Contents
Annular pancreas
Annular pancreas is a rare birth defect (congenital defect) that results in an abnormal ring or collar of pancreatic tissue that completely or incompletely encircles the duodenum (the part of the small intestine that connects to stomach) in continuity with the pancreatic head that affects males more commonly than females (65% cases are males) 1, 2, 3, 4, 5, 6, 7, 8. Annular pancreas is usually located above the papilla of Vater (also known as the hepatopancreatic ampulla) in approximately 85% of diagnosed cases 9. Of annular pancreas cases, 25% form a complete pancreatic ring, and 75% have a partial ring 10. The normal position of the pancreas is next to, but not surrounding the duodenum (Figure 4). Your pancreas can still function, but the abnormal ring or collar of pancreatic tissue can cause a number of symptoms. Annular pancreas can constrict the duodenum and block or impair the flow of food to the rest of your intestines. Symptoms from annular pancreas are nausea, vomiting, feeling of fullness after eating, and feeding problems especially in newborn infants (an infant less than four weeks old). People with annular pancreas may remain asymptomatic (have no symptoms) or present with pancreatitis, duodenal outlet obstruction, gastrointestinal bleeding, or abdominal pain alone 11, 12, 13, 14, 15, 16. Annular pancreas is generally symptomatic in children, especially in infants less than four weeks olds, and in adults it is usually asymptomatic (approximately 50% of the patients may be asymptomatic for life) and only found as an incidental finding on imaging for another condition. Surgical bypass of the obstructing segment of the duodenum is the usual treatment for annular pancreas.
Annular pancreas is a rare birth defect (congenital defect) caused by a failure of the ventral bud (ventral anlage) to rotate clockwise with the duodenum during the embryonic development (embryogenesis), resulting in a thin ring of pancreatic tissue that encircles, either completely or partially, the second part of the duodenum (the first part of the small intestine) 17. Conditions that may be associated with annular pancreas include 18:
- Down syndrome
- Excess amniotic fluid during pregnancy (polyhydramnios)
- Other congenital gastrointestinal problems such as intestinal atresia, pancreatico-biliary malrotation, and pancreas divisum
- Pancreatitis
The exact number of people born with annular pancreas is unknown, but older studies have reported the prevalence of annular pancreas in 3 per 20,000 autopsies and 3 per 24,519 surgical cases 8, 19. With the advent of newer and improved diagnostic modalities, annular pancreas is being recognized more frequently 4, 20, 21, 22.
Histologically annular pancreas has been classified into two types 9, 23:
- An intramural annular pancreas, in which pancreatic tissue is interposed to the muscle fibers in the duodenal wall, with small ducts that drain into the duodenum,
- An extramural annular pancreas, where the ventral pancreatic duct surrounds the duodenum and joins the major pancreatic duct.
Annular pancreas has also been classified into a complete or incomplete type 16:
- Complete type annular pancreas shows pancreatic parenchyma or annular pancreatic duct completely encircling the second part of the duodenum confirmed by macroscopic inspection,
- Incomplete type annular pancreas demonstrates partial pancreatic annulus does not surround the duodenum completely, giving a ‘crocodile jaw’ appearance confirmed by endoscopic retrograde cholangiopancreatography (ERCP) or surgical evaluation.
Depending on how the major pancreatic duct opens into the duodenum four distinct types of annular pancreas can be found 24, 25, 26:
- Type 1 the annular pancreatic duct (APD) opens itself normally into Wirsung’s duct;
- Type 2 the annular pancreatic duct (APD) opens itself into the common bile duct;
- Type 3 the annular pancreatic duct (APD) opens itself into the common bile duct and the duct of Wirsung is missing;
- Type 4 the annular pancreatic duct (APD) opens itself into Santorini’s duct.
The annular pancreatic duct (APD) commonly drains in the main pancreatic duct (MPD) but can communicate with the intrapancreatic common bile duct, the duct of Santorini, or the duct of Wirsung 27.
