
Contents
What is ageusia
Ageusia means the loss of the sense of taste. People can also experience a reduced ability to taste sweet, sour, bitter, salty, and umami—a condition called hypogeusia. However, true taste loss is rare. Most often, people are experiencing a loss of smell instead of a loss of taste. Ageusia is usually results from conditions that affect the tongue, usually caused by a very dry mouth. Conditions causing dry mouth include Sjögren’s syndrome, heavy smoking (especially pipe smoking), radiation therapy to the head and neck, dehydration, and use of drugs (including antihistamines and the antidepressant amitriptyline). Nutritional deficiencies, such as decreased zinc, copper, and nickel levels, can alter both taste and smell.
In Bell palsy (a disorder in which half of the face is paralyzed), the sense of taste is often impaired on the front two thirds of one side of the tongue (the side affected by the palsy). But this loss may not be noticed because taste is normal or increased in the rest of the tongue. Burns to the tongue may temporarily destroy taste buds. Neurologic disorders, including depression and seizures, may impair taste.
More than 200,000 people visit a doctor each year for problems with their ability to taste or smell. Scientists believe that up to 15 percent of adults might have a taste or smell problem, but many don’t seek a doctor’s help. The prevalence of disorders of taste and smell in the U.S. general population has been estimated from the US National Health and Nutrition Examination Survey (NHANES) 2011-2014 protocol. A total of 3519 men and women aged 40 and older were tested with a scratch-and-sniff olfactory test; smell, taste, and combined smell and taste impairment had estimated prevalences of 13.5%, 17.3%, and 2.2%, respectively 1.
It is also known that chemosensory dysfunction deteriorates with age starting in the fifth decade of life 2. Given the aging of the US population, therefore, it stands to reason that a significant and increasing number of individuals will experience age-related sensory loss 3. A 2002 study showed that the prevalence of objective olfactory impairment in adults older than 53 years is 24.5% and grows more prevalent with age, reaching 62.5 % in those aged 80-97 years. Extrapolating from these values, there are currently 14 million older adults with some degree of olfactory impairment. Self-reported impairment in this study was only 9.5%, which supports the need for more accurate data based on objective measures 4.
The senses of taste and smell are very closely related. Most people who go to the doctor because they think they have lost their sense of taste are surprised to learn that they have a smell disorder instead.
Taste disorders can weaken or remove an early warning system that most of us take for granted. Taste helps you detect spoiled food or liquids and, for some people, the presence of ingredients to which they are allergic.
Ageusia (loss of taste) can create serious health issues. A distorted sense of taste can be a risk factor for heart disease, diabetes, stroke, and other illnesses that require sticking to a specific diet. When taste is impaired, a person may change his or her eating habits. Some people may eat too little and lose weight, while others may eat too much and gain weight.
