Contents
What is adrenoleukodystrophy
Adrenoleukodystrophy also known as X-linked adrenoleukodystrophy or ALD disease, is an X-linked recessive genetic disorder caused by an abnormality in the ABCD1 gene on the X chromosome 1. The faulty ABCD1 gene means those affected are unable to process very long chain fatty acids (VLCFAs). It is thought that these very long chain fatty acids (VLCFAs) accumulate and destroy the myelin sheath that covers the nerves in the body and brain. The myelin acts like the coating around an electric cable, and allows messages to be transmitted along nerve cells. Some of those affected experience serious neurological problems that can affect mental function and lead to disability and reduced life span.
X-linked adrenoleukodystrophy is a genetic disorder that occurs primarily in males. X-linked adrenoleukodystrophy (X-ALD) mainly affects the nervous system and the adrenal glands, which are small glands located on top of each kidney and in some cases testicular insufficiency 2. In X-linked adrenoleukodystrophy (X-ALD), the fatty covering (myelin) that insulates nerves in the brain and spinal cord is prone to deterioration (demyelination), which reduces the ability of the nerves to relay information to the brain.
In cerebral adrenoleukodystrophy the damage to myelin happens in the brain. When the myelin is damaged the nerves in the brain cannot work properly, and the person’s physical and mental abilities begin to deteriorate. Functions such as reasoning, speech and mobility are lost. Eventually, they become completely dependent.
In most males with adrenoleukodystrophy the adrenal glands are also affected. Damage to the outer layer of the adrenal glands (adrenal cortex) causes a shortage of certain hormones such as adrenaline and cortisol (adrenocortical insufficiency), leading to abnormalities in blood pressure, heart rate, sexual development and reproduction. Adrenocortical insufficiency may cause weakness, weight loss, tiredness, skin changes, muscle pains, vomiting, and coma.
It is not possible to predict how the adrenoleukodystrophy gene will affect any one person: its effects can vary. Once diagnosis has been confirmed, the affected person needs to be closely monitored.
Adrenoleukodystrophy or ALD, is the most common leukodystrophy, accounting for about half of all leukodystrophies. The prevalence is approximately 1/20,000-1/50,000 births and most of those affected are boys. Approximately half of all females who carry the abnormal ABCD1 gene will develop some symptoms of ALD. Adrenoleukodystrophy occurs in all ethnic groups. The presentation of symptoms occurs somewhere between the ages of 4 and 10, and affects the brain with demyelination 3. Demyelination is the stripping away of the fatty coating that keeps nerve pulses confined and maintains the integrity of nerve signals. This process inhibits the nerves ability to conduct properly, thereby causing neurological deficits, including visual disturbances, auditory discrimination, impaired coordination, dementia, and seizures. Demyelination is an inflammatory response and nerve cells throughout the brain are destroyed.
Boys develop normally until the onset of symptoms occurs. Symptoms typically rival those of attention deficit disorder before serious neurological involvement becomes apparent. The symptoms progress rapidly and lead to vegetative state within two years, and death anytime thereafter.
Adrenocortical insufficiency, Addison’s Disease, is seen in 90 percent of the cases of ALD.
There are a wide range of clinical severities of X-linked adrenoleukodystrophy (X-ALD), and these have been classified into six broad categories: childhood cerebral ALD, adolescent cerebral ALD, adult cerebral, adrenomyeloneuropathy, adrenal insufficiency-only, and symptomatic heterozygotes. The clinical phenotypes of each are described below.
Adrenoleukodystrophy has been categorized into six types based on symptoms and age of onset:
- Childhood cerebral adrenoleukodystrophy (48% of cases): Childhood cerebral ALD is one of the most common forms of X-linked ALD, comprising approximately 30% of all patients with X-linked adrenoleukodystrophy. Onset of childhood cerebral adrenoleukodystrophy occurs between the ages of 2 and 10. Up to the point of onset, development is normal. The most common initial symptoms are difficulty in school, behavioral disturbance, impaired vision, or impaired hearing. After initial neurological symptoms appear, the health of the patients deteriorates rapidly. Further symptoms may include dementia, poor coordination, seizures, hyperactivity, difficulty with speech, and headaches. The average time between the initial symptoms and a vegetative state (where the patient is bedridden) or death is approximately 2 years, although it can range anywhere from 6 months to 20 years.
- Adolescent cerebral adrenoleukodystrophy (5% of cases): A small number of patients with X-linked adrenoleukodystrophy will present between the ages of 11 and 21 years. The symptoms are similar to those of childhood cerebral adrenoleukodystrophy, though progression of the disease may be somewhat slower.
- Adrenomyeloneuropathy (AMN) (26% of cases): Adrenomyeloneuropathy (AMN) is the most common form of adrenoleukodystrophy disease, and comprises approximately 40% of all X-linked adrenoleukodystrophy patients. The first symptoms of adrenomyeloneuropathy (AMN) usually occur in the twenties. Generally, initial symptoms noted are stiffness/clumsiness in the legs, weight loss, attacks of nausea, and generalized weakness. Adrenal impairment occurs, and other major manifestations may include difficulty with walking, urinary disturbance and impotence, cognitive defects, emotional disturbances, and depression. 70% of adrenomyelonueropathy (AMN) patients experience Addison’s disease. Adrenomyeloneuropathy (AMN) disease progresses slowly, and within 5 to 15 years the patient will generally need the aid of a cane or wheelchair.
