Contents
What is adenoidectomy
Adenoidectomy or adenoid removal surgery is one of the most commonly performed operations in children. Adenoidectomy is primarily performed as treatment of otitis media with effusion and obstructive sleep apnea in children 1. The adenoids are often taken out at the same time as the tonsils (tonsillectomy). The adenoid glands sit behind your nose above the roof of your mouth in the nasopharynx. Air passes over these glands when you take a breath. The adenoid is a proliferation of lymphoid tissue lining the roof and posterior wall of the nasopharynx, forming the superior aspect of Waldeyer’s lymphatic ring 2. Identifiable from 6 weeks gestation, it receives its blood supply from branches of the facial and maxillary arteries, and the thyrocervical trunk. The adenoid enlarges rapidly during early childhood and reaches its largest size in 7-year-olds before regressing 3. A relative mismatch between an enlarged adenoidal pad and a small nasopharynx in the pediatric population can result in choanal obstruction, leading to sleep-disordered breathing and obstructive sleep apnea. Obstruction of the Eustachian tube orifice, in conjunction with the presence of an increased bacterial load in the adenoid, is thought to produce a biofilm infection implicated in the pathogenesis of otitis media with effusion 4.
Adenoidectomy is usually carried out by an ear, nose and throat (ENT) surgeon and takes around 30 minutes. Afterwards, your child will need to stay in the recovery ward for up to an hour until the anesthetic has worn off.
Adenoidectomies are sometimes day cases if carried out in the morning, in which case your child may be able to go home on the same day. However, if the procedure is carried out in the afternoon, your child may need to stay in hospital overnight.
A health care provider may recommend adenoidectomy if:
- Enlarged adenoids are blocking your child’s airway. Symptoms in your child can include heavy snoring, problems breathing through the nose, and episodes of not breathing during sleep.
- Your child has chronic ear infections that occur often, continue despite use of antibiotics, cause hearing loss, or cause the child to miss a lot of school days.
Adenoidectomy may also be recommended if your child has tonsillitis that keeps coming back.
The adenoids normally shrink as children grow older. Adults rarely need to have them removed.
The main, evidence-based indications for adenoidectomy are the treatment of otitis media with effusion and obstructive sleep-disordered breathing in children 5. The latter procedure is often performed in conjunction with tonsillectomy in cases of gross tonsillar hypertrophy, or concurrent history of recurrent tonsillitis meeting the Paradise criteria 6.
Less frequent indications for adenoidectomy are in the holistic management of rhinosinusitis, hyposmia or anosmia, and suspected malignancy 2. The decision to operate should always be based on a clear positive history, clinical examination, and appropriate investigations. In otitis media with effusion, this includes audiometry and tympanometry, and in cases of sleep-disordered breathing, polysomnography is recommended.