Gromski and colleagues 28 from Indiana University recently published their experience of 46 patients with annular pancreas over a twenty-two year period. Nearly half of patients in their series had coexisting pancreas divisum 28. Roughly one-third of their patients had findings of chronic pancreatitis. They made the diagnosis of annular pancreas when they could visualize a pancreatic duct wrapping around the duodenum on endoscopic retrograde cholangiopancreatography (ERCP). The annular ductal branch originated from the ventral (main) pancreatic duct in 88% of those who received a formal pancreatogram 28. They also noted duodenal narrowing in 88% of cases, but only 5% had a duodenal stricture severe enough to restrict the flow of gastric chyme. Pancreaticobiliary neoplasms occur at higher rates in patients with an annular pancreas. Seven patients from this series were diagnosed with malignancies following biopsy on index ERCP. Nonetheless, causality between annular pancreas and neoplasm cannot be determined from these studies because many patients were sent to large referral centers once malignancy was suspected 28.
Magnetic resonance cholangiopancreatography (MRCP) and endoscopic retrograde cholangiopancreatography (ERCP) are the most prevalent method of diagnosing annular pancreas by the gastroenterologist. When the annular pancreatic duct encircling and extending to the right side of the duodenum is identified by MRCP or ERCP, the diagnosis of annular pancreas is established 27.
Endoscopic retrograde cholangiopancreatography (ERCP) is considered as the gold standard for the diagnosis of annular pancreas as it provides visualization of the descending duodenum and the pancreatic ductal system along with the major and minor papilla 29, 30. Duodenal narrowing is usually located just proximal to the major papilla, and the minor papilla is usually situated at the proximal rim of the annular ring. In the majority of patients, the duct of the annular pancreas communicates with the main pancreatic duct arising from the major papilla. However, ERCP via the major papilla will not be able to diagnose annular pancreas in patients where the annular duct opens into the minor papilla or directly into the duodenum 10. Moreover, ERCP is technically difficult in patients with significant duodenal obstruction. The annular duct can also be detected on MRCP, where it commonly connects with the main pancreatic duct near the major papilla but also may drain into the dorsal duct near the minor papilla or directly drain into the duodenum 31. MRCP, apart from being non-invasive and operator-independent, can also visualize pancreatic parenchyma around the duodenum.
Best practice guidelines for the management of annular pancreas are lacking, and the treatment of annular pancreas is individualized based on presenting symptoms 32. Asymptomatic patients who do not demonstrate signs and symptoms of annular pancreas can be followed up closely without any intervention 33. If annular pancreas causes problems, duodenal bypass procedures to bypass the blocked part of the duodenum such as gastrojejunostomy, duodenoduodenostomy, or duodenojejunostomy in both adults and children is the typical treatment and is superior to local resection of the annular pancreas, which may be complicated with postoperative pancreatitis, pancreatic fistula, or recurrent duodenal stenosis 34, 35. The annular pancreas itself is rarely removed as this would risk injuring the pancreatic tube and causing a leak of fluids within it resulting in postoperative pancreatitis, pancreatic fistula, or recurrent duodenal stenosis 34. But division may be possible in some cases of annular pancreas in the left anterior part without containing a duct 36.
Figure 1. Annular pancreas
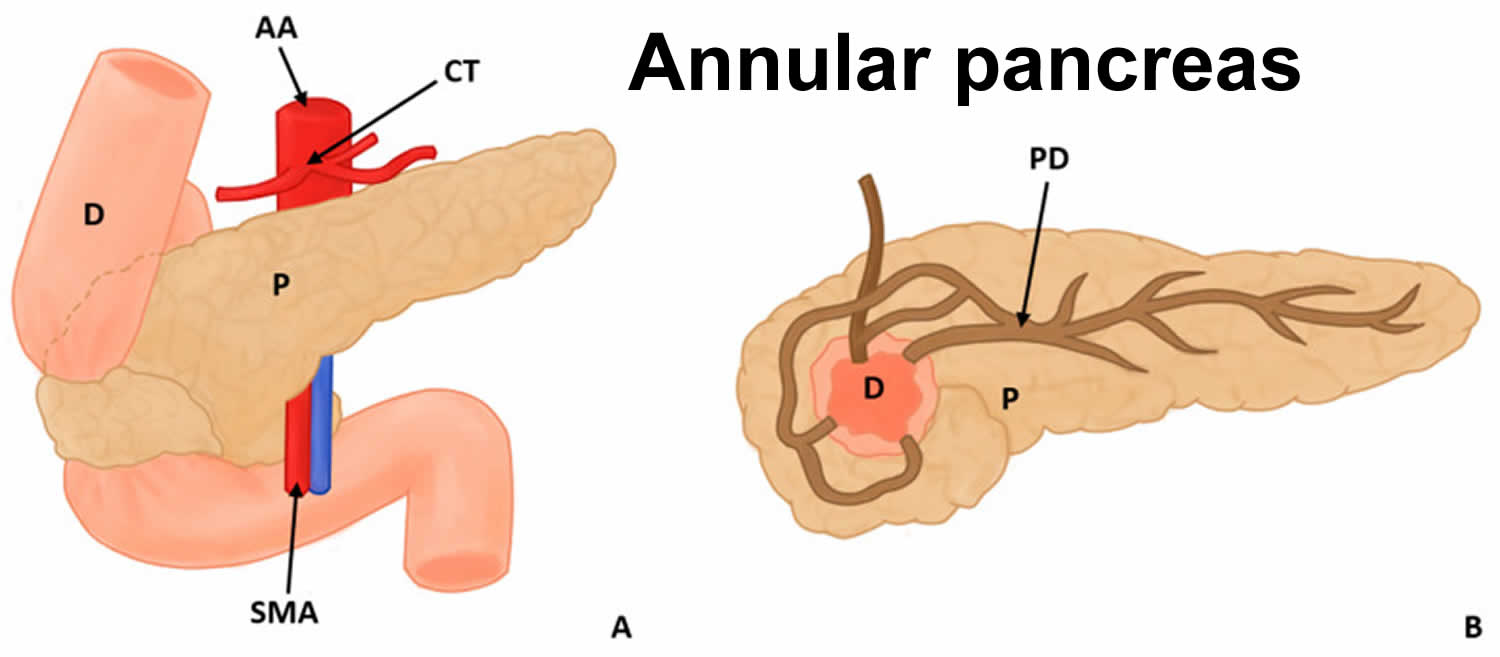
Footnotes: Annular pancreas surrounding the descending portion of the duodenum in 2 views, (A) anterior and (B) posterior
Abbreviations: D = duodenum; P = pancreas; PD = pancreatic duct; AA = abdominal aorta; CT = celiac trunk; SMA = superior mesenteric artery
[Source 37 ]Figure 2. Annular pancreas magnetic resonance cholangiopancreaticography (MRCP)
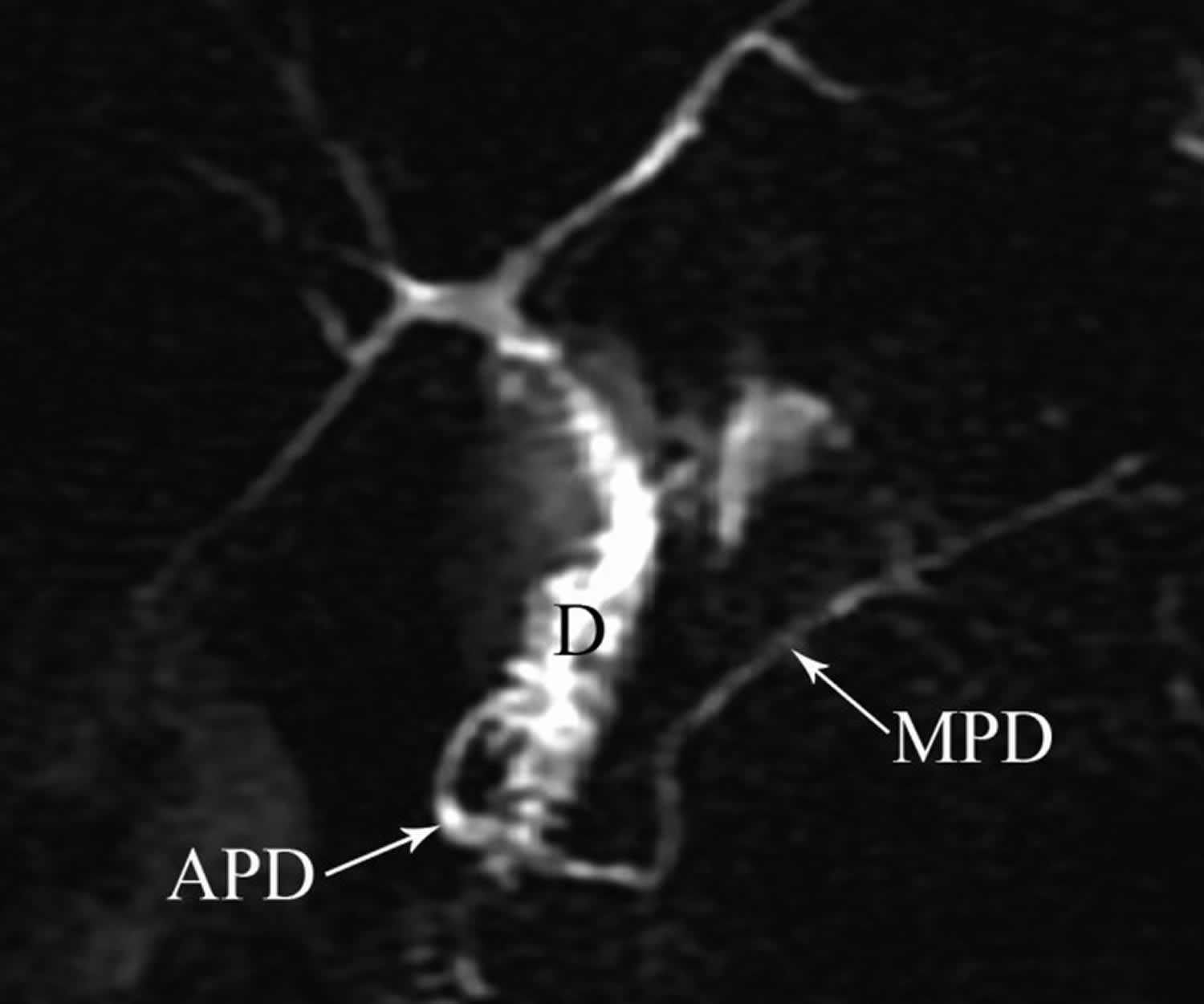
Footnote: Magnetic resonance cholangiopancreaticography (MRCP) image showing annular pancreatic duct (APD) communicating with main pancreatic duct (MPD) and completely encircling duodenum (D) in patient with annular pancreas.
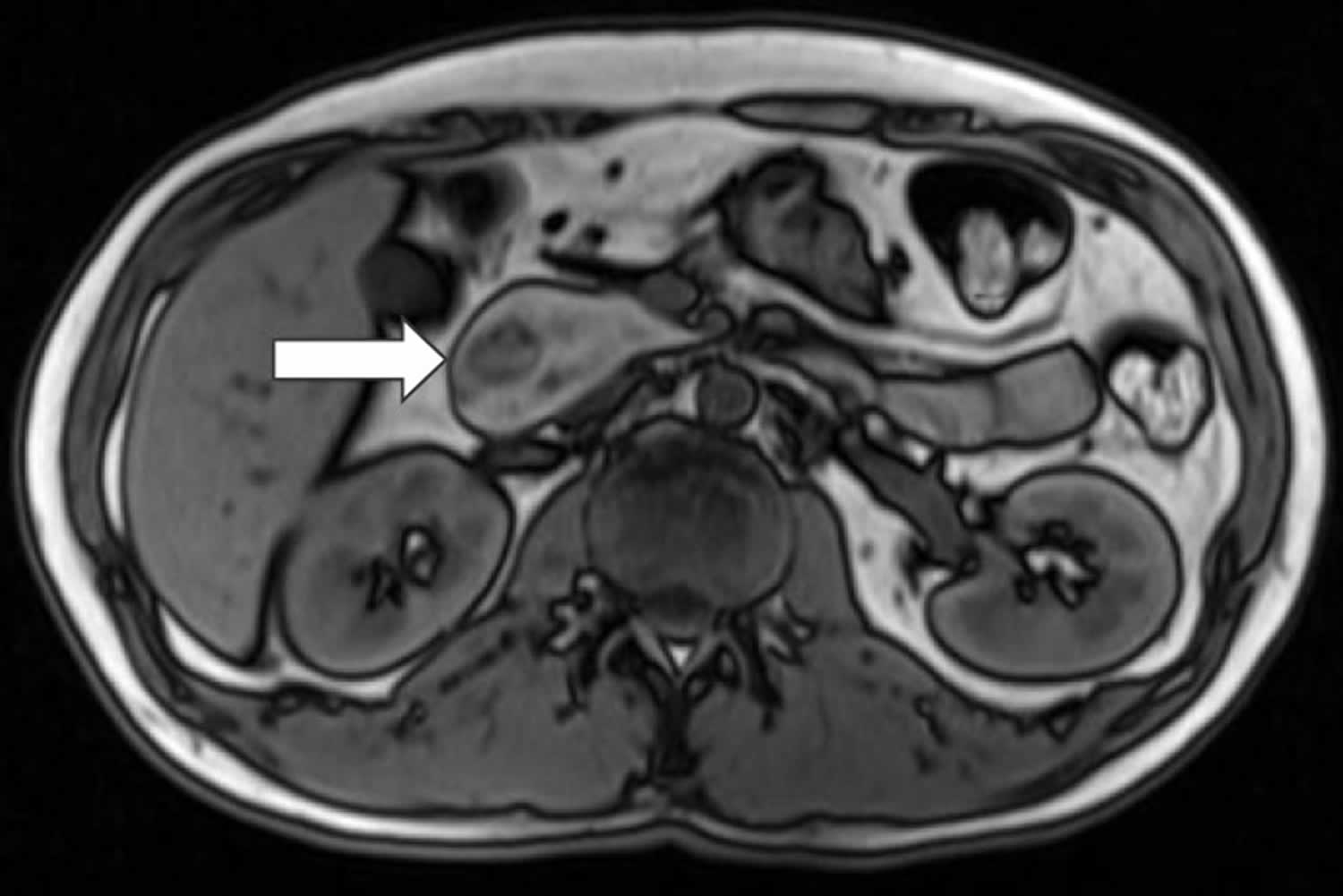
[Source 27 ]Figure 3. Annular pancreas CT
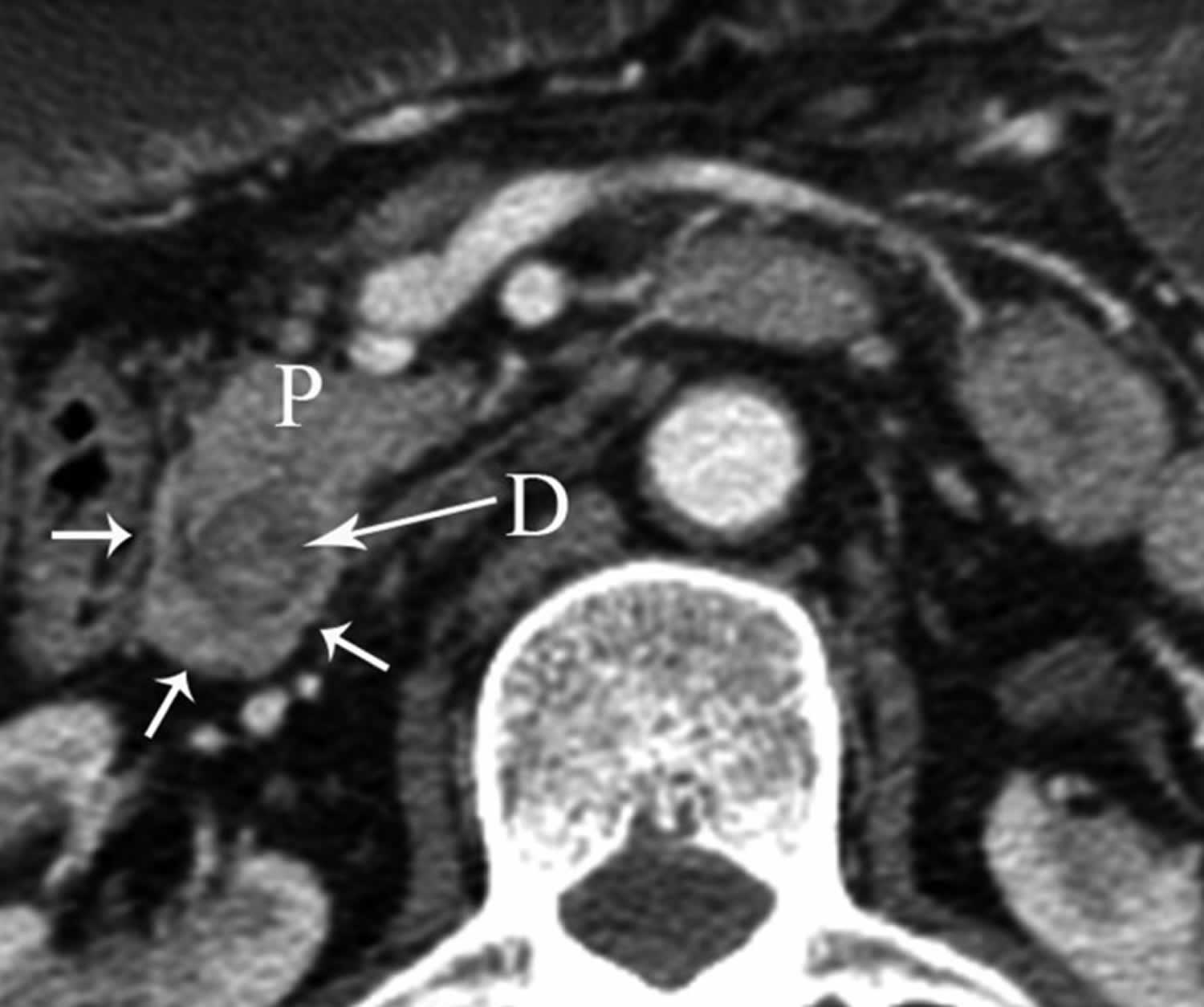
Footnote: Axial multidetector CT (computed tomography) image showing pancreatic tissue (arrows) completely encircling second part of duodenum (D) in patient with annular pancreas (P).
