
Contents
What is a compression fracture
Compression fracture the spine also called vertebral compression fracture is when the bone tissue of the vertebra collapses. Compression fracture the spine can occur because of trauma or a disease process such as osteoporosis or a tumor. Vertebral compression fractures by definition compromise the anterior column of the spine, thereby resulting in compromise to the anterior half of the vertebral body and the anterior longitudinal ligament 1. Vertebral compression fractures do not involve the posterior half of the vertebral body and do not involve the posterior osseous ligamentous complex 1. The former distinguishes a compression fracture from a burst fracture. The implications of these compression fractures are related to the stability of the resulting structure and potential for deformity progression. Compression fractures are usually considered stable and do not require surgical instrumentation 2.
Approximately 1 to 1.5 million vertebral compression fractures occur annually in the United States alone 1. Moreover, it is estimated that 40% to 50% of patients over age 80 years have sustained a vertebral compression fracture either acutely, or recognized incidentally during clinical workup for a separate condition 3. Recent reports cite the thoracolumbar junction (i.e., the segment from T12 to L2) as the location afflicted with 60% to 75% of vertebral compression fractures, and another 30% occur at the L2 to L5 region (lumbar compression fracture) 1.
In younger patients, about 50% compression fracture of spine are due to motor vehicle collisions with another 25% being due to falls. This is in stark contrast to the elderly mechanism of injury at presentation. Studies have reported an estimate of 30% of vertebral compression fractures occurring while the patient is in bed 1. As the population continues to age, the population at risk of sustaining low energy fragility fractures will continue to increase as well. Currently, 10 million Americans are already diagnosed with osteoporosis, and another 34 million have osteopenia 1. Population studies have shown that the annual incidence of vertebral compression fractures is 10.7 per 1000 women and 5.7 per 1000 men 1. However, compression fractures are reportedly under diagnosed due to clinically silent fractures, nonspecific back pain, and unreported fractures 4. Early diagnosis is important, as partial compression of one vertebral body portends increased risk for progressive fracturing of that vertebra, compression fracturing of one vertebra positively correlates with subsequent compression fracturing of other vertebrae, and vertebral compression increases the risk profile for hip fractures 5. Mild compression fractures increase patient risk for new fractures 6.
Due to the ligamentous and anatomical changes noted as one travels from the thoracic to the lumbar level, inherent areas of instability make this a frequent site of injury. For the spinal column, traditional teaching is that the column can be divided into three sections: (1) anterior column (anterior longitudinal ligament, anterior annulus, the anterior portion of the vertebral body, (2) middle column (posterior vertebral body, posterior annulus, and posterior longitudinal ligament), and (3) the posterior column (ligamentum flavum, neural arch, facets, posterior ligamentous complex). If two of these three columns are compromised, the injury is considered unstable, and the patient potentially needs surgery.
Compression fractures by definition only involve compromise to the anterior column alone 1. Thus, vertebral compression fractures are considered “stable” fracture patterns. When they progress to the middle and/or posterior column, they become burst fractures.
Compression fracture causes
The most common cause of vertebral compression fractures is osteoporosis, making these fractures the most common fragility fracture. Osteoporosis is a disease in which bones become fragile. Compression fractures demonstrate a bimodal distribution with younger patients sustaining these injuries secondary to high energy mechanisms (fall from a height, motor vehicle accident, etc.) 7. In most cases, bone loses calcium and other minerals with age. Other causes may include:
- Trauma to the back
- Tumors that started in the bone or spread to the bone from elsewhere
- Tumors that start in the spine, such as multiple myeloma
Having many compression fractures of the vertebrae (bones of the spine) can lead to kyphosis. This is a hump-like curvature of the spine.
During a fall or trauma, the spinal column will rotate around a center of axis for this rotation. There is also an associated axial force applied due to this flexion/extension of the spine. An axial force more than the forces tolerable by the vertebral body leads initially to a compression fracture with more significant forces resulting in a burst fracture. The resulting kyphotic (forward flexion of the spine) deformity of the compression fracture may alter the spine biomechanics, placing additional stresses on other spine levels. The altered biomechanics risk additional fractures and progressive deformity. The occurrence an osteoporotic compression fracture increases the risk of an additional compression fracture.
