Contents
What is blastocystis
Blastocystis is a common microscopic organism that inhabits the intestine and is found throughout the world. A full understanding of the biology of Blastocystis and its relationship to other organisms is not clear, but is an active area of research 1. Infection with Blastocystis is called blastocystosis. Blastocystis hominis can be found in healthy people who aren’t having digestive symptoms, and it’s also sometimes found in the stools of people who have diarrhea, abdominal pain or other gastrointestinal problems. Researchers don’t fully understand the role Blastocystis hominis plays, if any, in causing disease. Certain forms of the organism might be more likely to be linked to an infection with symptoms. Most commonly, blastocystis simply lives in a person’s digestive tract without causing harm.
Blastocystis hominis, also known as blastocystis spp or Blastocystis hominis infection, usually clears on its own. The taxonomic classification of Blastocystis hominis is mired in controversy. It has been previously considered as yeasts, fungi, or ameboid, flagellated, or sporozoan protozoa 2. Recently, however, based on molecular studies, especially dealing with the sequence information on the complete SSUrRNA gene, Blastocystis hominis has been placed within an informal group, the stramenopiles 3. Stramenopiles are defined, based on molecular phylogenies, as a heterogeneous evolutionary assemblage of unicellular and multicellular protists including brown algae, diatoms, chrysophytes, water molds, slime nets, etc. 4. Cavalier-Smith 5 considers stramenopiles to be identical to his infrakingdom Heterokonta under the kingdom Chromista. Therefore, according to Cavalier-Smith 5, Blastocystis hominis is a heterokontid chromista.
Blastocystis is a polymorphic protozoan, and four major forms have been described in the literature 6. In reality, Blastocystis species can present with a bewildering array of forms within a single culture, and it may be difficult to assign a specific form to the cell in question (Figure 1A and C). The extensive variation in Blastocystis forms has made studies of its cell biology challenging, resulting in misinterpretations of data from time to time.