- Adult cerebral adrenoleukodystrophy (3% of cases): Adult cerebral ALD is relatively rare, only representing approximately 3% of all ALD cases. Age of onset varies from the twenties to the fifties. The symptoms are similar to those of schizophrenia with dementia, and the progression of the disorder is rapid. The average time from the initial symptoms to vegetative state or death is approximately 3-4 years.
- Adrenoleukodystrophy that occurs in females: Women have two copies of the X chromosome, which is where the gene responsible for X-adrenoleukodystrophy resides. As a result, most women who carry a defective copy of a ABCD1 gene on the X-chromosome also carry one good copy of the ABCD1 gene, so they often won’t have any symptoms of the disease. However, some women who carry one good copy and one bad copy of the X-adrenoleukodystrophy gene (heterozygotes) do show some symptoms of adrenoleukodystrophy (symptomatic heterozygotes). The symptoms can range from very mild to very severe. They resemble those of other adrenoleukodystrophy patients, with the exception that heterozygote women rarely have impaired adrenal function.
- Adrenal insufficiency or Addison’s disease (10% of cases) only. Addison’s disease occurs when the adrenal glands do not produce enough of the hormone cortisol and, in some cases, the hormone aldosterone. Addison’s disease is also hypocortisolism.
Children with the cerebral form of X-linked adrenoleukodystrophy experience learning and behavioral problems that usually begin between the ages of 4 and 10. Over time the symptoms worsen, and these children may have difficulty reading, writing, understanding speech, and comprehending written material. Additional signs and symptoms of the cerebral form include aggressive behavior, vision problems, difficulty swallowing, poor coordination, and impaired adrenal gland function. The rate at which this disorder progresses is variable but can be extremely rapid, often leading to total disability within a few years. The life expectancy of individuals with this type depends on the severity of the signs and symptoms and how quickly the disorder progresses. Individuals with the cerebral form of X-linked adrenoleukodystrophy usually survive only a few years after symptoms begin but may survive longer with intensive medical support.
Signs and symptoms of the adrenomyeloneuropathy (AMN) type appear between early adulthood and middle age. Affected individuals develop progressive stiffness and weakness in their legs (paraparesis), experience urinary and genital tract disorders, and often show changes in behavior and thinking ability. Most people with the adrenomyeloneuropathy (AMN) type also have adrenocortical insufficiency. In some severely affected individuals, damage to the brain and nervous system can lead to early death.
People with X-linked adrenoleukodystrophy whose only symptom is adrenocortical insufficiency are said to have the Addison disease only form. In these individuals, adrenocortical insufficiency can begin anytime between childhood and adulthood. However, most affected individuals develop the additional features of the adrenomyeloneuropathy (AMN) type by the time they reach middle age. The life expectancy of individuals with this form depends on the severity of the signs and symptoms, but typically this is the mildest of the three types.
Rarely, individuals with X-linked adrenoleukodystrophy develop multiple features of the disorder in adolescence or early adulthood. In addition to adrenocortical insufficiency, these individuals usually have psychiatric disorders and a loss of intellectual function (dementia). It is unclear whether these individuals have a distinct form of the condition or a variation of one of the previously described types.
For reasons that are unclear, different forms of X-linked adrenoleukodystrophy can be seen in affected individuals within the same family.
Can female carriers display symptoms of adrenoleukodystrophy?
Women carriers of a defective adrenoleukodystrophy gene can display symptoms, though many remain asymptomatic for their entire lives. The symptoms vary dramatically, and tend to be displayed in later life. Symptoms may be similar to those of adrenomyeloneuropathy (AMN) (described earlier), though they are generally milder. Roughly half of all women who are carriers of adrenoleukodystrophy will eventually develop some sort of adrenomyeloneuropathy (AMN)-like symptoms in later life.
Can adrenoleukodystrophy be cured?
Sadly, once symptoms of cerebral adrenoleukodystrophy have appeared, there is currently no cure. However, it may be possible to prevent the disorder in people who carry the ABCD1 gene but have so far developed none or minor symptoms.
Why is genetic testing of the family important?
Once one member of a family has been diagnosed, it is very important to get the rest of your family checked genetically, especially if there are brothers, who could also have the disease. If the ABCD1 gene is discovered early, before symptoms appear, there is a chance of preventing adrenoleukodystrophy from developing. Sisters could be adrenoleukodystrophy carriers. When a boy is diagnosed with adrenoleukodystrophy it will most likely be inherited from his mother. You should be offered genetic counseling as soon as the diagnosis has been confirmed. Genetic tests are advised for all siblings and parents. The genetic counselor will talk you through the implications of the tests. If siblings are found to have adrenoleukodystrophy they should be considered for a preventative programme
Adrenoleukodystrophy causes
Mutations in the ABCD1 gene cause X-linked adrenoleukodystrophy. The ABCD1 gene provides instructions for producing the adrenoleukodystrophy protein (ALDP), which is involved in transporting certain fat molecules called very long-chain fatty acids into peroxisomes. Peroxisomes are small sacs within cells that process many types of molecules, including very long-chain fatty acids.
