
What is barotrauma
Barotrauma means injury to your body because of changes in barometric (air) or water pressure. Barotrauma can cause sinus injury, ear injury, facial injury, tooth injury, gastrointestinal (GI) cramping, pneumothorax, pulmonary hemorrhage, and subcutaneous emphysema 1. Sometimes pulmonary barotrauma is a precursor to arterial gas embolism. The most commonly affected sites are the middle ear and sinuses. One common barotrauma type happens to your ear is called ear barotrauma or middle ear barotrauma. A change in altitude may cause your ears to hurt. This can happen if you are flying in an airplane, driving in the mountains, or scuba diving. Divers can also get decompression sickness, which affects the whole body.
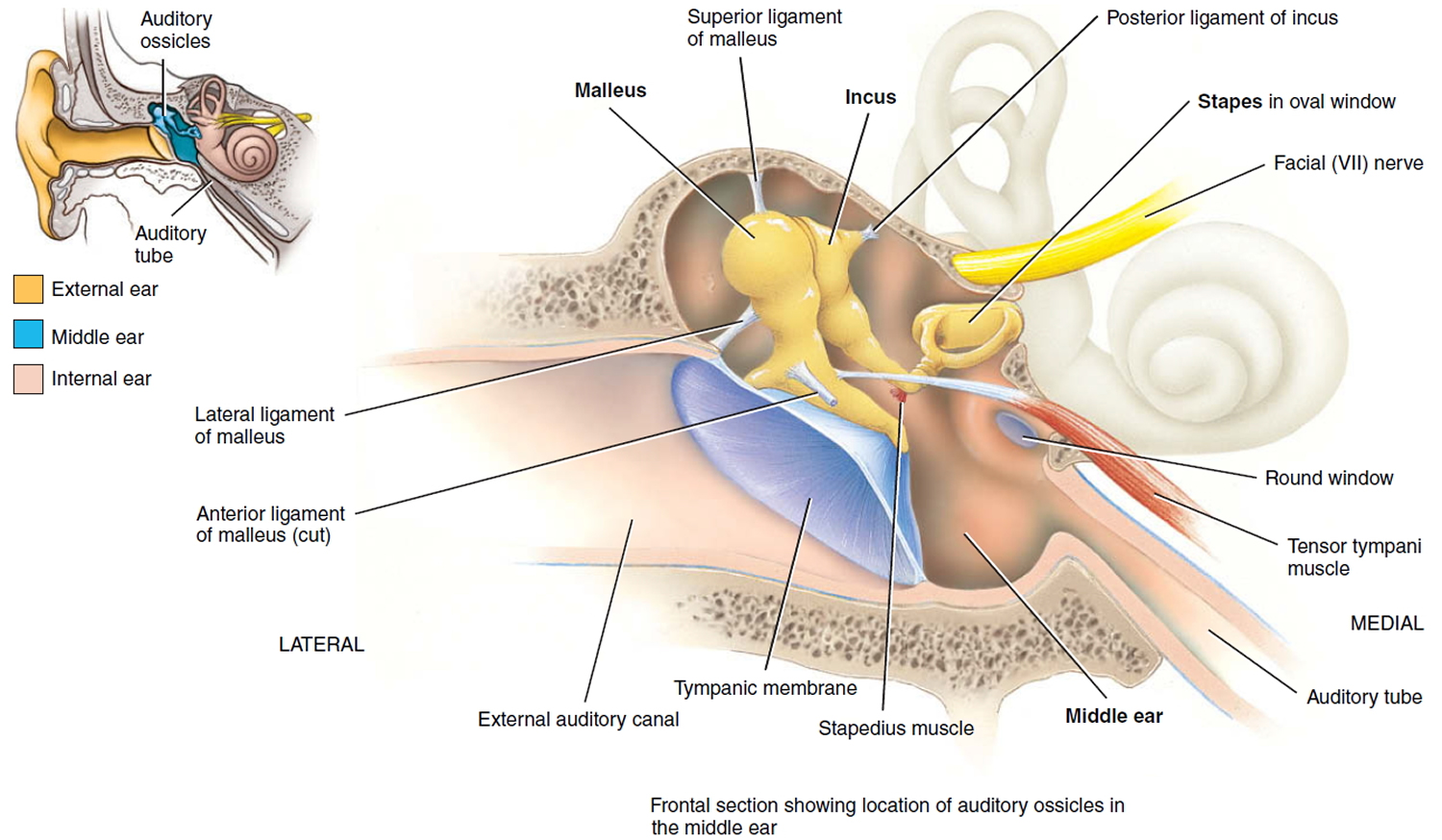
Ear barotrauma or middle ear barotrauma occurs when an imbalance in the air pressure in the middle ear and air pressure in the environment prevents your eardrum (tympanic membrane) from vibrating as it should. Air pressure regulation is the work of a narrow passage called the eustachian tube (auditory tube). One end is connected to the middle ear. The other end has a tiny opening where the back of the nasal cavity and the top of the throat meet (nasopharynx) (see Figures 2 and 3 below).
