
Contents
What are bed sores
Bed sores commonly called pressure ulcers, decubitus ulcers or pressure sores that are on your skin from prolonged pressure that cuts off the blood supply to the skin, causing the skin and other tissue to die. Bed sores are caused by being in a chair or bed for most of the day and night. The damage may occur in as little time as 12 hours of pressure, but it might not be noticed until days later when the skin begins to break down. Pressure sores usually develop over the bony parts of your body. Pressure sores occur in soft tissue that is compressed for prolonged periods of time between an external surface and a bony prominence. Bed sores are most common on the heels and on the hips. Other areas at risk include the base of the spine (tailbone), shoulder blades, the backs and sides of the knees, and the back of the head. Those are places with little padding from fat. The skin is especially likely to develop pressure sores if it is exposed to rubbing (friction) and moving the skin in one direction and the body in another (shear), as in sliding down when the bed head is raised. Dampness (such as from perspiration or incontinence) makes the skin even more liable to develop pressure sores. The pain level associated with bedsores depends on whether or not there is feeling in the area. A bedsore appears first as a reddened area of skin, which then starts to break down to form an open, raw, oozing wound.
Bed sores occur at areas of abnormal pressure on the body:
For people who use a wheelchair, pressure sores often occur on skin over the following sites:
- Tailbone (coccyx) or buttocks area
- Shoulder blades and spine
- Backs of arms and legs where they rest against the chair
For people who are confined to a bed, common sites include the following:
- Back or sides of the head (e.g., ears)
- Shoulder blades
- Hip, lower back or tailbone
- Heels, elbows, ankles, toes and skin behind the knees
You are more likely to get pressure sores if you are paralyzed, use a wheelchair, or spend most of your time in bed (such as in an assisted care facility). Risk factors for developing bed sores include older age, low body weight, black or Hispanic ethnicity, cognitive impairment, malnutrition, dehydration, immobility, moisture, venous insufficiency (lesions on the legs), sensory deficit, smoking, and fecal incontinence.
Even people who are able to walk can develop pressure sores when they must stay in bed because of an illness or an injury. Some chronic diseases make it difficult for pressure sores to heal. That’s because they affect your blood circulation. Examples of these diseases include diabetes and hardening of the arteries.
Who’s most at risk of getting pressure ulcers
Anyone can get a pressure ulcer, but the following things can make them more likely to form:
- People who cannot move themselves are at the greatest risk of getting bedsores, including people with:
- Spinal cord injury
- Paralysis
- Strokes
- Nerve (neurologic) disease
- Decreased mental awareness
- Being over 70 – older people are more likely to have mobility problems and have skin that’s more easily damaged through dehydration and other factors
- Being confined to bed with illness or after surgery
- Obesity
- Urinary incontinence and bowel incontinence
- A poor diet
- Medical conditions that affect blood supply, make skin more fragile or cause movement problems – such as diabetes, peripheral arterial disease, kidney failure, heart failure, multiple sclerosis (MS) and Parkinson’s disease
Most bedsores occur in older people (over the age of 70), as the skin of older people may be thinner and may heal more slowly.
People in nursing homes and hospitalized people (particularly for hip fracture or intensive care) develop bedsores more commonly.
Smokers and people who do not get good nutrition (malnourished or undernourished), have incontinence (problems with bladder or bowel control), diabetes, or problems with blood flow (circulation) also have increased risk.
For a sense of the total costs of the treatment of pressure ulcers, data from the 1990s, although old, can shed a light on current costs. In 1996, $6.4 billion was spent on pressure ulcers, which was 1.2% of total health care costs in the US 1. In 2006, excluding neonatal and maternal conditions, almost $11 billion was paid out for hospital stays in which pressure ulcer was either a primary or secondary diagnosis 2. For the individual patient, the current costs of providing care for one pressure ulcer can range from $3500 to over $60,000, depending on the stage of the ulcer 3.
Bed sores change appearance over 4 stages. In the beginning, bed sores look red. By stage 4 (the most serious), the sores are deep and open. You actually can see your muscle, bone, tendons, and joints.
Ways to stop pressure ulcers getting worse and help them heal include:
- applying special dressings that speed up the healing process and may help to relieve pressure
- moving and regularly changing your position
- using specially designed static foam mattresses or cushions, or dynamic mattresses and cushions that have a pump to provide a constant flow of air
- eating a healthy, balanced diet
- a procedure to clean the wound and remove damaged tissue (debridement)
Treatment options for pressure ulcers (sores) typically include regularly changing your position, using special mattresses to reduce or relieve pressure, and dressings to help heal the ulcer. In some cases, surgery may be needed. Surgery to remove damaged tissue and close the wound is sometimes used in the most serious cases.
When to see a doctor
If you notice warning signs of a bedsore, change your position to relieve the pressure on the area. If you don’t see improvement in 24 to 48 hours, contact your doctor.
Seek immediate medical care if you show signs of infection, such as a fever, drainage from a sore, a sore that smells bad, or increased redness, warmth or swelling around a sore.
Bed sores complications
Complications of pressure ulcers, some life-threatening, include:
- Cellulitis. Cellulitis is an infection of the skin and connected soft tissues. It can cause warmth, redness and swelling of the affected area. People with nerve damage often do not feel pain in the area affected by cellulitis.
- Bone and joint infections. An infection from a pressure sore can burrow into joints and bones. Joint infections (septic arthritis) can damage cartilage and tissue. Bone infections (osteomyelitis) can reduce the function of joints and limbs.
