Contents
What is ascites
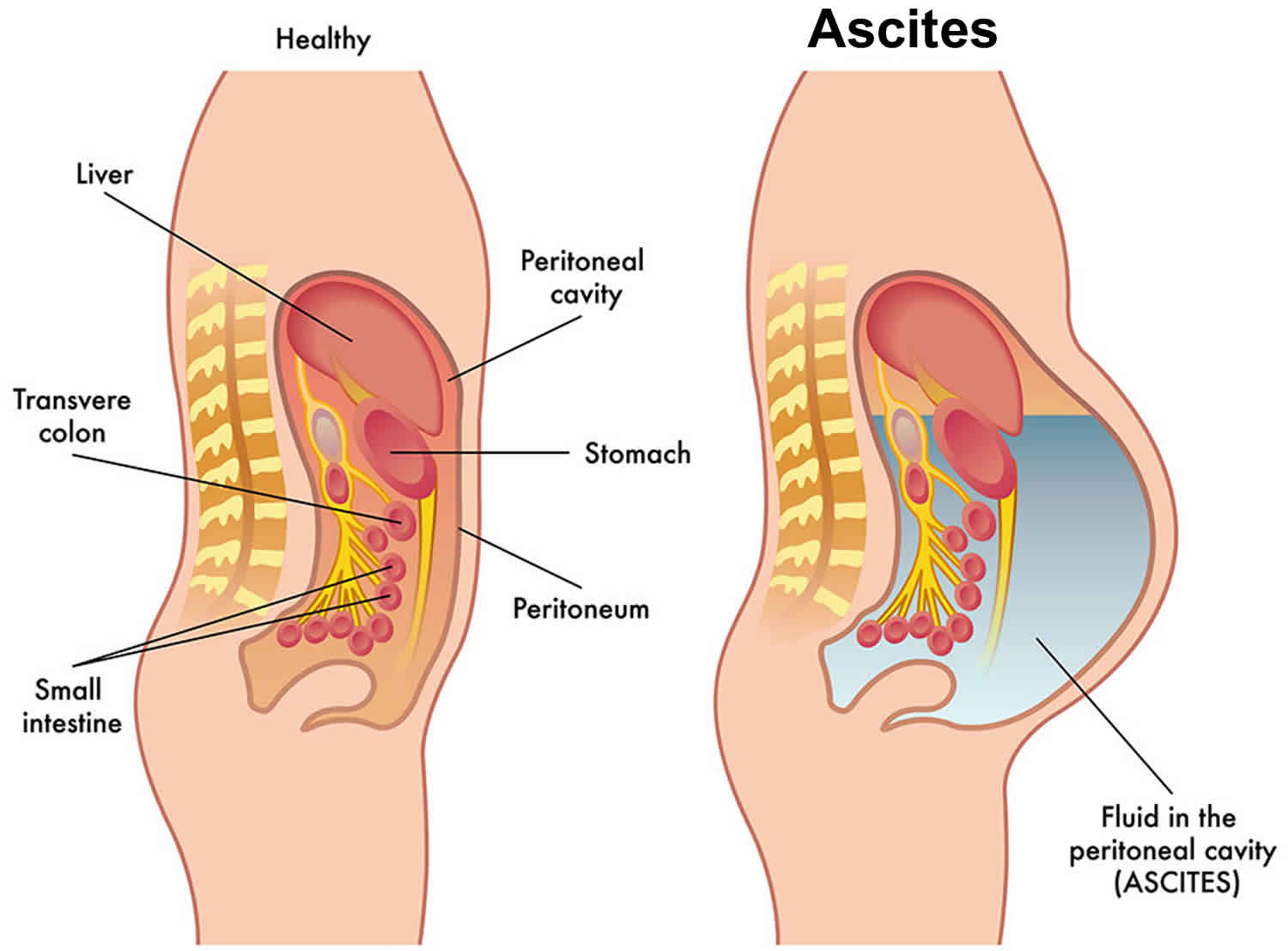
Ascites also called peritoneal effusion, is the build-up of peritoneal (abdominal) fluid in the space between the lining of the abdomen and abdominal organs. The tummy (abdomen) contains many organs, including the stomach, bowels, pancreas, liver, spleen and kidneys. There is a sheet of tissue (called the peritoneum) around these organs. It is made up of 2 layers. One layer lines the wall of the abdomen. The other covers the organs. The layers produce a small amount of fluid so that the organs in the abdomen can move smoothly. Sometimes fluid builds up between the 2 layers, which makes the abdomen swell. This can be very uncomfortable. This fluid build up is called ascites.
Ascites symptoms may develop slowly or suddenly depending on the cause of ascites. You may have no symptoms if there is only a small amount of fluid in your belly. As more fluid collects, you may have abdominal pain and bloating. Large amounts of fluid can cause shortness of breath. Many other symptoms of liver failure may also be present.
The two main reasons that ascites may collect in your abdominal cavity are:
- An imbalance between the pressure within blood vessels—which drives fluid out of blood vessels—and the amount of protein in blood—which keeps fluid in blood vessels. The fluid that accumulates in this case is called a transudate. Transudates are most often caused by congestive heart failure, nephrotic syndrome, or hepatic cirrhosis.
- An injury or inflammation of the peritoneum, in which case the fluid is called an exudate. This type of fluid may be the result of conditions such as infection, malignancies (metastatic cancer, lymphoma, mesothelioma), pancreatitis, ruptured gallbladder, or autoimmune disease.
Determining the type of ascites fluid present (transudate or exudates) is important because it helps narrow down the possible causes of ascites fluid buildup or inflammation. Healthcare practitioners and laboratorians use an initial set of tests, including cell count, serum and fluid albumin levels, and appearance of the ascites fluid, to distinguish between transudates and exudates. Once the fluid is determined to be one or the other, additional tests may be performed to further pinpoint the disease or condition causing ascites.
