
Contents
What is brachycephaly
Brachycephaly or short skull is usually as a result of baby spending a lot of time lying on their back. The skull is made up of plates of bone that strengthen and join together as a child gets older. Brachycephaly is defined by a skull shape where the cephalic ratio [biparietal diameter (width) to occipitofrontal diameter (length)] ratio of over 90%.
A young baby’s skull is still relatively soft and can change shape if there’s constant pressure on a particular part of their head.
Brachycephaly is quite common, affecting around 1 in every 5 babies at some point.
In most cases brachycephaly isn’t a major cause for concern, as it doesn’t have any effect on the brain and the head shape will often improve by itself over time.
Your baby won’t experience any pain or other symptoms, or any problems with their general development.
Brachycephaly quick facts:
- Brachycephaly is the most common type of skull deformity in infants
- Back of head is flat instead of rounded
- Normally noticed by caregivers at about six to 10 weeks of age
- Head is abnormally wide and tall.
- Unilateral occipital flattening
- Ear is positioned more anterior on the side of the occipital flattening (tips of ears protrude)
- Forehead may be asymmetrical and is positioned more anterior on the side of the occipital flattening
- Facial asymmetry may be present. Face appears small compared to size of head
- May be accompanied by torticollis, limited neck range of motion, weakness and preferential head positioning