[Source 27 ]Circumportal pancreas
Circumportal pancreas is an annular pancreas variant that occurs when pancreatic tissue envelops the portal vein or its immediate tributaries, the superior mesenteric and splenic veins 38. Circumportal pancreas is believed to arise when the developing uncinate process (of the ventral bud) fuses with pancreatic body tissue (of the dorsal bud), thereby entrapping the portal venous confluence. The annular segment classification is by its relation to the splenic vein—suprasplenic, infrasplenic, or combined subtypes, with a further description describing whether the main pancreatic duct courses: anteportal or retroportal 39, 40, 41.
Circumportal pancreas significantly increases the technical difficulty of pancreatic head resection. Moreover, this anatomic variant is often an intraoperative discovery not revealed by preoperative imaging. Resection of the retroportal annular segment requires intensive dissection and can complicate the creation of a pancreaticojejunal anastomosis. Postoperative pancreatic fistula is common with circumportal pancreas, approaching 70% in some studies, compared to 3 to 45% with the expected anatomy. Peritoneal drain amylase levels can be followed to monitor for fistula. Surgeons writing from Germany in 2017 described six cases of circumportal pancreas encountered intraoperatively. They advocated for wider resection—one-centimeter distally towards the tail—to decrease the incidence of pancreatic fistula 42.
Pancreas anatomy
The pancreas is a large gland that sits behind the greater curvature of the stomach and close to the first part of the small intestine (the duodenum). The pancreas is shaped a bit like a fish with a wide head, a tapering body, and a narrow, pointed tail. In adults it’s about 12–15 cm (5–6 inches) long and 2.5 cm (1 in.) thick but less than 2 inches (5 centimeters) wide. The pancreas is both an endocrine and exocrine gland (see Figures 2 and 3).
The pancreas has 3 parts, the head, body, and tail.
- the wide end is called the head. The head of the pancreas is on the right side of the abdomen (belly), behind where the stomach meets the duodenum (the first part of the small intestine).
- the bit in the middle is called the body. The body of the pancreas is behind the stomach.
- the thin end is called the tail. The tail of the pancreas is on the left side of the abdomen next to the spleen.
About 99% of the pancreas is exocrine tissue made up of small clusters of glandular epithelial cells called acinar cells (acini), which secretes 1,200 to 1,500 mL of pancreatic juice per day – that are released into the small intestines to help you digest foods (especially fats). The digestive enzymes are first released into tiny tubes called central ducts. These merge to form larger ducts, which empty into the pancreatic duct (duct of Wirsung). The pancreatic duct merges with the common bile duct (the duct that carries bile from the liver), and empties into the duodenum (the first part of the small intestine) at the ampulla of Vater (also known as the hepatopancreatic ampulla). The ampulla of Vater (hepatopancreatic ampulla) is where the pancreatic duct and bile duct join together to drain into the duodenum, which is the first part of the small intestine. The passage of pancreatic juice and bile through the hepatopancreatic ampulla (ampulla of Vater) into the duodenum of the small intestine is regulated by a mass of smooth muscle surrounding the ampulla known as the sphincter of the hepatopancreatic ampulla, or sphincter of Oddi. The other major duct of the pancreas, the accessory duct (duct of Santorini), that branches from the main pancreatic duct and opens independently into the duodenum about 2.5 cm (1 in.) superior to the hepatopancreatic ampulla (ampulla of Vater) at the minor duodenal papilla. The accessory duct (duct of Santorini) bypasses the sphincter and allows pancreatic juice to be released into the duodenum even when bile is held back.
The endocrine part of the pancreas consists of groups of cells that are closely associated with blood vessels. These remaining 1% of the cell clusters form “islands” of cells called pancreatic islets (Islets of Langerhans). The Islets of Langerhans cells secrete the hormones glucagon, insulin, somatostatin, and pancreatic polypeptide (PP). Islets of Langerhans main cell types are alpha cells (20%), beta cells (70%), and delta cells (5%). The pancreatic islets alpha cells secrete the hormone glucagon, and beta cells secrete the hormone insulin (Figure 4). Both insulin and glucagon are important hormones which help control blood sugar levels and are released directly into the bloodstream.
The Islets of Langerhans Delta (δ) cells, or D cells, secrete somatostatin (growth hormone–inhibiting hormone) concurrently with the release of insulin by the beta cells. Somatostatin is a peptide hormone that inhibits the secretion of glucagon and insulin by the nearby alpha and beta cells. Somatostatin also work with amylin to limit the secretion of stomach acid.
Other, minor types of pancreatic cells, about 5% of the total, are called pancreatic polypeptide (PP) and G cells. Pancreatic polypeptide (PP) cells secrete pancreatic polypeptide, a hormone that may inhibit the exocrine activity of the pancreas.
Pancreatic islets (Islets of Langerhans) are relatively concentrated in the tail of the pancreas, whereas the head is more exocrine. Over 90% of pancreatic cancers arise from the ducts of the exocrine portion (ductal carcinomas), so cancer is most common in the head of the pancreas.
Figure 4. The pancreas
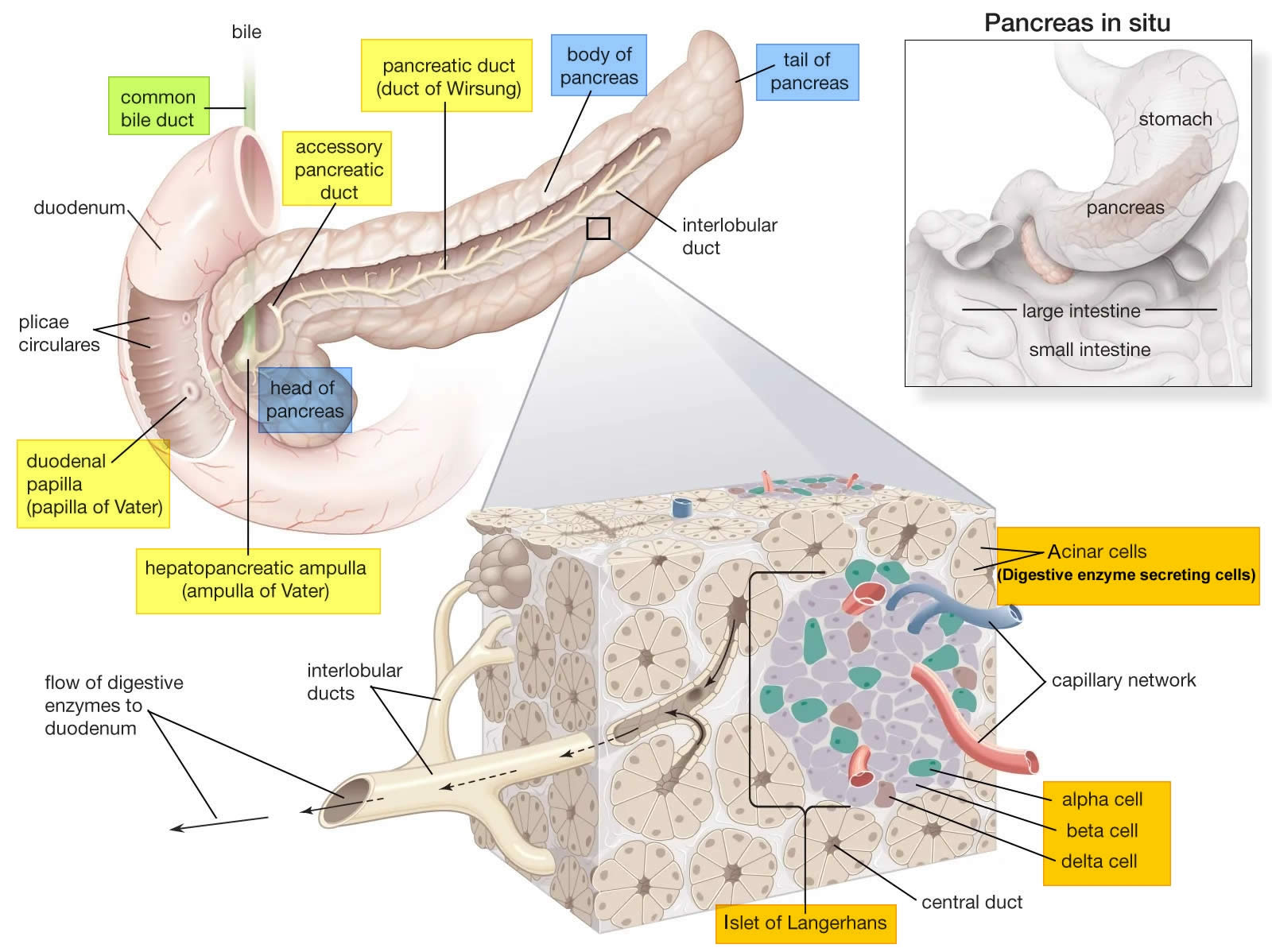
Figure 5. Pancreas cell types
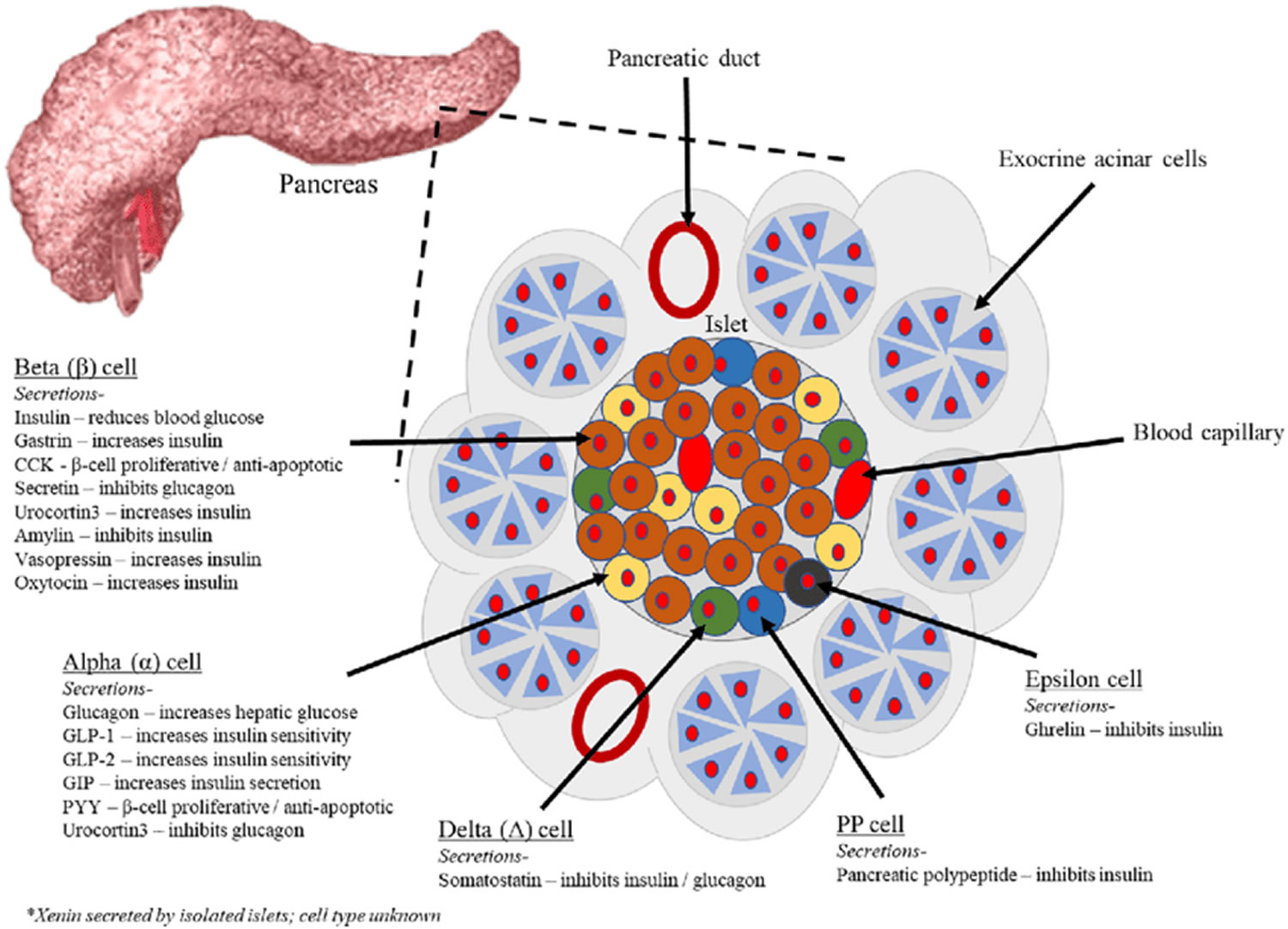
Footnotes: Exocrine pancreatic acinar cells constitute most of the pancreatic tissue, these cells produce digestive enzymes which are transported via the pancreatic ducts. The endocrine pancreas is illustrated with all cell types; alpha, beta, delta, pancreatic polypeptide (PP) and epsilon. The endocrine pancreas cells are arranged in compact Islets of Langerhans and secrete a number of classical and ‘nonclassical’ peptides, as depicted.