When an airplane climbs or descends, the air pressure in the environment changes rapidly, and your eustachian tube (auditory tube) often doesn’t react quickly enough. Swallowing or yawning activates muscles that open the eustachian tube and allow the middle ear to replenish its air supply, often eliminating the symptoms of airplane ear.
Ear barotrauma also may be caused by:
- Scuba diving
- Hyperbaric oxygen therapy chambers
- Explosions nearby
You may also experience a minor case of barotrauma while riding an elevator in a tall building or driving in the mountains.
Common barotrauma symptoms include:
- Dizziness
- Moderate ear discomfort or pain in one or both ears
- Hearing loss (slight) — muffled hearing or slight to moderate hearing loss
- Sensation of fullness or stuffiness in your ear
Other barotrauma symptoms may develop if the condition is very bad or goes on for a long time, such as:
- Severe ear pain
- Feeling of pressure in your ear similar to being underwater
- Moderate to severe hearing loss
- Ringing in your ear (tinnitus)
- Spinning sensation (vertigo)
- Vomiting resulting from vertigo
- Bleeding from your ear
- Nosebleed
Treatments for ear barotrauma include chewing gum and yawning to relieve the pressure. Medications such as decongestants may also help. If your ear discomfort, fullness or muffled hearing lasts more than a few hours or if you experience any severe signs or symptoms, see your doctor.
Barotrauma usually isn’t serious and responds to self-care. Long-term complications may occur when the condition is serious or prolonged or if there’s damage to middle or inner ear structures.
Rare ear barotrauma complications may include:
- Permanent hearing loss
- Ongoing (chronic) tinnitus
See your doctor if you have barotrauma and new symptoms develop, especially:
- If the discomfort does not ease after a few hours
- Drainage or bleeding from the ear
- Fever
- Severe ear pain
Figure 1. Ear structure
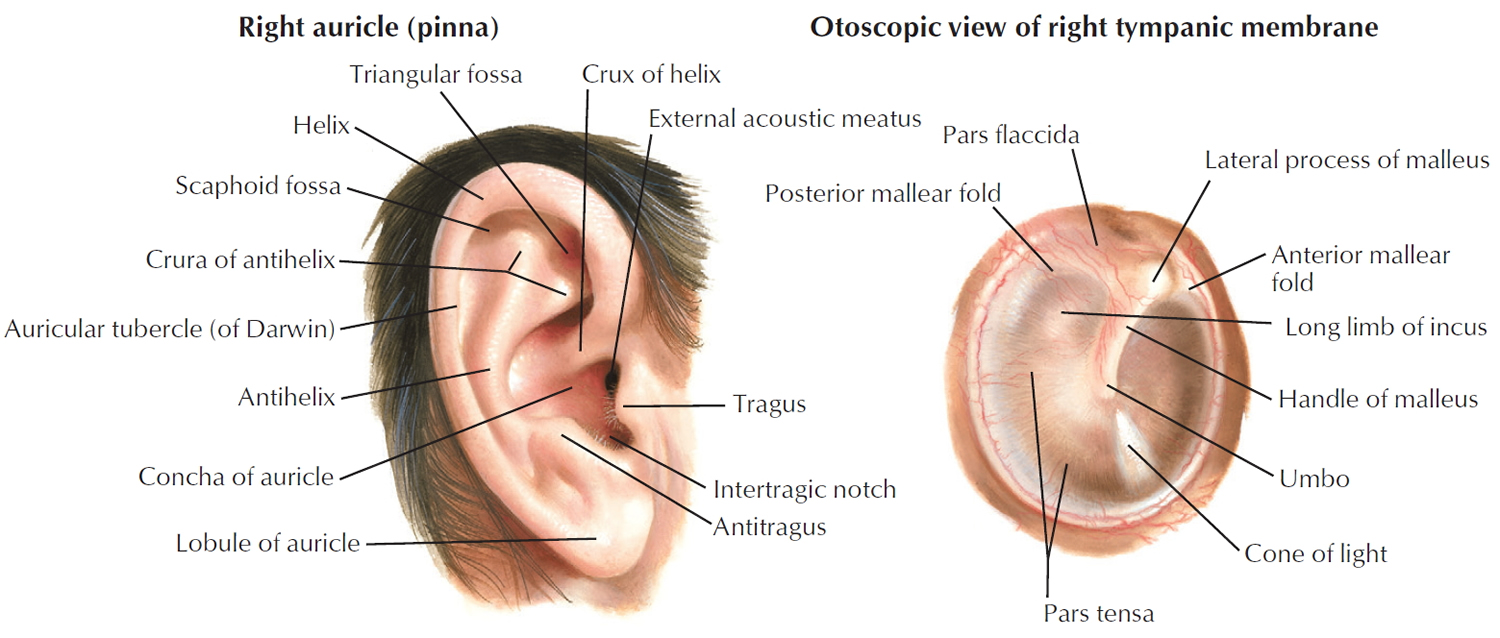
Figure 2. Ear anatomy

Figure 3. Middle ear and auditory ossicles
Ear barotrauma
Ear barotrauma or middle ear barotrauma, is discomfort in your middle ear due to pressure differences between the inside and outside of the eardrum (the middle ear) (Figures 2 and 3). Ear barotrauma may include damage to the ear. Middle ear barotrauma is most often caused by air pressure changes associated with air travel. Barotrauma is usually benign and responds to self-care. Hearing loss is almost always temporary.
