These signs and symptoms are typically transient and can occur within 30 minutes of nicotinic acid intake or over days or weeks with repeated dosing; they are considered an unpleasant, rather than a toxic, side effect 4. However, the flushing can be accompanied by more serious signs and symptoms, such as headache, rash, dizziness, and/or a decrease in blood pressure. Supplement users can reduce the flushing effects by taking nicotinic acid supplements with food, slowly increasing the dose over time, or simply waiting for the body to develop a natural tolerance 4.
When taken in pharmacologic doses of 1,000 to 3,000 mg/day used in the therapy of hyperlipidemia, nicotinic acid can also cause more serious side effects 28, 29, 9, 6. Many of these effects have occurred in patients taking high-dose nicotinic acid supplements to treat hyperlipidemias. These adverse effects can include hypotension severe enough to increase the risk of falls; fatigue; impaired glucose tolerance and insulin resistance; gastrointestinal effects, such as nausea, heartburn, and abdominal pain; and ocular effects, such as blurred or impaired vision and macular edema (a buildup of fluid at the center of the retina). High doses of nicotinic acid taken over months or years can also cause liver injury; effects can include increased levels of liver enzymes; hepatic dysfunction resulting in fatigue, nausea, and anorexia; hepatitis; and acute liver failure 15, 6, 30, 28, 31. Liver injury is more likely to occur with the use of extended-release forms of nicotinic acid 32, 33, 28.
To minimize the risk of adverse effects from nicotinic acid supplementation or to identify them before they become serious, the American College of Cardiology and the American Heart Association recommend measuring liver transaminase (liver enzyme), fasting blood glucose or hemoglobin A1C, and uric acid levels in all supplement users before they start therapy, while the dose is being increased to a maintenance level, and every 6 months thereafter 30. The American College of Cardiology and the American Heart Association also recommend that patients not use nicotinic acid supplements or stop using them if their liver transaminase (liver enzyme) levels are more than two or three times the upper limits of normal; if they develop persistent high blood sugar level (hyperglycemia), acute gout, unexplained abdominal pain, gastrointestinal symptoms, new-onset atrial fibrillation, or weight loss; or if they have persistent and severe skin reactions, such as flushing or rashes 30.
Nicotinamide does not cause skin flushing and has fewer adverse effects than nicotinic acid, and these effects typically begin with much higher doses 28. Nausea, vomiting, and signs of liver toxicity can occur with nicotinamide intakes of 3,000 mg/day 6. In several small studies of participants undergoing hemodialysis, the most common adverse effects from 500-1,500 mg/day nicotinamide supplementation for several months were diarrhea and thrombocytopenia (low platelet count) 29, 34, 35, 36.
The Food and Nutrition Board at the National Academies of Sciences, Engineering, and Medicine has established Tolerable Upper Intake Level (maximum daily intake unlikely to cause adverse health effects) for niacin that apply only to supplemental niacin for healthy infants, children, and adults 6. These Tolerable Upper Intake Levels (ULs) are based on the levels associated with skin flushing. The Food and Nutrition Board acknowledges that although excess nicotinamide does not cause flushing, a Tolerable Upper Intake Level for nicotinic acid based on flushing can prevent the potential adverse effects of nicotinamide 6. The Tolerable Upper Intake Level, therefore, applies to both forms of supplemental niacin. However, the Tolerable Upper Intake Level does not apply to individuals who are receiving supplemental niacin under medical supervision 6.
Niacin and its metabolites are rapidly excreted in urine. Following oral administration of single and multiple doses of an immediate-release (Niacor) or extended-release (Niaspan) niacin preparation, approximately 88 or 60-76% of the dose, respectively, was excreted in urine as unchanged drug and inactive metabolites 37.
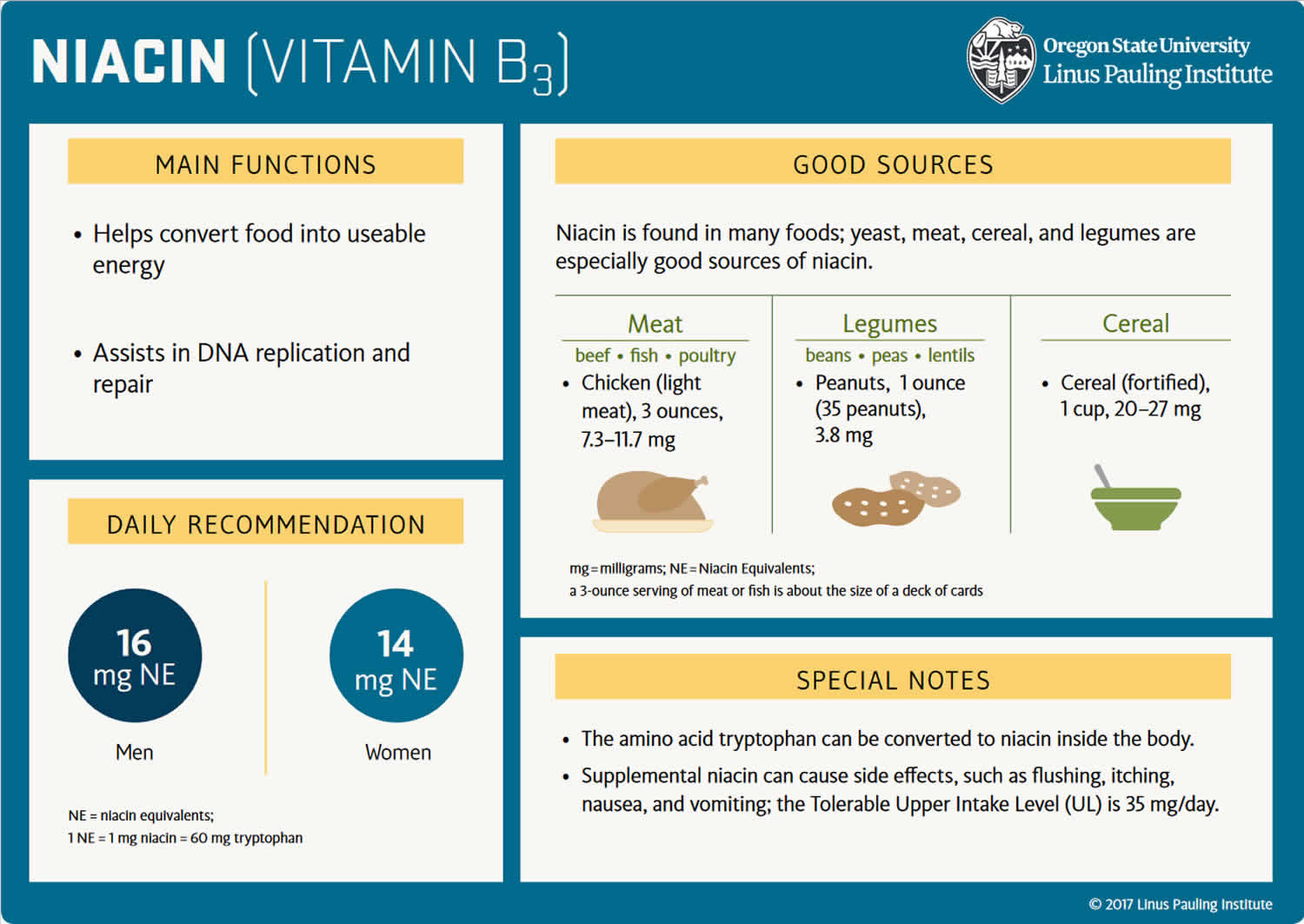
Figure 1. Dietary precursors of nicotinamide adenine dinucleotide (NAD)
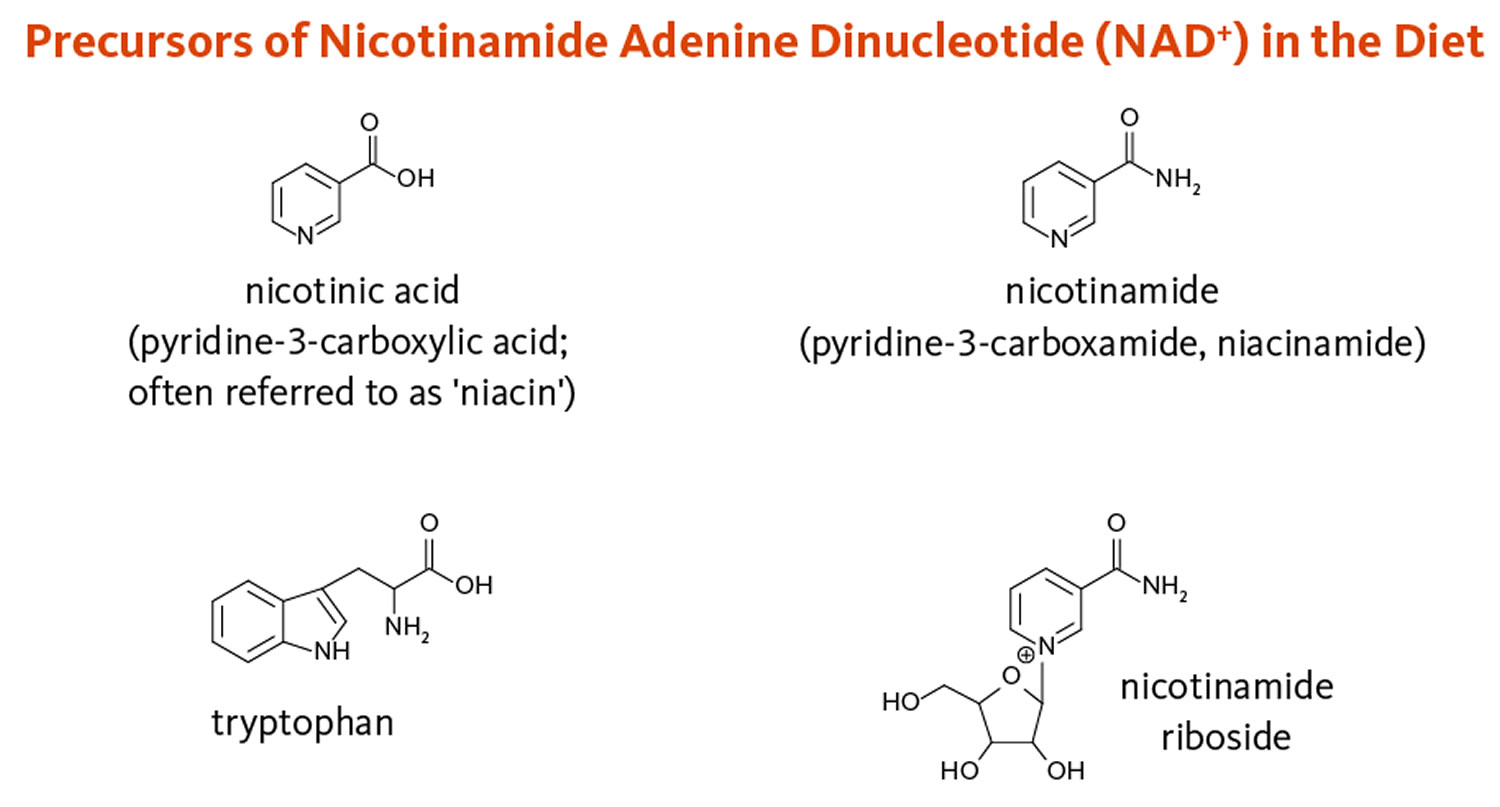
Footnote: Dietary precursors of nicotinamide adenine dinucleotide (NAD), including nicotinic acid, nicotinamide, and nicotinamide riboside, are collectively referred to as niacin or vitamin B3. The essential amino acid tryptophan can also be converted into NAD via the kynurenine pathway.
[Source 3 ]Figure 2. Nicotinamide adenine dinucleotide (NAD) synthesis
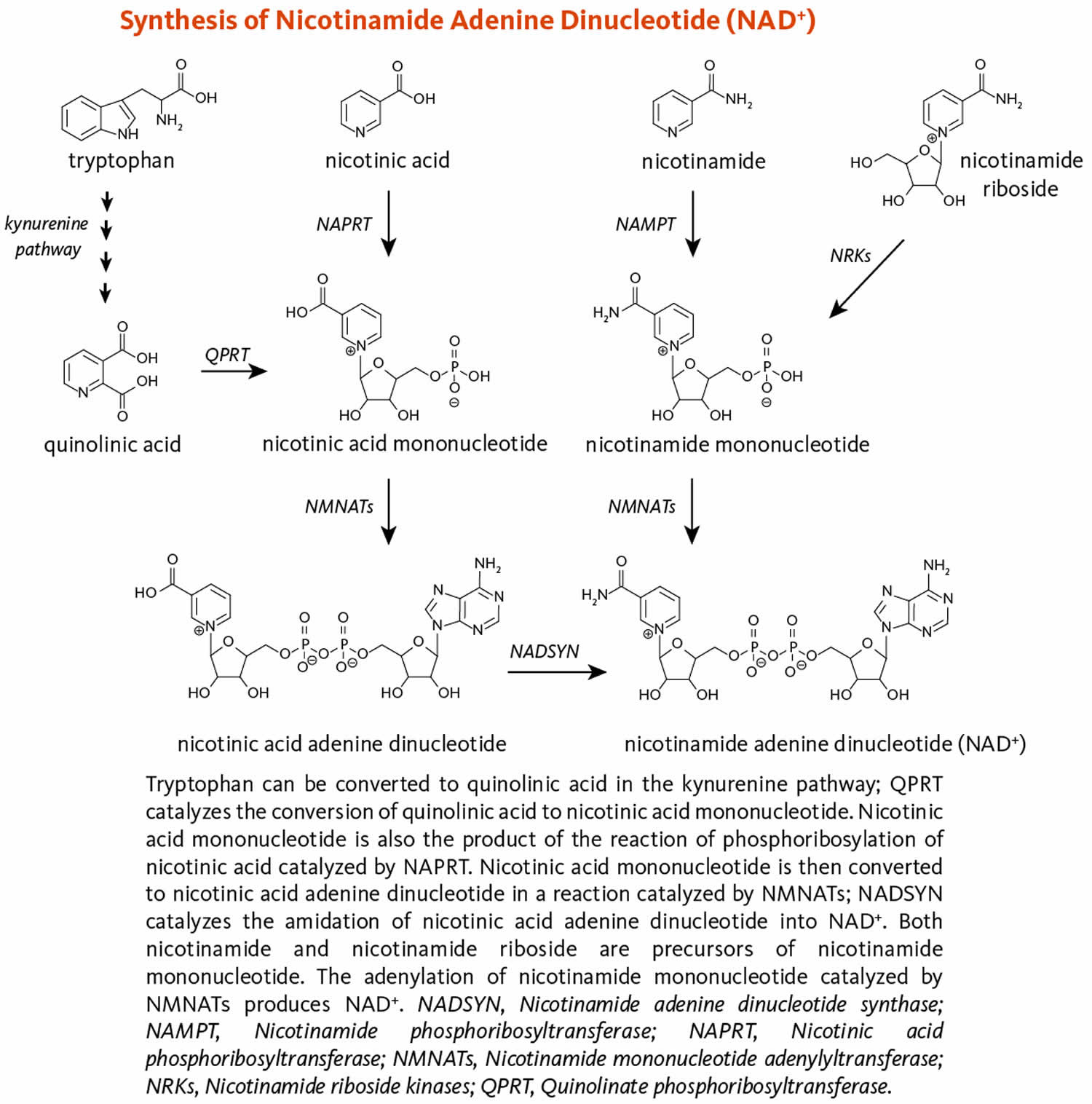
Footnote: Figure 2 illustrates the separate biosynthetic pathways that lead to nicotinamide adenine dinucleotide (NAD) production from the various dietary precursors. Nicotinamide adenine dinucleotide (NAD) is synthesized from nicotinamide and nicotinamide riboside via two enzymatic reactions, while the pathway that yields nicotinamide adenine dinucleotide (NAD) from nicotinic acid – known as the Preiss-Handler pathway — includes three steps 3. The kynurenine pathway is the longest nicotinamide adenine dinucleotide (NAD) biosynthetic pathway: the catabolism of tryptophan through kynurenine produces quinolinic acid, which is then converted to nicotinic acid mononucleotide, an intermediate in nicotinamide adenine dinucleotide (NAD) metabolism. Nicotinamide adenine dinucleotide (NAD) is then synthesized from nicotinic acid mononucleotide in the Preiss-Handler pathway 12.
[Source 3 ]Figure 3. Nicotinamide adenine dinucleotide (NAD) and nicotinamide adenine dinucleotide phosphate (NADP) functions
What does Niacin (vitamin B3) do?
Niacin is essential for maintaining cell function. Niacin is a component of nicotinamide adenine dinucleotide (NAD) and nicotinamide adenine dinucleotide phosphate (NADP) required by over 400 enzymes involved in the metabolism of carbohydrates, fats, proteins, and alcohol, as well as DNA repair and cell signalling. Therefore, tissues with a high energy requirement or cell turnover rate such as the skin, bowel, and brain are those affected by pellagra.
Living organisms derive most of their energy from redox reactions, which are processes involving the transfer of electrons. Over 400 enzymes require the niacin coenzymes, nicotinamide adenine dinucleotide (NAD) and nicotinamide adenine dinucleotide phosphate (NADP), mainly to accept or donate electrons for redox reactions 38. NAD and NADP appear to support distinct functions (Figure 3). NAD functions most often in energy-producing reactions involving the degradation (catabolism) of carbohydrates, fats, proteins, and alcohol. NADP generally serves in biosynthetic (anabolic) reactions, such as in the synthesis of fatty acids, steroids (e.g., cholesterol, bile acids, and steroid hormones), and building blocks of other macromolecules 39. NADP is also essential for the regeneration of components of detoxification and antioxidant systems (4). To support these functions, the cell maintains NAD in a largely oxidized state (NAD+) to serve as oxidizing agent for catabolic reactions, while NADP is kept largely in a reduced state (NADPH) to readily donate electrons for reductive cellular processes 39, 40.