For diagnosis of ascites, your doctor will do a physical exam to determine the amount of swelling in your belly.
You may also have the following tests to assess your liver and kidneys:
- 24-hour urine collection
- Electrolyte levels
- Kidney function tests
- Liver function tests
- Tests to measure the risk of bleeding and protein levels in the blood
- Urinalysis
- Abdominal ultrasound
Your doctor may also use a thin needle to withdraw ascites fluid from your belly. The peritoneal fluid is tested to look for the cause of ascites.
If you have ascites, see your health care provider right away if you have:
- Fever above 100.5°F (38.05°C), or a fever that does not go away
- Belly pain
- Blood in your stool or black, tarry stools
- Blood in your vomit
- Bruising or bleeding that occurs easily
- Build-up of fluid in your belly
- Swollen legs or ankles
- Breathing problems
- Confusion or problems staying awake
- Yellow color in your skin and the whites of your eyes (jaundice)
Ascites fluid analysis
Ascites fluid analysis is used to help diagnose the cause of fluid buildup in your abdomen (ascites) and/or inflammation of the peritoneum (peritonitis). There are two main reasons for fluid accumulation, and an initial set of tests is used to differentiate between the two types of fluid that may be produced, transudate or exudate. These tests typically include:
- Fluid albumin level—the serum-ascites albumin gradient (SAAG) calculation (serum albumin level minus the fluid albumin level) may be used to differentiate between transudates and exudates. A serum-ascites albumin gradient (SAAG) level of 1.1 g/dL or greater suggests the presence of a transudate and less than 1.1 g/dL, an exudate.
- Cell count and differential
- Appearance
Transudate—an imbalance between the pressure within blood vessels (which drives fluid out of the blood vessel) and the amount of protein in blood (which keeps fluid in the blood vessel) can result in accumulation of fluid (called a transudate). Transudates are most often caused by congestive heart failure , nephrotic syndrome, or hepatic cirrhosis. If the fluid is determined to be a transudate, then usually no more tests on the fluid are necessary.
Exudate—injury or inflammation of the peritoneum may cause abnormal collection of fluid (called an exudate). Exudates are associated with infections, malignancies, pancreatitis, ruptured gallbladder, or autoimmune disease. Laboratory tests may be performed to determine one of the following conditions:
- Infectious diseases caused by viruses, bacteria, or fungi; infections may originate in the peritoneum due to a rupture of the appendix, perforation of the intestines or the abdominal wall, contamination during surgery, or an infection from other places in the body that has spread to the peritoneum.
- Inflammatory conditions – peritonitis due to certain chemicals, irradiation, or rarely an autoimmune disorder
- Malignancies – such as mesothelioma, tumor of the liver (hepatoma), lymphoma, or metastatic cancer
- Pancreatitis – due to certain drugs, infections, blockages, and circulating lipids (fats)
Additional testing on exudate fluid may include:
- Peritoneal fluid glucose, amylase, tumor markers, bilirubin, creatinine, lactate dehydrogenase (LD)
- Microscopic examination – may be performed if infection or cancer is suspected; a laboratory professional may use a special centrifuge (cytocentrifuge) to concentrate the fluid’s cells on a slide. The slide is treated with a special stain and evaluated for abnormal cells, such as malignant cells (cancer cells).
- Gram stain – for direct observation of bacteria or fungi under a microscope
- Bacterial culture and susceptibility testing – ordered to detect the presence of any microbes that have grown in the culture and to guide antimicrobial therapy
- Less commonly ordered tests for infectious diseases, such as tests for viruses, mycobacteria (AFB testing in identifying tuberculosis), and parasites
- Adenosine deaminase – rarely ordered for detecting tuberculosis in peritoneal fluid
Ascites causes
Ascites results from high pressure in the blood vessels of the liver (portal hypertension) and low levels of a protein called albumin. Diseases that can cause severe liver damage can lead to ascites. These include long-term hepatitis C or B infection and alcohol abuse over many years, and more and more frequently, fatty liver disease (non-alcoholic steatohepatitis).
People with certain cancers in the abdomen may develop ascites. These include cancer of the appendix, colon, ovaries, uterus, pancreas, and liver.
Other conditions that can cause ascites include:
- Clots in the veins of the liver (portal vein thrombosis)
- Congestive heart failure
- Pancreatitis
- Thickening and scarring of the sac-like covering of the heart
Kidney dialysis may also be linked to ascites.
Transudate
Most ascitic fluids are transudates and are caused by either congestive heart failure or hepatic cirrhosis. Typical fluid analysis results include:
- Physical characteristics—fluid generally appears clear or straw-colored
- Protein—less than 3 g/dL
- Albumin level—low (typically evaluated as the difference between serum albumin and peritoneal fluid albumin, termed serum-ascites albumin gradient (SAAG); values above 1.1 g/dL are considered evidence of a transudate.)
- Lactate dehydrogenase (LD) fluid/serum ratio—less than 0.6
- Glucose—equal to glucose level in the blood
- Cell count—few cells are present, usually lymphocytes
- Specific gravity—less than 1.015
Exudate
- Physical characteristics—fluid may appear cloudy
- Protein—greater than 3 g/dL
- Albumin level—higher than in transudates (typically with a serum-ascites albumin gradient (SAAG) less than 1.1 g/dL)
- Lactate dehydrogenase (LD) fluid/serum ratio—greater than 0.6
- Glucose—less than 60 mg/dL
- Cell count—increased
- Specific gravity—greater than 1.015
Exudates can be caused by a variety of conditions and diseases and usually require further testing to aid in the diagnosis. Infections, trauma, various cancers, or pancreatitis may cause exudates. The following is a list of additional tests that a healthcare practitioner may order depending on the suspected cause and typical results.
