
Contents
What is Dengue fever
Dengue fever is a mosquito-borne tropical disease caused by four related viruses or serotypes: DENV 1, DENV 2, DENV 3, or DENV 4 carried by mosquitoes 1. The four dengue viruses originated in monkeys and independently jumped to humans in Africa or Southeast Asia between 100 and 800 years ago 1. Dengue fever occurs in tropical and subtropical areas of the world. The dengue viruses are transmitted to humans by the bite of an infected mosquito. In the Western Hemisphere, the Aedes aegypti mosquito is the most important transmitter or vector of dengue viruses, although a 2001 outbreak in Hawaii was transmitted by Aedes albopictus. Mild dengue fever causes a high fever, headaches, rashes and muscle and joint pain throughout the body. A severe form of dengue fever, also called dengue hemorrhagic fever, can cause severe bleeding, a sudden drop in blood pressure (shock) and death. However, most cases of dengue fever are mild and go away on their own after about a week.
There are not yet any widely vaccines to prevent infection with dengue virus and the most effective protective measures are those that avoid mosquito bites. When infected, early recognition and prompt supportive treatment can substantially lower the risk of medical complications and death. If severe, dengue fever can damage the lungs, liver or heart.
- In late 2015 and early 2016, the first dengue vaccine, Dengvaxia (CYD-TDV) by Sanofi Pasteur, was registered in several countries for use in individuals 9-45 years of age living in endemic areas 2. For now the best prevention is to reduce mosquito habitat in areas where dengue fever is common.
Dengue fever rarely strikes in the United States — the last reported outbreak was in Texas in 2005 and a small dengue outbreak occurred in Hawaii in 2001. Although dengue rarely occurs in the continental United States, it is endemic in Puerto Rico and in many popular tourist destinations in Latin America, Southeast Asia and the Pacific islands. Most dengue cases in U.S. citizens occur in those inhabitants of Puerto Rico, the U.S. Virgin Islands, Samoa and Guam, which are endemic for the virus. And if you plan to travel to a foreign country, especially one in the tropics, it’s wise to guard against dengue fever. Wearing insect repellent, covering sleep areas with netting, and avoiding the outdoors at dusk and dawn (when mosquitoes are most active) can help lower the chances of infection.
Dengue is found in parts of:
- southeast Asia
- the Caribbean
- the Indian subcontinent
- South and Central America
- Africa
- the Pacific Islands
- Australia
According to the Centers for Disease Control and Prevention (CDC), dengue infections have been reported in more than 100 countries from parts of Africa, the Americas, the Caribbean, the Eastern Mediterranean, Southeast Asia, and the Western Pacific. It is a fast emerging infectious disease, according to the World Health Organization (WHO), with an increasing number of cases and countries affected throughout the world. The actual number is not known because about 75% of cases are asymptomatic, but a recent estimate put the number of annual dengue infections as high as 390 million. Approximately there are over 100 million cases of dengue fever worldwide each year 3.
Millions of cases of dengue infection occur worldwide each year. Dengue fever is most common in Southeast Asia and the western Pacific islands, but the disease has been increasing rapidly in Latin America and the Caribbean.
There is no specific medication for treatment of a dengue infection. Persons who think they have dengue should use analgesics (pain relievers) with acetaminophen and avoid those containing aspirin. They should also rest, drink plenty of fluids, and consult a physician. If they feel worse (e.g., develop vomiting and severe abdominal pain) in the first 24 hours after the fever declines, they should go immediately to the hospital for evaluation.
Is dengue fever contagious?
No. In order for Dengue virus transmission to occur the mosquito must feed on a person during a 5- day period when large amounts of virus are in the blood; this period usually begins a little before the person become symptomatic. Some people never have significant symptoms but can still infect mosquitoes. After entering the mosquito in the blood meal, the virus will require an additional 8-12 days incubation before it can then be transmitted to another human 1. The mosquito remains infected for the remainder of its life, which might be days or a few weeks.
In rare cases dengue can be transmitted in organ transplants or blood transfusions from infected donors, and there is evidence of transmission from an infected pregnant mother to her fetus 1. But in the vast majority of infections, a mosquito bite is responsible.