The niacin coenzyme, nicotinamide adenine dinucleotide (NAD), is the substrate (reactant) for at least four classes of enzymes. Two classes of enzymes with mono adenosine diphosphate (ADP)-ribosyltransferase and/or poly (ADP-ribose) polymerase activities catalyze ADP-ribosyl transfer reactions. Silent information regulator-2 (Sir2)-like proteins (sirtuins) catalyze the removal of acetyl groups from acetylated proteins, utilizing ADP-ribose from NAD as an acceptor for acetyl groups. Finally, ADP-ribosylcyclases are involved in the regulation of intracellular calcium signaling 3.
Figure 4. Overview of NAD biosynthesis and function
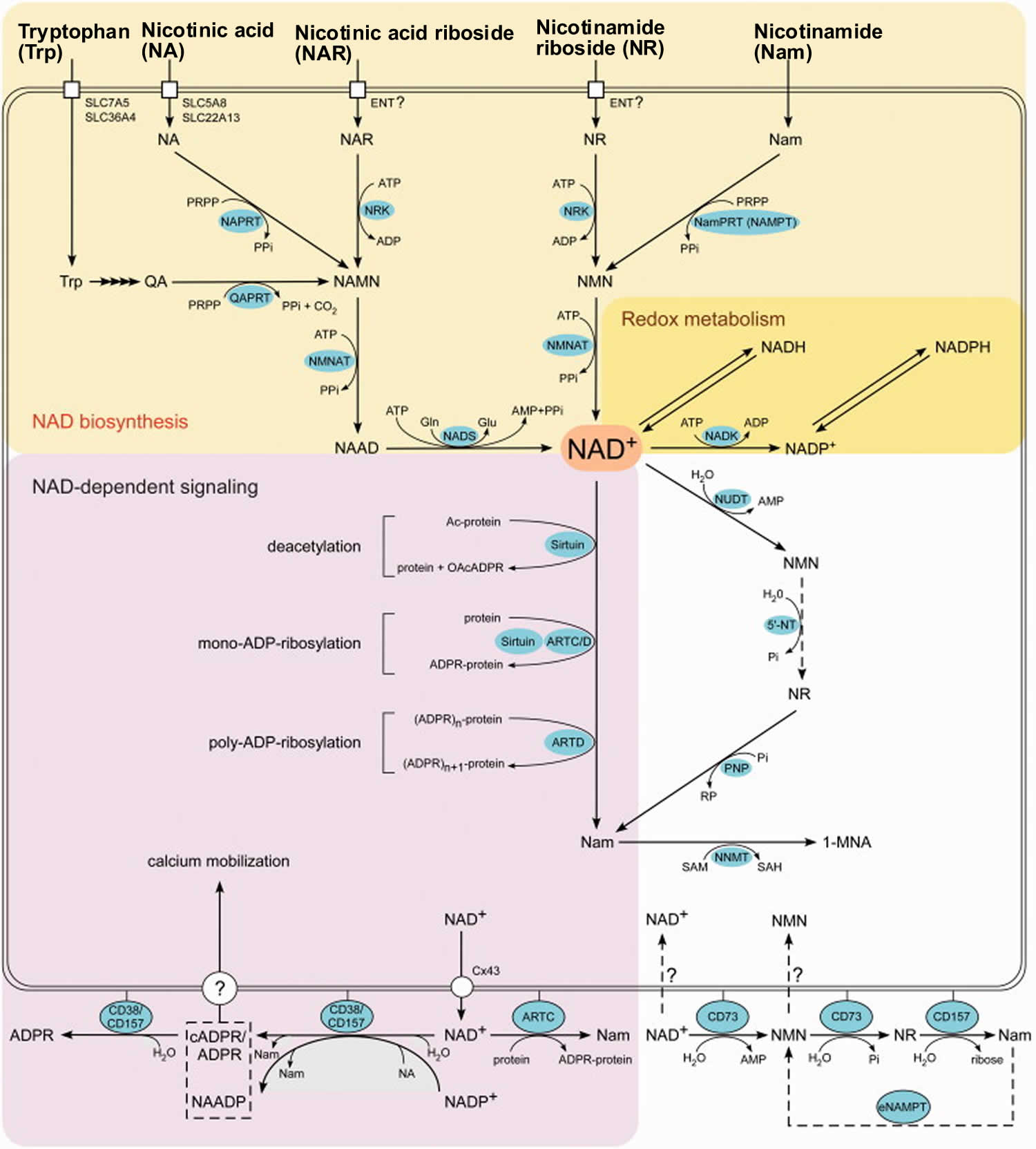
Footnotes: Overview of the NAD biosynthesis and function in humans. NAD can be synthesized from five precursors: tryptophan (Trp), the pyridine bases nicotinamide (Nam) and nicotinic acid (NA) or the nucleosides nicotinamide riboside (NR) and nicotinic acid riboside (NAR), which enter cells by different transport mechanisms. Quinolinic acid (QA), a Trp degradation product, is transformed to nicotinic acid mononucleotide (NAMN) by quinolinic acid phosphoribosyltransferase (QAPRT). Nicotinamide (Nam) and nicotinic acid (NA) are converted to the corresponding mononucleotides (NMN and NAMN) by nicotinamide phosphoribosyltransferase (NamPRT, also known as NAMPT) and nicotinic acid phosphoribosyltransferase (NAPRT), respectively. Nicotinamide mononucleotide (NMN) might also be synthesized by an extracellular NamPRT (eNAMPT). Nicotinamide mononucleotide (NMN) and nicotinic acid mononucleotide (NAMN) are also generated through phosphorylation of nicotinamide riboside (NR) and nicotinic acid riboside (NAR), respectively, by nicotinamide riboside kinases (NRK). Nicotinamide mononucleotide (NMN) and nicotinic acid mononucleotide (NAMN) are converted to the corresponding dinucleotide (NAAD or NAD+) by NMN adenylyltransferases (NMNAT). NAD synthetase (NADS) amidates NAAD to NAD+. Phosphorylation by NAD kinase (NADK) converts NAD+ to NADP+. The oxidized and reduced forms of the dinucleotides, NAD(P)+ and NAD(P)H, serve as reversible hydrogen carriers in redox reactions. Members of the Sirtuin family of protein deacetylases catalyze the transfer of the protein-bound acetyl group onto the ADP-ribose moiety, thereby forming O-acetyl-ADP ribose (OAcADPR). The transfer of a single (mono-ADP-ribosylation) or several (poly-ADP-ribosylation) ADP-ribose units from NAD+ to acceptor protein is catalyzed by diphtheria toxin-like ADP-ribosyltransferases (ARTD). Mono-ADP-ribosylation is also catalyzed by clostridial toxin-like ADP-ribosyltransferases (ARTC) and some Sirtuin proteins. NAD+ and NADP+ are also used for the synthesis of second messengers, nicotinic acid adenine dinucleotide phosphate (NAADP), cyclic ADP-ribose (cADPR) and ADPR, which mediate intracellular calcium mobilization. All the three molecules are synthesized by ecto-NAD glycohydrolases CD38 and CD157. The mechanism of how messengers reach their cytosolic targets is still debated. Signaling-independent interconversions of NAD and its intermediates include NAD hydrolysis to NMN and AMP by Nudix pyrophosphatases (NUDT); NMN dephosphorylation to nicotinamide riboside (NR) by cytosolic 5′-nucleotidases (5′-NT); phosphorolytic cleavage of nicotinamide riboside (NR) to nicotinamide (Nam) by purine nucleoside phosphorylase (PNP); and conversion of Nam to N-methylnicotinamide (1-MNA) by nicotinamide-N-methyltransferase (NNMT). NAD+ can possibly be released from cells through connexin 43 hemichannels (Cx43), and can be degraded to NR by ecto-nucleotidase CD73. Nicotinamide riboside (NR) is hydrolyzed to nicotinamide (Nam) by CD157. Whether cells can take up NAD or NMN is debated.
[Source 12 ]Lipid-lowering effects with pharmacologic doses of nicotinic acid
For over half a century, pharmacologic doses of nicotinic acid, but not nicotinamide, have been known to reduce serum cholesterol 41. However, the exact mechanisms underlying the lipid-lowering effect of nicotinic acid remain speculative. Two G-protein-coupled membrane receptors, GPR109A and GPR109B, bind nicotinic acid with high and low affinity, respectively. These nicotinic acid receptors are primarily expressed in adipose tissue and immune cells (but not lymphocytes). They are also found in retinal pigmented and colonic epithelial cells, keratinocytes, breast cells, microglia, and possibly at low levels in the liver 42. Therefore, lipid-modifying effects of nicotinic acid are likely to be mediated by receptor-independent mechanisms in major tissues of lipid metabolism like liver and skeletal muscle. Early in vitro data suggested that nicotinic acid could impair very-low-density lipoprotein (VLDL) secretion by inhibiting triglyceride synthesis and triggering ApoB lipoprotein degradation in hepatocytes 43. In another study, nicotinic acid affected the liver uptake of ApoA1 lipoprotein, thereby reducing high-density lipoprotein (HDL) removal from the circulation 44. In fat cells (adipocytes), the binding of nicotinic acid to GPR109A was found to initiate a signal transduction cascade resulting in reductions in free fatty acid production via the inhibition of hormone-sensitive lipase involved in triglyceride lipolysis 45. Nonetheless, recent observations have suggested that the lipid-lowering effect of nicotinic acid was not due to its anti-lipolytic activity (22). Trials showed that synthetic agonists of GPR109A acutely lowered free fatty acids yet failed to affect serum lipids 46. Aside from its impact on HDL and other plasma lipids, nicotinic acid has exhibited anti-atherosclerotic activities in cultured monocytes, macrophages, or vascular endothelial cells, by modulating inflammation and oxidative stress and regulating cell adhesion, migration, and differentiation 42.
Calcium mobilization
In humans, CD38 and CD157 belong to a family of NAD+ glycohydrolases or ADP-ribosylcyclases 3. These enzymes catalyze the formation of key regulators of calcium signaling, namely (linear) ADP-ribose, cyclic ADP-ribose, and nicotinic acid adenine dinucleotide phosphate. Cyclic ADP-ribose and nicotinic acid adenine dinucleotide phosphate works within cells to provoke the release of calcium ions from internal storage sites (i.e., endoplasmic reticulum, lysosomes, mitochondria), whereas ADP-ribose stimulates extracellular calcium entry through cell membrane TRPM2 cation channels 12. Another TRPM2 agonist, 2’-deoxy-ADP-ribose, was recently identified in vitro. CD38 was found to catalyze the synthesis of 2’-deoxy-ADP-ribose from nicotinamide mononucleotide and 2’-deoxy-ATP 47. O-acetyl-ADP-ribose generated by the activity of sirtuins also controls calcium entry through TRPM2 channels 40. Intracellular calcium-mediated signal transduction is regulated by transient calcium entry into the cell or release of calcium from intracellular stores. Calcium signaling is critically involved in processes like neurotransmission, insulin release from pancreatic β-cells, muscle cell contraction, and T-lymphocyte activation 40.
NAD as a ligand
NAD has been identified as an endogenous agonist of purinergic membrane receptors of the P2Y subclass. In particular, NAD was found to bind to P2Y1 receptor and act as an inhibitory neurotransmitter at neuromuscular junctions in visceral smooth muscles 48. Extracellular NAD was also found to behave like a proinflammatory cytokine, triggering the activation of isolated granulocytes. NAD binding to the P2Y11 receptor at the granulocyte surface activated a signaling cascade involving cyclic ADP-ribose and the rise of intracellular calcium, eventually stimulating superoxide generation and chemotaxis 49. Similar observations were made with lipopolysaccharide-activated monocytes 50. Extracellular NAADP+ and ADP-ribose might also bind to P2Y receptors and trigger intracellular NAADP+- and ADP-ribose-dependent calcium mobilization (see Calcium mobilization) 51, 52.
NAD-dependent deacetylation
Seven sirtuins (SIRT 1-7) have been identified in humans. Sirtuins are a class of NAD-dependent deacetylase enzymes that remove acetyl groups from the acetylated lysine residues of target proteins. During the deacetylation process, the acetyl group is transferred onto the ADP-ribose moiety cleaved off NAD, producing O-acetyl-ADP-ribose. Nicotinamide can exert feedback inhibition to the deacetylation reaction 53. Like ADP-ribosylation, acetylation is a post-translational modification that affects the function of target proteins. The initial interest in sirtuins followed the discovery that their activation could mimic caloric restriction, which has been shown to increase lifespan in lower organisms. Such a role in mammals is controversial, although sirtuins are energy-sensing regulators involved in signaling pathways that could play important roles in delaying the onset of age-related diseases (e.g., cardiovascular disease, cancer, dementia, arthritis). To date, the spectrum of their biological functions includes gene silencing, DNA damage repair, cell cycle regulation, and cell differentiation 54.
ADP-ribosylation
Enzymes with ADP-ribosyltransferase activities were formerly divided between mono ADP-ribosyltransferases (ARTs) and poly (ADP-ribose) polymerases (PARPs). ARTs were first discovered in certain pathogenic bacteria — like those causing cholera or diphtheria — where they mediate the actions of toxins. These enzymes transfer an ADP-ribose residue moiety from NAD to a specific amino acid of a target protein, with the creation of an ADP-ribosylated protein and the release of nicotinamide.
Because most PARPs have been found to exhibit only mono ADP-ribosyltransferase activities, a new nomenclature was proposed for enzymes catalyzing ADP-ribosylation: A family of mono ADP-ribosyltransferases with homology to bacterial diphteria toxins was named ARTD, while enzymes with either mono or poly ADP-ribosyltransferase activities and related to C2 and C3 clostridial toxins were included in the ARTC family 55, 56.
- ARTCs are extracellular enzymes that catalyze the mono ADP-ribosylation of membrane or secreted proteins involved in innate immunity and cell communication 12.
- ARTDs are intracellular enzymes with either mono or poly ADP-ribosyltransferase activities. At least 18 ARTDs have been identified. All ARTDs possess a diphtheria toxin-like catalytic domain that binds NAD+. Only ARTDs 1, 2, 5, and 6 catalyze poly (ADP-ribose) transfers; the others have mono ADP-ribosyltransferase activities. ARTDs were shown to be involved in DNA repair and stress responses, cell signaling, transcription regulation, apoptosis, cell differentiation, maintenance of genomic integrity, and antiviral defense 56.
How much Niacin (vitamin B3) do I need?
The amount of niacin you need depends on your age and sex. Average daily recommended amounts are listed below in milligrams (mg) of niacin equivalents (NE) (except for infants in their first 6 months) 13. The mg niacin equivalents (NE) measure is used because your body can also make niacin from tryptophan, an amino acid in proteins. For example, when you eat turkey, which is high in tryptophan, some of this amino acid is converted to niacin in your liver. Using mg niacin equivalents (NE) accounts for both the niacin you consume and the niacin your body makes from tryptophan. Infants in their first six months do not make much niacin from tryptophan.
Table 1 lists the current Recommended Dietary Allowances (RDAs) for niacin as mg of niacin equivalents (NE) 6. The Food and Nutrition Board defines 1 NE as 1 mg niacin or 60 mg of the amino acid tryptophan (which the body can convert to niacin). Niacin RDAs for adults are based on niacin metabolite excretion data. For children and adolescents, niacin RDAs are extrapolated from adult values on the basis of body weight. The Adequate Intake (AI) for infants from birth to 6 months is for niacin alone, as young infants use almost all the protein they consume for growth and development; it is equivalent to the mean intake of niacin in healthy, breastfed infants. For infants aged 7-12 months, the Adequate Intake (AI) for niacin is in mg NE and is based on amounts consumed from breast milk and solid foods.
Most people in the United States get enough niacin from the foods they eat. Niacin deficiency is very rare in the United States 13. However, some people are more likely than others to have trouble getting enough niacin:
- Undernourished people with AIDS, alcohol use disorder, anorexia, inflammatory bowel disease, or liver cirrhosis
- People whose diet has too little iron, riboflavin, or vitamin B6; these nutrients are needed to convert tryptophan to niacin
- People with Hartnup disease, a rare genetic disorder
- People with carcinoid syndrome, a condition in which slow-growing tumors develop in the gastrointestinal tract
An analysis of data from the 2015–2016 National Health and Nutrition Examination Survey (NHANES) found that the average daily niacin intake from foods and beverages was 21.4 mg for ages 2–19 57. In adults, the average daily niacin intake from foods and beverages was 31.4 mg in men and 21.3 mg in women. An analysis of data from the 2009-2012 NHANES found that only 1% of adults had intakes of niacin from foods and beverages below the Estimated Average Requirements (the average daily level of intake estimated to meet the requirements of 50% of healthy individuals; usually used to assess the nutrient intakes of groups of people and to plan nutritionally adequate diets for them; can also be used to assess the nutrient intakes of individuals) 58. Among all racial and ethnic groups, Hispanics had the greatest prevalence, 1.3%, of niacin intakes below the Estimated Average Requirement 59.
According to self-reported data from the 2013-2014 NHANES, 21% of all individuals aged 2 and older took a dietary supplement containing niacin 57. The proportion of users increased with age from 8% of those aged 12-19 years to 39% of men and 40% of women aged 60 and older. Supplement use doubled or tripled total niacin intakes compared with intakes from diet alone. According to data from the 2003-2006 NHANES, 10% of all individuals aged 2 and older who took dietary supplements had total niacin intakes that reached or exceeded the Tolerable Upper Intake Level (the maximum daily intake unlikely to cause adverse health effects) (see Table 2 below) 60.
