
Contents
What is BRCA testing
BRCA testing detects mutations in BRCA1 and BRCA2 genes that are linked mainly with hereditary breast and ovarian cancers. Breast cancer genes BRCA1 and BRCA2 are tumor suppressor genes whose mutations significantly increase the likelihood of developing particular types of epithelial malignancies, namely breast, ovarian and fallopian tube cancer, although other types are also associated 1. Normally, BRCA1 and BRCA2 genes help prevent cancer by producing proteins that suppress abnormal cell growth. Certain changes (mutations) in BRCA1 and BRCA2 genes affect their normal function, thereby potentially allowing cell growth to occur uncontrolled. While the risk for the development of breast cancer is the highest of the epithelial malignancies (between 40% to 80%), the likelihood of developing other cancers including ovarian, pancreatic, and prostate is also increased in patients with BRCA1 and BRCA2 mutations.
In the general population, 12.3% of women will develop breast cancer during their lifetime and 2.74% will die of the disease, whereas 1.4% of women will develop ovarian cancer and 1.0% will die of the disease 2. A woman’s risk for breast cancer increases to 45% to 65% by age 70 years if there are clinically significant mutations in either BRCA gene 3. Mutations in the BRCA1 gene increase ovarian cancer risk to 39% by age 70 years, and BRCA2 mutations increase ovarian cancer risk to 10% to 17% by age 70 years 4. In the general population, these mutations occur in an estimated 1 in 300 to 500 women (0.2% to 0.3%) 5. In a meta-analysis conducted for the U.S. Preventive Services Task Force (USPSTF), the combined prevalence of BRCA1 and BRCA2 mutations was 2.1% in a general population of Ashkenazi Jewish women9.
The incidence of BRCA1 or BRCA2 mutations within the general population is infrequent and only found in 1 out of every 300 to 800 people 6. Only about 0.2% of the U.S. population carries a BRCA1 or BRCA2 mutation. Because of this, BRCA testing is not recommended for the general population 7. A positive BRCA mutation indicates a higher likelihood of developing cancer but does not make or confirm the diagnosis of cancer. Subsequently, a negative BRCA test does not eliminate the risk of developing breast cancer from sporadic or other genetic causes 6.
Certain populations exhibit a higher likelihood of harboring genetic mutation than the general population. These include Ashkenazi Jewish patients, male patients who develop breast cancer, and patients younger than 30 years old who develop breast cancer. Founder mutations are particular mutations passed down between family members descendant from the same genetic lineage. The specific mutations found in members of Ashkenazi Jewish lineage include 185delAG and 5385insC in the BRCA1 genes and 6174delT in the BRCA2 gene at a rate of 1 in 40 6.
One in 8 women (12.5%) in the United States will develop breast cancer throughout their lifetime 6. Certain populations are at an increased risk of developing cancer due to genetic or hereditary predisposition. According to the American Cancer Society, more than 200,000 women are diagnosed with invasive breast cancer each year and over 20,000 with ovarian cancer. Of these cancers, about 3% of breast cancers and 10% of ovarian cancers will be due to a harmful mutation in BRCA1 or BRCA2 genes. Men can also inherit an increased risk of developing breast cancer. About 5% of breast cancers in men can be attributed to mutations in the BRCA1 or BRCA2 gene.
Women with inherited mutations in BRCA1 or BRCA2 have up to a 60% lifetime risk of developing breast cancer and a 15-40% lifetime risk of developing ovarian cancer. Men and women carrying BRCA mutations may be at slightly increased risk for other cancers, such as pancreatic or prostate cancer. Breast cancer in women with inherited mutations is likely to develop at an earlier age, before menopause.
BRCA1 and BRCA2 mutation testing should be considered for individuals with a personal or family history that suggests the presence of a harmful BRCA1/BRCA2 mutation. There are a variety of screening tools to help assess the risk of having a BRCA mutation. Some of the risk factors include:
- Cancer in both breasts
- Breast cancer diagnosed at a young age, before age 50 years
- Both breast and ovarian cancers in the same individual, or both breast and ovarian cancers in separate family members
- Multiple breast cancers in the family
- A single family member with two or more primary types of BRCA1- or BRCA2-related cancers
- Breast cancer in a man or male relative
- Breast cancer that is “triple negative” (estrogen receptor (ER), progesterone receptor (PR), and HER2 negative)
- Ashkenazi Jewish ancestry
These factors should be considered for both the mother’s and father’s sides of the family.
It is recommended that people be counseled by a genetics educator both before and after BRCA mutation testing to receive genetics education to fully understand the implications of a positive and/or negative result.
BRCA mutations are inherited and passed from generation to generation (autosomal dominant inheritance pattern). Each person will have two copies of BRCA1 and BRCA2, one copy from each parent. Mutations may be present in either copy of the gene. The DNA in cells is used to detect mutations in the BRCA genes. Cells from the blood or cells from the mouth are the most easily accessible sources of that DNA.
BRCA1 and BRCA2 are human genes that produce tumor suppressor proteins. These proteins help repair damaged DNA and, therefore, play a role in ensuring the stability of each cell’s genetic material. When either of these genes is mutated, or altered, such that its protein product is not made or does not function correctly, DNA damage may not be repaired properly. As a result, cells are more likely to develop additional genetic alterations that can lead to cancer.
Specific inherited mutations in BRCA1 and BRCA2 most notably increase the risk of female breast and ovarian cancers, but they have also been associated with increased risks of several additional types of cancer. People who have inherited mutations in BRCA1 and BRCA2 tend to develop breast and ovarian cancers at younger ages than people who do not have these mutations.