ABCD1 gene mutations result in a shortage (deficiency) of ALDP. When this protein is lacking, the transport and subsequent breakdown of very long-chain fatty acids is disrupted, causing abnormally high levels of these fats in the body. The accumulation of very long chain fatty acids (VLCFAs) may be toxic to the adrenal cortex and myelin. Research suggests that the accumulation of very long-chain fatty acids triggers an inflammatory response in the brain, which could lead to the breakdown of myelin. The destruction of these tissues leads to the signs and symptoms of X-linked adrenoleukodystrophy.
The faulty ABCD1 gene can also cause several related but different conditions, such as Asymptomatic ALD (for males affected by the gene who do not yet have symptoms). The other condition caused by the faulty ABCD1 gene is called adrenomyelonueropathy (AMN), which affects nerves in the spinal cord and body. Men that experience adrenomyelonueropathy (AMN) also endure demyelination, however, it most commonly restricts itself to the long tracts of the spinal column causing increasing difficulty with walking, as well as bladder and bowel disturbances over a period of decades. 70% of adrenomyelonueropathy (AMN) patients experience Addison’s disease. There is also an Addison’s-only form of the disease that appears to spare the nervous system. Many, but not all of the Addison’s-only patients develop adrenomyelonueropathy (AMN) characteristics later in life..
Adrenoleukodystrophy inheritance pattern
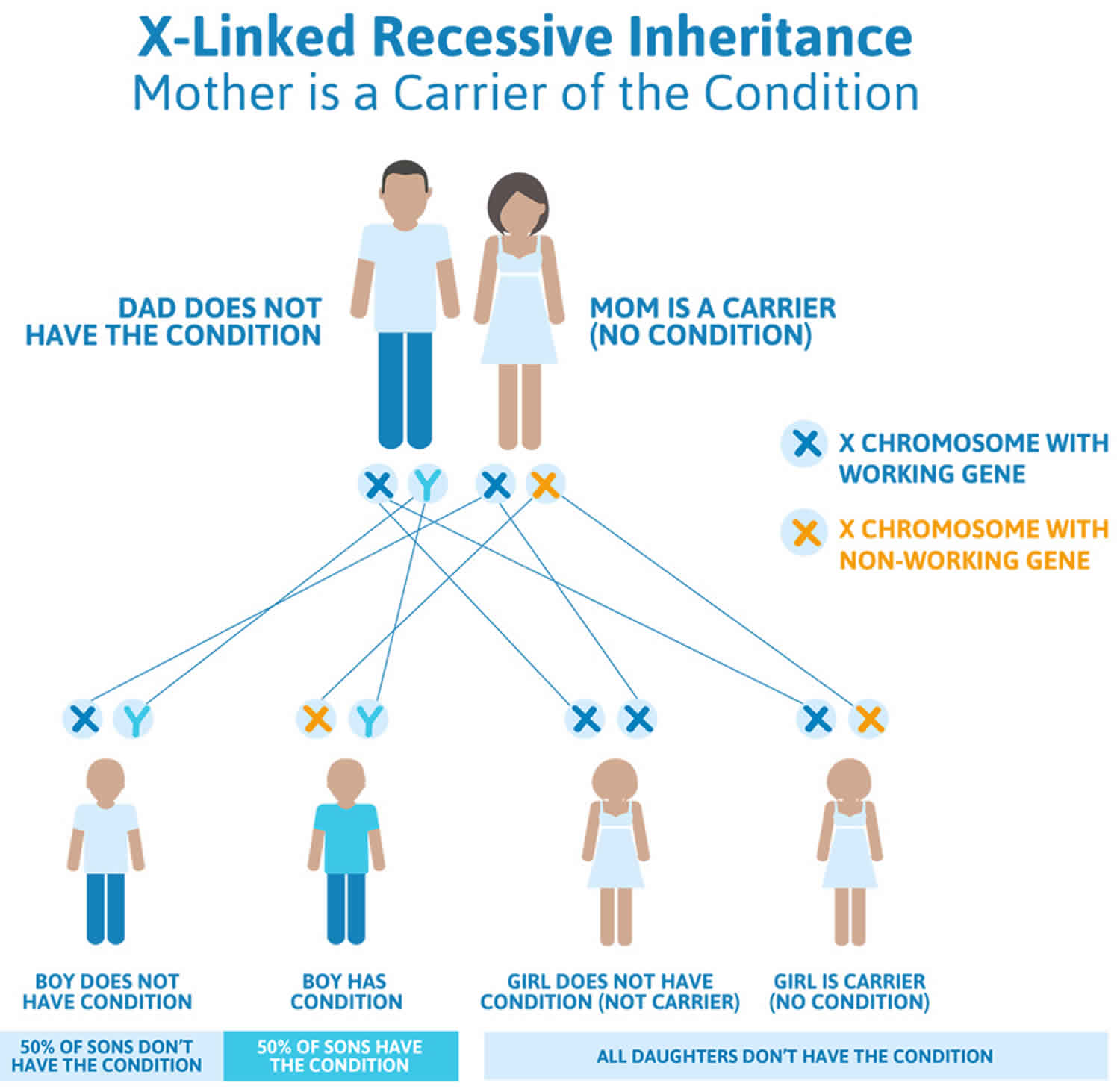
Adrenoleukodystrophy (ALD) is inherited as an X-linked recessive genetic disease. X-linked recessive genetic disorders are conditions caused by an abnormal gene on the X chromosome, one of the two sex chromosomes in each cell. Females have two X chromosomes but one of the X chromosomes is “turned off” and all of the genes on that chromosome are inactivated. Females who have a disease gene (ABCD1 gene) present on one of their X chromosomes are carriers for adrenoleukodystrophy (ALD). Carrier females often do not display symptoms of adrenoleukodystrophy (ALD) because it is usually the X chromosome with the abnormal gene that is turned off. Because females have two copies of the X chromosome, one altered copy of the ABCD1 gene in each cell usually does not cause any features of X-linked adrenoleukodystrophy; however, some females with one altered copy of ABCD1 gene have health problems associated with adrenoleukodystrophy (ALD). The signs and symptoms of X-linked adrenoleukodystrophy tend to appear at a later age in females than in males. Affected women usually develop features of the adrenomyeloneuropathy type.