Figure 6. Pancreas location
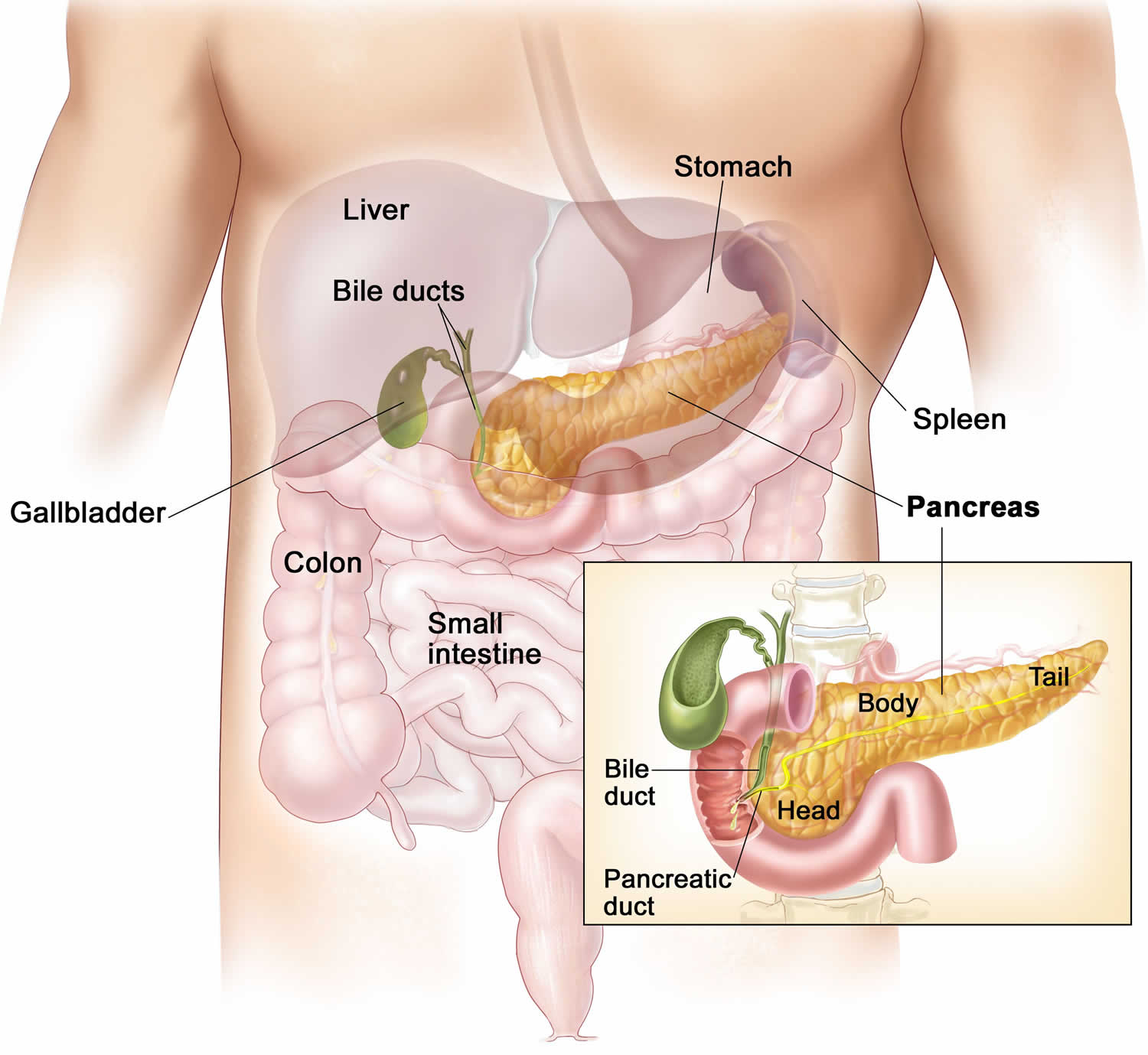
Figure 7. Relationship of the pancreas to the liver, gallbladder, and duodenum

Annular pancreas cause
The pancreas develops from dorsal pancreatic bud (dorsal anlage) and ventral pancreatic bud (ventral anlage) that first appear in the 5th gestational week as outgrowths of the primitive foregut (Figure 8) 27, 43. By the 7th gestational week, expansion of the duodenum causes the ventral pancreatic bud (from which originates the hepatobiliary system) to rotate and pass behind the duodenum from right to left and fuse with the dorsal pancreatic bud in the foregut (Figure 8). The dorsal pancreatic bud forms a majority of the head of the pancreas as well as the uncinate process (<25% of pancreatic tissue), whereas the dorsal pancreatic bud forms the anterior head, all of the body, and tail of the pancreas 2. Following this fusion, the ductal systems anastomose, a complicated process with a wide spectrum of possible outcomes. The portion of the ventral duct between the dorsal-ventral fusion and major papilla is termed the duct of Wirsung. The portion of the dorsal duct upstream to the dorsalventral fusion point is called the main pancreatic duct. The segment of the dorsal duct downstream to the dorsal-ventral fusion point is termed the duct of Santorini, or accessory pancreatic duct, which drains at the papilla minor 2.
Several theories, some dating back to the 1900s, have been proposed to explain the development of the annular pancreas, but none of them have convincingly been able to explain all cases of annular pancreas:
- Lecco’s theory: Adhesion of the right ventral bud to the duodenal wall
- Baldwin’s theory: Persistence of the left ventral bud
- Adherence of a small portion of the left ventral bud to the duodenal wall with concomitant pancreatic tissue enveloping the duodenum during rotation
Among them, Lecco’s and Baldwin’s theory concerning development of the annular pancreas from the ventral pancreatic bud were the most plausible 44. Immunohistochemistry studies have shown the origin of annular pancreas to be of the ventral pancreatic bud 45. Although not well studied, the role of genetic factors has been linked to annular pancreas based on isolated cases reports of familial annular pancreas and overexpression of the ventral-specific gene transmembrane 4 superfamily member 3 (tm4sf3) 21.
Conditions that may be associated with annular pancreas include 18:
- Down syndrome
- Excess amniotic fluid during pregnancy (polyhydramnios)
- Other congenital gastrointestinal problems such as intestinal atresia, pancreatico-biliary malrotation, and pancreas divisum
- Pancreatitis
Figure 8. Pancreas embryologic development
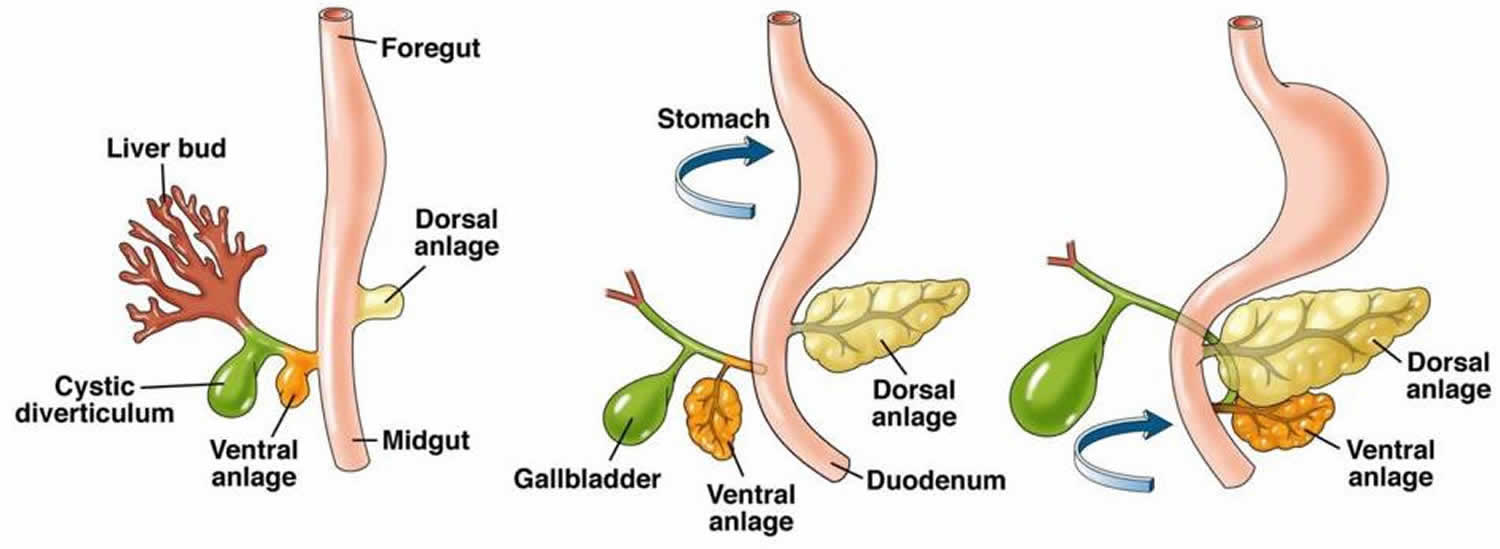
Footnotes: Drawings show normal embryologic development of the pancreas. Ventral pancreatic bud (ventral anlage) arises from hepatic diverticulum (the hepatobiliary system), and dorsal pancreatic bud (dorsal anlage) arises from dorsal mesogastrium. During 7th gestational week, expansion of duodenum causes ventral pancreatic bud to rotate and pass behind duodenum from right to left and fuse with dorsal pancreatic bud. Ventral bud (ventral anlage) forms posterior head and uncinate process, whereas dorsal bud (dorsal anlage) forms anterior head, body, and tail. Finally, ventral and dorsal pancreatic ducts fuse, and pancreas predominantly is drained through ventral duct, which joins common bile duct at level of major papilla and dorsal duct drains at level of minor papilla.