Figure 1. Blastocystis parasite morphological forms
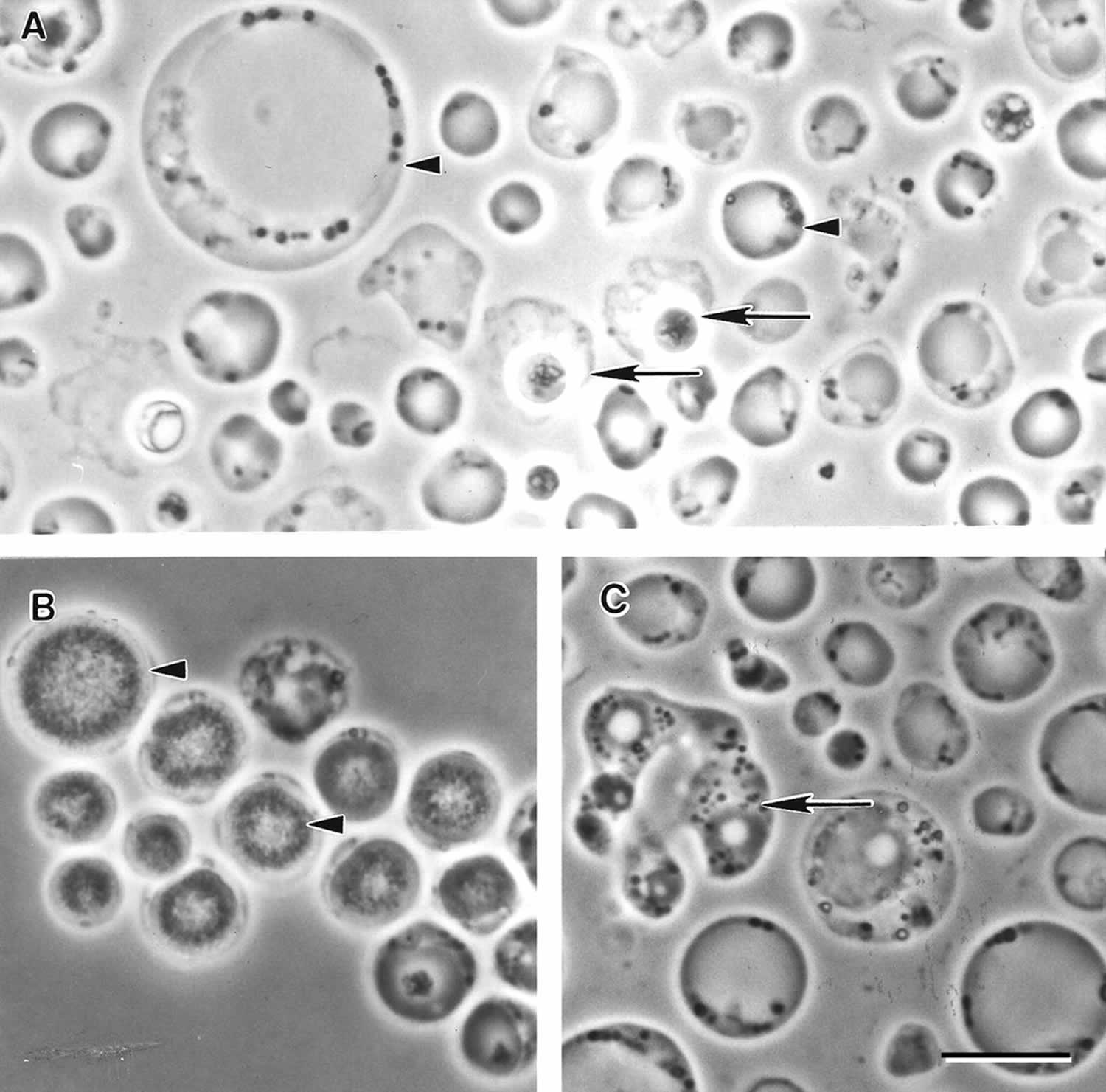
Footnote: Morphological forms of Blastocystis sp. subtype 4 by phase-contrast microscopy. (A) Vacuolar and fecal cyst forms from in vitro axenic culture displaying extensive size variation (arrowheads). Note the refractile appearance and loose outer coat of cysts (arrows). (B) Granular form with distinct granular inclusions within the central vacuole (arrowhead). (C) Amoeboid forms occasionally seen in culture showing pseudopod-like cytoplasmic extensions (arrow). Bar, 10 μm.
[Source 6 ]What should I do if I think I have blastocystosis?
See your health care provider who will ask you to provide stool samples for testing. Diagnosis may be difficult, so you may be asked to submit several stool samples.
Is medication available to treat blastocystosis?
Yes. Drugs are available by prescription to treat blastocystosis. However, sometimes medication is not effective, and a search for other possible causes of your symptoms may be necessary.
Is having blastocystosis common?
Yes. In fact, many people have Blastocystis in their intestine, some without ever having symptoms.
How long will I be infected?
Blastocystis can remain in the intestine for weeks, months, or years.
Blastocystis hominis life cycle
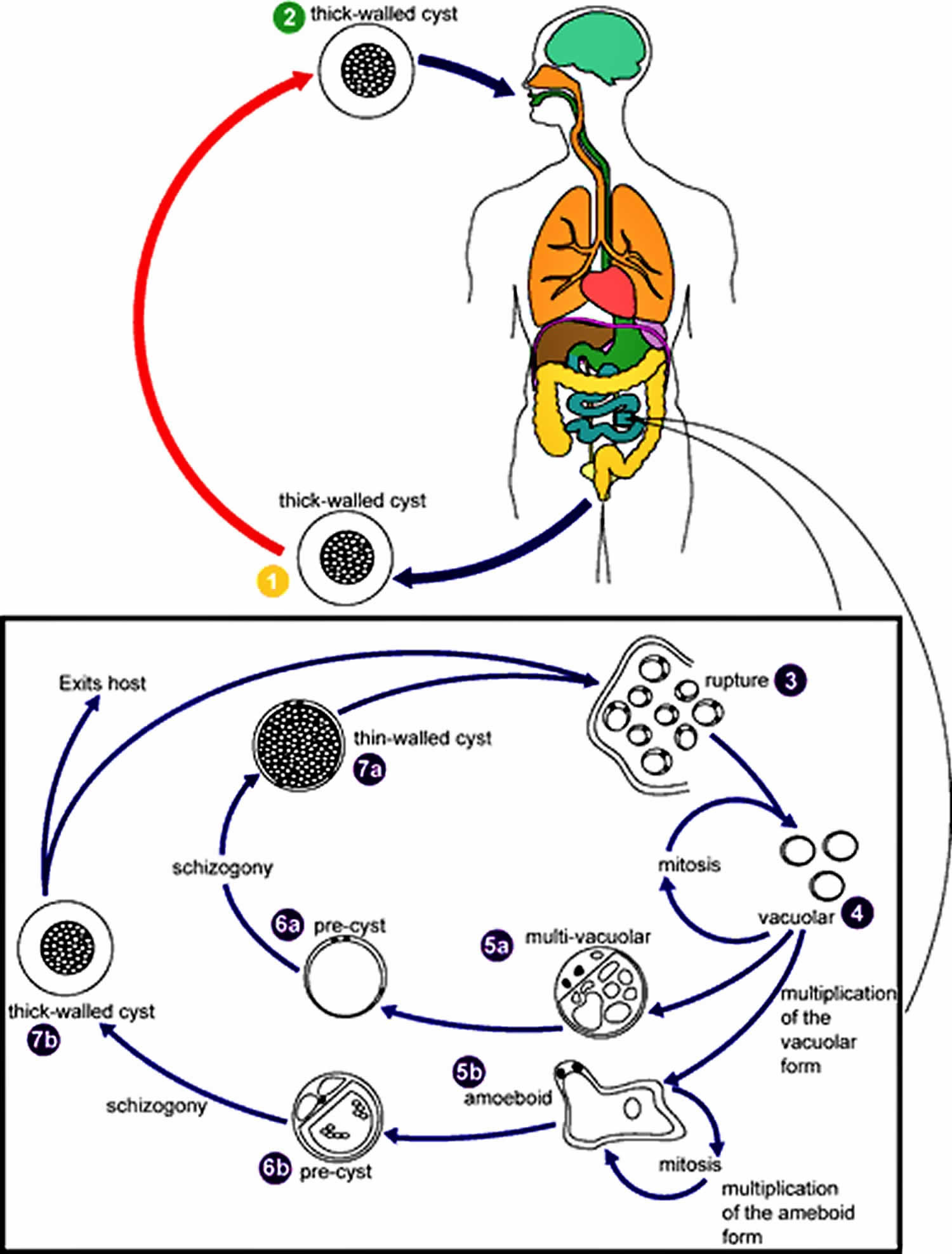
Blastocystis hominis life cycle and transmission is still under investigation, therefore this is a proposed life cycle for Blastocystis hominis. The classic form found in human stools is the cyst, which varies tremendously in size from 6 to 40 µm (#1). The thick-walled cyst present in the stools (#1) is believed to be responsible for external transmission, possibly by the fecal-oral route through ingestion of contaminated water or food (#2). The cysts infect epithelial cells of the digestive tract and multiply asexually (#3 and #4 ). Vacuolar forms of the parasite give origin to multi vacuolar (#5a) and ameboid forms (#5b). The multi-vacuolar develops into a pre-cyst (#6a) that gives origin to a thin-walled cyst (#7a), thought to be responsible for autoinfection. The ameboid form gives origin to a pre-cyst (#6b), which develops into thick-walled cyst by schizogony (#7b). The thick-walled cyst is excreted in feces (#1).