Physical characteristics – the normal appearance of a peritoneal fluid sample is usually straw-colored and clear. Abnormal appearances may give clues to conditions or diseases present and may include:
- Yellow with liver disease, milky from obstruction of the lymphatic system, and greenish from bile
- Reddish peritoneal fluid may indicate the presence of blood, most often due to trauma.
- Cloudy peritoneal fluid may indicate the presence of microbes and/or white blood cells (WBCs), pointing to an infection. It may also indicate lymph system blockage or trauma.
Chemical tests – tests that may be performed in addition to albumin may include:
- Glucose—typically about the same as blood glucose levels; may be lower with infection
- Amylase—increased with pancreatitis
- Tumor markers—to identify type of malignancy
Microscopic examination – may be performed if infection or cancer is suspected; normal peritoneal fluid has small numbers of white blood cells but no red blood cells (RBCs) or microbes. Results of an evaluation of the different kinds of cells present may include:
- Total cell counts—white blood cells and red blood cells in the sample are enumerated. Increased white blood cells may be seen with infections and malignant conditions.
- White blood cell differential—determination of percentages of different types of white blood cells; an increased number of neutrophils may be seen with bacterial infections.
- Cytology—a special centrifuge (cytocentrifuge) concentrates a small sample of cells that is then treated with a special stain to be examined under a microscope for abnormal cells and for white blood cell differentiation. The differential can help determine whether the cells are the result of an infection or the presence of a tumor.
Infectious disease tests – tests may be performed to look for microbes if an infection is suspected.
- Gram stain—for direct observation of bacteria or fungi under a microscope; there should be no microbes present in peritoneal fluid.
- Bacterial culture and susceptibility testing—if bacteria are present, susceptibility testing can be performed to guide antimicrobial therapy. If there are no microbes present, it does not rule out an infection; they may be present in small numbers or their growth may be inhibited because of prior antibiotic therapy.
- Fungal tests—if a culture is positive, the fungus or fungi causing the infection will be identified in the report and susceptibility testing may be done to guide therapy.
- Adenosine deaminase—a markedly elevated level in peritoneal fluid in a person with symptoms that suggest tuberculosis means it is likely that person has a Mycobacterium tuberculosis infection in that region of the body. This is especially true when there is a high prevalence of tuberculosis in the geographic region where a person lives.
Other less common tests for infectious diseases may be performed to identify a virus, mycobacteria (such as the mycobacterium that causes tuberculosis), or a parasite as the cause of an infection and fluid accumulation.
Ascites possible complications
Ascites complications may include:
- Spontaneous bacterial peritonitis (a life-threatening infection of the ascites fluid)
- Hepatorenal syndrome (kidney failure)
- Weight loss and protein malnutrition
- Mental confusion, change in the level of alertness, or coma (hepatic encephalopathy)
- Bleeding from the upper or lower intestine
- Other complications of liver cirrhosis
Ascites cancer
Advanced cancer can sometimes make fluid build up in the abdomen (ascites).
Cancers that can cause ascites include:
- Ovarian cancer
- Breast cancer
- Bowel cancer
- Stomach cancer
- Pancreatic cancer
- Mesothelioma in the peritoneum
- Lung cancer
- Liver cancer
- Womb (uterine) cancer
Fluid can build up when:
- cancer cells irritate the lining of the abdomen and make it produce too much fluid
- lymph glands in the abdomen get blocked and can’t drain fluid properly
- cancer has spread to the liver and raises the pressure in nearby blood vessels, which forces fluid out
- the liver can’t make enough blood proteins so fluid leaks out of veins into the abdominal cavity
Malignant ascites treatment
Your doctor can put a small tube into the abdomen to drain off the fluid. This reduces the swelling and makes you feel more comfortable. It’s called abdominal paracentesis or an ascitic tap. Draining the fluid relieves symptoms in 9 out of 10 people (90%). You might have this treatment as an outpatient or you might need to stay in hospital for up to a few days.
The fluid sometimes builds up again after a while so your doctor might suggest that you have medicines to try to slow the build up. They may suggest that you have a long term drain.
You lie down on a bed and a nurse helps you get comfortable. Your doctor cleans the skin on your tummy and gives a local anaesthetic injection to numb the area. They make a small cut in your tummy and gently use a needle to put a small tube into the fluid. You might have an ultrasound scan at the same time. This helps them guide the tube into the right area.
Your doctor then attaches the tube to a drainage bag. They might make a couple of stitches in the skin to hold it in place. You have a dressing over the tube which also helps to keep it in position.
You might only need to have the tube in for a few hours. But if you have more than a couple of liters of fluid you might have it in for a few days.
Possible problems of short term drain
- Low blood pressure – Your blood pressure may drop and make you feel ill if the fluid drains too quickly. Your nurses will check your blood pressure and pulse regularly.
- Pain and discomfort – Your nurse can give you painkillers if you need them. They can also help you change your position to make you comfortable.
- Fluid in separate areas in the abdomen – Your doctor might need to put the tube in more than one place if the fluid is in different areas.
- Infection (peritonitis) – Infections aren’t common. If you get one, you have antibiotics as tablets or through a drip.
- Tube blockage – The tube might stop draining. Changing your position or sitting upright can sometimes get rid of the blockage. If not, your doctor might need to replace the tube.
- Fluid leak after taking the tube out – You have a dressing to absorb fluid. If there is a lot of fluid leaking from the drain site you may have a collection bag instead of a dressing. You might need to have stitches put in if the wound still leaks after a couple of days.
Long term drains
Your doctor might recommend a long term tube to drain the fluid. These tubes (catheters) stay in the abdomen for several months.
There are different types of long term tube. The most common type is a PleurX drain.