Table 1. Recommended Dietary Allowances (RDAs) for Niacin
| Life Stage | Recommended Amount |
|---|---|
| Birth to 6 months* | 2 mg |
| Infants 7–12 months* | 4 mg NE |
| Children 1–3 years | 6 mg NE |
| Children 4–8 years | 8 mg NE |
| Children 9–13 years | 12 mg NE |
| Teen boys 14–18 years | 16 mg NE |
| Teen girls 14–18 years | 14 mg NE |
| Adult men 19+ years | 16 mg NE |
| Adult women 19+ years | 14 mg NE |
| Pregnant teens and women | 18 mg NE |
| Breastfeeding teens and women | 17 mg NE |
Footnote: Recommended Dietary Allowance (RDA) is the average daily level of intake sufficient to meet the nutrient requirements of nearly all (97%–98%) healthy individuals; often used to plan nutritionally adequate diets for individuals.
* Adequate Intake (AI) is intake at this level is assumed to ensure nutritional adequacy; established when evidence is insufficient to develop an RDA.
[Source 13 ]Table 2. Tolerable Upper Intake Levels (ULs) for Niacin
| Age | Male | Female | Pregnancy | Lactation |
|---|---|---|---|---|
| Birth to 6 months | None established* | None established* | ||
| 7–12 months | None established* | None established* | ||
| 1–3 years | 10 mg | 10 mg | ||
| 4–8 years | 15 mg | 15 mg | ||
| 9–13 years | 20 mg | 20 mg | ||
| 14–18 years | 30 mg | 30 mg | 30 mg | 30 mg |
| 19+ years | 35 mg | 35 mg | 35 mg | 35 mg |
Footnote: * Breast milk, formula, and food should be the only sources of niacin for infants.
[Source 4 ]What foods provide Niacin (vitamin B3)?
Niacin is found naturally in many foods, and is added to some foods. You can get recommended amounts of niacin by eating a variety of foods, including the following:
- Animal based foods foods, such as poultry, beef, pork, and fish, provide about 5-10 mg niacin per serving, primarily in the highly bioavailable forms of NAD and NADP 7.
- Plant-based foods, such as nuts, legumes, and grains, provide about 2-5 mg niacin per serving, mainly as nicotinic acid.
- Some types of nuts, legumes, and grains. In some grain products, however, naturally present niacin is largely bound to polysaccharides and glycopeptides that make it only about 30% bioavailable 7, 9.
- Many breads, cereals, and infant formulas in the United States and many other countries contain added niacin. Niacin that is added to enriched and fortified foods is in its free form and therefore highly bioavailable 6.
Tryptophan is another food source of niacin because this amino acid—when present in amounts beyond that required for protein synthesis—can be converted to NAD, mainly in the liver 7, 24. The most commonly used estimate of efficiency for tryptophan conversion to NAD is 1:60 (i.e., 1 mg niacin [NAD] from 60 mg tryptophan). Turkey is an example of a food high in tryptophan; a 3-oz portion of turkey breast meat provides about 180 mg tryptophan, which could be equivalent to 3 mg niacin 4. However, the efficiency of the conversion of tryptophan to NAD varies considerably in different people 7.
The U.S. Department of Agriculture’s (USDA’s) FoodData Central (https://fdc.nal.usda.gov) lists the nutrient content of many foods and provides a comprehensive list of foods containing niacin arranged by nutrient content (https://www.nal.usda.gov/sites/www.nal.usda.gov/files/niacin.pdf).
Table 3. Niacin Content of Selected Foods
| Food | Milligrams (mg) per serving | Percent Daily Value (DV)** |
|---|---|---|
| Beef liver, pan fried, 3 ounces | 14.9 | 93 |
| Chicken breast, meat only, grilled, 3 ounces | 10.3 | 64 |
| Marinara (spaghetti) sauce, ready to serve, 1 cup | 10.3 | 64 |
| Turkey breast, meat only, roasted, 3 ounces | 10 | 63 |
| Salmon, sockeye, cooked, 3 ounces | 8.6 | 54 |
| Tuna, light, canned in water, drained, 3 ounces | 8.6 | 54 |
| Pork, tenderloin, roasted, 3 ounces | 6.3 | 39 |
| Beef, ground, 90% lean, pan-browned, 3 ounces | 5.8 | 36 |
| Rice, brown, cooked, 1 cup | 5.2 | 33 |
| Peanuts, dry roasted, 1 ounce | 4.2 | 26 |
| Breakfast cereals fortified with 25% DV niacin | 4 | 25 |
| Rice, white, enriched, cooked, 1 cup | 2.3 | 14 |
| Potato (russet), baked, 1 medium | 2.3 | 14 |
| Sunflower seeds, dry roasted, 1 ounce | 2 | 13 |
| Bread, whole wheat, 1 slice | 1.4 | 9 |
| Pumpkin seeds, dry roasted, 1 ounce | 1.3 | 8 |
| Soymilk, unfortified, 1 cup | 1.3 | 8 |
| Bread, white, enriched, 1 slice | 1.3 | 8 |
| Lentils, boiled and drained, ½ cup | 1 | 6 |
| Bulgur, cooked, 1 cup | 0.9 | 6 |
| Banana, 1 medium | 0.8 | 5 |
| Edamame, frozen, prepared, ½ cup | 0.7 | 4 |
| Raisins, ½ cup | 0.6 | 4 |
| Tomatoes, cherry, ½ cup | 0.5 | 3 |
| Broccoli, boiled, drained, chopped, ½ cup | 0.4 | 3 |
| Cashews, dry roasted, 1 ounce | 0.4 | 3 |
| Yogurt, plain, low fat, 1 cup | 0.3 | 2 |
| Apple, 1 medium | 0.2 | 1 |
| Chickpeas, canned, drained, 1 cup | 0.2 | 1 |
| Milk, 1% milkfat, 1 cup | 0.2 | 1 |
| Spinach, frozen, chopped, boiled, ½ cup | 0.2 | 1 |
| Tofu, raw, firm, ½ cup | 0.2 | 1 |
| Onions, chopped, ½ cup | 0.1 | 1 |
| Egg, large | 0 | 0 |
Footnotes: These values are for the niacin content of foods only. They do not include the contribution of tryptophan, some of which is converted to NAD in the body.
** DV = Daily Value. The U.S. Food and Drug Administration (FDA) developed Daily Values (DVs) to help consumers compare the nutrient contents of foods and dietary supplements within the context of a total diet. The DV for niacin is 16 mg for adults and children aged 4 years and older 61. The FDA does not require food labels to list niacin content unless niacin has been added to the food. Foods providing 20% of more of the DV are considered to be high sources of a nutrient.
[Source 4 ]What kinds of Niacin supplements are available?
Niacin is found in multivitamin or multivitamin-mineral supplements. Niacin is also available in B-complex dietary supplements and supplements containing only niacin. The two main forms of niacin in dietary supplements are nicotinic acid and nicotinamide. Some niacin-only supplements contain 500 mg or more per serving, which is much higher than the Recommended Dietary Allowance (RDA) for this nutrient 4.Niacin (in the form of nicotinic acid) is also available as a prescription medicine used to treat high blood cholesterol levels.Nicotinic acid in supplemental amounts beyond nutritional needs can cause skin flushing, so some formulations are manufactured and labeled as prolonged, sustained, extended, or timed release to minimize this unpleasant side effect. Nicotinamide does not produce skin flushing because of its slightly different chemical structure 28. Niacin supplements are also available in the form of inositol hexanicotinate, and these supplements are frequently labeled as being “flush free” because they do not cause flushing. The absorption of niacin from inositol hexanicotinate varies widely but on average is 30% lower than from nicotinic acid or nicotinamide, which are almost completely absorbed 28, 62, 63. Two niacin-like compounds, nicotinamide riboside and nicotinamide mononucleotide (NMN; also referred to as β-NMN), are also available as dietary supplements, but are not marketed or labelled as sources of niacin 4. However, FDA ruled in November 2022 that nicotinamide mononucleotide (NMN) may not be legally marketed as a dietary supplement because it has been authorized for investigation by FDA as a new drug 64.
What happens if I don’t get enough Niacin?
You can develop niacin deficiency if you don’t get enough niacin or tryptophan from the foods you eat. Severe niacin deficiency leads to a disease called pellagra. Pellagra, which is uncommon in developed countries, can have these effects 13:
- Rough skin that turns red or brown in the sun
- A bright red tongue
- Vomiting, constipation, or diarrhea
- Depression
- Headaches
- Extreme tiredness
- Aggressive, paranoid, or suicidal behavior
- Hallucinations, apathy, loss of memory
In its final stages, pellagra leads to loss of appetite followed by death.
Niacin (vitamin B3) health benefits
Scientists are studying niacin to better understand how it affects health. Here is an example of what this research has shown.
Cardiovascular disease
Scientists have studied the use of large doses of niacin in the form of nicotinic acid to help reduce the risk of heart attack and stroke in people with atherosclerosis. They found that prescription-strength nicotinic acid (more than 100 times the recommended dietary allowance [RDA]) can lower blood levels of LDL (bad) cholesterol, raise levels of HDL (good) cholesterol, and lower levels of triglycerides 4. But these favorable effects on blood lipids (fats) don’t affect the risk of having a cardiovascular event, such as heart attack, sudden cardiac death, or stroke. In addition, experts do not recommend high doses of nicotinic acid for people taking a statin medication. Nicotinamide does not have this effect because, unlike nicotinic acid, it does not bind to the receptors that mediate nicotinic acid’s effects on lipid profiles 5. Your doctor should approve and supervise any use of very high doses of nicotinic acid (in the thousands of milligrams) to treat atherosclerosis.
Studies conducted since the late 1950s show that these doses can increase high-density lipoprotein (HDL; “good”) cholesterol levels by 10-30% and reduce low-density lipoprotein (LDL; “bad”) cholesterol levels by 10-25%, triglyceride levels by 20-50%, and lipoprotein(a) levels by 10-30% 28. Together, these changes in lipid parameters might be expected to reduce the risk of first-time or subsequent cardiac events, such as heart attacks and strokes, in adults with atherosclerotic cardiovascular disease. However, despite dozens of published clinical trials, experts do not agree on the value of nicotinic acid to treat cardiovascular disease, especially given its side effects, safety concerns, and poor patient compliance 65.
In one large clinical trial from the 1970s, 8,341 participants aged 30 to 64 years who had had one or more heart attacks were randomized to take one of five lipid-lowering medications, including 3,000 mg/day nicotinic acid, or a placebo for an average of 6.2 years 66. Those taking nicotinic acid lowered their serum cholesterol levels by an average of 9.9% and triglyceride levels by 26.1% over 5 years of treatment 66. During 5 to 8.5 years of treatment, these participants had significantly fewer nonfatal myocardial infarctions but more cardiac arrhythmias than those in the placebo group. Their overall rates of mortality and cause-specific mortality, including from coronary heart disease, did not decline 66. But 9 years after the study ended, participants who had taken the nicotinic acid experienced significantly fewer (11%) deaths from all causes than those who had taken the placebo 67, 68.
Statin medications have become the treatment of choice for hyperlipidemia and lowering the risks of atherosclerotic cardiovascular disease. For this reason, clinical trials of nicotinic acid in the past several decades have examined whether it provides any additional cardiovascular protection to people taking statins 30.
In the largest international, multicenter, clinical trial of nicotinic acid to date, 25,673 adults aged 50-80 years (83% men) with cardiovascular disease who were taking a statin were randomized to take 2000 mg/day extended-release nicotinic acid with a medication to reduce nicotinic acid’s flushing effect and therefore improve treatment compliance or a matching placebo for a median of 4 years 69, 70. The nicotinic acid group had a mean reduction in LDL cholesterol (of 10 mg/dl) and triglycerides (of 33 mg/dl) and an increase in HDL cholesterol (of 6 mg/dl), but this group had no significant reduction in rates of major vascular events compared with the placebo (statin-only) group 69, 70. Furthermore, the nicotinic acid group had a significantly greater risk of diabetes, gastrointestinal dyspepsia, diarrhea, ulceration, bleeding events in the gut and brain, and skin rashes and ulcerations. An earlier randomized clinical trial of 3,414 patients with established cardiovascular disease was stopped after 3 years when the researchers found that patients taking niacin (1,500-2,000 mg/day extended release) in addition to their cholesterol-reduction medications did not have fewer cardiovascular events than those taking medication alone, even though the niacin reduced triglyceride and LDL-cholesterol levels further and raised HDL cholesterol levels further 71. The results also showed that patients taking niacin had an increased risk of ischemic stroke.
The authors of two 2017 systematic reviews examining the clinical trial data concluded that nicotinic acid therapy provides little if any protection from atherosclerotic heart disease, even though the therapy raises HDL cholesterol levels and lowers total cholesterol, LDL cholesterol, and triglyceride levels 65. One of these reviews examined 23 randomized controlled trials of moderate to high quality in 39,195 participants aged 33-71 years (average 65 years; majority were male). Some had experienced a heart attack, and most were taking a statin. The doses used and treatment duration in these studies varied widely; the median dose of nicotinic acid was 2000 mg/day (range 500 to 4000 mg/day) for a median of 11.5 months (range 6 months to 6 years) 65. Overall, use of nicotinic acid did not reduce overall mortality or cardiovascular mortality rates or the number of fatal or nonfatal myocardial infarctions or strokes. Eighteen percent of participants taking nicotinic acid discontinued treatment because of side effects. The second review examined 13 randomized controlled trials with 35,206 participants with, or at risk of, atherosclerotic cardiovascular disease 72. Overall, the addition of nicotinic acid supplementation (dose range not specified) to statin therapy taken for a mean of 33 months (with a broad range of 6 to 60 months) did not lead to significant reductions in rates of all-cause or cardiovascular mortality, myocardial infarction, or stroke 72. Nicotinic acid treatment was associated with a significantly higher risk of gastrointestinal and musculoskeletal adverse events 72. In addition, four of the studies that examined diabetes as an outcome found that the patients taking niacin had a significantly higher risk of developing the disease.
A 2018 review of three randomized controlled trials with 29,195 patients found that all-cause mortality increased by 10% more in those who took 1000 to 3000 mg/day extended release nicotinic acid in addition to a statin medication than patients taking the statin alone 73.
In their guidelines for lowering blood cholesterol levels, the American College of Cardiology and the American Heart Association advise that nonstatin therapies, compared with or in addition to statin therapy, do not provide atherosclerotic cardiovascular disease risk-reduction benefits that outweigh the potential harms of their adverse effects 30. When discussing the use of nicotinic acid supplements to reduce the risk of hyperlipidemia (for example, in patients unable to tolerate statin medications), the two professional societies recommend that patients take 500 mg/day extended-release nicotinic acid supplements and increase the dose to a maximum of 2,000 mg/day over 4 to 8 weeks or take 100 mg immediate-release nicotinic acid three times a day and increase the dose to 3,000 mg/day divided into two or three doses. Their joint statement about monitoring supplement users who take niacin to reduce hyperlipidemia risk for adverse effects is described in the Health Risks from Excessive Niacin section below. In their 2018 report, these two professional societies stated what although niacin may be useful in some cases of severe hypertriglyceridemia, it has only mild LDL-lowering effects. The societies therefore do not recommend using it as an add-on drug to statin therapy 74.
Overall, the evidence indicates that nicotinic acid supplementation improves blood lipid profiles but has no significant effects on risk of cardiovascular events 4. Although nicotinic acid is a nutrient, if very high doses (thousands of mg) are taken to treat hyperlipidemias, the supplement is being used as a drug. Such doses should only be taken with medical approval and supervision 4.
Friedreich’s ataxia
Friedreich’s ataxia, a common form of inherited ataxia, is an early onset recessive disorder with clinical features that includes progressive ataxia, scoliosis, dysarthria, cardiomyopathy, and diabetes mellitus 75. Most affected subjects carry homozygous guanine-adenine-adenine (GAA) repeat expansions in the first intron of the gene FXN coding for the protein frataxin. These abnormal and unstable GAA repeats trigger gene silencing through heterochromatin formation, leading to significantly reduced frataxin expression 76. Frataxin is a mitochondrial protein needed for the making of iron-sulfur clusters (ISC). ISC-containing subunits are especially important for the mitochondrial respiratory chain and for the synthesis of heme-containing proteins 75.
Predominantly localized in the nucleus, SIRT1 is a NAD-dependent deacetylase that promotes gene silencing through heterochromatin formation. Nicotinamide has been shown to antagonize heterochromatization of the FXN locus and upregulate frataxin expression in lymphoblastoid cells derived from Friedreich’s ataxia-affected patients, possibly through inhibiting SIRT1 activity 76. In an open-label, dose escalating pilot trial in 10 adult patients with Friedreich’s ataxia, single and repeated doses of nicotinamide (2-8 g) for up to eight weeks were found to be well tolerated 77. Repeated daily doses of 3.5 to 6 g of nicotinamide led to significant increases in frataxin concentration in peripheral white blood cells 77. Yet, no neurological improvements were reported, suggesting that the duration of the treatment was too short and/or the nervous system of the participants was unresponsive to increases in frataxin 78. There is currently no ongoing trial designed to further investigate the effect of nicotinamide in Friedreich’s ataxia-affected patients.
HIV/AIDS
The first step in the kynurenine pathway is catalyzed by the extrahepatic enzyme, indoleamine 2,3-dioxygenase (IDO), which is responsible for the oxidative cleavage of tryptophan. The chronic stimulation of tryptophan oxidation, mediated by an increased activity of indoleamine 2,3-dioxygenase (IDO) and/or inadequate dietary niacin intakes, is observed with the infection of human immunodeficiency virus (HIV), the virus that causes acquired immunodeficiency syndrome (AIDS). Interferon-gamma (IFN-γ) is a cytokine produced by cells of the immune system in response to infection. Through stimulating the enzyme indoleamine 2,3-dioxygenase (IDO), IFN-γ increases the breakdown of tryptophan, thus supporting the finding that the average tryptophan concentration in blood is significantly lower in HIV patients compared to uninfected subjects 79. An increased degradation of tryptophan via the kynurenine pathway appears to coexist with intracellular niacin/NAD deficiency in HIV infection 80. An explanatory model for these paradoxical observations incriminates the oxidative stress induced by multiple nutrient deficiencies in HIV patients 80. In particular, the activation of PARP enzymes (ARTDs) by oxidative damage to DNA could be responsible for inducing niacin/NAD depletion. The breakdown of tryptophan would then be a compensatory response to inadequate niacin/NAD levels.