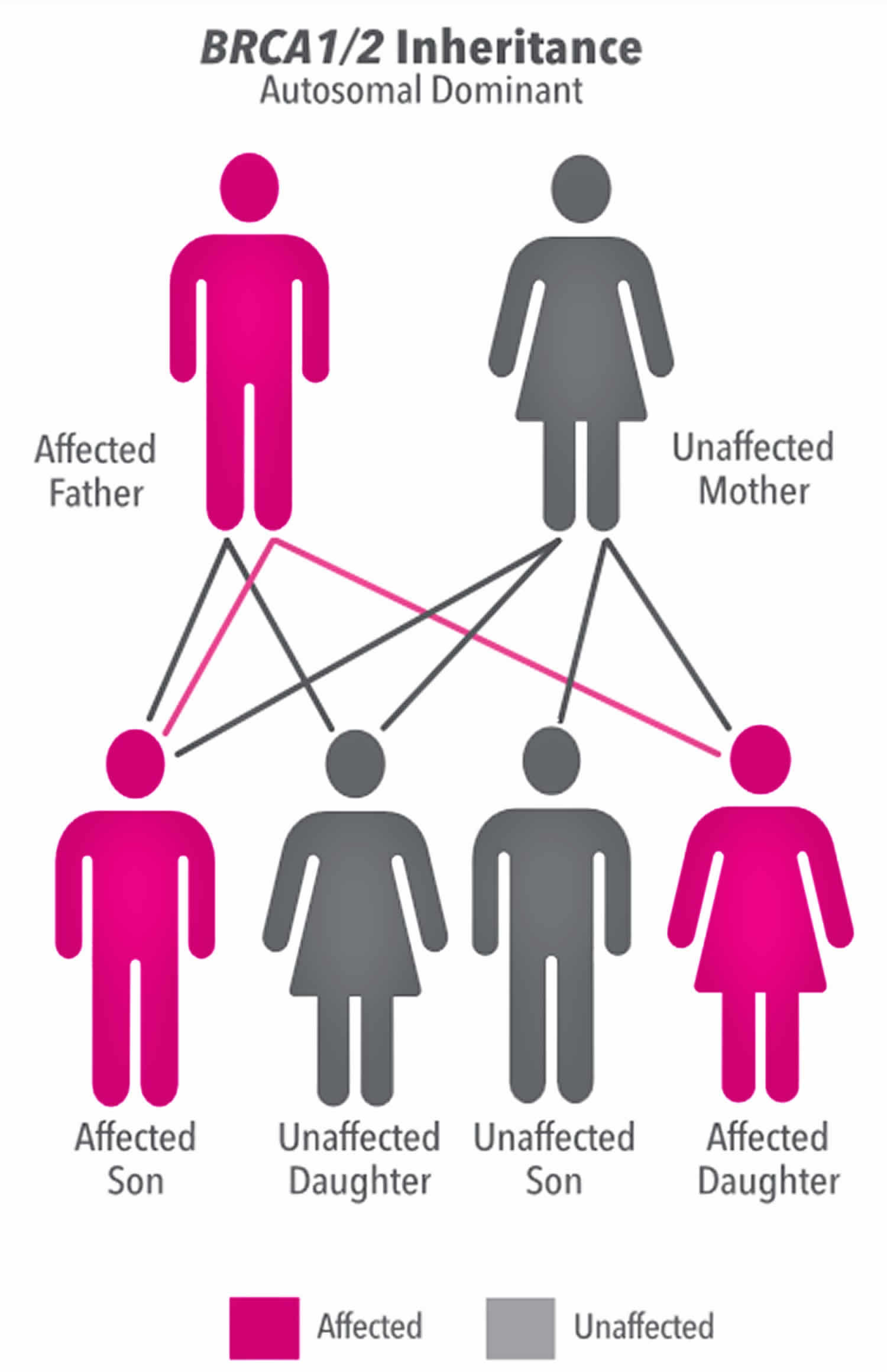
A harmful BRCA1 or BRCA2 mutation can be inherited from a person’s mother or father. Each child of a parent who carries a mutation in one of these genes has a 50% chance (or 1 chance in 2) of inheriting the mutation. The effects of mutations in BRCA1 and BRCA2 are seen even when a person’s second copy of the gene is normal.