Putting the drain in
- You usually have this as an outpatient at the hospital or you might need to stay there overnight.
- Your doctor cleans your skin and injects a local anaesthetic to numb the area. They then make 2 small cuts in the skin of your abdomen and gently push the tube in. There is a cuff under the skin to keep the tube in place and prevent infections.
- Your doctor stitches the tube to your skin. Then they put a dressing over the part of the tube that lies outside your body.
Draining the fluid
- When fluid builds up, you or a nurse take the cap off the end of the tube. You attach a drainage bottle. This bottle has a vacuum that helps drain the fluid. It usually takes between 5 and 15 minutes.
- When the fluid stops draining you remove the bottle and put a cap over the end of the tube. You also put a clean dressing on.
Possible problems of using a tube to drain the ascites fluid
There are ways of dealing with problems that occur with a PleurX drain.
- Pain and discomfort: Your nurse can give you painkillers if you need them. They can also help you change your position to make you comfortable.
- Infection: You might get an infection in the cuts made to put in the tube, or in the abdomen. If you get an infection you have antibiotics. These might be as tablets or through a drip. If you get a severe infection, your doctor might take the tube out.
- Tube blockage: The tube might stop draining. Changing your position or sitting upright can sometimes get rid of the blockage. If not, your doctor might need to replace the tube.
Other ways of draining fluid
Long term drains are one way of draining the fluid. Other ways of draining it include short term tubes, medicines, or having a shunt – an internal tube. There are different types, including the Hyde shunt, LaVeen shunt and Denver shunt.
Shunts drain fluid from a swollen tummy (ascites) caused by some kinds of cancer.
Putting the shunt in
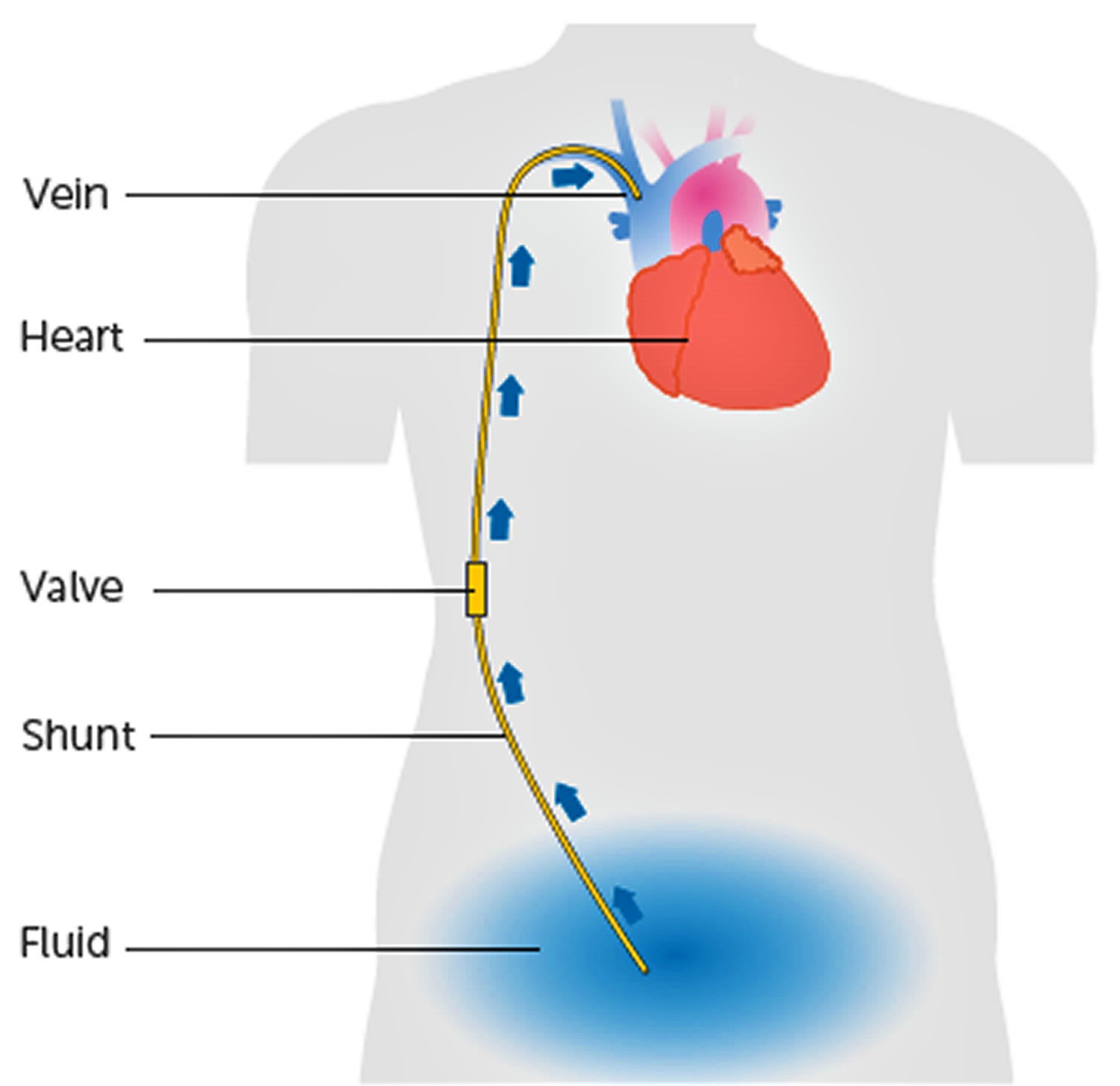
You need to be fairly fit to have this procedure. You have a medicine to make you drowsy (a sedative) or a general anaesthetic. Your doctor cleans the skin over one of the main veins in your neck. They inject a local anaesthetic to numb the area. They then gently pass a long needle down through the vein to widen it.
