
What is antiperspirant
An antiperspirant is a chemical agent that reduces perspiration or sweating. The active ingredients of roll-on, spray and powder formulations are traditionally the metallic salts aluminium chloride and aluminium chlorohydrate. These are formulated into preparations of varying strengths. More concentrated solutions are used to control excessive sweating (hyperhidrosis).
Newer generation antiperspirants contain aluminium zirconium compounds. These are better tolerated by the skin and are less likely to cause irritation or aggravation to razor burn.
Diphemanil methylsulfate powder may also be used to reduce perspiration. It is particularly useful on an amputation stump to reduce irritation by a prosthesis.
The National Library of Medicine’s Household Products Database (https://hpd.nlm.nih.gov/) has information about the ingredients used in most major brands of deodorants and antiperspirants.
Deodorants are not antiperspirants. Deodorants do not prevent sweating. Their aim is to mask the smell produced by sweat-eating bacteria. An antiperspirant preparation may contain a deodorant.
How do antiperspirants work?
Aluminium-based antiperspirants work by blocking the sweat ducts, thereby reducing the amount of sweat that reaches the skin’s surface. Aluminium salts are soluble as long as the formulation is acidic (low pH). When they are applied to the skin and come in contact with sweat, the pH rises causing the aluminium salts to precipitate out and form a plug over the sweat glands. Sweat continues to be produced by the sweat gland but it just isn’t able to reach the surface of the skin.
Diphemanil methylsulfate is a drug that opposes the action of the parasympathetic nerves that control sweat production.
How do you use an antiperspirant?
A higher concentration antiperspirant is usually more effective than a low concentration or aluminium-free preparation. However, increasing the strength can also increase the potential for side effects. A couple of simple rules apply to their use.
- Apply to dry skin, after a cool shower at bedtime. During sleep sweating is limited and the active ingredients have a better chance of being absorbed into the sweat glands. Wash off in the morning.
- Apply on a regular basis as directed by your doctor. Initially, this may be 7-10 nights in a row, then reducing to every other night for one week. When improvements are seen, patients can move to a maintenance schedule of using it once every 7–12 days. Over time reapplication may be needed even less frequently.
Where can you use an antiperspirant?
Antiperspirants are often the first line of treatment for underarm hyperhidrosis as they are readily available from the pharmacy or supermarket. Antiperspirants may also be used in other sites of the body that tend to sweat excessively. If standard preparations fail, stronger strength preparations are available at your pharmacy.
Sweat is a dilute salt solution produced by eccrine sweat glands spontaneously or in response to heat, exercise and stressful events. Eccrine sweat is initially odorless but can start to smell if bacteria get a chance to break down the stale sweat. The eccrine glands are distributed over the entire body but are most numerous under the arms and on the palms and soles.
Apocrine sweat glands are located under the arms, around the breasts and in the groin. After puberty, they produce a thick secretion that contains pheromones, the “personal scent” that most people find unpleasant. In addition, bacteria that normally live on the skin break down apocrine sweat and this produces offensive body odour. Body odour is worse if there are more bacteria present or the level of apocrine sweat production is high. Antiperspirants also help to reduce apocrine sweat production.
Precautions when using an antiperspirant
Avoid applying antiperspirants to mucous membranes (mouth, nose, eyelids, genitals, anus).
Antiperspirants may cause irritant or allergic contact dermatitis. This may be from the active ingredient or diluents in the preparation. The skin around the underarm area is particularly prone to develop these reactions because it is thin, delicate, moist and occluded.
People at risk of developing a reaction to an antiperspirant include those with:
- Eczema
- Sensitive skin
- Contact allergy to fragrance, preservative or dye
- Susceptibility to razor burn
To reduce the possibility of reactions less concentrated preparations should be used in susceptible groups.
In rare cases, where a hair follicle is blocked over a long period of time, a cyst may develop. Infected cysts damage the ducts and form painful hard lumps that may need to be surgically removed.
Use of diphemanil methylsulfate on the face may lead to dry mouth and other “muscarinic” (anticholinergic) side effects. It should not be used in young babies as it has been reported to cause toxicity.
Does antiperspirant cause breast cancer?
Use of antiperspirants and breast cancer
For some time, an email rumor 1 suggested that underarm antiperspirants cause breast cancer. Among its claims:
- Cancer-causing substances in antiperspirants are absorbed through razor nicks from underarm shaving. These substances are said to be deposited in the lymph nodes under the arm, which are not able to get rid of them by sweating because the antiperspirant keeps you from perspiring. This causes a high concentration of toxins, which leads to cells mutating into cancer.
- Most breast cancers develop in the upper outer quadrant of the breast because that area is closest to the lymph nodes exposed to antiperspirants. (Think of the breast as a circle divided by vertical and horizontal lines that cross at the nipple. Each of the 4 sectors you divide the breast into is called a quadrant. The upper outer quadrant of each breast is the part closest to the arm pit.)
- Men have a lower risk of breast cancer because they do not shave their underarms, and their underarm hair keeps chemicals in antiperspirants from being absorbed.
All of these claims are largely false and untrue 2.
There are no strong epidemiologic studies 3, 4, 5, 6, 7, 8, 9, 10, 11 in the medical literature that link breast cancer risk and antiperspirant use, and very little scientific evidence to support this claim. If you’re still concerned that your underarm antiperspirant or deodorant could increase your risk of cancer, choose products that don’t contain chemicals that worry you.
In fact, a carefully designed epidemiologic study of this issue published in 2002 12 compared 813 women with breast cancer and 793 women without the disease. The researchers found no link between breast cancer risk and antiperspirant use, deodorant use, or underarm shaving.
A study published in 2003 13 looked at responses from questionnaires sent out to women who had breast cancer. The researcher reported that women who were diagnosed with breast cancer at a younger age said they used antiperspirant and started shaving their underarms earlier and shaved more often than women who were diagnosed when they were older. But the study design did not include a control group of women without breast cancer and has been criticized by experts as not relevant to the safety of these underarm hygiene practices.
Probably, in general, younger women are more likely than older women to shave their underarms and use antiperspirants, whether or not they develop breast cancer later. For instance, most women born in the 1950s and 1960s might have started shaving earlier and using antiperspirants more often than women born in the 1930s and 1940s. Many women may also shave and use antiperspirants less often as they get older. These are more likely explanations of the researcher’s findings than the suggestion that these practices cause cancer. Of note, the study asked about underarm products that the women were using at the time the questions were answered, not what they used before they developed breast cancer.
How did the rumor about antiperspirants get started and spread?
Cancer experts don’t know who started this rumor. Most people who forwarded the email did so with good intentions. Cancer experts do know that this rumor has been posted on some websites that sell deodorants that are not antiperspirants, so some people might benefit financially from spread of this misinformation.
What is known about the ingredients in antiperspirants and deodorants?
Aluminum-based compounds are used as the active ingredient in antiperspirants. These compounds form a temporary “plug” within the sweat duct that stops the flow of sweat to the skin’s surface. Some research suggests that aluminum-containing underarm antiperspirants, which are applied frequently and left on the skin near the breast, may be absorbed by the skin and have estrogen-like (hormonal) effects 8.
Because estrogen can promote the growth of breast cancer cells, some scientists have suggested that the aluminum-based compounds in antiperspirants may contribute to the development of breast cancer 8. In addition, it has been suggested that aluminum may have direct activity in breast tissue 9. However, no studies to date have confirmed any substantial adverse effects of aluminum that could contribute to increased breast cancer risks. A 2014 review concluded there was no clear evidence showing that the use of aluminum-containing underarm antiperspirants or cosmetics increases the risk of breast cancer 14.
