Contents
What is central cord syndrome
Central cord syndrome also known as central cervical cord syndrome is the incomplete injury to the spinal cord with a pattern of resultant neurological deficits characterized by impairment in the arms and hands and to a lesser extent in the legs (Figures 1 and 2) 1, 2, 3. Spinal cord pathology is primarily associated with the medial portion of the lateral corticospinal tract in the cervical spine 4. An incomplete spinal cord injury means that the ability of the spinal cord to convey messages to or from the brain is not completely lost. Additionally, some sensation (even if it’s faint) and movement is possible below the level of injury. The brain’s ability to send and receive signals to and from parts of the body below the site of injury is reduced but not entirely blocked. Central cord syndrome is associated with damage to the large nerve fibers that carry information directly from the cerebral cortex to the spinal cord. These nerves are particularly important for hand and arm function. Central cord syndrome results in motor deficits that are worse in the upper extremities when compared to the lower extremities, as well as bladder dysfunction (retention) with varying sensory deficits below the level of injury 5. The typical neurological deficit is symmetrical incomplete quadriplegia affecting the upper limbs more than the lower limbs; sensory impairment is variable and urinary retention is common 6. Because of its unique clinical presentation, central cord syndrome is also described in the differential diagnosis of “man in a barrel” syndrome 3. The degree of clinical presentation is quite variable and corresponds to the extent of the injury to the nerve root. The extent of neurological deficit often correlates with surgical urgency 7.
Central cord syndrome is the most common type of incomplete cord injury and almost always occurs as a result of a traumatic hyperextension injury of the cervical spine leading to spinal cord impingement 8. Central cord syndrome commonly affects older adults with underlying cervical spondylosis who sustain a hyperextension injuries most commonly from a fall and may occur with or without fracture and dislocations 9, 10. While central cord syndrome is more classically seen in the spondylotic elderly spine there have been cases reported of central cord syndrome in patients with normal canal diameter. In these cases extreme cervical hyper flexion may result in a vascular mediated cord injury 11.
The proposed mechanism of action involved in central cord syndrome is hyperextension of the cervical spine resulting in anteriorly simultaneous compression of the spinal cord, either by bony spurs from anterior osteophytes or intervertebral disc material and posteriorly by the buckling of the ligamentum flavum resulting in acute focal spinal cord compression with resultant hemorrhage and spinal cord edema 7. This theory was aligned with early myelogram studies performed on cadavers 12, 13. Initially, Schneider et al. 14 postulated that spinal cord compression caused central hemorrhaging, resulting in adjacent white matter compression. Schneider 14 believed that the upper limbs were more affected than the lower limbs because of the somatotropic organization of the lateral corticospinal tract, with arm function lying more medial within the tract. Neuroanatomic studies have since shown a diffuse distribution of upper and lower limb nerve fibers within the corticospinal tract, leading to the possibility that the unique presentation of central cord syndrome is due more to the hand and upper limb being more densely represented within the lateral corticospinal tract 15. More recent studies have revealed intact gray matter without evidence of hemorrhage within the central canal. Conversely, white matter axonal disruption, particularly in the lateral corticospinal tracts, appears to be the primary feature 16.
There are approximately 300,000 individuals living with spinal cord injury in the United States, with approximately 18,000 new cases annually 17. The approximate annual incidence of central cord syndrome is 11,000 cases per year in the United States 15.
Central cord syndrome symptoms may include paralysis or loss of fine control of movements in the arms and hands, with relatively less impairment of leg movements. Sensory loss below the site of the injury and loss of bladder control may also occur, as well as painful sensations such as tinging, burning, or dull ache. The overall amount and type of functional loss is dependent upon the severity of nerve damage. Central cord syndrome is usually the result of trauma that causes damage to the vertebrae in the neck or herniation of the vertebral discs. Central cord syndrome also may develop in persons over the age of 50 due to gradual weakening of the vertebrae and discs, which narrows the spinal column and may contribute to compression of the spinal cord when the neck is hyper-extended.
There is no cure for central cord syndrome although some people recover near-normal function. There is no standard course of treatment, although drug therapy, surgery, and rest are often part of the program. Magnetic resonance imaging (MRI) is used to indicate the degree of spinal cord compression and vertebral instability. Vertebral instability due to acute traumatic injury or cervical disc herniation is often treated by surgery to prevent further damage to the spinal cord. Recent reports indicate that earlier surgery may improve chances for recovery. Numerous recent studies suggest that surgery also can be beneficial in individuals with persistent compression of the spinal cord and ongoing neurological deterioration.
Figure 1. Spinal cord anatomy
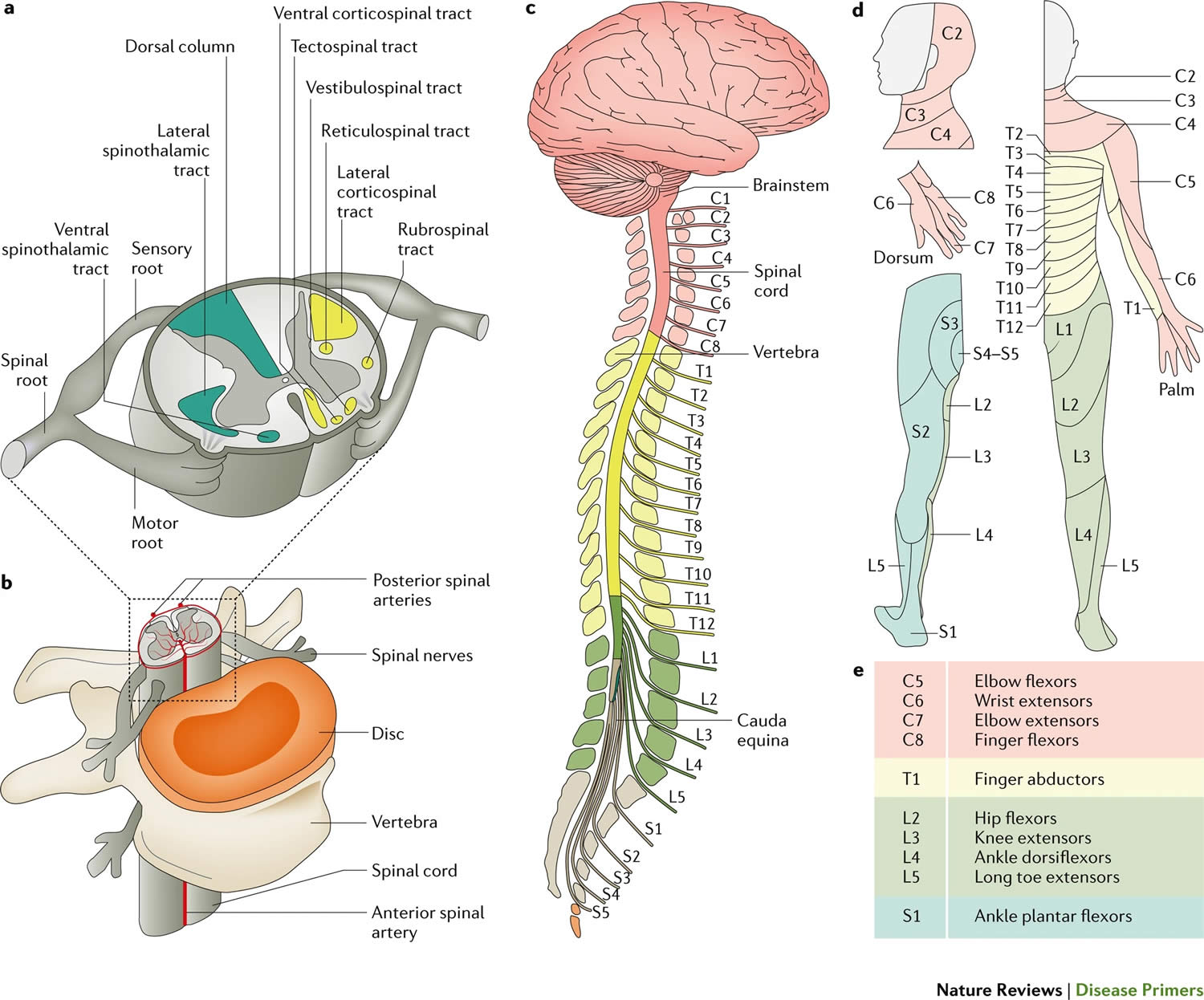
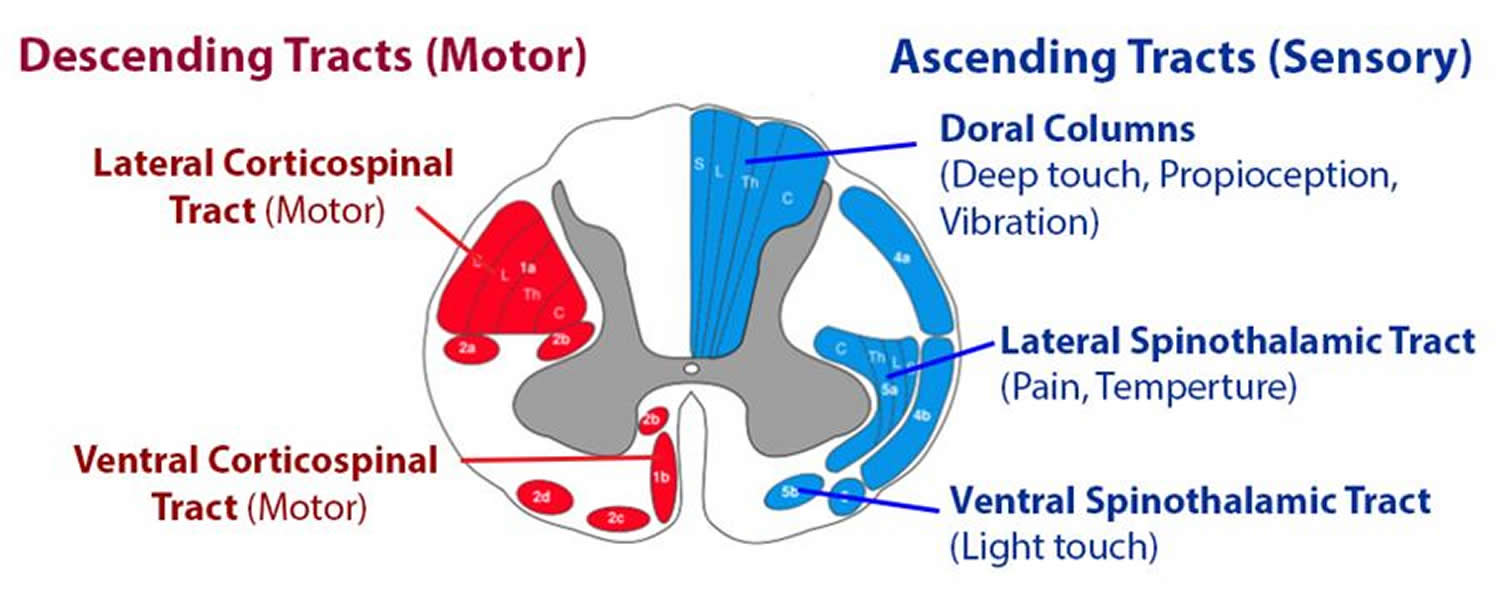
Footnotes: (a) The spinal cord itself is organized into grey matter (which contains neuronal cell bodies) and white matter (which contains myelinated axons). The white matter can be further subdivided into several ascending or descending tracts, which are composed of bundles of axons that originate from and project to specific regions in the brain and periphery. These tracts transmit specific information, such as sensory information (for example, temperature or itch) or motor information. Spinal nerve roots enter the spinal cord and either convey sensory information to the spinal cord (through the sensory or dorsal root) or convey motor information to the periphery (through the motor or ventral root). (b) The vertebral column encircles the spinal cord in protective bone and ligament, which, in humans, is segmented into 7 cervical, 12 thoracic, 5 lumbar and 5 sacral vertebrae. Blood is supplied to the spinal cord by the spinal arteries, which are located anteriorly and posteriorly and branch to perfuse the spinal cord parenchyma. The spinal cord is also surrounded by a protective layer of cerebrospinal fluid contained within the pachymeninges. (c–e) Each segmental region of the spinal cord (part c) innervates a specific region of the skin (part d), muscle (part e) or organ group. Damage to the spinal cord can result in partial or complete loss of function below the level of the injury. Note that part e describes the ‘key muscles’ as described in the International Standards for Neurological Classification of Spinal Cord Injury.