[Source 43 ]Figure 9. Annular pancreas embryologic development

Annular pancreas pathophysiology
The pathophysiology of annular pancreas is explained by the direct impact of the migratory defect during embryogenesis. Duodenal obstruction is secondary to a mechanical defect, which can be extrinsic from the encasement of the duodenum or intrinsic from scarring, stenosis, or the presence of duodenal webs. The pathogenesis of pancreatitis in annular pancreas is unclear. Pancreatitis, when it occurs, is usually confined to the annulus and the adjoining pancreatic head sparing the body and tail of the gland which is likely secondary to fibrosis resulting in the inability of the pancreatic secretions to pass through the annular duct and increased intrinsic susceptibility of the annular pancreatic tissue to damage 47, 48, 49. Peptic ulcer disease may be related to gastric stasis and antral overdistension with resulting hypergastrinemia 45, 23. Biliary ductal dilation is attributed likely due to the progression of chronic pancreatitis resulting in fibrosis or ductal compression by the annular gland 16.
Annular pancreas symptoms
Babies with annular pancreas may have symptoms of complete blockage of the intestine. However, up to one half of people with annular pancreas do not have symptoms until adulthood. There are also cases that are not detected because the symptoms are mild. Annular pancreas usually presents in newborn infants less than four weeks old with vomiting due to severe duodenal obstruction. Babies may not feed well. They may spit up more than normal, not drink enough breast milk or formula, and cry.
In adults, approximately 50% of the patients may be asymptomatic for life, with the anomaly discovered incidentally 27. When symptomatic, the presentation is usually in the 20 to 60 years of age with abdominal pain, fullness after eating and vomiting resulting from gastric outlet obstruction, upper gastrointestinal bleeding from peptic ulceration, acute or chronic pancreatitis, or in rare instances, jaundice resulting from biliary obstruction 50, 51, 33, 52, 45, 36, 16, 53.
Adult symptoms may include:
- Fullness after eating
- Nausea or vomiting.
Annular pancreas complications
Annular pancreas complications may include obstruction of the duodenum and poor liver function. Annular pancreas can result in pancreatitis, small intestine ulcers, intestinal blockage, and jaundice. In some cases, an abnormal connection between the windpipe and the esophagus can also be associated with an annular pancreas. In rare instances, pancreatic cancer is a complication related to annular pancreas.
Annular pancreas complications may include 54, 55:
- Obstructive jaundice
- Pancreatic cancer 56
- Pancreatitis (inflammation of the pancreas) due to either the difficulty in the release of the exocrine pancreatic secretion, linked to the anomaly of the excretory tract, or a possible increase in annular pancreas individual susceptibility to this condition
- Peptic ulcer especially duodenal ulcers (29–48% of cases), probably related to stasis of the chyme (semi-fluid mass of partly digested food) and gastric expansion of the segment upstream of the obstruction, condition which may favor the occurrence of hypergastrinemia.
- Perforation (tearing a hole) of the intestine due to obstruction
- Peritonitis
Annular pancreas diagnosis
Annular pancreas usually is a coincidental finding, and most adults with annular pancreas are asymptomatic. Your healthcare provider will perform an exam and get your medical history. The findings from an abdominal examination usually are normal.
Magnetic resonance cholangiopancreatography (MRCP) and endoscopic retrograde cholangiopancreatography (ERCP) are the most prevalent method of diagnosing annular pancreas by the gastroenterologist 57, 58. However, only through laparoscopy or laparotomy can your doctor confirm the diagnosis of annular pancreas 59, 60, 61, 62, 63, 64, 65, 66. Furthermore, laparoscopic surgery is a good choice for adult patients with annular pancreas both in diagnose and treatment with less postoperative complications and a short recovery time 67.
Endoscopic retrograde cholangiopancreatography (ERCP) is considered as the gold standard for diagnosing annular pancreas as it provides visualization of the descending duodenum and the pancreatic ductal system along with the major and minor papilla 29, 30. Duodenal narrowing is usually located just proximal to the major papilla, and the minor papilla is usually situated at the proximal rim of the annular ring. In the majority of patients, the duct of the annular pancreas communicates with the main pancreatic duct arising from the major papilla.
Endoscopic Retrograde Cholangiopancreatography (ERCP) is a non-invasive procedure where a flexible tube containing a tiny camera will be inserted into your mouth through the stomach and small intestine (duodenum). The gastroenterologist will inject a radiopaque dye and takes X-ray images of the pancreas. Upon endoscopic retrograde cholangiopancreatography (ERCP), the major papilla is often difficult to cannulate, and the duct of Wirsung (ventral duct) appears shortened and of small diameter (like a cutoff of the duct) with rapid filling of small accessory ducts. At this point, the accessory papilla should be cannulated. A variety of maneuvers have been used to facilitate cannulation. These include simple maneuvers, such as using the long scope position and accessories to include a taper cannula, slick wires, secretagogues, such as sincalide or secretin, and the application of vital dyes. This should reveal the duct of Santorini (dorsal duct) running the entire length of the pancreas.
However, endoscopic retrograde cholangiopancreatography (ERCP) via the major papilla will not be able to diagnose annular pancreas in patients where the annular duct opens into the minor papilla or directly into the duodenum 10. Moreover, ERCP is technically difficult in patients with significant duodenal obstruction. The annular duct can also be detected on magnetic resonance cholangiopancreatography (MRCP), where it commonly connects with the main pancreatic duct near the major papilla but also may drain into the dorsal duct near the minor papilla or directly drain into the duodenum 31. Magnetic resonance cholangiopancreatography (MRCP), apart from being non-invasive and operator-independent, can also visualize pancreatic parenchyma around the duodenum.
Magnetic resonance cholangiopancreatography (MRCP) produces comprehensive pictures of the pancreas and pancreatic ducts using a strong magnetic field and radio waves. The patient will be administered with a contrast material intravenously. The patient needs to be in supine position in the magnetic resonance imaging (MRI) scanner while the pancreas is scanned. Magnetic resonance cholangiopancreatography (MRCP) is a very accurate, noninvasive technique for visualizing the pancreatic and biliary duct system without the side effects of a contrast agent and without the risk of causing acute pancreatitis 68, 69, 70, 71. Maximum-intensity projection images from MRCP appear to best illustrate the “crossing duct” sign, in which the dominant dorsal duct crosses the intrapancreatic common bile duct to empty into the minor papilla 72.
When the annular pancreatic duct encircling and extending to the right side of the duodenum is identified by MRCP or ERCP, the diagnosis of annular pancreas is established 27. But sometimes the pancreatic duct without dilatation is invisible on MRCP. Secretin-enhanced MRCP (S-MRCP) may be the best non-invasive imaging modality for evaluating ductal anatomy. The annular pancreatic duct usually communicates with the main pancreatic duct (Figure 2) but may drain into the intrapancreatic common bile duct, the duct of Wirsung, or the duct of Santorini. At CT and magnetic resonance imaging (MRI), a ring of pancreatic tissue surrounds the descending duodenum, in continuity with the pancreatic head (Figure 3) 73, 74. However, a visualization of a complete ring of pancreatic tissue around the duodenum is not required for a diagnosis of annular pancreas 16. Pancreatic tissue extending in a posterolateral or anterolateral direction to the second part of the duodenum or pancreatic tissue anterior and posterior to the duodenum (‘crocodile jaw’ configuration), in the presence of a gastric outlet obstruction should raise the suspicion of annular pancreas (Figure 10) 16. It is most likely that these patients have a thin band of pancreatic tissue, not seen at CT and MRI, incorporated in the duodenal wall.
Other tests include:
- Abdominal ultrasound
- Abdominal x-ray
- Computed tomography (CT) scan. Computed tomography (CT) scan is a test that uses a combination of X-rays and computers to produce images of the pancreas. CT of the abdomen is very useful in finding and imaging pathologies of the pancreas, such as acute or chronic pancreatitis and pancreatic tumors.
- Esophagogastroduodenoscopy (EGD)
- Upper GI and small bowel series
- Blood tests. Blood tests can give clues about how the immune system, pancreas and related organs are working.
- Stool tests. Stool tests can measure levels of fat that could suggest your digestive system isn’t absorbing nutrients as it should.
Abdominal ultrasound or plain abdominal X-ray usually show the classic “double bubble” sign when a duodenal obstruction is present 75. However, this has limited diagnostic value, because it is neither specific nor sensitive without the ability of differentiate carcinoma involving the head of the pancreas and chronic pancreatitis 17. There are some findings that are typical, including annular defect on the second portion of the duodenum, dilatation of the proximal lumen, and retrograde intestinal movement from the proximal part to obstruction 18.
Sandrasegaran et al 16 showed that complete encasement of the duodenum with pancreatic tissue is not essential for the diagnosis of annular pancreas. Newer imaging techniques with positron emission tomography (PET)/CT incorporating radiotracers C-11 choline and F-18 fluciclovine have demonstrated the diagnosis of annular pancreas 76. Despite many advances in diagnostic techniques, the gold standard test for diagnosing annular pancreas remains to be laparotomy with a thorough gross examination of the duodenum and the head of the pancreas 77.
Esophagogastroduodenoscopy (EGD) could also find gastric obstruction, peptic ulceration, and duodenal extrinsic compression.
Endoscopic ultrasonography (EUS) is not a primary imaging modality for the diagnosis of annular pancreas but is a useful investigational modality for finding the cause of extrinsic compression of the duodenum 78, 79, 80. Like MRCP, endoscopic ultrasonography (EUS) can delineate both the pancreatic parenchyma and the pancreatic duct around the duodenum and thus help with the accurate diagnosis of annular pancreas 78. Even in patients with duodenal obstruction, EUS can help with the diagnosis of annular pancreas by scanning from the duodenal bulb 10. An added advantage of EUS is that it can help with the diagnosis of co-existent pancreatic pathologies like chronic pancreatitis and ductal calculi 81. Papachristou et al. 82 studied 5 patients with an annular pancreas with radial EUS and reported that CT could detect the annular pancreas in only 1 of 5 patients, whereas EUS could detect annular pancreas in all 5 patients. EUS detected an encircling band of pancreatic tissue by approximately 360° in 3, 270° in 1, and 180° in 1 patient, respectively. Additionally, within this band of encircling tissue, the pancreatic duct was identified in 4 of 5 patients. The authors suggested following technical maneuvers during radial EUS to facilitate the identification of encircling pancreatic tissue 78, 82:
- (a) use of glucagon to inhibit gut motility;
- (b) minimal balloon inflation to help avoid rapid uncontrolled scope withdrawal;
- (c) gentle scope deflection;
- (d) gentle forward pressure with an overinflated balloon into the narrowed region of the duodenum.