Figure 2. Blastocystis hominis life cycle
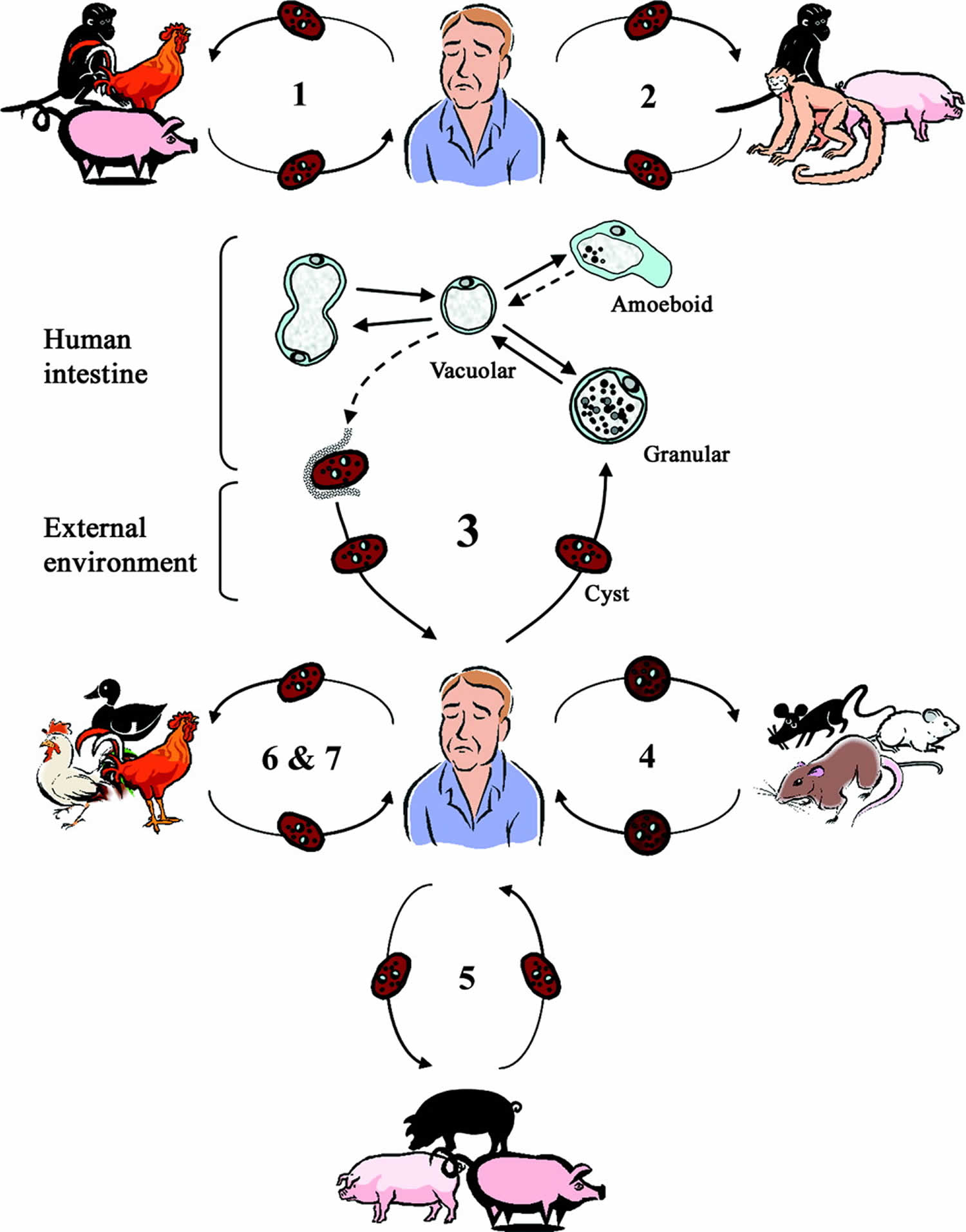
Proposed life cycle for Blastocystis cells taking into account recent studies 7, 8, suggesting the existence of zoonotic genotypes (subtypes 1 to 7) with various host specificities. Humans and animals are infected by fecal cysts, which develop into vacuolar forms in the large intestines. In humans, vacuolar forms divide by binary fission and may develop into amoeboid or granular forms. Vacuolar forms undergo encystation in the host intestines, and intermediate cyst forms may be surrounded by a thick fibrillar layer that is subsequently lost during passage in the external environment. Information on the transition from the amoeboid to the vacuolar form and from the vacuolar to the cyst form is lacking. These hypothetical pathways are represented by dotted lines. Subtype 1 is cross-infective among mammalian and avian isolates; subtypes 2, 3, 4, and 5 comprise primate/pig, human, cattle/pig, and rodent isolates, respectively; and subtypes 6 and 7 include avian isolates. The proposed scheme suggests that humans are potentially infected by seven or more species of Blastocystis and that certain animals represent reservoirs for transmission to humans.
Figure 3. Proposed life cycle for Blastocystis cells taking into account recent studies
Blastocystis hominis causes
Blastocystis is a parasite — a microscopic single-celled organism (protozoan). Many protozoans normally live in your gastrointestinal tract and are harmless or even helpful; others cause disease. The role of Blastocystis in causing disease is controversial among experts. Some types of Blastocystis may be more likely to be associated with symptoms. Finding Blastocystis in stool samples should be followed up with a careful search for other possible causes of your symptoms.