- Cancer. Long-term, nonhealing wounds (Marjolin’s ulcers) can develop into a type of squamous cell carcinoma
- Sepsis. Rarely, a skin ulcer leads to sepsis.
Pressure ulcers symptoms
Pressure ulcers can affect any part of the body that’s put under pressure. They’re most common on bony parts of the body, such as the heels, elbows, hips and base of the spine.
They often develop gradually, but can sometimes form in a few hours.
Early symptoms
Early symptoms of a pressure ulcer include:
- part of the skin becoming discolored – people with pale skin tend to get red patches, while people with dark skin tend to get purple or blue patches
- discolored patches not turning white when pressed
- a patch of skin that feels warm, spongy or hard
- pain or itchiness in the affected area
A doctor or nurse may call a pressure ulcer at this stage a category 1 pressure ulcer.
Later symptoms
The skin may not be broken at first, but if the pressure ulcer gets worse, it can form:
- an open wound or blister – a category two pressure ulcer
- a deep wound that reaches the deeper layers of the skin – a category three pressure ulcer
- a very deep wound that may reach the muscle and bone – a category four pressure ulcer
If you’re in hospital or a care home, tell your healthcare team as soon as possible if you develop symptoms of a pressure ulcer. It’ll probably continue to get worse if nothing is done about it.
You should be regularly monitored and offered advice and treatment to reduce the risk of pressure ulcers, but sometimes they can develop even with the highest standards of care.
If you’re recovering from illness or surgery at home, or are caring for someone confined to bed or a wheelchair, contact your GP surgery if you think you or the person you’re caring for might have a pressure ulcer.
Get medical advice immediately if there is:
- red, swollen skin