Compression fracture prevention
Taking steps to prevent and treat osteoporosis is the most effective way to prevent compression or insufficiency fractures. Getting regular load-bearing exercise (such as walking) can help you avoid bone loss.
Compression fracture symptoms
Compression fractures can occur suddenly. This can cause severe back pain.
- The pain is most commonly felt in the middle or lower spine. It can also be felt on the sides or in the front of the spine.
- The pain is sharp and “knife-like.” Pain can be disabling, and take weeks to months to go away.
Compression fractures due to osteoporosis may cause no symptoms at first. Often, they are discovered when x-rays of the spine are done for other reasons. Over time, the following symptoms may occur:
- Back pain that starts slowly, and gets worse with walking, but is not felt when resting
- Loss of height, as much as 6 inches (15 centimeters) over time
- Stooped-over posture, or kyphosis, also called a dowager’s hump
Pressure on the spinal cord from hunched over posture can, in rare cases, cause:
- Numbness
- Tingling
- Weakness
- Difficulty walking
- Loss of control of the bowel or bladder
Compression fracture possible complications
Compression fracture complications may include:
- Failure of the bones to fuse after surgery
- Humpback
- Spinal cord or nerve root compression
Compression fracture diagnosis
Your doctor will perform a physical exam. This may show:
- A humpback, or kyphosis
- Tenderness over the affected spinal bone or bones
A spine x-ray may show at least 1 compressed vertebra that is shorter than the other vertebrae.
Other tests that may be done:
- A bone density test to evaluate for osteoporosis
- A CT or MRI scan, if there is a concern that the fracture was caused by a tumor or severe trauma (such as a fall or car accident)
Evaluation of patients with suspected back trauma includes anterior-posterior (AP) and lateral radiographs of the impacted area. In the trauma setting these initially, should be obtained supine with spine precautions until cleared by the spine team or bracing has been provided. At some point, standing radiographs in the brace are helpful to guide treatment as a supine position may artificially reduce a displaced fracture 8.
A CT should also be obtained in all trauma settings. If there is a suspected posterior column injury not able to be confirmed on CT, an MRI will indicate disruption of the posterior ligamentous complex. Radiographs showing 30 degrees of traumatic kyphosis (forward flexion of the spine) and 50% vertebral body height loss are historically thought to be unstable fractures, but new evidence is changing this belief. Furthermore, any neurologic deficit necessitates an MRI for additional evaluation. Elderly patients with low energy compression fractures likely will not require an MRI. Serial standing lateral radiographs obtained in the clinic will help track the fracture progression and healing.