Brachycephaly in rare cases can be caused by the premature fusion of both coronal sutures, causing a shortened front-to-back diameter of the skull. The skull grows vertically and laterally leading to a high and wide skull shape. The coronal suture is the fibrous joint that unites the frontal bone with the two parietal bones of the skull. The parietal bones form the top and sides of the skull (see Figure 1). Coronal suture extends from ear to ear. Each frontal bone plate meets with a parietal bone plate at the coronal suture.
Sutures (metopic suture, coronal suture, sagittal suture and lambdoid sutures) allow the skull bones to move during the birth process. Sutures act like an expansion joint, allowing the bone to enlarge evenly as the brain grows and the skull expands, resulting in a symmetrically shaped head. However, if any of the sutures close too early (fuse prematurely), there may be no growth in that area. This may force growth to occur in another area or direction, resulting in an abnormal head shape.
Figure 1. Newborn skull
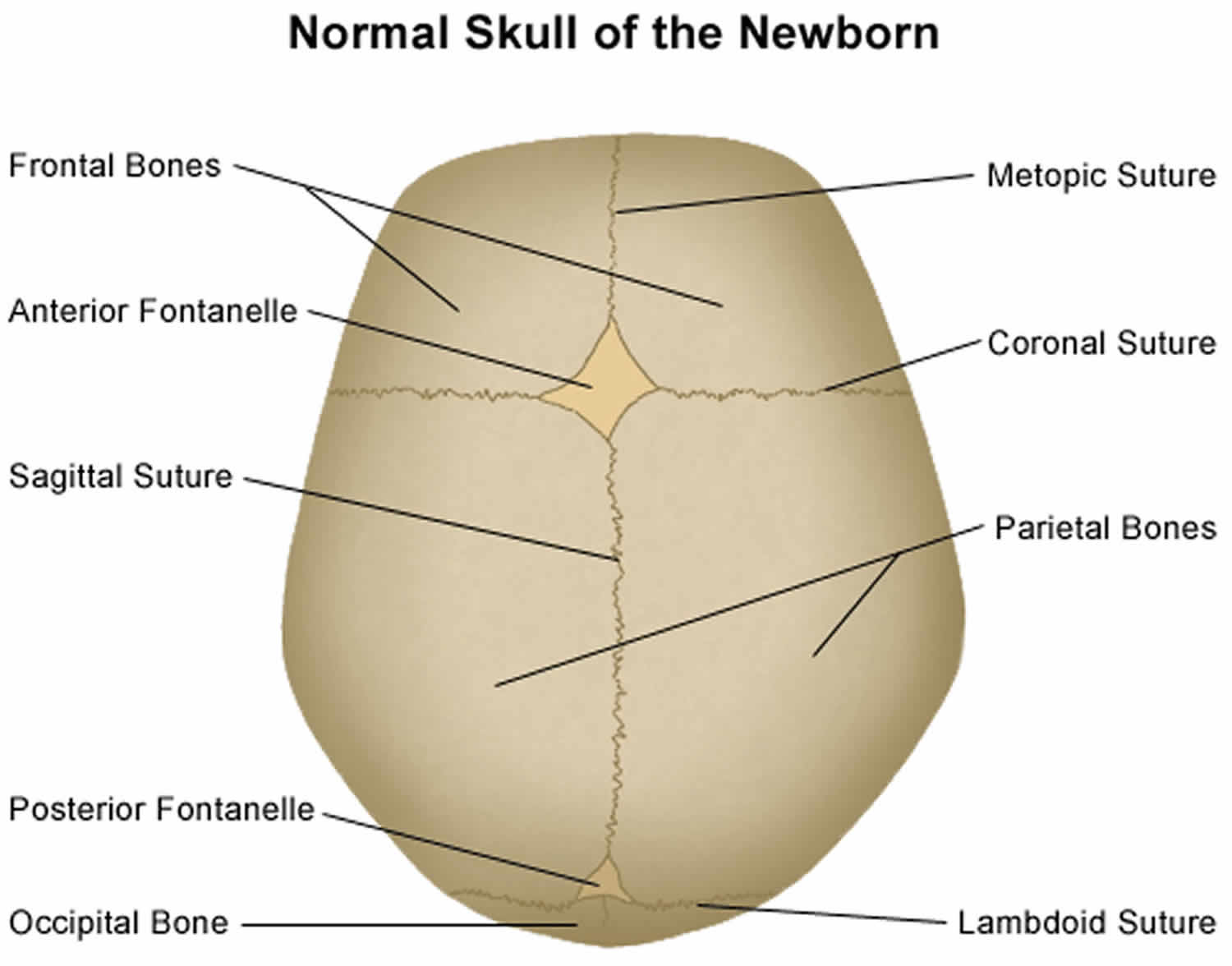
Footnote: The skull consists of five thin, curved, bony plates that are held together by fibrous material called sutures. These sutures allow a baby’s skull to expand with the growing brain. The sutures gradually harden to join the skull bones together. The spaces where sutures meet are called soft spots or fontanelles.
Speak to your health visitor or doctor if you’re concerned about the shape of your baby’s head or think they may have problems turning their head.
They can examine your baby’s head and suggest things you can do to help.
A slightly flattened head isn’t usually anything to worry about, but it’s a good idea to get advice early on so you can take steps to stop it getting any worse.
Figure 2. Brachycephaly baby

Figure 3. Brachycephaly skull measurement (measurement of biparietal diameter [A] and the occipitofrontal diameter [B])
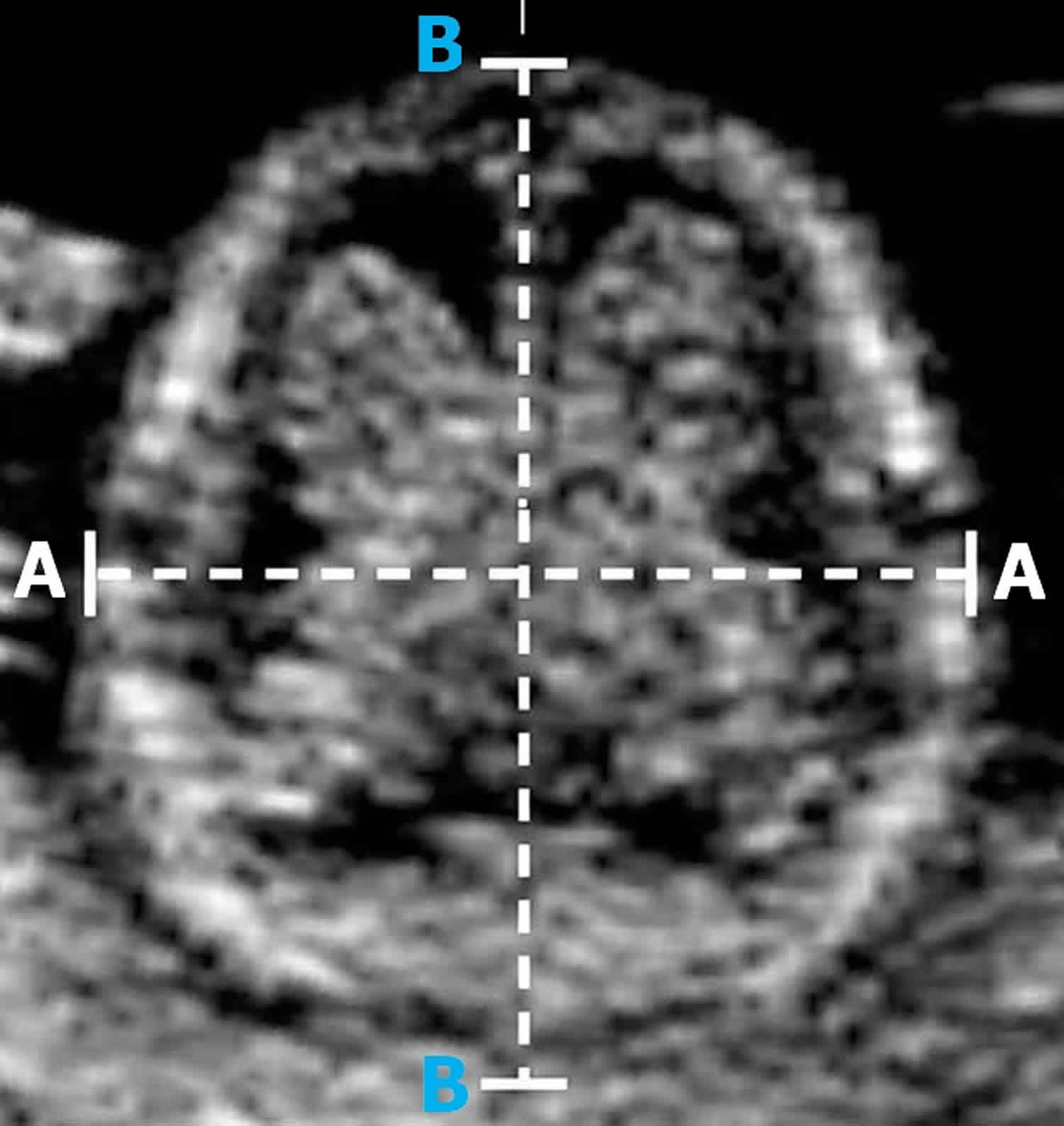
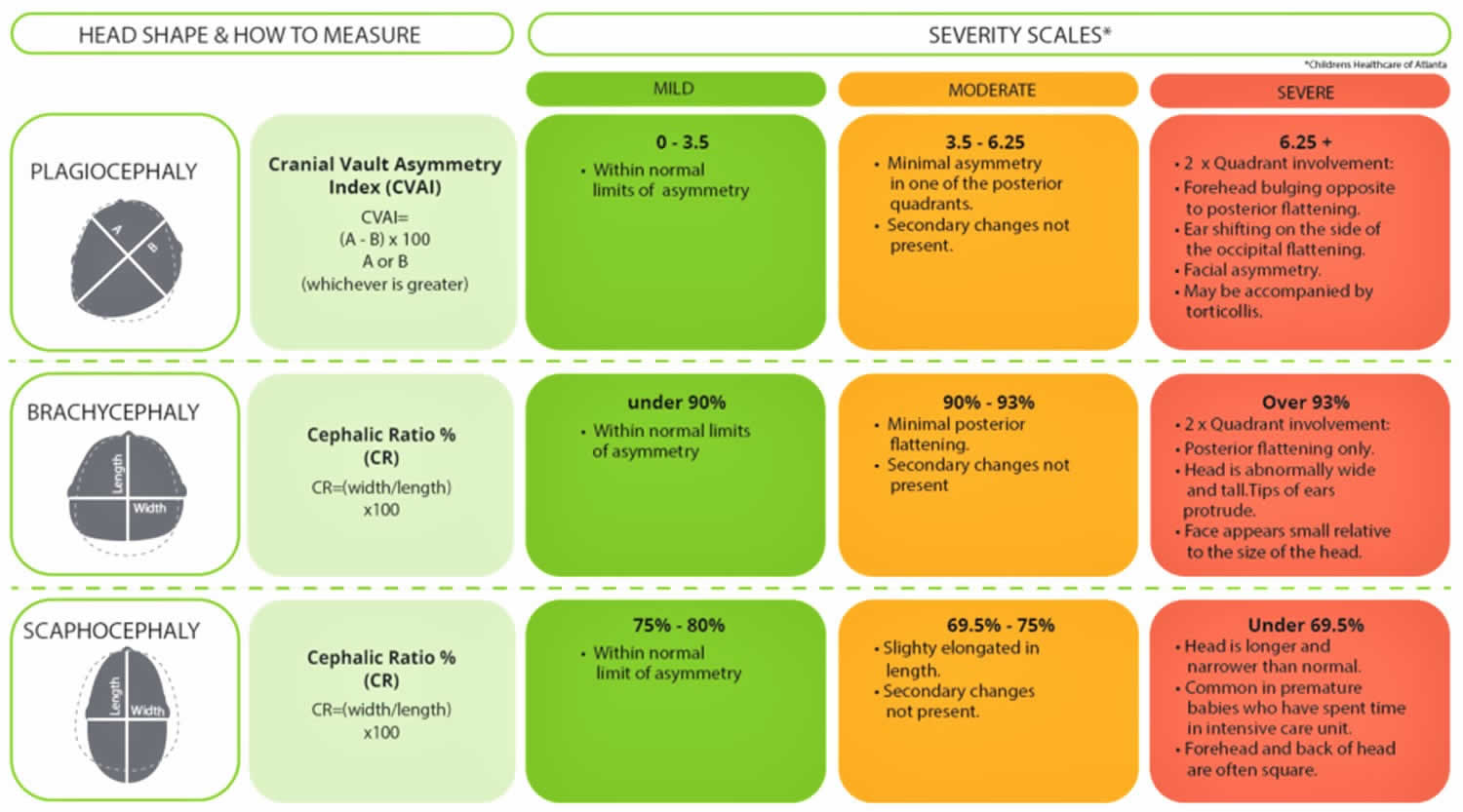