- pus coming from the pressure ulcer or wound
- cold skin and a fast heartbeat
- severe or worsening pain
- a high temperature (fever) of 38 °C (100.4 °F) or above
These symptoms could be a sign of a serious infection that needs to be treated as soon as possible.
Pressure ulcer staging
Ulcers that may have other causes, such as venous insufficiency, arterial occlusive disease, and diabetes mellitus, are not appropriate for the type of staging that is described here.
There are 4 stages of pressure sores. Symptoms look different at each stage.
The stage of a pressure ulcer depends on the depth of the ulcer. Figure 1 shows the various stages of pressure ulcers by layer of skin or subcutaneous tissue involvement 4. The total surface area that the ulcer encompasses is not the determining factor. For example, a stage 1 or 2 pressure ulcer may have a fairly large surface area, but a stage 3 or 4 may be of relatively smaller diameter but of greater depth. The development of pressure ulcers is a progressive process. If a patient has a lower-stage pressure ulcer and if preventive measures are not implemented to address the factors contributing to its development, then it will progress into a more complicated and severe ulcer.
Because staging is based on the depth of involvement, it is essential to be able to visualize the bottom of the ulcer. If the bottom of the ulcer is covered by thick eschar or adherent slough, then it cannot be staged and is referred to as unstageable. Only when the eschar is débrided and the base of the ulcer is fully visualized can the ulcer be accurately staged.
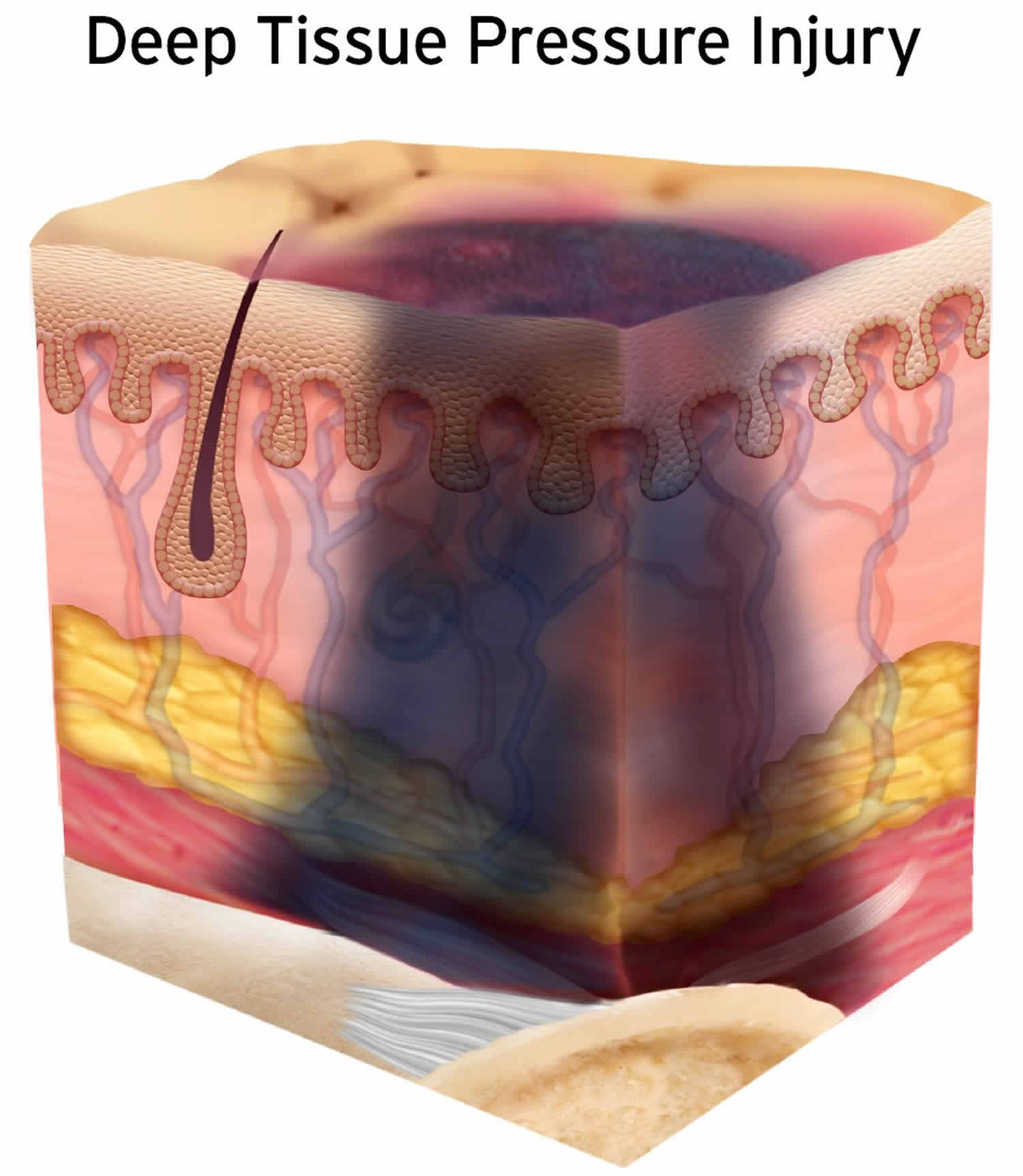