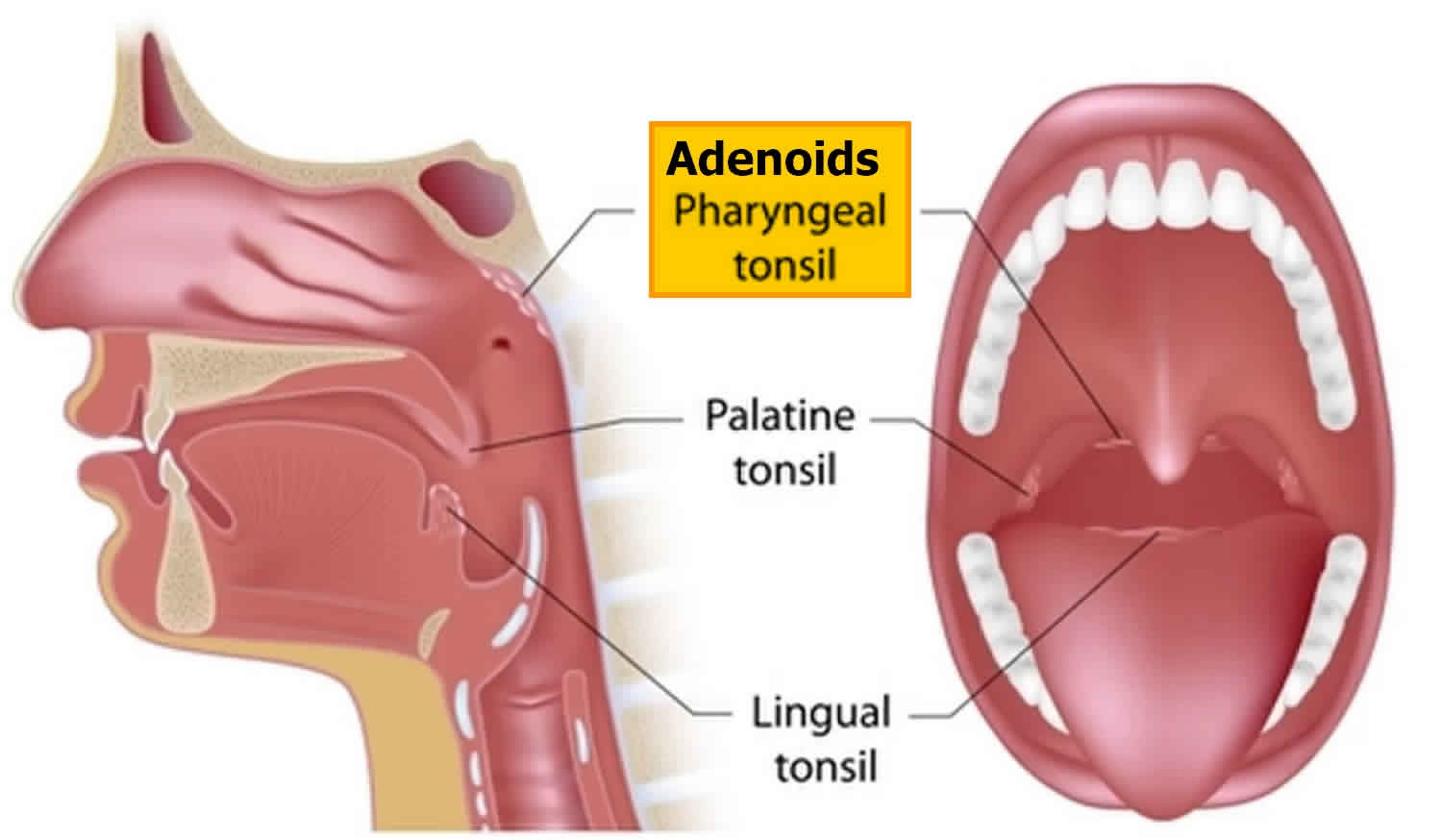
Figure 1. Adenoids and tonsils
Adenoidectomy indications
A child’s adenoids can sometimes become swollen or enlarged. This can happen after a bacterial or viral infection, or after a substance triggers an allergic reaction.
In most cases, swollen adenoids only cause mild discomfort and treatment isn’t needed. However, for some children, it can cause severe discomfort and interfere with their daily life.
The main, evidence-based indications for adenoidectomy are the treatment of otitis media with effusion and obstructive sleep-disordered breathing in children 5. The latter procedure is often performed in conjunction with tonsillectomy in cases of gross tonsillar hypertrophy, or concurrent history of recurrent tonsillitis meeting the Paradise criteria 6.
Less frequent indications for adenoidectomy are in the holistic management of rhinosinusitis, hyposmia or anosmia, and suspected malignancy 7. The decision to operate should always be based on a clear positive history, clinical examination, and appropriate investigations. In otitis media with effusion, this includes audiometry and tympanometry, and in cases of sleep-disordered breathing, polysomnography is recommended.
Adenoids may need to be removed if your child has:
- breathing problems – your child may have difficulty breathing through their nose and may have to breathe through their mouth instead, which can cause problems such as cracked lips and a dry mouth
- difficulty sleeping – your child may have problems sleeping and may start to snore; in severe cases, some children may develop sleep apnoea (irregular
- breathing during sleep and excessive sleepiness during the day)
- recurrent or persistent problems with the ears – such as middle ear infections (otitis media) or glue ear (where the middle ear becomes filled with fluid)
- recurrent or persistent sinusitis – leading to symptoms such as a constantly runny nose, facial pain and nasal-sounding speech
Adenoidectomy contraindications
Whilst there are no absolute contraindications to adenoidectomy, careful consideration must be given to palatal insufficiency. Individuals with known cleft palate or occult submucosal cleft palate are at a significantly increased risk of developing velopharyngeal insufficiency following adenoidectomy which can result in persistent hypernasal speech and nasal regurgitation. In such individuals a partial adenoidectomy limited to the lower third of the choana has been proposed 8. Other relative contraindications to adenoidectomy include significant bleeding diathesis and active infection 9.
Adenoidectomy procedure
Before the adenoidectomy surgery
Tell your ENT surgeon if your child has had a cold or sore throat in the week before the operation.
If your child has a high temperature and cough, the operation may have to be postponed for a few weeks to ensure they’ve fully recovered and to reduce their risk of developing complications as a result of the surgery.
Your child will be given general anesthesia before surgery. This means your child will be asleep and unable to feel pain.