Some research has focused on parabens, which are preservatives used in some deodorants and antiperspirants that have been shown to mimic the activity of estrogen in the body’s cells 15. It has been reported that parabens are found in breast tumors, but there is no evidence that they cause breast cancer. Although parabens are used in many cosmetic, food, and pharmaceutical products, most deodorants and antiperspirants in the United States do not currently contain parabens.
What is known about the relationship between antiperspirants or deodorants and breast cancer?
Only a few studies have investigated a possible relationship between breast cancer and underarm antiperspirants/deodorants. One study, published in 2002, did not show any increase in risk for breast cancer among women who reported using an underarm antiperspirant or deodorant 10. The results also showed no increase in breast cancer risk among women who reported using a blade (nonelectric) razor and an underarm antiperspirant or deodorant, or among women who reported using an underarm antiperspirant or deodorant within 1 hour of shaving with a blade razor. These conclusions were based on interviews with 813 women with breast cancer and 793 women with no history of breast cancer.
A subsequent study, published in 2006, also found no association between antiperspirant use and breast cancer risk, although it included only 54 women with breast cancer and 50 women without breast cancer 11.
A 2003 retrospective cohort study examining the frequency of underarm shaving and antiperspirant/deodorant use among 437 breast cancer survivors 16 reported younger age at breast cancer diagnosis for women who used antiperspirants/deodorants frequently or who started using them together with shaving at an earlier age. Because of the retrospective nature of the study, the results are not conclusive.
Because studies of antiperspirants and deodorants and breast cancer have provided conflicting results, additional research would be needed to determine whether a relationship exists 3.
Does using antiperspirant after shaving allow chemicals to enter the body from the armpit and increase breast cancer risk?
Razor nicks may increase the risk of skin infection. If the underarm skin is already broken or infected, it is possible that some antiperspirants could cause slight irritation. But it is unlikely that this is a major source of carcinogens (cancer-causing substances) that get into the body and reach the breast cells.
Should I be concerned about parabens?
Parabens are chemicals used as preservatives and as food additives. They can be found in many types of make-up (like lipstick, mascara, concealer, and foundation) and skin care products (like lotion, shaving products, and sunscreen). Parabens can be absorbed through the skin.
Intake of parabens is a possible concern because studies have shown that parabens have weak estrogen-like properties. Estrogen is a female hormone known to cause breast cells (both normal and cancerous) to grow and divide. And some conditions that increase the body’s exposure to estrogen (like not having children, late menopause, obesity, etc.) have been linked to an increased risk of breast cancer.
In 2004, a small study 17 found traces of parabens in some samples of breast cancer tumors. But there are some important points about the study findings:
- The researchers looked only for the presence of parabens in breast cancer samples. The study did not show that parabens caused or contributed to breast cancer development in these cases – it only showed that they were there. What this meant is not yet clear.
- Although parabens have weak estrogen-like properties, the estrogens that are made in the body are hundreds to many thousands of times stronger. So, natural estrogens (or those taken as hormone replacement) are much more likely to play a role in breast cancer development.
- Parabens are widely used as preservatives in shampoo, lotions, other cosmetics, and even foods. This study did not contain any information to help find the source of the parabens found in the breast tissue – it’s not clear if they might have come from antiperspirants or from some other source.
Most people are exposed to parabens. In fact, studies have found some form of parabens in the urine in up to 99% of people in the US. But so far, studies have not shown any direct link between parabens and any health problems, including breast cancer. There are also many other compounds in the environment that mimic naturally produced estrogen.
Although at this time there are no clear health risks from parabens in food, drugs, cosmetics, and skin care products, people concerned about exposure to parabens can avoid products containing them. Consumer products containing parabens are required to list them as ingredients. Most parabens have names containing the word “paraben,” making them easy to find. According to the US Food and Drug Administration, most major brands of antiperspirants and deodorants do not currently contain parabens.
Should I be concerned about aluminum in antiperspirants?
Aluminum-based compounds are the active ingredients in antiperspirants. They block the sweat glands to keep sweat from getting to the skin’s surface. Some research 18 has suggested that these aluminum compounds may be absorbed by the skin and cause changes in estrogen receptors of breast cells. Because estrogen can promote the growth of both cancer and non-cancer breast cells, some scientists have suggested that using the aluminum-based compounds in antiperspirants may be a risk factor for the development of breast cancer.
But it isn’t clear that much aluminum is absorbed through the skin. One study that looked at the absorption of aluminum from antiperspirants containing aluminum chlorohydrate applied to the underarms found that only a tiny fraction (0.012%) was absorbed. The actual amount of aluminum absorbed would be much less than what would be expected to be absorbed from the foods a person eats during the same time.
It also doesn’t seem that breast cancer tissue contains more aluminum than normal breast tissue. A study that looked at women with breast cancer found no real difference in the concentration of aluminum between the cancer and the surrounding normal tissue.
At this point, no clear link has been made between antiperspirants containing aluminum and breast cancer.
Do antiperspirants keep a person from sweating cancer-causing toxins out through their underarm lymph nodes?
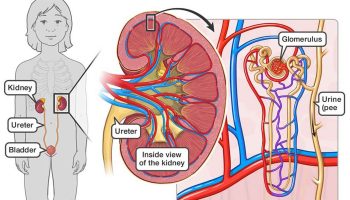
Lymph nodes help clear out bacteria, viruses, and other possible threats to the body, but the lymph nodes do not release waste or toxins through sweating. In fact, lymph nodes are not connected to sweat glands. Sweat glands are located in the skin, not in the lymph nodes. Most cancer-causing substances that enter the body are removed from the blood by the kidneys and by the liver. Substances removed by the kidneys are released into urine, while those taken by the liver are released into bile. The bile then mixes with and is eliminated with feces.
Are there lymph nodes in the upper outer quadrant where most breast tumors occur?
Lymph nodes can be found throughout the breasts and have an important role. The underarm (axillary) nodes filter most of the liquid lymph flowing out of the breast before it goes back into the body’s bloodstream. These nodes are under the arm, in the upper outer quadrant of the breast, and near the collarbone.
The breast quadrants are not actually all the same size. About half of all breast cancers develop in the upper outer part of the breast, probably because there is more breast tissue in this area. The number of breast cancers in the upper outer part of the breast is in proportion to the amount of breast tissue in that area.
There is no evidence to suggest that the location of cancers within the breast is related to using antiperspirants or underarm shaving.
Are men less likely to get breast cancer because antiperspirant gets caught in their underarm hair and is not absorbed by their skin?
Men are much less likely than women to develop breast cancer, mostly because men have much less breast tissue than women. Women have about 100 times more breast tissue than men and are about 100 times more likely to develop breast cancer.
Hormones also play a role. Men with metabolic or genetic conditions that lead to increased estrogen levels have an increased risk of developing breast cancer.
Underarm hair and antiperspirant absorption have not been linked to male breast cancer risk.
Why does my doctor tell me not to use antiperspirant or deodorant on the day of my mammogram?
You are asked to not use antiperspirant or deodorant on the day you get a mammogram because many of these products contain aluminum. This metal can show up on a mammogram as tiny specks. These specks can look like microcalcifications, which are one of the things doctors look for as a possible sign of cancer. Not using these products helps prevent any confusion when the mammogram films are reviewed.
How can I learn more about breast cancer risk factors and ways to find breast cancer early, when treatment works best?
Women concerned about breast cancer can learn about risk factors for breast cancer and possible strategies to reduce breast cancer risk in Breast Cancer Risk and Prevention.