In many parts of the tropics and subtropics, dengue is endemic, that is, it occurs every year, usually during a season when Aedes mosquito populations are high, often when rainfall is optimal for breeding. These areas are, however, additionally at periodic risk for epidemic dengue, when large numbers of people become infected during a short period. Dengue epidemics require a coincidence of large numbers of vector mosquitoes, large numbers of people with no immunity to one of the four virus types (DENV 1, DENV 2, DENV 3, DENV 4), and the opportunity for contact between the two. Although Aedes are common in the southern U. S., dengue is endemic in northern Mexico, and the U.S. population has no immunity, the lack of dengue transmission in the continental U.S. is primarily because contact between people and the vectors is too infrequent to sustain transmission.
How dengue is spread
Dengue is spread by infected mosquitoes, usually the Aedes aegypti (Figure 1) and Aedes albopictus (Figure 2) varieties.
Dengue viruses are mainly transmitted by the bite of infected Aedes aegypti mosquitoes; an invasive, domestic species with tropical and subtropical worldwide distribution that originated in Africa.
Aedes albopictus, which is another invasive species originally from Asia.
These mosquitoes bite during the day, most often early in the morning or in the early evening before dusk.
They’re often found living around sources of stagnant water in built-up areas, such as wells, water storage tanks or old car tyres.
Dengue isn’t spread from person to person.
You can get it again if you’ve had it before, as you’ll only be immune to one particular variant of the virus.
Figure 1. Aedes aegypti mosquito
 Figure 2. Aedes albopictus mosquito
Figure 2. Aedes albopictus mosquito
Mosquito Life-Cycle
Aedes aegypti, the principal mosquito vector of dengue viruses is an insect closely associated with humans and their dwellings. People not only provide the mosquitoes with blood meals but also water-holding containers in and around the home needed to complete their development.
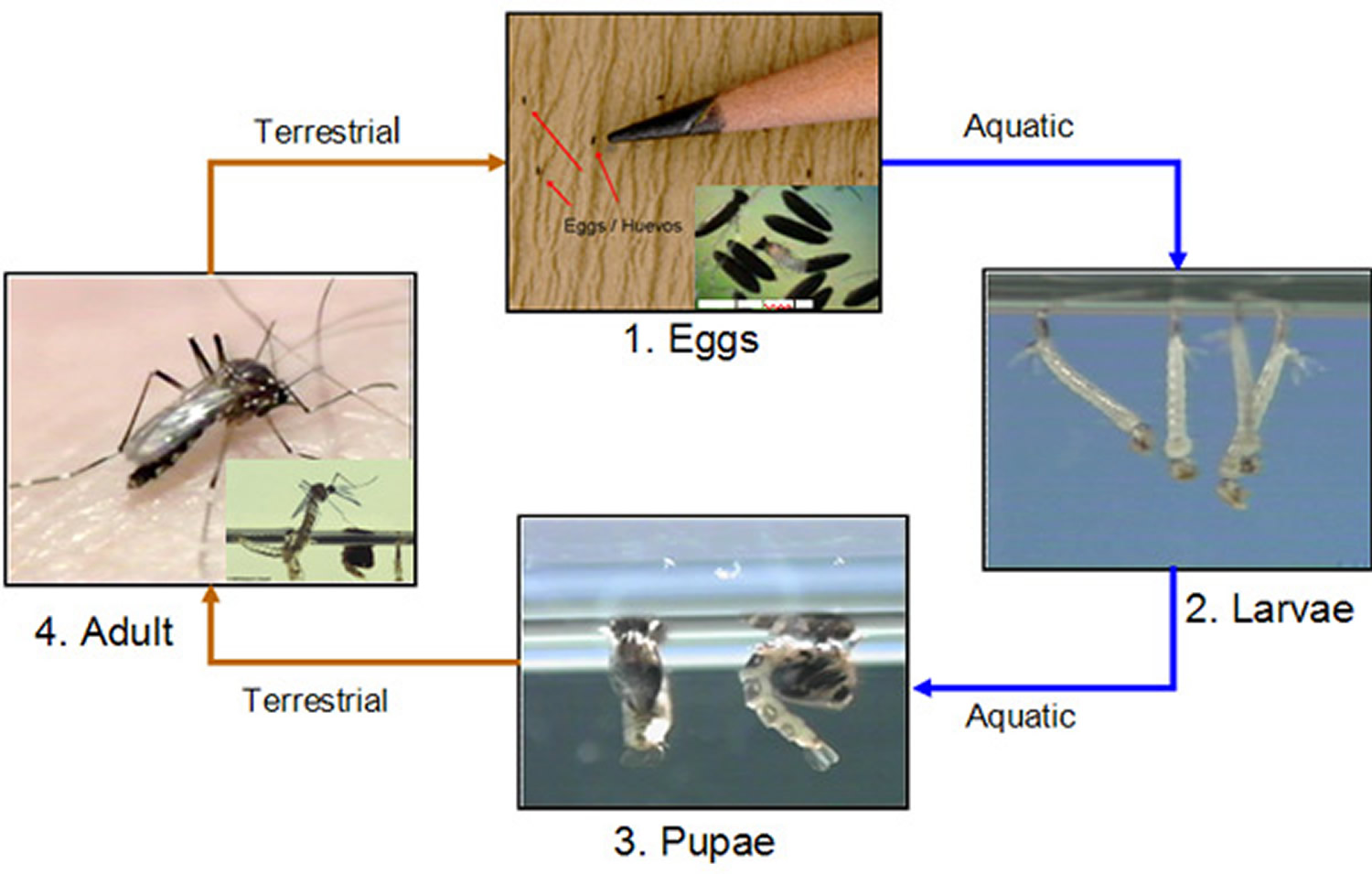
Aedes aegypti and other mosquitoes have a complex life-cycle with dramatic changes in shape, function, and habitat. Female mosquitoes lay their eggs on the inner, wet walls of containers with water. Larvae hatch (Figure 3 #1, inset) when water inundates the eggs as a result of rains or the addition of water by people. In the following days, the larvae (Figure 3 #2) will feed on microorganisms and particulate organic matter, shedding their skins three times to be able to grow from first to fourth instars. When the larva has acquired enough