During adenoidectomy surgery:
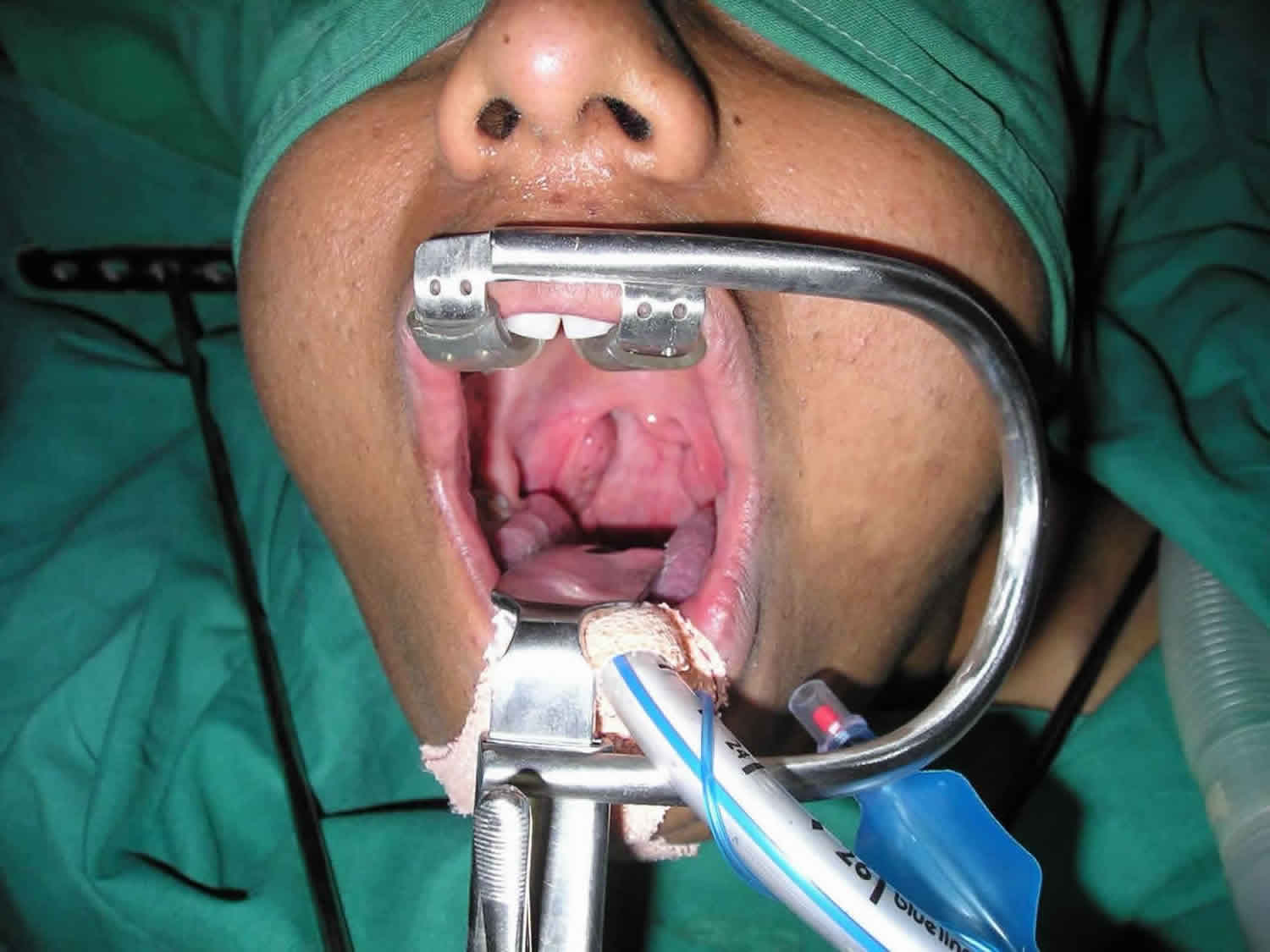
- The surgeon places a small tool into your child’s mouth to keep it open.
- The surgeon removes the adenoid glands using a spoon-shaped tool (curette). Or, another tool that helps cut away soft tissue is used.
- Some surgeons use electricity to heat the tissue, remove it, and stop bleeding. This is called electrocautery. Another method uses radiofrequency (RF) energy to do the same thing. This is called coblation. A cutting tool called a debrider can also be used to remove the adenoid tissue.
- Absorbent material called packing material may also be used to control bleeding.
Your child will stay in the recovery room after surgery. You will be allowed to take your child home when your child is awake and can breathe easily, cough, and swallow. In most cases, this will be a few hours after surgery.
Adenoidectomy technique
A wide range of techniques for adenoidectomy exist, including laser ablation, coblation, endoscopic excision, and power-assisted (microdebrider) excision. The 2 most commonly performed techniques are curettage and monopolar suction diathermy. Some surgeons favor monopolar suction diathermy for its simplicity, low post-operative hemorrhage rate, and comparable outcomes to more expensive and complex emergent techniques 10.