Another type of pressure ulcer that is difficult to stage is designated a deep tissue injury. The surface of the skin may appear to be like that of a stage 1 or 2 ulcer, as is shown in Figures 2 and 3, but the damage to underlying tissues is severe. Because the pressure forces are greatest at the interface between bone and surrounding soft tissue, tissues not visible may be severely compromised, even necrotic. Figure 2 shows how severe and how deep the damage can be to deep tissues 5. Areas of the skin with deep tissue injury can rapidly progress into deep stage 3 or 4 ulcers, appearing to seemingly materialize overnight. The clinician’s index of suspicion regarding these ulcers must be high. A patient with what appears to be a large stage 1 or 2 pressure ulcer who also has a low Braden score may very well have deep tissue injury. In Europe, deep tissue injury and unstageable pressure ulcers are classified as stage 4 6. Whatever classification is used, these patients should be treated as if they have a stage 3 or 4 pressure ulcer.
If your pressure sore becomes infected, it will take longer to heal. The infection can spread to the rest of your body. Signs of infection at the site include:
- Thick, yellow, or green pus.
- A bad smell coming from the sore.
- Redness or skin that is warm to the touch.
- Swelling around the sore.
- Tender to the touch around the sore.
Signs that the infection has spread include:
- Fever.
- Chills.
- Mental confusion or difficulty concentrating.
- Rapid heartbeat.
- Weakness.
Figure 1. Pressure ulcer staging
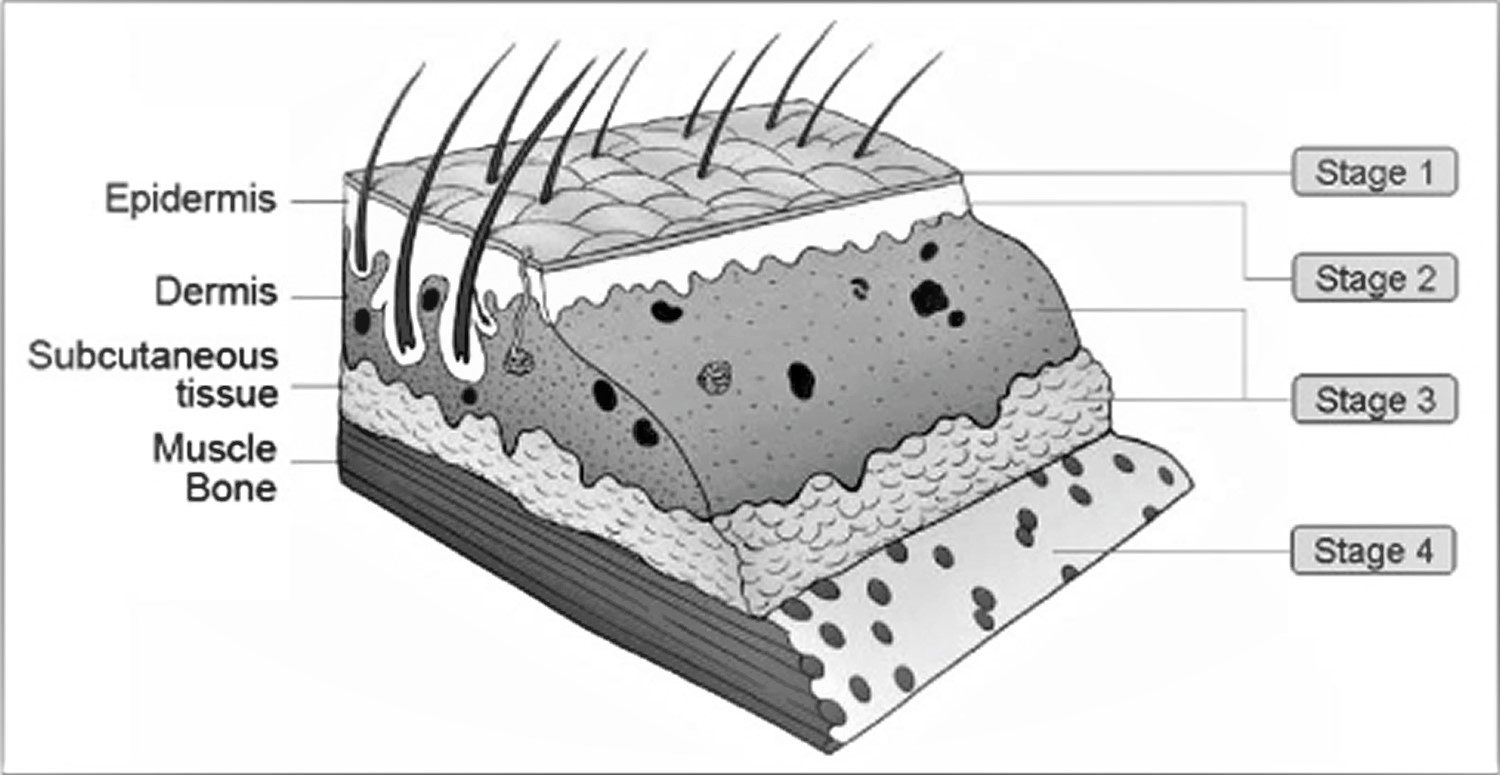
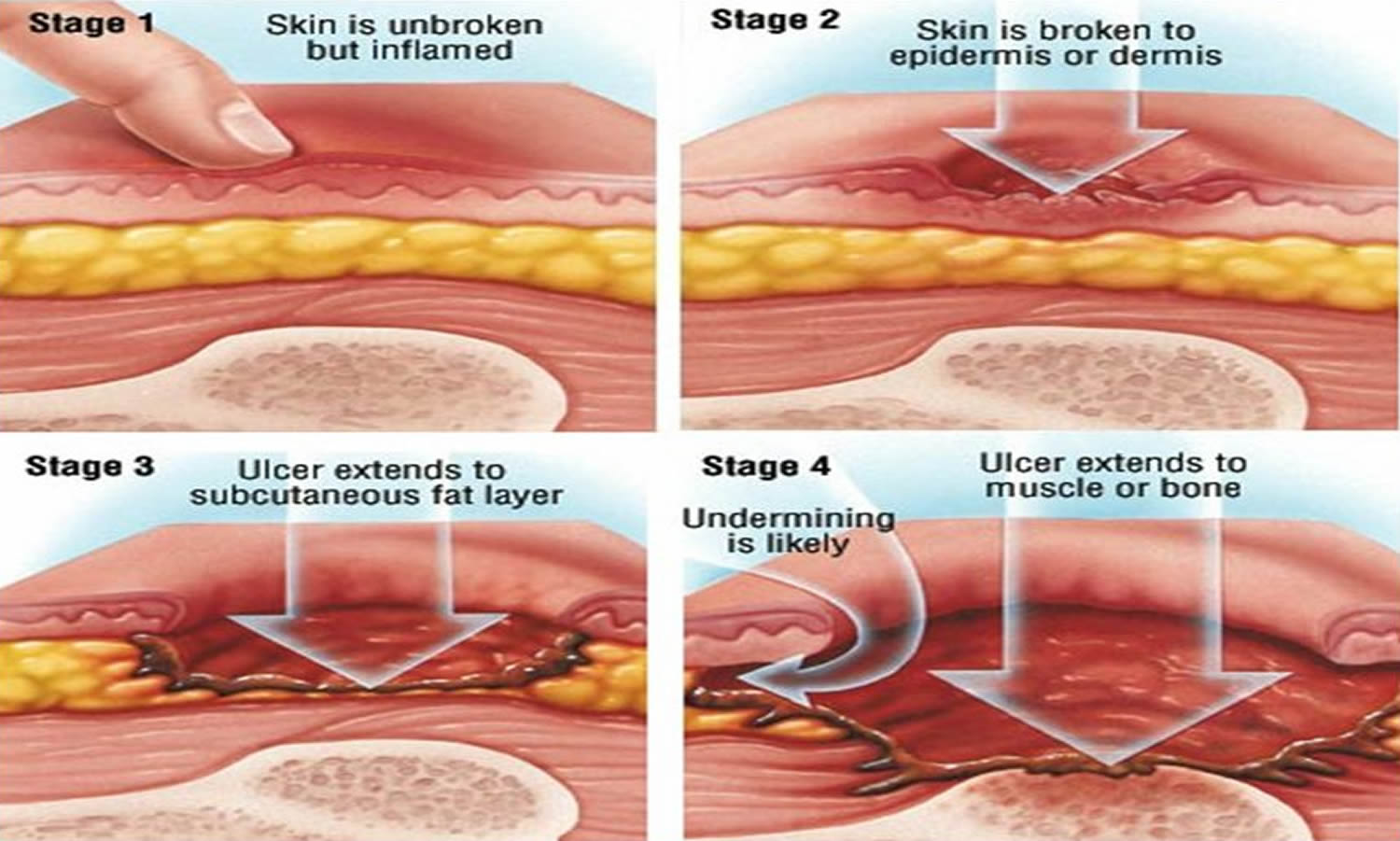
Figure 2. Deep tissue pressure injury

Stage 1 Pressure ulcer
In stage 1 pressure ulcers, there is a change in the color, consistency, or temperature of the skin, but the skin is intact and the underlying tissues are unaffected. The affected skin looks red and may feel warm to the touch. The area also may burn, hurt, or itch. In people who have dark skin, the pressure sore may have a blue or purple tint.