energy and size and is in the fourth instar, metamorphosis is triggered, changing the larva into a pupa (Figure 3 #3). Pupae do not feed; they just change in form until the body of the adult, flying mosquito is formed. Then, the newly formed adult emerges from the water after breaking the pupal skin (Figure 3 #4, inset). The entire life cycle lasts 8-10 days at room temperature, depending on the level of feeding. Thus, there is an aquatic phase (larvae, pupae) and a terrestrial phase (eggs, adults) in the Aedes aegypti life-cycle.
It is this life-cycle complexity that makes it rather difficult to understand where the mosquitoes come from. Similar complex life-cycles with aquatic and terrestrial forms are observed in amphibians.
There is a very important adaptation of dengue vectors that makes controlling their populations a difficult task. Their eggs can withstand desiccation for several months, which means that even if all larvae, pupae, and adults were eliminated at some point in time, repopulation will occur as soon as the eggs in the containers are flooded with water. For example, if you were to eliminate all larvae, pupae, and adult Aedes aegypti at once from a site, its population could recover two weeks later as a result of egg hatching following rainfall or the addition of water to containers harboring eggs. Unfortunately, there is no effective way to control the eggs in containers.
Figure 3. Mosquito Life-Cycle
Dengue fever virus
Dengue viruses are members of the genus Flavivirus, within the family Flaviviridae. There are 4 dengue virus serotypes (DEN-1, DEN-2, DEN-3 and DEN-4), all of which circulate globally, with most endemic countries reporting circulation of all 4 serotypes in recent years 4.
Flaviviruses are lipid-enveloped, positive-sense, single stranded RNA viruses. The structural premembrane (prM) and envelope (E) proteins are embedded in the lipid envelope and are displayed on the surface of virions. The 4 DEN serotypes share only about 60%–75% identity at the amino acid level, and are therefore distinct viruses 5.
Upon human inoculation, the virus replicates in local dendritic cells. Subsequent entry into macrophages and activation of lymphocytes is followed by entry into the bloodstream. Dengue viruses primarily infect cells of the myeloid lineage, including macrophages, monocytes, and dendritic cells. There is evidence of infection of hepatocytes and endothelial cells. Haematogenous spread is the likely mechanism for seeding of peripheral organs and the occasionally reported infection of the central nervous system.
Figure 4. Dengue fever virus (DENV)
How are dengue and dengue hemorrhagic fever spread?