However, metabolites derived from the oxidation of tryptophan in the kynurenine pathway regulate specific T-lymphocyte subgroups. As mentioned above, circulating IFN-γ, but also viral and bacterial products, can activate indoleamine 2,3-dioxygenase (IDO) during HIV infection. The overstimulation of the tryptophan pathway has been involved in the loss of normal T-lymphocyte function, which characterizes HIV infection 81, 82. The increased IDO activity has been linked to the altered immune response that contributes to the persistence of HIV 81. Antiretroviral therapy (ART) only partially restores normal IDO activity, without normalizing it, yet induces viral suppression and CD4 T-cell recovery 83. In a monkey model for HIV infection, a partial and transient blockade of IDO with IDO inhibitor 1-methyl tryptophan proved ineffective to reduce the viral load in plasma and intestinal tissues beyond the level achieved by antiretroviral therapy 84. At present, a better understanding of the role of kynurenine pathway and other NAD biosynthetic pathways during HIV infection is needed before the relevance and clinical implications of niacin supplementation in HIV treatment could be considered.
Nonetheless, pharmacologic doses of nicotinic acid have been shown to be well tolerated in HIV patients with hyperlipidemia 85. Abnormal lipid profiles observed in patients have been attributed to the HIV infection and to the highly active antiretroviral treatment (HAART) 86. Moreover, insulin resistance has been detected together with dyslipidemia in antiretroviral therapy-treated patients 87. Cardiovascular disease is the second most frequent cause of deaths in the HIV population, and the rate of cardiovascular disease is predicted to increase further as patients are living longer due to successful antiretroviral therapies. As for the general population, statin-based therapy appears to benefit HIV patients in terms of atherogenic protection and cardiovascular disease risk reduction, although contraindications exist due to drug interactions with anti-retroviral therapy. Other first-line treatments include lipid-lowering fibrates, which are preferred to nicotinic acid due to the increased risk of glucose intolerance and insulin resistance 88. Nevertheless, an unblinded, controlled pilot study showed that extended-release nicotinic acid (0.5-1.5 g/day for 12 weeks) could effectively improve endothelial function of the brachial artery in antiretroviral therapy-treated HIV subjects with low HDL-cholesterol and no history of cardiovascular disease 89. In addition, a combined treatment of fibrates, extended-release nicotinic acid (0.5-2 g/day), and lifestyle changes (low-fat diet and exercise) for 24 weeks was effective in normalizing lipid parameters in a cohort of 191 antiretroviral therapy-treated patients. Increased risk of liver dysfunction was detected in subjects receiving both fibrates and niacin, but insulin sensitivity was not affected by nicotinic acid treatment given alone or when combined with fibrates 90. Another 24-week, open-label, uncontrolled trial in 99 antiretroviral therapy-treated patients found that randomization to extended-release nicotinic acid (0.5-2 g/day) or fenofibrates increased blood HDL-cholesterol but did not reduce inflammatory markers or improve endothelial function when compared to baseline 91.
Schizophrenia
Schizophrenia is a neurologic disorder with unclear etiology that is diagnosed purely from its clinical presentation. Because neurologic disorders associated with pellagra resemble acute schizophrenia, niacin-based therapy for the condition was investigated during the 1950s-70s 92. The adjunctive use of nutrients like niacin to correct deficiencies associated with neurologic symptoms is called orthomolecular psychiatry 93. Such an approach has not been included in psychiatric practice; practitioners have instead relied solely on antipsychotic drugs to eliminate the clinical symptoms of schizophrenia. Nevertheless, recent scientific advances and new hypotheses on the benefit of nutrient supplementation in the treatment of psychiatric disorders have suggested the re-assessment of orthomolecular medicine by the medical community 94, 95.
Skin flushing is one major side effect of the therapeutic use of nicotinic acid and the primary reason for non-adherence to treatment (see side effects). Flushing is caused by the activation of phospholipase A2, an enzyme that stimulates the production of a specific lipid from the prostanoid family called prostaglandin D2. Prostaglandin D2, synthesized by antigen-presenting cells of the skin and mucosa (i.e., the Langerhans cells), can induce the dilation of blood vessels and trigger a flushing response. Interestingly, patients with schizophrenia tend not to flush following treatment with nicotinic acid. This blunted skin flushing response suggests abnormal prostanoid signaling in schizophrenic patients 96, 97. An association has been found between the altered niacin sensitivity and greater functional impairment in schizophrenic subjects 98, which supports other findings suggesting that altered lipid metabolism could critically impair brain development and contribute to the disease 99. Interestingly, blunted skin flushing responses are more prevalent in first-degree relatives of people with schizophrenia than in the general population, suggesting that reduced niacin sensitivity is a heritable trait within affected families 100.
Cancer prevention
Studies of cultured cells (in vitro) provide evidence that NAD content influences mechanisms that maintain genomic stability. Loss of genomic stability, characterized by a high rate of damage to DNA and chromosomes, is a hallmark of cancer 101. The current understanding is that the pool of NAD is decreased during niacin deficiency and that it affects the activity of NAD-consuming enzymes rather than redox and metabolic functions 102. Among NAD-dependent reactions, poly ADP-ribosylations catalyzed by PARP enzymes (ARTDs) are critical for the cellular response to DNA injury. After DNA damage, PARPs are activated; the subsequent poly ADP-ribosylations of a number of signaling and structural molecules by PARPs were shown to facilitate DNA repair at DNA strand breaks 103. Cellular depletion of NAD has been found to decrease levels of the tumor suppressor protein p53, a target for poly ADP-ribosylation, in human breast, skin, and lung cells 104. The expression of p53 was also altered by niacin deficiency in rat bone marrow cells 105. Impairment of DNA repair caused by niacin deficiency could lead to genomic instability and drive tumor development in rat models 106, 107. Both PARPs and sirtuins have been recently involved in the maintenance of heterochromatin, a chromosomal domain associated with genome stability, as well as in transcriptional gene silencing, telomere integrity, and chromosome segregation during cell division 108, 109. Neither the cellular NAD content nor the dietary intake of NAD precursors necessary for optimizing protective responses following DNA damage has been determined, but both are likely to be higher than that required for the prevention of pellagra.
Bone marrow
Cancer patients often suffer from bone marrow suppression following chemotherapy, given that bone marrow is one of the most proliferative tissues in the body and thus a primary target for chemotherapeutic agents. Niacin deficiency was found to decrease bone marrow NAD and poly-ADP-ribose levels and increase the risk of chemically induced leukemia in rats 110. Conversely, a pharmacologic dose of either nicotinic acid or nicotinamide was able to increase NAD and poly ADP-ribose in bone marrow and decrease the development of leukemia in rats 111. It has been suggested that niacin deficiency often observed in cancer patients could sensitize bone marrow tissue to the suppressive effect of chemotherapy. However, little is known regarding cellular NAD levels and the prevention of DNA damage or cancer in humans. One study in two healthy individuals involved elevating NAD levels in blood lymphocytes by supplementation with 100 mg/day of nicotinic acid for eight weeks. Compared to non-supplemented individuals, the supplemented individuals had reduced DNA strand breaks in lymphocytes exposed to free radicals in a test tube assay 112. However, nicotinic acid supplementation of up to 100 mg/day for 14 weeks in 21 healthy smokers failed to provide any evidence of a decrease in cigarette smoke-induced genetic damage in blood lymphocytes compared to placebo 113. More recently, the frequency of chromosome translocation was used to evaluate DNA damage in peripheral blood lymphocytes of 82 pilots chronically exposed to ionizing radiation, a known human carcinogen. In this observational study, the rate of chromosome aberrations was significantly lower in subjects with higher (28.4 mg/day) compared to lower (20.5 mg/day) dietary niacin intake 114. Higher availability of NAD in x-ray treated peripheral blood lymphocytes was found to favor DNA repair by enhancing survival, particularly through SIRT-mediated p53 deacetylation 115.
Upper digestive tract cancer
Generally, relationships between dietary factors and cancer are established first in epidemiological studies and followed up by basic cancer research at the cellular level. In the case of niacin, research on biochemical and cellular aspects of DNA repair has stimulated an interest in the relationship between niacin intake and cancer risk in human populations 116. A large case-control study found increased consumption of niacin, along with antioxidant nutrients, to be associated with decreased incidence of oral (mouth), pharyngeal (throat), and esophageal cancers in northern Italy and Switzerland. An increase in daily niacin intake of 6.2 mg was associated with about a 40% decrease in cases of cancers of the mouth and throat, while a 5.2 mg increase in daily niacin intake was associated with a similar decrease in cases of esophageal cancer 117, 118.
Skin cancer
Niacin deficiency can lead to severe sunlight sensitivity in exposed skin. Given the implication of NAD-dependent enzymes in DNA repair, there has been some interest in the effect of niacin on skin health. In vitro and animal experiments have helped gather information, but human data on niacin/NAD status and skin cancer are very limited. One study reported that niacin supplementation decreased the risk of ultraviolet light (UV)-induced skin cancers in mice, despite the fact that mice convert tryptophan to NAD more efficiently than rats and humans and thus do not get severely deficient 119. Hyper-proliferation and impaired differentiation of skin cells can alter the integrity of the skin barrier and increase the occurrence of pre-malignant and malignant skin conditions. A protective effect of niacin was suggested by topical application of myristyl nicotinate, a niacin derivative, which successfully increased the expression of epidermal differentiation markers in subjects with photodamaged skin 120. The activation of the nicotinic acid receptors, GPR109A and GPR109B, by pharmacologic doses of niacin could be involved in improving skin barrier function. Conversely, differentiation defects in skin cancer cells were linked to the abnormal cellular localization of defective nicotinic acid receptors 121. Nicotinamide restriction with subsequent depletion of cellular NAD was shown to increase oxidative stress-induced DNA damage in a precancerous skin cell model, implying a protective role of NAD-dependent pathways in cancer 122. Altered NAD availability also affects sirtuin expression and activity in UV-exposed human skin cells. Along with PARPs, NAD-consuming sirtuins could play an important role in the cellular response to photodamage and skin homeostasis 123.
A pooled analysis of two large US prospective cohort studies that followed 41,808 men and 72,308 women for up to 26 years suggested that higher versus lower intake of niacin (from diet and supplements) might be protective against squamous-cell carcinoma but not against basal-cell carcinoma and melanoma 124. A phase 3, randomized, double-blind, placebo-controlled trial in 386 subjects with a history of nonmelanoma skin cancer recently examined the effect of daily nicotinamide supplementation (1 g) for 12 months on skin cancer recurrence at three-month intervals over an 18-month period 125. Nicotinamide effectively reduced the rate of premalignant actinic keratose (-11%), squamous-cell carcinoma (-30%), and basal-cell carcinoma (-20%) compared to placebo after 12 months, yet this protection was not sustained during the six-month post-supplementation period 125. Larger trials are needed to assess whether nicotinamide could reduce the risk of melanomas, which are not as common as other skin cancer but are more deadly 126.
Type 1 diabetes mellitus
Type 1 diabetes mellitus in children is caused by the autoimmune destruction of insulin-secreting β-cells in the pancreas. Prior to the onset of symptomatic diabetes, specific antibodies, including islet cell autoantibodies (ICA), can be detected in the blood of high-risk individuals 127. In an experimental animal model of diabetes, high levels of nicotinamide are administered to protect β-cells from damage caused by streptozotocin 128.
Yet, pharmacologic doses of nicotinamide (up to 3 g/day) have not been found to be effective in delaying or preventing the onset of type 1 diabetes in at-risk subjects. An analysis of 10 trials, of which five were placebo-controlled, found evidence of improved β-cell function after one year of treatment with nicotinamide, but the analysis failed to find any clinical evidence of improved glycemic control 129. A large, multicenter randomized controlled trial of nicotinamide in islet cell autoantibodies-positive siblings (ages, 3-12 years) of type 1 diabetic patients also failed to find a difference in the incidence of type 1 diabetes after three years 129. A randomized, double-blind, placebo-controlled multicenter trial of nicotinamide (maximum of 3 g/day) was conducted in 552 islet cell autoantibodies (ICA)-positive relatives of patients with type 1 diabetes. The proportion of relatives who developed type 1 diabetes within five years was comparable whether they were treated with nicotinamide or placebo 130. Nicotinamide could reduce inflammation-related parameters in these high-risk subjects yet was ineffective to prevent disease onset 131. More recently, case reports of the combined use of nicotinamide (25 mg/kg/day) and acetyl-L-carnitine (50 mg/kg/day) in children at risk for type 1 diabetes showed promising results, warranting further investigation 132.
Niacin (vitamin B3) uses
Niacin is used with diet changes (restriction of cholesterol and fat intake) to reduce the amount of cholesterol (a fat-like substance) and other fatty substances in your blood (hyperlipidemia) and to increase the amount of high density lipoprotein (HDL; ”good cholesterol”). Niacin can be used in a number of situations including the following 133:
- alone or in combination with other medications, such as HMG-CoA inhibitors (statins) or bile acid-binding resins to treat high cholesterol and triglyceride (fat-like substances) levels in the blood;
- to decrease the risk of another heart attack in patients with high cholesterol who have had a heart attack;
- to prevent worsening of atherosclerosis (buildup of cholesterol and fats along the walls of the blood vessels) in patients with high cholesterol and coronary artery disease;
- to reduce the amount of triglycerides (other fatty substances) in the blood in patients with very high triglycerides who are at risk of pancreatic disease (conditions affecting the pancreas, a gland that produces fluid to break down food and hormones to control blood sugar);
- may help prevent the development of pancreatitis (inflammation of the pancreas) and other problems caused by high levels of cholesterol and triglycerides in the blood.
Niacin is also used to prevent and treat pellagra (niacin deficiency), a disease caused by inadequate niacin or tryptophan in your diet and other medical problems 133. Niacin is a B-complex vitamin. At therapeutic doses, only with your doctor’s prescription, niacin is a cholesterol-lowering medication.
Results of a clinical study in people with heart disease and well-controlled cholesterol levels that compared people who took niacin and simvastatin with people who took simvastatin alone and found similar results for the two groups in the rate of heart attacks or strokes. Taking niacin along with simvastatin or lovastatin also has not been shown to reduce the risk of heart disease or death compared with the use of niacin, simvastatin, or lovastatin alone. Talk to your doctor if you have questions about the risks and benefits of treating increased amounts of cholesterol in your blood with niacin and other medications.
Before taking niacin 133:
- tell your doctor and pharmacist if you are allergic to niacin, any other medications, or any of the ingredients in niacin tablets. Ask your pharmacist or check the manufacturer’s information for the patient for a list of the ingredients.
- tell your doctor and pharmacist what prescription and nonprescription medications, vitamins, nutritional supplements, and herbal products you are taking or plan to take. Be sure to mention any of the following: anticoagulants (‘blood thinners’) such as warfarin (Coumadin); aspirin; insulin or oral medications for diabetes; medications for high blood pressure; nutritional supplements or other products containing niacin; or other medications for lowering cholesterol or triglycerides. If you take insulin or oral diabetes medication, your dose may need to be changed because niacin may increase the amount of sugar in your blood and urine.
- if you are taking a bile acid-binding resin such as colestipol (Colestid) or cholestyramine (Questran), take it at least 4 to 6 hours before or 4 to 6 hours after niacin.
- tell your doctor if you drink large amounts of alcohol and if you have or have ever had diabetes; gout; ulcers; allergies; jaundice (yellowing of the skin or eyes); bleeding problems; or gallbladder, heart, kidney, or liver disease.
- tell your doctor if you are pregnant, plan to become pregnant, or are breast-feeding. If you become pregnant while taking niacin, stop taking niacin and call your doctor.
- if you are having surgery, including dental surgery, tell the doctor or dentist that you are taking niacin.
- ask your doctor about the safe use of alcoholic beverages while you are taking niacin. Alcohol can make the side effects from niacin worse.
- you should know that niacin causes flushing (redness, warmth, itching, tingling) of the face, neck, chest, or back. This side effect usually goes away after taking the medicine for several weeks. Avoid drinking alcohol or hot drinks or eating spicy foods around the time you take niacin. Taking aspirin or another nonsteroidal anti-inflammatory drug such as ibuprofen (Advil, Motrin) or naproxen (Aleve, Naprosyn) 30 minutes before niacin may reduce the flushing. If you take extended-release niacin at bedtime, the flushing will probably happen while you are asleep. If you wake up and feel flushed, get up slowly, especially if you feel dizzy or faint.
Niacin-responsive genetic disorders
Congenital NAD deficiency-related disorders can result from mutations in genes involved in the uptake and transport of the various dietary NAD precursors or in the distinct metabolic pathways leading to NAD production 3. Some of these disorders might respond to niacin supplementation. For example, defective transport of tryptophan into cells results in Hartnup disease, which features signs of severe niacin deficiency 134. Hartnup disease is due to mutations in the SLCA19 gene, which codes for a sodium-dependent neutral amino acid transporter expressed primarily in the kidneys and intestine. Hartnup disease interferes with the absorption of tryptophan in the small intestine and increases its loss in the urine via the kidneys 135, 6, 136. As a result, the body has less available tryptophan to convert to niacin. Hartnup disease management involves supplementation with nicotinic acid or nicotinamide 137. Recessive mutations in genes coding for enzymes of the kynurenine pathway — namely kynureninase and 3-hydroxyanthranilic-acid 3,4-dioxygenase — lead to combined vertebral, anal, cardiac, tracheo-esophageal, renal, and limb (VACTERL) congenital malformations 138. Depletion of NAD, rather than accumulation of intermediate metabolites in the kynurenine pathway, was found to be responsible for these malformations. Niacin supplementation throughout pregnancy ensured adequate levels of NAD and prevented congenital anomalies in mice with kynurenine pathway mutations 138. In humans, the dose of NAD precursors necessary to avert NAD deficiency-induced congenital VACTERL malformations has yet to be defined 139.
