What is bradykinin
Bradykinin is a nonapeptide messenger that is enzymatically produced from kallidin in the blood where it is a powerful but short-lived agent of arteriolar dilation (vasodilator) and increased capillary permeability. Bradykinin also plays a crucial role in inflammation. Bradykinin is released from mast cells during asthma attacks, from gut walls as a gastrointestinal vasodilator, from damaged tissues as a pain signal, and may be a neurotransmitter. Bradykinin can act as a vasoactive substance along with histamine in inflammation and swelling as it is a potent vasodilator 1. Bradykinin also plays a significant role in the pathophysiology of C1 esterase inhibitor deficiency and in the clinical application of considering whether to use angiotensin-converting enzyme inhibitors or angiotensin two receptor blockers 2.
Bradykinin is inactivated by angiotensin-converting enzyme (ACE) in the lungs and kidneys 3.
Bradykinin function
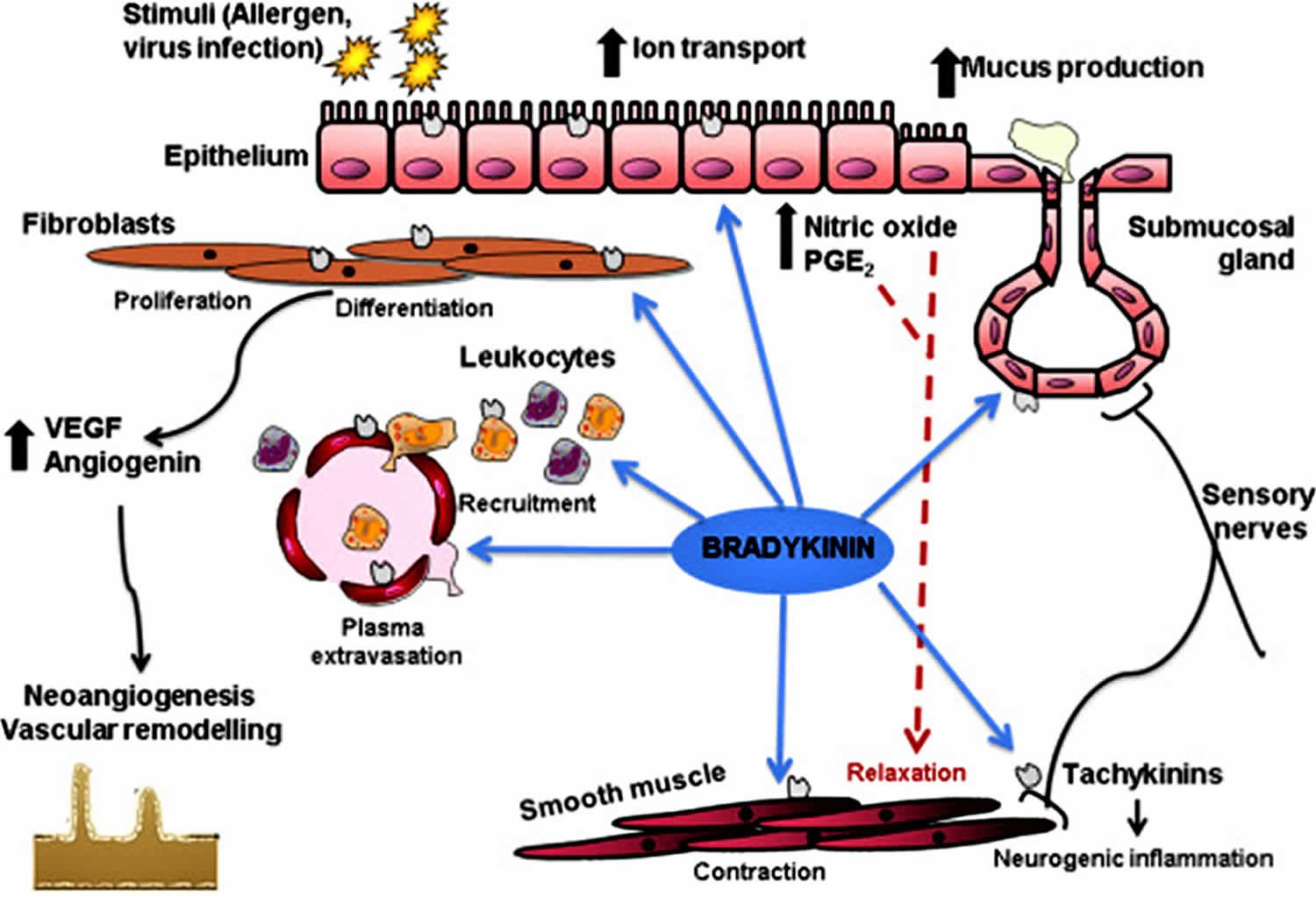
Bradykinin plays a prominent role in inflammation. Bradykinin, along with prostaglandins, and histamine, are mediators of vasodilation, in which the arteriolar smooth muscle relaxes, and in turn, increases blood flow. This increased blood flow causes the rubor, or redness, and calor, or warmth, components of the inflammation process. Bradykinin, along with prostaglandin E2 (PGE2), also plays a role in sensitization of sensory nerve endings, which causes the dolor, or pain, the component of the inflammation process. Thus in the process of inflammation, bradykinin causes an increase in vasodilation, and an increase in permeability, and an increase in pain 4.