You can also talk to your doctor, nurse, or other health care providers. The American Cancer Society has information about all aspects of breast cancer, from causes and prevention, to diagnosis and treatment.
Risk Factors for Breast Cancer
A risk factor is anything that affects your chance of getting a disease, such as breast cancer. But having a risk factor, or even many, does not mean that you are sure to get the disease. While you can’t change some breast cancer risk factors—family history and aging, for example—there are some risk factors that you can control.
Certain breast cancer risk factors are related to personal behaviors, such as diet and exercise. Other lifestyle-related risk factors include decisions about having children and taking medicines that contain hormones.
Drinking alcohol
Drinking alcohol is clearly linked to an increased risk of breast cancer. The risk increases with the amount of alcohol consumed. Compared with non-drinkers, women who have 1 alcoholic drink a day have a very small increase in risk. Those who have 2 to 3 drinks a day have about a 20% higher risk compared to women who don’t drink alcohol. Excessive alcohol consumption is known to increase the risk of other cancers, too.
The American Cancer Society recommends that women who drink have no more than 1 drink a day.
Being overweight or obese
Being overweight or obese after menopause increases breast cancer risk. Before menopause your ovaries make most of your estrogen, and fat tissue makes only a small amount. After menopause (when the ovaries stop making estrogen), most of a woman’s estrogen comes from fat tissue. Having more fat tissue after menopause can raise estrogen levels and increase your chance of getting breast cancer. Also, women who are overweight tend to have higher blood insulin levels. Higher insulin levels have been linked to some cancers, including breast cancer.
Still, the link between weight and breast cancer risk is complex. For instance, risk appears to be increased for women who gained weight as an adult, but may not be increased among those who have been overweight since childhood. Also, excess fat in the waist area may affect risk more than the same amount of fat in the hips and thighs. Researchers believe that fat cells in various parts of the body have subtle differences that may explain this.
Weight might also have different effects on different types of breast cancer. For example, some research suggests that being overweight before menopause might increase your risk of triple-negative breast cancer.
The American Cancer Society recommends you stay at a healthy weight throughout your life and avoid excess weight gain by balancing your food intake with physical activity.
Not being physically active
Evidence is growing that regular physical activity reduces breast cancer risk, especially in women past menopause. The main question is how much activity is needed. Some studies have found that even as little as a couple of hours a week might be helpful , although more seems to be better.
Exactly how physical activity might reduce breast cancer risk isn’t clear, but it may be due to its effects on body weight, inflammation, hormones, and energy balance.
The American Cancer Society recommends that adults get at least 150 minutes of moderate intensity or 75 minutes of vigorous intensity activity each week (or a combination of these), preferably spread throughout the week.
Not having children
Women who have not had children or who had their first child after age 30 have a slightly higher breast cancer risk overall. Having many pregnancies and becoming pregnant at an early age reduces breast cancer risk. Still, the effect of pregnancy seems to be different for different types of breast cancer. For a certain type of breast cancer known as triple-negative, pregnancy seems to increase risk.
Not breastfeeding
Some studies suggest that breastfeeding may slightly lower breast cancer risk, especially if it’s continued for 1½ to 2 years. But this has been hard to study, especially in countries like the United States, where breastfeeding for this long is uncommon.
The explanation for this possible effect may be that breastfeeding reduces a woman’s total number of lifetime menstrual cycles (the same as starting menstrual periods at a later age or going through early menopause).
Birth control
Some birth control methods use hormones, which might increase breast cancer risk.
- Oral contraceptives: Most studies have found that women using oral contraceptives (birth control pills) have a slightly higher risk of breast cancer than women who have never used them. Once the pills are stopped, this risk seems to go back to normal over time. Women who stopped using oral contraceptives more than 10 years ago do not appear to have any increased breast cancer risk.
- Birth control shot: Depo-Provera is an injectable form of progesterone that’s given once every 3 months for birth control. Some studies have found that women currently using birth-control shots seem to have an increase in breast cancer risk, but it appears that there is no increased risk in women 5 years after they stop getting the shots.
- Birth control implants, intrauterine devices (IUDs), skin patches, vaginal rings: These forms of birth control also use hormones, which in theory could fuel breast cancer growth. Some studies have shown a link between use of hormone-releasing IUDs and breast cancer risk, but few studies have looked at the use of birth control implants, patches, and rings and breast cancer risk.
When thinking about using hormonal birth control, women should discuss their other risk factors for breast cancer with their health care provider.
Hormone therapy after menopause
Hormone therapy with estrogen (often combined with progesterone) has been used for many years to help relieve symptoms of menopause and help prevent osteoporosis (thinning of the bones). This treatment goes by many names, such as post-menopausal hormone therapy, hormone replacement therapy (HRT), and menopausal hormone therapy.
There are 2 main types of hormone therapy. For women who still have a uterus (womb), doctors generally prescribe estrogen and progesterone (known as combined hormone therapy). Progesterone is needed because estrogen alone can increase the risk of cancer of the uterus. For women who’ve had a hysterectomy (who no longer have a uterus), estrogen alone can be used. This is known as estrogen replacement therapy or just estrogen therapy.
- Combined hormone therapy: Use of combined hormone therapy after menopause increases the risk of breast cancer. It may also increase the chances of dying from breast cancer. This increase in risk can be seen with as little as 2 years of use. Combined hormone therapy also increases the likelihood that the cancer may be found at a more advanced stage. The increased risk from combined hormone therapy appears to apply only to current and recent users. A woman’s breast cancer risk seems to return to that of the general population within 5 years of stopping treatment.
- Bioidentical hormone therapy: The word bioidentical is sometimes used to describe versions of estrogen and progesterone with the same chemical structure as those found naturally in people. The use of these hormones has been marketed as a safe way to treat the symptoms of menopause. But because there aren’t many studies comparing “bioidentical” or “natural” hormones to synthetic versions of hormones, there’s no proof that they’re safer or more effective. More studies are needed to know for sure. The use of these bioidentical hormones should be considered to have the same health risks as any other type of hormone therapy.
- Estrogen therapy: The use of estrogen alone after menopause does not seem to increase the risk of breast cancer much, if at all. But when used long term (for more than 15 years), estrogen therapy has been found to increase the risk of ovarian and breast cancer in some studies.
At this time there aren’t many strong reasons to use post-menopausal hormone therapy (either combined hormone therapy or estrogen therapy), other than possibly for the short-term relief of menopausal symptoms. Along with the increased risk of breast cancer, combined hormone therapy also appears to increase the risk of heart disease, blood clots, and strokes. It does lower the risk of colorectal cancer and osteoporosis, but this must be weighed against the possible harms, especially since there are other ways to prevent and treat osteoporosis, and screening can sometimes prevent colon cancer. Estrogen therapy does not seem to increase breast cancer risk, but it does increase the risk of stroke.
The decision to use hormone therapy should be made by a woman and her doctor after weighing the possible risks and benefits (including the severity of her menopausal symptoms), and considering her other risk factors for heart disease, breast cancer, and osteoporosis. If they decide she should try hormone therapy for symptoms of menopause, it’s usually best to use it at the lowest dose that works for her and for as short a time as possible.
Breast implants
Silicone breast implants can cause scar tissue to form in the breast. Implants make breast tissue harder to see on standard mammograms, but additional x-ray pictures called implant displacement views can be used to examine the breast tissue more completely.
Certain types of breast implants can be linked to a rare type of cancer called anaplastic large cell lymphoma (ALCL). It’ is sometimes referred to as breast implant-associated anaplastic large cell lymphoma (BIA-ALCL). This lymphoma appears to happen more often in implants with textured (rough) surfaces rather than smooth surfaces. If ALCL does show up after an implant, it can show up as a lump, a collection of fluid near the implant, pain, swelling or asymmetry (uneven breasts). It usually responds well to treatment.
