Contents
- What is cachexia
- Who gets cachexia?
- Is cachexia a sign of dying?
- Cancer cachexia
- Cardiac cachexia
- Cachexia causes
- Cachexia symptoms
- Cachexia survival time
- Cachexia diagnosis
- Cachexia treatment
What is cachexia
Cachexia has been defined as a complicated metabolic syndrome characterized by progressive loss of lean tissue or muscle mass loss with or without fat mass loss that is often associated with anorexia, an inflammatory process, insulin resistance, and increased protein turnover 1. Losses are often in excess to that explained by the associated anorexia. Anorexia just means loss of appetite and is often associated with cachexia, but not always. Cachexia is not simple starvation where fat stores replace glucose as the primary fuel. Cancer causes a change in metabolism as opposed to an energy deficit, so conventional nutritional support is not effective.
Cachexia causes weight loss and increased mortality 1. Increases in pro-inflammatory factors characterize cachexia. There is a decreased quality of life, decreased tolerance to surgical or medical interventions, and shortened survival 2. The major cause is cytokine excess. Other mediators include testosterone and insulin-like growth factor-1 (IGF-1) deficiency, excess myostatin, and excess glucocorticoids 1.
Cachexia is more than simply loss of appetite though. It is a very complex problem and involves changes in the way your body normally uses protein, carbohydrate, and fat. It leads to many problems including muscle wasting.
Cachexia is very different to general weight loss. It can’t be completely reversed even if you feel like eating.
Trying to eat more or being fed through a tube may not help reverse it either. People suffering from cachexia do not seem to feel hungry.
The early recognition and intervention of cachexia improve quality of life and survival 3.
Scientists don’t know exactly what happens in cachexia. Scientists think that the cancer releases chemicals into the blood that contributes to the loss of fat and muscle.
These chemicals may make your metabolism speed up so that you use up calories faster. Because your body is using up energy faster than it is getting it, you can have severe weight loss even if you are eating normally.
Cachexia occurs with various diseases, especially those that are chronic and debilitating. Diseases commonly associated with cachexia are cancer, HIV/AIDS, congestive heart failure, chronic obstructive pulmonary disease (COPD), chronic kidney disease, chronic liver disease, chronic infections, osteoarthritis and chronic inflammatory rheumatological diseases (e.g. rheumatoid arthritis, systemic lupus erythematosus (SLE), scleroderma, polymyositis, etc). The cachexia prevalence ranges from 5% to 15% in congestive heart failure (CHF) or chronic obstructive pulmonary disease (COPD) to 60% to 80% in advanced cancer. Mortality rates of patients COPD and cachexia are 10% to 15% per year. In patients with cachexia and congestive heart failure or chronic kidney, disease mortality is 20% to 30% per year, and it is 80% in patients in cachectic cancer patients 4.
Disease stages have been described as pre-cachexia, cachexia, and refractory cachexia. Consensus definitions for these stages are as follows 1:
- Pre-cachexia, when weight loss more than 1kg but less than 5%
- Cachexia, when weight loss is more than 5% or when weight loss is more than 2% with body mass index (BMI) less than 20kg/m²
- Refractory cachexia, when weight loss is more than 15% with body mass index (BMI) less than 23kg/m² or when weight loss is more than 20% with BMI less than 27 kg/m²
Although the prognostic usefulness of these definitions has not been established, it would appear that addressing cachexia at an earlier stage might reduce the destructive effects of the primary condition.
Who gets cachexia?
It isn’t usual to get cachexia with the early stages of cancer. Up to 6 out of 10 people (60%) with advanced cancer develop some degree of cachexia. Recent data have confirmed that patients with muscle wasting in cachexia are particularly affected by reduced exercise capacity, strength, and quality of life 5.
Cachexia in advanced cancer can be very upsetting and make you feel very weak. It isn’t just associated with cancer though.
It is common in the advanced stages of other illnesses such as HIV/AIDS, congestive heart failure, chronic obstructive pulmonary disease (COPD), chronic kidney disease, chronic liver disease, chronic infections, osteoarthritis and chronic inflammatory rheumatological diseases (e.g. rheumatoid arthritis, systemic lupus erythematosus (SLE), scleroderma, polymyositis, etc).
Losing muscle and fat can make it look as though you are ‘wasting away’. This can all be made worse because of the side effects of cancer treatment you are having.
Is cachexia a sign of dying?
Cachexia is a complicated metabolic syndrome characterized by progressive loss of lean tissue or muscle mass loss with or without fat mass loss that is often associated with anorexia, an inflammatory process, insulin resistance, and increased protein turnover 1. Losses are often in excess to that explained by the associated anorexia.
Cachexia is generally thought not to be reversible in the short term with conventional nutritional supplementation. The syndrome is most often associated with certain types of cancer, but can be seen in other chronic diseases, such as HIV/AIDS, congestive heart failure, chronic obstructive pulmonary disease (COPD), chronic kidney disease, chronic liver disease, chronic infections, osteoarthritis and chronic inflammatory rheumatological diseases (e.g. rheumatoid arthritis, systemic lupus erythematosus (SLE), scleroderma, polymyositis, etc). The cachexia prevalence ranges from 5% to 15% in congestive heart failure (CHF) or chronic obstructive pulmonary disease (COPD) to 60% to 80% in advanced cancer.
Mortality rates of patients COPD and cachexia are 10% to 15% per year. In patients with cachexia and congestive heart failure or chronic kidney, disease mortality is 20% to 30% per year, and it is 80% in patients in cachectic cancer patients 4.
Cancer cachexia
In cancer patients, the overall prevalence of cachexia ranges from 40% at cancer diagnosis to 70% in advanced disease 1. In 20% to 25% of patients with advanced solid tumors, it is considered the primary cause of death in addition to being a significant comorbidity reducing median survival by up to 30%. Significantly shorter survival in advanced cancer patients with cachexia has been identified relative to those without cachexia.
Weight loss in cancer cachexia is different to weight loss in simple starvation , due to accelerated loss of muscle compared with fat tissue, presence of proinflammatory cytokines and prolonged acute phase protein response that contributes to increased resting energy expenditure and weight loss. Patients with cancer cachexia experience anorexia, early satiety, weakness, sarcopenia, fatigue, anaemia and severe weight loss.