Figure 4. Brachycephaly severity scale
Will my baby’s head shape return to normal?
Mild flattening of the head will usually improve if you use the simple measures described below, although it may be a couple of months before you start to notice an improvement.
Your baby’s head may not return to a completely perfect shape, but by the time they’re 1 or 2 years old any flattening will be barely noticeable.
More severe flat head syndrome cases will also get better over time, although some flattening will usually remain.
The appearance of your child’s head should improve as they become more mobile and their hair grows.
It’s very rare for a child to experience problems such as teasing when they reach school age.
You may consider using a helmet or headband if you’re worried about your child, but it’s not clear whether these always work.
You should also bear in mind the inconvenience, expense and possible discomfort for you and your child.
Brachycephaly causes
The skull is made up of plates of bone that strengthen and join together as a child gets older.
A young baby’s skull is still relatively soft and can change shape if there’s constant pressure on a particular part of their head.
Reasons why flat head syndrome may happen in babies include:
- Sleeping on their back – the back or side of a baby’s head can become flattened as a result of always sleeping on their back, but it’s important they do this to reduce the risk of sudden infant death syndrome (SIDS)
- Problems in the womb – pressure can be placed on a baby’s head before it’s born if they’re a bit squashed in the womb or there’s a lack of amniotic fluid to cushion them
- Being born prematurely – premature babies are more likely to develop a flattened head because their skull is softer when they’re born, and they may prefer to rest their head on 1 side at first as they’re not yet able to move their head themselves