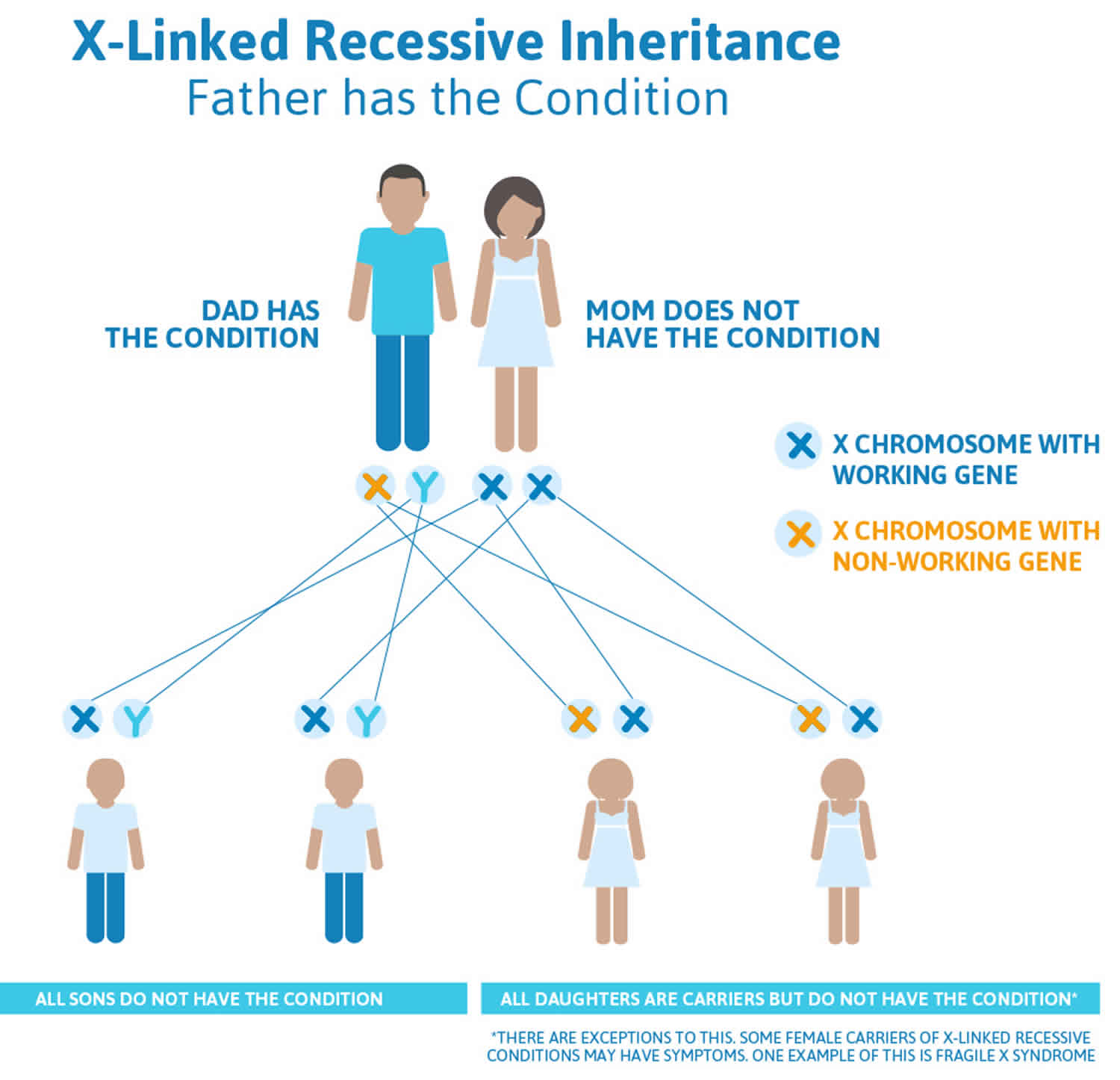
A male has only one X chromosome and if he inherits an X chromosome that contains a disease gene (ABCD1 gene), he will develop adrenoleukodystrophy (ALD). Males with X-linked disorders pass the disease gene to all of their daughters, who will be carriers. A male cannot pass an X-linked gene to his sons because males always pass their Y chromosome instead of their X chromosome to male offspring. Female carriers of an X-linked disorder have a 25% chance with each pregnancy to have a carrier daughter like themselves, a 25% chance to have a non-carrier daughter, a 25% chance to have a son affected with the disease, and a 25% chance to have an unaffected son.