Nicotinamide may also rescue NAD depletion secondary to an ultra-rare inborn error of glutamine metabolism 140. Glutamine is required for the conversion of nicotinic acid adenine dinucleotide to NAD catalyzed by NAD synthetase (Figure 2). Thus, inherited glutamine synthetase deficiency specifically affects the synthesis of NAD from the NAD precursors, tryptophan and nicotinic acid. If the combined deficiencies of glutamine and NAD are responsible for the severe clinical phenotype of subjects with inherited glutamine synthetase deficiency, it is likely that supplementation with both glutamine and nicotinamide would provide some relief 140.
Finally, many inborn errors of metabolism result from genetic mutations decreasing cofactor binding affinity and, subsequently, enzyme efficiency 141: relevance to genetic disease and polymorphisms. Am J Clin Nutr. 2002 Apr;75(4):616-58. doi: 10.1093/ajcn/75.4.616)). In many cases, the administration of high doses of the vitamins serving as precursors of cofactors can restore enzymatic activity — at least partially — and lessen signs of the genetic diseases 141: relevance to genetic disease and polymorphisms. Am J Clin Nutr. 2002 Apr;75(4):616-58. doi: 10.1093/ajcn/75.4.616)). Given the large number of enzymes requiring NAD, it is speculated that many of the conditions due to defective enzymes might be rescued by niacin supplementation 38.
Niacin (vitamin B3) side effects
The niacin that food and beverages naturally contain is safe 4, 6. However, dietary supplements with 30 mg or more of nicotinic acid can make the skin on your face, arms, and chest turn reddish color because of vasodilation of small subcutaneous blood vessels 4. The flushing is accompanied by burning, tingling, and itching sensations 28, 29. These signs and symptoms are typically transient and can occur within 30 minutes of nicotinic acid intake or over days or weeks with repeated dosing; they are considered an unpleasant, rather than a toxic, side effect 4. However, the flushing can be accompanied by more serious signs and symptoms, such as headache, rash, dizziness, and/or a decrease in blood pressure. Supplement users can reduce the flushing effects by taking nicotinic acid supplements with food, slowly increasing the dose over time, or simply waiting for the body to develop a natural tolerance 4.
If you take nicotinic acid as a medication in doses of 1,000 or more mg/day, it can cause more severe side effects. These include:
- Low blood pressure (which can increase the risk of falls)
- Extreme tiredness
- High blood sugar levels
- Nausea, heartburn, and abdominal pain
- Blurred or impaired vision and fluid buildup in the eyes
Long-term treatment, especially with extended-release forms of nicotinic acid, can cause liver problems, including hepatitis and liver failure.
Niacin in the form of nicotinamide has fewer side effects than nicotinic acid. However, at high doses of 500 mg/day or more, nicotinamide can cause diarrhea, easy bruising, and can increase bleeding from wounds. Even higher doses of 3,000 mg/day or more can cause nausea, vomiting, and liver damage.
When taken in pharmacologic doses of 1,000 to 3,000 mg/day used in the therapy of hyperlipidemia, nicotinic acid can also cause more serious side effects 28, 29, 9, 6. Many of these effects have occurred in patients taking high-dose nicotinic acid supplements to treat hyperlipidemias. These adverse effects can include hypotension severe enough to increase the risk of falls; fatigue; impaired glucose tolerance and insulin resistance; gastrointestinal effects, such as nausea, heartburn, and abdominal pain; and ocular effects, such as blurred or impaired vision and macular edema (a buildup of fluid at the center of the retina). High doses of nicotinic acid taken over months or years can also cause liver injury; effects can include increased levels of liver enzymes; hepatic dysfunction resulting in fatigue, nausea, and anorexia; hepatitis; and acute liver failure 15, 6, 30, 28, 31. Liver injury is more likely to occur with the use of extended-release forms of nicotinic acid 32, 33, 28.
To minimize the risk of adverse effects from nicotinic acid supplementation or to identify them before they become serious, the American College of Cardiology and the American Heart Association recommend measuring liver transaminase (liver enzyme), fasting blood glucose or hemoglobin A1C, and uric acid levels in all supplement users before they start therapy, while the dose is being increased to a maintenance level, and every 6 months thereafter 30. The American College of Cardiology and the American Heart Association also recommend that patients not use nicotinic acid supplements or stop using them if their liver transaminase (liver enzyme) levels are more than two or three times the upper limits of normal; if they develop persistent high blood sugar level (hyperglycemia), acute gout, unexplained abdominal pain, gastrointestinal symptoms, new-onset atrial fibrillation, or weight loss; or if they have persistent and severe skin reactions, such as flushing or rashes 30.
Nicotinamide does not cause skin flushing and has fewer adverse effects than nicotinic acid, and these effects typically begin with much higher doses 28. Nausea, vomiting, and signs of liver toxicity can occur with nicotinamide intakes of 3,000 mg/day 6. In several small studies of participants undergoing hemodialysis, the most common adverse effects from 500-1,500 mg/day nicotinamide supplementation for several months were diarrhea and thrombocytopenia (low platelet count) 29, 34, 35, 36.
The Food and Nutrition Board at the National Academies of Sciences, Engineering, and Medicine has established Tolerable Upper Intake Level (maximum daily intake unlikely to cause adverse health effects) for niacin that apply only to supplemental niacin for healthy infants, children, and adults 6. The daily Tolerable Upper Intake Level for niacin from dietary supplements are listed in Table 2 above. These Tolerable Upper Intake Levels (ULs) are based on the levels associated with skin flushing. The Food and Nutrition Board acknowledges that although excess nicotinamide does not cause flushing, a Tolerable Upper Intake Level for nicotinic acid based on flushing can prevent the potential adverse effects of nicotinamide 6. The Tolerable Upper Intake Level, therefore, applies to both forms of supplemental niacin. However, the Tolerable Upper Intake Level does not apply to individuals who are receiving supplemental niacin under medical supervision 6.
Interactions with Medications
Niacin can interact with certain medications, and several types of medications might adversely affect niacin levels. A few examples are provided below. Individuals taking these and other medications on a regular basis should discuss their niacin status with their doctors.
Isoniazid and pyrazinamide
Isoniazid and pyrazinamide (together in Rifater), used to treat tuberculosis, are structural analogs of niacin and interrupt the production of niacin from tryptophan by competing with a vitamin B6-dependent enzyme required for this process 142. In addition, isoniazid can interfere with niacin’s conversion to NAD 4. Although pellagra can occur in patients with tuberculosis treated with isoniazid, it can be prevented with increased intakes of niacin.
Antidiabetes medications
Large doses of nicotinic acid can raise blood glucose levels by causing or aggravating insulin resistance and increasing hepatic production of glucose 4. Some studies have found that nicotinic acid doses of 1500 mg/day or more are most likely to increase blood glucose levels in individuals with or without diabetes 32. People who take any antidiabetes medications should have their blood glucose levels monitored if they take high-dose nicotinic acid supplements concomitantly because they might require dose adjustments 4.
Niacin deficiency
Severe niacin deficiency or tryptophan (an amino acid) deficiency leads to pellagra, a disease characterized by a pigmented rash or brown discoloration on skin exposed to sunlight; the skin also develops a roughened, sunburned-like appearance (Figure 5) 9, 6, 19, 143. In advanced stages, increased pigmentation usually leads to thin varnish-like eruptive scales 19. The characteristic skin rash has a typical photosensitive distribution with welldefined borders, and is mostly observed on the face, the neck – forming the so-called Casal’s necklace -, the dorsa of the hands and the extensor surface of the forearms 16, 17, 18. In addition to skin changes, pellagra can cause a bright red tongue (glossitis) and changes in the digestive tract that lead to vomiting, constipation, or intractable diarrhea. The neurological symptoms of pellagrous encephalopathy can include depression; apathy; headache; fatigue; loss of memory that can progress to aggressive, paranoid, and suicidal behaviors; and auditory and visual hallucinations 6, 7, 9. As pellagra progresses, anorexia develops, and the affected individual eventually dies if pellagra is left untreated 7, 17, 144.
Pellagra is uncommon in industrialized populations and is mostly limited to people living in poverty, such as refugees and displaced people who eat very limited diets low in niacin and protein 142, 143. Pellagra was common in the early 20th century among individuals living in poverty in the southern United States and parts of Europe whose limited diets consisted mainly of corn or sorghum 7, 6. Pellagra was also common in the southern United States during the early 1900s where income was low and corn products were a major dietary staple 145. Interestingly, pellagra was not known in Mexico, where corn was also an important dietary staple and much of the population was also poor. In fact, if corn contains appreciable amounts of niacin, it is present in a bound form that is not nutritionally available to humans. The traditional preparation of corn tortillas in Mexico involves soaking the corn in a lime (calcium oxide) solution, prior to cooking. Heating the corn in an alkaline solution results in the release of bound niacin, increasing its bioavailability 146. Pellagra epidemics were also unknown to Native Americans who consumed immature corn that contains predominantly unbound (bioavailable) niacin 145.
Although frank niacin deficiencies leading to pellagra are very rare in the United States, some individuals have marginal or low niacin status 136, 19, 142.
Niacin deficiency or pellagra may result from inadequate dietary intake of NAD precursors, including tryptophan. Niacin deficiency — often associated with malnutrition — is observed in the homeless population, in individuals suffering from anorexia nervosa or obesity, and in consumers of diets high in maize and poor in animal protein 147, 148, 149, 150. Deficiencies of other B vitamins and some trace minerals may aggravate niacin deficiency 151, 152.
Niacin deficiency should especially be suspected in the following conditions: i) malnutrition (homelessness, anorexia nervosa or severe comorbid conditions like end-stage malignancy or HIV); ii) malabsorption (e.g. Crohn’s or Hartnup disease); iii) chronic alcoholism; iv) hemodialysis or peritoneal dialysis; v) drugs like isoniazid, ethionamide, 6-mercaptopurine and estrogens; vi) carcinoid syndrome (due to excess turnover of tryptophan, precursor of niacin, to serotonin) 16, 17, 144.
Malabsorptive disorders that can lead to pellagra include Crohn’s disease and megaduodenum 153, 154. Patients with Hartnup’s disease, a hereditary disorder resulting in defective tryptophan absorption, have developed pellagra. Carcinoid syndrome, a condition of increased secretion of serotonin and other catecholamines by carcinoid tumors, may also result in pellagra due to increased utilization of dietary tryptophan for serotonin rather than niacin synthesis. Furthermore, prolonged treatment with the anti-tuberculosis drug isoniazid has resulted in niacin deficiency 155. Other pharmaceutical agents, including the immunosuppressive drugs azathioprine (Imuran) and 6-mercaptopurine, the anti-cancer drug 5-fluorouracil (5-FU, Adrucil), and levodopa/carbidopa (Sinemet; two drugs given to people with Parkinson’s disease), are known to increase the reliance on dietary niacin by interfering with the tryptophan-kynurenine-niacin pathway 3. Finally, other populations at risk for niacin deficiency include dialysis patients, cancer patients 156, 157, individuals suffering from chronic alcoholism 17, and people with HIV/AIDS. Furthermore, chronic alcohol intake can lead to severe niacin deficiency through reducing dietary niacin intake and interfering with the tryptophan-to-NAD conversion 152.
The World Health Organization (WHO) recommends treating pellagra with 300 mg/day nicotinamide in divided doses for 3-4 weeks along with a B-complex or yeast product to treat likely deficiencies in other B vitamins 143.
Figure 5. Skin lesions of niacin deficiency (pellagra) involving face, neck, hand and forearm (A), after treatment with niacin for 2 weeks (B)

Figure 6. Pellagra rash

Footnote: This is a classical case of pellagra. A 42 year old woman was admitted to hospital with a one month history of progressive forgetfulness, irritability and confusion. There was no history of tremor or confabulation. Reportedly, she also had fever two weeks prior to admission. There was no history of headache, neck-ache or neck stiffness. Further inquiry revealed she had developed rash around her neck and in the distal parts of all four limbs a month prior to the onset of the altered mental status. There was no history of rash involving the mucosae or of having taken any drugs in the period preceding the rash.
[Source 159 ]Figure 7. Pellagra tongue

Niacin deficiency causes
Niacin deficiency or pellagra is caused by having too little niacin or tryptophan in your diet. It can also occur if your body fails to absorb niacin or tryptophan.
Half of your body’s niacin requirement comes from dietary intake of niacin. The other half is synthesized in your body from the amino acid tryptophan. Niacin is found in many animal products (as nicotinamide) and plants (as nicotinic acid). A varied diet including milk, eggs, red meat, poultry, fish, peanuts, legumes, and seeds provides sufficient niacin and tryptophan.
Niacin deficiency or pellagra may also develop due to 161, 162:
- Gastrointestinal diseases (chronic colitis, severe ulcerative colitis and regional ileitis)
- Prolonged diarrhea
- Weight loss (bariatric) surgery
- Gastric cancer surgery
- Anorexia nervosa
- Excessive alcohol use or chronic alcoholism
- Carcinoid syndrome (group of symptoms associated with carcinoid tumors of the small intestine, colon, appendix, and bronchial tubes in the lungs)
- Certain medicines, such as isoniazid, 5-fluorouracil, 6-mercaptopurine, pyrazinamide, hydantoin, ethionamide, phenobarbital, azathioprine, and chloramphenicol
- HIV infection
- Tuberculosis of the gastrointestinal tract
- Hepatic cirrhosis
- Hartnup disease.
Pellagra is most common among poor and food-limited populations. The disease is more common in parts of the world (such as certain parts of Africa) where people have a lot of untreated corn in their diet. Corn is a poor source of tryptophan, and niacin in corn is tightly bound to other components of the grain. Niacin is released from corn if soaked in limewater overnight. This method is used to cook tortillas in Central America where pellagra is rare. Pellagra is rare in the United States and may be associated with severe alcoholism or medical causes of malnutrition.
Groups at Risk of Niacin deficiency
Niacin inadequacy usually arises from insufficient intakes of foods containing niacin and tryptophan. It can also be caused by factors that reduce the conversion of tryptophan to niacin, such as low intakes of other nutrients 6, 142. The following groups are among those most likely to have inadequate niacin status.
People with undernutrition
People who are undernourished because they live in poverty or have anorexia, alcohol use disorder, AIDS, inflammatory bowel disease, or liver cirrhosis often have inadequate intakes of niacin and other nutrients 6, 142, 136, 19.
People with inadequate riboflavin (vitamin B2), pyridoxine (vitamin B6) and/or iron intakes
People who do not consume enough riboflavin (vitamin B2), pyridoxine (vitamin B6), or iron convert less tryptophan to niacin because enzymes in the metabolic pathway for this conversion depend on these nutrients to function 6, 142.
People with Hartnup disease
Hartnup disease is a rare genetic disorder caused by mutations in the SLC6A19 gene and is inherited in an autosomal recessive manner 135. The SLC6A19 gene produces a protein known as an amino acid transporter, which serves to assist the movement (or transport) of specific amino acids within the body. The amino acid transporter protein is especially active within the kidneys and the intestines, although these organs are otherwise unaffected and function normally. The amino acids affected include tryptophan, alanine, asparagine, glutamine, histidine, isoleucine, leucine, phenylalanine, serine, threonine, tyrosine, and valine 135. Hartnup disease interferes with the absorption of tryptophan in the small intestine and increases its loss in the urine via the kidneys 135, 6, 136. As a result, the body has less available tryptophan to convert to niacin.
The symptoms of Hartnup disease vary greatly from one person to another. The majority of affected individuals do not have any apparent symptoms (asymptomatic). When symptoms do develop, they most often occur between the ages of 3-9. In rare instances, symptoms first appear in adulthood.
The most common symptom are red, scaly light-sensitive (photosensitive) rashes on the face, arms, extremities, and other exposed areas of skin.
A wide variety of neurological abnormalities can occur including sudden episodes of impaired muscle coordination (ataxia), an unsteady walk (gait), impaired articulation of speech (dysarthria), occasional tremors of the hands and tongue, and spasticity, a condition marked by increased muscle tone and stiffness of the muscles, particularly those of the legs.
There have been reports of delayed cognitive development and, in rare instances, mild intellectual disability in some children. It is, however, unclear whether these symptoms are related to Hartnup disorder or incidentally occurred in the same individual and were therefore attributed to Hartnup disorder. Similarly, seizures, fainting, trembling, lack of muscle tone (hypotonia), headaches, dizziness and/or vertigo, and delays in motor development have been observed but may be unrelated. Some affected individuals may experience psychiatric abnormalities including emotional instability such as rapid mood changes, depression, confusion, anxiety, delusions, and/or hallucinations.
Some children experience growth delays and may be shorter than would be expected based upon age and gender (short stature). In some instances, the eyes may be affected and individuals may experience double vision (diplopia), involuntary rhythmic movements of the eyes (nystagmus), and droopy upper eyelids (ptosis).
Diarrhea may precede or follow an episode of this disorder. Some adults with Hartnup disease have been reported whose initial symptom was the onset of seizures during adulthood. Heartburn has been reported in adults with the disorder.
Hartnup disease has a good prognosis with treatment and symptoms tend to improve with age.
People with carcinoid syndrome
Carcinoid syndrome is caused by slow-growing tumors in the gastrointestinal tract that release serotonin and other substances. It is characterized by facial flushing, diarrhea, and other symptoms. In those with carcinoid syndrome, tryptophan is preferentially oxidized to serotonin and not metabolized to niacin 6. As a result, the body has less available tryptophan to convert to niacin.
Niacin deficiency prevention
Pellagra can be prevented by following a well-balanced diet.
Get treated for health problems that may cause pellagra.