Risk factors you Cannot Change
Some risk factors for breast cancer are things you cannot change, such as being a woman, getting older, and having certain gene changes. These make your risk of breast cancer higher.
Being a woman
- Simply being a woman is the main risk factor for breast cancer. Men can get breast cancer, too, but this disease is about 100 times more common in women than in men.
Getting older
- As you get older, your risk of breast cancer goes up. Most breast cancers are found in women age 55 and older.
Certain inherited genes
About 5% to 10% of breast cancer cases are thought to be hereditary, meaning that they result directly from gene defects (called mutations) passed on from a parent.
BRCA1 and BRCA2: The most common cause of hereditary breast cancer is an inherited mutation in the BRCA1 or BRCA2 gene. In normal cells, these genes help make proteins that repair damaged DNA. Mutated versions of these genes can lead to abnormal cell growth, which can lead to cancer.
- If you have inherited a mutated copy of either gene from a parent, you have a higher risk of breast cancer.
- On average, a woman with a BRCA1 or BRCA2 gene mutation has about a 7 in 10 chance of getting breast cancer by age 80. This risk is also affected by how many other family members have had breast cancer. (It goes up if more family members are affected.)
- Women with one of these mutations are more likely to be diagnosed with breast cancer at a younger age, as well as to have cancer in both breasts. They also have a higher risk of developing some other cancers, mainly ovarian cancer.
- In the United States, BRCA mutations are more common in Jewish people of Ashkenazi (Eastern Europe) origin than in other racial and ethnic groups, but anyone can have them.
Changes in other genes: Other gene mutations can also lead to inherited breast cancers. These gene mutations are much less common, and most of them do not increase the risk of breast cancer as much as the BRCA genes.
- ATM: The ATM gene normally helps repair damaged DNA (or helps kill the cell if the damaged can’t be fixed). Inheriting 2 abnormal copies of this gene causes the disease ataxia-telangiectasia. Inheriting one abnormal copy of this gene has been linked to a high rate of breast cancer in some families.
- TP53: The TP53 gene gives instructions for making a protein called p53 that helps stop the growth of abnormal cells. Inherited mutations of this gene cause Li-Fraumeni syndrome. People with this syndrome have an increased risk of breast cancer, as well as some other cancers such as leukemia, brain tumors, and sarcomas (cancers of bones or connective tissue). This mutation is a rare cause of breast cancer.
- CHEK2: The CHEK2 gene is another gene that normally helps with DNA repair. A CHEK2 mutation can increase breast cancer risk about 2-fold.
- PTEN: The PTEN gene normally helps regulate cell growth. Inherited mutations in this gene can cause Cowden syndrome, a rare disorder that puts people at higher risk for both non-cancer and cancer tumors in the breasts, as well as growths in the digestive tract, thyroid, uterus, and ovaries.
- CDH1: Inherited mutations in this gene cause hereditary diffuse gastric cancer, a syndrome in which people develop a rare type of stomach cancer. Women with mutations in this gene also have an increased risk of invasive lobular breast cancer.
- STK11: Defects in this gene can lead to Peutz-Jeghers syndrome. People affected with this disorder have pigmented spots on their lips and in their mouths, polyps (abnormal growths) in the urinary and digestive tracts, and a higher risk of many types of cancer, including breast cancer.
- PALB2: The PALB2 gene makes a protein that interacts with the protein made by the BRCA2 gene. Mutations in this gene can lead to a higher risk of breast cancer.
Mutations in several other genes have also been linked to breast cancer, but these account for only a small number of cases.
Genetic testing: Genetic testing can be done to look for mutations in the BRCA1 and BRCA2 genes (or less commonly in other genes such as PTEN or TP53). While testing can be helpful in some cases, not every woman needs to be tested, and the pros and cons need to be considered carefully.
One concern is that some genetic tests are promoted to doctors and the public without giving full information. For example, a test for a small number of BRCA1 and BRCA2 gene mutations has been approved by the FDA. However, there are more than 1,000 known BRCA mutations, and the ones included in the approved test are not the most common ones. This means there are many BRCA mutations that would not be detected by this test.
If you’re thinking about genetic testing, it’s strongly recommended that you first talk to a genetic counselor, nurse, or doctor who can explain these tests. It’s very important to understand what genetic testing can and can’t tell you, and to carefully weigh the benefits and risks of genetic testing before these tests are done. Testing costs a lot and might not be covered by some health insurance plans.
Having a family history of breast cancer
It’s important to note that most women (about 8 out of 10) who get breast cancer do not have a family history of the disease. But women who have close blood relatives with breast cancer have a higher risk:
- Having a first-degree relative (mother, sister, or daughter) with breast cancer almost doubles a woman’s risk. Having 2 first-degree relatives increases her risk about 3-fold.
- Women with a father or brother who have had breast cancer also have a higher risk of breast cancer.
Overall, less than 15% of women with breast cancer have a family member with this disease.
Having a personal history of breast cancer
A woman with cancer in one breast has a higher risk of developing a new cancer in the other breast or in another part of the same breast. (This is different from a recurrence or return of the first cancer.) Although this risk is low overall, it’s even higher for younger women with breast cancer.
Your race and ethnicity
Overall, white women are slightly more likely to develop breast cancer than African-American women. But in women under age 45, breast cancer is more common in African-American women. African-American women are also more likely to die from breast cancer at any age. Asian, Hispanic, and Native American women have a lower risk of developing and dying from breast cancer.
Having dense breast tissue
Breasts are made up of fatty tissue, fibrous tissue, and glandular tissue. Someone is said to have dense breasts (on a mammogram) when they have more glandular and fibrous tissue and less fatty tissue. Women with dense breasts on mammogram have a risk of breast cancer that is about 1.5 to 2 times that of women with average breast density. Unfortunately, dense breast tissue can also make it harder to see cancers on mammograms.
A number of factors can affect breast density, such as age, menopausal status, the use of certain drugs (including menopausal hormone therapy), pregnancy, and genetics.
Certain benign breast conditions
Women diagnosed with certain benign (non-cancer) breast conditions may have a higher risk of breast cancer. Some of these conditions are more closely linked to breast cancer risk than others. Doctors often divide benign breast conditions into 3 groups, depending on how they affect this risk.
Non-proliferative lesions: These conditions don’t seem to affect breast cancer risk, or if they do, the increase in risk is very small. They include:
- Fibrosis and/or simple cysts (sometimes called fibrocystic changes or disease)
- Mild hyperplasia
- Adenosis (non-sclerosing)
- Phyllodes tumor (benign)
- A single papilloma
- Fat necrosis
- Duct ectasia
- Periductal fibrosis
- Squamous and apocrine metaplasia
- Epithelial-related calcifications
- Other tumors (lipoma, hamartoma, hemangioma, neurofibroma, adenomyoepithelioma)
Mastitis (infection of the breast) is not a tumor and does not increase the risk of breast cancer.
Proliferative lesions without atypia (cell abnormalities): In these conditions there’s excessive growth of cells in the ducts or lobules of the breast, but the cells don’t look very abnormal. These conditions seem to raise a woman’s risk of breast cancer slightly. They include:
- Usual ductal hyperplasia (without atypia)
- Fibroadenoma
- Sclerosing adenosis
- Several papillomas (called papillomatosis)
- Radial scar
Proliferative lesions with atypia: In these conditions, the cells in the ducts or lobules of the breast tissue grow excessively, and some of them no longer look normal. These types of lesions include:
- Atypical ductal hyperplasia (ADH)
- Atypical lobular hyperplasia (ALH)
Breast cancer risk is about 4 to 5 times higher than normal in women with these changes. If a woman also has a family history of breast cancer and either hyperplasia or atypical hyperplasia, she has an even higher risk of breast cancer.