Cancer-related cachexia can be broken down into 3 categories 3:
- Metabolic derangement
- Anorexia
- Alimentary tract dysfunction
The causes of cachexia can be related to the disease, treatment, or emotional distress. Nausea, early satiety, and dysgeusia are factors in anorexia.
Cancer cachexia causes
Cytokines
Mediators of cachexia associated with cancer include tumor necrosis factor-alpha, interleukins (IL) 1 and 6, ciliary neurotrophic factor, and leukemia inhibitory factor, and interferon (INF)-gamma. These produced by tumor cells and host immune cells. These are procachectic factors, as they lead to anorexia, weight loss, protein, and fat breakdown, an acute-phase protein response, falls in insulin level, insulin resistance, rises in levels of cortisol and glucagon, fever, anemia, and elevated energy expenditure 6.
Host immune cells including macrophages, T-helper-one cells, and myeloid-derived suppressor cells produce procachectic cytokines.
Many tumors cause an elevated adrenergic state that results in an increased rate of energy expenditure. Skeletal muscle is the primary s as part of a persistent inflammatory response. Tumors only produce proteolysis-inducing (PIF) factor. Tumor necrosis factor (TNF)-alpha and PIF induce cachexia by activating nuclear factor kappa B transcription factor found in muscles.ite of lean body mass depletion. This is secondary to increased protein turnover without equivalent protein synthesis.
The JAK/STAT3 pathway is strongly activated by the IL-6 family ligands. STAT3 activation by IL-6 is necessary for muscle wasting. Inhibition STAT3 pharmacologically using STAT3 or JAK inhibitors reduce muscle atrophy. This indicates that STAT3 is a primary mediator of muscle wasting when there is high IL-6 family signaling.
Anorexia and weight loss in cancer patients do not correlate with serum levels of circulating IL-1, IL-6, IFN-gamma, and TNF-alpha. There may be a central mechanism of action producing of cachexia. Cytokines postulated to be involved include TNF-alpha, IFN-alpha, IL-1, IL-6, IL-8, and others.
Serotonin and dysfunction of neuropeptidergic circuits may be involved. Elevated plasma-free tryptophan was observed in patients with cancer and anorexia. This elevates tryptophan levels in the cerebrospinal fluid resulting in increased synthesis of serotonin. Elevated levels of serotonin contribute to cancer anorexia.
Insulin and Ghrelin
Insulin and leptin levels are proportional to body fat content. Central nervous system (CNS) concentrations are proportional to plasma levels. Insulin secretion increases as weight increase. This occurs at the basal state and in response to meals. Leptin is more involved in central nervous system (CNS) control of energy homeostasis than insulin. Leptin deficiency causes obesity with hyperphagia. This persists despite high insulin levels.
Ghrelin function is a peptide produced by ghrelin cells in the gastrointestinal (GI) tract and acts in the central nervous system (CNS). Ghrelin is secreted when the stomach is empty. Secretion stops when the stomach is stretched. Ghrelin acts centrally to increase hunger, gastric acid, secretion and gastrointestinal motility. The same brain cells have receptors for ghrelin and leptin, with opposing effects.
Alimentary Tract Dysfunction
Cancer patients often have abnormalities in the taste and smell. Oral intake may be impaired by tumors of the mouth, neck, esophagus, stomach. Obstruction can occur to tumors of the pancreas, liver, and peritoneum. Intestinal obstruction is common. Enzymatic insufficiency secondary to pancreatic insufficiency may contribute to malabsorption. Lymphoma of the intestine or mesentery can result in issues.
Slowing of peristalsis and delayed gastric emptying contributes to early satiety. Chemotherapy commonly causes nausea vomiting, mucositis, and abnormal perception of taste. Stomatitis, alterations in taste and smell, and xerostomia often occur secondary to radiotherapy to the head and neck. Abdominal radiation therapy can cause nausea, vomiting, anorexia, diarrhea, and malabsorption 7.
Biochemical and Metabolic Derangement
Neoplastic cells have high levels of glucose utilization and production of lactic acid, the Warburg effect.Hexokinase is the first step of the glycolytic pathway and overexpressed in tumor cells contributes to this process. Tumor glycolysis and host gluconeogenesis may be an important cause of cancer cachexia.
Recently, an extensive re-examination of Warburg effects shows that unlike the majority of cells, numerous cancer cell lines obtain a significant portion of their energy from aerobic glycolysis. Many malignant cells secrete hydrogen peroxide, oxygen free radicals drives mitophagy, aerobic glycolysis, and autophagy.
Cancer cachexia life expectancy
In patients with cancer cachexia mortality is 80% per year 4.
Stages of cancer cachexia 8:
- In pre-cachexia, there is anorexia and metabolic change with a weight loss of 5% or less.
- In cachexia, the BMI is less than 20, weight loss is more than 2%, or systemic sarcopenia and weight loss more than 2%.
- In refractory cachexia, the cancer is usually unresponsive, performance score is low, and predicted survival is less than three months.
Cancer cachexia treatment
Removal of the tumor is the best treatment for cancer cachexia. When definitive treatment is not possible, there has been some success with multiple treatment modalities 9.
Supportive care
Intervention from the stage of pre-cachexia is best. Early nutritional intervention can improve nutritional status. This may reduce the inflammatory response. Stabilization of body weight during chemotherapy often results in reduced toxicity and longer overall survival. The following have all shown limited success.
- Antiemetics
- Exogenous pancreas extract
- Frequent small feedings
- Home-made food supplements may be better tolerated
- Oral and parenteral nutritional supplements
- Treatment of stomatitis
- Transfusions of blood components
Exercise
Exercise is safe during active cancer treatments. It improves muscle strength, bone health, and quality of life, while decreasing depression, fatigue, and psychosocial distress. Physical activity can reduce the risk of comorbidities negatively affecting cancer survivors. There is evidence indicating that exercise is associated with a reduction in overall mortality. Physical exercise can improve insulin sensitivity, modulate muscle metabolism, and reduce the inflammation. Exercise has anti-inflammatory benefits. It up-regulates anti-inflammatory cytokines in skeletal muscle and adipose tissue. Recommendations should be made for exercise early in the treatment of cancer. Physical therapy evaluation can be helpful. Caregiver participation improves compliance.