[Source 18 ]Figure 2. Spinal cord lesions and syndromes
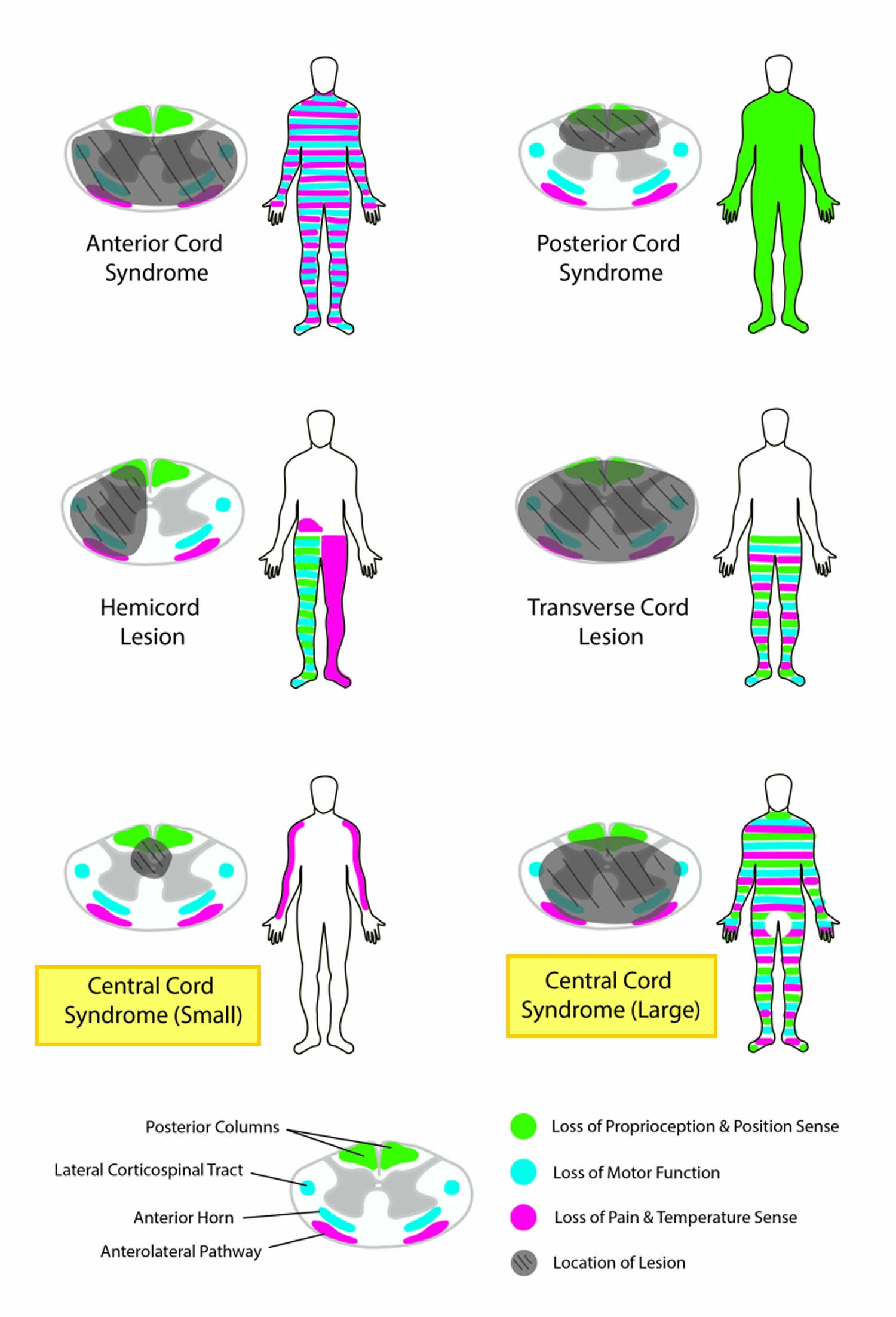
Footnote: Comparison of spinal cord lesions and syndromes with corresponding sensory or motor deficits.
[Source 3 ]Central cord syndrome causes
Central cord syndrome is an incomplete cord syndrome that results after a hyperextension injury of the cervical spine leading to spinal cord impingement. This commonly occurs with a fall forward, striking the chin, and having the neck extend backward at the time of the fall. The proposed mechanism of action involved in central cord syndrome is hyperextension of the cervical spine resulting in anteriorly simultaneous compression of the spinal cord, either by bony spurs from anterior osteophytes or intervertebral disc material and posteriorly by the buckling of the ligamentum flavum resulting in acute focal spinal cord compression with resultant hemorrhage and spinal cord edema 7. This theory was aligned with early myelogram studies performed on cadavers 12, 13. Initially, Schneider et al. 14 postulated that spinal cord compression caused central hemorrhaging, resulting in adjacent white matter compression. Schneider 14 believed that the upper limbs were more affected than the lower limbs because of the somatotropic organization of the lateral corticospinal tract, with arm function lying more medial within the tract. Neuroanatomic studies have since shown a diffuse distribution of upper and lower limb nerve fibers within the corticospinal tract, leading to the possibility that the unique presentation of central cord syndrome is due more to the hand and upper limb being more densely represented within the lateral corticospinal tract 15. More recent studies have revealed intact gray matter without evidence of hemorrhage within the central canal. Conversely, white matter axonal disruption, particularly in the lateral corticospinal tracts, appears to be the primary feature 16.
Other less common causes include cervical spondylosis, atlantoaxial instability, tethered cord, osteoporosis, and spinal arthropathies 19. The impairment of large nerve fibers causes damage to signal conduction and consequently results in motor and sensory problems, especially in the upper limbs and, to some extent, in the lower limbs. Overall, the amount of functional loss is dependent on the extent of the injury to the nerve 20.
Elderly patients often have underlying cervical spondylosis (stress defects within the vertebral bodies). This leads to the posterior cord being either irritated or compressed by the posterior ligamentum flavum or can lead to anterior cord compression from underlying spondylosis or osteolytic lesions. These two contusion type injuries to the cord can lead to symptoms secondary to edema of the cord at the site of injury. It could also lead to bleeding into the cord at the site of injury, which understandably has a worse prognosis 21.
Young patients often suffer from a higher velocity of trauma leading to cervical spine fractures/subluxations that lead to the above-described compression/contusion/bleeding.
The physical exam findings results due to the compression on the Spinothalamic (pain/temperature tract) and the corticospinal (motor) tracts of the spinal cord which can result in motor and sensory deficits. The upper extremity tracts are the most medial compared to the lower extremity/sacral segments being the most lateral, so when compression occurs the central portion becomes more effected then the external segments due to the external pressure.
Central cord syndrome predominantly affects males in a bimodal distribution (falls in those who are young and hyperextension injury in elderly patients with likely underlying spinal disease, including osteoarthritis, or cervical spondylosis) 3. Central cord syndrome has a prevalence of 15% to 25% in the United States and can occasionally be missed if the patient has mild symptoms at initial presentation 22.
Central cord syndrome symptoms
Central cord syndrome is associated with damage to the large nerve fibers that carry information directly from the brain’s cerebral cortex (involved with muscle movement in the body) to the spinal cord. These nerves are particularly important for hand and arm function. The overall amount and type of functional loss is dependent upon the severity of nerve damage. Patients with central spinal cord syndrome are typically left with more profound motor weakness of the upper extremities (your arms and hands) and less severe weakness of the lower extremities (your legs). A varying degree of sensory loss below the level of the lesion and bladder symptoms (most commonly urinary retention) may also occur.
Central cord syndrome symptoms may include:
- Paralysis or loss of fine control of movements in the arms and hands, with relatively less impairment of leg movements
- Loss of or change in sensation below the site of the injury
- Loss of bladder control
- Painful sensations such as tinging, burning, or dull ache
Historically, most of these patients will be elderly and present with symptoms after a fall with hyperextension of their neck. On examination, patients will have greater strength impairments in the upper extremities (especially the hands) compared to the lower extremities. They often complain of sensory deficits below the level of injury, but this is variable. Loss of pain and temperature are typically affected, but also the sensation of light touch may be affected. The most common sensory deficits are found in a “cape-like” distribution across their upper back and down their posterior upper extremities. They will often have neck pain at the site of spinal cord impingement.
Urinary retention and priapism can also occur as signs of upper motor neuron dysfunction 3. The sacral sensation is usually preserved, but the clinician should assess the rectal tone to evaluate the severity of the compression 23.
Differential diagnosis should include other cervical spine pathologies including fractures, dislocations, vascular injuries, or bilateral brachial plexus injuries or severe trauma resulting in avulsion of peripheral nerve roots in a bilateral distribution.
Central cord syndrome complications
Patients with central cord syndrome are at risk for a multitude of complications, like other spinal cord injuries. At first, changes in the way your body functions can be overwhelming. However, your rehabilitation team will help you develop tools to address the changes caused by the spinal cord injury, in addition to recommending equipment and resources to promote quality of life and independence. Areas often affected include:
- Bladder control. Neurogenic bladder is another prevalent condition among patients with central cord syndrome. In central cord syndrome, the sensation of bladder fullness, sphincter function of the bladder, and motor control of the bladder are impaired. Patients experience urgency, spasms, and frequency, along with urine incontinence 24. A Foley catheter is used for this purpose, and the majority of the patients regain bladder function. Patients who require long-term catheterization either use a clean intermittent catheter (CIC) or an indwelling catheter. A clean intermittent catheter is preferred over indwelling catheters as the rate of infection is much more with an indwelling catheter 23.