Monopolar Suction Diathermy
The custom monopolar suction diathermy device is bent to 70 to 90 degrees approximately 2 centimeters from its tip and the stylet removed. Under indirect visualization with an anti-fogged laryngeal mirror suction-diathermy (current 35 to 38 W) is carried out systematically, superiorly to inferiorly, from the choanal to the velopharyngeal portion of the adenoid. Lateral adenoidal tissue can be suctioned medially before ablation, avoiding trauma and scarring of the tubal cushion. The procedure is completed when a comprehensive view of the choana is achieved, the nasopharynx has a smooth contour and hemostasis ensured. Nasal packing is rarely required 11.
Curettage
An adenoid curette is introduced to the postnasal space and engages with the adenoid pad. A dental mirror can be used to facilitate indirect visualization and confirmation of positioning. The adenoids are removed superior to inferiorly in a single, firm movement, with the head stabilized by the non-dominant hand. The process may be repeated, and the nasopharynx re-examined either by palpation or with a mirror to ensure completeness of excision. The post nasal space may be packed with swabs to achieve hemostasis while a tonsillectomy is performed. These must be removed at the end of the procedure.
On completion of adenoidectomy, it is essential to suction any clots from the postnasal space using a nasal suction catheter and to ensure that hemostasis has been achieved. Care must be taken when removing the gag to ensure that the endotracheal tube has not herniated into the blade, to prevent inadvertent extubation.
Adenoidectomy recovery
Adenoidectomy is usually carried out by an ear, nose and throat (ENT) surgeon and takes around 30 minutes. Afterwards, your child will need to stay in the recovery ward for up to an hour until the anesthetic has worn off.
Adenoidectomies are sometimes day cases if carried out in the morning, in which case your child may be able to go home on the same day. However, if the procedure is carried out in the afternoon, your child may need to stay in hospital overnight.
It’s normal to have a sore throat after an adenoidectomy. Your child will usually be given painkillers while in hospital to help ease discomfort.
Your child may also feel groggy and sleepy after having an anaesthetic. After the operation, they’ll be observed for several hours to make sure they’re recovering normally. Once the doctor is satisfied, you’ll be able to take your child home.
Adenoidectomy complete recovery takes about 1 to 2 weeks.
Follow instructions on how to care for your child at home.
Pain relief
Your child may still have a sore throat, earache or stiff jaw after returning home, and they may need painkillers in the days after the operation.
Over-the-counter painkillers, such as paracetamol, are usually suitable. Younger children may find it easier to take liquid or soluble paracetamol, particularly if they have a sore throat.
Always make sure you follow the dosage instructions on the packet, and never give aspirin to a child who’s under the age of 16.
Eating and drinking
Your child should be able to drink liquids two to three hours after having an adenoidectomy. They can begin eating several hours after that.
To start with, eating normally may be difficult because of the sore throat. Encourage your child to eat soft or liquid foods, such as soups or yoghurts, which are easier to swallow.
Giving your child a dose of painkillers about an hour or so before they eat may make swallowing food easier.
It’s also important for them to drink plenty of fluids to avoid dehydration.
Returning to school
Your child will need to rest for several days after an adenoidectomy and should be kept off school for a week. This is to reduce their risk of getting an infection.
The skin and tissue where the adenoids used to be will take a while to heal. It’s important to try to prevent the wound becoming infected because an infection could cause complications.
Keep your child away from people with coughs or colds, and from smoky environments. They should also avoid swimming for three weeks after the operation.
Adenoidectomy complications
Risks of any anesthesia are:
- Reactions to medicines: With any surgery where an anaesthetic is required, there’s a risk of the person having an allergic reaction to the anaesthetic. If your child’s general health is good, their risk of having a serious allergic reaction (anaphylaxis) to the anaesthetic is extremely small (1 in 20,000). Around 1 in 10 children may experience some temporary symptoms, such as a headache, sickness or dizziness.
- Breathing problems
Risks of any surgery are:
- Bleeding: In rare cases, excessive bleeding can occur after the adenoids have been removed. This is known as a haemorrhage. Further surgery will be needed for cauterisation (where heat is applied to stop the bleeding) or to insert a dressing. Less than 1 in 100 children need emergency treatment to stop a haemorrhage. However, if it occurs, a hemorrhage needs to be dealt with quickly to prevent excessive blood loss.
- Infection: All surgery carries the risk of infection. The tissue in the area where the adenoids were removed may become infected with bacteria. Therefore, after the procedure, your child may be prescribed antibiotics to help prevent infection.
After an adenoidectomy, some children experience minor health problems. However, most of these are temporary and rarely require further treatment. They can include:
- sore throat
- earache
- stiff jaw
- blocked nose or nasal discharge
- bad breath (halitosis)
- a change in voice (your child may sound like they’re speaking through their nose)
Most of these symptoms will pass within one to two weeks, and shouldn’t last longer than four weeks. Contact your doctor if your child is still experiencing side effects after this time.
Common complications
Pain is self-limiting, and a short course of simple analgesics such as acetaminophen (paracetamol) and non-steroidal anti-inflammatory medications (NSAIDs) is usually sufficient.