Middle ear barotrauma is stress exerted on your eardrum when the air pressure in your middle ear and the air pressure in the environment are out of balance. If the pressure is severe, your eardrum can rupture. A ruptured eardrum or tympanic membrane perforation as it’s medically known — is a hole or tear in the thin tissue that separates your ear canal from your middle ear (eardrum) (see Figures 1 to 3). A ruptured eardrum can result in hearing loss. A ruptured eardrum can also make your middle ear vulnerable to infections or injury.
Signs and symptoms of a ruptured eardrum may include:
- Ear pain that may subside quickly
- Clear, pus-filled or bloody drainage from your ear
- Hearing loss
- Ringing in your ear (tinnitus)
- Spinning sensation (vertigo)
- Nausea or vomiting that can result from vertigo
A ruptured eardrum usually heals within a few weeks without treatment. In some cases, healing takes months. Sometimes, however, a ruptured eardrum requires a procedure or surgical repair to heal.
Other events that can cause sudden changes in pressure — and possibly a ruptured eardrum — include scuba diving and a direct blow to the ear, such as the impact of an automobile air bag.
Ear barotrauma how long does it last?
It depends. If you simply experienced changes in air pressure in your middle ear and the air pressure in the environment like in air travel, that problem should resolve once the pressure difference equalizes. However, if you ruptured you eardrum, you need to see your doctor if you experience any of the signs or symptoms of a ruptured eardrum or pain or discomfort in your ears. Your middle and inner ears are composed of delicate mechanisms that are sensitive to injury or disease. Prompt and appropriate treatment is important to preserve your hearing. Most ruptured eardrums heal without treatment within a few weeks. In some cases, healing takes months.
Signs and symptoms of a ruptured eardrum may include:
- Ear pain that may subside quickly
- Clear, pus-filled or bloody drainage from your ear
- Hearing loss
- Ringing in your ear (tinnitus)
- Spinning sensation (vertigo)
- Nausea or vomiting that can result from vertigo
Your eardrum (tympanic membrane) has two primary roles:
- Hearing. When sound waves strike it, your eardrum vibrates — the first step by which structures of your middle and inner ears translate sound waves into nerve impulses.