- Bowel control. Although your stomach and intestines work much like they did before your injury, control of your bowel movements is often altered. A high-fiber diet might help regulate your bowels, and you’ll learn ways to help control your bowel during rehabilitation.
- Pressure sores also known as pressure ulcers. Approximately one-third of the patients with central cord syndrome have multiple pressure ulcers. Pressure sores are areas of skin that have broken down because of continuous pressure on the skin and reduced blood flow to the area. Below the neurological level of your injury, you might have lost some or all skin sensations. Therefore, your skin can’t send a message to your brain when it’s injured by certain things such as prolonged pressure. Pressure ulcers are formed due to the tissue damage that typically occurs at bony prominences. This can make you more susceptible to pressure sores, but changing positions frequently — with help, if needed — can help prevent these sores. Pressure sores is usually managed by avoiding immobility, regularly examining the areas of skin that are prone to pressure sores, applying an emollient on the part exposed to friction, using cushions, and maintaining adequate weight and nutrition 25.
- Circulatory control. Cardiovascular complications arise largely due to impaired autonomic function 26. Central cord syndrome patients should be at lower risk of common cardiovascular complications due to the retained ability of lower limb function and ambulation. However, patients with decreased lower limb function are at higher risk for low baseline blood pressure, orthostatic hypotension, and venous thromboembolism 27, 28. These circulation changes can also increase your risk of developing blood clots, such as deep vein thrombosis or a pulmonary embolus. Another problem with circulatory control is a potentially life-threatening rise in blood pressure (autonomic dysreflexia) and abnormal heart rhythms (arrhythmias). Blood pressure needs to be closely monitored. Because the brain’s control of the cardiac nerves can be cut off, your heart can beat at a dangerously slow pace, or it can pound rapidly and irregularly. Changes in the control of blood vessels can cause them to widen and allow blood to pool in the small arteries far away from the heart. People with spinal cord injuries are at increased risk for blood clots due to stagnation of blood flow in the large veins in the legs. Treatment includes anticoagulant drugs and compression stockings to increase blood flow in the lower legs and feet.
- Low baseline blood pressures in acute injury are managed with fluid resuscitation. Orthostatic hypotension can be managed both with and without medications. Non-pharmacologic strategies include reducing rapid changes in posture, avoiding hot environments, and eating smaller meals to reduce postprandial cardiovascular shunting to gastrointestinal organs 29, 30. Pharmacologic options for orthostatic hypotension include fludrocortisone, ephedrine, and midodrine; however, only midodrine is approved by the Food and Drug Administration(FDA) for treating neurogenic orthostatic hypotension 29, 31, 32, 33.
- The Consortium of Spinal Medicine recommends venous thromboembolism (VTE) prophylaxis for a minimum of 8 weeks after injury and prefers low molecular weight heparin (LMWH) over other anticoagulant medications, though research is needed into the safety and efficacy of direct oral anticoagulants 28, 34. Currently, low-dose subcutaneous heparin and vitamin K antagonists are not recommended therapies 28.
- Blood pressure monitoring may be required in selective cases for the long term, even if the patient is not diagnosed as hypertensive. For blood pressure control, nitrates, hydralazine, and labetalol are used, but prescribers should avoid giving nitrates to patients taking sildenafil 35.
- Readdy et al. 35 showed that cardiogenic complications appeared in 68% of patients with no relation to conservative management, surgical management, or surgical timing. Furthermore, they noted that in patients 55 years or older, there was a significant increase in complications with dopamine compared to phenylephrine (83% versus 50%, respectively) 35. The utmost priority in managing cardiometabolic syndrome is essential 36.
- Breathing problems. Your injury might make it more difficult to breathe and cough if your abdominal and chest muscles are affected. Your neurological level of injury will determine what kind of breathing problems you have. If you have a cervical and thoracic spinal cord injury, you might have an increased risk of pneumonia or other lung problems. Medications and therapy can help prevent and treat these problems.
- About one-third of people with a neck injury will need temporary or permanent help with breathing and may require an inserted artificial breathing tube. Any injury to the spinal cord between the C1-C4 segments can stop breathing as the nerves in this region cause the diaphragm to move and the lungs to expand. Special training regarding breathing and swallowing may be needed.
- Pneumonia: Respiratory complications are the leading cause of death in people with spinal cord injury, commonly as a result of pneumonia. If you are placed on a ventilator to assist with breathing (intubation), you are at increased risk of developing pneumonia. You must be carefully monitored and treated with antibiotics if symptoms of pneumonia appear. Clearing secretions from the throat and preventing food and liquids from being sucked into the lungs (aspiration) can prevent pneumonia.
- Bone density. After spinal cord injury, there’s an increased risk of osteoporosis and fractures below the level of injury.
- Muscle spasticity and decreased muscle tone. Some people with spinal cord injuries have one of two types of muscle tone problems: uncontrolled tightening or motion in the muscles (spasticity) or soft and limp muscles lacking muscle tone (flaccidity) that may require special treatment. Muscles may deteriorate due to underuse.
- Spasticity can be defined as “disordered sensory-motor control resulting from an upper motor neuron lesion, presenting as intermittent or sustained involuntary activation of muscles” and is a significant problem in spinal cord injury patients 37, 38. A systematic review by Bovend’Erdt et al. 39 found inconclusive evidence of the beneficial effects of stretching on spasticity. Physical modalities such as cryotherapy and heat therapy (both superficial and deep) provide only short-term effects on spasticity 40. Neuromuscular stimulation and functional electrical stimulation have shown positive results in reducing spasticity 41. Transcranial and spinal cord magnetic stimulation has been proposed, but more research is required 42. Common oral pharmacologic options include gamma-aminobutyric acid (GABA) agonists baclofen, gabapentinoids and benzodiazepines, alpha-2-adrenergic agonists tizanidine and clonidine, and peripherally acting dantrolene 43. Alternative medications that are not FDA-approve include cyproheptadine, cannabinoids, and 4-aminopyridine 44, 45, 46. In patients with minimal response to oral medications or have contraindications to oral medications, chemodenervation with botulinum toxin or chemolysis with alcohol are alternative interventions 47, 48. Boviatsis et al. 49 found that intrathecal baclofen pumps improved functional improvement and reduced pain in spinal cord injury and multiple sclerosis. Surgical interventions for spasticity refractory to conservative management include tendon lengthening, tendon transfers, neurotomy, and selective rhizotomy 50, 51. Spinal cord stimulators have shown promising results in the past, but current clinical trials are needed to provide data on their safety and efficacy due to advances in technology and understanding of spasticity pathophysiology 52.
- Autonomic dysreflexia. Patients with central cord syndrome are usually prone to autonomic dysreflexia, a potentially life-threatening emergency that is more common in patients with spinal cord injury above the T6 level. Autonomic dysreflexia is a life-threatening reflex action that primarily affects those with injuries to the neck or upper back. Symptoms may include flushing or sweating, a pounding headache, anxiety, sudden increase in blood pressure, vision changes, or goose bumps on the arms and legs 53. Autonomic dysreflexia usually occurs in the first month of the injury. These symptoms are usually episodic, and they are conservatively managed. The initial management strategy is prevention by educating patients, caregivers, and hospital staff about the potential for autonomic dysreflexia as well as warning signs. During an acute episode, management should begin by placing the patient upright, removing all tight clothes, and removing any noxious stimuli such as skin pressure, urinary catheter dysfunction, and bowel impaction. A survey for noxious stimuli should be repeated until the patient’s autonomic dysreflexia episode has subsided 54.
- Traumatic brain injury (TBI). A meta-analysis by Budisin et al. 55 found that approximately 40 to 50% of traumatic spinal cord injury patients were also diagnosed with a traumatic brain injury (TBI). Motor vehicle collisions were more likely to cause comorbid traumatic brain injury (TBI) compared to falls (57.6% versus 31.6%). More recently, the prevalence of traumatic brain injury (TBI) in patients with a cervical spinal injury is approximately 40% 56.
- Fitness and wellness. Weight loss and muscle atrophy are common soon after a spinal cord injury. Limited mobility can lead to a more sedentary lifestyle, placing you at risk of obesity, cardiovascular disease and diabetes. A dietitian can help you eat a nutritious diet to sustain an adequate weight. Physical and occupational therapists can help you develop a fitness and exercise program.
- Sexual function. Depending on the level of injury and recovery from the trauma, sexual function and fertility may be affected. Men might notice changes in erection and ejaculation; women might notice changes in lubrication after a spinal cord injury. Physicians specializing in urology (urologist) or fertility can offer options for sexual functioning and fertility.
- Pain. Patients with central cord syndrome can develop neuropathic pain at the level of the injury and below the level of injury. Neuropathic pain can be caused by damage to either the spinal cord or nerve roots. It is typically described as “hot,” burning,” tingling,” “pins and needles,” “sharp,” “shooting,” or “electric” 57. First-line treatment for neuropathic pain in spinal cord injury is gabapentinoids (gabapentin and pregabalin) and tricyclic antidepressants (TCA), with additional consideration for selective serotonin reuptake inhibitors (SSRI) and serotonin and norepinephrine reuptake inhibitors (SNRI) 58, 59. Guidelines published by the CanPainSCI Working Group recommended tramadol as a second-line medication 60, 61. Lamotrigine was considered a second-line medication, specifically in incomplete spinal cord injury patients. Additional interventions to consider are visual illusion therapy, transcranial direct current stimulation, and physical and occupational therapy 60. Methylprednisolone has been advocated for acute neuropathic pain with allodynia 62.
- Depression. Coping with the changes a spinal cord injury brings and living with pain causes depression in some people. Therapy and medicine may help treat depression and other mental health conditions.
Central cord syndrome diagnosis
All patients with concern for spinal cord injury should have a thorough trauma evaluation performed, and these patients should have cervical immobilization maintained during initial evaluation while obtaining radiologic imaging. Plain radiographs can show fractures/dislocations of the cervical spine. Computed tomography scan (CT) of the cervical spine can show some impingement of the spinal canal, but the most sensitive test to diagnose direct spinal cord impingement is an magnetic resonance imaging (MRI) of the cervical spine. Diffusion tensor imaging is a promising radiological test 63.
- CT or CAT scan: Computerized tomography (CT) scan can provide a clearer image of abnormalities seen on X-ray (images of organs, bones, and tissues). CT scan uses computers to form a series of cross-sectional images that can define bone, disk and other problems. CT can detect bone fractures, bleeding, and spinal stenosis (narrowing of the spinal canal). It also shows shape and size of the spinal canal, its contents and the structures around it. It is usually performed prior to MRI scanning. Combined with MRI scans it provides a more comprehensive diagnostic data set for treatment decision making.