Resources for locating a genetics professional in your community are available online:
- The National Society of Genetic Counselors (https://www.findageneticcounselor.com/) offers a searchable directory of genetic counselors in the United States and Canada. You can search by location, name, area of practice/specialization, and/or ZIP Code.
- The American Board of Genetic Counseling (https://www.abgc.net/about-genetic-counseling/find-a-certified-counselor/) provides a searchable directory of certified genetic counselors worldwide. You can search by practice area, name, organization, or location.
- The Canadian Association of Genetic Counsellors (https://www.cagc-accg.ca/index.php?page=225) has a searchable directory of genetic counselors in Canada. You can search by name, distance from an address, province, or services.
- The American College of Medical Genetics and Genomics (http://www.acmg.net/ACMG/Genetic_Services_Directory_Search.aspx) has a searchable database of medical genetics clinic services in the United States.
- The National Cancer Institute provides a Cancer Genetics Services Directory (https://www.cancer.gov/about-cancer/causes-prevention/genetics/directory), which lists professionals who provide services related to cancer genetics. You can search by type of cancer or syndrome, location, and/or provider name.
If you have a health condition that has not been diagnosed, you may be interested in the Undiagnosed Diseases Network (https://undiagnosed.hms.harvard.edu/). They have information about how to apply for this multicenter research study.
Figure 1. Adrenoleukodystrophy X-linked inheritance pattern
Adrenoleukodystrophy symptoms
Adrenoleukodystrophy symptoms can vary depending on age, gender, and the body tissues affected. The tissues that are most severely affected in adrenoleukodystrophy are myelin, blood, and the adrenal glands. Not all tissues are affected at the same time in all patients. In the world of genetic disorders, doctors group collections of symptoms into “phenotypes” based on the cells and tissues that are most severely affected by a gene abnormality. Individuals with the adrenoleukodystrophy gene may have different phenotypes. In adrenoleukodystrophy, the phenotypes are not mutually exclusive. In fact, it is common for individuals to have more than one phenotype at any given time.
The childhood cerebral form of adrenoleukodystrophy usually begins between four and eight years of age and symptoms include attention deficit disorder, progressive loss of intellectual function, and vision, hearing and motor deterioration. Adolescent cerebral adrenoleukodystrophy begins between 11 and 21 years of age and the symptoms are similar to the childhood cerebral type but the disease progresses more slowly. The adrenomyeloneuropathy (AMN) type of adrenoleukodystrophy usually begins in the late twenties and is characterized by difficulty walking, a progressive weakness and stiffness in the legs (paraparesis), a loss in ability to coordinate muscle movements, excessive muscle tone (hypertonia), vision loss, difficulty speaking dysarthria), seizures and adrenal insufficiency. Adult cerebral adrenoleukodystrophy can begin between the twenties and fifties with symptoms similar to schizophrenia with dementia. Individuals with adrenal insufficiency only do not initially have neurological problems, but symptoms such as those seen in adrenomyeloneuropathy usually develop later. Adrenoleukodystrophy in females usually begins later in life and symptoms can vary greatly from mild to severe, but usually do not include adrenal insufficiency.
There are 4 primary phenotypes that can occur in MALES with the adrenoleukodystrophy gene:
1. Asymptomatic phenotype:
All individuals with the adrenoleukodystrophy gene are free of clinical symptoms for at least the first three years of life. And some may continue to have no symptoms. But the percentage of asymptomatic men and women decreases with age.
2. Adrenomyeloneuropathy (AMN) phenotype symptoms:
Walking and balance problems. General leg weakness and stiffness progresses into walking difficulty and reduced balance. With the weakening of leg muscles, changes in gait, or how a person walks, becomes noticeable. The use of mobility devices, such as canes, walkers, and wheelchairs may become necessary.
Pain, numbness, or tingling in the legs. Mild to moderate weakness of the arms/hands Urinary problems or incontinence and bowel urgency or incontinence Sexual dysfunction, or the inability to obtain or maintain an erection.
Adrenomyelopathy other symptoms include:
- Difficulty controlling urination
- Possible worsening muscle weakness or leg stiffness
- Problems with thinking speed and visual memory
3. Adrenal insufficiency (Addison’s disease) phenotype symptoms:
Adrenal insufficiency occurs as a result of permanent injury to the adrenal glands. Most men with adrenoleukodystrophy will eventually develop adrenal insufficiency over their lifespan. Women develop adrenal insufficiency much less commonly. Although it is easily treatable, adrenal insufficiency can be life-threatening if it is not recognized promptly. Symptoms are often non-specific and can include weakness/fatigue, nausea, abdominal pain, and low blood pressure. Darkening of the skin is also common.