Lobular carcinoma in situ (LCIS)
In lobular carcinoma in situ (LCIS), cells that look like cancer cells are growing in the lobules of the milk-producing glands of the breast, but they are not growing through the wall of the lobules. Lobular carcinoma in situ (LCIS) is also called lobular neoplasia. It’s sometimes grouped with ductal carcinoma in situ (DCIS) as a non-invasive breast cancer, but it differs from DCIS in that it doesn’t seem to become invasive cancer if it isn’t treated.
Women with lobular carcinoma in situ (LCIS) have a much higher risk of developing cancer in either breast.
Starting menstruation (periods) early
Women who have had more menstrual cycles because they started menstruating early (especially before age 12) have a slightly higher risk of breast cancer. The increase in risk may be due to a longer lifetime exposure to the hormones estrogen and progesterone.
Going through menopause after age 55
Women who have had more menstrual cycles because they went through menopause later (after age 55) have a slightly higher risk of breast cancer. The increase in risk may be because they have a longer lifetime exposure to the hormones estrogen and progesterone.
Having radiation to your chest
Women who were treated with radiation therapy to the chest for another cancer (such as Hodgkin disease or non-Hodgkin lymphoma) when they were younger have a significantly higher risk for breast cancer. This varies with the patient’s age when they got radiation. The risk is highest if you had radiation as a teen or young adult, when your breasts were still developing. Radiation treatment after age 40 does not seem to increase breast cancer risk.
Exposure to diethylstilbestrol (DES)
From the 1940s through the early 1970s some pregnant women were given an estrogen-like drug called DES because it was thought to lower their chances of losing the baby (miscarriage). These women have a slightly increased risk of developing breast cancer. Women whose mothers took DES during pregnancy may also have a slightly higher risk of breast cancer.
Factors with Unclear Effects on Breast Cancer Risk
There are some things that might be risk factors for breast cancer, but the research is not yet clear about whether they really affect breast cancer risk. They include things like tobacco smoke and working at night.
Diet and vitamins
While being overweight or obese and not being physically active have been linked to breast cancer risk, the possible link between diet and breast cancer risk is less clear. Results of some studies have shown that diet may play a role, while others have not found that diet influences breast cancer risk.
Most studies of women in the United States have not found a link between breast cancer risk and fat in the diet. Still, studies have found that breast cancer is less common in countries where the typical diet is low in total fat, low in polyunsaturated fat, and low in saturated fat. Researchers are still not sure how to explain this. It may be at least partly due to the effect of diet on body weight. Also, studies comparing diet and breast cancer risk in different countries are complicated by other differences (such as activity level, intake of other nutrients, and genetic factors) that might also affect breast cancer risk.
Cancer experts do know that high-fat diets can lead to being overweight or obese, which is a known breast cancer risk factor. A diet high in fat is also a risk factor for some other types of cancer. And intake of certain types of fat is clearly related to higher risk of heart disease.
Studies looking at vitamin levels have had inconsistent results. So far, no study has shown that taking vitamins reduces the risk of breast cancer (or any other cancer). But this does not mean that there’s no point in eating a healthy diet. A diet low in fat, low in red meat and processed meat, and high in fruits and vegetables can clearly have other health benefits, including lowering the risk of some other cancers.
Chemicals in the environment
A great deal of research has been reported and more is being done to understand possible environmental influences on breast cancer risk.
Compounds in the environment that have estrogen-like properties are of special interest. For example, substances found in some plastics, certain cosmetics and personal care products, pesticides, and PCBs (polychlorinated biphenyls) seem to have such properties. In theory, these could affect breast cancer risk.
This issue causes a great deal of public concern, but at this time research does not show a clear link between breast cancer risk and exposure to these substances. Studying such effects in humans is hard to do. More research is needed to better define the possible health effects of these substances and others like them.
Tobacco smoke
For a long time, studies showed no link between cigarette smoking and breast cancer. But in recent years, more studies have shown that heavy smoking over a long time might be linked to a higher risk of breast cancer. In some studies, the risk has been highest in certain groups, such as women who started smoking before they had their first child. The 2014 US Surgeon General’s report on smoking concluded that there is “suggestive but not sufficient” evidence that smoking increases the risk of breast cancer.
Researchers are also looking at whether secondhand smoke increases the risk of breast cancer. Both mainstream and secondhand smoke contain chemicals that, in high concentrations, cause breast cancer in rodents. Studies have shown that chemicals in tobacco smoke reach breast tissue and are found in breast milk of rodents. In human studies, the evidence on secondhand smoke and breast cancer risk is not clear. Most studies have not found a link, but some studies have suggested it may increase risk, particularly in premenopausal women. The 2014 US Surgeon General’s report concluded that there is “suggestive but not sufficient” evidence of a link at this point. In any case, this possible link to breast cancer is yet another reason to avoid secondhand smoke.
Night shift work
Some studies have suggested that women who work at night, such as nurses on a night shift, might have an increased risk of breast cancer. This is a fairly recent finding, and more studies are looking at this. Some researchers think the effect may be due to changes in levels of melatonin, a hormone that’s affected by the body’s exposure to light, but other hormones are also being studied.
Who decides which environmental exposures cause cancer in humans?
Two organizations—the National Toxicology Program (NTP), an interagency program of the U.S. Department of Health and Human Services (HHS), and the International Agency for Research on Cancer (IARC), the cancer agency of the World Health Organization—have developed lists of substances that, based on the available scientific evidence, are known or are reasonably anticipated to be human carcinogens.
Specifically, the National Toxicology Program publishes the Report on Carcinogens every few years. This congressionally mandated publication identifies agents, substances, mixtures, or exposures (collectively called “substances”) in the environment that may cause cancer in humans. The 2016, 14th Report on Carcinogens (https://ntp.niehs.nih.gov/pubhealth/roc/index-1.html) lists 248 known human carcinogens (https://ntp.niehs.nih.gov/ntp/roc/content/listed_substances_508.pdf) and includes descriptions of the process for preparing the science-based report and the criteria used to list a substance as a carcinogen.
The International Agency for Research on Cancer (IARC) also produces science-based reports (https://monographs.iarc.fr/agents-classified-by-the-iarc/) on substances that can increase the risk of cancer in humans. Since 1971, the agency has evaluated more than 900 agents (https://monographs.iarc.fr/list-of-classifications-volumes/), including chemicals, complex mixtures, occupational exposures, physical agents, biological agents, and lifestyle factors. Of these, more than 400 have been identified as carcinogenic (https://monographs.iarc.fr/wp-content/uploads/2018/07/Table4.pdf), probably carcinogenic, or possibly carcinogenic to humans.
The International Agency for Research on Cancer (IARC) convenes expert scientists to evaluate the evidence that an agent can increase the risk of cancer. The agency describes the principles, procedures, and scientific criteria that guide the evaluations. For instance, agents are selected for review based on two main criteria: (a) there is evidence of human exposure and (b) there is some evidence or suspicion of carcinogenicity.