Ageusia (loss of taste) can cause you to add too much sugar or salt to make food taste better. This can be a problem for people with certain medical conditions, such as diabetes or high blood pressure. In severe cases, loss of taste can lead to depression.
If you are experiencing a taste disorder, talk with your doctor.
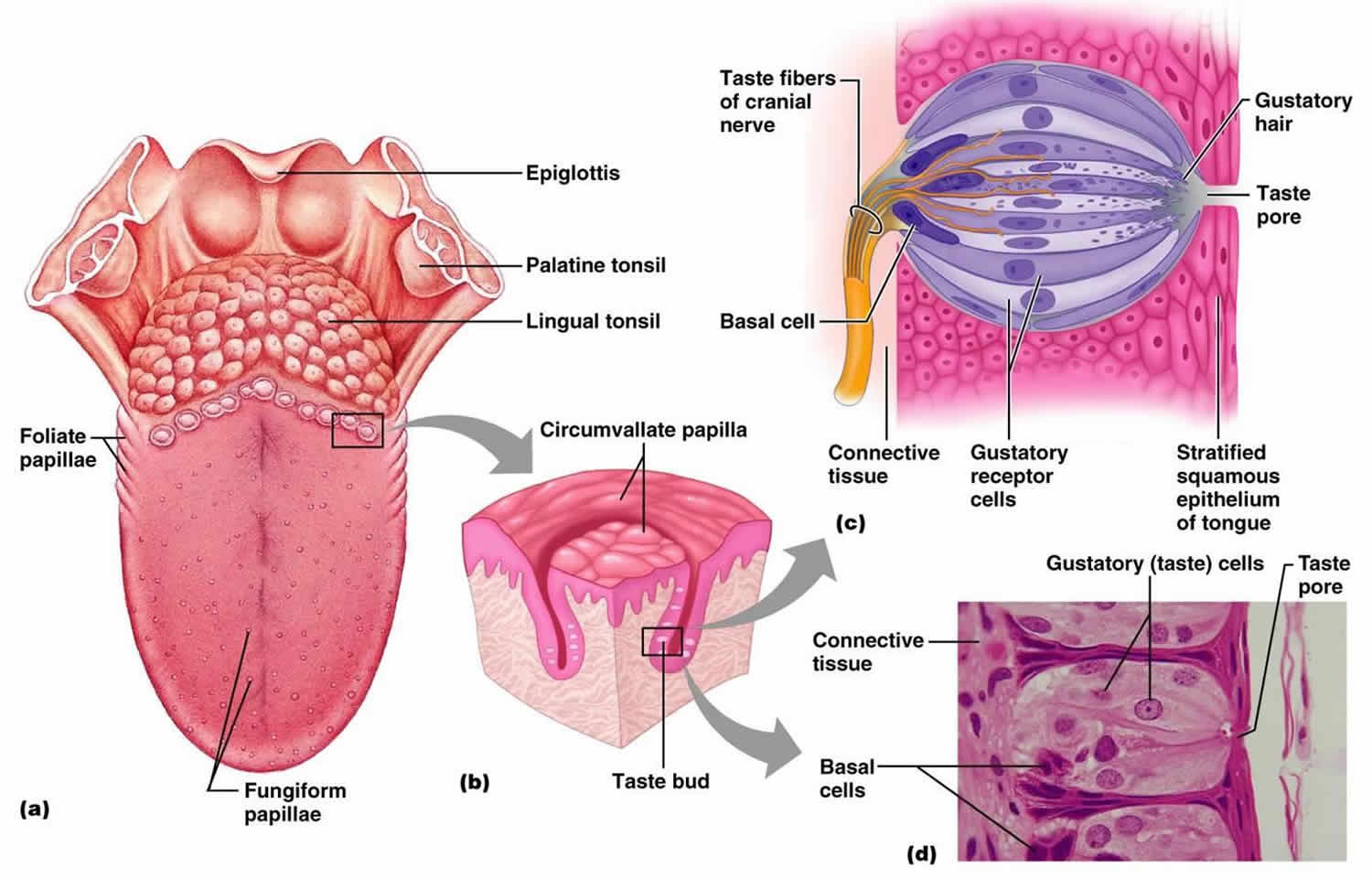
Figure 1. Taste buds on your tongue
How does your sense of taste work?
Your ability to taste comes from tiny molecules released when you chew, drink, or digest food; these molecules stimulate special sensory cells in the mouth and throat. These taste cells, or gustatory cells, are clustered within the taste buds of the tongue and roof of the mouth, and along the lining of the throat. Many of the small bumps on the tip of your tongue contain taste buds. At birth, you have about 10,000 taste buds, but after age 50, you may start to lose them.
Taste perception is mediated by individual taste buds, with 50-100 tightly packed cells in each taste bud. Taste buds are made up of modified epithelial cells and chemical receptor cells; however, the receptor cells are not direct neurons as in the olfactory system. Taste bud cells are classified into cell types I-IV and include supporting cells (types I and II), receptor cells (type III), and basal progenitor cells (type IV) 5. These cells have a life span of approximately 10 days and arise continuously from the underlying basal cell layer in a process of constant turnover, similar to that of olfactory receptor neurons. Any bud may contain any of the receptor cells necessary to identify each different taste.
When the taste cells are stimulated, they send messages through three specialized taste nerves to the brain, where specific tastes are identified. Taste cells have receptors that respond to one of at least five basic taste qualities: sweet, sour, bitter, salty, and umami. Umami, or savory, is the taste you get from glutamate, which is found in chicken broth, meat extracts, and some cheeses. A common misconception is that taste cells that respond to different tastes are found in separate regions of the tongue. In humans, the different types of taste cells are scattered throughout the tongue.
Taste quality is just one way that you experience a certain food. Another chemosensory mechanism, called the common chemical sense, involves thousands of nerve endings, especially on the moist surfaces of the eyes, nose, mouth, and throat. These nerve endings give rise to sensations such as the coolness of mint and the burning or irritation of chili peppers. Other specialized nerves create the sensations of heat, cold, and texture. When you eat, the sensations from the five taste qualities, together with the sensations from the common chemical sense and the sensations of heat, cold, and texture, combine with a food’s aroma to produce a perception of flavor. It is flavor that lets you know whether you are eating a pear or an apple.