A stage 1 pressure ulcer is a warning sign that there is a problem. Interventions at this point can help prevent further, more problematic skin conditions.
Figure 3. Stage 1 pressure ulcer

Stage 2 Pressure ulcer
Stage 2 pressure ulcers involve the epidermal layer of skin and may extend into the dermis as well. The affected skin is more damaged usually appear as shallow, open ulcers or intact serum-filled or serosanguineous blisters. Stage 2 pressure ulcer can result in an open sore that looks like a cut or blister. The skin around the wound may be discolored. Stage 2 pressure ulcer is very painful.
Figure 3 depicts a typical example of a stage 2 pressure ulcer, with excoriation of the involved skin and extension into deeper tissues. When a patient develops a stage 2 pressure ulcer, it is common to have to contend with issues such as serous drainage that complicate skin care and can cause problems with adjacent areas of the skin that would not otherwise be affected.
Figure 4. Stage 2 pressure ulcer

Stage 3 Pressure ulcer
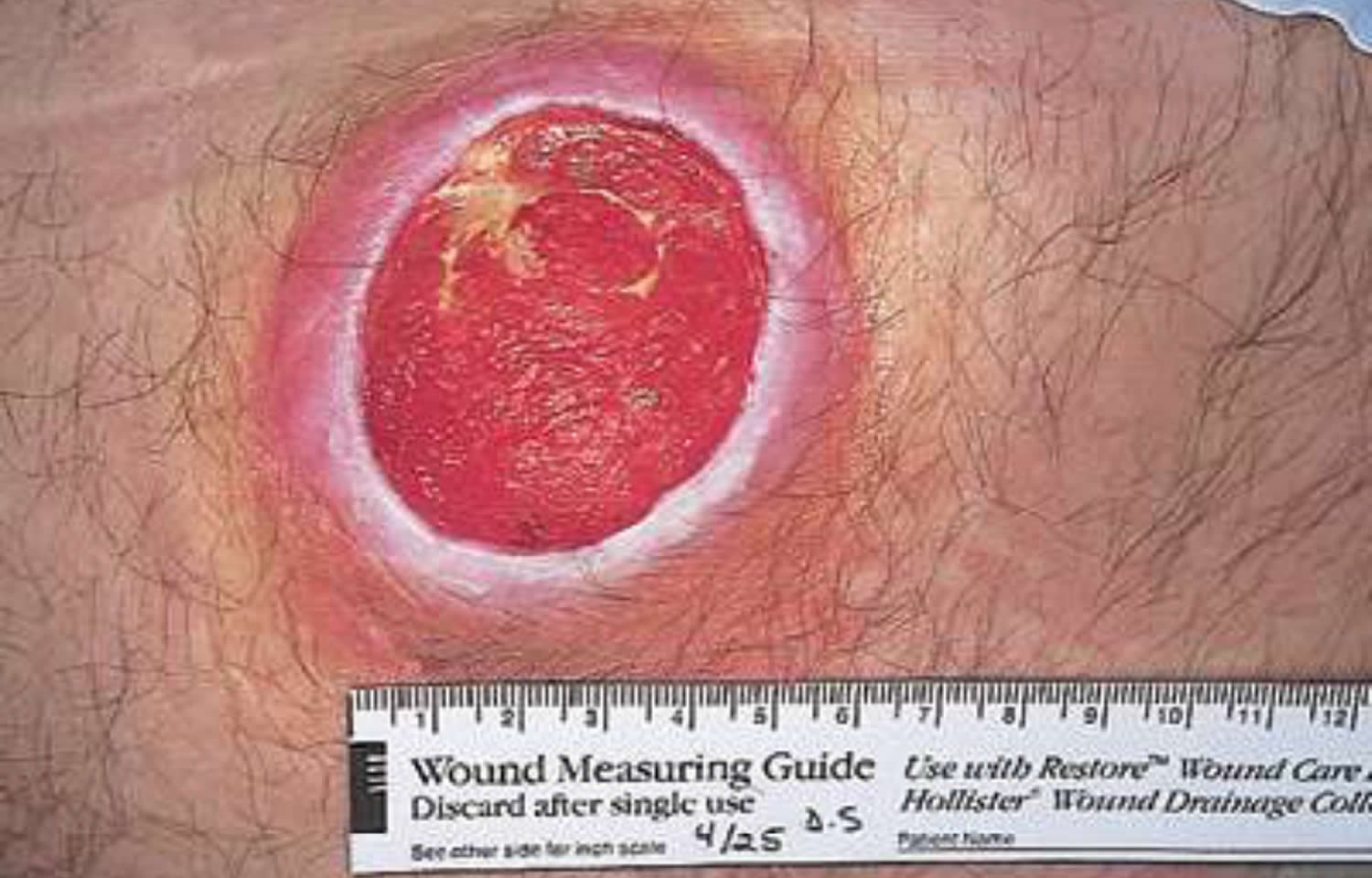
Stage 3 pressure ulcers, such as the one seen in Figure 5, usually have a crater-like appearance that extends into the subcutaneous tissue and although underlying bone, muscle, and fascia may be visible, the ulcer has no direct involvement of these structures. The presence of any necrotic slough in an ulcer that otherwise appears to be a stage 2 pressure ulcer automatically qualifies that ulcer to be a stage 3 ulcer. Stage 3 pressure ulcers may also involve tunneling and undermining, wherein the ulcer extends beneath normal tissue. This is due to increased damage to the tissue below the skin’s surface. This makes the wound deeper.