- Protection. Your eardrum also acts as a barrier, protecting your middle ear from water, bacteria and other foreign substances.
If your eardrum ruptures, complications can occur while your eardrum is healing or if it fails to heal.
Possible complications of ruptured eardrum include:
- Hearing loss. Usually, hearing loss is temporary, lasting only until the tear or hole in your eardrum has healed. The size and location of the tear can affect the degree of hearing loss.
- Middle ear infection (otitis media). A perforated eardrum can allow bacteria to enter your ear. If a perforated eardrum doesn’t heal or isn’t repaired, you may be vulnerable to ongoing (chronic) infections that can cause permanent hearing loss.
- Middle ear cyst (cholesteatoma). A cholesteatoma is a cyst in your middle ear composed of skin cells and other debris. Ear canal debris normally travels to your outer ear with the help of ear-protecting earwax. If your eardrum is ruptured, the skin debris can pass into your middle ear and form a cyst. A cholesteatoma provides a friendly environment for bacteria and contains proteins that can damage bones of your middle ear.
Ruptured eardrum treatment
Your doctor may prescribe antibiotic drops if there’s evidence of infection. If the tear or hole in your eardrum doesn’t heal by itself, treatment will involve procedures to close the perforation. These may include:
- Eardrum patch. If the tear or hole in your eardrum doesn’t close on its own, an ENT specialist may seal it with a patch. With this office procedure, your ENT doctor may apply a chemical to the edges of the tear to stimulate growth and then apply a patch over the hole. The procedure may need to be repeated more than once before the hole closes.
- Surgery. If a patch doesn’t result in proper healing or your ENT doctor determines that the tear isn’t likely to heal with a patch, he or she may recommend surgery. The most common surgical procedure is called tympanoplasty. Your surgeon grafts a tiny patch of your own tissue to close the hole in the eardrum. This procedure is done on an outpatient basis, meaning you can usually go home the same day unless medical anesthesia conditions require a longer hospital stay.
A ruptured eardrum usually heals on its own within weeks. In some cases, healing takes months. Until your doctor tells you that your ear is healed, protect it by doing the following:
- Keep your ear dry. Place a waterproof silicone earplug or cotton ball coated with petroleum jelly in your ear when showering or bathing.
- Refrain from cleaning your ears. Give your eardrum time to heal completely.
- Avoid blowing your nose. The pressure created when blowing your nose can damage your healing eardrum.
Ear barotrauma causes
The air pressure in your middle ear is most often the same as the air pressure outside of your body. The Eustachian tube is a connection between the middle ear and the back of the nose and upper throat (see Figures 2 and 3 – it’s called “auditory tube”).
Swallowing or yawning opens the Eustachian tube and allows air to flow into or out of the middle ear. This helps equalize pressure on either side of the ear drum. If the Eustachian tube is blocked, the air pressure in the middle ear is different than the pressure on the outside of the eardrum. This can cause barotrauma.
Many people have barotrauma at some time. The problem often occurs with altitude changes, such as flying, scuba diving, or driving in the mountains. If you have a congested nose from allergies, colds, or an upper respiratory infection, you are more likely to develop barotrauma.
Blockage of the Eustachian tube (auditory tube) could also be present before birth (congenital). It may also be caused by swelling in the throat.
Risk factors for ear barotrauma
Any condition that blocks the eustachian tube or limits its function can increase the risk of barotrauma. Common risk factors include:
- A small eustachian tube, especially in infants and toddlers
- The common cold
- Sinus infection
- Hay fever (allergic rhinitis)
- Middle ear infection (otitis media)
- Sleeping on an airplane during ascent and descent
Frequent or severe airplane ear may damage the tissues of the inner ear or eustachian tube, which increases your chances of experiencing the problem again.
Ear barotrauma prevention
To relieve ear pain or discomfort, you can take steps to open the Eustachian tube and relieve the pressure, such as:
- Chew gum
- Inhale, and then gently exhale while holding the nostrils closed and the mouth shut
- Use the Valsalva maneuver — gently blowing, as if blowing your nose, while pinching your nostrils and keeping your mouth closed.
- Suck on candy
- Yawn
When flying, DO NOT sleep as the plane prepares to land. Repeat the listed steps to open the Eustachian tube. For infants and small children, nursing or taking sips of a drink may help.