Medications
Multiple agents with different mechanisms of action can be used alone or in combination.
Olanzapine, a selective monoaminergic antagonist, has a strong affinity for dopamine and serotonin receptors. It has been used at low doses showing improvement in weight and nutritional status with a low incidence of side effects.
Ghrelin and its analogs, including anamorelin have been shown to be effective. Side effects included nausea and hyperglycemia.
Recombinant-human GH with insulin has been evaluated and showed improved whole-body protein net balance.
Anabolic androgenic steroids have been used to promote muscle growth and strength. Nandrolone decanoate was studied in patients with non-small cell lung cancer. The treated group had less weight loss, but survival was comparable. Fluoxymesterone, an anabolic steroid, was found to be inferior to megestrol acetate or dexamethasone.
Enobosarm (GTx-024) is an androgen receptor modulator. It has tissue-selective anabolic effects in muscle and bone. One study showed an increase in lean body mass.
Thalidomide suppresses TNF production in patients with cancer. It has been used in combination with medroxyprogesterone or megestrol acetate, oral eicosapentaenoic acid, and L-carnitine resulting a significant increase in lean body mass significantly, decreased fatigue, and improved appetite.
MABp1 (Xilonix; Xbiotech, Inc., Austin, TX) is a fully humanized, monoclonal anti-IL-1a antibody. It is a receptor antagonist that resulted in partial remission or stabilization of cachexia.
Corticosteroids have been found in uncontrolled studies to diminish anorexia, asthenia, and pain in patients with cancer. The improvements did not persist, and all nutritional status returned to baseline with no differences in mortality rate.
Megestrol acetate has been used historically. It improves appetite and increases body fat more than lean body mass. There is a reduction of serum levels of IL-1a and b, IL-2, IL-6, and TNF-a.
Medroxyprogesterone acetate is a synthetic progestagen that also has been used. It reduces production of cytokines and serotonin. It has been to increase appetite but not weight.
Metoclopramide can be used for patients with delayed gastric emptying or gastroparesis.
Dronabinol and Marijuana Dronabinol (Delta 9-tetrahydrocannabinol, THC) have been studied. Cannabinoids have not shown to be more effective than megestrol despite improved appetite.
The anti-tnf antibody has been studied with conflicting results.
Eicosapentaenoic acid was found to have antitumor and anti-cachexia activities in animal cachexia models, but randomized clinical studies show no unique benefit of EPA.
Myostatin inhibitors may be a new potential therapeutic target. Activin type-2 receptor (ActRIIB) has been used to treat of muscle wasting. ActRIIB is a high-affinity activin type 2 receptor that is known to mediate the signaling via a subset of TGF-b family ligands including myostatin, activin, GDF11, and others.
Bimagrumab is a fully humanized anti-ActRII monoclonal antibody that is to be studied for non-small cell lung cancer associated cachexia.
NSAIDs including indomethacin and celecoxib have not been shown to improve nutritional status.
Hydrazine sulfate is an inhibitor of the enzyme phosphoenolpyruvate carboxykinase. It interrupts gluconeogenesis in animals. Studies have shown no benefit.
Beta-hydroxy-beta-methyl butyrate with L-arginine and L-glutamine has been used for cachexia. HMB is a metabolite of leucine and interferes with the activation of NF-kB. In tumor-bearing mice, it inhibited PIF-induced protein degradation and attenuated the increased protein degradation.
OHR/AVR118 (OHR Pharmaceuticals, Inc., New York, NY) is a broad-spectrum peptide-nucleic acid immunomodulator is theorized to have cytoprotective properties. A study in patients with cancer showed stabilization of body mass and muscle mass, increased appetite, and enhanced quality of life.
Total parenteral nutrition (TPN) has not been shown to have significant benefit for patients undergoing chemotherapy or radiation therapy regarding tolerance, response, or survival.
Cardiac cachexia
Cardiac cachexia, which is characterized by loss of muscle, with or without loss of fat mass, is a serious and life-threatening complication of heart failure with reduced ejection fraction 10. Moreover, studies have demonstrated that it was an important independent prognostic factor for cardiovascular mortality after adjustment for age, left ventricular ejection fraction and functional capacity to perform physical activities 11. The presence of cardiac cachexia had been established as an independent risk factor for mortality in ambulatory patients with heart failure 12.
Treating wasting in patients with heart failure remains challenging. Approaches have included nutritional supplements 13, exercise training 14 and drug treatments 15.
Cachexia causes
Cachexia is characterized by a persistent increase in basal metabolic rate that is not compensated by increased caloric/protein intake 1. Factors involved in this abnormal metabolic cascade include digestive factors, tumor factors and hormonal responses to the primary disease 1. Digestive factors resulting in poor intake include dysgeusia, nausea, dysphagia, mucositis, and constipation. Tumor-mediated factors have been identified that activate proteolysis and lipolysis. Inflammatory mediators such as cytokines which include tumor necrosis factor and the interleukins induce anorexia while increasing glucagon, cortisol, and catecholamines producing a catabolic, hypermetabolic state. Hormonal anabolic mediators such as growth hormone, insulin-like growth factor-1 (IGF-1), testosterone, and ghrelin are reduced. In heart failure, angiotensin-2 causes muscle wasting likely through the ubiquitin-proteasome system, resulting in myocyte apoptosis and significant reduction of protein synthesis. Asthenia results in part from subsequent decreases in size and number of type 1 and type 2 muscle fibers and also reduced skeletal blood flow.