Figure 1. BRCA gene autosomal dominant inheritance pattern (mother has the defective BRCA gene)
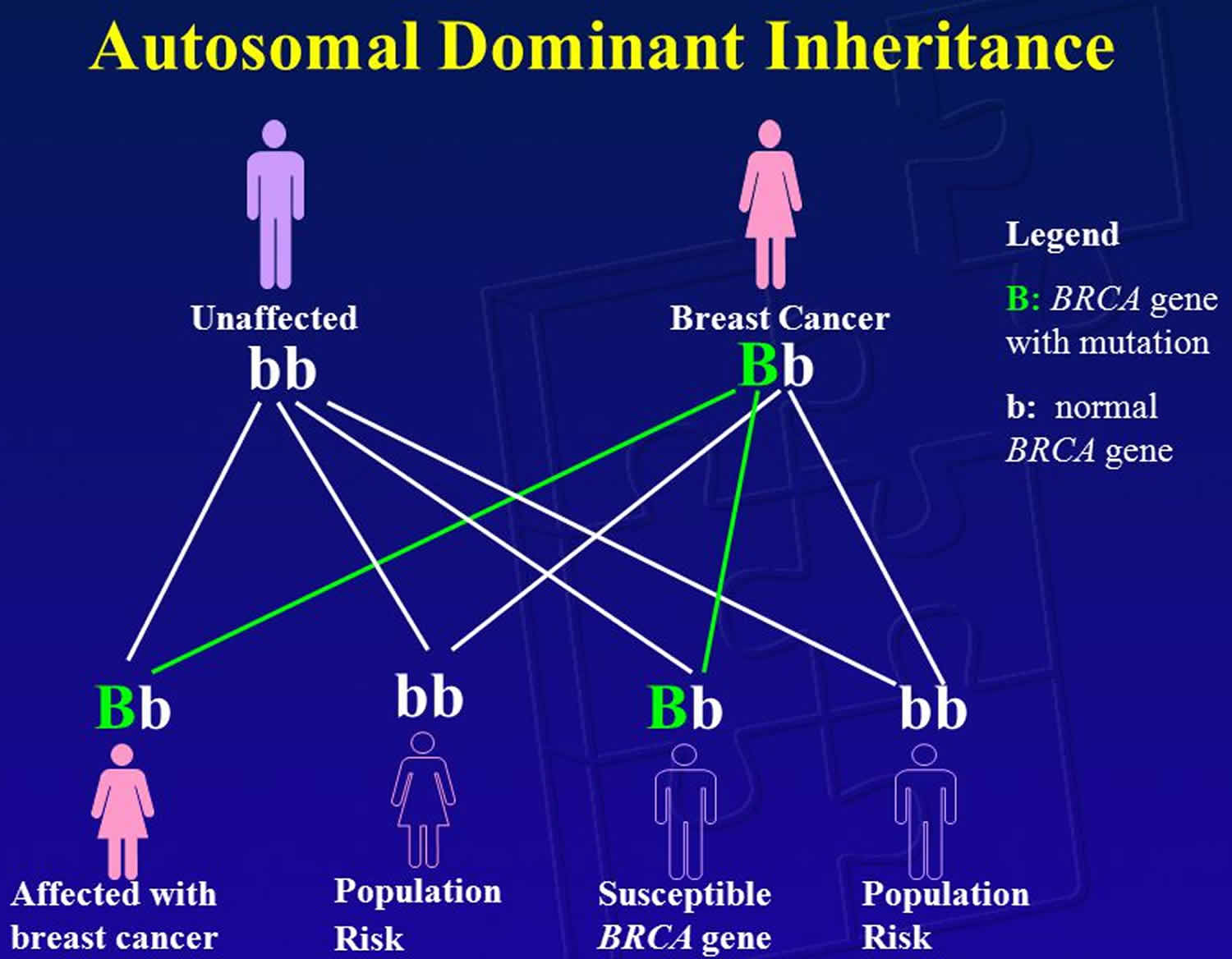
Figure 2. BRCA gene autosomal dominant inheritance pattern (father has the defective BRCA gene)
BRCA1 gene
The BRCA1 gene (breast cancer 1 gene) provides instructions for making a protein that acts as a tumor suppressor. Tumor suppressor proteins help prevent cells from growing and dividing too rapidly or in an uncontrolled way. Cytogenetic Location: 17q21.31, which is the long (q) arm of chromosome 17 at position 21.31
The BRCA1 protein is involved in repairing damaged DNA. In the nucleus of many types of normal cells, the BRCA1 protein interacts with several other proteins to mend breaks in DNA. These breaks can be caused by natural and medical radiation or other environmental exposures, and they also occur when chromosomes exchange genetic material in preparation for cell division. By helping to repair DNA, the BRCA1 protein plays a critical role in maintaining the stability of a cell’s genetic information.
Research suggests that the BRCA1 protein also regulates the activity of other genes and plays an essential role in embryonic development. To carry out these functions, the BRCA1 protein interacts with many other proteins, including other tumor suppressors and proteins that regulate cell division.
BRCA2 gene
The BRCA2 gene (breast cancer 2 gene) provides instructions for making a protein that acts as a tumor suppressor. Tumor suppressor proteins help prevent cells from growing and dividing too rapidly or in an uncontrolled way. Cytogenetic Location: 13q13.1, which is the long (q) arm of chromosome 13 at position 13.1
The BRCA2 protein is involved in repairing damaged DNA. In the nucleus of many types of normal cells, the BRCA2 protein interacts with several other proteins to mend breaks in DNA. These breaks can be caused by natural and medical radiation or other environmental exposures, and they also occur when chromosomes exchange genetic material in preparation for cell division. By helping to repair DNA, the BRCA2 protein plays a critical role in maintaining the stability of a cell’s genetic information.
Researchers suspect that the BRCA2 protein has additional functions within cells. For example, the protein may help regulate cytokinesis, which is the step in cell division when the fluid surrounding the nucleus (the cytoplasm) divides to form two separate cells. Researchers are investigating the protein’s other potential activities.
When is BRCA testing ordered?
BRCA1 and BRCA2 mutation testing is NOT recommended as a screening tool for the general population. When someone has a personal or family history that suggests the presence of a harmful BRCA mutation, that person may choose to undergo BRCA testing. Risk factors are listed above. Someone who is considering BRCA testing should talk to their healthcare practitioner and seek counseling by a genetics educator/counselor prior to and after testing.
Are people with BRCA mutations at risk for other cancers?
The BRCA mutations’ role in cancer risk is an active area of research. In addition to breast and ovarian cancer, the mutation has been linked to prostate and pancreatic cancer. As of 2015, studies have found that the BRCA mutation is present in 0.5%-4% of prostate cancers and 5%-8% of pancreatic cancers.
However, researchers are still gathering information about how BRCA mutation testing should be incorporated into screening for those cancers. For example, while researchers are finding that men carrying BRCA mutations have an increased risk for prostate cancer, it is still unclear what family or personal history factors should prompt men in the general population to receive BRCA mutation testing. The National Comprehensive Cancer Network does recommend that men carrying BRCA2 mutation begin prostate cancer screening at 40 years old. For pancreatic cancer, there are no data showing that BRCA mutation screening improves cancer survival. There are currently no guidelines for BRCA mutation testing and pancreatic cancer.
Who should get BRCA testing?