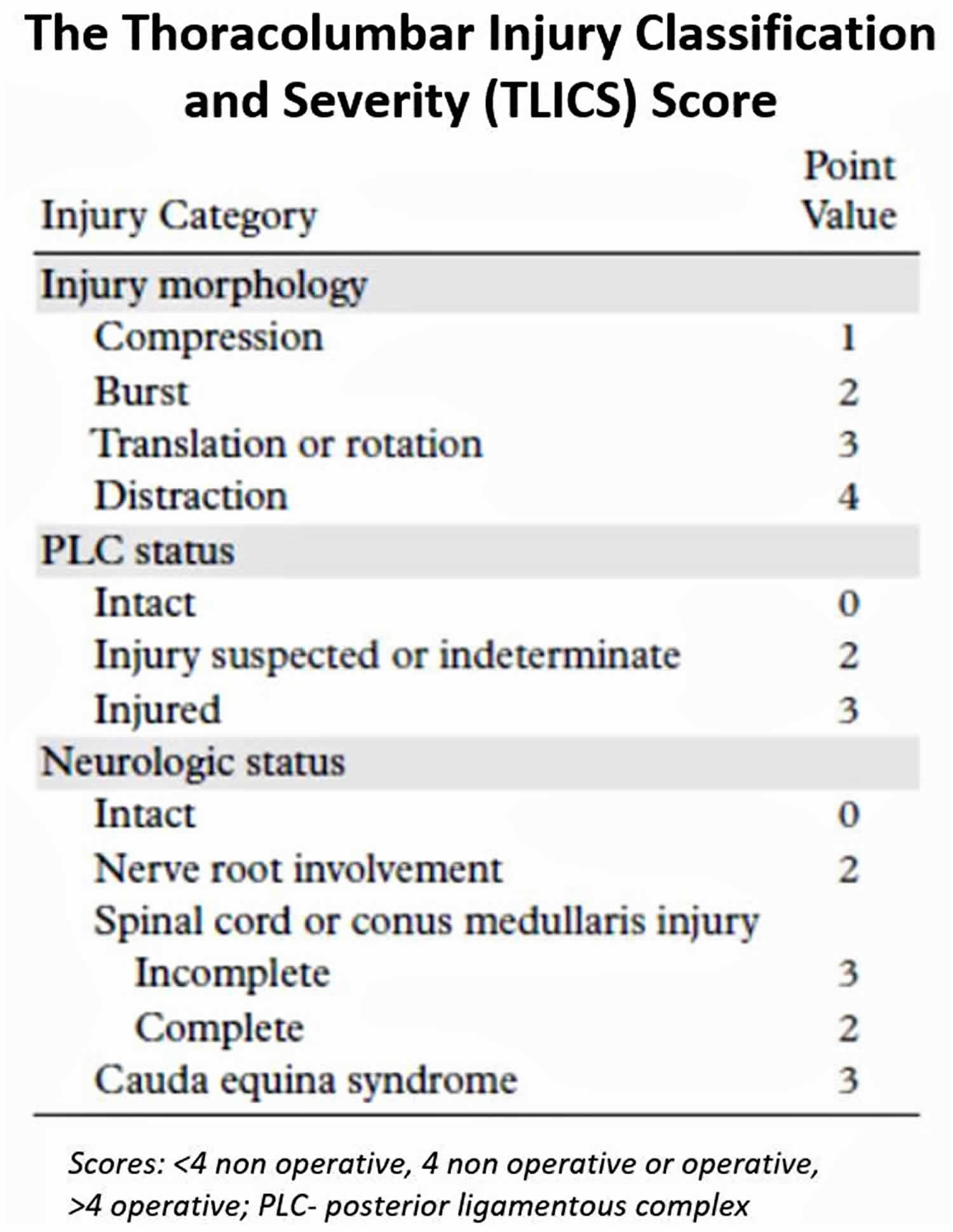
In 2005, a classifications system was introduced to provide more uniformity in management and provide simple treatment recommendations. The Thoracolumbar Injury Classification and Severity Scale (Figure 1) uses the posterior ligamentous complex, injury morphology, and neurological status to provide a score (one to ten) that can guide intervention: less than four favoring non-surgical treatment, more than four surgical, and four being managed by either. Of course, these are general guidelines, predominantly for trauma patients, and each case should be evaluated carefully. Interestingly, newer studies have shown that historical considerations such as loss of vertebral body height, segmental kyphosis, and canal compromise, do not correlate with the need for surgery (in those neurologically intact patients).
Figure 1. Thoracolumbar Injury Classification and Severity Scale
Compression fracture treatment
Most compression fractures are seen in older people with osteoporosis. These fractures often do not cause injury to the spinal cord. The condition is usually treated with medicines and calcium supplements to prevent further fractures.
Pain may be treated with:
- Pain medicine
- Bed rest
Other treatments may include:
- Back braces, but these may further weaken the bones and increase the risk of more fractures
- Physical therapy to improve movement and strength around the spine
- A medicine called calcitonin to help relieve bone pain
Orthosis/bracing modalities accomplish conservative management for a period of four to 12 weeks. Discontinuation of the bracing can be considered when there is radiographic evidence of healing, and the patient no longer is tender over the fracture site. In that bed rest, analgesic medications, and bracing are poorly tolerated in the elderly; many will alternatively consider percutaneous procedures such as kyphoplasties for stabilization of the fracture and faster clinical improvement.
Surgery may be done if you have severe and disabling pain for more than 2 months that does not get better with other treatments. Surgery can include:
- Balloon kyphoplasty
- Vertebroplasty
- Spinal fusion
Surgical options are largely dependent on fracture characteristics and neurologic injury. Rarely would compression fractures require instrumented stabilization. For patients with osteoporotic compression fractures, kyphoplasty is a relatively safe and simple procedure relying on the percutaneous insertion of a balloon into the vertebral body to restore the height followed by injection of bone cement to maintain the correction. Recent randomized controlled trials have shown kyphoplasties allowing for significantly more rapid improvement in the quality of life, function, pain, and mobility.