Figure 10. Annular pancreas diagnosis
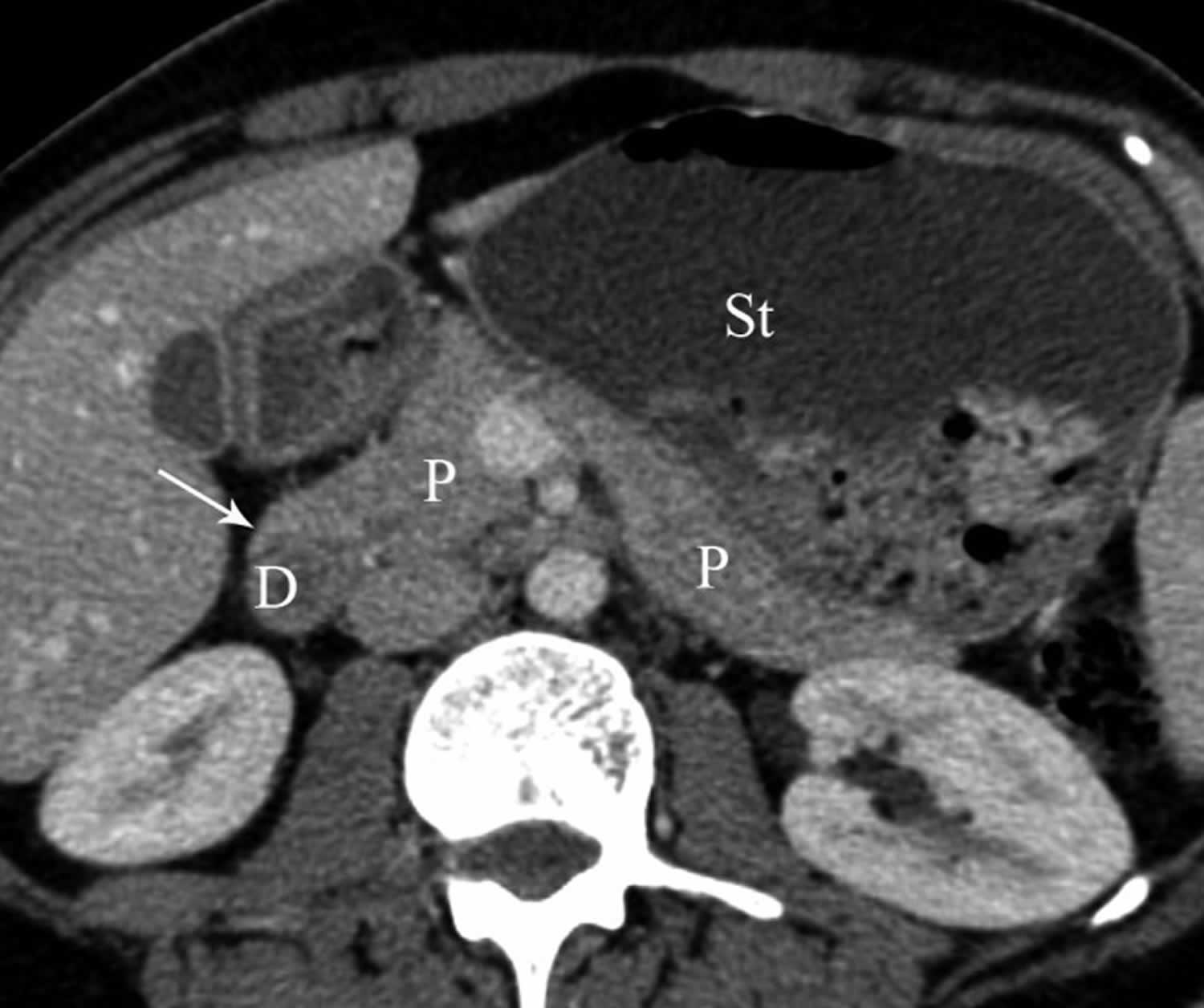
Footnote: Axial multidetector CT (computed tomography) image showing pancreatic tissue (arrow) extending in anterolateral direction to second part of duodenum (D) and dilatation of stomach (St) in patient with incomplete annular pancreas (P).
[Source 27 ]Figure 11. Annular pancreas MRI
Footnote: Magnetic resonance image (MRI) showing circumferential pancreas around the second portion of the duodenum with luminal narrowing.
[Source 83 ]Annular pancreas differential diagnosis
As the clinical manifestations of annular pancreas exhibit a bimodal age distribution presenting either early during infancy or adulthood, the differential diagnosis of this anomaly is also based on the age of presentation.
Infants commonly present with duodenal obstruction with the classic “double bubble sign” on imaging, and the differential diagnosis can be classified into either intrinsic or extrinsic causes 84. Duodenal atresia, duodenal stenosis, paraduodenal hernias, Meckel diverticulum, and duodenal webs are some important intrinsic causes that need to be considered 75.
Besides annular pancreas, the other extrinsic causes that need to be considered are malrotation of the gut or midgut volvulus. Peptic ulcer disease, pancreatic divisum, primary duodenal and pancreatic malignancies should be considered in the differential diagnosis of an adult patient suspected to have annular pancreas 85. Gastroduodenal tuberculosis should be considered in patients from geographical areas endemic for tuberculosis 20.
Annular pancreas treatment
Best practice guidelines for the management of annular pancreas are lacking, and the treatment of annular pancreas is individualized based on presenting symptoms 32. Asymptomatic patients who do not demonstrate signs and symptoms of annular pancreas can be followed up closely without any intervention 33. If annular pancreas causes problems, duodenal bypass procedures to bypass the blocked part of the duodenum such as gastrojejunostomy, duodenoduodenostomy, or duodenojejunostomy in both adults and children is the typical treatment and is superior to local resection of the annular pancreas, which may be complicated with postoperative pancreatitis, pancreatic fistula, or recurrent duodenal stenosis 34, 35. The annular pancreas itself is rarely removed as this would risk injuring the pancreatic tube and causing a leak of fluids within it resulting in postoperative pancreatitis, pancreatic fistula, or recurrent duodenal stenosis 34. But division may be possible in some cases of annular pancreas in the left anterior part without containing a duct 36.
Annular pancreas surgery
Since Vidal first reported successful gastrojejunostomy in a 3-year-old patient with annular pancreas in 1905, Zyromski et al 77 reported that duodenoduodenostomy or duodenojejunostomy caused less anastomotic site ulcers than gastrojejunostomy. Although duodenoduodenostomy or duodenojejunostomy is a routine procedure in neonates and children, duodenojejunostomy or gastrojejunostomy is recommended in adult patients due to less mobility of the duodenum, but choice should be tailored to the patient at hand 86, 60, 58.
In case of grossly scarred duodenal C-loop, gastrojejunostomy may be better choice but require an additional vagotomy as it caused more anastomotic site ulcers than duodenoduodenostomy or duodenojejunostomy 18. Laparotomy was the most widely used methods in the most published cases and less by laparoscope. Although there are no studies in which compared the two methods, some surgeons believe that laparoscopy can be safely and effectively conducted in the treatment of annular pancreas, with the benefit of minimally invasive surgery which means less trauma and fast recovery time, as were seen in cases described literature.
Laparoscopic gastrojejunostomy has been widely performed in patients with obesity or gastrointestinal cancers. This suggests that laparoscopic gastrojejunostomy is a useful treatment modality of the annular pancreas. It has been reported that laparoscopic duodenoduodenostomy and laparoscopic gastrojejunostomy are successfully performed in children and in adult patients, respectively 77, 18.
Annular pancreas prognosis
Annular pancreas prognosis (outlook) is most often good with surgery. The prognosis of annular pancreas in children is excellent with increased overall survival rates, despite the presence of associated congenital malformations and chromosomal anomalies 87. This has been attributed to improved neonatal care, nutritional management, early detection, and management of associated anomalies 88.
Adults with an annular pancreas are at increased risk for pancreatic or biliary tract cancer. The prognosis of annular pancreas in adults is favorable if it is not complicated by underlying cancer.