Your doctor then cleans and numbs the skin of the chest and makes a small cut. They put in a tube that has one end in the abdominal fluid and one end in the vein in the neck. A valve in the tube allows fluid to flow from the tummy into the vein in the neck.
Possible problems
- Pain and discomfort: Your nurse can give you painkillers to reduce any pain after you have the shunt put in. Tell them if you still have pain.
- Collapsed lung: There is a risk of making a hole in the lung while the doctor puts the tube in. If this happens they put a drain (tube) into the area around the lung for a few days.
- Infection: You might get an infection in the cuts made to put in the tube, or in the abdomen. If you get an infection you have antibiotics. These might be as tablets or through a drip. If you get a severe infection, your doctor might take the tube out.
- Tube blockage: The tube might stop draining. Changing your position or sitting upright can sometimes get rid of the blockage. If not, your doctor might need to replace the tube.
Figure 1. Shunt to drain malignant ascites
Ascites cirrhosis
Ascites is common in people with cirrhosis and it usually develops when the liver is starting to fail. In general, the development of ascites indicates advanced liver disease and patients should be referred for consideration of liver transplantation.
Cirrhosis of the liver is the most common cause of ascites but other conditions such as heart failure, kidney failure, infection or cancer can also cause ascites. Ascites is caused by a combination of elevated pressure in the veins running through the liver (portal hypertension) and a decrease in liver function caused by scarring of the liver, i.e., cirrhosis.
Liver ascites prognosis
In general, the development of ascites indicates evidence of advanced liver disease and patients should be referred for consideration of liver transplantation. The survival rate 5 years after ascites develops is only 30-40% and it is important that the patient and doctor discuss a referral to a liver specialist and a liver transplant center 1. More than half of these patients may not survive 2-3 years without liver transplantation.
Liver ascites symptoms
Most patients who develop ascites notice abdominal distension and rapid weight gain. Some people also develop swelling of ankles and shortness of breath from accumulation of fluid around the lungs. Additional symptoms or complication may occur and are listed below.
Abdominal pain, discomfort and difficulty breathing: These may occur when too much fluid accumulates in the abdominal cavity. This may limit the ability to eat, ambulate and perform activities of daily living.
Infection: This is called spontaneous bacterial peritonitis and it usually causes abdominal pain, tenderness, fever or nausea. If this is not promptly diagnosed or treated, a patient may develop kidney failure, severe infection in the blood stream or mental confusion. The diagnosis is generally made by taking a sample of the fluid from the abdominal cavity. This infection can be treated with intravenous antibiotics, and after recovery, patients will require long term treatment with antibiotics to prevent spontaneous bacterial peritonitis from recurring.
Ascites related hernias: Elevated intra-abdominal pressure can lead to the development of umbilical (around the bellybutton) and inguinal (groin) hernias that can cause abdominal discomfort. Surgical repair is generally avoided unless there is severe pain suggesting the intestines or tissue may be pinched or twisted along with a persistent bulge from the hernia. Surgeons who have experience in treating patients with cirrhosis should perform these operations.
Fluid accumulation in the chest: This is called hepatic hydrothorax and the abdominal fluid fills into the lung cavities (mostly on your right side) in addition to the abdominal cavity. This condition may result in shortness of breath with exertion or sometimes at rest also.
Liver ascites diagnosis
Depending on how much fluid is present in the abdomen, ascites may be diagnosed by the doctor on physical examination but is usually confirmed by tests such as ultrasound or CT scan of the abdomen. In the majority of patients, the doctor will recommend that a small needle be inserted through the abdominal wall (after local anesthesia) to remove fluid to be examined in the laboratory. This test is called a paracentesis. The fluid removed will be examined for signs of infection or cancer and to determine the cause for the fluid accumulation.
Ascites symptoms
The ascites fluid causes swelling that can make the tummy feel tight and very uncomfortable. It often develops over a few weeks but might happen over a few days.
The ascites fluid causes pressure on other organs in the abdominal area and may lead to:
- clothes feeling tighter or needing a bigger belt size
- bloating
- abdominal pain
- back pain
- difficulty sitting comfortably and moving around
- loss of appetite
- indigestion
- constipation
- needing to pass urine often
- breathlessness
- tiredness and weakness (fatigue)
Ascites treatment
The condition that causes ascites will be treated, if possible.
Treatments for ascites may include lifestyle changes:
- Avoiding alcohol
- Lowering salt in your diet (no more than 1,500 mg/day of sodium). The most important step to treat ascites is to strictly reduce your salt intake. Salt intake is limited to no more than 1,500 mg/day of sodium or less. As it can be difficult to determine the salt content of various foods, it is generally recommended that a patient with ascites see a nutritionist (dietician) for advice about various foods to avoid. Patients may use salt substitute but it is essential to choose one without potassium because the potassium levels can increase with certain medications to treat ascites. It is important to discuss with the doctor or the dietician which salt substitute may be safer to use.
- Limiting fluid intake. Checking body weight daily on a scale and contacting your physician whenever there is a gain of more than 10 pounds (or greater than 2 pounds per day for 3 consecutive days) is a good strategy for better management in patients with ascites.
You may also get medicines from your doctor, including:
- “Water pills” (diuretics) to get rid of extra fluid. Most often, patients will require water pills (diuretics) to treat ascites. Commonly used water pills are spironolactone (Aldactone) and/or furosemide (Lasix) and their dosages are appropriately adjusted. These water pills can cause problems with blood electrolytes (levels of sodium and potassium) and as such close monitoring by blood tests may be required. It is important to realize that taking water pills is not a substitute for reducing your salt intake, as water pills will work only when they are taken together with restricted salt intake.
- Antibiotics for infections.
