
Contents
Biliary colic
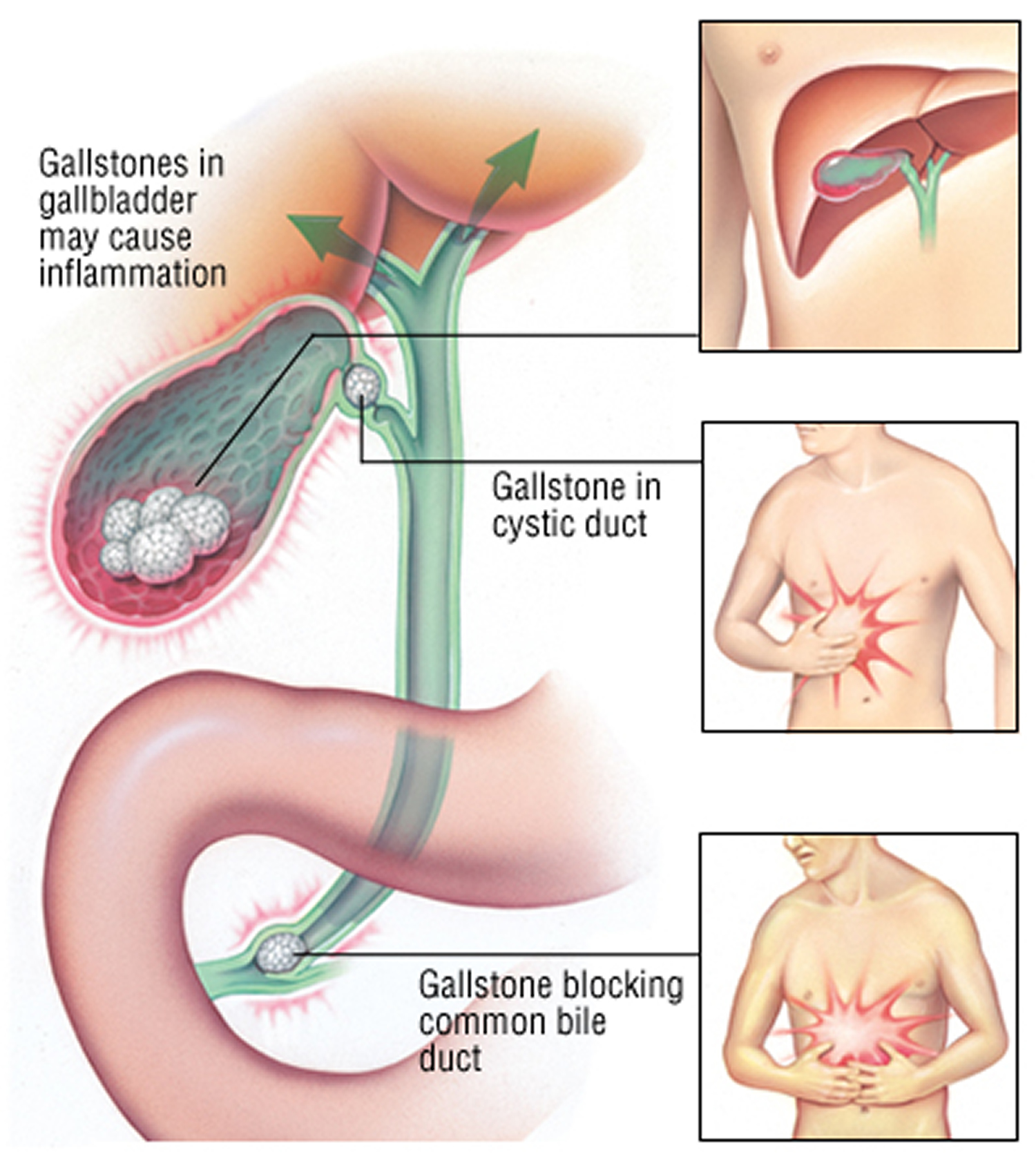
Biliary colic also known as a gallbladder attacks or gallstone attacks, is a steady or intermittent ache or pain that “comes and goes,” in your upper right abdomen, usually under the right side of your rib cage, sometimes lasting several hours 1. Biliary colic is a common presentation of a stone in the cystic duct or common bile duct of the biliary tree 2. Biliary colic happens when something blocks the normal flow of bile from the gallbladder. Bile is a liquid that helps to digest fats. Under normal circumstances, bile is made in the liver and stored in the gallbladder. When you eat a meal, bile passes from the gallbladder through the cystic duct and the common bile duct into the small intestine, where it mixes with partially digested food. Biliary colic or gallbladder attacks typically follow heavy meals, fatty meal which causes contraction of the gallbladder and usually occur in the evening or during the night. However, the pain is usually constant and not colicky. If you’ve had one gallbladder attack, more attacks will likely follow.
Gallstones are the most common reason for biliary colic. If a gallstone blocks either of these ducts, the normal flow of bile into the intestine is disrupted. The muscle cells in the bile duct contract vigorously to try to move the stone, causing the pain of biliary colic. A stricture of the bile duct or a tumor also can block bile flow and cause biliary colic.
Biliary colic has a female predominance due to the influence of estrogen on the formation of gallstones. Obesity and elevated cholesterol are also strongly correlated to biliary colic and gallbladder disease 3.
Cholelithiasis is the presence of one or more calculi (gallstones) in the gallbladder. In developed countries, about 10% of adults and 20% of people > 65 years have gallstones. In 1% to 3% of patients gallstones tend to be asymptomatic, also referred to as asymptomatic cholelithiasis or “silent gallstones”. Silent gallstones don’t stop your gallbladder, liver, or pancreas from working, so they do not need treatment.
The most common symptom of gallstones is biliary colic; gallbladder attacks usually stop when gallstones move and no longer block the bile ducts. However, if any of your bile ducts stay blocked for more than a few hours, you may develop gallstone complications. Gallstones that do not block your bile ducts do not cause symptoms. More serious complications include cholecystitis; biliary tract obstruction (by stones in the bile ducts [choledocholithiasis]), sometimes with infection (cholangitis); and gallstone pancreatitis.
Gallstones do not cause dyspepsia or fatty food intolerance 4.
Diagnosis is usually by ultrasonography. If cholelithiasis causes symptoms or complications, cholecystectomy is necessary.
Treatment of biliary colic is primarily surgical, involving removal of the gallbladder, typically using a laparoscopic technique. Biliary colic does not typically require hospital admission 5.