- Computed tomography (CT) is currently the first-line imaging as it provides rapid imaging of the axial skeleton. In suspected cervical spinal cord injury patients, neck flexion and extension images should also be obtained 64. CT of the cervical spine can show the impingement of the spinal canal to some extent 65, 66. In awake and asymptomatic patients, the American Association of Neurological Surgeons (AANS) does not recommend imaging prior to discontinuing cervical immobilizers 67. The Consortium of Spinal Medicine recommends imaging the entire spine for patients with spinal cord injuries 68.
- MRI: Magnetic resonance imaging (MRI) uses a strong magnetic field and radio waves to produce computer-generated three-dimensional images of body structures, including tissues, organs, bones, and nerves. MRI is helpful for looking at the spinal cord and identifying herniated discs (cartilage located between the vertebrae), vascular (blood vessel) irregularities, bleeding, blood clots, inflammation or other masses that might compress the spinal cord and injury to the ligaments that support the cervical spine. MRI can also show ligamentous and soft tissue injuries that might be missed by other imaging tests.
- Magnetic resonance imaging (MRI) is the gold standard imaging modality to evaluate the spinal cord and the adjacent soft tissue structures (vasculature, ligaments, intervertebral discs) 64. The Consortium of Spinal Medicine recommends imaging the entire spine for patients with spinal cord injuries 68.
- Hyperintensity on gradient T2 MRI within the cervical cord is the most consistent finding in central cord syndrome 69.
- X-ray: Application of radiation to produce a film or picture of a part of the body can show the structure of the vertebrae and the outline of the joints. X-rays of the spine delineate fractures and dislocations, as well as the degree and extent of spondylitic changes. Flexion/extension views assist in evaluation of ligamentous stability. Both the MRI and CAT scan images are static images. Flexion / extension plain X-rays can provide a simple means of determining dynamic stability or instability of the spinal column. These views can help determine whether or not a cervical collar or stabilizing cervical spine surgery is necessary or not.
Clinical diagnosis
Central cord syndrome is a clinical diagnosis with a presentation that includes disproportionate impairment of the upper limb motor function compared to the lower limbs, along with varying degrees of sensory deficits below the level of the spinal cord lesion and possibly urinary or gastrointestinal dysfunction. Pouw et al. 70 proposed that a difference of 10 between upper and lower limb motor scores on the International Standards for Neurological Classification of SCI (ISNCSCI) may be a more objective diagnostic criterion. The clinical evaluation of central cord syndrome mirrors other spinal cord injuries. Identifying the neurological level of injury is paramount as it can help determine prognosis and guide therapeutic strategies and functional rehabilitation goals. Additionally, a baseline neurological examination can track future improvements as well as future deficits as they arise.
The gold standard examination tool for any spinal cord injury is the International Standards for Neurological Classification of SCI (ISNCSCI). More severe findings on neurological examination should raise suspicion of a cervical vertebral fracture. When central cord syndrome is associated with a cervical spine fracture, it can prolong recovery 65, 66. Physicians must also assess for respiratory compromise, pressure injuries to the skin, neurogenic bowel and bladder, spasticity, autonomic dysreflexia, and temperature dysregulation.
Central cord syndrome treatment
Management of spinal cord injuries begins at the scene of the injury with a primary survey involving the airway, breathing, circulation, and disability (ABCD). Disability includes calculating a Glasgow coma scale (GCS), pupil examination, and identifying any lateralizing signs. This should be repeated as often as necessary whenever the patient’s status changes. At the accident scene, if a spinal cord injury is suspected, emergency personnel will place a rigid collar around your neck and carefully place you on a backboard to prevent further damage to your spinal cord. They may use sedatives to relax and prevent movement. A breathing tube may be inserted if you have problems breathing and your body isn’t receiving enough oxygen from the lungs. Lastly, physicians in the field should collect as much patient history as possible, noting any subjective complaints of neck pain. Restricting spinal motion is of the utmost importance in patients with suspected spinal cord injuries 71.
With trauma, the first priority is to limit the damage as much as possible and prevent more from happening. That usually involves immobilizing a person using specialized backboards, collars or braces to keep their spinal cord stable and prevent anything from pressing into or damaging it.
Other ways to prevent damage to the spinal cord from injuries and trauma include:
- Early surgery to relieve pressure around the spinal cord.
- Early surgery to stabilize or fuse vertebrae together to keep them from damaging the spinal cord.
Because of these factors, your doctor is the best person to explain the situation. He or she can offer you guidance and relevant information for your specific situation, including the possible treatments and the side effects or complications that can happen with those treatments.
Conservative management should only be considered in situations without fracture, dislocation, disc herniation, or spinal instability; otherwise, surgical intervention is preferred 15. Conservative management includes physical and occupational therapy in addition to standard medical care for complications of central cord syndrome.
In patients without instability, the decision for conservative versus surgical management of acute central cord syndrome is highly debated, with no clearly established guidelines 3. Research studies have produced mixed results comparing conservative management with early surgical intervention. Numerous studies showed that delaying surgery in traumatic central cord syndrome may be beneficial where the odds of mortality decreased within each day of delay. The goal of delayed surgery was to improve the patient’s underlying health, especially in older adults, and treat other potential comorbidities before the surgery 72, 73. On the other hand, Godzik et al. 74 performed a retrospective study identifying 2,379 central cord syndrome patients and hypothesized that increased mortality in early surgical patients was more likely related to higher injury severity than surgical timing.
Recently, the Spinal Cord Society and Spine Trauma Study Group released a position statement after a systematic review and meta-analysis regarding the management of acute central cord syndrome 53. Their recommendation was patients with acute traumatic central cord syndrome secondary to vertebral fracture, dislocation, traumatic disc herniation or instability have better outcomes with early surgery (less than 24 hours after injury) 53. In patients of acute traumatic central cord syndrome secondary to extension injury in stenotic cervical canal without fracture or fracture dislocation or traumatic disc herniation or instability, there is requirement of high-quality prospective randomized controlled trials to resolve controversy regarding early surgery versus conservative management and delayed surgery if recovery plateaus or if there is a neurological deterioration. Until such time decision on surgery and its timing should be left to the judgment of physician, deliberating on pros and cons relevant to the particular patient and involving the well-informed patient and relatives in decision making 53. The review did not find a difference in complications or outcomes between early surgery and conservative management with delayed surgery 53.
In addition to the treatment strategies and timing of surgical intervention, there remain many controversial management topics for patients with acute traumatic central cord syndrome 15. Anti-coagulation therapy is one such area of controversy. Fehlings et al 75 recommended the routine use of anticoagulant therapy after spinal cord injury beginning at 72 hours after injury to the high propensity of any cord injury patient to develop venous thromboembolism. More specifically, they recommended the use of low-molecular-weight heparin or fixed-dose unfractionated heparin. However, the authors rated the level of evidence supporting these recommendations to be limited 75.
Rarely patients will require extensive physical therapy without significant neurologic recovery. These patients may develop chronic issues including autonomic dysregulation with uncontrolled blood pressure, neurogenic bladder requiring catheterization, pressure ulcers, neuropathic pain, and spasticity with chronic pain issues.
Blood pressure can be managed with nifedipine or transdermal nitroglycerin.
Patients with neurogenic bladder may require intermittent self-catheterization but will remain at risk for iatrogenic bladder infections. Many of these patients will have the return of bladder function after six to eight months.
Neuropathic pain and spasticity are often managed with a regular stretching program, antispasmodic medications. Baclofen is the hallmark of spasticity management (oral initially, but can be placed as an intrathecal pump if severe enough). Patients may require additional medicinal therapy in consultation with a pain specialist or neurologist for their neuropathic pain and spasticity.
Induced pluripotent stem cell therapy might provide a newer therapeutic avenue in the near future 76.
Emergency actions
Urgent medical attention is critical to minimize the effects of head or neck trauma. Therefore, treatment for a spinal cord injury often begins at the accident scene. Emergency personnel typically immobilize the spine as gently and quickly as possible using a rigid neck collar and a rigid carrying board, which they use during transport to the hospital.
Early (acute) stages of treatment
In the emergency room, doctors focus on:
- Maintaining your ability to breathe
- Preventing shock
- Immobilizing your neck to prevent further spinal cord damage
- Avoiding possible complications, such as stool or urine retention, respiratory or cardiovascular difficulty, and formation of deep vein blood clots in the extremities. The American Association of Neurosurgeons and Congress of Neurosurgeons recommend preventing hypotension to the injured spine and spinal cord with a target mean arterial pressure (MAP) between 85 and 90 mmHg for at least seven days 77. However, the current research is inconclusive on the optimal blood pressure range 15.
If you have a spinal cord injury, you’ll usually be admitted to the intensive care unit (ICU) for treatment. You might be transferred to a regional spine injury center that has a team of neurosurgeons, orthopedic surgeons, spinal cord medicine specialists, psychologists, nurses, therapists and social workers with expertise in spinal cord injury.
- Medications. Methylprednisolone (Solu-Medrol) given through a vein in the arm (IV) has been used as a treatment option for an acute spinal cord injury in the past. But recent research has shown that the potential side effects, such as blood clots and pneumonia, from using this medication outweigh the benefits. Because of this, methylprednisolone is no longer recommended for routine use after a spinal cord injury.
- Immobilization. You might need traction to stabilize or align your spine. Options include soft neck collars and various braces.
- Surgery. Often surgery is necessary to remove fragments of bones, foreign objects, herniated disks or fractured vertebrae that appear to be compressing the spine. Surgery might also be needed to stabilize the spine to prevent future pain or deformity.
- Experimental treatments. Scientists are trying to figure out ways to stop cell death, control inflammation and promote nerve regeneration. For example, lowering body temperature significantly — a condition known as hypothermia — for 24 to 48 hours might help prevent damaging inflammation. More study is needed.
Medications
The use of corticosteroids in spinal cord injury has a long history of controversy. The goal of intravenous (IV) methylprednisolone therapy is to halt the inflammatory cascade that results in secondary spinal cord injury. The landmark Second National Spinal Cord Injury Study (NASCIS-II) did show statistically significant neurological benefits with the administration of IV methylprednisolone if given within 8 hours of initial injury; however, there was also an increased risk of adverse events. Therefore, the Congress of Neurological Surgeons recommends against IV methylprednisolone administration 78. On the other hand, in 2016, AO Spine published a position statement recommending a 24-hour infusion of IV methylprednisolone within 8 hours of injury but not offering infusion for patients who present greater than 8 hours after the initial injury 79.. Additionally, AO Spine does not recommend a 48-hour infusion of methylprednisolone 79.
Surgical approach
At this time, there are no guidelines for the surgical approach, and it is left to the surgeon to decide the most appropriate course for intervention that will optimize outcomes and reduce complications. Generally, single-level anterior compressive lesions necessitate an anterior approach. A posterior approach should be considered in patients with compression at multiple levels. Patients with spinal fractures or dislocations should undergo reduction and stabilization, which may require a combined anterior and posterior approach 69.
Ongoing care
After the initial injury or condition stabilizes, doctors turn their attention to preventing secondary problems that may arise, such as deconditioning, muscle contractures, pressure ulcers, bowel and bladder issues, respiratory infections, and blood clots.