An altered voice is usually the resolution of preexisting hyponasal speech and is often seen as a benefit rather than a complication.
Adenoid regrowth is noted in a small number of patients, and occasionally a revision adenoidectomy is necessary.
Rare complications
Dental trauma and minor injuries to the lips and tongue can occur following adenoidectomy and tonsillectomy. The surgeon must enquire preoperatively about loose teeth and fillings, and exercise caution when introducing and opening the Boyle-Davis mouth gag to minimize these risks.
Bleeding is rare, and with the widespread adoption of diathermy and techniques involving direct visualization, rates have declined to as low as 0.07% 12. Management of bleeding involves admission and packing of the postnasal space. Intraoperative bleeding can result in the formation of a “coroner’s” clot in the nasopharynx that can dislodge and result in fatal aspiration. For this reason, it is mandatory to suction the post nasal space before completing the surgery.
Atlantoaxial subluxation (Grisel syndrome) is a rare but serious complication following adenoidectomy. Pre-existing laxity of the anterior spinal ligament (often seen in Down syndrome) and excessive use of diathermy are recognized risk factors. Management consists of analgesia, immobilization, and neurosurgical intervention in refractory cases 13.
Long-term velopharyngeal insufficiency is rare, occurring in between 1 in 1500 and 1 in 10,000 cases. It results in hypernasal speech and nasal regurgitation. Risk factors include a known cleft palate or an occult submucosal cleft palate. A partial adenoidectomy retaining tissue at the velopharyngeal junction may be considered in these cases to minimize the risk. Rarely, reconstructive surgery is performed to improve severe speech and swallowing impairment 14.
Adenoidectomy prognosis
After adenoidectomy procedure, most children:
- Breathe better through the nose
- Have fewer and milder sore throats
- Have fewer ear infections
In rare cases, adenoid tissue may grow back. This does not cause problems most of the time. However, it can be removed again if necessary.
Tonsillectomy adenoidectomy
If your child has large tonsils, or has had severe or frequent bouts of tonsillitis, removing the tonsils and adenoids at the same time may be recommended. This procedure is called an adenotonsillectomy or bilateral tonsillectomy and adenoidectomy.
Removing the adenoids and tonsils in a single procedure reduces the risk of complications. However, adenoidectomies, tonsillectomies and adenotonsillectomies are quick and straightforward procedures with few associated risks. Several complications are documented with tonsillectomy and include, bleeding, velopharyngeal insufficiency, and dehydration.
The tonsils help protect against infections. But children with large tonsils may have problems breathing at night. The tonsils may also trap excess bacteria which can lead to frequent or very painful sore throats. In either of these cases, the child’s tonsils have become more harmful than protective.
You and your child’s health care provider may consider a tonsillectomy if:
- Your child has infections often (7 or more times in 1 year, or 5 or more times over 2 years).
- Your child misses a lot of school.
- Your child has trouble breathing and does not sleep well because the tonsils block the airway (sleep apnea).
- Your child has an abscess or a growth on the tonsils.
In the United States, tonsillectomy is one of the most commonly performed surgical procedures. Over 500,000 cases are performed annually in children less than 15 years of age 15. Two common reasons for tonsillectomy surgery are sleep-disordered breathing and recurrent tonsillitis. According to the American Academy of Otolaryngology-Head and Neck Surgery, the definition of tonsillectomy is a “surgical procedure performed with or without adenoidectomy that completely removes the tonsil, including its capsule, by dissecting the peritonsillar space between the tonsil capsule and the muscular wall. Depending on the context in which it is used, it may indicate tonsillectomy with adenoidectomy, especially in relation to sleep-disordered breathing” 16.
Sleep-disordered breathing is the recurrent partial or complete upper airway obstruction during sleep, resulting in the disruption of normal ventilation and sleep patterns. It can be diagnosed based on history and physical. Symptoms of sleep-disordered breathing include hyperactivity, daytime tiredness, and aggression. Signs of sleep-disordered breathing include heroic snoring, witnessed apnea, restless sleeping, growth retardation, poor school performance, and nocturnal enuresis. Children with sleep-disordered breathing have significantly higher rates of antibiotic use, 40% more hospital visits, and a 215% elevation in healthcare usage from increased upper respiratory infections compared to children without sleep-disordered breathing. Tonsillar and adenoid hypertrophies are the most common cause of sleep-disordered breathing. Tonsillar size does not always correlate to the severity of sleep-disordered breathing and polysomnography can further evaluate patients with signs and symptoms of sleep-disordered breathing who are without tonsillar hypertrophy.