Bradykinin plays a prominent role in the pathophysiology of C1 esterase inhibitor deficiency 1. This is an autosomal dominant hereditary disease which presents with recurrent episodes of angioedema without urticaria of the face, extremities, oropharynx, and abdomen. It can also cause angioedema of the gastrointestinal tract which manifests with severe abdominal pain as well as gastrointestinal upset. These episodes of angioedema are often preceded by a period of fatigue and flu-like symptoms. When assessing a patient with angioedema, the airway must be examined and the patient must be intubated if necessary 5. The angioedema in these patients is not responsive to epinephrine or antihistamines. Therefore, resolution of the angioedema requires treatment with plasma-derived C1 inhibitor or recombinant human C1 inhibitor. If neither of these forms of C1 inhibitor are available for treatment, fresh frozen plasma can be used for treatment 6.
C1 esterase deficiency is a complement regulatory protein deficiency that causes hereditary angioedema. C1 esterase is a protein inhibitor, it inhibits the complement system in order to prevent spontaneous activation of the complement system. Without the C1 esterase inhibitor, there is unchecked activation of C1, C2, and C4 complement proteins before other inhibitors are able to stop the cascade.
Angioedema is due to unregulated activation of kallikrein. This activation of kallikrein increases levels of bradykinin because kallikrein activates bradykinin. This excessive bradykinin induces increases permeability, increased vasodilation, and increased pain 3.
Decreased levels of C4 complement characterize C1 esterase inhibitor deficiency disease, because without the C1 esterase inhibitor to inhibit spontaneous activation of the complement system such that there is unchecked activation of C1, C2, and C4, and these complement proteins get consumed as they are activated, decreasing their levels. Thus, the best initial test is decreased C4 and C2 protein levels. However, C1 inhibitor deficiency would be unlikely if C4 levels were detected to be at normal levels. If the initial test indicates decreased levels of C4 complement protein, a confirmatory diagnostic test would be run, and confirmation of C1 esterase deficiency would show by decreased C1 inhibitor antigenic levels and decreased C1 inhibitor functional levels.
In C1 esterase deficiency, there is an excessive buildup of bradykinin. Therefore, angiotensin-converting enzyme (ACE) inhibitors are contraindicated for patients with this disease, as ACE inhibitors also have the risk of increasing bradykinin further, which would then exacerbate the manifestations of the patient’s C1 esterase deficiency due to excessive inflammation. This exacerbation is because ACE inactivates bradykinin, thus, inhibiting the ACE enzyme inhibits this inactivation, which would allow for the continuation of bradykinin, leading to angioedema 7.
ACE inhibitor and bradykinin
Angiotensin-converting enzyme (ACE) is an enzyme that breaks down and inactivates bradykinin 3. ACE is present in the lungs and the kidneys and also converts angiotensin 1 to angiotensin 2. This conversion is a crucial step in blood pressure control as angiotensin II causes vasoconstriction and increases blood pressure and constriction of efferent arterioles in the kidneys. Therefore, inhibition of ACE has clinically applied as a mechanism for decreasing blood pressure. ACE inhibitors such as captopril, enalapril, lisinopril, and ramipril all inhibit ACE and are clinically used to manage patients with hypertension, leading to decreased mortality in patients with heart failure, patients with proteinuria, and patients with diabetic nephropathy. ACE inhibitors can reduce the heart remodeling that is caused by chronic hypertension. ACE inhibitors are used in patients with chronic kidney disease such as those with diabetic nephropathy, as they decrease intraglomerular pressure, thereby slowing thickening of the glomerular basement membrane.