Scuba divers should go down and come up slowly. Diving while you have allergies or a respiratory infection is dangerous. Barotrauma may be severe in these situations.
Follow these tips to avoid a ruptured or perforated eardrum:
- Get treatment for middle ear infections. Be aware of the signs and symptoms of middle ear infection, including earache, fever, nasal congestion and reduced hearing. Children with a middle ear infection often rub or pull on their ears. Seek prompt evaluation from your primary care doctor to prevent potential damage to the eardrum.
- Yawn and swallow during ascent and descent. Yawning and swallowing activate the muscles that open your eustachian tubes. You can suck on candy or chew gum to help you swallow.
- Use the Valsalva maneuver during ascent and descent. Gently blow, as if blowing your nose, while pinching your nostrils and keeping your mouth closed. Repeat several times, especially during descent, to equalize the pressure between your ears and the airplane cabin.
- Don’t sleep during takeoffs and landings. If you’re awake during ascents and descents, you can do the necessary self-care techniques when you feel pressure on your ears.
- Reconsider travel plans. If possible, don’t fly when you have a cold, sinus infection, nasal congestion or ear infection. If you’ve recently had ear surgery, talk to your doctor about when it’s safe to travel.
- Use filtered earplugs. These earplugs slowly equalize the pressure against your eardrum during ascents and descents. You can purchase these at drugstores, airport gift shops or your local hearing clinic.
- Use an over-the-counter decongestant nasal spray. If you have nasal congestion, use a nasal decongestant about 30 minutes to an hour before takeoff and landing. Avoid overuse, however, because nasal decongestants taken over several days can increase congestion.
- Use oral decongestant pills cautiously. Oral decongestants may be helpful if taken 30 minutes to an hour before an airplane flight. However, if you have heart disease, a heart rhythm disorder or high blood pressure, or if you’ve experienced possible medication interactions, avoid taking an oral decongestant unless your doctor approves. If you’re a man older than age 50, you may experience serious side effects after taking decongestants containing pseudoephedrine (Actifed, Sudafed) such as urinary retention, especially if you have an enlarged prostate. If you’re pregnant, talk to your doctor before taking oral decongestants.
- Take allergy medication. If you have allergies, take your medication about an hour before your flight.
If you’re prone to severe airplane ear and must fly often, your doctor may surgically place tubes in your eardrums to aid fluid drainage, ventilate your middle ear, and equalize the pressure between your outer ear and middle ear.
Helping children prevent ear barotrauma
These additional tips can help young children avoid ear barotrauma:
- Encourage swallowing. Give a baby or toddler a beverage during ascents and descents to encourage frequent swallowing. A pacifier also may help. Have the child sit up while drinking. Children older than age 4 can try chewing gum, drinking through a straw or blowing bubbles through a straw.
- Consider eardrops. Talk to your child’s doctor about prescribing your child eardrops that contain a pain reliever and numbing agent for the flight.
- Avoid decongestants. Decongestants aren’t recommended for young children.
Ear barotrauma symptoms
Common barotrauma symptoms include:
- Dizziness
- Moderate ear discomfort or pain in one or both ears
- Hearing loss (slight) — muffled hearing or slight to moderate hearing loss
- Sensation of fullness or stuffiness in your ear
Other barotrauma symptoms may develop if the condition is very bad or goes on for a long time, such as:
- Severe ear pain
- Feeling of pressure in your ear similar to being underwater
- Moderate to severe hearing loss
- Ringing in your ear (tinnitus)
- Spinning sensation (vertigo)
- Vomiting resulting from vertigo
- Bleeding from your ear
- Nosebleed
Ear barotrauma possible complications
Complications may include:
- Acute ear infection
- Hearing loss
- Ruptured or perforated eardrum
- Vertigo
Ear barotrauma diagnosis
Your doctor will likely be able to make a diagnosis based on questions he or she asks and an examination of your ear with a lighted instrument (otoscope). Signs of airplane ear might include a slight outward or inward bulging of your eardrum. If your condition is more severe, your doctor may see a tear in the eardrum or a pooling of blood or other fluids behind your eardrum.
If you’re experiencing a spinning sensation (vertigo), there may be damage to structures of your inner ear. Your doctor may suggest a hearing test (audiometry) to determine how well you detect sounds and whether the source of hearing problems is in the inner ear.