Figure 5. Stage 3 pressure ulcer
Stage 4 Pressure ulcer
Stage 4 pressure ulcers extend into bone or muscle, as is seen in Figure 6. Stage 4 pressure ulcer is the most serious type of pressure sore. The skin and tissue is severely damaged. This causes a large wound. Infection can occur at this stage. You are likely able to see muscle, bones, tendons, and joints in stage 4 pressure sores.
Patients outside of acute-care hospitals with stage 3 and stage 4 pressure ulcers qualify for Medicare Durable Medical Equipment coverage for more specialized mattresses and hospital beds.
Figure 6. Stage 4 pressure ulcer

What causes pressure sores?
Bedsores are caused by pressure against the skin that limits blood flow to the skin. Pressure sores are caused by sitting or lying in one position for too long (more than 2 hours for a stage 1 pressure sore). This puts pressure on certain areas of your body. This reduces blood supply to the skin and the tissue under the skin. If you don’t change position frequently, the blood supply will get too low. A sore will develop.
Three primary contributing factors for bedsores are:
- Pressure. Constant pressure on any part of your body can lessen the blood flow to tissues. Blood flow is essential to delivering oxygen and other nutrients to tissues. Without these essential nutrients, skin and nearby tissues are damaged and might eventually die. For people with limited mobility, this kind of pressure tends to happen in areas that aren’t well-padded with muscle or fat and that lie over a bone, such as the spine, tailbone, shoulder blades, hips, heels and elbows.
- Friction. Friction occurs when the skin rubs against clothing or bedding. It can make fragile skin more vulnerable to injury, especially if the skin is also moist.
- Shear. Shear occurs when two surfaces move in the opposite direction. For example, when a bed is elevated at the head, you can slide down in bed. As the tailbone moves down, the skin over the bone might stay in place — essentially pulling in the opposite direction.
Risk factors for developing pressure sores
People are at risk of developing pressure sores if they have difficulty moving and are unable to easily change position while seated or in bed. Risk factors include:
- Immobility. This might be due to poor health, spinal cord injury and other causes.
- Lack of sensory perception. Spinal cord injuries, neurological disorders and other conditions can result in a loss of sensation. An inability to feel pain or discomfort can result in not being aware of warning signs and the need to change position.
- Poor nutrition and hydration. People need enough fluids, calories, protein, vitamins and minerals in their daily diet to maintain healthy skin and prevent the breakdown of tissues.
- Medical conditions affecting blood flow. Health problems that can affect blood flow, such as diabetes and vascular disease, increase the risk of tissue damage.
Pressure ulcer prevention
It can be difficult to completely prevent pressure ulcers, but there are some things you or your care team can do to reduce the risk. The best way to prevent pressure sores is to avoid spending long periods of time in a chair or bed. If you are unable to turn and move, ask your caretaker to help. If you know you will be having surgery and will spend long amounts of time in bed, prepare in advance. Talk to the person who will be assisting with your care to come up with a plan to help you move.
Pressure ulcer prevention include:
- Regularly changing your position – if you’re unable to change position yourself, a relative or carer will need to help you. If you use a wheelchair, try shifting your weight about every 15 minutes. Ask for help with repositioning about once an hour.
- Lift yourself, if possible. If you have enough upper body strength, do wheelchair pushups — raising your body off the seat by pushing on the arms of the chair.
- Look into a specialty wheelchair. Some wheelchairs allow you to tilt them, which can relieve pressure.
- Select cushions or a mattress that relieves pressure. Use cushions or a special mattress to relieve pressure and help ensure your body is well-positioned. Do not use doughnut cushions, as they can focus pressure on surrounding tissue.
- Adjust the elevation of your bed. If your bed can be elevated at the head, raise it no more than 30 degrees. This helps prevent shearing.
- Checking your skin every day for early signs and symptoms of pressure ulcers – this will be done by your care team if you’re in a hospital or care home
- Keep skin clean and dry. Wash the skin with a gentle cleanser and pat dry. Do this cleansing routine regularly to limit the skin’s exposure to moisture, urine and stool.
- Protect your skin. Use plain talcum powder to protect skin at friction points. Apply lotion to dry skin. Change bedding and clothing frequently if needed. Watch for buttons on the clothing and wrinkles in the bedding that irritate the skin.
- Having a healthy, balanced diet that contains enough protein and a good variety of vitamins and minerals – if you’re concerned about your diet or caring for someone whose diet may be poor, ask your doctor or healthcare team for a referral to a dietitian
- Stopping smoking – smoking makes you more likely to get pressure ulcers because of the damage caused to blood circulation
If you’re recovering from illness or surgery at home, or are caring for someone confined to bed or a wheelchair, ask your doctor for an assessment of the risk of developing pressure ulcers.
Keep your skin healthy. This includes keeping your skin clean and dry. A mild soap and warm (not hot) water can help. Apply moisturizers to your skin so it doesn’t get too dry. If you must spend a lot of time in bed or in a wheelchair, check your entire body daily. Look for spots, color changes, or other signs of sores. Pay special attention to the pressure points where sores are most likely to occur. If you’re in a hospital or care home, your healthcare team should be aware of the risk of developing pressure ulcers. They should carry out a risk assessment, monitor your skin and use preventative measures, such as regular repositioning.