Biliary colic key points
- In developed countries, about 10% of adults and 20% of people > 65 years have gallstones, but 80% are asymptomatic.
- Abdominal ultrasonography is 95% sensitive and specific for detecting gallbladder stones.
- Once symptoms develop (usually biliary colic), pain returns in 20 to 40% of patients/year.
- Treat most patients who have symptomatic gallstones with laparoscopic cholecystectomy.
Seek care right away for a biliary colic.
See a doctor right away if you are having these symptoms during or after a gallbladder attack:
- pain in your abdomen lasting several hours
- nausea and vomiting
- fever—even a low-grade fever—or chills
- yellowish color of your skin or whites of your eyes, called jaundice
- tea-colored urine and light-colored stools
These symptoms may be signs of a serious infection or inflammation of the gallbladder, liver, or pancreas. Gallstone symptoms may be similar to symptoms of other conditions, such as appendicitis, ulcers, pancreatitis, and gastroesophageal reflux disease, all of which should be treated by a doctor as soon as possible.
Gallstone complications can occur if your bile ducts stay blocked. Left untreated, blockages of the bile ducts or pancreatic duct can be fatal.
Who is more likely to develop gallstones?
Certain groups of people have a higher risk of developing gallstones than others 6:
- Women are more likely to develop gallstones than men. Women who have extra estrogen in their body due to pregnancy, hormone replacement therapy, or birth control pills may be more likely to produce gallstones.
- Older people are more likely to develop gallstones. As you age, the chance that you’ll develop gallstones becomes higher.
- People with a family history of gallstones have a higher risk.
- American Indians have genes that raise the amount of cholesterol in their bile, and have the highest rate of gallstones in the United States.
- Mexican Americans are also at higher risk of developing gallstones.
You are more likely to develop gallstones if you have one of the following health conditions:
- Cirrhosis. Cirrhosis is severe scarring of the liver, a condition in which your liver slowly breaks down and stops working due to chronic, or long-lasting, injury
- Cholangitis or infections in the bile ducts, which can also be a complication of gallstones
- Hemolytic anemias, conditions in which red blood cells are continuously broken down, such as sickle cell anemia
- Some intestinal diseases that affect normal absorption of nutrients, such as Crohn’s disease
- High triglyceride levels (hypertriglyceridemia)
- Low HDL cholesterol
- Metabolic syndrome, which can also raise the risk of gallstone complications
- Diabetes and insulin resistance
- Bone marrow or solid organ transplant
- Failure of the gallbladder to empty bile properly (this is more likely to happen during pregnancy)
You are more likely to develop gallstones if you:
- have obesity, especially if you are a woman
- have had rapid weight loss from eating a very low-calorie diet, or after weight loss surgery, also called metabolic and bariatric surgery
- have been on a diet high in calories and refined carbohydrates and low in fiber
- are receiving nutrition through a vein for a long period of time (intravenous feedings)
- are taking birth control pills.
How does weight affect gallstones?
Being overweight or having obesity may make you more likely to develop gallstones, especially if you are a woman. Researchers have found that people who have obesity may have higher levels of cholesterol in their bile, which can cause gallstones. People who have obesity may also have large gallbladders that do not work well. Some studies have shown that people who carry large amounts of fat around their waist may be more likely to develop gallstones than those who carry fat around their hips and thighs.
Losing weight very quickly may raise your chances of forming gallstones, however. Talk with your health care professional about how to lose weight safely.
How does my fast weight loss affect gallstones?
When you don’t eat for a long period of time or you lose weight quickly, your liver releases extra cholesterol into the bile. Fast weight loss can also prevent the gallbladder from emptying properly. Weight-loss surgery may lead to fast weight loss and higher risk of gallstones.
Your chances of developing gallstones may depend on the type of weight-loss treatment you choose. Diets or surgeries that cause fast weight loss may be more likely to lead to gallstone problems than diets or surgeries that lead to slower weight loss. If you have silent gallstones, you may also be more likely to develop gallstone symptoms.
Several factors may raise your chances of having problems with gallstones after weight-loss surgery or a very low-calorie diet. These factors include:
- gallstones that you had before your weight-loss surgery or before you went on a very low-calorie diet, especially if the stones caused symptoms
- a large amount of extra weight before you have weight-loss surgery or go on a very low-calorie diet
- very quick weight loss after the surgery or a very low-calorie diet
If you are starting a very low-calorie diet or having weight-loss surgery, talk with your doctor about how to lower your chances of developing gallstones. The medicine ursodiol can help prevent gallstones in people who lose weight rapidly through very low-calorie diets or weight-loss surgery.
Is weight cycling a problem?
Weight cycling, or losing and regaining weight repeatedly, may also lead to gallstones. The more weight you lose and regain during a cycle, the greater your chances of developing gallstones.
Stay away from “crash diets” that promise to help you drop the pounds quickly. Aim for losing weight at a slower pace and keeping it off over time.
How can I safely lose weight to lower my chances of getting gallstones?
Losing weight at a slow pace may make it less likely that you will develop gallstones. For people who are overweight or have obesity, experts recommend beginning with a weight loss of 5 to 10 percent of your starting weight over a period of 6 months 7. In addition, weight loss may bring you other benefits such as better mood, more energy, and positive self-image.
When making healthy food choices to help you lose weight, you can choose food that may also lower your chances of developing gallstones.
Regular physical activity, which will improve your overall health, may also lower your chances of developing gallstones. To improve health or prevent weight gain, aim for at least 150 minutes a week of moderate-intensity physical activity, like brisk walking or fast dancing. Adults also need muscle-strengthening activity, like lifting weights or doing push-ups, at least 2 days a week 8.
Talk with your doctor before you start an eating and physical activity plan to improve your health or maintain your weight loss.
The gallbladder
The gallbladder is a small, pouch-like organ found underneath the liver. Its main purpose is to store and concentrate bile.
Bile is a liquid produced by the liver to help digest fats. It’s passed from the liver into the gallbladder through a series of channels known as bile ducts.
The bile is stored in the gallbladder and, over time, becomes more concentrated, which makes it better at digesting fats.
The gallbladder releases bile into the digestive system when it’s needed.