Other things you can do to help take care of your liver disease are:
- Get vaccinated for diseases such as influenza, hepatitis A and hepatitis B, and pneumococcal pneumonia
- Talk to your doctor about all medicines you take, including herbs and supplements and over-the-counter medicines
When fluid accumulation cannot be treated optimally with water pills and salt restricted diet, patients may require a large amount of fluid be removed (paracentesis) for relief of symptoms. Other procedures such as having a radiologist place a shunt within the liver (called transjugular intrahepatic portosystemic shunt [TIPS]) to prevent significant fluid accumulation from ascites are available for patients who have difficult to treat ascites.
Procedures that you may have are:
- Inserting a needle into the belly to remove large volumes of fluid (called a large-volume paracentesis)
- Placing a special tube or shunt inside your liver [transjugular intrahepatic portosystemic shunt (TIPS)] to repair blood flow to the liver
People with end-stage liver disease may need a liver transplant. If you have cirrhosis, avoid taking nonsteroidal anti-inflammatory medicines, such as ibuprofen (Advil, Motrin) and naproxen (Aleve, Naprosyn).
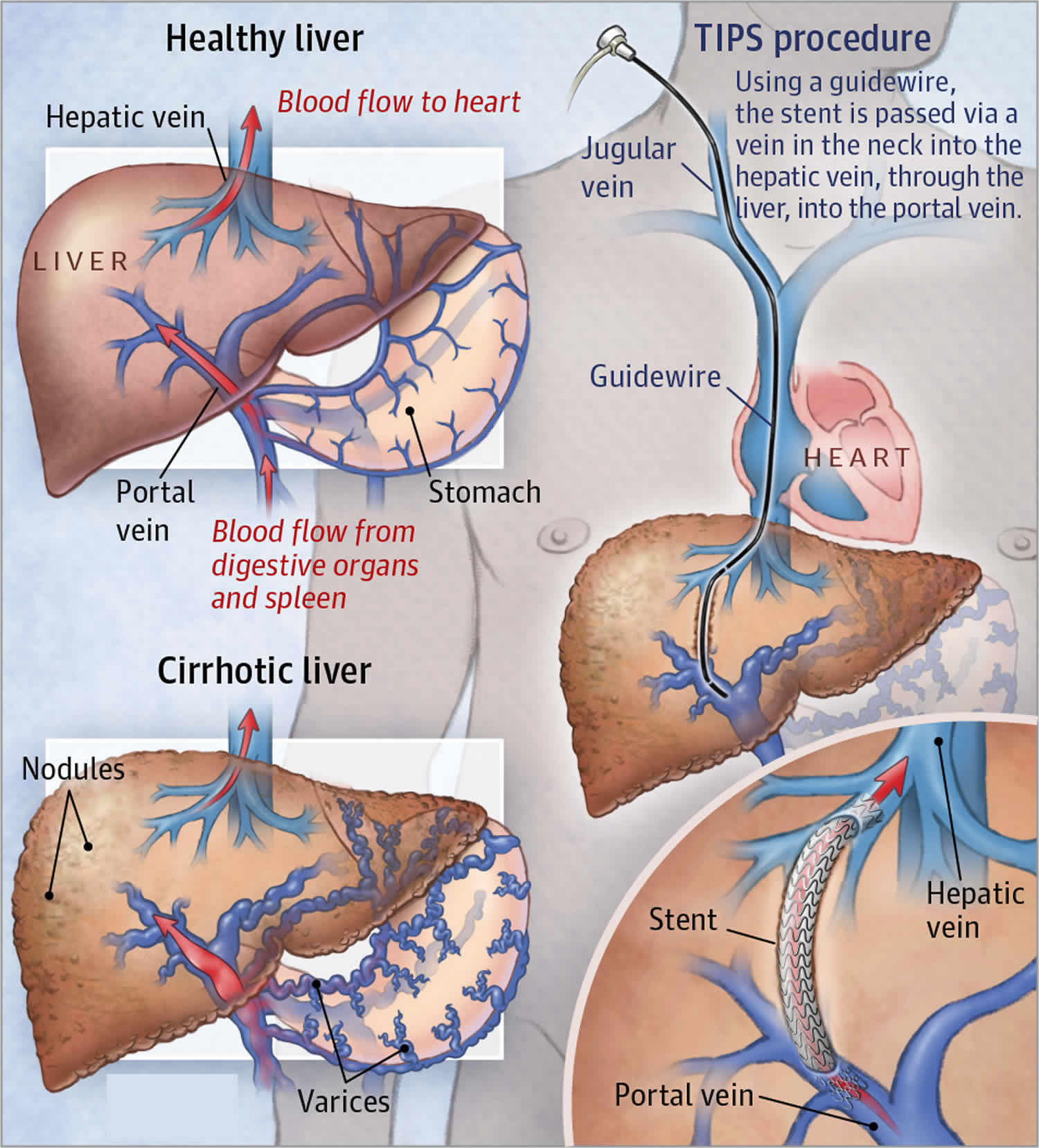
Figure 2. Transjugular intrahepatic portosystemic shunt (TIPS)
Sodium and fluid retention are frequent complications of end-stage liver disease and as a consequence, around 50% of patients with cirrhosis will develop ascites over a 10-year period of follow-up 3. Ascites significantly impairs the quality of life of patients with cirrhosis and is associated with poor prognosis: 1-year and 5-year survival rates of 85% and 56%, respectively are reported 4.