If you smoke, quit. People who smoke are more likely to develop pressure sores. Exercise can help improve blood flow. Do what you can to strengthen your muscles and improve your overall health. Talk to your doctor if physical activity is hard for you. He or she can suggest exercises that can work for you. Your doctor also can refer you to a physical therapist for help.
How to treat bed sores
Treatments for pressure ulcers depend on how severe they are. Do not attempt self-care for any ulcer beyond stage 2 in appearance.
Treatment options for pressure ulcers (sores) typically include regularly changing your position, using special mattresses to reduce or relieve pressure, and dressings to help heal the ulcer. In some cases, surgery may be needed.
In the early stages (1 and 2) of bedsores, the area may heal with relief of pressure and by applying care to the affected skin.
A good diet will aid skin healing, especially by taking in enough vitamin C and zinc, which are available as supplements.
Treatment of an infected pressure sore depends on the seriousness of the infection. If only the sore is infected, an antibiotic cream can be applied to the sore. When bone or deeper tissue is infected, systemic (not topical) antibiotics are often required. Antibiotics can be given intravenously (through a small needle inserted into a vein) or orally (by mouth).
For effective skin care:
- If the skin is not broken, gently wash the area with a mild soap and water.
- Clean open sores on the skin with salt water (saline, which can be made by boiling 1 quart of water with 1 teaspoon of salt for 5 minutes and kept cooled in a sterile container).
- Apply a thin layer of petroleum jelly (Vaseline®) and then cover with a soft gauze dressing.
- Be sure to keep urine and stool away from affected areas.
To relieve pressure:
- Change positions often (every 15 minutes in a chair and every 2 hours in a bed).
- Use special soft materials or supports (pads, cushions, and mattresses) to reduce pressure against the skin.
Other treatments include:
- Use foam pads or pillows to take pressure off the sore. Special mattresses, mattress covers, foam wedges, or seat cushions can help support you in bed or in a chair to reduce or relieve pressure. Avoid resting directly on your hip bone when you’re lying on your side. Use pillows under one side so that your weight rests on the fatty part of your buttocks instead of on your hip bone. Also, use pillows to keep your knees and ankles apart. When lying on your back, place a pillow under your lower calves to lift your ankles slightly off the bed. When lying in bed, change your position at least every 2 hours.
- When sitting in a chair or wheelchair, sit upright and straight. An upright, straight position allows you to move more easily and help prevent new sores. Change positions every 15 minutes when sitting in a chair or wheelchair. If you cannot move by yourself, have your caregiver help you shift your position.
- Improve your nutrition to help the sore heal.
- Maintain good hygiene. Stage 1 sores can be cleaned with mild soap and water. You can clean stage 2 sores by rinsing the area with a salt and water solution. The saltwater removes extra fluid and loose material. Your doctor or nurse can show you how to clean your stage 1 and 2 pressure sores. Your doctor or nurse will likely need to clean stage 3 and 4 pressure sores because of their seriousness.
Pressure ulcer treatment
In addition to self-care, your doctor might prescribe special pads or mattresses. Special dressings may be used, and whirlpool baths or surgery may be recommended to remove dead tissue. Infection requires antibiotic treatment. Sometimes deep wounds may require surgery to restore the tissue. Experimental work is now being done using honey preparations, high-pressure (hyperbaric) oxygen, and application of chemicals that stimulate cell growth (growth factors).
Changing position
Moving and regularly changing your position helps to relieve the pressure on ulcers that have already developed. It also helps prevent pressure ulcers developing.
After your care team has carried out an assessment of your risk of developing pressure ulcers, they will draw up a repositioning timetable. This states how often you need to move, or be moved if you’re unable to do so yourself.
For some people, this may be as often as once every 15 minutes. Others may need to be moved only once every two to four hours.
You may also be given training and advice about:
- correct sitting and lying positions
- how you can adjust your sitting and lying positions
- how best to support your feet to relieve pressure on your heels
- any special equipment you need and how to use it
Mattresses and cushions
If you’re at risk of getting pressure ulcers or have a minor ulcer, your care team will recommend a specially designed static foam or dynamic mattress.
If you have a more serious ulcer, you will require a more sophisticated mattress or bed system, such as a mattress connected to a pump that delivers a constant flow of air into the mattress itself.
There are also a range of foam or pressure-redistributing cushions available. Ask your carer about the types most suitable for you.
But according to the National Institute for Health and Care Excellence, there’s limited evidence on what kinds of pressure-redistributing devices are best for the relief and prevention of pressure ulcers in different places, such as heels or hips.
Dressings
Specially designed dressings can be used to protect pressure ulcers and speed up the healing process.
These dressings include:
- alginate dressings – these are made from seaweed and contain sodium and calcium, which are known to speed up the healing process
- hydrocolloid dressings – contain a special gel that encourages the growth of new skin cells in the ulcer, while keeping the surrounding healthy skin dry
- other dressing types – such as foams, films, hydrofibres/gelling fibres, gels and antimicrobial (antibiotic) dressings may also be used
Ask your carer about which type of dressing they’re using for the management of your pressure ulcer.
Gauze dressings aren’t recommended for either the prevention or treatment of pressure ulcers.
Creams and ointments
Topical antiseptic or antimicrobial (antibiotic) creams and ointments aren’t usually recommended for treating pressure ulcers.