Adrenal gland failure (Addison’s disease type) symptoms include:
- Coma
- Decreased appetite
- Increased skin color
- Loss of weight and muscle mass (wasting)
- Muscle weakness
- Vomiting
Adrenal insufficiency is sometimes referred to as Addison’s disease (based on the doctor, Thomas Addison MD, who first described it). There are many causes of adrenal insufficiency in the general population. adrenoleukodystrophy is the cause of approximately 33% of all cases of adrenal insufficiency. This means that not all patients diagnosed with adrenal insufficiency have adrenoleukodystrophy. Nonetheless, all patients with adrenal insufficiency should be tested for adrenoleukodystrophy (and vice versa).
4. Cerebral adrenoleukodystrophy symptoms:
Affected boys’ symptoms may include “spacing out” in school: inattention, deterioration in handwriting skills, and decreased school performance; difficulty in understanding speech (though sound perception is normal); difficulty in reading and understanding written material; clumsiness; visual disturbances and occasionally double-vision; and aggressive or unexplained inappropriate behavior. In some boys, seizures may be the first symptom. Symptom severity varies from patient to patient and is not determined by phenotype. Even identical twins may have different experiences with symptom onset and severity. Other symptoms may include:
- Behavioral problems
- Hyperactivity
- Eye pain/Childhood onset migraines
- Recurring viral infections
- Lethargy, tires easily, clumsiness
- Hypoglycemia
- Tanning or bronzing of the skin
- Adrenal insufficiency
- Attention deficit and hyperactivity disorder (ADHD)
- Changes in muscle tone, especially muscle spasms and uncontrolled movements
- Crossed eyes
- Handwriting that gets worse
- Difficulty at school
- Difficulty understanding what people are saying
- Hearing loss
- Worsening nervous system damage, including coma, decreased fine motor control, and paralysis
- Seizures
- Swallowing difficulties
- Visual impairment or blindness
Adrenoleukodystrophy diagnosis
X-adrenoleukodystrophy is diagnosed by a simple blood test that analyzes the amount of very long chain fatty acids (VLCFAs); the levels of these very long chain fatty acids (VLCFAs) are elevated in in 99% of males with adrenoleukodystrophy and in approximately 85% of female carriers of the abnormal ABCD1 gene. While the test is accurate in males, in about 15-20% of women who are proven carriers, the test shows normal results and thus gives a “false negative” result. A DNA-based blood test is available. This test permits accurate identification of carriers by genetic testing, and if it is normal can assure a woman that she is not a carrier.
Molecular testing for the ABCD1 gene is available and is used primarily to confirm a diagnosis if other testing is not conclusive, to provide genetic counseling to family members and for prenatal diagnosis.
Additionally, the patient will be evaluated for adrenal insufficiency (by another blood test), as this is a common symptom of the disease that can be corrected. Adrenal function tests are abnormal in 90% of boys with adrenoleukodystrophy who have neurologic symptoms and in approximately 70% of men with adrenomyeloneuropathy.
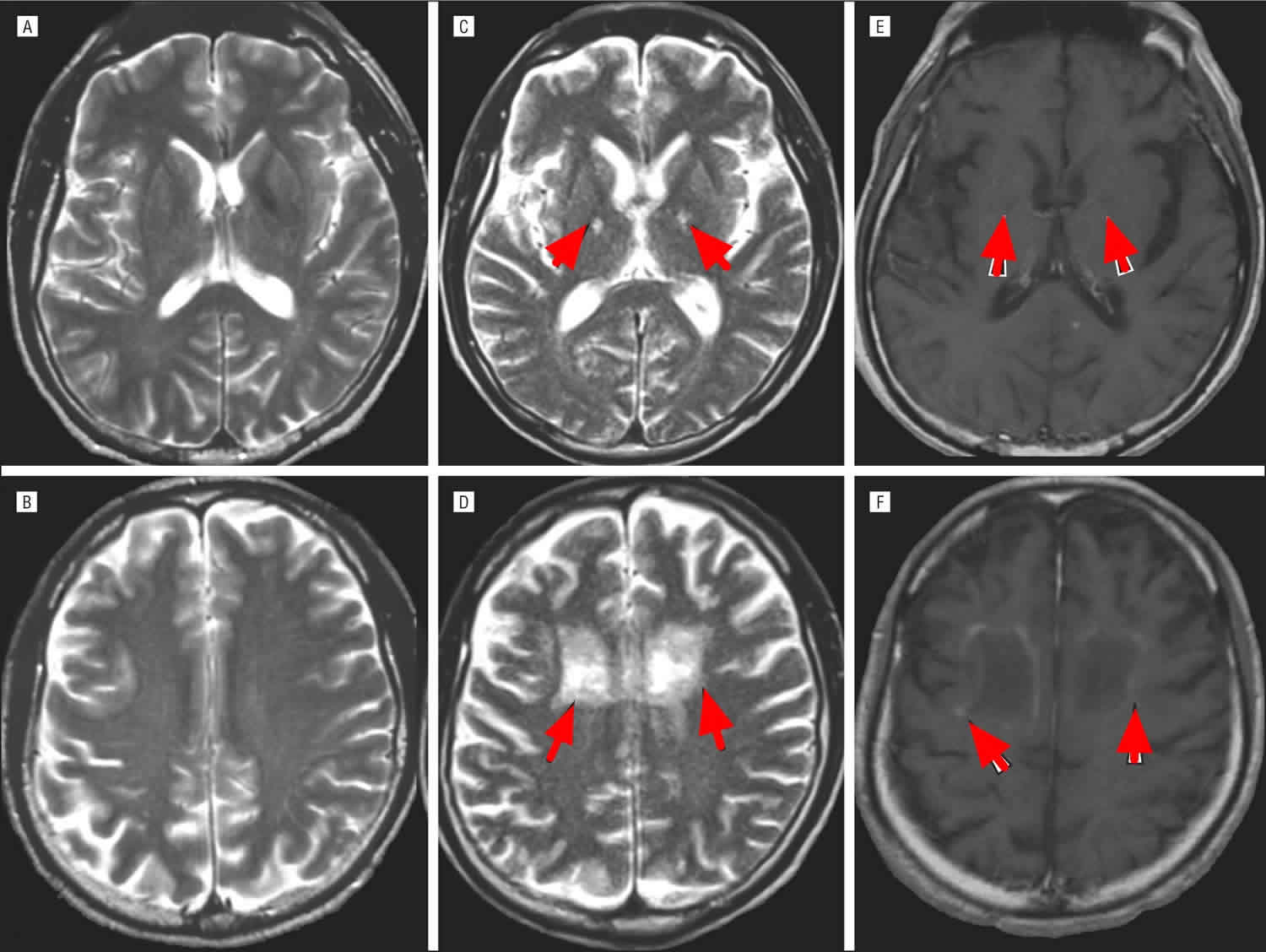
If the blood test suggests X-adrenoleukodystrophy, then generally an MRI will be performed in order to assess cerebral involvement. Additionally, the patient will be evaluated for adrenal insufficiency (by another blood test), as this is a common symptom of the disease that can be corrected.
Adrenoleukodystrophy prognosis
Prognosis for patients with childhood cerebral X-adrenoleukodystrophy is generally poor due to progressive neurological deterioration unless bone marrow transplantation is performed early. It leads to a long-term coma (vegetative state) about 2 years after nervous system symptoms develop. The child can live in this condition for as long as 10 years until death occurs. Death usually occurs within 1 to 10 years after the onset of symptoms.