Figure 1. Gallbladder location
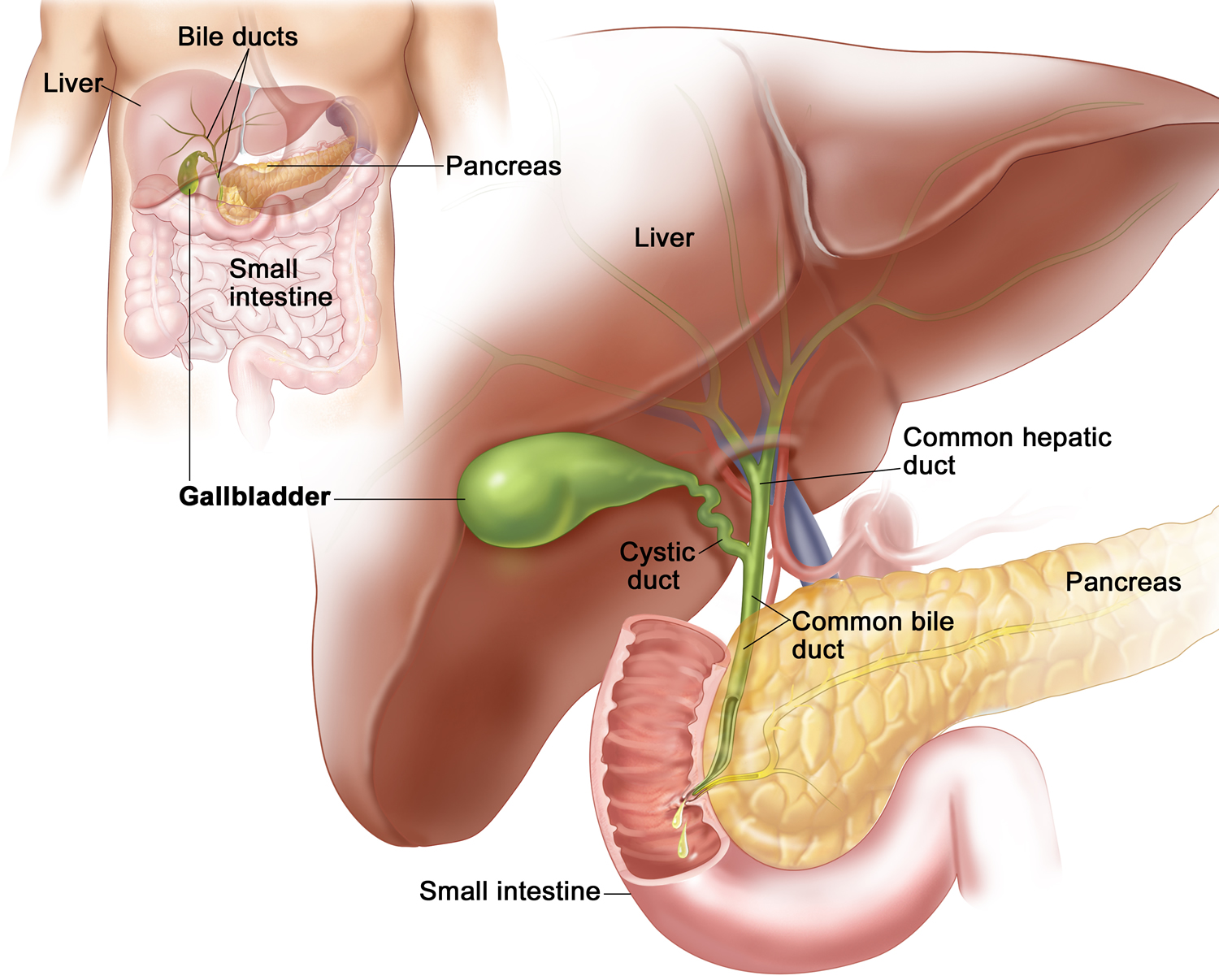
Figure 2. Gallbladder anatomy
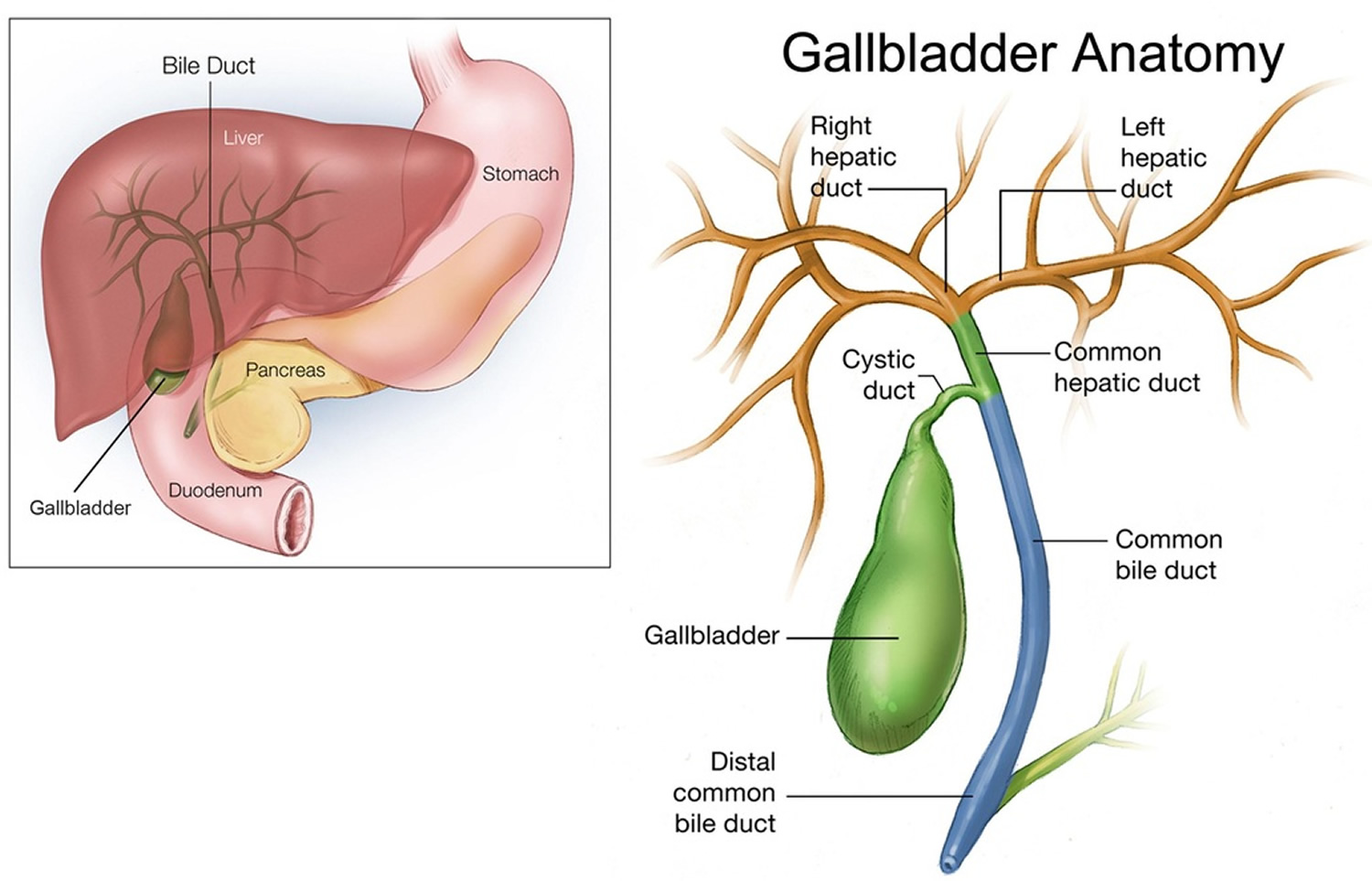
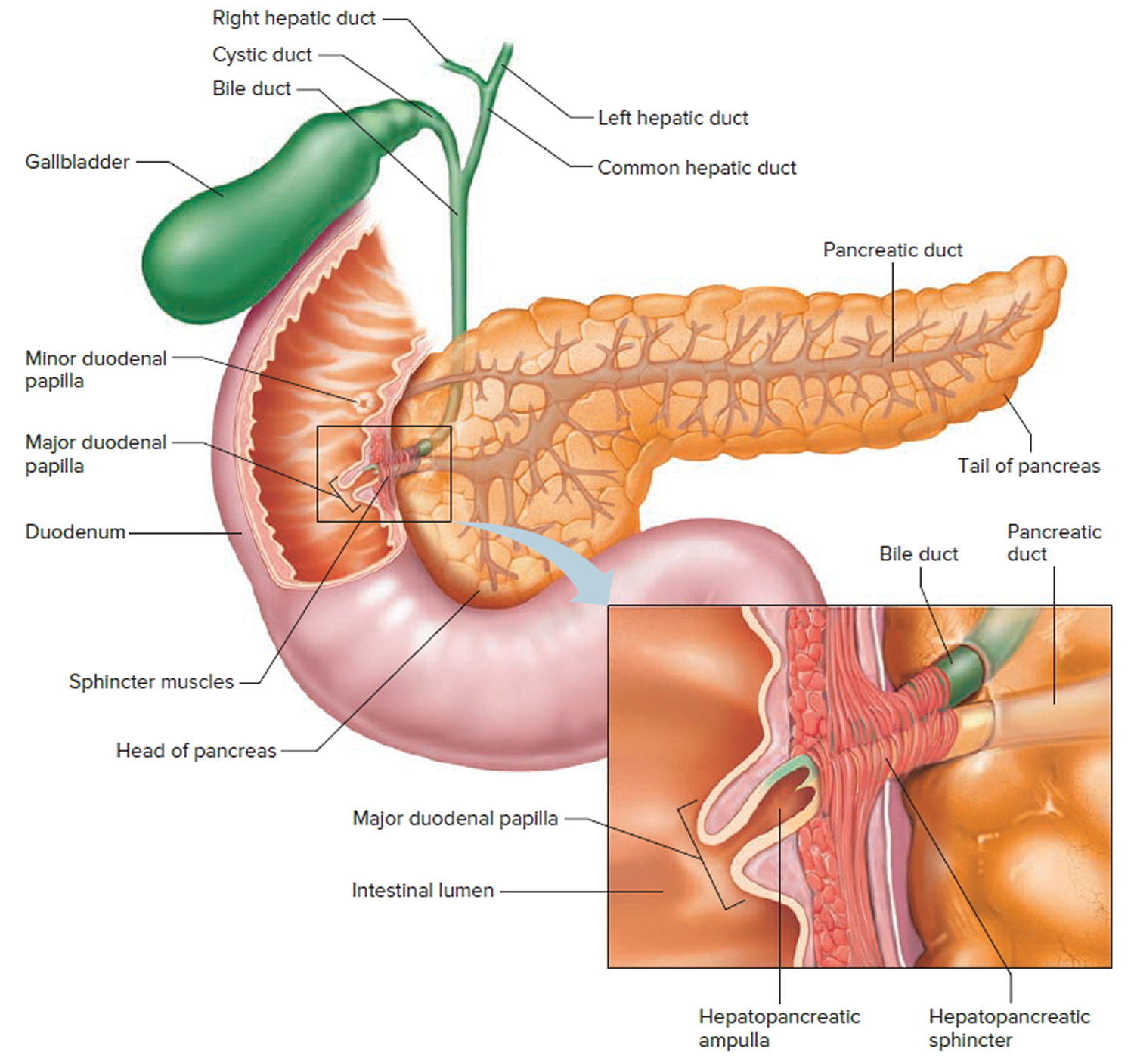
Figure 3. The common bile duct is closely associated with the pancreatic duct and the duodenum
Gallbladder function
Following a meal, the mixing movements of the stomach wall aid in producing a semifluid paste of food particles and gastric juice called chyme.
As chyme enters the duodenum (the proximal portion of the small intestine), accessory organs—the pancreas, liver, and gallbladder—add their secretions.
Bile is a yellowish-green liquid continuously secreted from hepatic (liver) cells. In addition to water, bile contains bile salts, bile pigments (bilirubin and biliverdin), cholesterol, and electrolytes. Of these, bile salts are the most abundant and are the only bile components that have a digestive function.
Bile pigments are breakdown products of hemoglobin from red blood cells and are normally secreted in the bile.
Normally bile does not enter the duodenum until cholecystokinin stimulates the gallbladder to contract. Proteins and fats in chyme in the duodenum stimulate
the intestinal wall to release cholecystokinin. Cholecystokinin travels via the bloodstream to the pancreas also, where it stimulate the pancreas to release its pancreatic juice that has a high concentration of digestive enzymes.
The hepatopancreatic sphincter usually remains contracted until a peristaltic wave in the duodenal wall approaches it. Then the sphincter relaxes, and bile is squirted into the duodenum (see Figure 4).
Note: Cholecystokinin produced by the intestinal wall cells, in response to proteins and fats in the small intestine, decreases secretory activity of gastric glands and inhibits gastric motility; stimulates pancreas to secrete fluid with a high digestive enzyme concentration and stimulates gallbladder to contract and release bile.