Most people who carry Blastocystis have no signs or symptoms, but it’s also found in people who have diarrhea and other digestive problems. Blastocystis often appears with other organisms, so it’s not known whether it causes disease.
Experts suspect that blastocystis gets into the digestive system when people eat contaminated food or are exposed to the stool of a contaminated person, such as when changing a diaper in a child care setting. Rates of the organism in stool increase where there’s inadequate sanitation and poor personal hygiene.
Risk factors for Blastocystis hominis
Blastocystis hominis is common, and anyone can have the organism in his or her stools. You might be at higher risk if you travel or live where sanitation is inadequate or where the water might not be safe or if you handle contaminated animals, such as pigs and poultry.
How did people get blastocystosis?
How Blastocystis is transmitted is not known for certain, although the number of people infected seems to increase in areas where sanitation and personal hygiene is not adequate. Studies have suggested that risk of infection may increase through:
- ingesting contaminated food or water,
- exposure to a day care environment, or
- exposure to animals.
Blastocystis prevention
You might be able to prevent Blastocystis hominis or other gastrointestinal infection by taking precautions, especially while traveling in high-risk countries.
- Wash your hands with soap and warm water after using the toilet, changing diapers, and before handling food.
- Teach children the importance of washing hands to prevent infection.
- Avoid water or food that may be contaminated.
- Wash and peel all raw vegetables and fruits before eating.
- When traveling in countries where the water supply may be unsafe, avoid drinking unboiled tap water and avoid uncooked foods washed with unboiled tap water. Bottled or canned carbonated beverages, seltzers, pasteurized fruit drinks, and steaming hot coffee and tea are safe to drink.
Watch what you eat
The general rule of thumb is this: If you can’t boil it, cook it or peel it — forget it.
- Avoid food from street vendors.
- Don’t eat soft-cooked eggs.
- Avoid unpasteurized milk and dairy products, including ice cream.