Substances Listed in the National Toxicology Program Fourteenth Report on Carcinogens (https://ntp.niehs.nih.gov/ntp/roc/content/listed_substances_508.pdf):
Known To Be Human Carcinogens
- Aflatoxins
- Alcoholic Beverage Consumption
- 4‑Aminobiphenyl
- Analgesic Mixtures Containing Phenacetin (see Phenacetin and Analgesic Mixtures Containing Phenacetin)
- Aristolochic Acids
- Arsenic and Inorganic Arsenic Compounds
- Asbestos
- Azathioprine
- Benzene
- Benzidine (see Benzidine and Dyes Metabolized to Benzidine)
- Beryllium and Beryllium Compounds
- Bis(chloromethyl) Ether and Technical-Grade Chloromethyl Methyl Ether
- 1,3-Butadiene
- 1,4-Butanediol Dimethanesulfonate
- Cadmium and Cadmium Compounds
- Chlorambucil
- 1-(2-Chloroethyl)-3-(4-methylcyclohexyl)-1-nitrosourea (see Nitrosourea Chemotherapeutic Agents)
- Chromium Hexavalent Compounds
- Coal Tars and Coal-Tar Pitches
- Coke-Oven Emissions
- Cyclophosphamide
- Cyclosporin A
- Diethylstilbestrol
- Dyes Metabolized to Benzidine (Benzidine Dye Class) (see Benzidine and Dyes Metabolized to Benzidine)
- Epstein-Barr Virus (see Viruses: Eight Listings)
- Erionite
- Estrogens, Steroidal
- Ethylene Oxide
- Formaldehyde
- Hepatitis B Virus (see Viruses: Eight Listings)
- Hepatitis C Virus (see Viruses: Eight Listings)
- Human Immunodeficiency Virus Type 1 (see Viruses: Eight Listings)
- Human Papillomaviruses: Some Genital-Mucosal Types (see Viruses: Eight Listings)
- Human T-Cell Lymphotrophic Virus Type 1 (see Viruses: Eight Listings)
- Kaposi Sarcoma–Associated Herpesvirus (see Viruses: Eight Listings)
- Melphalan
- Merkel Cell Polyomavirus (see Viruses: Eight Listings)
- Methoxsalen with Ultraviolet A Therapy
- Mineral Oils: Untreated and Mildly Treated
- Mustard Gas
- 2-Naphthylamine
- Neutrons (see Ionizing Radiation)
- Nickel Compounds (see Nickel Compounds and Metallic Nickel)
- Radon (see Ionizing Radiation)
- Silica, Crystalline (Respirable Size)
- Solar Radiation (see Ultraviolet Radiation Related Exposures)
- Soots
- Strong Inorganic Acid Mists Containing Sulfuric Acid
- Sunlamps or Sunbeds, Exposure to (see Ultraviolet Radiation Related Exposures)
- Tamoxifen
- 2,3,7,8-Tetrachlorodibenzo-p-dioxin
- Thiotepa
- Thorium Dioxide (see Ionizing Radiation)
- Tobacco Smoke, Environmental (see Tobacco-Related Exposures)
- Tobacco Smoking (see Tobacco-Related Exposures)
- Tobacco, Smokeless (see Tobacco-Related Exposures)
- o‑Toluidine
- Trichloroethylene
- Ultraviolet Radiation, Broad-Spectrum (see Ultraviolet Radiation Related Exposures)
- Vinyl Chloride (see Vinyl Halides [selected])
- Wood Dust
- X-Radiation and Gamma Radiation (see Ionizing Radiation)
Reasonably Anticipated To Be Human Carcinogens
- Acetaldehyde
- 2‑Acetylaminofluorene
- Acrylamide
- Acrylonitrile
- Adriamycin
- 2‑Aminoanthraquinone
- o‑Aminoazotoluene
- 1-Amino-2,4-dibromoanthraquinone
- 2‑Amino-3,4-dimethylimidazo[4,5‑f]quinoline (see Heterocyclic Amines [Selected])
- 2‑Amino-3,8-dimethylimidazo[4,5‑f]quinoxaline (see Heterocyclic Amines [Selected])
- 1‑Amino-2-methylanthraquinone
- 2‑Amino-3-methylimidazo[4,5‑f]quinoline (see Heterocyclic Amines [Selected])
- 2‑Amino-1-methyl-6-phenylimidazo[4,5‑b]pyridine (see Heterocyclic Amines [Selected])
- Amitrole
- o-Anisidine and Its Hydrochloride
- Azacitidine
- Basic Red 9 Monohydrochloride
- Benz[a]anthracene (see Polycyclic Aromatic Hydrocarbons: 15 Listings)
- Benzo[b]fluoranthene (see Polycyclic Aromatic Hydrocarbons: 15 Listings)
- Benzo[j]fluoranthene (see Polycyclic Aromatic Hydrocarbons: 15 Listings)
- Benzo[k]fluoranthene (see Polycyclic Aromatic Hydrocarbons: 15 Listings)
- Benzo[a]pyrene (see Polycyclic Aromatic Hydrocarbons: 15 Listings)
- Benzotrichloride
- 2,2-Bis(bromomethyl)-1,3-propanediol (Technical Grade)
- Bis(chloroethyl) Nitrosourea (see Nitrosourea Chemotherapeutic Agents)
- Bromodichloromethane
- 1-Bromopropane
- Butylated Hydroxyanisole
- Captafol
- Carbon Tetrachloride
- Ceramic Fibers (Respirable Size)
- Chloramphenicol
- Chlorendic Acid
- Chlorinated Paraffins (C12, 60% Chlorine)
- Chloroform
- 1-(2-Chloroethyl)-3-cyclohexyl-1-nitrosourea (see Nitrosourea Chemotherapeutic Agents)
- 3-Chloro-2-methylpropene
- 4-Chloro-o-phenylenediamine
- Chloroprene
- p-Chloro-o-toluidine and Its Hydrochloride
- Chlorozotocin (see Nitrosourea Chemotherapeutic Agents)
- Cisplatin
- Cobalt and Cobalt Compounds That Release Cobalt Ions In Vivo (see Cobalt-Related Exposures)
- Cobalt–Tungsten Carbide: Powders and Hard Metals (see Cobalt-Related Exposures)
- p‑Cresidine
- Cumene
- Cupferron
- Dacarbazine
- Danthron
- 2,4‑Diaminoanisole Sulfate
- 2,4‑Diaminotoluene
- Diazoaminobenzene
- Dibenz[a,h]acridine (see Polycyclic Aromatic Hydrocarbons: 15 Listings)
- Dibenz[a,j]acridine (see Polycyclic Aromatic Hydrocarbons: 15 Listings)
- Dibenz[a,h]anthracene (see Polycyclic Aromatic Hydrocarbons: 15 Listings)
- 7H-Dibenzo[c,g]carbazole (see Polycyclic Aromatic Hydrocarbons: 15 Listings)
- Dibenzo[a,e]pyrene (see Polycyclic Aromatic Hydrocarbons: 15 Listings)
- Dibenzo[a,h]pyrene (see Polycyclic Aromatic Hydrocarbons: 15 Listings)
- Dibenzo[a,i]pyrene (see Polycyclic Aromatic Hydrocarbons: 15 Listings)
- Dibenzo[a,l]pyrene (see Polycyclic Aromatic Hydrocarbons: 15 Listings)
- 1,2-Dibromo-3-chloropropane
- 1,2-Dibromoethane
- 2,3-Dibromo-1-propanol
- 1,4-Dichlorobenzene
- 3,3′-Dichlorobenzidine and Its Dihydrochloride
- Dichlorodiphenyltrichloroethane
- 1,2-Dichloroethane
- Dichloromethane
- 1,3-Dichloropropene (Technical Grade)
- Diepoxybutane
- Diesel Exhaust Particulates
- Di(2-ethylhexyl) Phthalate
- Diethyl Sulfate
- Diglycidyl Resorcinol Ether
- 3,3′-Dimethoxybenzidine (see 3,3′-Dimethoxybenzidine and Dyes Metabolized to 3,3′-Dimethoxybenzidine)
- 4‑Dimethylaminoazobenzene
- 3,3′-Dimethylbenzidine (see 3,3′-Dimethylbenzidine and Dyes Metabolized to 3,3′-Dimethylbenzidine)
- Dimethylcarbamoyl Chloride
- 1,1‑Dimethylhydrazine
- Dimethyl Sulfate
- Dimethylvinyl Chloride
- 1,6-Dinitropyrene (see Nitroarenes [Selected])