The first-line of management of liver ascites is restriction of dietary sodium by use of a ‘no added salt’ diet which contains <90 mmol/day (5.2 g of salt/day) and diuretic therapy, using spironolactone with or without added furosemide 5. These measures are effective in the majority of people with ascites secondary to cirrhosis. Refractory ascites develops in <10% of cases and is due to either inadequate urinary sodium excretion despite diuretics, or development of diuretic-induced complications that preclude the use of an effective dosage 6. Patients with large volume or refractory ascites may be treated by therapeutic paracentesis 7 accompanied by volume expansion using 20% human albumin solution, providing 6-8 g of albumin per liter of ascites drained 8, but this procedure generally needs to be repeated at regular intervals to maintain control of the fluid retention. Alternatively, transjugular intrahepatic portosystemic shunt (TIPS) has been advocated as a treatment in patients with refractory ascites needing frequent paracentesis (>3/month) who are not candidates for liver transplantation 9. However this procedure is complicated by the development of hepatic encephalopathy. Transjugular intrahepatic portosystemic shunt (TIPS) decrease the effective vascular resistance of the liver by the creation of a tract between the higher-pressure portal vein and the lower-pressure hepatic vein, decreasing the portal venous pressure. This in turn lessens the congestive pressure in veins in the intestine reducing production of ascites. The tract is maintained by placement of a special mesh tube known as a stent. Early stents were bare metal but more recently polytetrafluoroethylene (PTFE)-coated grafts have been employed to improve patency 10.
It is generally perceived that both transjugular intrahepatic portosystemic shunt (TIPS) and large-volume paracentesis improve quality of life in patients with refractory ascites, but there is disagreement concerning the impact of transjugular intrahepatic portosystemic shunt (TIPS) on long-term survival.
Clinical evidence statements
Transjugular intrahepatic portosystemic shunt (TIPS) was considered to have a clinically important benefit over large-volume paracentesis for the following outcomes:
There was clinical benefit in favor of transjugular intrahepatic portosystemic shunt (TIPS) for the critical outcomes of re-accumulation of ascites and transplant-free survival (albeit Low quality evidence) 11 versus large-volume paracentesis (large-volume paracentesis) for ascites. Available from: https://www.ncbi.nlm.nih.gov/books/NBK385213)). Only 1 study reported the critical outcome of health-related quality of life using the SF-36 tool. The paper reported that there was an improvement in scores for both groups, but there was no significant difference between the two groups. In the study, the SF-36 score was broken down into physical and mental components but the scale for each was not reported. Therefore, the National Institute for Health and Care Excellence found it difficult to assess whether the difference between groups was of clinical importance 11 versus large-volume paracentesis (large-volume paracentesis) for ascites. Available from: https://www.ncbi.nlm.nih.gov/books/NBK385213)).
Although there was a lack of evidence for quality of life, the National Institute for Health and Care Excellence discussed the potential benefits of a successful transjugular intrahepatic portosystemic shunt (TIPS) procedure over repeated large-volume paracentesis. For large-volume paracentesis, patients are required to attend hospital regularly every few weeks. This procedure is not a cure for the refractory ascites. The National Institute for Health and Care Excellence discussed that avoiding repeated large-volume paracentesis is likely to improve quality of life in the majority of patients who are able to undergo the transjugular intrahepatic portosystemic shunt (TIPS) procedure. Given this, the National Institute for Health and Care Excellence felt able to make a ‘consider’ recommendation.
Evidence was available from 2 studies for the outcome of renal failure (Moderate quality) and spontaneous bacterial peritonitis (Low quality), with contradictory results in small numbers of patients. The National Institute for Health and Care Excellence, despite the Moderate quality, placed less weight on these results given the small number of reported outcomes.
When considering the evidence the National Institute for Health and Care Excellence noted that the data available were largely older studies and of Low quality. The National Institute for Health and Care Excellence felt that if an randomized clinical trial had been conducted now, patient selection (particularly screening for hepatic encephalopathy and cardiac dysfunction) would have been more stringent and may have shown more benefit for transjugular intrahepatic portosystemic shunt (TIPS). The National Institute for Health and Care Excellence also noted that technical failures affected the outcomes in the transjugular intrahepatic portosystemic shunt (TIPS) groups and modern radiological techniques and stent design may reduce the effect of these technical failures. For example, even the most recent study (2011) used uncovered stents which are more likely to stenose. In addition, older studies may have included patients with more severe liver disease, who would not be considered for transjugular intrahepatic portosystemic shunt (TIPS) now.
The National Institute for Health and Care Excellence discussed the benefits of transjugular intrahepatic portosystemic shunt (TIPS) in improving the nutritional status of patients with cirrhosis. Whilst the National Institute for Health and Care Excellence did not look for evidence about nutritional status following both procedures, anecdotally it was felt that, when transjugular intrahepatic portosystemic shunt (TIPS) was successful, it indirectly improved the person’s nutritional status. The National Institute for Health and Care Excellence noted the suggestion of some benefit of transjugular intrahepatic portosystemic shunt (TIPS) for health-related quality of life, although this was not clinically significant.
The National Institute for Health and Care Excellence noted that in patients with hepatic encephalopathy there was a clinical benefit of large-volume paracentesis over transjugular intrahepatic portosystemic shunt (TIPS) 11 versus large-volume paracentesis (large-volume paracentesis) for ascites. Available from: https://www.ncbi.nlm.nih.gov/books/NBK385213)). Hepatic encephalopathy can become disabling and require reversal of the transjugular intrahepatic portosystemic shunt (TIPS) procedure by blockage of the stent 11 versus large-volume paracentesis (large-volume paracentesis) for ascites. Available from: https://www.ncbi.nlm.nih.gov/books/NBK385213)). The National Institute for Health and Care Excellence noted that the transjugular intrahepatic portosystemic shunt (TIPS) procedure is unsuitable for people with a past or current history of hepatic encephalopathy 11 versus large-volume paracentesis (large-volume paracentesis) for ascites. Available from: https://www.ncbi.nlm.nih.gov/books/NBK385213)).