- Avoid raw or undercooked meat, fish and shellfish.
- Steer clear of moist food at room temperature, such as sauces and buffet offerings.
- Eat foods that are well-cooked and served hot.
- Stick to fruits and vegetables that you can peel yourself, such as bananas, oranges and avocados. Stay away from salads and fruits you can’t easily peel, such as grapes and berries.
- Avoid frozen pops and flavored ice.
- Skip salsa and other condiments made with fresh ingredients.
Don’t drink the water
When visiting high-risk countries, keep the following tips in mind:
- Avoid unsterilized water — from tap, well or stream. If you need to drink or wash fruits or vegetables in local water, boil it for at least three minutes and let it cool to room temperature.
- Avoid ice cubes or fruit juices made with tap water.
- Keep your mouth closed while showering.
- Use bottled water to brush your teeth.
- Make sure hot beverages, such as coffee or tea, are steaming hot.
Feel free to drink canned or bottled drinks in their original containers — including water, carbonated beverages, beer or wine — as long as you break the seals on the containers yourself. Wipe off any can or bottle before drinking or pouring.
You can chemically disinfect water with iodine or chlorine. Iodine tends to be more effective, but limit its use, because too much iodine can be harmful to your body.
Take precautions against passing a parasite to others
If you have Blastocystis hominis or another gastrointestinal infection, good personal hygiene can help keep you from spreading the infection to others:
- Wash hands with soap and water frequently, especially after using the toilet and before, during and after handling food. Rub soapy, wet hands together for at least 20 seconds before rinsing. Lather the backs of your hands and between your fingers. Dry your hands well with a clean towel. If soap and water aren’t available, use an alcohol-based hand sanitizer that contains at least 60 percent alcohol.
- Wash hands well after changing a diaper, especially if you work in a child care center, even if you wear gloves.
Should I be concerned about spreading infection to the rest of my household?
There is little risk of spreading infection if you practice adequate personal hygiene. This includes thorough hand washing with soap and warm water after using the toilet and before handling food.
Blastocystis hominis symptoms
Whether Blastocystis hominis can cause symptomatic infection in humans is a point of active debate. This is because of the common occurrence of the organism in both asymptomatic and symptomatic persons. Those who believe symptoms could be related to infection with this parasite have described a spectrum of illness including watery diarrhea, abdominal pain, anal itching, weight loss, constipation, and excessive flatulence 2. Many people have no symptoms at all.
Signs and symptoms possibly associated with Blastocystis hominis include:
- Watery diarrhea
- Nausea
- Abdominal pain
- Bloating
- Excessive gas (flatulence)
- Loss of appetite
- Fatigue
See your doctor if you have signs and symptoms, such as diarrhea or cramps, that last longer than three days.
Blastocystis hominis laboratory diagnosis
The cause of your diarrhea might be difficult to diagnose. Even if Blastocystis hominis is found in your stool, it might not be causing your symptoms. More commonly, it suggests you’ve been exposed to contaminated food or water that contains other organisms that can cause gastrointestinal symptoms.
Your doctor likely will take your medical history, ask you about recent activities, such as traveling, and perform a physical exam. A number of lab tests help diagnose parasitic diseases and other noninfectious causes of gastrointestinal symptoms:
- Stool (fecal) exam. This test looks for parasites or their eggs. Your doctor might give you a special container with preservative fluid for your stool samples. Refrigerate — don’t freeze — your samples until you take them to your doctor’s office or lab.
- Endoscopy. If you have symptoms, but the fecal exam doesn’t reveal the cause, your doctor might request this test. After you’re sedated, a doctor, usually a gastroenterologist, inserts a tube into your mouth or rectum to look for the cause of your symptoms. You’ll need to fast beginning the night before the test.
- Blood tests. A blood test that can detect blastocystis is available but not commonly used. However, your doctor might order blood tests to look for other causes of your signs and symptoms.