The length of your hospital stay will depend on your condition and the medical issues you face. Once you’re well enough to participate in therapies and treatment, you might transfer to a rehabilitation facility.
Rehabilitation
Rehabilitation team members will begin to work with you while you’re in the early stages of recovery. Rehabilitation programs combine physical therapies with skill-building activities and counseling to provide social and emotional support, as well as to increase independence and quality of life. Your rehabilitation team might include a physical therapist, an occupational therapist, a rehabilitation nurse, a rehabilitation psychologist, a social worker, a dietitian, a recreation therapist, and a doctor who specializes in physical medicine (physiatrist) or spinal cord injuries.
- Physical therapy includes exercise programs geared toward strengthening muscles. Physical therapy for quadriplegia focuses on helping individuals strengthen weakened or underused muscles and maintain full range of motion through targeted exercises. A physical therapist will teach individuals the most effective exercises to stimulate neuroplasticity in the central nervous system. A physical therapist may also recommend orthotics such as braces and splints to promote correct musculoskeletal alignment and assist with mobility.
- Occupational therapy helps redevelop fine motor skills, particularly those needed to perform activities of daily living (ADLs) such as getting in and out of a bed, self-grooming, eating, and using the toilet. An occupational therapist will work with individuals with quadriplegia and their caregivers to teach them the most effective ways to perform everyday activities such as transferring, bathing, and grooming. This may involve learning how to use adaptive tools, such as a universal cuff, or adaptive techniques like tenodesis. Tenodesis is a natural movement that all of your body make. When you bend your wrist forward, the hand should open up. Likewise, when you extend the wrist (bend it backward), the fingers should curl in. Learning to utilize a tenodesis grasp can help individuals with quadriplegia become more independent. You may learn how to cope with spasticity, autonomic dysreflexia, and neurogenic pain.
- Vocational rehabilitation includes identifying basic work skills and physical and cognitive capabilities to determine the likelihood for employment; identifying potential workplaces and any assistive equipment that will be needed; and arranging a user-friendly workplace.
- Speech therapy. Individuals with quadriplegia often experience oral motor impairments that affect their ability to chew, swallow, and speak. Additionally, individuals with spinal cord injuries at the C5 level or above may experience breathing difficulties due to impaired innervation of the diaphragm. A speech therapist can help individuals with quadriplegia improve their oral motor functions, communication skills, and breathing.
- Educational training can help you develop skills for a new line of work that may be less dependent upon physical abilities and more dependent upon computer or communication skills. People with spinal cord injury or other disabilities are encouraged to participate in activities that provide a sense of satisfaction and self-esteem, such as educational classes, hobbies, special interest groups, and participating in family and community events.
- Recreation therapy encourages people with spinal cord injury to participate in sports or activities at their level of mobility, as well as achieve a more balanced lifestyle that provides opportunities for socialization and self-expression.
- Psychotherapy. Individuals with quadriplegia may develop mental health problems such as depression or anxiety due to feelings of isolation, lack of support, or difficulties adjusting to life with paralysis. Working with a psychotherapist can help individuals with quadriplegia better understand their negative feelings and find more effective ways to cope.
During the initial stages of your rehabilitation, therapists usually emphasize maintaining and strengthening muscle function, redeveloping fine motor skills, and learning ways to adapt to do day-to-day tasks. For some individuals, mobility will only be possible with assistive or adaptive devices such as a walker, leg braces, or a wheelchair. Communication skills such as writing, typing, and using the telephone may also require adaptive devices for those with tetraplegia.
You’ll be educated on the effects of a spinal cord injury and how to prevent complications, and you’ll be given advice on rebuilding your life and increasing your quality of life and independence.
You’ll be taught many new skills, and you’ll use equipment and technologies that can help you live on your own as much as possible. You’ll be encouraged to resume your favorite hobbies, participate in social and fitness activities, and return to school or the workplace.
Assistive medical devices
Assistive medical devices can help people with a spinal cord injury become more independent and more mobile, thereby promoting their well-being. Depending on the severity of the injury, people may need a wheelchair, electronic stimulators, assisted training with walking, neural prosthetics (assistive devices that may stimulate the nerves to restore lost functions), computer adaptations, and other computer-assisted technology.
- Modern wheelchairs. Improved, lighter weight wheelchairs are making people with spinal cord injuries more mobile and more comfortable. Some people need an electric wheelchair. Some wheelchairs can even climb stairs, travel over rough ground and elevate a user to reach high places without help.
- Computer adaptations. For someone who has limited hand function, computers can be difficult to operate. Computer adaptations range from simple to complex, such as key guards and voice recognition.
- Electronic aids to daily living. Essentially any device that uses electricity can be controlled with an electronic aid to daily living. Devices can be turned on or off by switch or voice-controlled and computer-based remotes.
- Electrical stimulation devices. Often called functional electrical stimulation systems, these sophisticated devices use electrical stimulators to control arm and leg muscles to allow people with spinal cord injuries to stand, walk, reach and grip.
Central cord syndrome prognosis
The prognosis for central cord syndrome varies among individuals, but most people whose central cord syndrome is caused by trauma have some recovery of neurological function and some people recover near-normal function with some neurological deficits remain 80, 81. Improvement usually occurs in an ascending fashion, with motor leg function recovering first, followed by bladder control, then proximal arms. The hand function appears to return last. Abnormal MRI signals can help predict the likelihood of neurological recovery that may occur later in the course of recovery 53. Young trauma patients and those who receive medical intervention soon after their injury have better chances of neurological recovery. If the underlying cause is swelling (edema), recovery may occur relatively soon after an initial phase of motor paralysis or paresis. Leg function usually returns first, followed by bladder control and then arm function. Hand movement and finger dexterity improves last. If the central lesion is caused by hemorrhage or ischemia, then recovery is less likely and the prognosis is more devastating. Roth et al. 82 found age to be the most important prognostic indicator, as patients younger than 50 have more favorable outcomes. Hohl et al. 83 developed a classification system for central cord syndrome that combined initial International Standards for Neurological Classification of SCI (ISNCSCI) motor score and evidence of MRI signal abnormality to predict functional outcomes at one year, but this has not been validated.
Many people with central cord syndrome recover substantial function after their initial injury, and the ability to walk is recovered in most cases, although some impairment may remain. Improvement occurs first in the legs, then the bladder, and may be seen in the arms. Hand function recovers last, if at all. Recovery is generally better in younger patients, compared to those over the age of 50.
Recovery generally plateaus at two years post-injury 69. At three years post-injury, patients should recover at least 90% of their motor score regardless of surgical versus conservative management; however, patients who underwent surgical intervention had greater functional scores and were more likely to attain their pre-injury mobility status 84. Aito et al. 85 performed a retrospective analysis on 82 central cord syndrome patients and found that 47% of patients had persistent neuropathic pain, 68% achieved spontaneous voiding, and 66% reported spasticity at follow-up (at least 1.5 years).
Several studies have sought to identify initial postinjury factors and findings that are predictors for recovery of acute traumatic central cord syndrome 15. Prognostic factors include age, the severity of the initial neurologic deficit, and initial MRI findings 69. Initial severity of neurologic exam, age, presence of fracture or dislocation, presence of hematoma, and ongoing spinal cord compression are significant prognostic factors of poor patient outcomes 86, 87, 88, 89, 90. Additionally, elderly patients with significant comorbidities have been shown to have a worse prognosis, a lower rate of operative intervention, and a higher inpatient mortality rate 91. Schroeder et al 92 identified that patients with acute traumatic central cord syndrome associated with fracture have a worse initial neurologic status but better neurologic recovery in the first week after injury compared with those without fracture. In a separate study, Schroeder et al 93 found that patients with increased T2 signal intensity in their spinal cord on magnetic resonance imaging had a more severe initial neurological injury but had minimal early deterioration compared with those with less cord signal intensity.
A European multicenter study comparing 110 patients with central cord syndrome with other incomplete spinal cord injury patients revealed that central cord syndrome patients tended to have greater improvement in their ASIA Impairment Scale (AIS) grade as well as better ability to ambulate after one year 94. However, central cord syndrome patients had lower “self-care” scores from injury onset up to one year based on the Spinal Cord Independence Measure (SCIM), likely due to impaired hand function 94. Patients admitted to acute inpatient rehabilitation with normal leg strength and those who experienced both upper and lower limb motor recovery had the greatest improvement in completing activities of daily living (ADL) at discharge. Patients who did not demonstrate objective neurologic recovery also made substantial functional improvements after acute inpatient rehabilitation 82.
A national database study from 2009 through 2012 showed fall as the predominant cause, with a mean age of involvement of 60 years. 55% of cases were managed conservatively, 39% with cervical fusion surgery (62% anterior decompression and fusion), and 6% underwent laminoplasty 95. The mortality rate was 2.6%, with increased odds among older patients age and those with greater comorbidities 95.
Early decompression and stabilization have been advocated for cohorts presenting with instability and major or worsening neurological deficits 15. Surgery within 12 hours of the injury can improve neurologic recovery and is associated with fewer post-surgical complications 96.
No difference has been observed in the overall outcomes between early and late surgical interventions 15. Early surgery may, however, accelerate recovery in selected cohorts 97. Long-term follow-up has failed to demonstrate any significant differences among patients undergoing conservative versus surgical treatment 85.
Lower preoperative Japanese Orthopedic Association (JOA) score, long segment signal changes, and impingement connote poor prognosis 98, 63. Intramedullary lesion length (IMLL) was the only significant variable predictive of American Spinal Injury Association (ASIA) Impairment Scale (AIS) grade conversion to a better grade 99. The severity of AIS at admission was the strongest predictor of functional outcomes 100. The majority of American Spinal Injury Association (ASIA) Impairment Scale (AIS) conversion should occur within the first 6 to 9 months, with a peak observed in the first three months 101.
The neuroanatomical–functional paradox observed among patients with central cord syndrome is due to the interplay between motor synergy encoding (MSE) neurons, as well as lesion-affected and recovery-related networks 102. The neuronal plasticity, meta-inflammation, and diaschisis also have ripple effects 102.