Figure 4. Fatty chyme entering the duodenum stimulates the gallbladder to release bile
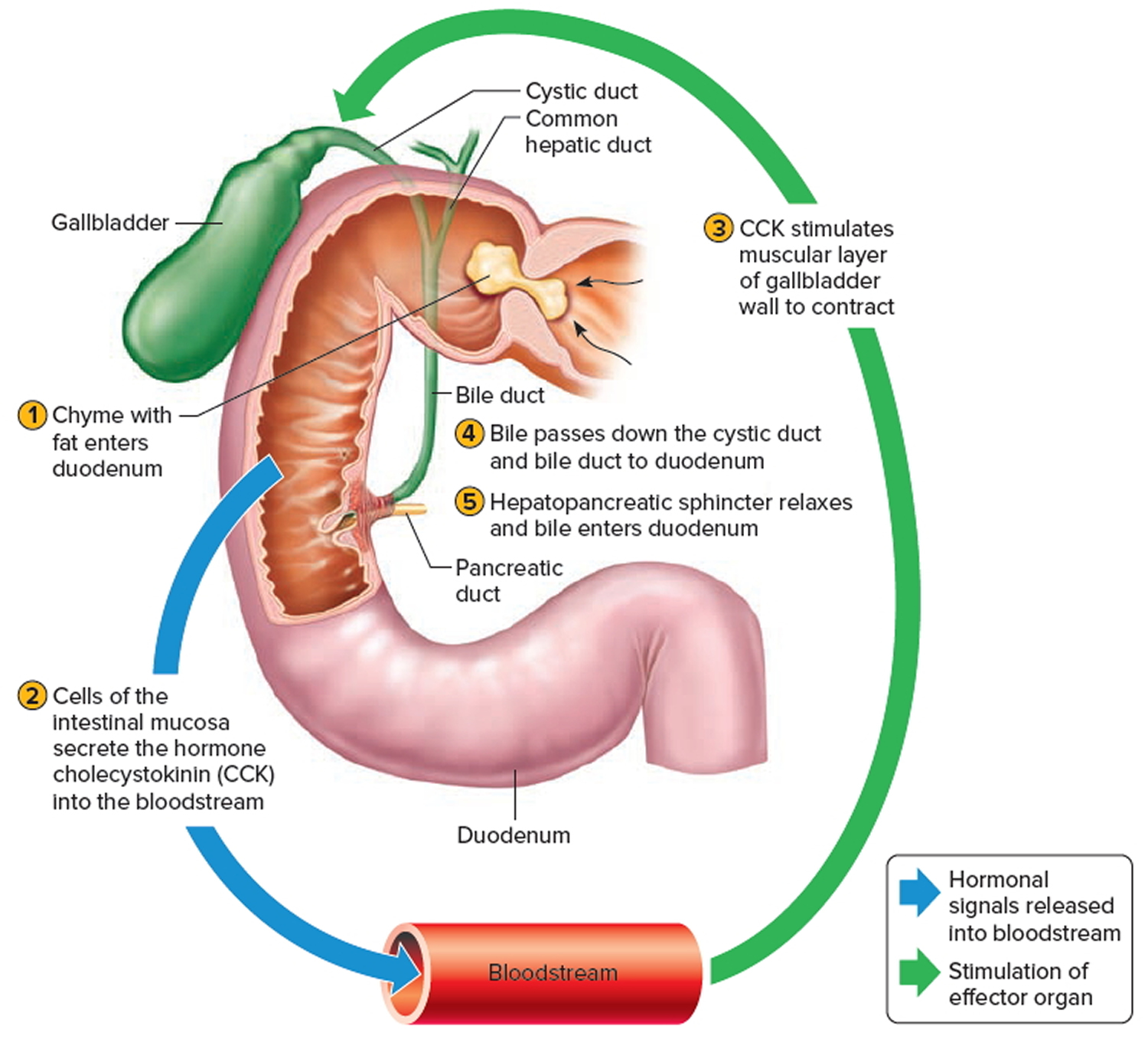
Figure 5. Gallstones
Biliary colic without gallstones
Biliary colic without gallstones also called acalculous biliary pain, can occur in the absence of gallstones, particularly in young women due to structural or functional disorders; it is sometimes treated with laparoscopic cholecystectomy 9.
Biliary colic without gallstones or acalculous biliary pain accounts for up to 15% of laparoscopic cholecystectomies.
Common causes of such biliary pain without gallstones include the following:
- Microscopic stones—not detected by routine abdominal ultrasonography
- Abnormal gallbladder emptying
- An overly sensitive biliary tract
- Sphincter of Oddi dysfunction
- Hypersensitivity of the adjacent duodenum
- Possibly gallstones that have spontaneously passed
Some patients eventually develop other functional gastrointestinal disorders.
Biliary colic without gallstones diagnosis
The best diagnostic approach remains unclear.
Biliary colic without gallstones or acalculous biliary pain is suspected in patients with biliary colic when diagnostic imaging cannot detect gallstones. Imaging should include ultrasonography and, where available, endoscopic ultrasonography (for small stones < 1 cm).
Abnormal laboratory tests may reveal evidence of a biliary tract abnormality (eg, elevated alkaline phosphatase, bilirubin, ALT, or AST) or a pancreatic abnormality (eg, elevated lipase) during an episode of acute pain. Cholescintigraphy with cholecystokinin infusion measures gallbladder emptying (ejection fraction); potentially interfering drugs such as calcium channel blockers, opioids, and anticholinergics should not be used. Endoscopic retrograde cholangiopancreatography (ERCP) with biliary manometry detects sphincter of Oddi dysfunction.
Biliary colic without gallstones treatment
Biliary colic without gallstones treatment remains unclear, but sometimes laparoscopic cholecystectomy. Laparoscopic cholecystectomy improves outcomes for patients with microscopic stones and possibly abnormal gallbladder motility. Otherwise, the role of laparoscopic cholecystectomy or endoscopic sphincterotomy remains unclear. Drug therapies have no proven benefit.
Biliary colic causes
Gallstones are formed within the gallbladder and may be composed of either cholesterol or bilirubin. Gallstones may form if bile contains too much cholesterol, too much bilirubin, or not enough bile salts. Researchers do not fully understand why these changes in bile occur. Gallstones also may form if the gallbladder does not empty completely or often enough. Certain people are more likely to have gallstones than others because of their risk factors for gallstones, including obesity and certain kinds of dieting.