Currently, there have been no randomized trials evaluating surgery versus brace treatment in “unstable” compression fractures 9.
Regarding a kyphoplasty treatment for compression fractures, several contraindications should be remembered. These include current neurologic compromise, burst fractures (fractures of the posterior vertebral body wall), spine infections, current sepsis, or underlying bleeding diatheses. Not addressed above are patients with diffuse idiopathic skeletal hyperostosis (DISH) and ankylosing spondylitis 1. Both of these result in brittle spinal columns and a fracture of any type should be considered unstable and require CT, MRI, and potentially surgery.
Other surgery may be done to remove bone if the fracture is due to a tumor.
After surgery you may need:
- A brace for 6 to 10 weeks if the fracture was due to an injury.
- More surgery to join spine bones together or to relieve pressure on a nerve.
Compression fracture prognosis
Most compression fractures due to injury heal in 8 to 10 weeks with rest, wearing of a brace, and pain medicines. However, recovery can take much longer if surgery was done.
Compression fractures due to osteoporosis often become less painful with rest and pain medicines. Some compression fractures, though, can lead to long-term (chronic) pain and disability.
Medicines to treat osteoporosis can help prevent future fractures. However, medicines cannot reverse damage that has already occurred.
For compression fractures caused by tumors, the outcome depends on the type of tumor involved. Tumors that involve the spine include:
- Breast cancer
- Lung cancer
- Lymphoma
- Prostate cancer
- Multiple myeloma
- Hemangioma
- Donnally III CJ, Varacallo M. Vertebral Compression Fractures. [Updated 2019 Jun 10]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2019 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK448171[↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Chen YC, Zhang L, Li EN, Ding LX, Zhang GA, Hou Y, Yuan W. Unilateral versus bilateral percutaneous vertebroplasty for osteoporotic vertebral compression fractures in elderly patients: A meta-analysis. Medicine (Baltimore). 2019 Feb;98(8):e14317[↩]
- Kim HJ, Park S, Park SH, Park J, Chang BS, Lee CK, Yeom JS. Prevalence of Frailty in Patients with Osteoporotic Vertebral Compression Fracture and Its Association with Numbers of Fractures. Yonsei Med. J. 2018 Mar;59(2):317-324[↩]
- Burns JE, Yao J, Summers RM. Vertebral Body Compression Fractures and Bone Density: Automated Detection and Classification on CT Images. Radiology. 2017;284(3):788–797. doi:10.1148/radiol.2017162100 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5584647[↩]
- Adams JE. Opportunistic identification of vertebral fractures. J Clin Densitom 2016;19(1):54–62.[↩]
- Samelson EJ, , Christiansen BA, , Demissie S, , et al. . Reliability of vertebral fracture assessment using multidetector CT lateral scout views: the Framingham Osteoporosis Study. Osteoporos Int 2011;22(4):1123–1131.[↩]
- Maempel JF, Maempel FZ. The speedboat vertebral fracture: a hazard of holiday watersports. Scott Med J. 2019 May;64(2):42-48[↩]
- Expert Panels on Neurological Imaging, Interventional Radiology, and Musculoskeletal Imaging: Shah LM, Jennings JW, Kirsch CFE, Hohenwalter EJ, Beaman FD, Cassidy RC, Johnson MM, Kendi AT, Lo SS, Reitman C, Sahgal A, Scheidt MJ, Schramm K, Wessell DE, Kransdorf MJ, Lorenz JM, Bykowski J. ACR Appropriateness Criteria® Management of Vertebral Compression Fractures. J Am Coll Radiol. 2018 Nov;15(11S):S347-S364[↩]
- Watanabe Y, Ishikawa S, Nagata H, Kojima M. Determinants Associated with Prolonged Hospital Stays for Patients Aged 65 Years or Older with a Vertebral Compression Fracture in a Rural Hospital in Japan. Tohoku J. Exp. Med. 2019 Jan;247(1):27-34.[↩]




{kind=link}