X-linked cerebral adrenoleukodystrophy – left untreated, all but 10% of patients are bedridden, blind, lacking speech and require fulltime care, dying within 2-5 years 4. Arrested X-linked cerebral adrenoleukodystrophy may enter a phase of rapid neurological deterioration at any time.
Adult-onset adrenomyeloneuropathy (AMN) will progress over decades.
The deterioration rate is different for each patient. Some will continue to walk and talk several years before succumbing to the effects of the disease, and will then suddenly deteriorate very quickly into a dependent state. Others will deteriorate into the dependent state within a few months of diagnosis. There is no way to predict how quickly or slowly the process will happen.
Adrenoleukodystrophy life expectancy
Medical guidelines say that on average, boys with symptomatic cerebral adrenoleukodystrophy live for 2-4 years. But many boys have gone on to live for longer periods. There are boys who have symptomatic adrenoleukodystrophy that are living in their teens and early 20s with quality of life 5.
Adrenoleukodystrophy treatment
1. The first treatment deals with the replacement of the faulty adrenal function often present in adrenoleukodystrophy. The adrenal glands are next to the kidney, and produce certain important hormones. If the adrenal functions are not properly functioning, these hormones need to be replaced. The abnormal adrenal function is treated with corticosteroid replacement therapy.
2. Lorenzo’s oil. This is a mixture of two oils (glyceryl trieucate, or GTE, and glyceryl trioleate, or GTO). It is thought to aid in the normalization of the fatty acid levels. However, this oil does not seem to alter the progression of the disease once the brain is involved. It is not yet clear if Lorenzo’s oil could prevent progression prior to symptoms. Lorenzo’s Oil has been successfully used as a therapy for boys with ALD. If started early, it can help lessen the risk of developing the childhood cerebral form of ALD. This oil, along with a low-fat diet, can help to reduce the very long chain fatty acids that accumulate. Lorenzo’s Oil is not approved by the FDA. To learn more about obtaining the Lorenzo’s Oil, please visit (https://www.myelin.org/lorenzos-oil/). Financial assistance through the Myelin Project is also available. Eating a diet low in very-long-chain fatty acids and taking special oils can lower the blood levels of very-long-chain fatty acids, such as Lorenzo’s Oil, which may be help slow the progression of ALD disease.
3. Bone marrow transplantation. This is the most successful treatment for adrenoleukodystrophy so far identified. Bone marrow transplantation has been successful in individuals who are in the early stages of adrenoleukodystrophy. However, it must be noted that bone marrow transplantation has not been successful in patients with advanced neurological involvement, but only in patients in earlier stages of the disease. Although this procedure is considered risky, successful transplants are possible with early intervention. Outcomes depend on the child’s clinical status at the time of the evaluation, along with interpretation of the brain MRI. Only about roughly 30% of boys who undergo transplant will go on to develop childhood cerebral disease. Currently, doctors typically will not perform stem cell transplantation on adults with adrenoleukodystrophy, generally because the risks of the treatment are considered to outweigh the potential benefits. But as transplantation technology improves and becomes safer, it is possible that stem cell transplantation will be available for men with adrenomyelonueropathy (AMN).