- 1,8-Dinitropyrene (see Nitroarenes [Selected])
- 1,4-Dioxane
- Disperse Blue 1
- Dyes Metabolized to 3,3′-Dimethoxybenzidine (3,3′-Dimethoxybenzidine Dye Class) (see 3,3′-Dimethoxybenzidine and Dyes Metabolized to
- 3,3′-Dimethoxybenzidine)
- Dyes Metabolized to 3,3′-Dimethylbenzidine (3,3′-Dimethylbenzidine Dye Class) (see 3,3′-Dimethylbenzidine and Dyes Metabolized to
- 3,3′-Dimethylbenzidine)
- Epichlorohydrin
- Ethylene Thiourea
- Ethyl Methanesulfonate
- Furan
- Glass Wool Fibers (Inhalable), Certain
- Glycidol
- Hexachlorobenzene
- Hexachloroethane
- Hexamethylphosphoramide
- Hydrazine and Hydrazine Sulfate
- Hydrazobenzene
- Indeno[1,2,3-cd]pyrene (see Polycyclic Aromatic Hydrocarbons: 15 Listings)
- Iron Dextran Complex
- Isoprene
- Kepone
- Lead and Lead Compounds
- Lindane, Hexachlorocyclohexane (Technical Grade), and Other Hexachlorocyclohexane Isomers
- 2-Methylaziridine
- 5-Methylchrysene (see Polycyclic Aromatic Hydrocarbons: 15 Listings)
- 4,4′-Methylenebis(2-chloroaniline)
- 4,4′-Methylenebis(N,N-dimethyl)benzenamine
- 4,4′‑Methylenedianiline and Its Dihydrochloride
- Methyleugenol
- Methyl Methanesulfonate
- N-Methyl-N′-Nitro-N-Nitrosoguanidine (see N-Nitrosamines: 15 Listings)
- Metronidazole
- Michler’s Ketone
- Mirex
- Naphthalene
- Nickel, Metallic (see Nickel Compounds and Metallic Nickel)
- Nitrilotriacetic Acid
- o-Nitroanisole
- Nitrobenzene
- 6-Nitrochrysene (see Nitroarenes [Selected])
- Nitrofen
- Nitrogen Mustard Hydrochloride
- Nitromethane
- 2-Nitropropane
- 1-Nitropyrene (see Nitroarenes [Selected])
- 4-Nitropyrene (see Nitroarenes [Selected])
- N-Nitrosodi-n-butylamine (see N-Nitrosamines: 15 Listings)
- N-Nitrosodiethanolamine (see N-Nitrosamines: 15 Listings)
- N-Nitrosodiethylamine (see N-Nitrosamines: 15 Listings)
- N-Nitrosodimethylamine (see N-Nitrosamines: 15 Listings)
- N-Nitrosodi-n-propylamine (see N-Nitrosamines: 15 Listings)
- N-Nitroso-N-ethylurea (see N-Nitrosamines: 15 Listings)
- 4-(N-Nitrosomethylamino)-1-(3-pyridyl)-1-butanone (see N-Nitrosamines: 15 Listings)
- N-Nitroso-N-methylurea (see N-Nitrosamines: 15 Listings)
- N-Nitrosomethylvinylamine (see N-Nitrosamines: 15 Listings)
- N-Nitrosomorpholine (see N-Nitrosamines: 15 Listings)
- N-Nitrosonornicotine (see N-Nitrosamines: 15 Listings)
- N-Nitrosopiperidine (see N-Nitrosamines: 15 Listings)
- N-Nitrosopyrrolidine (see N-Nitrosamines: 15 Listings)
- N-Nitrososarcosine (see N-Nitrosamines: 15 Listings)
- o-Nitrotoluene
- Norethisterone
- Ochratoxin A
- 4,4′‑Oxydianiline
- Oxymetholone
- Pentachlorophenol and By-products of Its Synthesis
- Phenacetin (see Phenacetin and Analgesic Mixtures Containing Phenacetin)
- Phenazopyridine Hydrochloride
- Phenolphthalein
- Phenoxybenzamine Hydrochloride
- Phenytoin and Phenytoin Sodium
- Polybrominated Biphenyls
- Polychlorinated Biphenyls
- Procarbazine and Its Hydrochloride
- Progesterone
- 1,3‑Propane Sultone
- β‑Propiolactone
- Propylene Oxide
- Propylthiouracil
- Reserpine
- Riddelliine
- Safrole
- Selenium Sulfide
- Streptozotocin (see Nitrosourea Chemotherapeutic Agents)
- Styrene
- Styrene-7,8-oxide
- Sulfallate
- Tetrachloroethylene
- Tetrafluoroethylene
- Tetranitromethane
- Thioacetamide
- 4,4′-Thiodianiline
- Thiourea
- Toluene Diisocyanates
- Toxaphene
- 2,4,6-Trichlorophenol
- 1,2,3-Trichloropropane
- Tris(2,3-dibromopropyl) Phosphate
- Ultraviolet Radiation A (see Ultraviolet Radiation Related Exposures)
- Ultraviolet Radiation B (see Ultraviolet Radiation Related Exposures)
- Ultraviolet Radiation C (see Ultraviolet Radiation Related Exposures)
- Urethane
- Vinyl Bromide (see Vinyl Halides [Selected])
- 4-Vinyl-1-cyclohexene Diepoxide
- Vinyl Fluoride (see Vinyl Halides [Selected])
What is cobalt and where is it found?
Cobalt is a metal found naturally in soil, dust, and seawater. It is usually found in association with nickel. Cobalt and its salts have many uses, the table below shows some of the many sources of cobalt and where or how we may come into contact with them either at home or at work. Cobalt is may be found in some antiperspirant preparations.
Home/personal sources
- Cobalt blue pigment in porcelain, glass, pottery, ceramics and enamels
- Cobalt blue in blue and green watercolor paints and crayons
- Metal-plated objects
- Buckles
- Buttons
- Zippers
- Snaps
- Costume jewellery
- Utensils
- Tools
Medical uses
- Vitamin B12 preparations for the treatment of anemia
- Metal prostheses
- Dental plates
Hair dyes; cobalt pigment produces light brown shades of hair
Antiperspirant preparations
Work sources
- Cobalt used as binding agent in hard metals to create drills, cutting tools, mechanical parts
- Cobalt naphthenate is a common catalyst in the manufacture of polyester resins
- Manufacture of cobalt-containing alloys
- As an oxidizing agent in automobile exhaust controls, in the rubber tire industry and in electroplating
- Cement industry; cement contains cobalt oxides
- Cobalt siccatives or driers are found in certain paints and varnishes
- Binding agent in the carbide industry
- Wet clay containing cobalt used by pottery workers
Methods to minimise cobalt exposure
- Use metal instruments such as scissors, kitchen utensils and combs that have plastic or wooden handle grips
- If necessary, wear vinyl or rubber gloves to avoid contact (however, do not use for wet work as moisture increases the penetration of cobalt into the skin)
- Items such as keys can be coated with several layer of clear nail polish
- In the workplace, wear protective clothing and employ no-touch techniques
In the workplace try to avoid exposure to cobalt, however this may not be practicable thus use measures to minimize exposure as described above. Identify potential sources of exposure using Material Safety Data Sheets; these are required for all chemicals and substances that you may come into contact with in the workplace. If you must use products that contain cobalt, wear gloves or other protective clothing to avoid contact with your skin.