Niacin deficiency symptoms
Symptoms of niacin deficiency or pellagra include 21:
- Delusions or mental confusion
- Diarrhea
- Weakness
- Loss of appetite
- Pain in abdomen
- Inflamed mucous membrane
- Scaly skin sores, especially in sun-exposed areas of the skin
The most common symptoms of niacin deficiency involve the skin, the digestive system, and the nervous system 3. The symptoms of pellagra are commonly referred to as the 4 “Ds”: sun-sensitive dermatitis, diarrhea, and dementia. A fourth “D,” death, occurs if pellagra is left untreated 38. In the skin, a thick, scaly, darkly pigmented rash develops symmetrically in areas exposed to sunlight. In fact, the word “pellagra” comes from “pelle agra,” the Italian phrase for rough skin. Symptoms related to the digestive system include inflammation of the mouth and tongue (“bright red tongue”), vomiting, constipation, abdominal pain, and ultimately, diarrhea. Gastrointestinal disorders and diarrhea contribute to the ongoing malnourishment of the patients. Neurologic symptoms include headache, apathy, fatigue, depression, disorientation, and memory loss and are more consistent with delirium than with the historically described dementia 17. Disease presentations vary in appearance since the classic triad rarely presents in its entirety. The absence of dermatitis, for example, is known as pellagra sine pellagra 3.
Niacin deficiency complication
Left untreated, niacin deficiency or pellagra can result in malnutrition and cachexia (wasting of the body), nerve damage, particularly in the brain. Progression of the neuropsychiatric symptoms can lead to delusions, hallucinations, psychosis, and eventually coma and death 19. Skin sores may become infected.
Niacin deficiency diagnosis
Niacin deficiency or pellagra diagnosis is a clinical diagnosis and biochemical testing is rarely used 160. Investigations such as blood tests and skin biopsy are not diagnostic but may be used to exclude other diagnoses 163. If needed, niacin deficiency can be assessed by two methods 164, 162, 19:
- Biochemical assessment. This approach is not widely used. Measurement of urinary N-methylnicotinamide or erythrocyte NAD: NADP (ratio) can be obtained to evaluate the metabolic rate of niacin in the body. The combined urinary excretion of N methylnicotinamide and pyridone of less than 1.5 mg in 24 hours indicates severe niacin deficiency. Low urinary levels of N-methylnicotinamide and pyridone suggest niacin deficiency and support the diagnosis of pellagra.
- Low serum niacin, tryptophan, NAD, and NADP levels can reflect niacin deficiency and confirm the diagnosis of pellagra.
- Blood counts (anemia), findings of hypoproteinemia, higher levels of serum calcium and lower levels of serum kalium and phosphorus, liver function test results, and serum porphyrin levels can help in diagnosing pellagra.
- Clinical assessment. It is more widely used by assessing for diarrhea, glossitis, and dermatitis. The skin is assessed for hyperpigmentation, dryness and scaling, facial butterfly sign, and/or Casal’s collar (necklace) in sun-exposed areas. It is important to note that diarrhea and dementia may not always be present.
The rapid response to niacin supplementation usually confirms the diagnosis.
Hartnup disease is diagnosed on the detection of neutral amino acids in the urine. Molecular genetic testing can confirm a diagnosis of Hartnup disease in some cases. Molecular genetic testing can detect genetic alterations in the SLC19A6 gene known to cause the disorder, but usually is not necessary to obtain a diagnosis 135.
Niacin deficiency treatment
To treat niacin deficiency or pellagra, the World Health Organization (WHO) recommends administering nicotinamide to avoid the flushing commonly caused by nicotinic acid 143. Treatment guidelines suggest using 300 mg/day of oral nicotinamide in divided doses, or 100 mg/day administered parenterally in divided doses, for three to four weeks 157, 143, 165. Because patients with pellagra often display additional vitamin deficiencies, administration of a vitamin B-complex preparation is advised 143.
Individuals with Hartnup disease who do not develop symptoms will usually not require any treatment 135. Low protein diets (vegan or similar) may trigger symptomatic episodes, which can be reduced or avoided by maintaining good nutrition including a high protein diet, avoiding excess exposure the sun, and avoiding certain drugs such as sulphonamide drugs 135. Supplementing the diet with nicotinamide or niacin is also of benefit in preventing Hartnup disease episodes 135. In some instances, during a symptomatic episode, treatment with nicotinamide may be recommended. According to the medical literature, at least one individual showed an improvement of symptoms after treatment with the compound L-tryptophan ethyl ester, which restored tryptophan levels in both the serum and cerebrospinal fluid 135. Other treatment is symptomatic and supportive. Genetic counseling may be helpful for affected families.
Niacin deficiency prognosis
Diarrhea and glossitis are the first to improve within days usually improve in 2 to 3 days, while recovery from dementia and dermatitis is seen within 7 days of treatment 166, 167, 162. The skin changes typically resolve within two weeks. However, a longer recovery may be seen in chronic cases 168.
- Institute of Medicine (US) Standing Committee on the Scientific Evaluation of Dietary Reference Intakes and its Panel on Folate, Other B Vitamins, and Choline. Dietary Reference Intakes for Thiamin, Riboflavin, Niacin, Vitamin B6, Folate, Vitamin B12, Pantothenic Acid, Biotin, and Choline. Washington (DC): National Academies Press (US); 1998. Available from: https://www.ncbi.nlm.nih.gov/books/NBK114310/ doi: 10.17226/6015[↩]
- Trammell SA, Schmidt MS, Weidemann BJ, Redpath P, Jaksch F, Dellinger RW, Li Z, Abel ED, Migaud ME, Brenner C. Nicotinamide riboside is uniquely and orally bioavailable in mice and humans. Nat Commun. 2016 Oct 10;7:12948. doi: 10.1038/ncomms12948[↩][↩]
- Niacin. https://lpi.oregonstate.edu/mic/vitamins/niacin[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Niacin. https://ods.od.nih.gov/factsheets/Niacin-HealthProfessional[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Penberthy WT, Kirkland JB. Niacin. In: Erdman JW, Macdonald IA, Zeisel SH, eds. Present Knowledge in Nutrition, 10th ed. Washington, DC: Wiley-Blackwell; 2012:293-306.[↩][↩][↩][↩][↩]
- Institute of Medicine. Food and Nutrition Board. Dietary Reference Intakes: Thiamin, Riboflavin, Niacin, Vitamin B6, Folate, Vitamin B12, Pantothenic Acid, Biotin, and Choline. Washington, DC: National Academy Press, 1998.[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Kirkland JB. Niacin. In: Ross AC, Caballero B, Cousins RJ, Tucker KL, Ziegler TR, eds. Modern Nutrition in Health and Disease, 11th ed. Baltimore, MD: Williams & Wilkins; 2014:331-40.[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Peechakara BV, Gupta M. Vitamin B3. [Updated 2022 Jun 11]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK526107[↩][↩]
- Bourgeois C, Moss J. Niacin. In: Coates PM, Betz JM, Blackman MR, Cragg GM, Levine M, Moss J, White JD, eds. Encyclopedia of Dietary Supplements, 2nd ed. New York, NY: Informa Healthcare; 2010:562-9.[↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Nicotinic acid. http://www.hmdb.ca/metabolites/HMDB01488[↩]
- Organization for Economic Cooperation and Development; Screening Information Data Set for 3-Pyridinecarboxamide (Nicotinamide) CAS #: 98-92-0 p.40 (2002). Available from, as of February 20, 2007: http://www.inchem.org/pages/sids.html[↩]
- Nikiforov A, Kulikova V, Ziegler M. The human NAD metabolome: Functions, metabolism and compartmentalization. Crit Rev Biochem Mol Biol. 2015;50(4):284-97. doi: 10.3109/10409238.2015.1028612[↩][↩][↩][↩][↩][↩]
- Niacin. https://ods.od.nih.gov/factsheets/Niacin-Consumer[↩][↩][↩][↩][↩]
- McEvoy, G.K. (ed.). American Hospital Formulary Service. AHFS Drug Information. American Society of Health-System Pharmacists, Bethesda, MD. 2007., p. 1715[↩]
- LiverTox: Clinical and Research Information on Drug-Induced Liver Injury [Internet]. Bethesda (MD): National Institute of Diabetes and Digestive and Kidney Diseases; 2012-. Niacin. [Updated 2020 Jul 9]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK548176[↩][↩][↩][↩]
- Russel RM. Vitamin and trace mineral deficiency and excess. : Kasper DL, Braunwald E, Fauci AS, et al., Harrison’s principles of internal medicine. 16th ed New York: McGraw-Hill; 2005. pp 404-405[↩][↩][↩]
- Oldham MA, Ivkovic A. Pellagrous encephalopathy presenting as alcohol withdrawal delirium: a case series and literature review. Addict Sci Clin Pract. 2012 Jul 6;7(1):12. doi: 10.1186/1940-0640-7-12[↩][↩][↩][↩][↩][↩]
- A. MacDonald , A. Forsyth, Nutritional deficiencies and the skin, Clinical and Experimental Dermatology, Volume 30, Issue 4, 1 July 2005, Pages 388–390, https://doi.org/10.1111/j.1365-2230.2005.01787.x[↩][↩]
- Savvidou S. Pellagra: a non-eradicated old disease. Clin Pract. 2014 Apr 28;4(1):637. doi: 10.4081/cp.2014.637[↩][↩][↩][↩][↩][↩][↩]
- Coates, P.M., Blackman, M.R., Cragg, G.M., Levine, M., Moss, J., White, J.D. (Ed), Encyclopedia of Dietary Supplements. Marcel Dekker, New York, NY, p. 483 (2005[↩]
- Pellagra. https://medlineplus.gov/ency/article/000342.htm[↩][↩]
- Dart, R.C. (ed). Medical Toxicology. Third Edition, Lippincott Williams & Wilkins. Philadelphia, PA. 2004., p. 1022[↩]
- McEvoy, G.K. (ed.). American Hospital Formulary Service. AHFS Drug Information. American Society of Health-System Pharmacists, Bethesda, MD. 2007., p. 3622[↩]
- Gibson, RS. Principles of Nutritional Assessment, Second Edition. New York: Oxford University Press. Copyright 2005.[↩][↩][↩]
- Jacobson EL, Jacobson MK. Tissue NAD as a biochemical measure of niacin status in humans. Methods Enzymol. 1997;280:221-30. doi: 10.1016/s0076-6879(97)80113-9[↩]
- Shah GM, Shah RG, Veillette H, Kirkland JB, Pasieka JL, Warner RR. Biochemical assessment of niacin deficiency among carcinoid cancer patients. Am J Gastroenterol. 2005 Oct;100(10):2307-14. doi: 10.1111/j.1572-0241.2005.00268.x[↩]
- Fu CS, Swendseid ME, Jacob RA, McKee RW. Biochemical markers for assessment of niacin status in young men: levels of erythrocyte niacin coenzymes and plasma tryptophan. J Nutr. 1989 Dec;119(12):1949-55. doi: 10.1093/jn/119.12.1949[↩]
- Douglas MacKay and others, Niacin: chemical forms, bioavailability, and health effects, Nutrition Reviews, Volume 70, Issue 6, 1 June 2012, Pages 357–366, https://doi.org/10.1111/j.1753-4887.2012.00479.x[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Clara Minto and others, Definition of a tolerable upper intake level of niacin: a systematic review and meta-analysis of the dose-dependent effects of nicotinamide and nicotinic acid supplementation, Nutrition Reviews, Volume 75, Issue 6, June 2017, Pages 471–490, https://doi.org/10.1093/nutrit/nux011[↩][↩][↩][↩][↩][↩]
- Stone NJ, Robinson JG, Lichtenstein AH, Bairey Merz CN, Blum CB, Eckel RH, Goldberg AC, Gordon D, Levy D, Lloyd-Jones DM, McBride P, Schwartz JS, Shero ST, Smith SC Jr, Watson K, Wilson PW; American College of Cardiology/American Heart Association Task Force on Practice Guidelines. 2013 ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2014 Jul 1;63(25 Pt B):2889-934. doi: 10.1016/j.jacc.2013.11.002. Epub 2013 Nov 12. Erratum in: J Am Coll Cardiol. 2014 Jul 1;63(25 Pt B):3024-3025. Erratum in: J Am Coll Cardiol. 2015 Dec 22;66(24):2812.[↩][↩][↩][↩][↩][↩][↩][↩]
- McKenney JM, Proctor JD, Harris S, Chinchili VM. A Comparison of the Efficacy and Toxic Effects of Sustained- vs Immediate-Release Niacin in Hypercholesterolemic Patients. JAMA. 1994;271(9):672–677. doi:10.1001/jama.1994.03510330050033[↩][↩]
- McKenney J. New perspectives on the use of niacin in the treatment of lipid disorders. Arch Intern Med. 2004 Apr 12;164(7):697-705. doi: 10.1001/archinte.164.7.697[↩][↩][↩]
- Leung K, Quezada M, Chen Z, Kanel G, Kaplowitz N. Niacin-Induced Anicteric Microvesicular Steatotic Acute Liver Failure. Hepatol Commun. 2018 Sep 25;2(11):1293-1298. doi: 10.1002/hep4.1253[↩][↩]
- Shahbazian H, Zafar Mohtashami A, Ghorbani A, Abbaspour MR, Belladi Musavi SS, Hayati F, Lashkarara GR. Oral nicotinamide reduces serum phosphorus, increases HDL, and induces thrombocytopenia in hemodialysis patients: a double-blind randomized clinical trial. Nefrologia. 2011;31(1):58-65. doi: 10.3265/Nefrologia.pre2010.Nov.10734[↩][↩]
- Takahashi Y, Tanaka A, Nakamura T, Fukuwatari T, Shibata K, Shimada N, Ebihara I, Koide H. Nicotinamide suppresses hyperphosphatemia in hemodialysis patients. Kidney Int. 2004 Mar;65(3):1099-104. doi: 10.1111/j.1523-1755.2004.00482.x[↩][↩]
- Cheng SC, Young DO, Huang Y, Delmez JA, Coyne DW. A randomized, double-blind, placebo-controlled trial of niacinamide for reduction of phosphorus in hemodialysis patients. Clin J Am Soc Nephrol. 2008 Jul;3(4):1131-8. doi: 10.2215/CJN.04211007[↩][↩]
- McEvoy, G.K. (ed.). American Hospital Formulary Service. AHFS Drug Information. American Society of Health-System Pharmacists, Bethesda, MD. 2007., p. 1716[↩]
- Penberthy WT, Kirkland JB. Niacin. In: Erdman JW, MacDonald I, Zeisel SH, eds. Present Knowledge in Nutrition. 10th ed. Ames: International Life Sciences Institute; 2012:293-306.[↩][↩][↩]
- Agledal L, Niere M, Ziegler M. The phosphate makes a difference: cellular functions of NADP. Redox Rep. 2010;15(1):2-10. doi: 10.1179/174329210X12650506623122[↩][↩]
- Kirkland JB. Niacin. In: Ross AC, Caballero B, Cousins RJ, Tucker KL, Ziegler TR, eds. Modern Nutrition in Health and Disease. 11th ed. Baltimore: Lippincott Williams & Wilkins; 2014:331-340.[↩][↩][↩]
- Knopp RH. Drug treatment of lipid disorders. N Engl J Med. 1999 Aug 12;341(7):498-511. doi: 10.1056/NEJM199908123410707[↩]
- Graff EC, Fang H, Wanders D, Judd RL. Anti-inflammatory effects of the hydroxycarboxylic acid receptor 2. Metabolism. 2016 Feb;65(2):102-13. doi: 10.1016/j.metabol.2015.10.001[↩][↩]
- Jin FY, Kamanna VS, Kashyap ML. Niacin accelerates intracellular ApoB degradation by inhibiting triacylglycerol synthesis in human hepatoblastoma (HepG2) cells. Arterioscler Thromb Vasc Biol. 1999 Apr;19(4):1051-9. doi: 10.1161/01.atv.19.4.1051[↩]