For women whose family history is associated with an increased risk for potentially harmful mutations in the BRCA1 or BRCA2 genes, adequate evidence suggests that the benefits of BRCA testing for potentially harmful BRCA mutations are moderate 7.
Criteria for BRCA testing in patients with personal history of breast cancer and one or more of the following (from the National Comprehensive Cancer Network and the American Society of Breast Surgeons Consensus Guideline on Hereditary Genetic Testing):
- Age of onset less than or equal to 50
- Triple negative tumor (ER-PR-HER2-) and age less than or equal to 60
- Ashkenazi Jewish heritage and breast cancer at any age
- Two or more primary breast cancer (either asynchronous, synchronous, bilateral, or multicentric)
- A first-degree relative with breast cancer diagnosed at age less than or equal to 50
- Two relatives on the same side of the family with breast cancer and/or pancreatic cancer
- Family or personal history of ovarian cancer, fallopian cancer, or primary peritoneal cancer
- Male breast cancer
- Known mutation carrier in the family
Testing patients who have not been diagnosed with cancer is typically reserved for situations when the affected family member or members cannot be tested.
Criteria for BRCA testing patients without a personal history of breast cancer but with one or more of the following (from the National Comprehensive Cancer Network and American Society of Breast Surgeons Consensus Guideline on Hereditary Genetic Testing):
- First-degree or second-degree relative with age onset of breast cancer less than or equal to 45
- Ashkenazi Jewish heritage and family history of breast cancer at any age
- Two or more primary breast cancer (either asynchronous, synchronous, bilateral, or multicentric) in a single family member
- Two or more relatives on the same side of the family with breast and/or pancreatic cancer
- Family or personal history of ovarian, fallopian, or primary peritoneal cancer
- Male breast cancer
- Known mutation carrier in the family
In addition to the above criteria, likelihood or risk assessment models such as the BRCAPRO, BOADICEA, Penn II and IBIS can also be used to determine whether a patient is at an increased risk for carrying BRCA mutations and thus indicate the need for genetic testing or referral to a genetic counselor or breast surgeon. Though these models estimate the risk of developing breast cancer, no particular test or level of risk determines the need for or against BRCA testing.
For women whose family history is not associated with an increased risk for potentially harmful mutations in the BRCA1 or BRCA2 genes, there is adequate evidence that the benefits of BRCA testing for potentially harmful BRCA mutations are few to none 7.
The U.S. Preventive Services Task Force Assessment
For women whose family history is associated with an increased risk for potentially harmful mutations in the BRCA1 or BRCA2 genes, there is moderate certainty that the net benefit of testing for potentially harmful BRCA mutations and early intervention is moderate 7.
For women whose family history is not associated with an increased risk for potentially harmful mutations in the BRCA1 or BRCA2 genes, there is moderate certainty that the net benefit of testing for potentially harmful BRCA mutations and early intervention ranges from minimal to potentially harmful 7.
Adequate evidence suggests that the overall harms of detection of and early intervention for potentially harmful BRCA mutations are small to moderate.
Timing of BRCA screening
Consideration of screening for potentially harmful BRCA mutations should begin once women have reached the age of consent (18 years). Primary care providers should periodically assess all patients for changes in family history (for example, comprehensive review at least every 5 to 10 years) 8.
BRCA testing criteria
Recommendations made by the U.S. Preventive Services Task Force (USPSTF) Recommendation Summary 7:
Women who have Family Members with Breast, Ovarian, Tubal, or Peritoneal Cancer
The U.S. Preventive Services Task Force recommends that primary care providers screen women who have family members with breast, ovarian, tubal, or peritoneal cancer with 1 of several screening tools designed to identify a family history that may be associated with an increased risk for potentially harmful mutations in breast cancer susceptibility genes (BRCA1 or BRCA2). Women with positive screening results should receive genetic counseling and, if indicated after counseling, BRCA testing.
This recommendation applies to asymptomatic women who have not been diagnosed with BRCA-related cancer.
Women who have 1 or more family members with a known potentially harmful mutation in the BRCA1 or BRCA2 genes should be offered genetic counseling and testing.
The U.S. Preventive Services Task Force recognizes the potential importance of further evaluating women who have a diagnosis of breast or ovarian cancer. Some women receive genetic testing as part of a cancer evaluation at the time of diagnosis of breast cancer. The U.S. Preventive Services Task Force did not review the appropriate use of BRCA testing in the evaluation of women who are newly diagnosed with breast cancer. That assessment is part of disease management and is beyond the scope of this recommendation. Women who have been diagnosed with breast cancer in the past and who did not receive BRCA testing as part of their cancer care but have a family history of breast or ovarian cancer should be encouraged to discuss further evaluation with their clinician.
These recommendations do not apply to men, although male family members may be identified for testing during evaluation.
Women Whose Family History is not Associated with an Increased Risk
The U.S. Preventive Services Task Force recommends against routine genetic counseling or BRCA testing for women whose family history is not associated with an increased risk for potentially harmful mutations in the BRCA1 or BRCA2 genes.
BRCA testing guidelines
The United States Preventive Service Task Force recommends that primary care physicians evaluate women who are candidates for hereditary cancer genetic testing by inquiring about family history of breast, ovarian, tubal or other cancers during annual examinations. If questioning reveals increased risk, referral to a certified genetic counselor for possible testing is indicated. Certified genetic counselors and breast surgeons may also aid in the decision regarding tests for BRCA alone, or for different genetic mutations related to other hereditary cancers.
American Society of Breast Surgeons emphasizes the importance of thorough patient history and uses the following criteria (similar to the National Comprehensive Cancer Network guidelines for genetic risk evaluation).