These stones may stay in the gallbladder and remain asymptomatic or may enter the cystic duct or common bile duct where they may become lodged and cause pain when the gallbladder contracts. The pain typically arises after meals, when the gallbladder contracts to release bile into the duodenum to aid in digestion by emulsifying fats. Stones commonly exist within the gallbladder without symptoms, also referred to as asymptomatic cholelithiasis. Asymptomatic cholelithiasis typically requires no medical or surgical treatment and may be managed expectantly and does not require further follow up. However, if pain, nausea, or vomiting do present, most commonly as right upper quadrant (RUQ) abdominal pain, the patient may be diagnosed with symptomatic cholelithiasis and will require surgical evaluation 10.
Gallstones are formed in the gallbladder and can be composed of cholesterol or bilirubin. Fatty meals cause the release of cholecystokinin (CCK) from the duodenum, which subsequently causes contraction of the gallbladder. This contraction can expel stones from the gallbladder into the cystic duct or common bile duct. Less commonly, stones may also be formed within the common bile duct (CBD) and are referred to as primary common bile duct stones. These stones irritate the lining of the ducts, causing pain, which notably is present during times of gallbladder and duct contraction 11.
Risk factors for biliary colic
There are three main pathways in the formation of gallstones:
- Cholesterol supersaturation: Normally, bile can dissolve the amount of cholesterol excreted by the liver. But if the liver produces more cholesterol than bile can dissolve, the excess cholesterol may precipitate as crystals. Crystals are trapped in gallbladder mucus, producing gallbladder sludge. With time, the crystals may grow to form stones and occlude the ducts which ultimately produce the gallstone disease.
- Excess bilirubin: Bilirubin, a yellow pigment derived from the breakdown of red blood cells, is secreted into bile by liver cells. Certain hematologic conditions cause the liver to make too much bilirubin through the processing of breakdown of hemoglobin. This excess bilirubin may also cause gallstone formation.
- Gallbladder hypomotility or impaired contractility: If the gallbladder does not empty effectively, bile may become concentrated and form gallstones.
Depending on the cause, gallstones have different compositions. The three most common types are cholesterol gallstones, black pigment gallstones, and brown pigment gallstones. Ninety percent of gallstones are cholesterol gallstones.
You are more likely to develop gallstones if you have one of the following health conditions and risk factors:
- Being female
- Being age 40 or older
- Being a Native American
- Being a Mexican-American
- Being overweight or obese
- Having metabolic syndrome, which can also raise the risk of gallstone complications
- Being sedentary
- Being pregnant
- Eating a high-fat diet
- Eating a high-cholesterol diet
- Eating a low-fiber diet
- Diet high in calories and refined carbohydrates
- Having a family history of gallstones
- Having diabetes and insulin resistance
- Losing weight very quickly like from weight-loss surgery, also called metabolic and bariatric surgery
- Taking medications that contain estrogen, such as oral contraceptives or hormone therapy drugs
- Having liver disease such as cirrhosis, a condition in which your liver slowly breaks down and stops working due to chronic, or long-lasting, injury
- Having infections in the bile ducts, which can also be a complication of gallstones
- Having hemolytic anemias, conditions in which red blood cells are continuously broken down, such as sickle cell anemia
- Some intestinal diseases that affect normal absorption of nutrients, such as Crohn’s disease
- High triglyceride levels
- Low HDL cholesterol
Gallstones pathophysiology
Biliary sludge is often a precursor of gallstones. It consists of calcium bilirubinate (a polymer of bilirubin), cholesterol microcrystals, and mucin. Sludge develops during gallbladder stasis, as occurs during pregnancy or use of TPN (total parenteral nutrition – a method of feeding that bypasses the gastrointestinal tract where fluids are given into a vein to provide most of the nutrients the body needs). Most sludge is asymptomatic and disappears when the primary condition resolves. Alternatively, sludge can evolve into gallstones or migrate into the biliary tract, obstructing the ducts and leading to biliary colic, cholangitis, or pancreatitis.
There are several types of gallstones.
Cholesterol stones account for > 85% of gallstones in the Western world. For cholesterol gallstones to form, the following is required:
- Bile must be supersaturated with cholesterol. Normally, water-insoluble cholesterol is made water soluble by combining with bile salts and lecithin to form mixed micelles. Supersaturation of bile with cholesterol most commonly results from excessive cholesterol secretion (as occurs in obesity or diabetes) but may result from a decrease in bile salt secretion (eg, in cystic fibrosis because of bile salt malabsorption) or in lecithin secretion (eg, in a rare genetic disorder that causes a form of progressive intrahepatic familial cholestasis).
- The excess cholesterol must precipitate from solution as solid microcrystals. Such precipitation in the gallbladder is accelerated by mucin, a glycoprotein, or other proteins in bile.
- The microcrystals must aggregate and grow. This process is facilitated by the binding effect of mucin forming a scaffold and by retention of microcrystals in the gallbladder with impaired contractility due to excess cholesterol in bile.
Black pigment stones are small, hard gallstones composed of calcium (Ca) bilirubinate and inorganic Ca salts (eg, Ca carbonate, Ca phosphate). Factors that accelerate stone development include alcoholic liver disease, chronic hemolysis, and older age.
Brown pigment stones are soft and greasy, consisting of bilirubinate and fatty acids (Ca palmitate or stearate). They form during infection, inflammation, and parasitic infestation (eg, liver flukes in Asia).
Gallstones grow at about 1 to 2 mm/year, taking 5 to 20 year before becoming large enough to cause problems. Most gallstones form within the gallbladder, but brown pigment stones form in the ducts. Gallstones may migrate to the bile duct after cholecystectomy or, particularly in the case of brown pigment stones, develop behind strictures as a result of stasis and infection.
Gallstones prevention
You can help prevent gallstones by:
- adjusting your eating plan to include more foods high in fiber and healthy fats, fewer refined carbohydrates, and less sugar
- losing weight safely if you are overweight or have obesity
- maintaining a healthy weight through healthy eating and regular physical activity.
Eating, diet and nutrition for gallstones
You can lower your risk of gallstones by following a healthy eating plan and getting regular physical activity to help you reach and maintain a healthy weight.
Experts recommend the following to help prevent gallstones:
- Eat more foods that are high in fiber, such as:
- fruits, vegetables, beans, and peas.
- whole grains, including brown rice, oats, and whole wheat bread.
- Eat fewer refined carbohydrates and less sugar.
- Eat healthy fats, like fish oil and olive oil, to help your gallbladder contract and empty on a regular basis.
- Avoid unhealthy fats, like those often found in desserts and fried foods.
Talk with your health care professional before you make any changes to your eating plan. Losing weight too quickly may cause health problems. Very low-calorie diets and weight-loss surgery can lead to rapid weight loss and raise your risk of gallstones.