Dengue is transmitted to people by the bite of an Aedes mosquito that is infected with a dengue virus. The mosquito becomes infected with dengue virus when it bites a person who has dengue virus in their blood. The person can either have symptoms of dengue fever or dengue hemorrhagic fever, or they may have no symptoms. After about one week, the mosquito can then transmit the virus while biting a healthy person. Dengue cannot be spread directly from person to person.
Where can outbreaks of dengue occur?
Outbreaks of dengue occur primarily in areas where Aedes aegypti (sometimes also Aedes albopictus) mosquitoes live. This includes most tropical urban areas of the world. Dengue viruses may be introduced into areas by travelers who become infected while visiting other areas of the tropics where dengue commonly exists.
What can be done to reduce the risk of acquiring dengue?
There is no vaccine for preventing dengue. The best preventive measure for residents living in areas infested with Aedes aegypti is to eliminate the places where the mosquito lays her eggs, primarily artificial containers that hold water.
Items that collect rainwater or to store water (for example, plastic containers, 55-gallon drums, buckets, or used automobile tires) should be covered or properly discarded. Pet and animal watering containers and vases with fresh flowers should be emptied and cleaned (to remove eggs) at least once a week. This will eliminate the mosquito eggs and larvae and reduce the number of mosquitoes present in these areas.
Using air conditioning or window and door screens reduces the risk of mosquitoes coming indoors. Proper application of mosquito repellents containing 20% to 30% DEET as the active ingredient on exposed skin and clothing decreases the risk of being bitten by mosquitoes. The risk of dengue infection for international travelers appears to be small. There is increased risk if an epidemic is in progress or visitors are in housing without air conditioning or screened windows and doors.
How can we prevent epidemics of dengue hemorrhagic fever?
The emphasis for dengue prevention is on sustainable, community-based, integrated mosquito control, with limited reliance on insecticides (chemical larvicides, and adulticides). Preventing epidemic disease requires a coordinated community effort to increase awareness about dengue fever/dengue hemorrhagic fever, how to recognize it, and how to control the mosquito that transmits it. Residents are responsible for keeping their yards and patios free of standing water where mosquitoes can be produced.
Dengue fever prevention
There is no widely vaccine available against dengue, and there are no specific medications to treat a dengue infection. This makes prevention the most important step, and prevention means avoiding mosquito bites if you live in or travel to an endemic area.
Reduce mosquito habitat. The mosquitoes that carry the dengue virus typically live in and around houses, breeding in standing water that can collect in such things as used automobile tires. You can help lower mosquito populations by eliminating habitats where they lay their eggs. At least once a week, empty and clean containers that hold standing water, such as planting containers, animal dishes and flower vases. Keep standing water containers covered between cleanings.
The best way to reduce mosquitoes is to eliminate the places where the mosquito lays her eggs, like artificial containers that hold water in and around the home. Outdoors, clean water containers like pet and animal watering containers, flower planter dishes or cover water storage barrels. Look for standing water indoors such as in vases with fresh flowers and clean at least once a week.
The adult mosquitoes like to bite inside as well as around homes, during the day and at night when the lights are on. To protect yourself, use repellent on your skin while indoors or out. When possible, wear long sleeves and pants for additional protection. Also, make sure window and door screens are secure and without holes. If available, use air-conditioning.
If someone in your house is ill with dengue, take extra precautions to prevent mosquitoes from biting the patient and going on to bite others in the household. Sleep under a mosquito bed net, eliminate mosquitoes you find indoors and wear repellent!
List of repellant products approved by the EPA : https://www.epa.gov/insect-repellents/find-repellent-right-you
The following can reduce your risk of being bitten:
- use insect repellent – products containing 50% DEET are most effective, but lower concentrations (15-30% DEET) should be used in children, and alternatives to DEET should be used in children younger than two months
- wear loose but protective clothing – mosquitoes can bite through tight-fitting clothes; trousers, long-sleeved shirts, and socks and shoes (not sandals) are ideal
- sleep under a mosquito net – ideally one that has been treated with insecticide
- be aware of your environment – mosquitoes that spread dengue breed in standing water in urban areas
- stay in air-conditioned or well-screened housing. The mosquitoes that carry the dengue viruses are most active from dawn to dusk, but they can also bite at night.