Criteria for BRCA testing in patients with personal history of breast cancer and one or more of the following (from the National Comprehensive Cancer Network and the American Society of Breast Surgeons Consensus Guideline on Hereditary Genetic Testing):
- Age of onset less than or equal to 50
- Triple negative tumor (ER-PR-HER2-) and age less than or equal to 60
- Ashkenazi Jewish heritage and breast cancer at any age
- Two or more primary breast cancer (either asynchronous, synchronous, bilateral, or multicentric)
- A first-degree relative with breast cancer diagnosed at age less than or equal to 50
- Two relatives on the same side of the family with breast cancer and/or pancreatic cancer
- Family or personal history of ovarian cancer, fallopian cancer, or primary peritoneal cancer
- Male breast cancer
- Known mutation carrier in the family
Testing patients who have not been diagnosed with cancer is typically reserved for situations when the affected family member or members cannot be tested.
Criteria for BRCA testing patients without a personal history of breast cancer but with one or more of the following (from the National Comprehensive Cancer Network and American Society of Breast Surgeons Consensus Guideline on Hereditary Genetic Testing):
- First-degree or second-degree relative with age onset of breast cancer less than or equal to 45
- Ashkenazi Jewish heritage and family history of breast cancer at any age
- Two or more primary breast cancer (either asynchronous, synchronous, bilateral, or multicentric) in a single family member
- Two or more relatives on the same side of the family with breast and/or pancreatic cancer
- Family or personal history of ovarian, fallopian, or primary peritoneal cancer
- Male breast cancer
- Known mutation carrier in the family
In addition to the above criteria, likelihood or risk assessment models such as the BRCAPRO, BOADICEA, Penn II and IBIS can also be used to determine whether a patient is at an increased risk for carrying BRCA mutations and thus indicate the need for genetic testing or referral to a genetic counselor or breast surgeon. Though these models estimate the risk of developing breast cancer, no particular test or level of risk determines the need for or against BRCA testing.
How to test for BRCA gene
The test for BRCA mutations is done on a blood sample collected by needle from a vein in the arm or from a special oral rinse that collects cells from the mouth. BRCA testing does not require surgical biopsy of breast or ovarian tissue.
No test preparation is needed, but genetic counseling is strongly recommended to confirm that you meet the BRCA testing criteria. If the sample is a saliva-based specimen, it is recommended that the person being tested not eat, drink, or chew gum for at least an hour prior to the testing appointment. Furthermore, kissing should also be avoided immediately prior to BRCA testing.
BRCA test can be ordered by a healthcare practitioner or genetic counselor. The sample will be sent to a laboratory that specializes in BRCA mutation testing. The American Society of Clinical Oncology and the National Breast Cancer Coalition encourage women seeking the test to participate in long-term outcome studies to help gather information on the effectiveness of different check-up and treatment options.
Testing for BRCA mutations should be done only when an individual has personal or family history that suggests an inherited cancer susceptibility, when an individual has access to a health professional who is trained to provide genetic counseling and interpret test results, and when test results will aid in decision making. Initial testing of a family member who has breast or ovarian cancer is the preferred strategy in most cases, but it is reasonable to test if no affected relative is available. It is essential that before testing, the individual is fully informed about the implications of testing and has expressed a desire for it.
The type of mutation analysis required depends on family history. Individuals from families with known mutations or from ethnic groups in which certain mutations are more common (for example, Ashkenazi Jewish women) can be tested for these specific mutations.
Individuals without linkages to families or groups with known mutations receive more comprehensive testing. In these cases, when possible, testing should begin with a relative who has breast or ovarian cancer to determine whether affected family members have a clinically significant mutation.
Tests for BRCA mutations are highly sensitive and specific for known mutations, but interpretation of results is complex and generally requires posttest counseling. Test results for genetic mutations are reported as positive (that is, potentially harmful mutation detected), variants of uncertain clinical significance, uninformative-negative, or true-negative. Women who have relatives with known BRCA mutations can be reassured about their inherited risk for a potentially harmful mutation if the results are negative (that is, a true negative). Some studies suggest increased breast cancer risk in some women with true-negative results 9. However, a comprehensive meta-analysis conducted for the USPSTF that included these studies found that breast cancer risk is generally not increased in women with true-negative results 10. An uninformative-negative result occurs when a woman’s test does not detect a potentially harmful mutation but no relatives have been tested or no mutations have been detected in tested relatives. Available tests may not be able to identify mutations in these families. Risk for breast cancer is increased in women with uninformative-negative results 10.
How is BRCA testing used?
Standard BRCA1 and BRCA2 tests are used to detect mutations that are known to increase the risk of breast and ovarian cancer development. If a BRCA1 or BRCA2 mutation has been identified in a family member with breast and/or ovarian cancer, then that specific mutation can be tested in other family members to assess their risk. Specific BRCA1 and BRCA2 mutations are associated with some ethnic groups, such as those of Ashkenazi Jewish descent, and can be used to evaluate the risk of individuals in this group.
What does the BRCA test result mean?
The normal risk for cancer development in the general population is 12.5% for female breast cancer, 0.1% for male breast cancer and 1% to 2% for ovarian cancer. The presence of a BRCA1 or BRCA2 mutation means that the person tested is at an increased risk for developing hereditary breast and/or ovarian cancer syndrome. It also indicates that the individual’s family members may be at increased risk for breast or ovarian cancer. However, even within a family with the same BRCA mutation, not everyone will develop cancer and those who do may develop it at different times during their lives. According to the National Cancer Institute, estimates of lifetime risk for breast cancer in women are 55% to 65% for BRCA1 mutation and 45% for BRCA2 mutation. Risk of ovarian cancer is 39% with BRCA1 mutation and 11% to 19% with BRCA2 mutation.