- Schneider RC, Cherry G, Pantek H. The syndrome of acute central cervical spinal cord injury; with special reference to the mechanisms involved in hyperextension injuries of cervical spine. J Neurosurg. 1954;11:546–547. doi: 10.3171/jns.1954.11.6.0546[↩]
- Stobart Gallagher MA, Gillis CC. Central Cord Syndrome. [Updated 2019 Feb 22]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2019 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK441932[↩]
- Ameer MA, Tessler J, Munakomi S, et al. Central Cord Syndrome. [Updated 2023 Aug 13]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK441932[↩][↩][↩][↩][↩][↩]
- Jimenez O, Marcillo A, Levi AD. A histopathological analysis of the human cervical spinal cord in patients with acute traumatic central cord syndrome. Spinal Cord. 2000 Sep;38(9):532-7. doi: 10.1038/sj.sc.3101052[↩]
- Khorasanizadeh M, Yousefifard M, Eskian M, Lu Y, Chalangari M, Harrop JS, Jazayeri SB, Seyedpour S, Khodaei B, Hosseini M, Rahimi-Movaghar V. Neurological recovery following traumatic spinal cord injury: a systematic review and meta-analysis. J Neurosurg Spine. 2019 Feb 15;:1-17[↩]
- Chen TY, Lee ST, Lui TN, Wong CW, Yeh YS, Tzaan WC, Hung SY. Efficacy of surgical treatment in traumatic central cord syndrome. Surg Neurol. 1997;48:435–440. doi: 10.1016/S0090-3019(97)00037-2[↩]
- Lenehan B, Street J, O’Toole P, Siddiqui A, Poynton A. Central cord syndrome in Ireland: the effect of age on clinical outcome. Eur Spine J. 2009 Oct;18(10):1458-63. doi: 10.1007/s00586-009-1107-5[↩][↩][↩]
- Harrop JS, Sharan A, Ratliff J. Central cord injury: pathophysiology, management, and outcomes. Spine J. 2006 Nov-Dec;6(6 Suppl):198S-206S. doi: 10.1016/j.spinee.2006.04.006[↩]
- Ishida Y, Tominaga T. Predictors of neurologic recovery in acute central cervical cord injury with only upper extremity impairment. Spine (Phila Pa 1976). 2002 Aug 1;27(15):1652-8; discussion 1658. doi: 10.1097/00007632-200208010-00011[↩]
- Rupp R, Biering-Sørensen F, Burns SP, Graves DE, Guest J, Jones L, Read MS, Rodriguez GM, Schuld C, Tansey-Md KE, Walden K, Kirshblum S. International Standards for Neurological Classification of Spinal Cord Injury: Revised 2019. Top Spinal Cord Inj Rehabil. 2021 Spring;27(2):1-22. doi: 10.46292/sci2702-1[↩]
- GROS C, VLAHOVITCH B, MOHASSEB G. [Traumatic tetraplegia with predominantly brachial involvement]. Neurochirurgia (Stuttg). 1960 Jul;3:92-112. French. doi: 10.1055/s-0028-1095483[↩]
- TAYLOR AR. The mechanism of injury to the spinal cord in the neck without damage to vertebral column. J Bone Joint Surg Br. 1951 Nov;33-B(4):543-7. doi: 10.1302/0301-620X.33B4.543[↩][↩]
- SCHNEIDER RC, THOMPSON JM, BEBIN J. The syndrome of acute central cervical spinal cord injury. J Neurol Neurosurg Psychiatry. 1958 Aug;21(3):216-27. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC497322/pdf/jnnpsyc00283-0058.pdf[↩][↩]
- SCHNEIDER RC, CHERRY G, PANTEK H. The syndrome of acute central cervical spinal cord injury; with special reference to the mechanisms involved in hyperextension injuries of cervical spine. J Neurosurg. 1954 Nov;11(6):546-77. doi: 10.3171/jns.1954.11.6.0546[↩][↩][↩][↩]
- Divi SN, Schroeder GD, Mangan JJ, Tadley M, Ramey WL, Badhiwala JH, Fehlings MG, Oner FC, Kandziora F, Benneker LM, Vialle EN, Rajasekaran S, Chapman JR, Vaccaro AR. Management of Acute Traumatic Central Cord Syndrome: A Narrative Review. Global Spine J. 2019 May;9(1 Suppl):89S-97S. doi: 10.1177/2192568219830943[↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Quencer RM, Bunge RP, Egnor M, Green BA, Puckett W, Naidich TP, Post MJ, Norenberg M. Acute traumatic central cord syndrome: MRI-pathological correlations. Neuroradiology. 1992;34(2):85-94. doi: 10.1007/BF00588148[↩][↩]
- Lo J, Chan L, Flynn S. A Systematic Review of the Incidence, Prevalence, Costs, and Activity and Work Limitations of Amputation, Osteoarthritis, Rheumatoid Arthritis, Back Pain, Multiple Sclerosis, Spinal Cord Injury, Stroke, and Traumatic Brain Injury in the United States: A 2019 Update. Arch Phys Med Rehabil. 2021 Jan;102(1):115-131. doi: 10.1016/j.apmr.2020.04.001[↩]
- Ahuja, C., Wilson, J., Nori, S. et al. Traumatic spinal cord injury. Nat Rev Dis Primers 3, 17018 (2017). https://doi.org/10.1038/nrdp.2017.18[↩]
- Dydyk AM, Givler A. Central Pain Syndrome. [Updated 2023 Feb 19]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK553027[↩]
- Arul K, Ge L, Ikpeze T, Baldwin A, Mesfin A. Traumatic spinal cord injuries in geriatric population: etiology, management, and complications. J Spine Surg. 2019 Mar;5(1):38-45. doi: 10.21037/jss.2019.02.02[↩]
- Hashmi SZ, Marra A, Jenis LG, Patel AA. Current Concepts: Central Cord Syndrome. Clin Spine Surg. 2018 Dec;31(10):407-412.[↩]
- Peterson MD, Kamdar N, Whitney DG, Ng S, Chiodo A, Tate DG. Psychological morbidity and chronic disease among adults with nontraumatic spinal cord injuries: a cohort study of privately insured beneficiaries. Spine J. 2019 Oct;19(10):1680-1686. doi: 10.1016/j.spinee.2019.05.591[↩]
- Sacco E. Fisiopatologia della vescica iperattiva [Physiopathology of overactive bladder syndrome]. Urologia. 2012;79(1):24-35. Italian. doi: 10.5301/RU.2012.8972[↩][↩]
- Grundy L, Caldwell A, Brierley SM. Mechanisms Underlying Overactive Bladder and Interstitial Cystitis/Painful Bladder Syndrome. Front Neurosci. 2018 Dec 12;12:931. doi: 10.3389/fnins.2018.00931[↩]
- Dulamea AO, Sirbu-Boeti MP, Bleotu C, Dragu D, Moldovan L, Lupescu I, Comi G. Autologous mesenchymal stem cells applied on the pressure ulcers had produced a surprising outcome in a severe case of neuromyelitis optica. Neural Regen Res. 2015 Nov;10(11):1841-5. doi: 10.4103/1673-5374.165325[↩]
- Biering-Sørensen F, Biering-Sørensen T, Liu N, Malmqvist L, Wecht JM, Krassioukov A. Alterations in cardiac autonomic control in spinal cord injury. Auton Neurosci. 2018 Jan;209:4-18. doi: 10.1016/j.autneu.2017.02.004[↩]
- Teasell RW, Arnold JM, Krassioukov A, Delaney GA. Cardiovascular consequences of loss of supraspinal control of the sympathetic nervous system after spinal cord injury. Arch Phys Med Rehabil. 2000 Apr;81(4):506-16. doi: 10.1053/mr.2000.3848[↩]
- Prevention of Venous Thromboembolism in Individuals with Spinal Cord Injury: Clinical Practice Guidelines for Health Care Providers, 3rd ed.: Consortium for Spinal Cord Medicine. Top Spinal Cord Inj Rehabil. 2016 Summer;22(3):209-240. doi: 10.1310/sci2203-209[↩][↩][↩]
- Gibbons CH, Schmidt P, Biaggioni I, Frazier-Mills C, Freeman R, Isaacson S, Karabin B, Kuritzky L, Lew M, Low P, Mehdirad A, Raj SR, Vernino S, Kaufmann H. The recommendations of a consensus panel for the screening, diagnosis, and treatment of neurogenic orthostatic hypotension and associated supine hypertension. J Neurol. 2017 Aug;264(8):1567-1582. doi: 10.1007/s00415-016-8375-x[↩][↩]
- Jansen RW, Lipsitz LA. Postprandial hypotension: epidemiology, pathophysiology, and clinical management. Ann Intern Med. 1995 Feb 15;122(4):286-95. doi: 10.7326/0003-4819-122-4-199502150-00009[↩]
- Barber DB, Rogers SJ, Fredrickson MD, Able AC. Midodrine hydrochloride and the treatment of orthostatic hypotension in tetraplegia: two cases and a review of the literature. Spinal Cord. 2000 Feb;38(2):109-11. doi: 10.1038/sj.sc.3100959[↩]
- Davies B, Bannister R, Sever P. Pressor amines and monoamine-oxidase inhibitors for treatment of postural hypotension in autonomic failure. Limitations and hazards. Lancet. 1978 Jan 28;1(8057):172-5. doi: 10.1016/s0140-6736(78)90610-4[↩]
- Groomes TE, Huang CT. Orthostatic hypotension after spinal cord injury: treatment with fludrocortisone and ergotamine. Arch Phys Med Rehabil. 1991 Jan;72(1):56-8.[↩]
- Fehlings MG, Tetreault LA, Aarabi B, Anderson P, Arnold PM, Brodke DS, Burns AS, Chiba K, Dettori JR, Furlan JC, Hawryluk G, Holly LT, Howley S, Jeji T, Kalsi-Ryan S, Kotter M, Kurpad S, Kwon BK, Marino RJ, Martin AR, Massicotte E, Merli G, Middleton JW, Nakashima H, Nagoshi N, Palmieri K, Singh A, Skelly AC, Tsai EC, Vaccaro A, Wilson JR, Yee A, Harrop JS. A Clinical Practice Guideline for the Management of Patients With Acute Spinal Cord Injury: Recommendations on the Type and Timing of Anticoagulant Thromboprophylaxis. Global Spine J. 2017 Sep;7(3 Suppl):212S-220S. doi: 10.1177/2192568217702107[↩]
- Readdy WJ, Whetstone WD, Ferguson AR, Talbott JF, Inoue T, Saigal R, Bresnahan JC, Beattie MS, Pan JZ, Manley GT, Dhall SS. Complications and outcomes of vasopressor usage in acute traumatic central cord syndrome. J Neurosurg Spine. 2015 Nov;23(5):574-580. doi: 10.3171/2015.2.SPINE14746[↩][↩][↩]