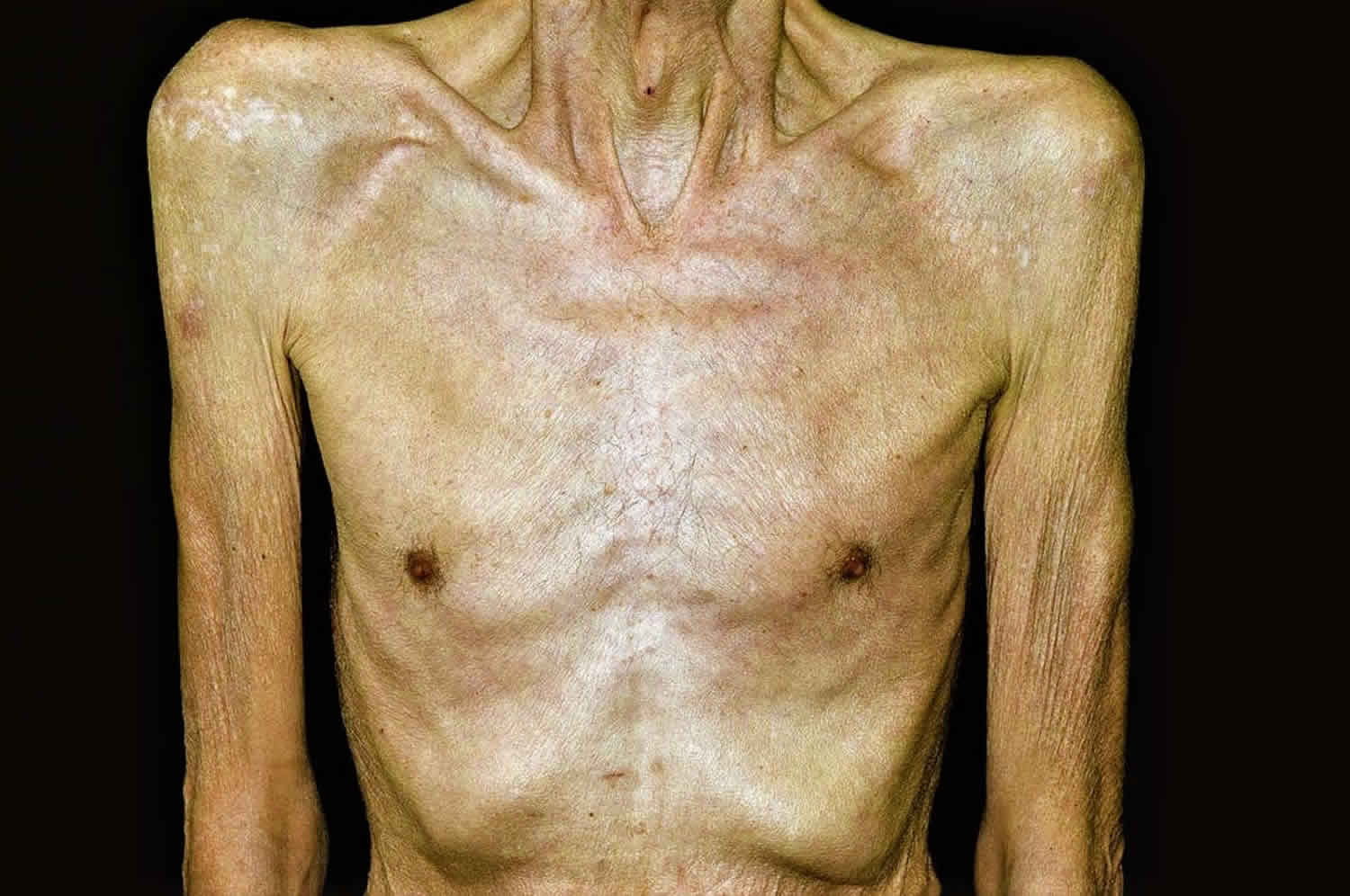
Cachexia symptoms
Cachexia seems to be more common in people with lung cancer or with cancers anywhere in the digestive system. The main symptoms are:
- severe loss of weight, including loss of fat and muscle mass
- loss of appetite
- feeling sick (nausea)
- feeling full after eating small amounts
- anemia (low red blood cells)
- weakness and fatigue
Cachexia survival time
Mortality rates of patients COPD and cachexia are 10% to 15% per year. In patients with cachexia and congestive heart failure or chronic kidney, disease mortality is 20% to 30% per year, and it is 80% in patients in cachectic cancer patients 4.
Cachexia diagnosis
There are no definitive methods for diagnosis of cancer cachexia. Clinical signs of anorexia and weight loss ≥5% in 6 months would be expected but clinical judgement is required. History frequently includes a report of significant weight loss associated with the lack of appetite. Also, there is a reduction of quality of life associated with increased fatigue and poor tolerance to activity. In advanced cancer patients, cachexia is correlated with increased severity of multiple symptoms. These include lack of appetite, dry mouth, vomiting, dysgeusia, early satiety, and diarrhea. It also increases the severity of less intuitive symptoms such as pain, fatigue, and loss of energy, sleep disturbances, and anxiety. This excess symptom burden is independent of age, tumor stage, and treatment type. Diagnostic criteria for cachexia are a 5% weight loss in 12 months or a body mass index of less than 20 kg/m² in the presence of a known chronic disease with at least 3 of the following factors:
- Loss of muscle mass,
- Asthenia (lack of energy)
- Loss of body fat, in the presence of inflammation as evidenced by albumen less than 3.2 g/dL or increased C–reactive protein.
The physical exam is nonspecific. Exam findings may be normal early in the course of the disease. Other findings might include bitemporal muscle wasting, supraclavicular wasting, and general lack of muscle definition.
Supporting laboratory evidence includes albumen less than 3.2 g/lL, a pre-albumin value of less than 10 mg/dL, a transferrin level less than 100 mg/dL, and an elevated C–reactive protein.
Cachexia treatment
The cause of the cachexia is multifactorial and is best managed by a multidisciplinary team that consists of an oncologist, dietitian, social worker, pharmacist, physical therapist and a mental health counselor. The key is to recognize the problem early, when treatment is most successful. Even though there are many pharmacological agents that may help boost appetite, long-term studies on the effectiveness of these agents are lacking. At a minimum, the patient should be seen by a dietitian and a therapist. Improving the mood and offering supportive services may also help.
Treatment of cachexia should be directed towards:
- Treatment of underlying disease
- Controlling the symptoms of cachexia
Cachexia treatment involves adding more calories to your diet to help you put on weight and increase your protein intake for growth and repair.
Treatment of underlying disease
A multimodal approach aimed at improving appetite, reducing the inflammatory response, improving outcomes and quality of life is the focus of ongoing research. Currently, no proven therapy accomplishes all of these goals 1. Most of the research has focused on improving appetite. Adequate nutrition remains an important aspect of this multimodal approach. However, increasing calorie–protein intake by definition does not reverse this abnormal metabolic state. Reversing the metabolic derangement through attenuation of tumor-related.