- Neck muscle tightness – this can prevent a baby turning their head a particular way, meaning 1 side of their head is placed under more pressure
Occasionally, a brachycephaly can be caused by the plates of the skull joining together too early. This is known as craniosynostosis.
Craniosynostosis is a rare birth anomaly and is present in about three to five cases per 10,000 live births. The most common type is sagittal synostosis, followed by metopic synostosis, followed by unilateral coronal craniosynostosis and lambdoid synostosis is the rarest. Associated syndromic conditions such as Apert syndrome or Crouzon syndrome are quite rare. Doctors and scientists are not sure of the exact cause of craniosynostosis. Some think it is a genetic condition, while others think the premature closure is caused by the abnormal suture itself and still others believe that it is an abnormality of the dura which is the covering overlying the brain which causes premature fusion of the suture.
Craniosynostosis is treated with surgical correction. A team of surgeons consisting of a neurosurgeon and a craniofacial surgeon performs the surgery. The surgery can be done with an open technique or with a minimally-invasive endoscopic approach, depending on the condition and timing of repair.
Brachycephaly can be associated with numerous syndromes which include:
- Apert syndrome
- Carpenter syndrome
- Cornelia de Lange syndrome
- Cleidocranial dysostosis
- Chromosomal anomalies: Trisomy 21 or Down syndrome
- Larsen syndrome
- Roberts syndrome
How to prevent brachycephaly
A baby’s head position needs to be varied during sleep and when they are awake to avoid them developing brachycephaly.