It’s a good idea to speak to your doctor, practice nurse or a travel clinic before traveling to get specific advice about what you can do to avoid dengue and other travel illnesses.
Dengue fever vaccine
In late 2015 and early 2016, the first dengue vaccine, Dengvaxia (CYD-TDV) by Sanofi Pasteur, was registered in several countries for use in individuals 9-45 years of age living in endemic areas 2. Dengvaxia (CYD-TDV) is a live attenuated (recombinant) tetravalent vaccine.
The World Health Organization (WHO) recommends that countries should consider introduction of the dengue vaccine CYD-TDV only in geographic settings (national or subnational) where epidemiological data indicate a high burden of disease.
The vaccination schedule of Dengvaxia (CYD-TDV) consists of 3 injections of 0.5 mL administered at 6-month intervals. The indication from the first licenses is for the prevention of dengue illness caused by dengue virus serotypes 1, 2, 3, and 4 in individuals 9–45 years or 9–60 years of age (depending on the license), living in dengue endemic areas. The lower limit of the indication at 9 years of age was chosen due to a safety concern in children aged 2–5 years identified in the Phase 3 clinical trials (discussed under vaccine safety).
Based on data collected from Phase 2 studies, following 2 doses the majority of seropositive subjects have a tetravalent response.32 In seronegative subjects, the proportion with a tetravalent response is lower than in the seropositive subjects. The 3-dose series increased the proportion of subjects with a tetravalent response as compared to the 2-dose series, although many seronegative subjects still did not have a tetravalent response after 3 doses 6. However, seroconversion alone does not predict protection. Additional investigations are ongoing to further characterize the relationship between immunologic markers and protection against disease.
Vaccine efficacy varied by country, with efficacy ranging from 31.3% in Mexico to 79.0% in Malaysia 7. This variability in efficacy likely reflects at least in part the baseline seropositivity and circulating serotypes, both of which affect the performance of the vaccine. As completion of the 3-dose series in the Phase 3 trials was very high (over 90%), efficacy after each dose could not be assessed, except in the 6 months following each dose. In the pooled analysis in the indicated age range (9–16 years), vaccine efficacy between doses 1 and 2 was 70.8%, between doses 2 and 3 efficacy was 66.6%, and between dose 3 and 6 months post-dose 3 efficacy was 62.4% 6. The protective effect of doses 1 and 2 beyond 6 months after these doses is unknown, as is the additional protection derived from doses 2 and 3. Second and third doses may influence the duration of efficacy and may have different effects in those seropositive or seronegative at baseline. These research gaps remain to be addressed.
Dengue fever vaccine contraindications
The manufacturer stipulates that vaccination is contraindicated in: (1) individuals with a history of severe allergic reaction to any component of the dengue vaccine or after prior administration of the dengue vaccine or a vaccine containing the same components; (2) individuals with congenital or acquired immune deficiency that impairs cell-mediated immunity; (3) individuals with symptomatic HIV infection or with asymptomatic HIV infection when accompanied by evidence of impaired immune function; (4) pregnant or breastfeeding women; and that vaccination should be postponed in individuals with moderate to severe febrile or acute disease.
Dengue fever symptoms
Symptoms of infection usually begin 4 – 7 days after the mosquito bite and typically last 3 – 10 days.
The principal symptoms of dengue are:
- High fever, which can reach 100.4 °F (40 °C) or higher and at least two of the following:
- Severe headache
- Severe eye pain (behind eyes)
- Joint pain
- Muscle and/or bone pain
- A widespread red rash
- Mild bleeding manifestation (e.g., nose or gum bleed, petechiae, or easy bruising)
- Low white cell count
- Loss of appetite
The symptoms normally pass in about a week, although you may feel tired and slightly unwell for several weeks afterwards.
Generally, younger children and those with their first dengue infection have a milder illness than older children and adults.
In rare cases severe dengue can develop after the initial symptoms. Watch for warning signs as temperature declines 3 to 7 days after symptoms began.
Go IMMEDIATELY to an emergency room or the closest health care provider if any of the following warning signs appear:
- Severe abdominal pain or persistent vomiting
- Red spots or patches on the skin
- Bleeding from nose or gums
- Vomiting blood
- Black, tarry stools (feces, excrement)
- Drowsiness or irritability
- Pale, cold, or clammy skin
- Difficulty breathing
Go to a local doctor or hospital if you develop symptoms while traveling or living in an area where dengue is common.