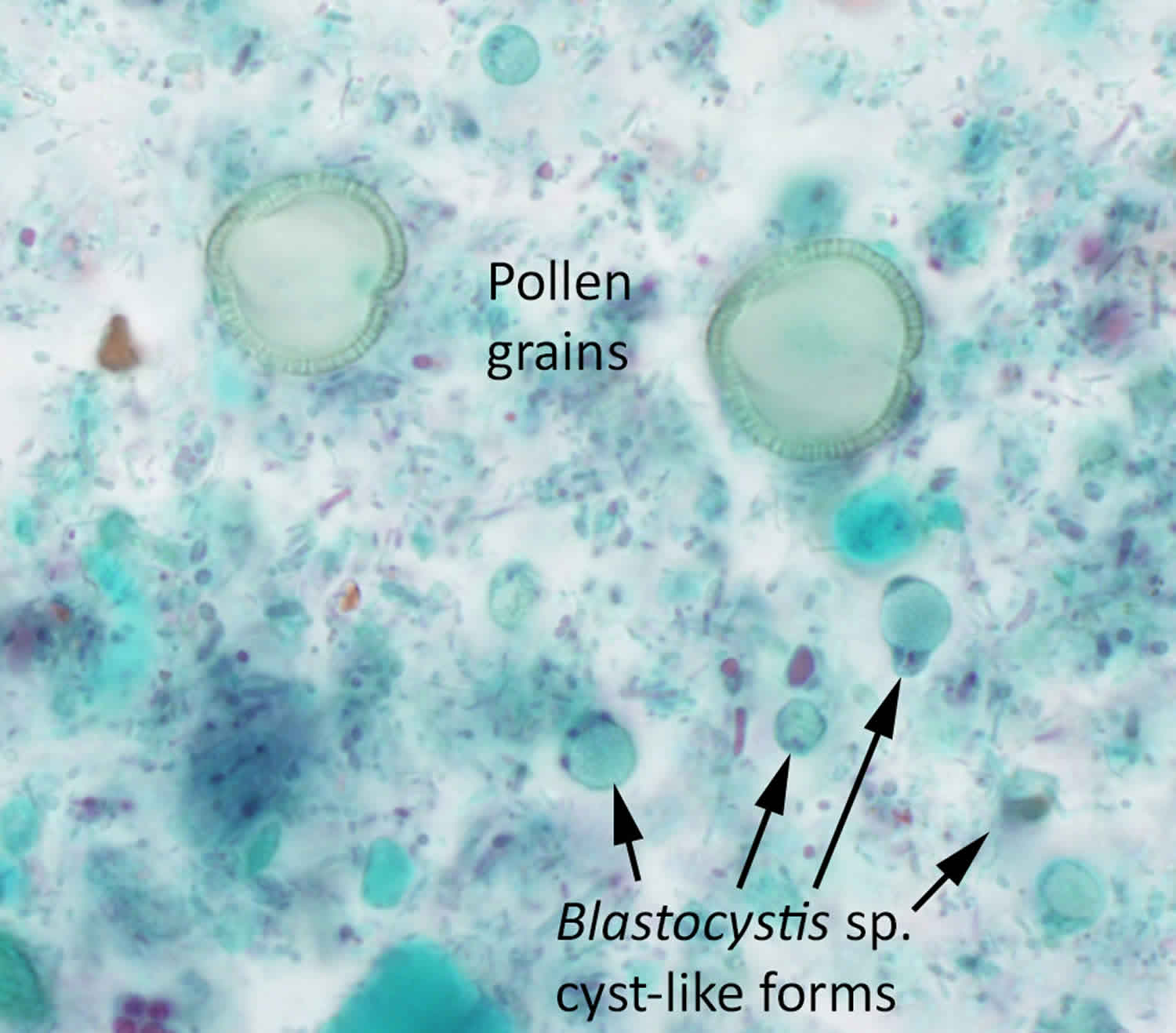
Blastocystis hominis diagnosis is based on finding the cyst-like stage in feces. Permanently stained smears are preferred over wet mount preparations because fecal debris may be mistaken for the organisms in the latter. Do not wash specimens in water (e.g., during concentration procedures) as this will lyse the organisms, resulting in false negatives.
Basic guidelines:
- A. Multiple stool samples (at least 3) should be tested before a negative result is reported.
- B. To maximize recovery of cyst-like forms, stool samples in formalin, or other fixatives, should be concentrated prior to microscopic examination (e.g., 10 min at 500 × g when using the formalinethyl-acetate concentration procedure).
- C. Choice of diagnostic techniques depends on available equipment and reagents, experience, and considerations of time and cost.
1. Wet mount
Blastocystis hominis is not easily seen in concentrated wet mount preparations. It is generally round and measures approximately 6 to 40 μm. Cyst-like forms have a large central body that looks like a large vacuole surrounded by small, multiple nuclei.
2. Trichrome stain
In trichrome stained smears, the large central body is usually green to gray in color. The inclusion bodies in the cytoplasm stain bright to dark red. Because of its uncertain pathogenicity, Blastocystis hominis should be reported when found in stool specimens.
Blastocystis treatment
The clinical significance of Blastocystis species is controversial 9. If you have Blastocystis hominis without signs or symptoms, then you don’t need treatment. Mild signs and symptoms might improve on their own within a few days.
Potential medications for treating Blastocystis hominis include:
- Antibiotics, such as metronidazole (Flagyl) or tinidazole (Tindamax)
- Combination medications, such as sulfamethoxazole and trimethoprim (Bactrim, Septra, others)
- Anti-protozoal medications, such as paromomycin or nitazoxanide (Alinia)
Response to medication for Blastocystis hominis varies greatly from person to person. And because the organism might not be the cause of your symptoms, improvement might be due to the medication’s effect on another organism.