But barrier creams may be needed to protect skin that’s been damaged or irritated by incontinence.
Antibiotics
Antibiotics may be prescribed to treat an infected ulcer or if you have a serious infection, such as:
- blood poisoning (sepsis)
- bacterial infection of tissues under the skin (cellulitis)
- infection of the bone (osteomyelitis)
Diet and nutrition
Eating a healthy, balanced diet that contains enough protein and a good variety of vitamins and minerals can speed up the healing process.
If your diet is poor, you may see a dietitian. They can draw up a suitable dietary plan for you.
It’s also important to keep up fluid intake to avoid dehydration, as being dehydrated can slow down the healing process.
Removing damaged tissue (debridement)
In some cases, it may be necessary to remove dead tissue from the pressure ulcer to help it heal. This is known as debridement.
If there’s a small amount of dead tissue, it may be removed using specially designed dressings.
Larger amounts of dead tissue may be removed using:
- high-pressure water jets
- ultrasound
- surgical instruments, such as scalpels and forceps
A local anaesthetic should be used to numb the area around the ulcer so debridement (if not being treated with a dressing) doesn’t cause you any pain.
Surgery
Severe pressure ulcers might not heal on their own. In such cases, surgery may be required to seal the wound, speed up healing, and minimise the risk of infection.
Surgical treatment involves:
- cleaning the wound and closing it by bringing the edges of the ulcer together
- cleaning the wound and using tissue from healthy skin nearby to close the ulcer
Pressure ulcer surgery can be challenging, especially because most people who have the procedure are already in a poor state of health.
Risks after surgery include:
- implanted skin tissue dying
- blood poisoning
- infection of the bone (osteomyelitis)
- abscesses
- deep vein thrombosis
Ask your surgeon about the benefits and risks of surgery if it’s recommended for you.
Living with bed sores
Living with pressure sores means making plans to move and turn frequently. Also, it means maintaining good hygiene. Pressure sores should be kept covered with a bandage or dressing. Sometimes gauze is used. The gauze is kept moist and must be changed at least once a day. Newer kinds of dressings include a see-through film and a hydrocolloid dressing. A hydrocolloid dressing is a bandage made of a gel that molds to the pressure sore and helps promote healing and skin growth. These dressings can stay on for several days at a time.
Dead tissue (which may look like a scab) in the sore can interfere with healing and lead to infection. There are many ways to remove dead tissue from the pressure sore. Rinsing the sore every time you change the bandage is helpful. There are special dressings that help your body dissolve the dead tissue on its own. The dressing must be left in place for several days.
Another way to remove dead tissue is to put wet gauze bandages on the sore and allow them to dry. The dead tissue sticks to the gauze and is removed when the gauze is pulled off. For more severe pressure sores, dead tissue must be removed surgically by your doctor.
Removing dead tissue and cleaning the sore can hurt. Your doctor can suggest a pain medicine for you to take 30 to 60 minutes before your dressing is changed.
Good nutrition is important because it helps your body heal the sore. If you don’t get enough calories, protein, and other nutrients (vitamin C and zinc help heal wounds), your body won’t be able to heal. Your doctor, nurse, or a dietitian can give you advice about a healthy diet. Be sure to tell your doctor if you have lost or gained weight recently.
As a pressure sore heals, it slowly gets smaller. Less fluid drains from it. New, healthy tissue starts growing at the bottom of the sore. This new tissue is light red or pink and looks lumpy and shiny. It may take 2 to 4 weeks of treatment before you see these signs of healing.
- Pompeo MQ. The role of “wound burden” in determining the costs associated with wound care. Ostomy Wound Manage. 2001 Mar;47(3):65–71.[↩]
- Russo CA, Steiner C, Spector W. Statistical Brief #64: Hospitalizations related to pressure ulcers among adults 18 years and older, 2006 [monograph on the Internet]. Rockville, MD: US Agency for Healthcare Research and Quality: Healthcare Cost and Utilization Project (HCUP); 2008 Dec. https://www.hcup-us.ahrq.gov/reports/statbriefs/sb64.jsp[↩]
- Pressure ulcers [monograph on the Internet] Publication 1999/23. The Hague: Health Council of the Netherlands; 1999 Dec 31. https://www.gezondheidsraad.nl/en/publications/pressure-ulcers[↩]
- Auerbach PS. Wilderness medicine. 5th ed. St Louis, MO: Mosby; 2007.[↩]
- Pressure ulcer staging illustrations [monograph on the Internet]. Washington, DC: National Pressure Ulcer Advisory Panel; 2007. http://www.npuap.org/resources/educational-and-clinical-resources/pressure-injury-staging-illustrations/[↩]
- European Pressure Ulcer Advisory Panel & National Pressure Ulcer Advisory Panel. Prevention and treatment of pressure ulcers: quick reference guide [monograph on the Internet]. Washington DC: National Pressure Ulcer Advisory Panel; 2009. http://www.epuap.org/[↩]
- Wake WT. Pressure Ulcers: What Clinicians Need to Know. The Permanente Journal. 2010;14(2):56-60. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2912087/[↩]
- Pressure ulcer staging illustrations [monograph on the Internet]. Washington, DC: National Pressure Ulcer Advisory Panel; 2007. http://www.npuap.org/wp-content/uploads/2012/03/Deep-Tissue-Pressure-Injury-April-2016.jpg[↩]





{kind=link}