During an exam of the ear, your health care provider may see a slight outward bulge or inward pull of the eardrum. If the condition is severe, there may be blood or bruising behind the eardrum.
Severe barotrauma may look similar to an ear infection.
Ear barotrauma treatment
For most people, ear barotrauma usually heals with time.
To relieve ear pain or discomfort yourself, you can take these steps to open the Eustachian tube and relieve the pressure, such as:
- Chew gum
- Inhale, and then gently exhale while holding the nostrils closed and the mouth shut
- Use the Valsalva maneuver — To do this, you pinch your nostrils shut, close your mouth and gently force air into the back of your nose, as if you were blowing your nose. Once the medications (see below) have improved the function of the eustachian tubes, use of the Valsalva maneuver may force the tubes open.
- Suck on candy
- Yawn
When flying, DO NOT sleep as the plane prepares to land. Repeat the listed steps to open the Eustachian tube. For infants and small children, nursing or taking sips of a drink may help.
Scuba divers should go down and come up slowly. Diving while you have allergies or a respiratory infection is dangerous. Barotrauma may be severe in these situations.
If self-care steps do not ease discomfort within a few hours or the problem is severe, you may need to see your healthcare provider.
You may need medicine to relieve nasal congestion and allow the Eustachian tube to open. Your doctor may prescribe medications or direct you to take over-the-counter medications to control conditions that may prevent the eustachian tubes from functioning well. These drugs may include:
- Decongestants taken by mouth, or by a nose spray
- Steroids
- Oral antihistamines
To ease discomfort, you may want to take a nonsteroidal anti-inflammatory drug, such as ibuprofen (Advil, Motrin IB, others) or naproxen sodium (Aleve, others), or an analgesic pain reliever, such as acetaminophen (Tylenol, others).
You may need antibiotics to prevent an ear infection if barotrauma is severe.
Rarely, surgery may be needed if other treatments do not work to open the eustachian tube. In this procedure, a surgical cut is made in the eardrum (myringotomy) to allow pressure to become equal and fluid to drain.
Severe injuries, such as a ruptured eardrum or ruptured membranes of the inner ear, usually will heal on their own. However, in rare cases, surgery may be needed to repair them.
If you must change altitude often or you are prone to barotrauma, you may need to have surgery to place tubes in the ear drum. This is not an option for scuba diving.
Pulmonary barotrauma
Pulmonary barotrauma occurs most commonly while scuba diving, but also may occur during flying, mountain climbing, or skiing 1. About 500 to 1000 nonfatal dive injuries in the United States and Canada each year. Many of these are related to barotrauma 1. During scuba diving, pulmonary barotrauma may be caused by ascending or descending too rapidly or by breath holding. The squeezes are caused by the inability to equalize pressure on the descent. Types are mask, sinus, and ear. Mask squeeze can cause skin ecchymosis in the mask pattern, conjunctival hemorrhage, and rarely, orbital hemorrhage. Ear squeeze can occur in the ear canal or middle ear. Risk factors for barotrauma include asthma, chronic obstructive pulmonary disease (COPD), seizures, sinus and ear problems, syncope, panic disorders, vertigo, poor training, inexperience, and Eustachian tube dysfunction.
Any patient receiving mechanical ventilation is at risk for pulmonary barotrauma, but it is most commonly associated with acute respiratory distress syndrome (ARDS) 1. Historically, this was the most common complication of mechanical ventilation, but modern strategies have mitigated the incidence of ventilator-associated acute respiratory distress syndrome (ARDS) by limiting tidal volume (6 to 8 mL/kg) and plateau pressure to less than 30 to 50 cm 1. As an indicator of transalveolar pressure, which predicts alveolar distention, plateau pressure is the best predictor of risk, but there is no accepted safe pressure at which there is no risk. Aspiration of stomach contents and pre-existing diseases such as pneumonia and chronic lung disease also increase risk.
Pulmonary barotrauma causes
pulmonary barotraumas of descent are caused by a lack free exchange of gas in a closed space in contact with the diver. The resulting pressure difference between the tissues and the gas space and the unbalanced force due to this pressure difference causes deformation of the tissues resulting in cell rupture.