These tips can help prevent a brachycephaly:
- Provide plenty of tummy time while your baby is awake. This means letting your baby lie down on the stomach while you are watching closely. This also helps your baby build strength and motor skills.
- Provide plenty of cuddle time by holding your baby in an upright position.
- Head and cot position for sleep: A young baby will generally stay in the position they are placed for sleep, until they can move themselves. Alternate your baby’s head position when they sleep. Place your baby at alternate ends of the cot to sleep, or change the position of the cot in the room. Babies often like to look at fixed objects like windows or wall murals, so changing their cot position will encourage them to look at things that interest them from different angles.
- Change the direction your baby lies in the crib each night. For example, have your baby’s feet point one way in the crib one night and then switch the direction the next night. Alternate each night after that. This encourages your baby to turn his or her head a different way to look at people or things in the room.
- Change the location of the crib in your baby’s room. This also encourages your baby to turn his or her head in a different direction. Babies usually turn their heads away from the wall, toward the inside of a room.
- If your baby has a flattened head, encourage your baby to turn the rounded side of the head toward the mattress. Use the tips above, such as changing the crib location or the direction your baby lies in the crib.
- Avoid having your baby spend too much time in car seats, carriers, or similar seats. But always put your baby in a car seat when he or she is riding in a car.
- Play time: When your baby is awake and alert, play or interact with them facing you (face time) or place them lying down on their front (tummy time) or on their side from as early as one or two weeks of age. Place rattles or toys (or other people’s faces) that your baby likes to look at in different positions to encourage your baby to turn their head both ways. Even at two weeks of age your baby can follow your voice or eyes (maintain eye contact) and turn their head themselves each way if you support their head in your hands while they are awake and alert.
- Sleeping position: Your baby must always be placed on their back to sleep to reduce the risk of SIDS (Sudden Infant Death Syndrome or Cot Death). Do not use pillows in the cot for positioning.
If your baby has a flattened head, there are things you can do to help your baby’s head become rounder. Encourage your baby to turn the rounded side of the head toward the mattress. Use the tips above, such as changing the crib location or the direction your baby lies in the crib. Other treatments may include exercises recommended by your doctor or a physiotherapist. If your baby’s head shape does not get better by around 6 months of age, be sure to let your doctor know.
If the flattened head is severe or other treatments haven’t worked, your doctor may recommend treatment such as a custom helmet. The helmet may help correct the shape of your baby’s head. Surgery usually isn’t recommended except in rare cases.
How you can reduce the risk of SIDS?
To help reduce the risk of SIDS, place your baby on his or her back to sleep. Even if your baby has a flattened head, don’t stop placing your baby on his or her back to sleep. Just offer plenty of tummy time and cuddle time, and change your baby’s head position.
Talk with your doctor about how to position your baby so that you don’t increase your baby’s risk of SIDS.
Brachycephaly signs and symptoms
It is quite common for a newborn baby to have an unusually shaped head. This can be either related to their position in the uterus during pregnancy, or caused by molding (changing shape) during labor, including changes caused by instruments used during delivery. Depending on the cause of the unusual shape, most babies’ heads should go back to a normal shape within about six weeks after birth.
Sometimes a baby’s head does not return to a normal shape, or they may have developed a flattened spot at the back or side of their head. Sometimes a flat spot develops when a baby has limited neck movement and prefers resting their head in one particular position.
Brachycephaly diagnosis
Brachycephaly is very common, and can typically be diagnosed with a thorough physical evaluation by a clinician who specializes in treating craniofacial differences. Because brachycephaly can be confused with craniosynostosis, especially unilateral lambdoid synostosis and unicoronal synostosis, accurate diagnosis by an experienced team is extremely important to managing your child’s condition.
Craniofacial experts will be able to differentiate readily between these conditions. In rare cases, your child’s medical team may use a CT scan to confirm the diagnosis and further evaluate your child’s condition. It is important that cases of craniosynostosis be identified early, as these conditions often require surgical treatment, and if left untreated, may result in elevated intracranial pressure.
Brachycephaly treatment
The shape of your baby’s head should improve naturally over time as their skull develops and they start moving their head, rolling around and crawling.