- Farkas GJ, Burton AM, McMillan DW, Sneij A, Gater DR Jr. The Diagnosis and Management of Cardiometabolic Risk and Cardiometabolic Syndrome after Spinal Cord Injury. J Pers Med. 2022 Jun 30;12(7):1088. doi: 10.3390/jpm12071088[↩]
- van den Noort JC, Bar-On L, Aertbeliën E, Bonikowski M, Braendvik SM, Broström EW, Buizer AI, Burridge JH, van Campenhout A, Dan B, Fleuren JF, Grunt S, Heinen F, Horemans HL, Jansen C, Kranzl A, Krautwurst BK, van der Krogt M, Lerma Lara S, Lidbeck CM, Lin JP, Martinez I, Meskers C, Metaxiotis D, Molenaers G, Patikas DA, Rémy-Néris O, Roeleveld K, Shortland AP, Sikkens J, Sloot L, Vermeulen RJ, Wimmer C, Schröder AS, Schless S, Becher JG, Desloovere K, Harlaar J. European consensus on the concepts and measurement of the pathophysiological neuromuscular responses to passive muscle stretch. Eur J Neurol. 2017 Jul;24(7):981-e38. doi: 10.1111/ene.13322[↩]
- Hsieh JT, Wolfe DL, Miller WC, Curt A; SCIRE Research Team. Spasticity outcome measures in spinal cord injury: psychometric properties and clinical utility. Spinal Cord. 2008 Feb;46(2):86-95. doi: 10.1038/sj.sc.3102125[↩]
- Bovend’Eerdt TJ, Newman M, Barker K, Dawes H, Minelli C, Wade DT. The effects of stretching in spasticity: a systematic review. Arch Phys Med Rehabil. 2008 Jul;89(7):1395-406. doi: 10.1016/j.apmr.2008.02.015[↩]
- Ottoson D. The effects of temperature on the isolated muscle spindle. J Physiol. 1965 Oct;180(3):636-48. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1357407/pdf/jphysiol01167-0190.pdf[↩]
- Bekhet AH, Bochkezanian V, Saab IM, Gorgey AS. The Effects of Electrical Stimulation Parameters in Managing Spasticity After Spinal Cord Injury: A Systematic Review. Am J Phys Med Rehabil. 2019 Jun;98(6):484-499. doi: 10.1097/PHM.0000000000001064[↩]
- Korzhova J, Sinitsyn D, Chervyakov A, Poydasheva A, Zakharova M, Suponeva N, Chernikova L, Piradov M. Transcranial and spinal cord magnetic stimulation in treatment of spasticity: a literature review and meta-analysis. Eur J Phys Rehabil Med. 2018 Feb;54(1):75-84. doi: 10.23736/S1973-9087.16.04433-6[↩]
- Cabahug P, Pickard C, Edmiston T, Lieberman JA. A Primary Care Provider’s Guide to Spasticity Management in Spinal Cord Injury. Top Spinal Cord Inj Rehabil. 2020 Summer;26(3):157-165. doi: 10.46292/sci2603-157[↩]
- Barbeau H, Richards CL, Bédard PJ. Action of cyproheptadine in spastic paraparetic patients. J Neurol Neurosurg Psychiatry. 1982 Oct;45(10):923-6. doi: 10.1136/jnnp.45.10.923[↩]
- Whiting PF, Wolff RF, Deshpande S, Di Nisio M, Duffy S, Hernandez AV, Keurentjes JC, Lang S, Misso K, Ryder S, Schmidlkofer S, Westwood M, Kleijnen J. Cannabinoids for Medical Use: A Systematic Review and Meta-analysis. JAMA. 2015 Jun 23-30;313(24):2456-73. doi: 10.1001/jama.2015.6358. Erratum in: JAMA. 2015 Aug 4;314(5):520. Erratum in: JAMA. 2015 Aug 25;314(8):837. Erratum in: JAMA. 2015 Dec 1;314(21):2308. Erratum in: JAMA. 2016 Apr 12;315(14):1522.[↩]
- Wiener J, Hsieh J, McIntyre A, Teasell R. Effectiveness of 4-Aminopyridine for the Management of Spasticity in Spinal Cord Injury: A Systematic Review. Top Spinal Cord Inj Rehabil. 2018 Fall;24(4):353-362. doi: 10.1310/sci17-00048[↩]
- Moeini-Naghani I, Hashemi-Zonouz T, Jabbari B. Botulinum Toxin Treatment of Spasticity in Adults and Children. Semin Neurol. 2016 Feb;36(1):64-72. doi: 10.1055/s-0036-1571847[↩]
- Lui J, Sarai M, Mills PB. Chemodenervation for treatment of limb spasticity following spinal cord injury: a systematic review. Spinal Cord. 2015 Apr;53(4):252-64. doi: 10.1038/sc.2014.241[↩]
- Boviatsis EJ, Kouyialis AT, Korfias S, Sakas DE. Functional outcome of intrathecal baclofen administration for severe spasticity. Clin Neurol Neurosurg. 2005 Jun;107(4):289-95. doi: 10.1016/j.clineuro.2004.09.007[↩]
- Jozefczyk PB. The management of focal spasticity. Clin Neuropharmacol. 2002 May-Jun;25(3):158-73. doi: 10.1097/00002826-200205000-00006[↩]
- Madsen PJ, Isaac Chen HC, Lang SS. Neurosurgical Approaches. Phys Med Rehabil Clin N Am. 2018 Aug;29(3):553-565. doi: 10.1016/j.pmr.2018.04.002[↩]
- Nagel SJ, Wilson S, Johnson MD, Machado A, Frizon L, Chardon MK, Reddy CG, Gillies GT, Howard MA 3rd. Spinal Cord Stimulation for Spasticity: Historical Approaches, Current Status, and Future Directions. Neuromodulation. 2017 Jun;20(4):307-321. doi: 10.1111/ner.12591[↩]
- Yelamarthy, P.K.K., Chhabra, H.S., Vaccaro, A. et al. Management and prognosis of acute traumatic cervical central cord syndrome: systematic review and Spinal Cord Society—Spine Trauma Study Group position statement. Eur Spine J 28, 2390–2407 (2019). https://doi.org/10.1007/s00586-019-06085-z Erratum in: Eur Spine J. 2021 Jan;30(1):232-233.[↩][↩][↩][↩][↩][↩]
- Krassioukov A, Warburton DE, Teasell R, Eng JJ; Spinal Cord Injury Rehabilitation Evidence Research Team. A systematic review of the management of autonomic dysreflexia after spinal cord injury. Arch Phys Med Rehabil. 2009 Apr;90(4):682-95. doi: 10.1016/j.apmr.2008.10.017[↩]
- Budisin B, Bradbury CC, Sharma B, Hitzig SL, Mikulis D, Craven C, McGilivray C, Corbie J, Green RE. Traumatic Brain Injury in Spinal Cord Injury: Frequency and Risk Factors. J Head Trauma Rehabil. 2016 Jul-Aug;31(4):E33-42. doi: 10.1097/HTR.0000000000000153[↩]
- Pandrich MJ, Demetriades AK. Prevalence of concomitant traumatic cranio-spinal injury: a systematic review and meta-analysis. Neurosurg Rev. 2020 Feb;43(1):69-77. doi: 10.1007/s10143-018-0988-3[↩]
- Gilron I, Baron R, Jensen T. Neuropathic pain: principles of diagnosis and treatment. Mayo Clin Proc. 2015 Apr;90(4):532-45. doi: 10.1016/j.mayocp.2015.01.018[↩]
- Levendoglu F, Ogün CO, Ozerbil O, Ogün TC, Ugurlu H. Gabapentin is a first line drug for the treatment of neuropathic pain in spinal cord injury. Spine (Phila Pa 1976). 2004 Apr 1;29(7):743-51. doi: 10.1097/01.brs.0000112068.16108.3a[↩]
- Bates D, Schultheis BC, Hanes MC, Jolly SM, Chakravarthy KV, Deer TR, Levy RM, Hunter CW. A Comprehensive Algorithm for Management of Neuropathic Pain. Pain Med. 2019 Jun 1;20(Suppl 1):S2-S12. doi: 10.1093/pm/pnz075. Erratum in: Pain Med. 2023 Feb 1;24(2):219.[↩]
- Guy SD, Mehta S, Casalino A, Côté I, Kras-Dupuis A, Moulin DE, Parrent AG, Potter P, Short C, Teasell R, Bradbury CL, Bryce TN, Craven BC, Finnerup NB, Harvey D, Hitzig SL, Lau B, Middleton JW, O’Connell C, Orenczuk S, Siddall PJ, Townson A, Truchon C, Widerström-Noga E, Wolfe D, Loh E. The CanPain SCI Clinical Practice Guidelines for Rehabilitation Management of Neuropathic Pain after Spinal Cord: Recommendations for treatment. Spinal Cord. 2016 Aug;54 Suppl 1:S14-23. doi: 10.1038/sc.2016.90[↩][↩]
- Norrbrink C, Lundeberg T. Tramadol in neuropathic pain after spinal cord injury: a randomized, double-blind, placebo-controlled trial. Clin J Pain. 2009 Mar-Apr;25(3):177-84. doi: 10.1097/AJP.0b013e31818a744d[↩]
- Li L, Han Y, Li T, Zhou J, Sun C, Xue Y. The analgesic effect of intravenous methylprednisolone on acute neuropathic pain with allodynia due to central cord syndrome: a retrospective study. J Pain Res. 2018 Jun 25;11:1231-1238. doi: 10.2147/JPR.S160463[↩]
- Parthiban J, Zileli M, Sharif SY. Outcomes of Spinal Cord Injury: WFNS Spine Committee Recommendations. Neurospine. 2020 Dec;17(4):809-819. doi: 10.14245/ns.2040490.245[↩][↩]
- Yue JK, Winkler EA, Rick JW, Deng H, Partow CP, Upadhyayula PS, Birk HS, Chan AK, Dhall SS. Update on critical care for acute spinal cord injury in the setting of polytrauma. Neurosurg Focus. 2017 Nov;43(5):E19. doi: 10.3171/2017.7.FOCUS17396[↩][↩]
- Fehlings MG, Tetreault LA, Wilson JR, et al. A Clinical Practice Guideline for the Management of Patients With Acute Spinal Cord Injury and Central Cord Syndrome: Recommendations on the Timing (≤24 Hours Versus >24 Hours) of Decompressive Surgery. Global Spine J. 2017 Sep;7(3 Suppl):195S-202S. doi: 10.1177/2192568217706367[↩][↩]
- Ahuja CS, Schroeder GD, Vaccaro AR, Fehlings MG. Spinal Cord Injury-What Are the Controversies? J Orthop Trauma. 2017 Sep;31 Suppl 4:S7-S13. doi: 10.1097/BOT.0000000000000943[↩][↩]
- Ryken TC, Hadley MN, Walters BC, Aarabi B, Dhall SS, Gelb DE, Hurlbert RJ, Rozzelle CJ, Theodore N. Radiographic assessment. Neurosurgery. 2013 Mar;72 Suppl 2:54-72. doi: 10.1227/NEU.0b013e318276edee[↩]
- Consortium for Spinal Cord Medicine. Early acute management in adults with spinal cord injury: a clinical practice guideline for health-care professionals. J Spinal Cord Med. 2008;31(4):403-79. doi: 10.1043/1079-0268-31.4.408[↩][↩]
- Brooks NP. Central Cord Syndrome. Neurosurg Clin N Am. 2017 Jan;28(1):41-47. doi: 10.1016/j.nec.2016.08.002[↩][↩][↩][↩]