Regarding recurrent tonsillitis, it is recommended to use watchful waiting in patients with fewer than seven episodes in the prior year or fewer than five episodes annually in the past 2 years or fewer than three episodes annually in the past 3 years. If the frequency of infections exceeds these numbers, tonsillectomy can be recommended as an option for treatment. Documentation of each infection should include a sore throat and one or more of the following: temperature > 100.94 °F (38.3 degrees Celsius), cervical adenopathy, tonsillar exudates, or a positive group A beta-hemolytic streptococci (GABHS) bacteria. Modifying factors such as antibiotic allergy/intolerance, PFAPA (periodic fever, aphthous stomatitis, pharyngitis, and adenitis) or peritonsillar abscess could warrant earlier surgical intervention in recurrent tonsillitis patients 6.
Additional indications for tonsillectomy include tonsillar asymmetry (to rule out malignancy) and malignancy. The most common malignancies of the palatine tonsils are squamous cell carcinoma and lymphoma. Most malignant neoplasms in children are lymphoma 17.
Tonsillectomy indications
The following guidelines are from the Clinical Practice Guideline: Tonsillectomy in Children from the American Academy of Otolaryngology-Head and Neck Surgery 6:
- “Clinicians should recommend watchful waiting for recurrent throat infection if there have been fewer than 7 episodes in the past year or fewer than 5 episodes per year in the past 2 years or fewer than 3 episodes per year in the past 3 years.
- Clinicians may recommend tonsillectomy for recurrent throat infection with a frequency of at least 7 episodes in the past year or at least 5 episodes per year for 2 years or at least 3 episodes per year for 3 years with documentation in the medical record for each episode of sore throat and one or more of the following: temperature >38.3°C, cervical adenopathy, tonsillar exudate, or a positive test for group A beta-hemolytic streptococci (GABHS) bacteria.
- Clinicians should assess the child with recurrent throat infection who does not meet criteria in Statement 2 for modifying factors that may nonetheless favor tonsillectomy, which may include but are not limited to multiple antibiotic allergy/intolerance, PFAPA (periodic fever, aphthous stomatitis, pharyngitis, and adenitis), or history of peritonsillar abscess.
- Clinicians should ask caregivers of children with sleep-disordered breathing and tonsil hypertrophy about comorbid conditions that might improve after tonsillectomy, including growth retardation, poor school performance, enuresis, and behavioral problems.
- Clinicians should counsel caregivers about tonsillectomy as a means to improve health in children with abnormal polysomnography who also have tonsil hypertrophy and sleep-disordered breathing.
- Clinicians should counsel caregivers and explain that sleep-disordered breathing may persist or recur after tonsillectomy and may require further management.
- Clinicians should administer a single, intraoperative dose of intravenous dexamethasone to children undergoing tonsillectomy.
- Clinicians should not routinely administer or prescribe perioperative antibiotics to children undergoing tonsillectomy.
- The clinician should advocate for pain management after tonsillectomy and educate caregivers about the importance of managing and reassessing pain.
- Clinicians who perform tonsillectomy should determine their rate of primary and secondary post-tonsillectomy hemorrhage at least annually”
Tonsillectomy procedure
Tonsillectomy can be either extracapsular or intracapsular. The “hot” extracapsular technique with monopolar cautery is the most popular technique in the United States. The superior pole of the tonsil is grasped with the Allis clamp, and the tonsil is medialized. The lateral edge of the tonsil is identified submucosally. The superior pole is incised using around 20W of power if a traditional tip is used. The avascular plane between the tonsil and musculature is identified. The entire palatine tonsil is removed typically from the superior to the inferior pole. Maintenance of hemostasis is by packing, suction cautery, or ties.
“Cold” tonsillectomy is performed using sharp dissection. The tonsil is grasped with the Allis clamp and medialized. The lateral aspect of the tonsil is again identified and incised using a number 12 scalpel. A Metzenbaum scissors is then used to identify the avascular plane. Once within the plane, a Fisher tonsil dissector removes the tonsil from the fossa until the tonsil attachment remains only at the inferior pole. A Tyding snare is then used to separate the tonsil from its inferior pole. Maintenance of hemostasis is with pressure from a tonsil sponge, suction cautery or ties.
Coblation can be used to remove the tonsil using a technique similar to monopolar cautery. Coblation utilizes saline irrigation that converts into an ionized plasma layer resulting in a molecular breakdown of tissue. Minimal heat generation takes place, and this is a common technique for partial tonsillectomies. A micro-debrider can be used as well to perform a partial tonsillectomy 18.
Debate remains over the advantages of one technique over the other 19. Overall, the benefit of one technique depends on the cost, decreased complication rates (i.e., bleeding rates), time in the operating room, and post-operative pain. “Cold” tonsillectomy is thought to result in less post-operative pain, while some studies show “hot” tonsillectomy results in less intraoperative blood loss and surgical time. Choice of technique depends on the surgeon’s experience and comfort level.
Tonsillectomy and adenoidectomy recovery
A tonsillectomy is most often done in a hospital or surgery center. Your child will go home the same day as the surgery. Children rarely need to stay overnight in the hospital for observation.