Patients with BRCA1 and BRCA2 mutation experience worse breast cancer specific survival when compared to BRCA-negative patients. BRCA1 carriers have worse overall survival than BRCA2 and BRCA- negative patients 6.
The incidence and associated risk for cancer development by age 70 for BRCA1 and BRCA2 mutations are listed below 6:
BRCA 1 Mutation
- Responsible for approximately 35% of hereditary breast cancer
- Increased risk of developing breast cancer by age 70 to 44% to 78%
- Increased risk of developing ovarian cancer by age 70 to 18% to 54%
- Increased risk of developing male breast cancer by age 70 to 0.22 to 2.8%
BRCA 2 Mutation
- Responsible for approximately 25% of hereditary breast cancer
- Increased risk of developing breast cancer by age 70 to 31% to 56%
- Increased risk of developing ovarian cancer by age 70 to 2.4% to 19%
- Increased risk of developing male breast cancer by age 70 to 3.2% to 12%
The degree of risk conferred with a positive result is difficult to quantify for a specific person. Results must be interpreted in conjunction with the tested person’s personal and family history. A genetic counselor should explain the meaning of the results, treatment options for the individual that are intended to decrease risk, and testing options for other family members.
Table 1. Risk of Malignancy in Individuals with a Germline BRCA1 or BRCA2-Pathogenic Variant
| Cancer Type | General Population Risk | Risk for Malignancy | |
|---|---|---|---|
| BRCA1 | BRCA2 | ||
| Breast | 12% | 46%-87% | 38%-84% |
| Second primary breast | 2% within 5 years | 21.1% within 10 yrs 83% by age 70 | 10.8% within 10 yrs 62% by age 70 |
| Ovarian | 1%-2% | 39%-63% | 16.5%-27% |
| Male breast | 0.1% | 1.2% | Up to 8.9% |
| Prostate | 6% through age 69 | 8.6% by age 65 | 15% by age 65 20% lifetime |
| Pancreatic | 0.50% | 1%-3% | 2%-7% |
| Melanoma (cutaneous & ocular) | 1.6% | Elevated Risk | |
Genetic testing for BRCA1 and BRCA2 mutations cannot detect 100% of these mutations; thus, even with a negative result there is very small chance that there is a BRCA1/BRCA2 gene mutation present that was not identified by the testing method utilized. In addition, there are other genes that may have mutations that can contribute to a family’s risk for cancer. Genetic testing for just BRCA1 or BRCA2 will only detect mutations in these two genes; therefore, if a mutation is present in another gene known to cause an increased risk for breast cancer, BRAC1/BRCA2 mutation testing will not detect it.
In addition, sometimes a personal or family history of cancer may suggest a factor or combination of other factors that contribute to a person’s risk. In these families, it is likely that common risk factors such as shared genes that only sometimes cause cancer (low penetrance), shared environment and exposures, and shared lifestyle habits are increasing the risk for cancer above that of the general population. While individuals in these families typically do not have increased risks anywhere near as high as those seen in individuals with BRCA1 or BRCA2 mutations, they often will have increased risks for cancer slightly above those of the general population and sometimes increased cancer surveillance is recommended.
Positive test results may have implications for other family members. When one member of a family is tested for BRCA mutations, issues often arise about how to share this information with other family members. It may be helpful to seek advice from a genetic counselor about how to communicate results with other family members.
Pre- and post-test consultation with a genetic counselor about genetic testing cannot be overemphasized. There are many issues to be considered when preparing for a genetic test and upon learning the results, and a genetic counselor has the knowledge and expertise to help sort through them.
If the BRCA mutation test is positive, what are my options?
If the BRCA mutation test is positive, the options include earlier, more frequent, or intensive cancer screenings and screening starting earlier in life (e.g., mammography, breast MRI, blood tests for CA-125 or CA 15-3, or transvaginal ultrasonography); risk-reducing medications (for example, tamoxifen or raloxifene); and risk-reducing surgical removal of the ovaries or breasts (for example, mastectomy or salpingo-oophorectomy). However, the strength of evidence varies across the types of interventions. There are a number of variables involved and it is important to discuss your options with your healthcare provider and genetic counselor.
Evidence is lacking on the effect of intensive screening for BRCA-related cancer on clinical outcomes in women who are BRCA mutation carriers. Medications, such as tamoxifen and raloxifene, have been shown to reduce the incidence of invasive breast cancer in high-risk women in the general population, but they have not been studied specifically in women who are BRCA mutation carriers 12.
In high-risk women and those who are BRCA mutation carriers, cohort studies of risk-reducing surgery (mastectomy and salpingo-oophorectomy) showed substantially reduced risk for breast or ovarian cancer. Breast cancer risk was reduced by 85% to 100% with mastectomy 13 and by 37% to 100% with oophorectomy, and ovarian cancer risk was reduced by 69% to 100% with oophorectomy or salpingo-oophorectomy 12. Salpingo-oophorectomy was also associated with a 55% relative reduction in all-cause mortality (as measured during the course of the study) in women with BRCA1 or BRCA2 mutations and without a history of breast cancer 14.
Surveillance for Patients with BRCA1 and BRCA2 Mutations
An increased level of monitoring is mandatory for all patients with known BRCA mutations. The National Comprehensive Cancer Network guidelines are widely accepted in the management of patients with BRCA mutation. The main goal of monitoring is early detection of malignancy and high-risk premalignant lesions. Early detection begins with breast awareness and self-breast examination beginning at age 18 and annual or semiannual clinical breast examination at age 25 (though neither of these has shown to benefit survival).
Breast MRI increases sensitivity from approximately 33% to approximately 80% sensitivity in detection of malignancy in patients with familial or hereditary predisposition and has proven especially useful in this younger subset of patients. According to the National Comprehensive Cancer Network guidelines, annual screening breast MRI with contrast is recommended annually from age 25 to 29 if available, or mammogram annually, if not. From age 30 to 75, annual mammogram and MRI of the breast with contrast is performed.