Factors and inflammatory mediators remain of central importance. Studies indicate that interleukin-6 has a primary role in initiating inflammatory cascade along with the contribution of tumor necrosis factor-alpha and other cytokines. Interventions that are used or that are under current investigation may be useful theoretically due to their effects on this inflammatory cascade, abnormal hormone responses, and/or the hypermetabolic derangements seen in cachexia.
Physical activity may attenuate the effects of cachexia by altering muscle metabolism through increased protein synthesis and reduced degradation pathways. In addition, exercise may increase insulin sensitivity, reduce oxidative stress, and reduce response to inflammation. Both aerobic exercise and resistance exercise have proven beneficial. Resistance exercise supplemented with branched-chain amino acids can reduce sarcopenia and cachexia.
The most studied and effective treatment for anorexia has been megestrol acetate and a dose of 320 mg to 800 mg per day 1. The literature supports that 30% of patients demonstrate an increased appetite associated with an increased body mass index primarily through increased fat and some associated improvement in the quality of life. However, no study has demonstrated improved survival. Side effects include adrenal suppression and increase the incidence of DVT in a minority of patients. Corticosteroid has been shown to have a positive effect on appetite but, due to side effect profile, is only indicated for short-term (less than 4 weeks) treatment. In addition to appetite stimulation, steroids theoretically may reduce the inflammatory state.
Other medications that require additional confirmation includes cannabinoids (only effective in AIDS so far), non-steroidal anti-inflammatory drugs, and omega-3 fatty acids. Existing evidence suggests it is reasonable to initiate a trial of omega-3 fatty acids in patients with life expectancies longer than 8 weeks. Other medications including Ghrelin, beta-2 agonists, selective androgen receptor modulators, aliskiren, resveratrol, leucine, and thalidomide are all under active investigation with some positive early trends.
In patients with cardiac cachexia, treatment with the beta-blocker carvedilol has demonstrated meaningful reversal of cachexia 1. This may be in part due to improvement in the hypermetabolic state seen in cachexia. Pre-clinical studies suggest that ACE-inhibitors and angiotensin 2 receptor blockers have muscle-protective properties related to mitochondrial function, insulin sensitivity, and local inflammation.
Pharmacologic Management
Multiple agents with different mechanisms of action can be used alone or in combination.
Olanzapine, a selective monoaminergic antagonist, has a strong affinity for dopamine and serotonin receptors. It has been used at low doses showing improvement in weight and nutritional status with a low incidence of side effects.
Ghrelin and its analogs, including anamorelin have been shown to be effective. Side effects included nausea and hyperglycemia.
Recombinant-human GH with insulin has been evaluated and showed improved whole-body protein net balance.
Anabolic androgenic steroids have been used to promote muscle growth and strength. Nandrolone decanoate was studied in patients with non-small cell lung cancer. The treated group had less weight loss, but survival was comparable. Fluoxymesterone, an anabolic steroid, was found to be inferior to megestrol acetate or dexamethasone.
Enobosarm (GTx-024) is an androgen receptor modulator. It has tissue-selective anabolic effects in muscle and bone. One study showed an increase in lean body mass.
Thalidomide suppresses TNF production in patients with cancer. It has been used in combination with medroxyprogesterone or megestrol acetate, oral eicosapentaenoic acid, and L-carnitine resulting a significant increase in lean body mass significantly, decreased fatigue, and improved appetite.
MABp1 (Xilonix; Xbiotech, Inc., Austin, TX) is a fully humanized, monoclonal anti-IL-1a antibody. It is a receptor antagonist that resulted in partial remission or stabilization of cachexia.
Corticosteroids have been found in uncontrolled studies to diminish anorexia, asthenia, and pain in patients with cancer. The improvements did not persist, and all nutritional status returned to baseline with no differences in mortality rate.
Megestrol acetate has been used historically. It improves appetite and increases body fat more than lean body mass. There is a reduction of serum levels of IL-1a and b, IL-2, IL-6, and TNF-a.
Medroxyprogesterone acetate is a synthetic progestagen that also has been used. It reduces production of cytokines and serotonin. It has been to increase appetite but not weight.
Metoclopramide can be used for patients with delayed gastric emptying or gastroparesis.
Dronabinol and Marijuana Dronabinol (Delta 9-tetrahydrocannabinol, THC) have been studied. Cannabinoids have not shown to be more effective than megestrol despite improved appetite.
The anti-tnf antibody has been studied with conflicting results.
Eicosapentaenoic acid was found to have antitumor and anti-cachexia activities in animal cachexia models, but randomized clinical studies show no unique benefit of EPA.
Myostatin inhibitors may be a new potential therapeutic target. Activin type-2 receptor (ActRIIB) has been used to treat of muscle wasting. ActRIIB is a high-affinity activin type 2 receptor that is known to mediate the signaling via a subset of TGF-b family ligands including myostatin, activin, GDF11, and others.
Bimagrumab is a fully humanized anti-ActRII monoclonal antibody that is to be studied for non-small cell lung cancer associated cachexia.
NSAIDs including indomethacin and celecoxib have not been shown to improve nutritional status.
Hydrazine sulfate is an inhibitor of the enzyme phosphoenolpyruvate carboxykinase. It interrupts gluconeogenesis in animals. Studies have shown no benefit.
Beta-hydroxy-beta-methyl butyrate with L-arginine and L-glutamine has been used for cachexia. HMB is a metabolite of leucine and interferes with the activation of NF-kB. In tumor-bearing mice, it inhibited PIF-induced protein degradation and attenuated the increased protein degradation.
OHR/AVR118 (OHR Pharmaceuticals, Inc., New York, NY) is a broad-spectrum peptide-nucleic acid immunomodulator is theorized to have cytoprotective properties. A study in patients with cancer showed stabilization of body mass and muscle mass, increased appetite, and enhanced quality of life.
Total parenteral nutrition (TPN) has not been shown to have significant benefit for patients undergoing chemotherapy or radiation therapy regarding tolerance, response, or survival.