Outside of the workplace, the best way to avoid cobalt allergy is by being aware of the possible sources of cobalt. Read product labels and do not use any that contain cobalt or any of its alternative names. If unsure ask your pharmacist for advice or a suitable alternative. Only use cosmetics, antiperspirants and hair dyes that you know do not contain cobalt. Avoid metallic costume jewellery. Sterling silver and platinum jewellery is usually tolerated.
A cobalt allergy spot test kit containing disodium-1-nitroso-2-naphthol-3,6-disulfonate (nitroso R salt) is available from contact allergen supply companies and can be used to detect cobalt in metal items such as jewellery.
Alert your doctor or dentist to the fact that you have an allergy to cobalt. Your dermatologist may have further specific advice, particularly if you are highly sensitive to cobalt.
What are the reactions to cobalt allergy?
Reactions to contact with cobalt in an allergic individual include allergic contact dermatitis and irritant contact dermatitis. Cobalt was named Contact Allergen of the Year 2016 by the American Contact Dermatitis Society.
Vitamin B12 injections administered to allergic individuals may produce a red, tender and itchy area around the site of the injection. Oral ingestion of vitamin B12 is known to cause intractable hand eczema is some patients.
In many cases, allergic reactions are not caused solely by cobalt sensitization. For example, metal objects almost always also contain nickel and in the cement industry nickel and chromium are present. Nickel and chromium are also potent sensitizers therefore; allergic reactions may not be due solely to cobalt but also to simultaneous specific allergy to nickel and chromium.
Cobalt allergy may cause an erythema multiforme-like eruption. It may also cause an airborne contact dermatitis.
Am I allergic to cobalt?
Cobalt allergy is diagnosed from the clinical history and by performing patch tests.
Nickel and cobalt are always found together in alloys and salts because it is too costly and impracticable to separate these two metals. Thus patch testing should always include both cobalt and nickel. Patch test results with cobalt and nickel can be confusing as it is extremely difficult to obtain pure solutions of each individual metal. Cross-reaction between cobalt and nickel is not very frequent, as patch tests have shown several patients with strong reactions to cobalt but not to nickel. Combined allergic reactions are not uncommon and represent simultaneous specific sensitisations to each individual metal as opposed to being cross-reactions. Intradermal testing with cobalt may also be performed to diagnose cobalt sensitivity. Current thinking is that a diagnosis of allergic dermatitis to cobalt is justified if the following criteria are matched.
Confirmed diagnosis of allergic cobalt dermatitis
- Patient actually exposed to cobalt
- Positive patch test to 2% cobalt chloride in aqueous solution
- Intracutaneous test with 1:1000 cobalt chloride gives a delayed tuberculin reaction in a non-atopic individual
Management of cobalt allergy
Identifying possible sources of contact and avoiding them is the only long-term management strategy for cobalt allergy. Once the dermatitis appears on the skin, treatment is as for any acute dermatitis/eczema:
- Topical corticosteroids
- Emollients
- Treatment of secondary bacterial infection (Staphylococcus aureus).
Where avoidance is not achievable, several methods can be used to try to minimize exposure. Brief contact with metal devices is usually not a problem except in highly sensitive individuals.
- Robb-Nicholson C. By the way, doctor. I recently received an e-mail warning about a risk for breast cancer associated with using antiperspirants. Are you familiar with this theory? Is it valid? Harvard Womens Health Watch. 2001;8:7[↩]
- Antiperspirants/Deodorants and Breast Cancer. https://www.cancer.gov/about-cancer/causes-prevention/risk/myths/antiperspirants-fact-sheet[↩]
- Dieterich M, Stubert J, Reimer T, Erickson N, Berling A. Influence of lifestyle factors on breast cancer risk. Breast Care 2014; 9(6):407-414.[↩][↩]
- Hardefeldt PJ, Edirimanne S, Eslick GD. Deodorant use and breast cancer risk. Epidemiology. 2013 Jan;24(1):172.[↩]
- McGrath KG. An earlier age of breast cancer diagnosis related to more frequent use of antiperspirants/deodorants and underarm shaving. Eur J Cancer Prev. 2003;12:479-485[↩]
- Namer M, Luporsi E, Gligorov J, Lokiec F, Spielmann M. The use of deodorants/antiperspirants does not constitute a risk factor for breast cancer [article in French]. Bull Cancer. 2008;95:871-880.[↩]
- Surendran A. Studies linking breast cancer to deodorants smell rotten, experts say. Nature Medicine. 2004;10:216.[↩]
- Darbre PD. Aluminium, antiperspirants and breast cancer. Journal of Inorganic Biochemistry 2005; 99(9):1912–1919.[↩][↩][↩]
- Darbre PD, Mannello F, Exley C. Aluminium and breast cancer: Sources of exposure, tissue measurements and mechanisms of toxicological actions on breast biology. Journal of Inorganic Biochemistry 2013; 128:257-261.[↩][↩]
- Mirick DK, Davis S, Thomas DB. Antiperspirant use and the risk of breast cancer. Journal of the National Cancer Institute 2002; 94(20):1578–1580.[↩][↩]
- Fakri S, Al-Azzawi A, Al-Tawil N. Antiperspirant use as a risk factor for breast cancer in Iraq. Eastern Mediterranean Health Journal 2006; 12(3–4):478–482.[↩][↩]
- Mirick DK, Davis S, Thomas, DB: Antiperspirant Use and the Risk of Breast Cancer. J Natl Cancer Inst. 2002;94:1578-1580.[↩]
- An earlier age of breast cancer diagnosis related to more frequent use of antiperspirants/deodorants and underarm shaving. Eur J Cancer Prev. 2003 Dec;12(6):479-85. https://www.ncbi.nlm.nih.gov/pubmed/14639125[↩]
- Willhite CC, Karyakina NA, Yokel RA, et al. Systematic review of potential health risks posed by pharmaceutical, occupational and consumer exposures to metallic and nanoscale aluminum, aluminum oxides, aluminum hydroxide and its soluble salts. Critical Reviews in Toxicology 2014; 44 Suppl 4:1-80.[↩]
- Final amended report on the safety assessment of Methylparaben, Ethylparaben, Propylparaben, Isopropylparaben, Butylparaben, Isobutylparaben, and Benzylparaben as used in cosmetic productsExit Disclaimer. International Journal of Toxicology 2008; 27 Suppl 4:1-82. doi: 10.1080/10915810802548359[↩]
- McGrath KG. An earlier age of breast cancer diagnosis related to more frequent use of antiperspirants/deodorants and underarm shaving. European Journal of Cancer 2003; 12(6):479–485.[↩]
- Darbre PD, Aljarrah A, Miller WR, et al. Concentrations of parabens in human breast tumours. J Appl Toxicol. 2004;24:5-13.[↩]
- Rodrigues-Peres RM, Cadore S, Febraio S, Heinrich JK, Serra KP, Derchain SF, Vassallo J, Sarian LO. Aluminum concentrations in central and peripheral areas of malignant breast lesions do not differ from those in normal breast tissues. BMC Cancer. 2013 Mar 8;13:104.[↩]


{kind=link}