To take pressure off the flattened part of your baby’s head:
- give your baby time on their tummy during the day – encourage them to try new positions during play time, but make sure they always sleep on their back as this is safest for them
- switch your baby between a sloping chair, a sling and a flat surface – this ensures there isn’t constant pressure on 1 part of their head
- change the position of toys and mobiles in their cot – this will encourage your baby to turn their head on to the non-flattened side
- alternate the side you hold your baby when feeding and carrying
- reduce the time your baby spends lying on a firm flat surface, such as car seats and prams – try using a sling or front carrier when practical
If treatment is necessary, you may be referred to a specialist clinic where your baby will be treated by a team that may include a pediatrician, plastic surgeon, physiotherapist and orthotist.
If your baby has difficulty turning their head, physiotherapy may help loosen and strengthen their neck muscles. The most common treatment is provided by the physiotherapist who will encourage active movement, and teach parents how to position their baby and do exercises with them to help improve the head shape.
A very small number of babies with flat head syndrome (less than one in 10) have a severe and persistent deformity, and they may need to be treated with helmet therapy.
Corrective surgery may be needed if they have craniosynostosis.
The indications for surgical intervention in craniosynostosis include the following:
- Prevention of elevated intracranial pressure that can occur in some patients with uncorrected craniosynostosis.
- Prevention of progression of the skull deformity.
- Prevention of progression of the facial deformity.
- Optimization of growth potential of the brain.
The general consensus currently holds that the best time for surgical repair is between three and six months of age. A delay in surgery typically leads to continuation of the deformity of the craniofacial skeleton. In addition, if increased intracranial pressure is present, this will adversely affect the development of the child.
Brachycephaly helmets, headbands, pillows and mattresses
There are specially designed helmets and headbands that some people claim can help improve the shape of a baby’s skull as they grow.
These devices apply pressure to “bulging” parts of the skull and relieve pressure from other parts, potentially allowing growth in the flatter areas.
Treatment is started when the child’s skull is still soft, usually at around 5 or 6 months old, and the device is worn almost continuously (up to 23 hours a day) for several months.
But these helmets and headbands generally aren’t recommended because:
- there isn’t clear evidence to suggest they work
- they often cause problems such as skin irritation and rashes
- they’re expensive, typically costing around $2,000
- your baby will need to be checked every few weeks to monitor their head growth and make any necessary adjustments
- they may be uncomfortable and distressing for your baby
Some people try special curved mattresses that are designed to distribute the weight of a baby’s head over a larger area so less pressure is placed on a particular point of their skull.
These are cheaper than helmets and headbands, but there’s currently only limited evidence to suggest they may help.
Brachycephaly helmet
A lightweight helmet is made by an orthotist using 3D images and fitted for your baby. Brachycephaly helmet helps to reshape the skull by taking pressure off the flat area and allowing the skull to grow into the space provided.
Helmet therapy is most effective if treatment starts between six and eight months of age and is completed before 12 months, as this is the time of rapid growth of the skull.
Wearing the brachycephaly helmet doesn’t hurt and babies usually get used to it very quickly. Parents can sometimes feel quite emotional when their baby first wears the helmet. It can be helpful to know this is a common feeling and to remember treatment is temporary and outcomes are normally very good.
When your baby first gets their helmet, it will usually be worn for a two-hours-on/two-hours-off cycle for the first two days. This will allow you to monitor your baby’s skin and give your baby time to get used to the helmet. Following a review around two days after fitting, your baby will start wearing the helmet 23 hours a day. The orthotist will then review your baby about every three weeks.
Caring for your baby during helmet therapy:
- There should be some space in the helmet for your baby’s ears. Make sure their ears sit comfortably in these spaces and the helmet is not twisted.
- When you take the helmet off, check your baby’s skin to make sure there is no rubbing, blisters or broken skin. Mild redness over the high spots of the head is normal.
- You can put sorbolene cream on dry skin or mild rashes. You can buy sorbolene from a chemist or larger supermarkets. If the dry skin or rash does not get better, call your baby’s orthotist.
- Rather than taking the helmet off during hot weather, it is better to dress your baby in light clothing to keep them cool.
- Your baby’s head will become sweaty under the helmet. You should wash their hair daily and clean the inside of the helmet with a soft nailbrush or face washer and warm, soapy water. Rinse the helmet well and towel dry.





{kind=link}