The treatment is personalized for each patient who is found to have a BRCA1 or BRCA2 mutation. This may include increased surveillance only, chemoprevention using tamoxifen or raloxifene, bilateral prophylactic salpingo-oophorectomy and or bilateral prophylactic mastectomy. Bilateral prophylactic mastectomy reduces the risk of developing breast cancer by 90% to 95%. Referral to a breast surgeon for discussion regarding the option of risk-reducing mastectomy is indicated.
Potential harms of cancer screening and treatment
Intensive screening for breast and ovarian cancer is associated with false-positive results, unnecessary imaging, and unneeded surgery. In 2 studies comparing mammography with magnetic resonance imaging for breast cancer screening in which 18% to 100% of study participants were BRCA mutation carriers, mammography was associated with higher false-positive rates (14% vs. 5.5% in the first round of screening; 15% vs. 11% in another study) 15 and more false-negative results (12 vs. 1 case in the first round of screening; 12 vs. 4 cases in subsequent rounds) 16. In a retrospective analysis of a cohort of women with potentially harmful BRCA mutations or first-degree relatives with BRCA mutations, those who were screened with mammography were more likely to have unneeded imaging than those who were screened with magnetic resonance imaging; however, rates of unneeded biopsy were similar 15.
Risk-reducing medications (for example, tamoxifen or raloxifene) can increase risk for thromboembolic events (4 to 7 events per 1000 women over 5 years). Tamoxifen increased the risk for endometrial cancer (4 to 5 cases per 1000 women) compared with placebo or raloxifene, and it also increased risk for cataracts (15 per 1000 women) compared with raloxifene 17.
Data on the long-term physical harms of risk-reducing mastectomy are limited. In high-risk women having risk-reducing mastectomy with immediate reconstruction, 21% in 1 series had complications (for example, hematoma, contracture, or implant rupture) 18. In another series, 64% reported postsurgical symptoms (for example, numbness, pain, tingling, infection, swelling, breast hardness, bleeding, organizing hematoma, failed reconstruction, breathing problems, thrombosis, and pulmonary embolism) 19. After risk-reducing oophorectomy, 5% of women in 1 study had postsurgical complications (for example, wound infection, bladder or uterine perforation, or small-bowel obstruction) 20.
Seven observational studies provided data on psychological distress due to risk-reducing mastectomy 21 or oophorectomy 22. In 1 study of 90 women who had risk-reducing bilateral mastectomy 23, there were significant reductions in scores for anxiety and sexual pleasure and no significant differences in depression scores, body image concerns, or other measures. In another study 24, there were no significant differences in psychological measures between women who had risk-reducing mastectomy and a reference sample that did not have the procedure. Ten years after risk-reducing mastectomy, most women in another study reported that their family lives were unchanged, but 39% reported negative effects on spousal relationships because of decreased sensation and changed body appearance 25. After risk-reducing salpingo-oophorectomy, premenopausal women reported significant worsening of vasomotor symptoms and decreased sexual function 22.
Estimate of magnitude of net benefit
For women whose family history is associated with an increased risk for potentially harmful mutations in the BRCA1 or BRCA2 genes, the United States Preventive Service Task Force found adequate evidence that the benefits of testing, detection, and early intervention are moderate. For women whose family history is not associated with an increased risk for potentially harmful mutations in the BRCA1 or BRCA2 genes, the United States Preventive Service Task Force found adequate evidence that the benefits of testing, detection, and early intervention are few to none. The United States Preventive Service Task Force found adequate evidence that the overall harms of testing, detection, and early intervention are small to moderate.
For women whose family history is associated with an increased risk for potentially harmful mutations in the BRCA1 or BRCA2 genes, the United States Preventive Service Task Force concludes with moderate certainty that the net benefit of testing, detection, and early intervention is moderate. For women whose family history is not associated with an increased risk for potentially harmful mutations in the BRCA1 or BRCA2 genes, the United States Preventive Service Task Force concludes with moderate certainty that the net benefit of testing, detection, and early intervention ranges from minimal to potentially harmful.