- Papachristou G.I., Topazian M.D., Gleeson F.C., Levy M.J. EUS features of annular pancreas (with video) Gastrointest. Endosc. 2007;65:340–344. doi: 10.1016/j.gie.2006.10.010[↩]
- Schulte SJ. Embryology, normal variation, and congenital anomalies of the pancreas. In: Stevenson GW, Freeny PC, Margulis AR, Burhenne HJ, editors. Margulis’ and Burhenne’s alimentary tract radiology. 5th ed. St. Louis: Mosby; 1994. pp. 1039–1051.[↩][↩][↩]
- Annular pancreas. https://radiopaedia.org/articles/annular-pancreas?lang=us[↩]
- Aleem A, Shah H. Annular Pancreas. [Updated 2023 May 29]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK559236[↩][↩]
- Alexander LF. Congenital pancreatic anomalies, variants, and conditions. Radiol Clin North Am. 2012 May;50(3):487-98. doi: 10.1016/j.rcl.2012.03.006[↩]
- Türkvatan A., Erden A., Türkoğlu M.A., Yener Ö. Congenital variants and anomalies of the pancreas and pancreatic duct: Imaging by magnetic resonance cholangiopancreaticography and multidetector computed tomography. Korean J. Radiol. 2013;14:905–913. doi: 10.3348/kjr.2013.14.6.905[↩]
- Nagpal SJS, Peeraphatdit T, Sannapaneni SK, Sharma A, Takahashi N, Kendrick ML, Majumder S, Vege SS. Clinical spectrum of adult patients with annular pancreas: Findings from a large single institution cohort. Pancreatology. 2019 Mar;19(2):290-295. doi: 10.1016/j.pan.2018.12.009[↩]
- RAVITCH MM, WOODS AC Jr. Annular pancreas. Ann Surg. 1950 Dec;132(6):1116-27. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1616673/pdf/annsurg01399-0112.pdf[↩][↩]
- Benassai G, Perrotta S, Furino E, De Werra C, Aloia S, Del Giudice R, Amato B, Vigliotti G, Limite G, Quarto G. “Ductal adenocarcinoma in anular pancreas”. Int J Surg. 2015 Sep;21 Suppl 1:S95-7. https://doi.org/10.1016/j.ijsu.2015.04.086[↩][↩]
- Kandpal H, Bhatia V, Garg P, Sharma R. Annular pancreas in an adult patient: diagnosis with endoscopic ultrasonography and magnetic resonance cholangiopancreatography. Singapore Med J. 2009 Jan;50(1):e29-31. http://smj.sma.org.sg/5001/5001cr8.pdf[↩][↩][↩][↩]
- Christodoulidis G, Zacharoulis D, Barbanis S, Katsogridakis E, Hatzitheofilou K. Heterotopic pancreas in the stomach: a case report and literature review. World J Gastroenterol. 2007 Dec 7;13(45):6098-100. doi: 10.3748/wjg.v13.45.6098[↩]
- Sakorafas GH, Sarr MG. Ectopic gastric submucosal pancreatic tissue. JOP. 2003 Nov;4(6):214-5.[↩]
- Ormarsson OT, Gudmundsdottir I, Mårvik R. Diagnosis and treatment of gastric heterotopic pancreas. World J Surg. 2006 Sep;30(9):1682-9. doi: 10.1007/s00268-005-0669-6[↩]
- Zhang L, Sanderson SO, Lloyd RV, Smyrk TC. Pancreatic intraepithelial neoplasia in heterotopic pancreas: evidence for the progression model of pancreatic ductal adenocarcinoma. Am J Surg Pathol. 2007 Aug;31(8):1191-5. doi: 10.1097/PAS.0b013e31806841e1[↩]
- Foo FJ, Gill U, Verbeke CS, Guthrie JA, Menon KV. Ampullary carcinoma associated with an annular pancreas. JOP. 2007 Jan 9;8(1):50-4.[↩]
- Sandrasegaran K, Patel A, Fogel EL, Zyromski NJ, Pitt HA. Annular pancreas in adults. AJR Am J Roentgenol. 2009 Aug;193(2):455-60. doi: 10.2214/AJR.08.1596[↩][↩][↩][↩][↩][↩][↩]
- Fu PF, Yu JR, Liu XS, Shen QY, Zheng SS. Symptomatic adult annular pancreas: report of two cases and a review of the literature. Hepatobiliary Pancreat Dis Int. 2005 Aug;4(3):468-71.[↩][↩]
- De Ugarte DA, Dutson EP, Hiyama DT. Annular pancreas in the adult: management with laparoscopic gastrojejunostomy. Am Surg. 2006 Jan;72(1):71-3.[↩][↩][↩][↩][↩]
- THEODORIDES T. PANCR’EAS ANNULAIRE [ANNULAR PANCREAS]. J Chir (Paris). 1964 Apr;87:445-62. French.[↩]
- Wani AA, Maqsood S, Lala P, Wani S. Annular pancreas in adults: a report of two cases and review of literature. JOP. 2013 May 10;14(3):277-9. doi: 10.6092/1590-8577/1454[↩][↩]
- Etienne D, John A, Menias CO, Ward R, Tubbs RS, Loukas M. Annular pancreas: a review of its molecular embryology, genetic basis and clinical considerations. Ann Anat. 2012 Sep;194(5):422-8. doi: 10.1016/j.aanat.2012.04.006[↩][↩]
- Choi JY, Kim MJ, Kim JH, Lim JS, Oh YT, Chung JJ, Song SY, Chung JB, Yoo HS, Lee JT, Kim KW. Annular pancreas: emphasis on magnetic resonance cholangiopancreatography findings. J Comput Assist Tomogr. 2004 Jul-Aug;28(4):528-32. doi: 10.1097/00004728-200407000-00015[↩]
- Johnston DW. Annular pancreas: a new classification and clinical observations. Can J Surg. 1978 May;21(3):241-4.[↩][↩]
- Zheng HM, Cai XJ, Shen LG, Finley R. Surgical treatment of annular pancreas in adults: a report. Chin Med J (Engl). 2007 Apr 20;120(8):724-5.[↩]
- De Rai P, Zerbi A, Castoldi L, Bassi C, Frulloni L, Uomo G, Gabbrielli A, Pezzilli R, Cavallini G, Di Carlo V; ProInf-AISP (Progetto Informatizzato Pancreatite Acuta, Associazione Italiana per lo Studio del Pancreas [Computerized Project on Acute Pancreatitis, Italian Association for the Study of the Pancreas]) Study Group. Surgical management of acute pancreatitis in Italy: lessons from a prospective multicentre study. HPB (Oxford). 2010 Nov;12(9):597-604. doi: 10.1111/j.1477-2574.2010.00201.x[↩]
- Yogi Y, Shibue T, Hashimoto S. Annular pancreas detected in adults, diagnosed by endoscopic retrograde cholangiopancreatography: report of four cases. Gastroenterol Jpn. 1987 Feb;22(1):92-9. doi: 10.1007/BF02806340[↩]
- Türkvatan A, Erden A, Türkoğlu MA, Yener Ö. Congenital variants and anomalies of the pancreas and pancreatic duct: imaging by magnetic resonance cholangiopancreaticography and multidetector computed tomography. Korean J Radiol. 2013 Nov-Dec;14(6):905-13. doi: 10.3348/kjr.2013.14.6.905[↩][↩][↩][↩][↩][↩][↩][↩]
- Gromski MA, Lehman GA, Zyromski NJ, Watkins JL, El Hajj II, Tan D, McHenry L, Easler JJ, Tirkes T, Sherman S, Fogel EL. Annular pancreas: endoscopic and pancreatographic findings from a tertiary referral ERCP center. Gastrointest Endosc. 2019 Feb;89(2):322-328. doi: 10.1016/j.gie.2018.09.008[↩][↩][↩][↩]
- Dharmsathaphorn K., Burrell M., Dobbins J. Diagnosis of annular pancreas with endoscopic retrograde cholangiopancreatography. Gastroenterology. 1979;77:1109–1114. doi: 10.1016/S0016-5085(79)80087-6[↩][↩]
- Gromski M.A., Lehman G.A., Zyromski N.J., Watkins J.L., El Hajj I.I., Tan D., McHenry L., Easler J.J., Tirkes T., Sherman S., et al. Annular pancreas: Endoscopic and pancreatographic findings from a tertiary referral ERCP center. Gastrointest. Endosc. 2019;89:322–328. doi: 10.1016/j.gie.2018.09.008[↩][↩]
- Choi J.Y., Kim M.J., Kim J.H., Lim J.S., Oh Y.T., Chung J.J., Song S.Y., Chung J.B., Yoo H.S., Lee J.T., et al. Annular pancreas: Emphasis on magnetic resonance cholangiopancreatography findings. J. Comput. Assist. Tomogr. 2004;28:528–532. doi: 10.1097/00004728-200407000-00015[↩][↩]
- Rondelli F, Bugiantella W, Stella P, Boni M, Mariani E, Crusco F, Sanguinetti A, Polistena A, Avenia N. Symptomatic annular pancreas in adult: Report of two different presentations and treatments and review of the literature. Int J Surg Case Rep. 2016;20S(Suppl):21-4. doi: 10.1016/j.ijscr.2016.02.001[↩][↩]
- Nobukawa B, Otaka M, Suda K, Fujii H, Matsumoto Y, Miyano T. An annular pancreas derived from paired ventral pancreata, supporting Baldwin’s hypothesis. Pancreas. 2000 May;20(4):408-10. doi: 10.1097/00006676-200005000-00012[↩][↩][↩]
- Moodley S, Hegarty M, Thomson SR. Annular pancreas. S Afr Med J. 2004 Jan;94(1):28-30.[↩][↩][↩][↩]
- Huddleston VS, Lippuner V, Dyer AW. Annular Pancreas in an Adult Presenting with Acute Pancreatitis. J Radiol Case Rep. 2018 Oct 31;12(10):11-16. doi: 10.3941/jrcr.v12i10.3461[↩][↩]
- Kiernan PD, ReMine SG, Kiernan PC, et al. Annular pancreas: May Clinic experience from 1957 to 1976 with review of the literature. Arch Surg 1980;115:46-50. 10.1001/archsurg.1980.01380010038007[↩][↩][↩]
- Orellana-Donoso M, Milos-Brandenberg D, Benavente-Urtubia A, Guerra-Loyola J, Bruna-Mejias A, Nova-Baeza P, Becerra-Farfán Á, Sepulveda-Loyola W, Luque-Bernal RM, Valenzuela-Fuenzalida JJ. Incidence and Clinical Implications of Anatomical Variations in the Pancreas and Its Ductal System: A Systematic Review and Meta-Analysis. Life (Basel). 2023 Aug 9;13(8):1710. doi: 10.3390/life13081710[↩]
- Ehrhardt JD, Gomez F. Embryology, Pancreas. [Updated 2023 Aug 14]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK545243[↩]
- Kiuchi R, Mizuno T, Okamura Y, Sugiura T, Kanemoto H, Uesaka K. Circumportal pancreas – a hazardous anomaly in pancreatic surgery. HPB (Oxford). 2018 May;20(5):385-391. doi: 10.1016/j.hpb.2017.10.009[↩]
- Ohtsuka T, Mori Y, Ishigami K, Fujimoto T, Miyasaka Y, Nakata K, Ohuchida K, Nagai E, Oda Y, Shimizu S, Nakamura M. Clinical significance of circumportal pancreas, a rare congenital anomaly, in pancreatectomy. Am J Surg. 2017 Aug;214(2):267-272. doi: 10.1016/j.amjsurg.2016.11.018[↩]
- Connelly TM, Sakala M, Tappouni R. Circumportal pancreas: a review of the literature and image findings. Surg Radiol Anat. 2015 Jul;37(5):431-7. doi: 10.1007/s00276-015-1436-5[↩]
- Luu AM, Braumann C, Herzog T, Janot M, Uhl W, Chromik AM. Circumportal Pancreas-a Must Know Pancreatic Anomaly for the Pancreatic Surgeon. J Gastrointest Surg. 2017 Feb;21(2):344-351. doi: 10.1007/s11605-016-3315-8[↩]
- Gutta A, Fogel E, Sherman S. Identification and management of pancreas divisum. Expert Rev Gastroenterol Hepatol. 2019 Nov;13(11):1089-1105. doi: 10.1080/17474124.2019.1685871[↩][↩]
- Etienne D, John A, Menias CO, et al. Annular pancreas: a review of its molecular embryology, genetic basis and clinical considerations. Ann Anat 2012;194:422-8. 10.1016/j.aanat.2012.04.006[↩]