Pulmonary barotraumas of ascent are also caused by prevention of the free exchange of volume of the gas in a closed space. In this instance, pressure change causes a difference in tension of the adjacent tissues exceeding their tensile strength. Aside from rupture of tissues, the overpressure may cause gases to enter the tissues further down the circulatory system. This pulmonary barotrauma of ascent is also known as a pulmonary over-inflation syndrome (POIS), lung over-pressure injury (LOP), and burst lung. Consequent injuries may include pneumothorax, mediastinal, interstitial, or subcutaneous emphysema, and possibly arterial gas embolism, not usually all at the same time.
Breathing gas at depth during SCUBA causes the in gas in the lungs to be at a higher pressure than the atmospheric pressure. While a free diver can dive to 33 feet or 10 meters and safely go up without exhaling because the gas in the lungs had been inhaled at atmospheric pressure, a diver who inhales compressed gas from scuba at 10 meters and ascends without exhaling will rupture his lungs and have extensive pulmonary barotrauma. The lungs in the second scenario would contain twice the amount of gas at atmospheric pressure and therefore need to expand to twice the normal volume upon surfacing.
Descending diving injuries include the squeezes, specifically, ear or sinus squeeze which can result in middle ear pain, sinus pain, vertigo, and/or tinnitus. With ear squeeze, pressure does not equalize in middle ear through the Eustachian tube. This is common when diving with an upper respiratory tract infection (URTI) and may result in severe pain and eardrum rupture. Water can then enter the middle ear causing vertigo/incapacitation. If pressure does not equalize in frontal or maxillary sinus which is common when diving with upper respiratory tract infection, one may have severe pain.
Breath-holding causes lung trauma-pulmonary overpressure syndrome (POPS) during ascent. Compressed air in lungs expands, and lung tissue ruptures, resulting in pneumothorax, pneumomediastinum, subcutaneous emphysema, or pulmonary arterial gas embolism. This may occur with an ascent from shallow depths. Symptoms are usually present on surfacing or within 10 minutes.
Signs and symptoms include shortness of breath, crackles, crepitance, tachypnea, respiratory distress, substernal chest pain, and in the case of pneumothorax, diminished breath sounds.
Breath-holding can cause an arterial gas embolism during ascent leading to lung tissue tears, air entering pulmonary circulation, air entering the left heart, pumped to systemic circulation, and clogging of the cerebral circulation.
Pulmonary barotrauma diagnosis
History and physical is the most important key to making this pulmonary barotrauma diagnosis.
When taking the history of a diver, it is important to note the events preceding the dive, temperature, sea conditions, dive conditions, depth of dive, the onset of symptoms concerning the dive profile (on the descent, at the bottom, on ascent or after surfacing). Ask about chest pain, shortness of breath, hemoptysis, epistaxis, vertigo, nausea, vomiting or loss of consciousness. On physical exam check sinuses for anatomic obstructions or hemorrhage. Check tympanic membranes for fluid, hemorrhage or rupture.
A complete neurologic exam is indicated for anyone with pulmonary barotrauma to screen for signs of arterial gas embolism which could include numbness, weakness, paralysis, visual deficits, ataxia, aphasia, sensory loss, nystagmus, and confusion.
Laboratory studies are not very useful. Arterial blood gas may be of value to look for a-a gradient in those suspected of having an air embolism. Rising creatine phosphokinase levels may signal worsening tissue damage due to microemboli.
Perform radiographic studies as needed according to symptoms: chest x-ray, CT head. An echocardiogram may show gas bubbles in the heart in patients with arterial gas embolism.
Pulmonary barotrauma treatment
Treat supportively for mild injuries such as sinus squeeze, middle ear squeeze 1. Use NSAIDs, decongestants, or analgesics as needed. For tympanic membrane rupture, prescribe oral amoxicillin/clavulanate and fluoroquinolone ear drops. Otolaryngology referral is also warranted for tympanic membrane ruptures.
Most pulmonary barotrauma can be treated conservatively with rest and oxygen as needed. The exception is pneumothorax with often requires decompression (needle, pigtail, or chest tube) 1.
Pulmonary barotrauma prognosis
The prognosis for barotrauma is good, most of these conditions are self-limiting.





{kind=link}