- Kamanna VS, Ganji SH, Kashyap ML. Recent advances in niacin and lipid metabolism. Curr Opin Lipidol. 2013 Jun;24(3):239-45. doi: 10.1097/MOL.0b013e3283613a68[↩]
- CARLSON LA. Studies on the effect of nicotinic acid on catecholamine stimulated lipolysis in adipose tissue in vitro. Acta Med Scand. 1963 Jun;173:719-22. doi: 10.1111/j.0954-6820.1963.tb17457.x[↩]
- Lauring B, Taggart AK, Tata JR, Dunbar R, Caro L, Cheng K, Chin J, Colletti SL, Cote J, Khalilieh S, Liu J, Luo WL, Maclean AA, Peterson LB, Polis AB, Sirah W, Wu TJ, Liu X, Jin L, Wu K, Boatman PD, Semple G, Behan DP, Connolly DT, Lai E, Wagner JA, Wright SD, Cuffie C, Mitchel YB, Rader DJ, Paolini JF, Waters MG, Plump A. Niacin lipid efficacy is independent of both the niacin receptor GPR109A and free fatty acid suppression. Sci Transl Med. 2012 Aug 22;4(148):148ra115. doi: 10.1126/scitranslmed.3003877[↩]
- Fliegert R, Bauche A, Wolf Pérez AM, Watt JM, Rozewitz MD, Winzer R, Janus M, Gu F, Rosche A, Harneit A, Flato M, Moreau C, Kirchberger T, Wolters V, Potter BVL, Guse AH. 2′-Deoxyadenosine 5′-diphosphoribose is an endogenous TRPM2 superagonist. Nat Chem Biol. 2017 Sep;13(9):1036-1044. doi: 10.1038/nchembio.2415[↩]
- Mutafova-Yambolieva VN, Hwang SJ, Hao X, Chen H, Zhu MX, Wood JD, Ward SM, Sanders KM. Beta-nicotinamide adenine dinucleotide is an inhibitory neurotransmitter in visceral smooth muscle. Proc Natl Acad Sci U S A. 2007 Oct 9;104(41):16359-64. doi: 10.1073/pnas.0705510104[↩]
- Moreschi I, Bruzzone S, Nicholas RA, Fruscione F, Sturla L, Benvenuto F, Usai C, Meis S, Kassack MU, Zocchi E, De Flora A. Extracellular NAD+ is an agonist of the human P2Y11 purinergic receptor in human granulocytes. J Biol Chem. 2006 Oct 20;281(42):31419-29. doi: 10.1074/jbc.M606625200[↩]
- Klein C, Grahnert A, Abdelrahman A, Müller CE, Hauschildt S. Extracellular NAD(+) induces a rise in [Ca(2+)](i) in activated human monocytes via engagement of P2Y(1) and P2Y(11) receptors. Cell Calcium. 2009 Oct;46(4):263-72. doi: 10.1016/j.ceca.2009.08.004[↩]
- Huang C, Hu J, Subedi KP, Lin AH, Paudel O, Ran P, Sham JS. Extracellular Adenosine Diphosphate Ribose Mobilizes Intracellular Ca2+ via Purinergic-Dependent Ca2+ Pathways in Rat Pulmonary Artery Smooth Muscle Cells. Cell Physiol Biochem. 2015;37(5):2043-59. doi: 10.1159/000438564[↩]
- Moreschi I, Bruzzone S, Bodrato N, Usai C, Guida L, Nicholas RA, Kassack MU, Zocchi E, De Flora A. NAADP+ is an agonist of the human P2Y11 purinergic receptor. Cell Calcium. 2008 Apr;43(4):344-55. doi: 10.1016/j.ceca.2007.06.006[↩]
- Hwang ES, Song SB. Nicotinamide is an inhibitor of SIRT1 in vitro, but can be a stimulator in cells. Cell Mol Life Sci. 2017 Sep;74(18):3347-3362. doi: 10.1007/s00018-017-2527-8[↩]
- Morris BJ. Seven sirtuins for seven deadly diseases of aging. Free Radic Biol Med. 2013 Mar;56:133-71. doi: 10.1016/j.freeradbiomed.2012.10.525[↩]
- Hottiger MO, Hassa PO, Lüscher B, Schüler H, Koch-Nolte F. Toward a unified nomenclature for mammalian ADP-ribosyltransferases. Trends Biochem Sci. 2010 Apr;35(4):208-19. doi: 10.1016/j.tibs.2009.12.003[↩]
- Liu C, Yu X. ADP-ribosyltransferases and poly ADP-ribosylation. Curr Protein Pept Sci. 2015;16(6):491-501. doi: 10.2174/1389203716666150504122435[↩][↩]
- Food Surveys Research Group: Beltsville, MD. https://www.ars.usda.gov/northeast-area/beltsville-md-bhnrc/beltsville-human-nutrition-research-center/food-surveys-research-group/docs/wweia-data-tables/[↩][↩]
- Blumberg JB, Frei BB, Fulgoni VL, Weaver CM, Zeisel SH. Impact of Frequency of Multi-Vitamin/Multi-Mineral Supplement Intake on Nutritional Adequacy and Nutrient Deficiencies in U.S. Adults. Nutrients. 2017 Aug 9;9(8):849. doi: 10.3390/nu9080849[↩]
- Blumberg JB, Frei B, Fulgoni VL III, Weaver CM, Zeisel SH. Contribution of Dietary Supplements to Nutritional Adequacy in Race/Ethnic Population Subgroups in the United States. Nutrients. 2017 Nov 28;9(12):1295. doi: 10.3390/nu9121295[↩]
- Fulgoni VL 3rd, Keast DR, Bailey RL, Dwyer J. Foods, fortificants, and supplements: Where do Americans get their nutrients? J Nutr. 2011 Oct;141(10):1847-54. doi: 10.3945/jn.111.142257[↩]
- Food Labeling: Revision of the Nutrition and Supplement Facts Labels. https://www.federalregister.gov/documents/2016/05/27/2016-11867/food-labeling-revision-of-the-nutrition-and-supplement-facts-labels[↩]
- Keenan JM. Wax-matrix extended-release niacin vs inositol hexanicotinate: a comparison of wax-matrix, extended-release niacin to inositol hexanicotinate “no-flush” niacin in persons with mild to moderate dyslipidemia. J Clin Lipidol. 2013 Jan-Feb;7(1):14-23. doi: 10.1016/j.jacl.2012.10.004[↩]
- Norris, R.B. (2006), “Flush-Free Niacin”: Dietary Supplement May Be “Benefit-Free”. Preventive Cardiology, 9: 64-65. https://doi.org/10.1111/j.1520-037X.2006.04736.x[↩]
- B-Nicotinamide Mononucleotide (NMN) from Inner Mongolia Kingdomway Pharmaceutical Limited. https://www.regulations.gov/document/FDA-2022-S-0023-0051[↩]
- Schandelmaier S, Briel M, Saccilotto R, Olu KK, Arpagaus A, Hemkens LG, Nordmann AJ. Niacin for primary and secondary prevention of cardiovascular events. Cochrane Database Syst Rev. 2017 Jun 14;6(6):CD009744. doi: 10.1002/14651858.CD009744.pub2[↩][↩][↩]
- Clofibrate and Niacin in Coronary Heart Disease. JAMA. 1975;231(4):360–381. doi:10.1001/jama.1975.03240160024021[↩][↩][↩]
- Berge KG, Canner PL. Coronary drug project: experience with niacin. Coronary Drug Project Research Group. Eur J Clin Pharmacol. 1991;40 Suppl 1:S49-51.[↩]
- Canner PL, Berge KG, Wenger NK, Stamler J, Friedman L, Prineas RJ, Friedewald W. Fifteen year mortality in Coronary Drug Project patients: long-term benefit with niacin. J Am Coll Cardiol. 1986 Dec;8(6):1245-55. doi: 10.1016/s0735-1097(86)80293-5[↩]
- HPS2-THRIVE Collaborative Group; Landray MJ, Haynes R, Hopewell JC, Parish S, Aung T, Tomson J, Wallendszus K, Craig M, Jiang L, Collins R, Armitage J. Effects of extended-release niacin with laropiprant in high-risk patients. N Engl J Med. 2014 Jul 17;371(3):203-12. doi: 10.1056/NEJMoa1300955[↩][↩]
- Lloyd-Jones DM. Niacin and HDL cholesterol–time to face facts. N Engl J Med. 2014 Jul 17;371(3):271-3. doi: 10.1056/NEJMe1406410[↩][↩]
- AIM-HIGH Investigators; Boden WE, Probstfield JL, Anderson T, Chaitman BR, Desvignes-Nickens P, Koprowicz K, McBride R, Teo K, Weintraub W. Niacin in patients with low HDL cholesterol levels receiving intensive statin therapy. N Engl J Med. 2011 Dec 15;365(24):2255-67. doi: 10.1056/NEJMoa1107579 Erratum in: N Engl J Med. 2012 Jul 12;367(2):189.[↩]
- Garg A, Sharma A, Krishnamoorthy P, Garg J, Virmani D, Sharma T, Stefanini G, Kostis JB, Mukherjee D, Sikorskaya E. Role of Niacin in Current Clinical Practice: A Systematic Review. Am J Med. 2017 Feb;130(2):173-187. doi: 10.1016/j.amjmed.2016.07.038[↩][↩][↩]
- Jenkins DJA, Spence JD, Giovannucci EL, Kim YI, Josse R, Vieth R, Blanco Mejia S, Viguiliouk E, Nishi S, Sahye-Pudaruth S, Paquette M, Patel D, Mitchell S, Kavanagh M, Tsirakis T, Bachiri L, Maran A, Umatheva N, McKay T, Trinidad G, Bernstein D, Chowdhury A, Correa-Betanzo J, Del Principe G, Hajizadeh A, Jayaraman R, Jenkins A, Jenkins W, Kalaichandran R, Kirupaharan G, Manisekaran P, Qutta T, Shahid R, Silver A, Villegas C, White J, Kendall CWC, Pichika SC, Sievenpiper JL. Supplemental Vitamins and Minerals for CVD Prevention and Treatment. J Am Coll Cardiol. 2018 Jun 5;71(22):2570-2584. doi: 10.1016/j.jacc.2018.04.020[↩]
- Grundy SM, Stone NJ, Bailey AL, Beam C, Birtcher KK, Blumenthal RS, Braun LT, de Ferranti S, Faiella-Tommasino J, Forman DE, Goldberg R, Heidenreich PA, Hlatky MA, Jones DW, Lloyd-Jones D, Lopez-Pajares N, Ndumele CE, Orringer CE, Peralta CA, Saseen JJ, Smith SC Jr, Sperling L, Virani SS, Yeboah J. 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA Guideline on the Management of Blood Cholesterol: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol. 2019 Jun 25;73(24):e285-e350. doi: 10.1016/j.jacc.2018.11.003. Epub 2018 Nov 10. Erratum in: J Am Coll Cardiol. 2019 Jun 25;73(24):3237-3241.[↩]
- Bürk K. Friedreich Ataxia: current status and future prospects. Cerebellum Ataxias. 2017 Apr 7;4:4. doi: 10.1186/s40673-017-0062-x[↩][↩]
- Ping K. Chan and others, Heterochromatinization induced by GAA-repeat hyperexpansion in Friedreich’s ataxia can be reduced upon HDAC inhibition by vitamin B3, Human Molecular Genetics, Volume 22, Issue 13, 1 July 2013, Pages 2662–2675, https://doi.org/10.1093/hmg/ddt115[↩][↩]
- Libri V, Yandim C, Athanasopoulos S, Loyse N, Natisvili T, Law PP, Chan PK, Mohammad T, Mauri M, Tam KT, Leiper J, Piper S, Ramesh A, Parkinson MH, Huson L, Giunti P, Festenstein R. Epigenetic and neurological effects and safety of high-dose nicotinamide in patients with Friedreich’s ataxia: an exploratory, open-label, dose-escalation study. Lancet. 2014 Aug 9;384(9942):504-13. doi: 10.1016/S0140-6736(14)60382-2[↩][↩]
- Lynch DR, Fischbeck KH. Nicotinamide in Friedreich’s ataxia: useful or not? Lancet. 2014 Aug 9;384(9942):474-5. doi: 10.1016/S0140-6736(14)60573-0[↩]
- Murray MF. Tryptophan depletion and HIV infection: a metabolic link to pathogenesis. Lancet Infect Dis. 2003 Oct;3(10):644-52. doi: 10.1016/s1473-3099(03)00773-4[↩]
- Taylor EW. The oxidative stress-induced niacin sink (OSINS) model for HIV pathogenesis. Toxicology. 2010 Nov 28;278(1):124-30. doi: 10.1016/j.tox.2009.10.018[↩][↩]
- Favre D, Mold J, Hunt PW, Kanwar B, Loke P, Seu L, Barbour JD, Lowe MM, Jayawardene A, Aweeka F, Huang Y, Douek DC, Brenchley JM, Martin JN, Hecht FM, Deeks SG, McCune JM. Tryptophan catabolism by indoleamine 2,3-dioxygenase 1 alters the balance of TH17 to regulatory T cells in HIV disease. Sci Transl Med. 2010 May 19;2(32):32ra36. doi: 10.1126/scitranslmed.3000632[↩][↩]
- Jenabian MA, Patel M, Kema I, Kanagaratham C, Radzioch D, Thébault P, Lapointe R, Tremblay C, Gilmore N, Ancuta P, Routy JP. Distinct tryptophan catabolism and Th17/Treg balance in HIV progressors and elite controllers. PLoS One. 2013 Oct 16;8(10):e78146. doi: 10.1371/journal.pone.0078146. Erratum in: PLoS One. 2014;9(1). doi:10.1371/annotation/11698dd2-0bc1-4fe0-ad92-b161b5594e81[↩]
- Chen J, Shao J, Cai R, Shen Y, Zhang R, Liu L, Qi T, Lu H. Anti-retroviral therapy decreases but does not normalize indoleamine 2,3-dioxygenase activity in HIV-infected patients. PLoS One. 2014 Jul 1;9(7):e100446. doi: 10.1371/journal.pone.0100446[↩]
- Dunham RM, Gordon SN, Vaccari M, Piatak M, Huang Y, Deeks SG, Lifson J, Franchini G, McCune JM. Preclinical evaluation of HIV eradication strategies in the simian immunodeficiency virus-infected rhesus macaque: a pilot study testing inhibition of indoleamine 2,3-dioxygenase. AIDS Res Hum Retroviruses. 2013 Feb;29(2):207-14. doi: 10.1089/AID.2012.0162[↩]
- Souza SA, Chow DC, Walsh EJ, Ford S 3rd, Shikuma C. Pilot study on the safety and tolerability of extended release niacin for HIV-infected patients with hypertriglyceridemia. Hawaii Med J. 2010 May;69(5):122-5. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3111654[↩]
- Dubé MP, Lipshultz SE, Fichtenbaum CJ, Greenberg R, Schecter AD, Fisher SD; Working Group 3. Effects of HIV infection and antiretroviral therapy on the heart and vasculature. Circulation. 2008 Jul 8;118(2):e36-40. doi: 10.1161/CIRCULATIONAHA.107.189625[↩]
- Carr A, Samaras K, Burton S, Law M, Freund J, Chisholm DJ, Cooper DA. A syndrome of peripheral lipodystrophy, hyperlipidaemia and insulin resistance in patients receiving HIV protease inhibitors. AIDS. 1998 May 7;12(7):F51-8. doi: 10.1097/00002030-199807000-00003[↩]
- Giannarelli C, Klein RS, Badimon JJ. Cardiovascular implications of HIV-induced dyslipidemia. Atherosclerosis. 2011 Dec;219(2):384-9. doi: 10.1016/j.atherosclerosis.2011.06.003[↩]
- Chow DC, Stein JH, Seto TB, Mitchell C, Sriratanaviriyakul N, Grandinetti A, Gerschenson M, Shiramizu B, Souza S, Shikuma C. Short-term effects of extended-release niacin on endothelial function in HIV-infected patients on stable antiretroviral therapy. AIDS. 2010 Apr 24;24(7):1019-23. doi: 10.1097/QAD.0b013e3283383016[↩]
- Balasubramanyam A, Coraza I, Smith EO, Scott LW, Patel P, Iyer D, Taylor AA, Giordano TP, Sekhar RV, Clark P, Cuevas-Sanchez E, Kamble S, Ballantyne CM, Pownall HJ. Combination of niacin and fenofibrate with lifestyle changes improves dyslipidemia and hypoadiponectinemia in HIV patients on antiretroviral therapy: results of “heart positive,” a randomized, controlled trial. J Clin Endocrinol Metab. 2011 Jul;96(7):2236-47. doi: 10.1210/jc.2010-306[↩]
- Dubé MP, Komarow L, Fichtenbaum CJ, Cadden JJ, Overton ET, Hodis HN, Currier JS, Stein JH; AIDS Clinical Trials Group A5293 Study Team. Extended-Release Niacin Versus Fenofibrate in HIV-Infected Participants With Low High-Density Lipoprotein Cholesterol: Effects on Endothelial Function, Lipoproteins, and Inflammation. Clin Infect Dis. 2015 Sep 1;61(5):840-9. doi: 10.1093/cid/civ385[↩]
- Hoffer LJ. Vitamin therapy in schizophrenia. Isr J Psychiatry Relat Sci. 2008;45(1):3-10.[↩]
- Pauling L. Orthomolecular psychiatry. Varying the concentrations of substances normally present in the human body may control mental disease. Science. 1968 Apr 19;160(3825):265-71. doi: 10.1126/science.160.3825.265[↩]
- Seybolt SE. Is it time to reassess alpha lipoic acid and niacinamide therapy in schizophrenia? Med Hypotheses. 2010 Dec;75(6):572-5. doi: 10.1016/j.mehy.2010.07.034[↩]
- Zell M, Grundmann O. An orthomolecular approach to the prevention and treatment of psychiatric disorders. Adv Mind Body Med. 2012 Fall;26(2):14-28.[↩]
- Yao JK, Dougherty GG Jr, Gautier CH, Haas GL, Condray R, Kasckow JW, Kisslinger BL, Gurklis JA, Messamore E. Prevalence and Specificity of the Abnormal Niacin Response: A Potential Endophenotype Marker in Schizophrenia. Schizophr Bull. 2016 Mar;42(2):369-76. doi: 10.1093/schbul/sbv130[↩]
- Sun L, Yang X, Jiang J, Hu X, Qing Y, Wang D, Yang T, Yang C, Zhang J, Yang P, Wang P, Cai C, Wang J, He L, Wan C. Identification of the Niacin-Blunted Subgroup of Schizophrenia Patients from Mood Disorders and Healthy Individuals in Chinese Population. Schizophr Bull. 2018 Jun 6;44(4):896-907. doi: 10.1093/schbul/sbx150[↩]
- Messamore E. Niacin subsensitivity is associated with functional impairment in schizophrenia. Schizophr Res. 2012 May;137(1-3):180-4. doi: 10.1016/j.schres.2012.03.00[↩]