Controlling the symptoms of cachexia
Several treatment options have been outlined to treat cachexia. The principle is to improve the nutrition of the patients and to suppress the inflammatory response that is eating up the body’s energy. These include:
- Feeding the patient with high calorie food
- Drugs to stimulate the appetite
- Drugs to stimulate the body to build up more muscle mass
- Exercise
It has been proposed that eicosapentaenoic acid (EPA), an omega-3 polyunsaturated fatty acid, may reduce the production of proinflammatory cytokines and thus may improve energy and protein intake, performance status and quality of life in cancer patients with cachexia. This may be taken as fish oil capsules or commercial nutrition supplements. However, the results of studies into the effects of eicosapentaenoic acid (EPA) have been inconsistent. Your dietitian can provide more information about the dietary management of cancer cachexia.
Benefits of using fish oil:
- fish oil is natural
- non-toxic at recommended doses
- relatively inexpensive
- readily available.
Fish oil intake:
To achieve the recommended intake of 1.4–2.0 grams of eicosapentaenoic acid (EPA) per day 16, you need to consume:
- 8-11 fish oil capsules containing 180 mg EPA/capsule, or
- 8-11 mls (2 teaspoons) of fish oil that contains 180 mg EPA/ml, or
- 300-400 grams of oily fish per day (salmon, mackerel, sardines), or
- 310-445 ml of a high energy supplement enriched with EPA (0.45g EPA/100 ml), e.g., Resource Support, Prosure
- or a combination of the above.
Supplementation for no less than four weeks to see benefits.
Potential risks of using fish oils:
- Caution needs to be exercised in clients on anti-coagulant medication as effects may be amplified.
- Large doses may have potential gastrointestinal symptoms such as diarrhea, reflux, bad taste, and nausea.
- Cod liver and halibut liver oil are not suitable as they contain a higher level of vitamin A, which could lead to toxicity.
- Fish oils are not a major source of mercury.
- Mercury can accumulate in fresh fish. Shark (flake), billfish (swordfish/broadbill and marlin) should be limited to once per week and no other fish that week.
Exercise
Exercise is safe during active cancer treatments. It improves muscle strength, bone health, and quality of life, while decreasing depression, fatigue, and psychosocial distress. Physical activity can reduce the risk of comorbidities negatively affecting cancer survivors. There is evidence indicating that exercise is associated with a reduction in overall mortality. Physical exercise can improve insulin sensitivity, modulate muscle metabolism, and reduce the inflammation. Exercise has anti-inflammatory benefits. It up-regulates anti-inflammatory cytokines in skeletal muscle and adipose tissue. Recommendations should be made for exercise early in the treatment of cancer. Physical therapy evaluation can be helpful. Caregiver participation improves compliance.
The role of physical activity in relation to health and the reduced risk of developing cancers is well documented. Exercise increases insulin sensitivity and the rate of protein synthesis. According to Ardies 17 exercise exerts a positive effect on the body’s immune response and in addition attenuates the inflammatory response, which triggers the cachexia cascade.
Progressive resistance training has a positive effect on lean tissue mass, muscular strength and function and has been found useful in counteracting some of the negative consequences of muscle wasting in a variety of populations 18.
Research suggests negative psychological effects stem from fatigue and the inability to perform activity of daily living, which leads to reduced quality of life. For those clients who are motivated and well enough, increasing muscle mass reduces fatigue, which directly affects their ability to perform activity of daily living and therefore has the potential to increase their quality of life 19.
Your physiotherapist will advise on which exercises are suitable, how many sets and the number of repetitions. There is also an option for bed bound clients.
Boosting energy and protein in everyday foods
There are ways to boost the energy (calories) and protein in everyday foods to help with weight loss due to cancer or its treatment.
Eating more calories gives you the energy to help you to regain the weight you have lost. Extra energy may be helpful if you have higher nutritional needs due to cancer treatment.
Protein is important for growth and repair of tissues and the immune function. A higher protein intake will help you to put on weight.
Protein requirements: Recommendations for cachexia are 1.2–2.0g/kg/day 20 e.g., 60kg person: 60 x (1.2–2.0) = 72–120 grams protein/day.
Example of what 72 grams of protein looks like over one day:
- 3/4 cup milk (on cereal)
- + 1 tin of salmon (95g)
- + 2 slices of bread
- + 60g whey powder added to 1 cup of milk
- + 50 grams meat/chicken.
Eating a high calorie (kcal) and protein diet is something that you might find difficult. Some of the suggestions here may seem to go against healthy eating messages. But don’t worry. You can return to a lower energy diet once your appetite and weight have recovered.
You will feel better and have more energy if you can get back up to a normal weight for your height and build.
Get advice on regaining weight
Speak to your doctor if swallowing problems are making eating and drinking hard. Your doctor may refer you to a speech and language therapist.
The therapist check that your swallowing is safe. Also, that food or drink is not going down the wrong way. They might suggest that you stick to eating soft foods. Or they might tell you about the types of textures that are better for you.
Everyone is different. One person may be able to eat certain foods that cause problems for another. Some people may not be able to manage high fibre foods such as vegetables and grains. People vary in the type of textures of different foods they like.
There are different ways of putting weight on. You can try to eat a diet that is higher in energy and protein. And you can drink nourishing fluids to supplement your diet.
You might need some specific advice from a dietician. You can ask your hospital doctor or nurse to refer you.
Ask your doctor or nurse to refer you to a dietician at your local hospital. They might suggest that you try liquid supplements to boost your diet.
Every hospital and most cancer centers have a dietitian who can tell you what to do.
Remember that fat is the best way to get concentrated calories. But after surgery to your stomach, pancreas or bowel, you may find it difficult to cope with high-fat foods. In these cases, you definitely need help and advice from your dietitian.
Eating regularly
Try to eat regular, smaller meals and snacks, every 2 hours or so. Do this by the clock rather than waiting until you feel hungry. Try to include protein at each meal including breakfast.
It is better to eat something regularly than to try to eat one big meal and only manage a few mouthfuls.
Tips to boost energy and protein in everyday foods
There are various ways of adding calories and protein to your meals and snacks. Remember to choose full fat and high-calorie options whenever you can.
Foods that contain protein are:
- red meat like pork, lamb and beef
- white meat like turkey and chicken
- meat alternatives like tofu, quorn and soya
- fish and shell fish
- eggs
- beans, lentils, chickpeas and other pulses or legumes
- milk, yogurt and cheese
Below are some ways you can boost your diet.