Most people who think they have a taste disorder actually have a problem with smell. When you chew food, aromas are released that activate your sense of smell by way of a special channel that connects the roof of the throat to the nose. If this channel is blocked, such as when your nose is stuffed up by a cold or flu, odors can’t reach sensory cells in the nose that are stimulated by smells. As a result, you lose much of our enjoyment of flavor. Without smell, foods tend to taste bland and have little or no flavor.
Ageusia causes
Some people are born with taste disorders, but most develop them after an injury or illness. Among the causes of taste problems are:
- Upper respiratory and middle ear infections
- Radiation therapy for cancers of the head and neck
- Exposure to certain chemicals, such as insecticides and some medications, including some common antibiotics and antihistamines
- Head injury
- Some surgeries to the ear, nose, and throat (such as middle ear surgery) or extraction of the third molar (wisdom tooth)
- Poor oral hygiene and dental problems.
Much of what is perceived as ageusia (a loss of the sense of taste) is truly a primary defect in olfaction (sense of smell) resulting in an alteration of flavor. The components that comprise the sensation of flavor include the food’s smell, taste, texture, and temperature. Each of these sensory modalities is stimulated independently to produce a distinct flavor when food enters the mouth.
Taste may be enhanced by tongue movements, which increase the distribution of the substance over a greater number of taste buds. Adaptation in taste perception exerts a greater influence than in other sensory modalities.
Other than smell dysfunction, the most frequent causes of taste dysfunction are prior upper respiratory tract infection, head injury, and idiopathic causes, but many other causes can be responsible.
Lesions at any site from the mucosa, taste buds, unmyelinated nerves, or cranial nerves to the brain stem may impair the ability to taste.
Oral cavity and mucosal disorders including oral infections, inflammation, and radiation-induced mucositis can impair taste sensation. The site of injury with radiotherapy is probably the microvilli of the taste buds, not the taste buds themselves, since taste buds are thought to be radioresistant.
Poor oral hygiene is a leading cause of hypogeusia and cacogeusia. Viral, bacterial, fungal, and parasitic infections may lead to taste disturbances because of secondary taste bud involvement.
Normal aging produces taste loss due to changes in taste cell membranes involving altered function of ion channels and receptors rather than taste bud loss 6.
More than 200 medications have been associated with taste disorders 7. Clinicians need to be aware of this, especially with regard to patients taking numerous drugs 8.
Cancers of the head and neck, as well as of other sites, are associated with decreased appetite and inability to appreciate flavors.
Use of dentures or other palatal prostheses may impair sour and bitter perception, and tongue brushing has been shown to decrease taste acuity.
Surgical manipulation may alter taste permanently or temporarily. Resection of the tongue and/or portions of the oral cavity, most commonly for reasons of malignancy, decreases the number of taste buds. Radiation and chemotherapy damage taste receptors and decrease salivary flow, altering taste perception. In otologic surgery, stretching or transection of the chorda tympani nerve may result in temporary dysgeusia. Bilateral injury still may not result in permanent taste dysfunction, because of the alternate innervation through the otic ganglion to the geniculate ganglion via the greater superficial petrosal nerve.
Gastric bypass surgery can also have adverse olfactory and gustatory effects. In a study by Graham et al 9 of 103 patients who underwent Roux-en-Y gastric bypass, sensory changes in taste and smell were reported by 73% and 42% of these individuals, respectively, although patients seem to have less olfactory loss if the bypass is done laparoscopically.
Nutritional deficiencies are involved in taste aberrations. Decreased zinc, copper, and nickel levels can correlate with taste alterations. Nutritional deficiencies may be caused by anorexia, malabsorption, and/or increased urinary losses.
Endocrine disorders also are involved in taste and olfactory disorders. Diabetes mellitus, hypogonadism, Sjögren syndrome, and pseudohypoparathyroidism may decrease taste sensation, while hypothyroidism and adrenal cortical insufficiency may increase taste sensitivity. Hormonal fluctuations in menstruation and pregnancy also influence taste.
AIDS patients often complain of alterations in taste, and detection thresholds of glutamic acid and hydrochloride are higher in patients suffering from AIDS 5.
Heredity is involved in some aspects of gustation. The ability to taste phenylthiourea (bitter) and other compounds with an –N-C= group is an autosomal dominant trait. Studies have shown that phenylthiourea tasters detect saccharin, potassium chloride (KCl), and caffeine as more bitter. Type I familial dysautonomia (ie, Riley-Day syndrome) causes severe hypogeusia or ageusia because of the absence of taste bud development.