- Horrobin DF. The membrane phospholipid hypothesis as a biochemical basis for the neurodevelopmental concept of schizophrenia. Schizophr Res. 1998 Apr 10;30(3):193-208. doi: 10.1016/s0920-9964(97)00151-5[↩]
- Messamore E. The niacin response biomarker as a schizophrenia endophenotype: A status update. Prostaglandins Leukot Essent Fatty Acids. 2018 Sep;136:95-97. doi: 10.1016/j.plefa.2017.06.014[↩]
- Negrini S, Gorgoulis VG, Halazonetis TD. Genomic instability–an evolving hallmark of cancer. Nat Rev Mol Cell Biol. 2010 Mar;11(3):220-8. doi: 10.1038/nrm2858[↩]
- Kirkland JB. Niacin requirements for genomic stability. Mutat Res. 2012 May 1;733(1-2):14-20. doi: 10.1016/j.mrfmmm.2011.11.008[↩]
- Bürkle A. Poly(ADP-ribose). The most elaborate metabolite of NAD+. FEBS J. 2005 Sep;272(18):4576-89. doi: 10.1111/j.1742-4658.2005.04864.x[↩]
- Jacobson EL, Shieh WM, Huang AC. Mapping the role of NAD metabolism in prevention and treatment of carcinogenesis. Mol Cell Biochem. 1999 Mar;193(1-2):69-74.[↩]
- Spronck JC, Nickerson JL, Kirkland JB. Niacin deficiency alters p53 expression and impairs etoposide-induced cell cycle arrest and apoptosis in rat bone marrow cells. Nutr Cancer. 2007;57(1):88-99. doi: 10.1080/01635580701268337[↩]
- Spronck JC, Kirkland JB. Niacin deficiency increases spontaneous and etoposide-induced chromosomal instability in rat bone marrow cells in vivo. Mutat Res. 2002 Oct 31;508(1-2):83-97. doi: 10.1016/s0027-5107(02)00188-4[↩]
- Kostecki LM, Thomas M, Linford G, Lizotte M, Toxopeus L, Bartleman AP, Kirkland JB. Niacin deficiency delays DNA excision repair and increases spontaneous and nitrosourea-induced chromosomal instability in rat bone marrow. Mutat Res. 2007 Dec 1;625(1-2):50-61. doi: 10.1016/j.mrfmmm.2007.05.008[↩]
- Dantzer F, Santoro R. The expanding role of PARPs in the establishment and maintenance of heterochromatin. FEBS J. 2013 Aug;280(15):3508-18. doi: 10.1111/febs.12368[↩]
- El Ramy R, Magroun N, Messadecq N, Gauthier LR, Boussin FD, Kolthur-Seetharam U, Schreiber V, McBurney MW, Sassone-Corsi P, Dantzer F. Functional interplay between Parp-1 and SirT1 in genome integrity and chromatin-based processes. Cell Mol Life Sci. 2009 Oct;66(19):3219-34. doi: 10.1007/s00018-009-0105-4[↩]
- Boyonoski AC, Spronck JC, Gallacher LM, Jacobs RM, Shah GM, Poirier GG, Kirkland JB. Niacin deficiency decreases bone marrow poly(ADP-ribose) and the latency of ethylnitrosourea-induced carcinogenesis in rats. J Nutr. 2002 Jan;132(1):108-14. doi: 10.1093/jn/132.1.108[↩]
- Boyonoski AC, Spronck JC, Jacobs RM, Shah GM, Poirier GG, Kirkland JB. Pharmacological intakes of niacin increase bone marrow poly(ADP-ribose) and the latency of ethylnitrosourea-induced carcinogenesis in rats. J Nutr. 2002 Jan;132(1):115-20. doi: 10.1093/jn/132.1.115[↩]
- Weitberg AB. Effect of nicotinic acid supplementation in vivo on oxygen radical-induced genetic damage in human lymphocytes. Mutat Res. 1989 Aug;216(4):197-201. doi: 10.1016/0165-1161(89)90005-8[↩]
- Hageman GJ, Stierum RH, van Herwijnen MH, van der Veer MS, Kleinjans JC. Nicotinic acid supplementation: effects on niacin status, cytogenetic damage, and poly(ADP-ribosylation) in lymphocytes of smokers. Nutr Cancer. 1998;32(2):113-20. doi: 10.1080/01635589809514728[↩]
- Yong LC, Petersen MR. High dietary niacin intake is associated with decreased chromosome translocation frequency in airline pilots. Br J Nutr. 2011 Feb;105(4):496-505. doi: 10.1017/S000711451000379X[↩]
- Weidele K, Beneke S, Bürkle A. The NAD+ precursor nicotinic acid improves genomic integrity in human peripheral blood mononuclear cells after X-irradiation. DNA Repair (Amst). 2017 Apr;52:12-23. doi: 10.1016/j.dnarep.2017.02.001[↩]
- Jacobson EL. Niacin deficiency and cancer in women. J Am Coll Nutr. 1993 Aug;12(4):412-6. doi: 10.1080/07315724.1993.10718330[↩]
- Negri, E., Franceschi, S., Bosetti, C., Levi, F., Conti, E., Parpinel, M. and La Vecchia, C. (2000), Selected micronutrients and oral and pharyngeal cancer. Int. J. Cancer, 86: 122-127. https://doi.org/10.1002/(SICI)1097-0215(20000401)86:1<122::AID-IJC19>3.0.CO;2-2[↩]
- Franceschi, S., Bidoli, E., Negri, E., Zambon, P., Talamini, R., Ruol, A., Parpinel, M., Levi, F., Simonato, L. and La Vecchia, C. (2000), Role of macronutrients, vitamins and minerals in the aetiology of squamous-cell carcinoma of the oesophagus. Int. J. Cancer, 86: 626-631. https://doi.org/10.1002/(SICI)1097-0215(20000601)86:5<626::AID-IJC4>3.0.CO;2-Y[↩]
- Gensler HL, Williams T, Huang AC, Jacobson EL. Oral niacin prevents photocarcinogenesis and photoimmunosuppression in mice. Nutr Cancer. 1999;34(1):36-41. doi: 10.1207/S15327914NC340105[↩]
- Jacobson EL, Kim H, Kim M, Williams JD, Coyle DL, Coyle WR, Grove G, Rizer RL, Stratton MS, Jacobson MK. A topical lipophilic niacin derivative increases NAD, epidermal differentiation and barrier function in photodamaged skin. Exp Dermatol. 2007 Jun;16(6):490-9. doi: 10.1111/j.1600-0625.2007.00553.x[↩]
- Bermudez Y, Benavente CA, Meyer RG, Coyle WR, Jacobson MK, Jacobson EL. Nicotinic acid receptor abnormalities in human skin cancer: implications for a role in epidermal differentiation. PLoS One. 2011;6(5):e20487. doi: 10.1371/journal.pone.0020487[↩]
- Benavente CA, Jacobson EL. Niacin restriction upregulates NADPH oxidase and reactive oxygen species (ROS) in human keratinocytes. Free Radic Biol Med. 2008 Feb 15;44(4):527-37. doi: 10.1016/j.freeradbiomed.2007.10.006[↩]
- Benavente CA, Schnell SA, Jacobson EL. Effects of niacin restriction on sirtuin and PARP responses to photodamage in human skin. PLoS One. 2012;7(7):e42276. doi: 10.1371/journal.pone.0042276[↩]
- Park SM, Li T, Wu S, Li WQ, Weinstock M, Qureshi AA, Cho E. Niacin intake and risk of skin cancer in US women and men. Int J Cancer. 2017 May 1;140(9):2023-2031. doi: 10.1002/ijc.30630[↩]
- Chen AC, Martin AJ, Choy B, Fernández-Peñas P, Dalziell RA, McKenzie CA, Scolyer RA, Dhillon HM, Vardy JL, Kricker A, St George G, Chinniah N, Halliday GM, Damian DL. A Phase 3 Randomized Trial of Nicotinamide for Skin-Cancer Chemoprevention. N Engl J Med. 2015 Oct 22;373(17):1618-26. doi: 10.1056/NEJMoa1506197[↩][↩]
- Minocha R, Damian DL, Halliday GM. Melanoma and nonmelanoma skin cancer chemoprevention: A role for nicotinamide? Photodermatol Photoimmunol Photomed. 2018 Jan;34(1):5-12. doi: 10.1111/phpp.12328[↩]
- Orban T, Sosenko JM, Cuthbertson D, Krischer JP, Skyler JS, Jackson R, Yu L, Palmer JP, Schatz D, Eisenbarth G; Diabetes Prevention Trial-Type 1 Study Group. Pancreatic islet autoantibodies as predictors of type 1 diabetes in the Diabetes Prevention Trial-Type 1. Diabetes Care. 2009 Dec;32(12):2269-74. doi: 10.2337/dc09-0934[↩]
- Szkudelski T. Streptozotocin-nicotinamide-induced diabetes in the rat. Characteristics of the experimental model. Exp Biol Med (Maywood). 2012 May;237(5):481-90. doi: 10.1258/ebm.2012.011372[↩]
- Lampeter EF, Klinghammer A, Scherbaum WA, Heinze E, Haastert B, Giani G, Kolb H. The Deutsche Nicotinamide Intervention Study: an attempt to prevent type 1 diabetes. DENIS Group. Diabetes. 1998 Jun;47(6):980-4. doi: 10.2337/diabetes.47.6.980[↩][↩]
- Gale EA, Bingley PJ, Emmett CL, Collier T; European Nicotinamide Diabetes Intervention Trial (ENDIT) Group. European Nicotinamide Diabetes Intervention Trial (ENDIT): a randomised controlled trial of intervention before the onset of type 1 diabetes. Lancet. 2004 Mar 20;363(9413):925-31. doi: 10.1016/S0140-6736(04)15786-3[↩]
- Hedman M, Ludvigsson J, Faresjö MK. Nicotinamide reduces high secretion of IFN-gamma in high-risk relatives even though it does not prevent type 1 diabetes. J Interferon Cytokine Res. 2006 Apr;26(4):207-13. doi: 10.1089/jir.2006.26.207[↩]
- Fernandez IC, Del Carmen Camberos M, Passicot GA, Martucci LC, Cresto JC. Children at risk of diabetes type 1. Treatment with acetyl-L-carnitine plus nicotinamide – case reports. J Pediatr Endocrinol Metab. 2013;26(3-4):347-55. doi: 10.1515/jpem-2012-0128[↩]
- Niacin. https://medlineplus.gov/druginfo/meds/a682518.html[↩][↩][↩]
- Patel AB, Prabhu AS. Hartnup disease. Indian J Dermatol. 2008 Jan;53(1):31-2. doi: 10.4103/0019-5154.39740[↩]
- Hartnup Disease. https://rarediseases.org/rare-diseases/hartnup-disease[↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Crook MA. The importance of recognizing pellagra (niacin deficiency) as it still occurs. Nutrition. 2014 Jun;30(6):729-30. doi: 10.1016/j.nut.2014.03.004[↩][↩][↩][↩]
- A. OAKLEY , J. WALLACE, Hartnup disease presenting in an adult, Clinical and Experimental Dermatology, Volume 19, Issue 5, 1 September 1994, Pages 407–408, https://doi.org/10.1111/j.1365-2230.1994.tb02694.x[↩]
- Shi H, Enriquez A, Rapadas M, Martin EMMA, Wang R, Moreau J, Lim CK, Szot JO, Ip E, Hughes JN, Sugimoto K, Humphreys DT, McInerney-Leo AM, Leo PJ, Maghzal GJ, Halliday J, Smith J, Colley A, Mark PR, Collins F, Sillence DO, Winlaw DS, Ho JWK, Guillemin GJ, Brown MA, Kikuchi K, Thomas PQ, Stocker R, Giannoulatou E, Chapman G, Duncan EL, Sparrow DB, Dunwoodie SL. NAD Deficiency, Congenital Malformations, and Niacin Supplementation. N Engl J Med. 2017 Aug 10;377(6):544-552. doi: 10.1056/NEJMoa1616361[↩][↩]
- Vander Heiden MG. Metabolism and Congenital Malformations – NAD’s Effects on Development. N Engl J Med. 2017 Aug 10;377(6):509-511. doi: 10.1056/NEJMp1707487[↩]
- Hu L, Ibrahim K, Stucki M, Frapolli M, Shahbeck N, Chaudhry FA, Görg B, Häussinger D, Penberthy WT, Ben-Omran T, Häberle J. Secondary NAD+ deficiency in the inherited defect of glutamine synthetase. J Inherit Metab Dis. 2015 Nov;38(6):1075-83. doi: 10.1007/s10545-015-9846-4[↩][↩]
- Ames BN, Elson-Schwab I, Silver EA. High-dose vitamin therapy stimulates variant enzymes with decreased coenzyme binding affinity (increased K(m[↩][↩]
- Li, R., Yu, K., Wang, Q., Wang, L., Mao, J. and Qian, J. (2016), Pellagra Secondary to Medication and Alcoholism. Nutrition in Clinical Practice, 31: 785-789. https://doi.org/10.1177/0884533616660991[↩][↩][↩][↩][↩][↩]
- Pellagra and its prevention and control in major emergencies. https://apps.who.int/iris/rest/bitstreams/63163/retrieve[↩][↩][↩][↩][↩][↩]
- Pipili C, Cholongitas E, Ioannidou D. The diagnostic importance of photosensitivity dermatoses in chronic alcoholism: report of two cases. Dermatol Online J. 2008 Nov 15;14(11):15.[↩][↩]
- Kirkland JB. Niacin. In: Zempleni J, Suttie JW, Gregory III JF, Stover PJ, eds. Handbook of Vitamins. 5th ed. Boca Raton: CRC Press; 2013:149-190.[↩][↩]
- Gregory JF 3rd. Nutritional Properties and significance of vitamin glycosides. Annu Rev Nutr. 1998;18:277-96. doi: 10.1146/annurev.nutr.18.1.277[↩]
- Jagielska G, Tomaszewicz-Libudzic EC, Brzozowska A. Pellagra: a rare complication of anorexia nervosa. Eur Child Adolesc Psychiatry. 2007 Oct;16(7):417-20. doi: 10.1007/s00787-007-0613-4[↩]
- Dawson, B., Favaloro, E.J., Taylor, J. and Aggarwal, A. (2006), Unrecognized pellagra masquerading as odynophagia. Internal Medicine Journal, 36: 472-474. https://doi.org/10.1111/j.1445-5994.2006.01108.x[↩]
- Kertesz SG. Pellagra in 2 homeless men. Mayo Clin Proc. 2001 Mar;76(3):315-8. doi: 10.4065/76.3.315[↩]
- Prakash R, Gandotra S, Singh LK, Das B, Lakra A. Rapid resolution of delusional parasitosis in pellagra with niacin augmentation therapy. Gen Hosp Psychiatry. 2008 Nov-Dec;30(6):581-4. doi: 10.1016/j.genhosppsych.2008.04.011[↩]
- Majewski M, Kozlowska A, Thoene M, Lepiarczyk E, Grzegorzewski WJ. Overview of the role of vitamins and minerals on the kynurenine pathway in health and disease. J Physiol Pharmacol. 2016 Feb;67(1):3-19.[↩]
- Abdulla A.-B. Badawy, Pellagra and Alcoholism: A Biochemical Perspective, Alcohol and Alcoholism, Volume 49, Issue 3, May/June 2014, Pages 238–250, https://doi.org/10.1093/alcalc/agu010[↩][↩]
- Rosmaninho A, Sanches M, Fernandes IC, Pinto-Almeida T, Vilaça S, Oliveira A, Selores M. Letter: Pellagra as the initial presentation of Crohn disease. Dermatol Online J. 2012 Apr 15;18(4):12.[↩]
- Zaraa, I., Belghith, I., EI Euch, D., Karoui, S., Mokni, M., Fillali, A. and Ben Osman, A. (2013), A Case of Pellagra Associated With Megaduodenum in a Young Woman. Nutrition in Clinical Practice, 28: 218-222. https://doi.org/10.1177/0884533612464783[↩]
- Bilgili SG, Karadag AS, Calka O, Altun F. Isoniazid-induced pellagra. Cutan Ocul Toxicol. 2011 Dec;30(4):317-9. doi: 10.3109/15569527.2011.574303[↩]
- Dreizen S, McCredie KB, Keating MJ, Andersson BS. Nutritional deficiencies in patients receiving cancer chemotherapy. Postgrad Med. 1990 Jan;87(1):163-7, 170. doi: 10.1080/00325481.1990.11704531[↩]
- Nogueira A, Duarte AF, Magina S, Azevedo F. Pellagra associated with esophageal carcinoma and alcoholism. Dermatol Online J. 2009 May 15;15(5):8.[↩][↩]
- Paudel V, Chudal D. Classical pellagra, the disease of 4 Ds, the forgotten entity. Pan Afr Med J. 2020 Jul 27;36:219. doi: 10.11604/pamj.2020.36.219.24806[↩]
- Segula D, Banda P, Mulambia C, Kumwenda JJ. Case report–A forgotten dermatological disease. Malawi Med J. 2012 Mar;24(1):19-20. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3588195[↩]
- Mousa TY, Mousa OY. Nicotinic Acid Deficiency. [Updated 2022 Aug 8]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK557749[↩][↩]
- Hegyi J, Schwartz RA, Hegyi V. Pellagra: Dermatitis, dementia, and diarrhoea. Int J Dermatol 2004;43:1–5. 10.1111/j.1365-4632.2004.01959.x[↩]
- Terada N, Kinoshita K, Taguchi S, Tokuda Y. Wernicke encephalopathy and pellagra in an alcoholic and malnourished patient. BMJ Case Rep. 2015 Oct 21;2015:bcr2015209412. doi: 10.1136/bcr-2015-209412[↩][↩][↩]
- Pellagra. https://dermnetnz.org/topics/pellagra[↩]
- Pitche PT. Pellagre et érythèmes pellagroïdes [Pellagra]. Sante. 2005 Jul-Sep;15(3):205-8.[↩]
- Soni BP, McLaren DS, Sherertz MF. Cutaneous changes in nutritional disease. In: Freedberg IM, Eisen AZ, Wolf K et al., eds. Dermatology in General Medicine. New York: McGraw-Hill, 1999:1725–37.[↩]
- Segula D, Banda P, Mulambia C, Kumwenda JJ. Case report–A forgotten dermatological disease. Malawi Med J. 2012 Mar;24(1):19-20. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3588195/[↩]
- Prousky JE. Pellagra may be a rare secondary complication of anorexia nervosa: a systematic review of the literature. Altern Med Rev. 2003 May;8(2):180-5.[↩]
- Matapandeu G, Dunn SH, Pagels P. An Outbreak of Pellagra in the Kasese Catchment Area, Dowa, Malawi. Am J Trop Med Hyg. 2017 May;96(5):1244-1247. doi: 10.4269/ajtmh.16-0423[↩]





{kind=link}