- Dowsett JF, Rode J, Russell RC. Annular pancreas: a clinical, endoscopic, and immunohistochemical study. Gut. 1989 Jan;30(1):130-5. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1378243/pdf/gut00607-0142.pdf[↩][↩][↩]
- AN UNUSUAL CASE OF ANNULAR PANCREAS PRESENTING IN AN ADULT FEMALE AS ACUTE PANCREATITIS. https://medical.dpu.edu.in/document/monthly-clinical-meeting/2022/Mar/ANNULAR-PANCREAS.pdf[↩]
- Itoh Y, Hada T, Terano A, Itai Y, Harada T. Pancreatitis in the annulus of annular pancreas demonstrated by the combined use of computed tomography and endoscopic retrograde cholangiopancreatography. Am J Gastroenterol. 1989 Aug;84(8):961-4.[↩]
- DREY NW. Symptomatic annular pancreas in the adult. Ann Intern Med. 1957 Apr;46(4):750-72. doi: 10.7326/0003-4819-46-4-750[↩]
- Jarry J, Wagner T, Rault A, Sa Cunha A, Collet D. Annular pancreas: a rare cause of acute pancreatitis. JOP. 2011 Mar 9;12(2):155-7. http://www.serena.unina.it/index.php/jop/article/view/3345/3592[↩]
- Rondelli F, Bugiantella W, Stella P, et al. Symptomatic annular pancreas in adult: Report of two different presentations and treatments and review of the literature. Int J Surg Case Rep 2016;20S:21-4. 10.1016/j.ijscr.2016.02.001[↩]
- Chen YC, Yeh CN, Tseng JH. Symptomatic adult annular pancreas. J Clin Gastroenterol 2003;36:446-50. 10.1097/00004836-200305000-00019[↩]
- Cai H, Wang X, Cai YQ, Li YB, Meng LW, Peng B. Laparoscopic Roux-en-Y duodenojejunostomy for annular pancreas in adults: case report and literature review. Ann Transl Med. 2018 Jun;6(11):211. doi: 10.21037/atm.2018.05.13[↩]
- Payne RL., Jr Annular pancreas. Ann Surg 1951;133:754-63. 10.1097/00000658-195106000-00002[↩]
- Benassai G, Mastrorilli M, Quarto G, Cappiello A, Giani U, Forestieri P, Mazzeo F. Factors influencing survival after resection for ductal adenocarcinoma of the head of the pancreas. J Surg Oncol. 2000 Apr;73(4):212-8. doi: 10.1002/(sici)1096-9098(200004)73:4<212::aid-jso5>3.0.co;2-d[↩]
- Cheng L, Tian F, Zhao T, Pang Y, Luo Z, Ren J. Annular pancreas concurrent with pancreaticobiliary maljunction presented with symptoms until adult age: case report with comparative data on pediatric cases. BMC Gastroenterol. 2013 Oct 25;13:153. doi: 10.1186/1471-230X-13-153[↩]
- Whittingham-Jones PM, Riaz AA, Clayton G, et al. Annular pancreas – a rare cause of gastric obstruction in an 82-year-old patient. Ann R Coll Surg Engl 2005;87:W13-5. 10.1308/147870804902[↩]
- Yamaguchi Y, Sugiyama M, Sato Y, et al. Annular pancreas complicated by carcinoma of the bile duct: diagnosis by MR cholangiopancreatography and endoscopic ultrasonography. Abdom Imaging 2003;28:381-3. 10.1007/s00261-002-0051-1[↩]
- Maker V, Gerzenshtein J, Lerner T. Annular pancreas in the adult: two case reports and review of more than a century of literature. Am Surg. 2003 May;69(5):404-10.[↩][↩]
- Zeineb M, Sadri BA, Nizar M, Hassen H, Nafaa A, Taher K. Annular pancreas intra operatively discovered: a case report. Clin Pract. 2011 Oct 28;1(4):e82. doi: 10.4081/cp.2011.e82[↩]
- Urayama S, Kozarek R, Ball T, Brandabur J, Traverso L, Ryan J, Wechter D. Presentation and treatment of annular pancreas in an adult population. Am J Gastroenterol. 1995 Jun;90(6):995-9.[↩][↩]
- Pezzilli R, Uomo G, Gabbrielli A, Zerbi A, Frulloni L, De Rai P, Castoldi L, Cavallini G, Di Carlo V; ProInf-AISP Study Group. A prospective multicentre survey on the treatment of acute pancreatitis in Italy. Dig Liver Dis. 2007 Sep;39(9):838-46. doi: 10.1016/j.dld.2007.05.014[↩]
- Benassai G, Mastrorilli M, Quarto G, Cappiello A, Giani U, Mosella G. Survival after pancreaticoduodenectomy for ductal adenocarcinoma of the head of the pancreas. Chir Ital. 2000 May-Jun;52(3):263-70.[↩]
- Castoldi L, De Rai P, Zerbi A, Frulloni L, Uomo G, Gabbrielli A, Bassi C, Pezzilli R; ProInf-AISP (Progetto Informatizzato Pancreatite Acuta, Associazione Italiana per lo Studio del Pancreas) Study Group. Long term outcome of acute pancreatitis in Italy: results of a multicentre study. Dig Liver Dis. 2013 Oct;45(10):827-32. doi: 10.1016/j.dld.2013.03.012[↩]
- Conzo G, Circelli L, Pasquali D, Sinisi A, Sabatino L, Accardo G, Renzullo A, Santini L, Salvatore F, Colantuoni V. Lessons to be learned from the clinical management of a MEN 2A patient bearing a novel 634/640/700 mutation of the RET proto-oncogene. Clin Endocrinol (Oxf). 2012 Dec;77(6):934-6. doi: 10.1111/j.1365-2265.2012.04412.x[↩]
- Dicitore A, Caraglia M, Gaudenzi G, Manfredi G, Amato B, Mari D, Persani L, Arra C, Vitale G. Type I interferon-mediated pathway interacts with peroxisome proliferator activated receptor-γ (PPAR-γ): at the cross-road of pancreatic cancer cell proliferation. Biochim Biophys Acta. 2014 Jan;1845(1):42-52. doi: 10.1016/j.bbcan.2013.11.003[↩]
- Conzo G, Tartaglia E, Gambardella C, Mauriello C, Esposito D, Mascolo M, Russo D, Stornaiuolo G, Gaeta GB, Santini L. Suprarenal solitary fibrous tumor associated with a NF1 gene mutation mimicking a kidney neoplasm: implications for surgical management. World J Surg Oncol. 2014 Apr 7;12:87. doi: 10.1186/1477-7819-12-87[↩]
- Noh TH, Lee SE, Park JM. Laparoscopic treatment of annular pancreas in adults: report of a case. Korean J Hepatobiliary Pancreat Surg 2012;16:43-5. 10.14701/kjhbps.2012.16.1.43[↩]
- Turkvatan A, Erden A, Turkoglu MA, Yener O. Congenital variants and anomalies of the pancreas and pancreatic duct: imaging by magnetic resonance cholangiopancreaticography and multidetector computed tomography. Korean J Radiol. 2013;14(6):905–913. doi: 10.3348/kjr.2013.14.6.905[↩]
- Adibelli ZH, Adatepe M, Imamoglu C, Esen OS, Erkan N, Yildirim M. Anatomic variations of the pancreatic duct and their relevance with the Cambridge classification system: MRCP findings of 1158 consecutive patients. Radiol Oncol. 2016;50(4):370–377. doi: 10.1515/raon-2016-0041[↩]
- Bulow R, Simon P, Thiel R, Thamm P, Messner P, Lerch MM, Mayerle J. et al. Anatomic variants of the pancreatic duct and their clinical relevance: an MR-guided study in the general population. Eur Radiol. 2014;24(12):3142–3149. doi: 10.1007/s00330-014-3359-7[↩]
- Vitellas KM, Keogan MT, Spritzer CE, Nelson RC. MR cholangiopancreatography of bile and pancreatic duct abnormalities with emphasis on the single-shot fast spin-echo technique. Radiographics. 2000 Jul-Aug;20(4):939-57; quiz 1107-8, 1112. doi: 10.1148/radiographics.20.4.g00jl23939. Erratum in: Radiographics 2000 Sep-Oct;20(5):1494.[↩]
- Li YL, Yu ML, Lee KH. The crossing duct sign. Abdom Radiol (NY). 2018 Jun;43(6):1506-1507. doi: 10.1007/s00261-017-1312-3[↩]
- Rizzo RJ, Szucs RA, Turner MA. Congenital abnormalities of the pancreas and biliary tree in adults. Radiographics. 1995 Jan;15(1):49-68; quiz 147-8. doi: 10.1148/radiographics.15.1.7899613[↩]
- Nijs EL, Callahan MJ. Congenital and developmental pancreatic anomalies: ultrasound, computed tomography, and magnetic resonance imaging features. Semin Ultrasound CT MR. 2007 Oct;28(5):395-401. doi: 10.1053/j.sult.2007.08.001[↩]
- Whittingham-Jones PM, Riaz AA, Clayton G, Thompson HH. Annular pancreas – a rare cause of gastric obstruction in an 82-year-old patient. Ann R Coll Surg Engl. 2005 Jan;87(1):W13-5. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1963855/pdf/16790121.pdf[↩][↩]
- Nguyen BD. C-11 Choline and F-18 Fluciclovine PET/CT demonstration of annular pancreas. Dig Liver Dis. 2018 Aug;50(8):853. doi: 10.1016/j.dld.2018.03.018[↩]
- Zyromski NJ, Sandoval JA, Pitt HA, Ladd AP, Fogel EL, Mattar WE, Sandrasegaran K, Amrhein DW, Rescorla FJ, Howard TJ, Lillemoe KD, Grosfeld JL. Annular pancreas: dramatic differences between children and adults. J Am Coll Surg. 2008 May;206(5):1019-25; discussion 1025-7. doi: 10.1016/j.jamcollsurg.2007.12.009[↩][↩][↩]
- Chatterjee A, Rana SS. Endoscopic Ultrasound in Pancreatic Duct Anomalies. Diagnostics (Basel). 2023 Oct 5;13(19):3129. doi: 10.3390/diagnostics13193129[↩][↩][↩]
- Reinhart RD, Brown JJ, Foglia RP, Aliperti G. MR imaging of annular pancreas. Abdom Imaging. 1994 Jul-Aug;19(4):301-3. doi: 10.1007/BF00198183[↩]
- Dharmsathaphorn K, Burrell M, Dobbins J. Diagnosis of annular pancreas with endoscopic retrograde cholangiopancreatography. Gastroenterology. 1979 Nov;77(5):1109-14.[↩]
- Gress F., Yiengpruksawan A., Sherman S., Ikenberry S., Kaster S., Ng R.Y., Cerulli M.A., Lehman G.A. Diagnosis of annular pancreas by endoscopic ultrasound. Gastrointest. Endosc. 1996;44:485–489. doi: 10.1016/S0016-5107(96)70108-6[↩]
- Papachristou GI, Topazian MD, Gleeson FC, Levy MJ. EUS features of annular pancreas (with video). Gastrointest Endosc. 2007 Feb;65(2):340-4. doi: 10.1016/j.gie.2006.10.010[↩][↩]
- Noh TH, Lee SE, Park JM. Laparoscopic treatment of annular pancreas in adults: report of a case. Korean J Hepatobiliary Pancreat Surg. 2012 Feb;16(1):43-5. doi: 10.14701/kjhbps.2012.16.1.43[↩]
- Traubici J. The double bubble sign. Radiology. 2001 Aug;220(2):463-4. doi: 10.1148/radiology.220.2.r01au11463[↩]
- Adedeji OA, Trescoli-Serrano C, Garcia-Zarco M. Primary duodenal carcinoma. Postgrad Med J. 1995 Jun;71(836):354-8. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2398148/pdf/postmedj00030-0036.pdf[↩]
- Thomford NR, Knight PR, Pace WG, et al. Annular pancreas in the adult: selection of operation. Ann Surg 1972;176:159-62. 10.1097/00000658-197208000-00007[↩]
- Jimenez JC, Emil S, Podnos Y, Nguyen N. Annular pancreas in children: a recent decade’s experience. J Pediatr Surg. 2004 Nov;39(11):1654-7. doi: 10.1016/j.jpedsurg.2004.07.003[↩]
- Yigiter M, Yildiz A, Firinci B, Yalcin O, Oral A, Salman AB. Annular pancreas in children: a decade of experience. Eurasian J Med. 2010 Dec;42(3):116-9. doi: 10.5152/eajm.2010.33[↩]





{kind=link}