Use full fat and fortified milk and butter
- Use full cream milk instead of semi-skimmed.
- Put 2 to 4 tablespoons of milk powder into a pint of full cream milk to make fortified milk. Use it instead of regular milk.
- Always use plenty of butter or margarine where you can.
Drinks
- Make milky coffee (or use fortified milk).
- Add fortified milk to tea and coffee, or bedtime drinks such as Horlicks, Ovaltine or drinking chocolate.
- Try buttermilk as a drink.
Breakfast
- Soak porridge oats with added sugar overnight in full cream milk. This softens them and makes them easier to eat.
- Add dried fruit or seeds to boost nutrients and calories in your cereal. About 75g (or 3oz) of oats treated this way will give you about 500 calories.
- Add toppings like cheddar or full fat cream cheese and baked beans, kippers or scrambled eggs with extra butter on toast.
Snacks
- Keep snacks like nuts, pasteurized cheese, fresh and dried fruit, biscuits, crackers, yogurts or fromage frais handy to nibble at.
- Make sure you buy full fat fromage frais and yogurt.
- Spread fillings thickly in sandwiches.
- Add a dessertspoon of mayonnaise to sandwich fillings such as hard boiled egg or tuna.
- Snack on quiche, hard boiled eggs or chicken pieces dipped into mayonnaise.
Sauces and soups
- Make up packet sauces or soups with milk (or fortified milk) instead of water.
- Make sauces with milk instead of water, or fortified milk instead of standard milk.
- Stir a tablespoon of cream or full fat yogurt into canned soups.
- Add plenty of pulses or meat to stews and casseroles.
Vegetables
- Mix grated cheese or cream with mashed potato.
- Melt butter on top of hot vegetables or garnish with grated cheese or chopped hard-boiled egg.
- Serve vegetables with a sauce made with fortified milk.
Desserts
- Add ice cream, cream or evaporated milk to cold puddings.
- Add custard made with fortified milk to hot puddings.
- Add sugar, glucose powder, honey or syrup to desserts.
- Try lassi made with fortified milk.
Drinking nourishing fluids
Have nourishing drinks such as milky drinks and smoothies. Drinking only water, squash or tea can fill you up without giving you many calories or any protein. Any milk-based drink gives you calories and protein.
Your dietitian may suggest high energy supplement drinks to have between meals.
Adding energy and protein to a soft diet
There are ways to add energy (calories) and protein to a soft diet.
A soft diet
If you need a soft diet, you might sometimes find it hard to eat all the protein and calories that you need.
A soft diet means you often have to add water to food to soften it. This adds bulk and reduces the nutritional value and flavor of the food. But there are ways of increasing calories in a soft diet.
Tips for boosting energy and protein
You can increase your calorie intake and improve your strength and energy levels by trying the following tips:
- Use whole milk and not skimmed or semi-skimmed.
- Boost the protein content of whole milk by adding a couple of tablespoons of dried milk powder to a pint. Use this exactly as ordinary milk for drinking and cooking.
- Porridge is a very nutritious breakfast – make it with whole or fortified milk, and add syrup or sugar and cream.
- Mash vegetables with milk and add some grated cheese and egg.
- Make up instant soups with milk instead of water, and top with grated cheese or cream.
- Add minced meat, lentils, beans, noodles or pasta shapes to soups.
- Add cheese and a little cream to an omelette.
- Dip cooked, soft vegetables in dips such as hummus or sour cream.
- Make coffee, hot chocolate or Horlicks with full fat milk and enrich with a spoonful of cream. And dunk your favorite biscuits.
- Make milkshakes with build up drinks, ice cream, yogurt and fresh fruit – banana with a chocolate build up drink is delicious.
High calorie drinks
You can boost your diet by having high calorie and protein drinks.
Making your own
You can make your own energy filled drinks by liquidizing combinations of milk, fresh fruit, yogurt, honey or sugar and ice cream as a smoothie or milkshake.
Smoothies
Use fresh apple, strawberries, banana or other soft fruit. Blend it with fortified milk, fruit juice or yogurt in a liquidizer or blender.
Smoothies made with fruit juice will have much less protein. So they are less nutritious than those based on milk or yogurt. Supermarkets sell mixed fruit and frozen smoothie mixes. These work well if you are making your own.
Try adding a handful of pumpkin or sesame seeds to add a few extra calories. The best thing about making your smoothies is that they usually taste great. You can also control the flavor.
Milkshakes
Make a nutritious milkshake by mixing fortified milk with either puréed fruit or a fruit yogurt. Top with a scoop of ice cream for extra energy.
Make a chocolate and banana milkshake. Use chocolate flavor milk and whizz in a blender with a banana. This is delicious and nutritious and easy to eat if you can’t face a meal.
Ready made drinks (liquid supplements)
High calorie meals in a drink or energy drinks are also called liquid food supplements or sip feeds.
They can be useful short term if your appetite is poor and you can’t manage to take in enough nourishment. You can use them to replace a meal or to boost your calorie intake between meals.
Many come in different flavours such as chocolate, vanilla, strawberry and banana. There are also savoury ones in the form of soups. Your dietitian can suggest recipes or other ways to make supplements more palatable.
There are several ready-made commercial brands available on the market. You can buy these from your chemist, but they are quite expensive. Your doctor can give you a prescription for them. Prescriptions are free if you live in Scotland, Wales and Northern Ireland. In England, if you have cancer, you can apply to get them for free.
Some ready-made drinks have enough nutrients and calories in them to replace your meals. But it is always best to carry on eating if you can.
In most cases, you have these between meals and carry on with your normal diet as well. You will boost your nutritional intake if you drink between 2 and 3 cartons a day.
Do not take more than your doctor or dietitian recommends. The drinks contain vitamins that could be harmful in large amounts. Tell your doctor, dietitian or pharmacist if you are taking any vitamin supplements.
You may need to avoid taking certain medicines soon after or before having the drinks. The drink may change how much you absorb of the medicine. Ask your pharmacist or dietitian about when to take your medicines and when to have the drinks.
Some drinks should be used alongside meals, to give you more energy. There are 2 types of liquid supplements.
Balanced supplements
You can buy these supplements over the counter and in some supermarkets. They come as a powder that you make up into milkshakes, soups, hot drinks or cold drinks.