Treatment with metronidazole* at various doses has been reported, for example (adults):
- 250 mg to 750 mg metronidazole* orally 3 times daily for 10 days
- 1500 mg metronidazole* orally once daily for 10 days
Lack of response to metronidazole has been noted in some areas 10.
NOTE: *Not FDA-approved for this indication.
Treatment with trimethoprim (TMP)*/sulfamethoxazole (SMX)* at various doses has been reported, for example (adults):
- 6 mg/kg trimethoprim*, 30 mg/kg sulfamethoxazole* once daily for 7 days
- 320mg trimethoprim*, 1600 mg sulfamethoxazole* once daily for 7 days
- 160 mg trimethoprim*, 800 mg sulfamethoxazole* twice daily for 7 days
NOTE: *Not FDA-approved for this indication.
Treatment with nitazoxanide* has been shown to be effective in clearing organisms and improving symptoms at the following doses:
- Adults, 500 mg nitazoxanide* orally twice daily for 3 days.
- Children, 200 mg nitazoxanide* orally twice daily for 3 days in patients aged 4–11 years, and 100 mg nitazoxanide* orally twice daily for 3 days in patients aged 1–3 years.
Tinidazole*, paromomycin*, iodoquinol*, and ketoconazole* have also been used for clearing Blastocystis, as presented in case reports or small series.
NOTE: *Not FDA-approved for this indication.
Metronidazole
- Note on Treatment in Pregnancy
- Metronidazole is in pregnancy category B. Data on the use of metronidazole in pregnant women are conflicting. The available evidence suggests use during pregnancy has a low risk of congenital anomalies. Metronidazole may be used during pregnancy in those patients who will clearly benefit from the drug, although its use should be weighed against any potential risks.
- Pregnancy Category B: Either animal-reproduction studies have not demonstrated a fetal risk but there are no controlled studies in pregnant women or animal-reproduction studies have shown an adverse effect (other than a decrease in fertility) that was not confirmed in controlled studies in women in the first trimester (and there is no evidence of a risk in later trimesters).
- Note on Treatment During Lactation
- Metronidazole is excreted in breast milk. The American Academy of Pediatrics classifies metronidazole as a drug for which the effect on nursing infants is unknown but may be of concern. The World Health Organization (WHO) advises to avoid metronidazole treatment in lactating women. Metronidazole should be used during lactation only if the potential benefit of therapy to the mother justifies the potential risk to the infant.
- Note on Treatment in Pediatric Patients
- The safety of metronidazole in children has not been established. Metronidazole is listed as an antiamebic and antigiardiasis medicine on the WHO Model List of Essential Medicines for Children, intended for the use of children up to 12 years of age.
Trimethoprim–sulfamethoxazole
- Note on Treatment in Pregnancy
- Trimethoprim–sulfamethoxazole (TMP–SMX) is in pregnancy category C. TMP–SMX should be used during pregnancy only if the potential benefit justifies the potential risk to the fetus. TMP-SMX should be avoided near-term because of the potential for hyperbilirubinemia and kernicterus in the newborn.
- Pregnancy Category C: Either studies in animals have revealed adverse effects on the fetus (teratogenic or embryocidal, or other) and there are no controlled studies in women or studies in women and animals are not available. Drugs should be given only if the potential benefit justifies the potential risk to the fetus.
- Note on Treatment During Lactation
- Trimethoprim–sulfamethoxazole (TMP–SMX) is excreted in breast milk. TMP–SMX generally is compatible with breastfeeding of healthy, full-term infants after the newborn period. However, TMP-SMX generally should be avoided by women when nursing infants who are premature, jaundiced, ill, or stressed, or who have glucose-6-phosphate dehydrogenase deficiency.
- Note on Treatment in Pediatric Patients
- The safety of trimethoprim–sulfamethoxazole (TMP–SMX) in children has not been systematically evaluated. Use in children less than 2 months of age generally is not recommended.
Nitazoxanide
- Note on Treatment in Pregnancy
- Nitazoxanide is in pregnancy category B. Data on the use of nitazoxanide in pregnant women are limited, and risk to the embryo-fetus is unknown. Nitazoxanide should be used during pregnancy only if the potential benefit justifies the potential risk to the fetus.
- Pregnancy Category B: Either animal-reproduction studies have not demonstrated a fetal risk but there are no controlled studies in pregnant women or animal-reproduction studies have shown an adverse effect (other than a decrease in fertility) that was not confirmed in controlled studies in women in the first trimester (and there is no evidence of a risk in later trimesters).
- Note on Treatment During Lactation
- It is not known whether nitazoxanide is excreted in breast milk. Nitazoxanide should be used with caution in breastfeeding women.