Biliary colic symptoms
About 80% of people with gallstones are asymptomatic. The remainder have symptoms ranging from a characteristic type of pain (biliary colic) to cholecystitis to life-threatening cholangitis. Biliary colic is the most common symptom.
Stones occasionally traverse the cystic duct without causing symptoms. However, most gallstone migration leads to cystic duct obstruction, which, even if transient, causes biliary colic. Patients typically present with postprandial (after meal) pain that “comes and goes,” hence the term colic. Biliary colic characteristically begins in the right upper quadrant of the abdomen (under the right side of your rib cage) and may have radiation into the back but may occur elsewhere in the abdomen. It is often poorly localized, particularly in diabetics and the elderly. With uncomplicated biliary colic, patients will likely present only with pain. However, some may also report nausea and/or vomiting. These symptoms are accentuated after meals.
Episodes begin suddenly, become intense within 15 min to 1 h, remain at a steady intensity (not colicky) for up to 12 h (usually < 6 h), and then gradually disappear over 30 to 90 min, leaving a dull ache. The pain is usually severe enough to send patients to the emergency department for relief. Nausea and some vomiting are common, but fever and chills do not occur unless cholecystitis has developed. Mild right upper quadrant or epigastric tenderness may be present; peritoneal findings are absent. Between episodes, patients feel well.
Although biliary colic can follow a heavy meal, fatty food is not a specific precipitating factor. Nonspecific GI symptoms, such as gas, bloating, and nausea, have been inaccurately ascribed to gallbladder disease. These symptoms are common, having about equal prevalence in cholelithiasis, peptic ulcer disease, and functional GI disorders.
Little correlation exists between the severity and frequency of biliary colic and pathologic changes in the gallbladder. Biliary colic can occur in the absence of cholecystitis. If colic lasts > 12 h, particularly if it is accompanied by vomiting or fever, acute cholecystitis or pancreatitis is likely.
Biliary colic patients are afebrile and will commonly have no abnormal vitals in contrast to acute cholecystitis or cholangitis, which may present with fevers, tachycardia, or even hypotension if they progress to septic shock.
Patients with biliary colic will generally only have right upper quadrant (RUQ) or epigastric tenderness on physical exam. Abdominal distension and rebound tenderness are less common. Jaundice is not seen with blockage of the cystic duct; however, it is common with blockage of the common bile duct due to an elevation of direct bilirubin.
Biliary colic complications
Biliary colic complications include:
- Acute cholecystitis
- Pancreatitis
- Cholangitis and
- Gallbladder perforation
- depending on the location of the stone in the biliary tree.
These diseases are more serious and do require hospital admission and medical management.
Biliary colic diagnosis
Doctors use your medical history, a physical exam, and lab and imaging tests to diagnose gallstones.
A health care professional will ask you about your symptoms. He or she will ask if you have a history of health conditions or health concerns that make you more likely to get gallstones. The health care professional also may ask if you have a family history of gallstones and what you typically eat. During a physical exam, the health care professional examines your body and checks for pain in your abdomen.
Health care professionals may use lab or imaging tests to diagnose gallstones.
Laboratory tests to be ordered include a complete blood count (CBC) and a metabolic panel with liver function tests. It is important to have these tests to rule out more serious gallbladder pathology such as acute cholecystitis or cholangitis. With an elevated white blood cell (WBC) count, the suspicion of acute cholecystitis or ascending cholangitis rises. Elevated liver enzymes such as direct bilirubin, AST, ALT, ALP, and GGT suggest a stone or blockage in the common bile duct. Stones within the gallbladder or cystic duct typically do not produce any laboratory abnormalities 12.
Right upper quadrant abdominal ultrasound is the first radiologic test to evaluate suspected biliary pathology. Ultrasound is the best imaging test for finding gallstones. Ultrasound uses a device called a transducer, which bounces safe, painless sound waves off your organs to create an image or picture of their structure. If you have gallstones, they will be seen in the image. Sometimes, health care professionals find silent gallstones when you don’t have any symptoms.
Hydroxyl iminodiacetic acid scan (HIDA) scans also called cholescintigraphy or hepatobiliary scans, are useful in evaluating acute or chronic cholecystitis and biliary dyskinesia. HIDA scan, or hepatobiliary scan—uses a safe radioactive material to produce pictures of your biliary tract. You’ll lie on a table while a health care professional injects a small amount of the radioactive material into a vein in your arm. The health care professional may also inject a substance that causes your gallbladder to squeeze. A special camera takes pictures of the radioactive material as it moves through your biliary tract. Doctors use cholescintigraphy to diagnose abnormal contractions of your gallbladder or a blockage in the bile ducts.
Abdominal CT is less sensitive than ultrasound at evaluating stones within the gallbladder. However, CT scans are a common modality used by emergency room physicians for nonspecific severe abdominal pain, which may find gallstones present. Magnetic resonance cholangiopancreatography (MRCP) may be used for better visualization of the biliary tree, especially when evaluating for choledocholithiasis.
Endoscopic retrograde cholangiopancreatography (ERCP) can be used to evaluate for common bile duct stones if all other imaging is equivocal. ERCP is also a therapeutic intervention for choledocholithiasis.
Classic findings on right upper quadrant ultrasound for biliary colic include stones (size may vary) or stone shadow. Findings of pericholecystic fluid, thickened wall (greater than 0.4 cm), and distended gallbladder are more indicative of acute cholecystitis.
Biliary colic treatment
Management of biliary colic is primarily surgical. Medical management of biliary colic involves strict maintenance of a low-fat diet and supportive management with antiemetics and pain control 2. There is no role for antibiotics in biliary colic as there is no infectious etiology, such as in acute cholecystitis or cholangitis 2. Oral ursodeoxycholic acid has also been used to help dissolve gallstones. Surgical intervention with laparoscopic cholecystectomy remains the gold standard. In patients who are poor surgical candidates, extracorporeal shockwave lithotripsy may be considered, but there is a considerable chance of stone recurrence. Open cholecystectomy is a less common approach, used in patients who are not candidates for laparoscopic surgery 13
Endoscopic retrograde cholangiopancreatography (ERCP) is both diagnostic and therapeutic for common bile duct stones. Sphincterotomy of the ampulla of Vater can assist in removing stones after ERCP and prevent future stones from becoming lodged in the common bile duct.