Complete recovery takes about 1 to 2 weeks. During the first week, your child should avoid people who are sick. It will be easier for your child to become infected during this time.
Nearly everyone experiences pain after a tonsillectomy. Pain is most often in the throat and frequently in the ears but may also be located in the jaw or the neck.
Steps that you can take to reduce pain, promote recovery and prevent complications include the following:
- Medications. Take pain medications as directed by your surgeon or the hospital staff.
- Fluids. It’s important to get plenty of fluids after surgery to avoid dehydration. Water and ice pops are good choices.
- Food. Bland foods that are easy to swallow, such as applesauce or broth, are the best choices immediately after surgery. Foods such as ice cream and pudding can be added to the diet if they’re tolerated. Foods that are easy to chew and swallow should be added to the diet as soon as possible. Avoid acidic, spicy, hard or crunchy foods as they may cause pain or bleeding.
- Rest. Bed rest is important for several days after surgery, and strenuous activities — such as running and bike riding — should be avoided for two weeks after surgery. You or your child should be able to return to work or school after resuming a normal diet, sleeping normally through the night and not needing pain medication. Talk to your doctor about any activities that should be avoided.
Watch for the following complications that require prompt medical care:
- Bleeding. You may see small specks of dark blood from the nose or in the saliva, but any bright red blood requires a trip to the emergency room for a prompt evaluation and treatment. Surgery to stop bleeding may be necessary.
- Fever. Call your doctor if you or your child has a fever of 102 °F (38.9 °C) or higher.
- Dehydration. Call your doctor if you observe signs of dehydration, such as reduced urination, thirst, weakness, headache, dizziness or lightheadedness. Common signs of dehydration in children include urinating fewer than two or three times a day or crying with no tears.
- Breathing problems. Snoring or noisy breathing is common during the first week or so of recovery. However, if you or your child is having difficulty breathing, get emergency care.
Tonsillectomy and adenoidectomy complications
The risks for any anesthesia are:
- Reaction to medicines
- Breathing problems
The risks for any surgery are:
- Bleeding
- Infection
Rarely, bleeding after surgery can go unnoticed and cause very bad problems. Swallowing a lot may be a sign of bleeding from the tonsils.
Another risk includes injury to the uvula (soft palate).
Bleeding is one of the most common and feared complications following tonsillectomy with or without adenoidectomy. A study from 2009 to 2013 involving over one hundred thousand children showed that 2.8% of children had unplanned revisits for bleeding following tonsillectomy, 1.6% percent of patients came through the emergency department, and 0.8% required a procedure 20. Frequency is higher at night with 50% of bleeding occurring between 10pm-1am and 6am-9am; this is thought to be from changes in circadian rhythm, vibratory effects of snoring on the oropharynx, or drying of the oropharyngeal mucosa from mouth breathing 21. Risk of bleeding in patients with known coagulopathies may be significantly higher 22.
Postoperative nausea and vomiting is another common complication following tonsillectomy. It occurs in up to 70% of patients who did not receive prophylactic anti-emetics. Postoperative nausea and vomiting can lead to increased admission rates, increased need for intravenous hydration, increased need for pain medicine, and decreased patient satisfaction. The recommendation to counter these sequelae is to administer a single dose of intraoperative dexamethasone during tonsillectomy. Some clinicians will routinely prescribe a single dose of ondansetron for outpatient surgeries, as postoperative nausea and vomiting is most likely within the first 24 hours after surgery.
The leading cause of morbidity following tonsillectomy is pain, subsequently leading to diminished oral intake and dehydration, dysphagia, and weight loss. It is important that caregivers are competent to monitor for signs of dehydration and continuously encourage their child to stay hydrated. One method to decrease oropharyngeal pain is alternating scheduled doses or acetaminophen and ibuprofen 6.
Velopharyngeal insufficiency may also occur following tonsillectomy and adenoidectomy 23. Symptoms can include hypernasal speech and food regurgitation through the nasal passage during feeding.