- Note on Treatment in Pediatric Patients
- Nitazoxanide tablets should not be used in children age 11 years or younger as a single tablet contains a greater dose than recommended for pediatric dosing. Nitazoxanide oral suspension may be used for dosing in children, although the safety in children age 1 and younger is not certain.
Paromomycin
- Note on Treatment in Pregnancy
- Oral paromomycin has not been assigned to a pregnancy category by the Food and Drug Administration. Data on the use of oral paromomycin in pregnant women are limited, and the risk to the embryo-fetus probably is low. Oral paromomycin generally is poorly absorbed from the gastrointestinal tract, with minimal, if any, systemic availability.
- Note on Treatment During Lactation
- Oral paromomycin is unlikely to be excreted in breast milk, and the drug generally is poorly absorbed from the gastrointestinal tract.
- Note on Treatment in Pediatric Patients
- The safety of oral paromomycin in children has not been formally evaluated. However, the safety profiles likely are comparable in children and adults.
Iodoquinol
- Note on Treatment in Pregnancy
- Oral iodoquinol has not been assigned a pregnancy category by the Food and Drug Administration. Data on the use of iodoquinol in pregnant women are limited, and risk to the embryo-fetus is unknown. Iodoquinol should be used during pregnancy only if the potential benefit justifies the potential risk to the fetus.
- Note on Treatment During Lactation
- It is not known whether iodoquinol is excreted in breast milk. Iodoquinol should be used with caution in breastfeeding women.
- Note on Treatment in Pediatric Patients
- The safety of iodoquinol in children has not been established.
Ketoconazole
- Note on Treatment in Pregnancy
- Ketoconazole is in pregnancy category C. Data on the use of ketoconazole in pregnant women are limited, and the risk to the embryo-fetus is unknown. Ketoconazole should be used during pregnancy only if the potential benefit justifies the potential risk to the fetus.
- Pregnancy Category C: Either studies in animals have revealed adverse effects on the fetus (teratogenic or embryocidal, or other) and there are no controlled studies in women or studies in women and animals are not available. Drugs should be given only if the potential benefit justifies the potential risk to the fetus.
- Note on Treatment During Lactation
- According to a case report, ketoconazole was excreted in breast milk and the nursing infant did not have adverse effects. The American Academy of Pediatrics classifies ketoconazole as compatible with breastfeeding.
- Note on Treatment in Pediatric Patients
- The safety of ketoconazole has not been evaluated systematically for children of any age, and essentially no data are available about its use in children less than 2 years of age. Ketoconazole should not be used in children unless the potential benefit outweighs the risks.
- Parasites – Blastocystis spp. infection. https://www.cdc.gov/parasites/blastocystis/[↩]
- Blastocystis hominis. https://www.cdc.gov/dpdx/blastocystis/index.html[↩][↩][↩]
- Silberman JD, Sogin ML, Leipe DD, Clark CG. Human parasite finds taxonomic home. Nature 1996;380:398.[↩]
- Patterson DJ. Protozoa, evolution and systematics. In: Housmann K, Hulsmann N, editors. Progress in Protozoology. Stuttgart: Fischer; 1994. p. 1-14.[↩]
- Cavalier-Smith T. A revised six-kingdom system of life. Biol Rev Camb Philos Soc 1998;73:203-266.[↩][↩]
- New Insights on Classification, Identification, and Clinical Relevance of Blastocystis spp. Kevin S. W. Tan. Clinical Microbiology Reviews Oct 2008, 21 (4) 639-665; DOI: 10.1128/CMR.00022-08 https://cmr.asm.org/content/21/4/639[↩][↩][↩]
- Navarro, C., M. V. Domínguez-Márquez, M. M. Garijo-Toledo, S. Vega-García, S. Fernández-Barredo, M. T. Pérez-Gracia, A. García, R. Borrás, and M. T. Gómez-Muñoz. 2008. High prevalence of Blastocystis sp. in pigs reared under intensive growing systems: frequency of ribotypes and associated risk factors. Vet. Parasitol. 153:347-358.[↩]
- Noël, C., F. Dufernez, D. Gerbod, V. P. Edgcomb, P. Delgado-Viscogliosi, L. C. Ho, M. Singh, R. Wintjens, M. L. Sogin, M. Capron, R. Pierce, L. Zenner, and E. Viscogliosi. 2005. Molecular phylogenies of Blastocystis isolates from different hosts: implications for genetic diversity, identification of species, and zoonosis. J. Clin. Microbiol. 43:348-355.[↩]
- Parasites – Blastocystis spp. infection. https://www.cdc.gov/parasites/blastocystis/health_professionals/index.html[↩]
- Yakoob et al., Br J Biomed Sci 2004;61:75[↩]





{kind=link}