- Lindor NM, McMaster ML, Lindor CJ, Greene MH; National Cancer Institute, Division of Cancer Prevention, Community Oncology and Prevention Trials Research Group. Concise handbook of familial cancer susceptibility syndromes: second edition. J Natl Cancer Inst Monogr. 2008:1-93.[↩]
- Howlader N, Noone AM, Krapcho M, Garshell J, Neyman N, Altekruse SF, et al, eds. SEER Cancer Statistics Review, 1975–2010. Bethesda, MD: National Cancer Institute; 2013.[↩]
- Chen S, Parmigiani G. Meta-analysis of BRCA1 and BRCA2 penetrance. J Clin Oncol. 2007;25:1329-33.[↩]
- Antoniou A, Pharoah PD, Narod S, Risch HA, Eyfjord JE, Hopper JL, et al. Average risks of breast and ovarian cancer associated with BRCA1 or BRCA2 mutations detected in case series unselected for family history: a combined analysis of 22 studies. Am J Hum Genet. 2003;72:1117-30.[↩]
- Prevalence and penetrance of BRCA1 and BRCA2 mutations in a population-based series of breast cancer cases. Anglian Breast Cancer Study Group. Br J Cancer. 2000;83(10):1301-08.[↩]
- Casaubon JT, Regan JP. BRCA 1 and 2. [Updated 2018 Oct 27]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2018 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK470239[↩][↩][↩][↩][↩][↩]
- BRCA-Related Cancer: Risk Assessment, Genetic Counseling, and Genetic Testing. Final Recommendation Statement. https://www.uspreventiveservicestaskforce.org/Page/Document/RecommendationStatementFinal/brca-related-cancer-risk-assessment-genetic-counseling-and-genetic-testing[↩][↩][↩][↩][↩][↩]
- Finch A, Metcalfe KA, Chiang J, Elit L, McLaughlin J, Springate C, et al. The impact of prophylactic salpingo-oophorectomy on quality of life and psychological distress in women with a BRCA mutation. Psychooncology. 2013;22:212-9.[↩]
- Vos JR, de Bock GH, Teixeira N, van der Kolk DM, Jansen L, Mourits MJ, et al. Proven non-carriers in BRCA families have an earlier age of onset of breast cancer. Eur J Cancer. 2013.[↩]
- Nelson HD, Fu R, Goddard K, Mitchell Priest J, Okinaka-Hu L, Pappas M, Zakher B. Risk Assessment, Genetic Counseling, and Genetic Testing for BRCA-Related Cancer: Systematic Review to Update the U.S. Preventive Services Task Force Recommendation. Evidence Synthesis No. 101. AHRQ Publication No. 12-05164-EF-1. Rockville, MD: Agency for Healthcare Research and Quality; April 2013.[↩][↩]
- Petrucelli N, Daly MB, Pal T. BRCA1- and BRCA2-Associated Hereditary Breast and Ovarian Cancer. 1998 Sep 4 [Updated 2016 Dec 15]. In: Adam MP, Ardinger HH, Pagon RA, et al., editors. GeneReviews® [Internet]. Seattle (WA): University of Washington, Seattle; 1993-2019. Available from: https://www.ncbi.nlm.nih.gov/books/NBK1247[↩]
- Nelson HD, Smith ME, Griffin JC, Fu R. Use of medications to reduce risk for primary breast cancer: a systematic review for the U.S. Preventive Services Task Force. Ann Intern Med. 2013;158:604-14.[↩][↩]
- Skytte AB, Crüger D, Gerster M, Laenkholm AV, Lang C, Brøndum-Nielsen K, et al. Breast cancer after bilateral risk-reducing mastectomy. Clin Genet. 2011;79(5):431-7.[↩]
- Domchek SM, Friebel TM, Singer CF, Evans DG, Lynch HT, Isaacs C, et al. Association of risk-reducing surgery in BRCA1 or BRCA2 mutation carriers with cancer risk and mortality. JAMA. 2010;304(9):967-75.[↩]
- Le-Petross HT, Whitman GJ, Atchley DP, Yuan Y, Gutierrez-Barrera A, Hortobagyi GN, et al. Effectiveness of alternating mammography and magnetic resonance imaging for screening women with deleterious BRCA mutations at high risk of breast cancer. Cancer. 2011;117(17):3900-07.[↩][↩]
- Kriege M, Brekelmans CT, Boetes C, Muller SH, Zonderland HM, Obdeijn IM, et al; Dutch MRI Screening (MRISC) Study Group. Differences between first and subsequent rounds of the MRISC breast cancer screening program for women with a familial or genetic predisposition. Cancer. 2006;106(11):2318-26.[↩]
- Nelson HD, Fu R, Humphrey L, Smith ME, Griffin JC, Nygren P. Comparative Effectiveness of Medications to Reduce Risk of Primary Breast Cancer in Women. Comparative Effectiveness Review No. 17. Rockville, MD: Agency for Healthcare Research and Quality; 2009[↩]
- Contant CM, Menke-Pluijmers MB, Seynaeve C, Meijers-Heijboer EJ, Klijn JG, Verhoog LC, et al. Clinical experience of prophylactic mastectomy followed by immediate breast reconstruction in women at hereditary risk of breast cancer (HB(O)C) or a proven BRCA1 and BRCA2 germ-line mutation. Eur J Surg Oncol. 2002;28(6):627-32.[↩]
- Metcalfe KA, Esplen MJ, Goel V, Narod SA. Psychosocial functioning in women who have undergone bilateral prophylactic mastectomy. Psychooncology. 2004;13(1):14-25.[↩]
- Kauff ND, Satagopan JM, Robson ME, Scheuer L, Hensley M, Hudis CA, et al. Risk-reducing salpingo-oophorectomy in women with a BRCA1 or BRCA2 mutation. New Eng J Med. 2002;346(21):1609-15.[↩]
- Brandberg Y, Arver B, Johansson H, Wickman M, Sandelin K, Liljegren A. Less correspondence between expectations before and cosmetic results after risk-reducing mastectomy in women who are mutation carriers: a prospective study. Eur J Surg Oncol. 2012;38(1):38-43.[↩]
- Finch A, Metcalfe KA, Chiang JK, Elit L, McLaughlin J, Springate C, et al. The impact of prophylactic salpingo-oophorectomy on menopausal symptoms and sexual function in women who carry a BRCA mutation. Gynecol Oncol. 2011;121(1):163-8.[↩][↩]
- Brandberg Y, Arver B, Johansson H, Wickman M, Sandelin K, Liljegren A. Less correspondence between expectations before and cosmetic results after risk-reducing mastectomy in women who are mutation carriers: a prospective study. Eur J Surg Oncol. 2012;38(1):38-43.[↩]
- Gahm J, Wickman M, Brandberg Y. Bilateral prophylactic mastectomy in women with inherited risk of breast cancer—prevalence of pain and discomfort, impact on sexuality, quality of life and feelings of regret two years after surgery. Breast. 2010;19(6):462-9.[↩]
- Wasteson E, Sandelin K, Brandberg Y, Wickman M, Arver B. High satisfaction rate ten years after bilateral prophylactic mastectomy—a longitudinal study. Eur J Cancer Care (Engl). 2011;20(4):508-13.[↩]





{kind=link}