Direct nerve or CNS damage, as in multiple sclerosis, facial paralysis, and thalamic or uncal lesions, can decrease taste perception.
Many other diseases can affect gustation (eg, lichen planus, aglycogeusia, Sjögren syndrome, renal failure with uremia and dialysis, erythema multiforme, geographic tongue, cirrhosis).
Ageusia symptoms
Symptoms can range from the not being able to smell or taste at all to the reduced ability to smell or taste specific things that are sweet, sour, bitter or salty. In some cases, normally pleasant tastes or smells may become unpleasant.
Ageusia diagnosis
Both taste and smell disorders are diagnosed by an otolaryngologist (sometimes called an ENT doctor), a doctor of the ear, nose, throat, head, and neck. An otolaryngologist can determine the extent of your taste disorder by measuring the lowest concentration of a taste quality that you can detect or recognize. You may be asked to compare the tastes of different substances or to note how the intensity of a taste grows when a substance’s concentration is increased.
Scientists have developed taste tests in which the patient responds to different chemical concentrations. This may involve a simple “sip, spit, and rinse” test, or chemicals may be applied directly to specific areas of the tongue.
An accurate assessment of your taste loss will include, among other things, a physical examination of your ears, nose, and throat; a dental examination and assessment of oral hygiene; a review of your health history; and a taste test supervised by a health care professional.
Ageusia treatment
Diagnosis by an ENT specialist is important to identify and treat the underlying cause of your ageusia. If a certain medication is the cause, stopping or changing your medicine may help eliminate the problem. Do not stop taking your medications unless directed by your doctor. Often, the correction of a general medical problem can correct the ageusia. For example, people who lose their sense of taste because of respiratory infections or allergies may regain it when these conditions resolve. Occasionally, a person may recover his or her sense of taste spontaneously. Proper oral hygiene is important to regaining and maintaining a well-functioning sense of taste. If your taste disorder can’t be successfully treated, counseling may help you adjust to your problem.
If you lose some or all of your sense of taste, here are things you can try to make your food taste better:
- Prepare foods with a variety of colors and textures.
- Use aromatic herbs and hot spices to add more flavor; however, avoid adding more sugar or salt to foods.
- If your diet permits, add small amounts of cheese, bacon bits, butter, olive oil, or toasted nuts on vegetables.
- Avoid combination dishes, such as casseroles, that can hide individual flavors and dilute taste.
- Liu G, Zong G, Doty RL, Sun Q. Prevalence and risk factors of taste and smell impairment in a nationwide representative sample of the US population: a cross-sectional study. BMJ Open. 2016 Nov 9. 6 (11):e013246[↩]
- Zhang C, Wang X. Initiation of the age-related decline of odor identification in humans: a meta-analysis. Ageing Res Rev. 2017 Nov. 40:45-50[↩]
- Boesveldt S, Lindau ST, McClintock MK, Hummel T, Lundstrom JN. Gustatory and olfactory dysfunction in older adults: a national probability study. Rhinology. 2011 Aug. 49(3):324-30[↩]
- Murphy C, Schubert CR, Cruickshanks KJ, Klein BE, Klein R, Nondahl DM. Prevalence of olfactory impairment in older adults. JAMA. 2002 Nov 13. 288(18):2307-12[↩]
- Feng P, Huang L, Wang H. Taste bud homeostasis in health, disease, and aging. Chem Senses. 2014 Jan. 39(1):3-16.[↩][↩]
- Barresi M, Ciurleo R, Giacoppo S, Foti Cuzzola V, Celi D, Bramanti P. Evaluation of olfactory dysfunction in neurodegenerative diseases. J Neurol Sci. 2012 Dec 15. 323(1-2):16-24.[↩]
- Wang T, Glendinning J, Grushka M, Hummel T, Mansfield K. From the Cover: Drug-Induced Taste Disorders in Clinical Practice and Preclinical Safety Evaluation. Toxicol Sci. 2017 Apr 1. 156 (2):315-24.[↩]
- Zerrweck C, Gallardo VC, Calleja C, Sepulveda E, Guilber L. Gross Olfaction Before and After Laparoscopic Gastric Bypass. Obes Surg. 2017 Nov. 27 (11):2988-92[↩]
- Graham L, Murty G, Bowrey DJ. Taste, smell and appetite change after Roux-en-Y gastric bypass surgery. Obes Surg. 2014 Mar 8.[↩]





{kind=link}