- Ruben RJ. The adenoid: Its history and a cautionary tale. Laryngoscope. 2017 Jun;127 Suppl 2:S13-S28[↩]
- Gross CW, Harrison SE. Tonsils and adenoids. Pediatr Rev. 2000 Mar;21(3):75-8[↩][↩]
- Vogler RC, Ii FJ, Pilgram TK. Age-specific size of the normal adenoid pad on magnetic resonance imaging. Clin Otolaryngol Allied Sci. 2000 Oct;25(5):392-5[↩]
- Fergie N, Bayston R, Pearson JP, Birchall JP. Is otitis media with effusion a biofilm infection? Clin Otolaryngol Allied Sci. 2004 Feb;29(1):38-46[↩]
- Miller BJ, Gupta G. Adenoidectomy. [Updated 2018 Dec 13]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2019 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK535352[↩][↩]
- Baugh RF, Archer SM, Mitchell RB, Rosenfeld RM, Amin R, Burns JJ, Darrow DH, Giordano T, Litman RS, Li KK, Mannix ME, Schwartz RH, Setzen G, Wald ER, Wall E, Sandberg G, Patel MM., American Academy of Otolaryngology-Head and Neck Surgery Foundation. Clinical practice guideline: tonsillectomy in children. Otolaryngol Head Neck Surg. 2011 Jan;144(1 Suppl):S1-30[↩][↩][↩][↩][↩]
- Gross CW, Harrison SE. Tonsils and adenoids. Pediatr Rev. 2000 Mar;21(3):75-8.[↩]
- Finkelstein Y, Wexler DB, Nachmani A, Ophir D. Endoscopic partial adenoidectomy for children with submucous cleft palate. Cleft Palate Craniofac. J. 2002 Sep;39(5):479-86.[↩]
- Ingram DG, Friedman NR. Toward Adenotonsillectomy in Children: A Review for the General Pediatrician. JAMA Pediatr. 2015 Dec;169(12):1155-61[↩]
- Sjogren PP, Thomas AJ, Hunter BN, Butterfield J, Gale C, Meier JD. Comparison of pediatric adenoidectomy techniques. Laryngoscope. 2018 Mar;128(3):745-749[↩]
- Hartley BE, Papsin BC, Albert DM. Suction diathermy adenoidectomy. Clin Otolaryngol Allied Sci. 1998 Aug;23(4):308-9[↩]
- Lowe D, Brown P, Yung M. Adenoidectomy technique in the United Kingdom and postoperative hemorrhage. Otolaryngol Head Neck Surg. 2011 Aug;145(2):314-8[↩]
- Miller BJ, Lakhani R, Rashid A, Tostevin P. Painful torticollis following adenotonsillectomy: a cardinal sign of atlantoaxial subluxation. BMJ Case Rep. 2018 Mar 01;2018[↩]
- Stewart KJ, Ahmad T, Razzell RE, Watson AC. Altered speech following adenoidectomy: a 20 year experience. Br J Plast Surg. 2002 Sep;55(6):469-73.[↩]
- Bohr C, Shermetaro C. Tonsillectomy and Adenoidectomy. [Updated 2019 Jan 13]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2019 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK536942[↩]
- Baugh RF, Archer SM, Mitchell RB, Rosenfeld RM, Amin R, Burns JJ, Darrow DH, Giordano T, Litman RS, Li KK, Mannix ME, Schwartz RH, Setzen G, Wald ER, Wall E, Sandberg G, Patel MM., American Academy of Otolaryngology-Head and Neck Surgery Foundation. Clinical practice guideline: tonsillectomy in children. Otolaryngol Head Neck Surg. 2011 Jan;144(1 Suppl):S1-30.[↩]
- Rokkjaer MS, Klug TE. Malignancy in routine tonsillectomy specimens: a systematic literature review. Eur Arch Otorhinolaryngol. 2014 Nov;271(11):2851-61[↩]
- Chan KH, Friedman NR, Allen GC, Yaremchuk K, Wirtschafter A, Bikhazi N, Bernstein JM, Kelley PE, Lee KC. Randomized, controlled, multisite study of intracapsular tonsillectomy using low-temperature plasma excision. Arch. Otolaryngol. Head Neck Surg. 2004 Nov;130(11):1303-7[↩]
- Leinbach RF, Markwell SJ, Colliver JA, Lin SY. Hot versus cold tonsillectomy: a systematic review of the literature. Otolaryngol Head Neck Surg. 2003 Oct;129(4):360-4[↩]
- Mahant S, Keren R, Localio R, Luan X, Song L, Shah SS, Tieder JS, Wilson KM, Elden L, Srivastava R., Pediatric Research in Inpatient Settings (PRIS) Network. Variation in quality of tonsillectomy perioperative care and revisit rates in children’s hospitals. Pediatrics. 2014 Feb;133(2):280-8[↩]
- Harounian JA, Schaefer E, Schubart J, Carr MM. Pediatric adenotonsillectomy and postoperative hemorrhage: Demographic and geographic variation in the US. Int. J. Pediatr. Otorhinolaryngol. 2016 Aug;87:50-4[↩]
- Warad D, Hussain FT, Rao AN, Cofer SA, Rodriguez V. Haemorrhagic complications with adenotonsillectomy in children and young adults with bleeding disorders. Haemophilia. 2015 May;21(3):e151-5[↩]
- De Buys Roessingh A, El Ezzi O, Richard C, Béguin C, Zbinden-Trichet C, La Scala G, Leuchter I. [Velopharyngeal insufficiency in children]. Rev Med Suisse. 2017 Feb 15;13(550):400-405[↩]





{kind=link}