- Pouw, M., van Middendorp, J., van Kampen, A. et al. Diagnostic criteria of traumatic central cord syndrome. Part 1: A systematic review of clinical descriptors and scores. Spinal Cord 48, 652–656 (2010). https://doi.org/10.1038/sc.2009.155[↩]
- Galvagno SM Jr, Nahmias JT, Young DA. Advanced Trauma Life Support® Update 2019: Management and Applications for Adults and Special Populations. Anesthesiol Clin. 2019 Mar;37(1):13-32. doi: 10.1016/j.anclin.2018.09.009[↩]
- Wilson JR, Witiw CD, Badhiwala J, Kwon BK, Fehlings MG, Harrop JS. Early Surgery for Traumatic Spinal Cord Injury: Where Are We Now? Global Spine J. 2020 Jan;10(1 Suppl):84S-91S. doi: 10.1177/2192568219877860[↩]
- Zheng C, Yu Q, Shan X, Zhu Y, Lyu F, Ma X, Zhou S, Jiang J. Early Surgical Decompression Ameliorates Dysfunction of Spinal Motor Neuron in Patients With Acute Traumatic Central Cord Syndrome: An Ambispective Cohort Analysis. Spine (Phila Pa 1976). 2020 Jul 15;45(14):E829-E838. doi: 10.1097/BRS.0000000000003447[↩]
- Godzik J, Dalton J, Hemphill C, Walker C, Chapple K, Cook A, Uribe JS, Turner JD. Early surgical intervention among patients with acute central cord syndrome is not associated with higher mortality and morbidity. J Spine Surg. 2019 Dec;5(4):466-474. doi: 10.21037/jss.2019.09.26[↩]
- Fehlings MG, Tetreault LA, Wilson JR, et al. A clinical practice guideline for the management of acute spinal cord injury: introduction, rationale, and scope. Global Spine J. 2017;7(3 suppl):84S–94S. doi:10.1177/2192568217703387[↩][↩]
- Doulames VM, Plant GW. Induced Pluripotent Stem Cell Therapies for Cervical Spinal Cord Injury. Int J Mol Sci. 2016 Apr 9;17(4):530. doi: 10.3390/ijms17040530[↩]
- Lee YS, Kim KT, Kwon BK. Hemodynamic Management of Acute Spinal Cord Injury: A Literature Review. Neurospine. 2021 Mar;18(1):7-14. doi: 10.14245/ns.2040144.072[↩]
- Evaniew N, Noonan VK, Fallah N, Kwon BK, Rivers CS, Ahn H, Bailey CS, Christie SD, Fourney DR, Hurlbert RJ, Linassi AG, Fehlings MG, Dvorak MF; RHSCIR Network. Methylprednisolone for the Treatment of Patients with Acute Spinal Cord Injuries: A Propensity Score-Matched Cohort Study from a Canadian Multi-Center Spinal Cord Injury Registry. J Neurotrauma. 2015 Nov 1;32(21):1674-83. doi: 10.1089/neu.2015.3963[↩]
- Fehlings MG, Tetreault LA, Wilson JR, Kwon BK, Burns AS, Martin AR, Hawryluk G, Harrop JS. A Clinical Practice Guideline for the Management of Acute Spinal Cord Injury: Introduction, Rationale, and Scope. Global Spine J. 2017 Sep;7(3 Suppl):84S-94S. doi: 10.1177/2192568217703387[↩][↩]
- Wiginton JG 4th, Brazdzionis J, Mohrdar C, Sweiss R, Lawandy S. Spinal Cord Reperfusion Injury: Case Report, Review of the Literature, and Future Treatment Strategies. Cureus. 2019 Jul 30;11(7):e5279. doi: 10.7759/cureus.5279[↩]
- Schlaff CD, Sack KD, Elliott RJ, Rosner MK. Early Experience with Electric Scooter Injuries Requiring Neurosurgical Evaluation in District of Columbia: A Case Series. World Neurosurg. 2019 Dec;132:202-207. doi: 10.1016/j.wneu.2019.08.237[↩]
- Roth EJ, Lawler MH, Yarkony GM. Traumatic central cord syndrome: clinical features and functional outcomes. Arch Phys Med Rehabil. 1990 Jan;71(1):18-23.[↩][↩]
- Hohl JB, Lee JY, Horton JA, Rihn JA. A novel classification system for traumatic central cord syndrome: the central cord injury scale (CCIS). Spine (Phila Pa 1976). 2010 Apr 1;35(7):E238-43. doi: 10.1097/BRS.0b013e3181c15887[↩]
- Nasri A, Kacem I, Sidhom Y, Djebara MB, Gargouri A, Gouider R. Isolated spinal cord compression syndrome revealing delayed extensive superficial siderosis of the central nervous system secondary to cervical root avulsion. J Spinal Cord Med. 2018 Jul;41(4):490-495. doi: 10.1080/10790268.2017.1329053[↩]
- Aito S, D’Andrea M, Werhagen L, Farsetti L, Cappelli S, Bandini B, Di Donna V. Neurological and functional outcome in traumatic central cord syndrome. Spinal Cord. 2007 Apr;45(4):292-7. doi: 10.1038/sj.sc.3101944[↩][↩]
- Molliqaj G, Payer M, Schaller K, Tessitore E. Acute traumatic central cord syndrome: a comprehensive review. Neurochirurgie. 2014;60:5–11. doi:10.1016/j.neuchi.2013.12.002[↩]
- Uribe J, Green BA, Vanni S, Moza K, Guest JD, Levi AD. Acute traumatic central cord syndrome—experience using surgical decompression with open-door expansile cervical laminoplasty. Surg Neurol. 2005;63:505–510. doi:10.1016/j.surneu.2004.09.037[↩]
- Bose B, Northrup BE, Osterholm JL, Cotler JM, DiTunno JF. Reanalysis of central cervical cord injury management. Neurosurgery. 1984 Sep;15(3):367-72. doi: 10.1227/00006123-198409000-00012[↩]
- Chen TY, Lee ST, Lui TN, Wong CW, Yeh YS, Tzaan WC, Hung SY. Efficacy of surgical treatment in traumatic central cord syndrome. Surg Neurol. 1997 Nov;48(5):435-40; discussion 441. doi: 10.1016/s0090-3019(97)00037-2[↩]
- Chen TY, Dickman CA, Eleraky M, Sonntag VK. The role of decompression for acute incomplete cervical spinal cord injury in cervical spondylosis. Spine (Phila Pa 1976). 1998 Nov 15;23(22):2398-403. doi: 10.1097/00007632-199811150-00007[↩]
- Samuel AM, Grant RA, Bohl DD, et al. Delayed surgery after acute traumatic central cord syndrome is associated with reduced mortality. Spine (Phila Pa 1976). 2015;40:349–356. doi:10.1097/BRS.0000000000000756[↩]
- Schroeder GD, Kepler CK, Hjelm N, Vaccaro AR, Weinstein MS. The effect of vertebral fracture on the early neurologic recovery in patients with central cord syndrome. Eur Spine J. 2015;24:985–989. doi:10.1007/s00586-015-3865-6[↩]
- Schroeder GD, Hjelm N, Vaccaro AR, Weinstein MS, Kepler CK. The effect of increased T2 signal intensity in the spinal cord on the injury severity and early neurological recovery in patients with central cord syndrome. J Neurosurg Spine. 2016;24:792–796. doi:10.3171/2015.9.SPINE15661[↩]
- Blasetti G, Pavese C, Maier DD, Weidner N, Rupp R, Abel R, Yorck BK, Jiri K, Curt A, Molinari M, Schubert M, Scivoletto G. Comparison of outcomes between people with and without central cord syndrome. Spinal Cord. 2020 Dec;58(12):1263-1273. doi: 10.1038/s41393-020-0491-x[↩][↩]
- Segal DN, Grabel ZJ, Heller JG, Rhee JM, Michael KW, Yoon ST, Jain A. Epidemiology and treatment of central cord syndrome in the United States. J Spine Surg. 2018 Dec;4(4):712-716. doi: 10.21037/jss.2018.11.02[↩][↩]
- Yousefifard M, Rahimi-Movaghar V, Baikpour M, Ghelichkhani P, Hosseini M, Jafari A, Aziznejad H, Tafakhori A. Early versus late spinal decompression surgery in treatment of traumatic spinal cord injuries; a systematic review and meta-analysis. Emerg (Tehran). 2017;5(1):e37. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5325907[↩]
- OSCIS investigators; Chikuda H, Koyama Y, Matsubayashi Y, et al. Effect of Early vs Delayed Surgical Treatment on Motor Recovery in Incomplete Cervical Spinal Cord Injury With Preexisting Cervical Stenosis: A Randomized Clinical Trial. JAMA Netw Open. 2021 Nov 1;4(11):e2133604. doi: 10.1001/jamanetworkopen.2021.33604. Erratum in: JAMA Netw Open. 2021 Dec 1;4(12):e2143306.[↩]
- Li J, Shi D, Hua Z, Wang L. The Assessment of Dynamic Spinal Cord Impingement by Kinematic Magnetic Resonance Imaging in Patients with Traumatic Central Cord Syndrome. Ther Clin Risk Manag. 2021 Jan 7;17:23-29. doi: 10.2147/TCRM.S288076[↩]
- Aarabi B, Akhtar-Danesh N, Chryssikos T, Shanmuganathan K, Schwartzbauer GT, Simard JM, Olexa J, Sansur CA, Crandall KM, Mushlin H, Kole MJ, Le EJ, Wessell AP, Pratt N, Cannarsa G, Lomangino C, Scarboro M, Aresco C, Oliver J, Caffes N, Carbine S, Mori K. Efficacy of Ultra-Early (< 12 h), Early (12-24 h), and Late (>24-138.5 h) Surgery with Magnetic Resonance Imaging-Confirmed Decompression in American Spinal Injury Association Impairment Scale Grades A, B, and C Cervical Spinal Cord Injury. J Neurotrauma. 2020 Feb 1;37(3):448-457. doi: 10.1089/neu.2019.6606[↩]
- Nakajima H, Yokogawa N, Sasagawa T, Ando K, Segi N, Watanabe K, Nori S, Watanabe S, Honjoh K, Funayama T, Eto F, Terashima Y, Hirota R, Furuya T, Yamada T, Inoue G, Kaito T, Kato S; JASA Study Group. Prognostic Factors for Cervical Spinal Cord Injury without Major Bone Injury in Elderly Patients. J Neurotrauma. 2022 May;39(9-10):658-666. doi: 10.1089/neu.2021.0351[↩]
- Kirshblum S, Snider B, Eren F, Guest J. Characterizing Natural Recovery after Traumatic Spinal Cord Injury. J Neurotrauma. 2021 May 1;38(9):1267-1284. doi: 10.1089/neu.2020.7473[↩]
- Fouad K, Popovich PG, Kopp MA, Schwab JM. The neuroanatomical-functional paradox in spinal cord injury. Nat Rev Neurol. 2021 Jan;17(1):53-62. doi: 10.1038/s41582-020-00436-x. Epub 2020 Dec 11. Erratum in: Nat Rev Neurol. 2023 Aug 8[↩][↩]





{kind=link}