4. Medications. Your doctor may prescribe medications to help relieve symptoms, including stiffness and seizures.
5. Exercise and physical therapy. Patients who experience walking difficulties may benefit from seeing a physical therapist, who can provide exercises to strengthen muscles and improve walking ability.
Affected individuals can benefit from supportive care from psychologists, educators, physical therapists, urologists, and family and vocational counselors. Genetic counseling is recommended for affected individuals and their family members.
Resources for locating a genetics professional in your community are available online:
- The National Society of Genetic Counselors (https://www.findageneticcounselor.com/) offers a searchable directory of genetic counselors in the United States and Canada. You can search by location, name, area of practice/specialization, and/or ZIP Code.
- The American Board of Genetic Counseling (https://www.abgc.net/about-genetic-counseling/find-a-certified-counselor/) provides a searchable directory of certified genetic counselors worldwide. You can search by practice area, name, organization, or location.
- The Canadian Association of Genetic Counsellors (https://www.cagc-accg.ca/index.php?page=225) has a searchable directory of genetic counselors in Canada. You can search by name, distance from an address, province, or services.
- The American College of Medical Genetics and Genomics (http://www.acmg.net/ACMG/Genetic_Services_Directory_Search.aspx) has a searchable database of medical genetics clinic services in the United States.
- The National Cancer Institute provides a Cancer Genetics Services Directory (https://www.cancer.gov/about-cancer/causes-prevention/genetics/directory), which lists professionals who provide services related to cancer genetics. You can search by type of cancer or syndrome, location, and/or provider name.
If you have a health condition that has not been diagnosed, you may be interested in the Undiagnosed Diseases Network (https://undiagnosed.hms.harvard.edu/). They have information about how to apply for this multicenter research study.
How does blood or marrow transplant work for adrenoleukodystrophy?
Bone marrow transplant or blood stem cell transplant, can stop the adrenoleukodystrophy from causing more damage. Bone marrow transplant replaces the blood-forming cells (stem cells) that are missing the important protein with healthy ones. With healthy blood-forming cells, the body is able to break down fat-based substances normally. This keeps the brain, spinal cord and nervous system from more damage. But, bone marrow transplant can’t fix any damage that has already happened.
Allogeneic transplant is used for adrenoleukodystrophy. This type of transplant uses healthy, blood-forming cells donated by someone else to replace the unhealthy blood-forming cells. These healthy cells can come from a family member, unrelated donor or umbilical cord blood. First, you get chemotherapy (chemo), with or without radiation, to kill the unhealthy cells. Then, the healthy, donated cells are given to you through an intravenous (IV) catheter. The new cells travel to the inside of the bones and begin to make healthy cells.
The entire transplant process, from the start of chemo or radiation, until hospital discharge, can last weeks to months. This is followed by many months of recovery near the transplant center and at home. The transplant team will closely care for you to prevent and treat any complications.
When should I see a transplant doctor?
Most people have a better chance of a cure if they have a bone marrow transplant soon after diagnosis. You or your child should see a transplant doctor as soon as you’re diagnosed.
Your first appointment with a transplant doctor
At the first appointment, the transplant doctor will:
- Review your or your child’s medical history
- Talk with you about treatment options
- Discuss the risks and benefits of transplant
- Recommend the best time for you or your child to get a transplant and prepare for treatment
- Start a donor search
- Schedule appointments with other doctors, like a neurologist.
Questions to ask your doctor
Ask questions so you understand your treatment options and can make decisions that are best for you and your child. Questions you may want to ask include:
- What are the chances transplant will stop the adrenoleukodystrophy from causing more damage?
- What are the possible side effects of transplant? How can they be reduced?
- How might my or my child’s quality of life change over time, with or without transplant?
- Adrenoleukodystrophy. https://rarediseases.org/rare-diseases/adrenoleukodystrophy/[↩]
- X-linked adrenoleukodystrophy. https://www.orpha.net/consor/cgi-bin/Disease_Search.php?lng=EN&data_id=761&Disease_Disease_Search_diseaseGroup=adrenoleukodystrophy&Disease_Disease_Search_diseaseType=Pat&Disease(s)/group%20of%20diseases=X-linked-adrenoleukodystrophy&title=X-linked%20adrenoleukodystrophy&search=Disease_Search_Simple[↩]
- What is ALD? http://www.aldfoundation.org/ald.php[↩]
- X-linked cerebral adrenoleukodystrophy. https://www.orpha.net/consor/cgi-bin/Disease_Search.php?lng=EN&data_id=16884&Disease_Disease_Search_diseaseGroup=adrenoleukodystrophy&Disease_Disease_Search_diseaseType=Pat&Disease(s)/group%20of%20diseases=X-linked-cerebral-adrenoleukodystrophy&title=X-linked%20cerebral%20adrenoleukodystrophy&search=Disease_Search_Simple[↩]
- PRACTICAL INFORMATION FOR MALES WITH SYMPTOMATIC ALD. http://www.aldlife.org/wp-content/uploads/2015/04/Practical-Information-for-Males-with-Symptomatic-ALD.pdf[↩]





{kind=link}