Patients with biliary colic do not necessarily require hospital admission 2. They may be treated symptomatically with a low-fat diet, pain control, and anti-emetics, and follow up for a laparoscopic cholecystectomy as an outpatient within a reasonable time-frame. However, if the patient has severe or intractable abdominal pain, hospital admission, and more urgent surgical management are warranted for symptomatic relief. Other considerations for possible admission include large gallstones. Stones greater than 1 cm in size have a greater propensity to obstruct the cystic duct and may predispose to acute cholecystitis, so they should be treated with surgical management more urgently. If the patient is unable to tolerate anything by mouth (even liquid), admission should be considered.
Surgery
Surgery to remove the gallbladder, called cholecystectomy, is one of the most common operations performed on adults in the United States. The gallbladder is not an essential organ, which means you can live normally without a gallbladder.
A health care professional will usually give you general anesthesia for surgery. Once the surgeon removes your gallbladder, bile flows out of your liver through the hepatic duct and common bile duct and directly into the duodenum, instead of being stored in the gallbladder.
Surgeons perform two types of cholecystectomy:
- Laparoscopic cholecystectomy. Almost all surgeons perform cholecystectomies with laparoscopy. Surgeons perform many laparoscopic cholecystectomies on an outpatient basis, meaning you may be able to go home the same day. You will probably be able to return to normal physical activity in about a week.
- Open cholecystectomy. A surgeon performs an open cholecystectomy when your gallbladder is severely inflamed, infected, or scarred from other operations. Your doctor may perform a cholecystectomy if problems occur during a laparoscopic cholecystectomy. After the surgery, you may need to stay in the hospital for up to a week. You will probably be able to return to normal physical activity after about a month.
What happens after gallbladder removal?
A small number of people have softer and more frequent stools after gallbladder removal, because bile now flows into your duodenum more often. Changes in bowel habits are usually temporary; however, discuss them with your doctor.
All surgeries come with a possible risk of complications; however, gallbladder surgery complications are very rare. The most common complication is injury to the bile ducts, which can cause infection. You may need one or more additional operations to repair the bile ducts.
Nonsurgical treatments
Doctors use nonsurgical treatments for gallstones only in special situations, like if you have cholesterol stones and you have a serious medical condition that prevents surgery. Even with treatment, gallstones can return. Therefore, you may have to be regularly treated for gallstones for a very long time, or even for the rest of your life.
A doctor may use the following types of nonsurgical treatments to remove or break up cholesterol gallstones:
- Endoscopic retrograde cholangiopancreatography (ERCP). Sometimes doctors use ERCP to remove a gallstone that is stuck in the common bile duct.
- Oral dissolution therapy. Ursodiol (Actigall) and chenodiol (Chenix) are medicines that contain bile acids that can break up gallstones. These medicines work best to break up small cholesterol stones. You may need months or years of treatment to break up all stones.
- Shock wave lithotripsy. A doctor can use shock wave lithotripsy to blast gallstones into small pieces. Doctors use this procedure only rarely, and sometimes along with ursodiol.
Biliary colic prognosis
Patients with asymptomatic gallstones become symptomatic at a rate of about 2%/year. The symptom that develops most commonly is biliary colic rather than a major biliary complication. Once biliary symptoms begin, they are likely to recur; pain returns in 20 to 40% of patients/year, and about 1 to 2% of patients/year develop complications such as cholecystitis, choledocholithiasis, cholangitis, and gallstone pancreatitis.
- Biliary Colic. https://www.health.harvard.edu/a_to_z/biliary-colic-a-to-[↩]
- Gossman W, Dayal N, Meseeha M. Biliary Colic. [Updated 2020 Jan 3]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2020 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK430772[↩][↩][↩][↩]
- Hedström J, Nilsson J, Andersson R, Andersson B. Changing management of gallstone-related disease in pregnancy – a retrospective cohort analysis. Scand. J. Gastroenterol. 2017 Sep;52(9):1016-1021.[↩]
- Cholelithiasis. https://www.merckmanuals.com/professional/hepatic-and-biliary-disorders/gallbladder-and-bile-duct-disorders/cholelithiasis?query=biliary%20colic[↩]
- Baiu I, Hawn MT. Gallstones and Biliary Colic. JAMA. 2018 Oct 16;320(15):1612.[↩]
- Portincasa P, Wang DQ-H. Gallstones. In: Podolsky, DK, Camilleri M, Fitz JG, Kalloo, AN, Shanahan F, Wang, TC, eds. Yamada’s Textbook of Gastroenterology. Volume 2. 6th edition. Hoboken, NJ: Wiley-Blackwell; 2015:1808–1834.[↩]
- Jensen MD, Ryan DH, Apovian CM, et al. American College of Cardiology/American Heart Association Task Force on Practice Guidelines; Obesity Society. 2013 AHA/ACC/TOS guideline for the management of overweight and obesity in adults: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and The Obesity Society. Circulation. 2014 Jun 24;129(25 Suppl 2):S102-38. doi: 10.1161/01.cir.0000437739.71477.ee. Epub 2013 Nov 12. Erratum in: Circulation. 2014 Jun 24;129(25 Suppl 2):S139-40.[↩]
- U.S. Department of Health and Human Services, Office of Disease Prevention and Health Promotion. Physical Activity Guidelines for Americans, 2nd edition. Washington, DC: U.S. Department of Health and Human Services; 2019. https://health.gov/sites/default/files/2019-09/Physical_Activity_Guidelines_2nd_edition.pdf[↩]
- Acalculous Biliary Pain. https://www.merckmanuals.com/professional/hepatic-and-biliary-disorders/gallbladder-and-bile-duct-disorders/acalculous-biliary-pain?query=biliary%20colic[↩]
- Saurabh S, Green B. Is hyperkinetic gallbladder an indication for cholecystectomy? Surg Endosc. 2019 May;33(5):1613-1617.[↩]
- Tsai TJ, Chan HH, Lai KH, Shih CA, Kao SS, Sun WC, Wang EM, Tsai WL, Lin KH, Yu HC, Chen WC, Wang HM, Tsay FW, Lin HS, Cheng JS, Hsu PI. Gallbladder function predicts subsequent biliary complications in patients with common bile duct stones after endoscopic treatment? BMC Gastroenterol. 2018 Feb 27;18(1):32.[↩]
- Naim H, Hasan SA, Khalid S, Abbass A, DSouza J. Clinical Cholecystitis in the Absence of the Gallbladder. Cureus. 2017 Nov 10;9(11):e1834[↩]
- Demehri FR, Alam HB. Evidence-Based Management of Common Gallstone-Related Emergencies. J Intensive Care Med. 2016 Jan;31(1):3-13.[↩]





{kind=link}