They include products such as Meritene and Complan.
Complete meal supplements
These products contain the nutrients to replace a meal. Your doctor, GP or dietitian can prescribe them. A district nurse or specialist nurse can help arrange a prescription for you.
It’s possible to buy them yourself but they are expensive. If you use them you should be monitored by your doctor or dietitian. These supplements come as a liquid in a carton or bottle, and are either milkshake style or fruit juice style.
Some examples of milk based supplements:
- Ensure Plus
- Fresubin Energy
- Fortisip
- Resource shake
- Ensure Plus Yoghurt Style
- Fortifresh Yoghurt Style
- Clinutren
Some examples of fruit based supplements:
- Ensure Plus Juce
- Fortijuce
- Clinutren Fruit
- Resource Fruit
- Provide Xtra
Protein and energy supplements
These products are powders or liquids. They contain either energy or protein with a small amount of energy. You can add them to many different foods and drinks. They are not nutritionally balanced and not suitable as a meal replacement. But they are helpful to boost either energy or protein levels.
When taking these products, you should still eat and drink normally if possible. The products can be expensive, so it’s best for your doctor to prescribe them if you need them.
Protein supplements
Protein-only supplements should only be used if your doctor prescribes them for you.
- Maxipro
- Protifar
- ProSource
- ProCal shot
Energy supplements
- Polycal
- Maxijul
- Calogen
- Liquigen
- Baker Rogers J, Minteer JF. Cachexia. [Updated 2018 Oct 27]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2018 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK470208[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Del Fabbro E. Combination therapy in cachexia. Ann Palliat Med. 2018 Aug 27[↩]
- Ohnuma T, Adigun R. Cancer, Anorexia and Cachexia. [Updated 2018 Dec 2]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2018 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK430977[↩][↩]
- Barajas Galindo DE, Vidal-Casariego A, Calleja-Fernández A, Hernández-Moreno A, Pintor de la Maza B, Pedraza-Lorenzo M, Rodríguez-García MA, Ávila-Turcios DM, Alejo-Ramos M, Villar-Taibo R, Urioste-Fondo A, Cano-Rodríguez I, Ballesteros-Pomar MD. Appetite disorders in cancer patients: Impact on nutritional status and quality of life. Appetite. 2017 Jul 01;114:23-27.[↩][↩][↩][↩]
- Emami A, Saitoh M, Valentova M, Sandek A, Evertz R, Ebner N, Loncar G, Springer J, Doehner W, Lainscak M, Hasenfuß G, Anker SD, von Haehling S. Comparison of sarcopenia and cachexia in men with chronic heart failure: results from the Studies Investigating Co‐morbidities Aggravating Heart Failure (SICA‐HF). Eur J Heart Fail 2018; 20: 1580–1587[↩]
- Tsai VWW, Husaini Y, Sainsbury A, Brown DA, Breit SN. The MIC-1/GDF15-GFRAL Pathway in Energy Homeostasis: Implications for Obesity, Cachexia, and Other Associated Diseases. Cell Metab. 2018 Sep 04;28(3):353-368[↩]
- Zhang F, Shen A, Jin Y, Qiang W. The management strategies of cancer-associated anorexia: a critical appraisal of systematic reviews. BMC Complement Altern Med. 2018 Aug 09;18(1):236.[↩]
- Fearon K, Strasser F, Anker SD, et al. Definition and classification of cancer cachexia: an international consensus. Lancet Oncol 2011;12:489-95[↩]
- Hagmann C, Cramer A, Kestenbaum A, Durazo C, Downey A, Russell M, Geluz J, Ma JD, Roeland EJ. Evidence-based Palliative Care Approaches to Non-pain Physical Symptom Management in Cancer Patients. Semin Oncol Nurs. 2018 Aug;34(3):227-240.[↩]
- Adropin and Irisin in Patients with Cardiac Cachexia. Arq Bras Cardiol. 2018 Jul; 111(1): 39–47. doi: 10.5935/abc.20180109 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6078358[↩]
- Mechanisms for cachexia in heart failure. Pureza V, Florea VG. Curr Heart Fail Rep. 2013 Dec; 10(4):307-14.[↩]
- Anker SD, Ponikowski P, Varney S, Chua TP, Clark AL, Webb‐Peploe KM, Harrington D, Kox WJ, Poole‐Wilson PA, Coats AJ. Wasting as independent risk factor for mortality in chronic heart failure. Lancet 1997; 349: 1050–1053.[↩]
- Burden ST, Gibson DJ, Lal S, Hill J, Pilling M, Soop M, Ramesh A, Todd C. Pre‐operative oral nutritional supplementation with dietary advice versus dietary advice alone in weight‐losing patients with colorectal cancer: single‐blind randomized controlled trial. J Cachexia Sarcopenia Muscle 2017; 8: 437–446.[↩]
- von Haehling S, Ebner N, Dos Santos MR, Springer J, Anker SD. Muscle wasting and cachexia in heart failure: mechanisms and therapies. Nat Rev Cardiol 2017; 14: 323–341.[↩]
- von Haehling S. Casting the net broader to confirm our imaginations: the long road to treating wasting disorders. J Cachexia Sarcopenia Muscle 2017; 8: 870–880.[↩]
- Bauer, J, Ash, S, Davidson, W et al 2005, ‘Evidence based practice guidelines for nutritional management of cancer cachexia’.[↩]
- Ardies, CM 2002, ‘Exercise, cachexia, and cancer therapy: A molecular rationale’, Nutrition and Cancer, vol. 42, no.2, pp.143-157.[↩]
- Little, JP & Phillips, SM 2009, ‘Resistance exercise and nutrition to counteract muscle wasting’ Applied Physiology, Nutrition and Metabolism, vol.34, pp.817-828.[↩]
- Oldervoll, L, Loge, J, Paltiel, PT et al. 2006, ‘The effect of a physical exercise program in palliative care: A phase II study.’ Journal of Pain and Symptom Management, vol.31, no.5, pp.421-430.[↩]
- Arends, J, Bodoky, G, Fearon, K et al. 2006, ‘ESPEN guidelines on Enteral nutrition: Non-surgical oncology’, Clinical Nutrition, vol.25, pp.245-259.[↩]





{kind=link}