Recommendation
Consider a transjugular intrahepatic portosystemic shunt (TIPS) for people with cirrhosis who have refractory ascites. The National Institute for Health and Care Excellence emphasised that all patients with cirrhosis and refractory ascites should be reviewed by a hepatologist and considered for liver transplantation. Those who are suitable for liver transplantation may undergo transjugular intrahepatic portosystemic shunt (TIPS) as a ‘holding procedure’ while on the liver transplant waiting list. Those who are not suitable for liver transplantation would undergo transjugular intrahepatic portosystemic shunt (TIPS) as a definitive procedure 11 versus large-volume paracentesis (large-volume paracentesis) for ascites. Available from: https://www.ncbi.nlm.nih.gov/books/NBK385213)).
How is transjugular intrahepatic portosystemic shunt performed?
A transjugular intrahepatic portosystemic shunt (TIPS) procedure is performed by an interventional radiologist. A catheter (small flexible tube) is inserted into a large vein in the neck that leads to the hepatic veins. From there, the portal vein is found and a stent (metal tube) is placed to create a large channel. This allows for brisk blood flow through the liver. Afterward, pressures are measured across the liver to ensure that portal hypertension has improved. This procedure requires an overnight hospitalization to monitor for complications.
Transjugular intrahepatic portosystemic shunt risks and complications
A transjugular intrahepatic portosystemic shunt (TIPS) procedure can place a large amount of stress on the heart and lungs because of the rapid increase in blood flow. Therefore, patients who undergo transjugular intrahepatic portosystemic shunt (TIPS) are first assessed for congestive heart failure (when the heart cannot pump blood properly) and pulmonary hypertension (elevated pressure in lung blood vessels). The transjugular intrahepatic portosystemic shunt (TIPS) procedure requires contrast, which can affect kidney function. Thus, kidney function is closely monitored before and after a transjugular intrahepatic portosystemic shunt (TIPS) procedure.
By shunting a fraction of blood flow from the portal vein to the hepatic vein, the transjugular intrahepatic portosystemic shunt (TIPS) procedure impairs some functions of the liver, such as the ability to filter natural poisons such as ammonia. The increased concentration of poisons can travel to the brain and cause hepatic encephalopathy (which causes confusion). Therefore, in people with advanced cirrhosis or history of recurrent confusion episodes, transjugular intrahepatic portosystemic shunt (TIPS) carries more risks. Treatment of this complication can include medications, narrowing the transjugular intrahepatic portosystemic shunt (TIPS), and liver transplantation in some cases.
The procedure itself has risks such as bleeding, infection, and, rarely, death. Additionally, the transjugular intrahepatic portosystemic shunt (TIPS) can become deformed or narrowed. Routine ultrasound imaging and clinical evaluation are performed to ensure good transjugular intrahepatic portosystemic shunt (TIPS) function.
- Ascites: A Common Problem in People with Cirrhosis. http://patients.gi.org/topics/ascites/[↩]
- Transjugular Intrahepatic Portosystemic Shunts. JAMA. 2017;317(8):880. doi:10.1001/jama.2016.20899 https://jamanetwork.com/journals/jama/fullarticle/2605801[↩]
- Gines P, Quintero E, Arroyo V, Teres J, Bruguera M, Rimola A, et al. Compensated cirrhosis: natural history and prognostic factors. Hepatology. 1987;7(1):122–128.[↩]
- Planas R, Montoliu S, Balleste B, Rivera M, Miquel M, Masnou H, et al. Natural history of patients hospitalized for management of cirrhotic ascites. Clinical Gastroenterology and Hepatology. 2006;4(11):1385–1394.[↩]
- National Guideline Centre (UK). Cirrhosis in Over 16s: Assessment and Management. London: National Institute for Health and Care Excellence (UK); 2016 Jul. (NICE Guideline, No. 50.) 12, Transjugular intrahepatic portosystemic shunt (TIPS) versus large-volume paracentesis (LVP) for ascites. Available from: https://www.ncbi.nlm.nih.gov/books/NBK385213/[↩]
- Santos J, Planas R, Pardo A, Durandez R, Cabre E, Morillas R, et al. Spironolactone alone or in combination with furosemide in the treatment of moderate ascites in nonazotemic cirrhosis. A randomized comparative study of efficacy and safety. Journal of Hepatology. 2003;39(2):187–192.[↩]
- Gines P, Arroyo V, Quintero E, Planas R, Bory F, Cabrera J, et al. Comparison of paracentesis and diuretics in the treatment of cirrhotics with tense ascites. Results of a randomized study. Gastroenterology. 1987;93(2):234–241.[↩]
- Runyon BA. Introduction to the revised American Association for the Study of Liver Diseases Practice Guideline management of adult patients with ascites due to cirrhosis 2012. Hepatology. 2013;57(4):1651–1653[↩]
- D’Amico G, Luca A, Morabito A, Miraglia R, D’Amico M. Uncovered transjugular intrahepatic portosystemic shunt for refractory ascites: a meta-analysis. Gastroenterology. 2005;129(4):1282–1293.[↩]
- Yang Z, Han G, Wu Q, Ye X, Jin Z, Yin Z, et al. Patency and clinical outcomes of transjugular intrahepatic portosystemic shunt with polytetrafluoroethylene-covered stents versus bare sents: a meta-analysis. Journal of Gastroenterology and Hepatology. 2010;25(11):1718–1725.[↩]
- National Guideline Centre (UK). Cirrhosis in Over 16s: Assessment and Management. London: National Institute for Health and Care Excellence (UK); 2016 Jul. (NICE Guideline, No. 50.) 12, Transjugular intrahepatic portosystemic shunt (transjugular intrahepatic portosystemic shunt (TIPS[↩][↩][↩][↩][↩][↩]





{kind=link}