Inhibition of ACE decreases the amount of angiotensin 2 formed from angiotensin 1. This decrease in angiotensin 2 causes a decrease in the glomerular filtration rate by preventing the constriction of efferent arterioles. This dilation of efferent arterioles causes an increase in renin due to loss of negative feedback. Inhibition of ACE, however, also inhibits the inactivation of bradykinin. Because bradykinin is a potent vasodilator, the prevention of bradykinin inactivation causes excessive amounts of bradykinin to build-up. This increased bradykinin can cause the side effect of angioedema which can be seen in some patients taking ACE inhibitors and is the reason for the contraindication of ACE inhibitors in C1 esterase deficiency 8.
Therefore, clinically, angiotensin 2 receptor blockers (ARBs) can be used instead of ACE inhibitors for blood pressure control in hypertensive patients, heart failure, proteinuria, chronic kidney disease including diabetic nephropathy, or patients with intolerance to ACE inhibitors such as those who have excessive coughing or angioedema 9. In contrast to ACE inhibitors, angiotensin II receptor blockers, such as losartan, candesartan, and valsartan, selectively block binding of angiotensin 2 to the AT1 receptor. Though ultimately the effects are similar to ACE inhibitors, angiotensin 2 receptor blockers (ARBs) do not increase bradykinin as they are not inhibiting ACE. Therefore angioedema is not an adverse effect for patients using angiotensin 2 receptor blockers (ARBs) 10.
FDA has approved medications for treating the acute attacks of hereditary angioedema like C-1 esterase inhibitor concentrate, B2 bradykinin receptor inhibitor, a kallikrein inhibitor, and plasma free recombinant C1-inhibitor concentrate. FDA approved prophylaxis to prevent attacks of hereditary angioedema are C1 esterase inhibitor, plasma-derived concentrate of C1-esterase inhibitor and plasma kallikrein inhibitor (monoclonal antibody) 11.
- Pirahanchi Y, Sharma S. Physiology, Bradykinin. [Updated 2019 Jan 6]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2019 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK537187[↩][↩]
- Hofman Z, de Maat S, Hack CE, Maas C. Bradykinin: Inflammatory Product of the Coagulation System. Clin Rev Allergy Immunol. 2016 Oct;51(2):152-61[↩]
- Qadri F, Bader M. Kinin B1 receptors as a therapeutic target for inflammation. Expert Opin. Ther. Targets. 2018 Jan;22(1):31-44.[↩][↩][↩]
- Choi SI, Hwang SW. Depolarizing Effectors of Bradykinin Signaling in Nociceptor Excitation in Pain Perception. Biomol Ther (Seoul). 2018 May 01;26(3):255-267[↩]
- Grumach AS, Ferraroni N, Olivares MM, López-Serrano MC, Bygum A. An ABC of the Warning Signs of Hereditary Angioedema. Int. Arch. Allergy Immunol. 2017;174(1):1-6.[↩]
- Farkas H. Pharmacological Management of Hereditary Angioedema with C1-Inhibitor Deficiency in Pediatric Patients. Paediatr Drugs. 2018 Apr;20(2):135-151.[↩]
- Schmaier AH. The hereditary angioedema syndromes. J. Clin. Invest. 2019 Jan 02;129(1):66-68[↩]
- Lancellotti P, Ancion A, D’Orio V, Gach O, Maréchal P, Krzesinski JM. [Bradykinin and cardiovascular protection. Role of perindopril, an inhibitor of angiotensin conversion enzyme]. Rev Med Liege. 2018 Apr;73(4):197-205.[↩]
- Sobotková M. Angiotensin-converting enzyme inhibitor-induced angioedema: epidemiology, pathogenesis and management. Vnitr Lek. 2018 Fall;64(10):928-933.[↩]
- Sobczuk P, Szczylik C, Porta C, Czarnecka AM. Renin angiotensin system deregulation as renal cancer risk factor. Oncol Lett. 2017 Nov;14(5):5059-5068.[↩]
- Barmettler S, Li Y, Banerji A. New and evolving therapies for hereditary angioedema. Allergy Asthma Proc. 2019 Jan 01;40(1):7-13.[↩]





{kind=link}