There’s little a doctor can do to help you recover, but it’s important to get a proper diagnosis in case there’s another cause of your symptoms.
You may need a blood test to confirm that you have dengue.
Figure 5. Dengue fever rash

Dengue hemorrhagic fever
Dengue hemorrhagic fever is characterized by a fever that lasts from 2 to 7 days, with general signs and symptoms consistent with dengue fever. When the fever declines, warning signs including persistent vomiting, severe abdominal pain, and difficulty breathing may develop. This marks the beginning of a 24 to 48 hour period when the smallest blood vessels (capillaries) become excessively permeable (“leaky”), allowing the fluid component to escape from the blood vessels into the peritoneum (causing ascites) and pleural cavity (leading to pleural effusions). This may lead to failure of the circulatory system and shock, and possibly death without prompt, appropriate treatment. In addition, the patient with Dengue hemorrhagic fever has a low platelet count and hemorrhagic manifestations, tendency to bruise easily or have other types of skin hemorrhages, bleeding nose or gums, and possibly internal bleeding.
What causes Dengue fever
Dengue fever is caused by any one of four types of dengue viruses spread by mosquitoes that thrive in and near human lodgings. When a mosquito bites a person infected with a dengue virus, the virus enters the mosquito. When the infected mosquito then bites another person, the virus enters that person’s bloodstream.
After you’ve recovered from dengue fever, you have immunity to the type of virus that infected you — but not to the other three dengue fever virus types. The risk of developing severe dengue fever, also known as dengue hemorrhagic fever, actually increases if you’re infected a second, third or fourth time.
Risk factors for getting Dengue fever
Factors that put you at greater risk of developing dengue fever or a more severe form of the disease include:
- Living or traveling in tropical areas. Being in tropical and subtropical areas increases your risk of exposure to the virus that causes dengue fever. Especially high-risk areas are Southeast Asia, the western Pacific islands, Latin America and the Caribbean.
- Prior infection with a dengue fever virus. Previous infection with a dengue fever virus increases your risk of having severe symptoms if you’re infected again.
Dengue fever diagnosis
Dengue fever is usually diagnosed via some combination of blood tests because the body’s immune response to the virus is dynamic and complex. Laboratory tests may include:
- Molecular tests for dengue virus (PCR)—detect the presence of the virus itself; these tests can diagnose dengue fever up to 7 days after the onset of symptoms and can be used to determine which of the 4 different serotypes of dengue virus is causing the infection.
- Antibody tests, IgM and IgG—detect antibodies produced by the immune system when a person has been exposed to the virus; these tests are most effective when performed at least 4 days after exposure.
- Complete blood count (CBC)—to look for low platelet count typical of the later stages of the illness and to detect the decrease in hemoglobin, hematocrit, and red blood cell (RBC) count (evidence of anemia) that would occur with blood loss associated with severe dengue fever
- Basic metabolic panel (BMP) – to monitor kidney function and look for evidence of dehydration that can occur with severe illness
Laboratory confirmation of dengue virus infection is usually done by serology [IgM antibody-capture enzyme-linked immunosorbent assay (MAC-ELISA), IgG ELISA, plaque reduction and neutralization test (PRNT)], or by molecular methods [reverse transcriptase-polymerase chain reaction (RT-PCR) and detection of dengue non-structural protein 1 (NS1)]; virus isolation is used less commonly.
Diagnosis by serology typically does not allow for serotyping the infecting virus (except by PRNT), and is susceptible to cross-reactivity with other flaviviruses, variable sensitivity by timing of specimen collection, and the need for multiple samples (IgG acute and convalescent samples). RT-PCR and NS1 tests offer earlier and more specific diagnosis (80%–90% sensitivity if assessed 1–3 days after the onset of illness) and are considered virological proof of infection 9.
Testing Algorithms for Dengue 10:
A) Polymerase chain reaction (PCR)
- DENV can be detected in the blood (serum) from patients for approximately the first 5 days of symptoms. Currently, several PCR tests are employed to detect the viral genome in serum. In addition, virus can be isolated and sequenced for additional characterization. Real time RT–PCR assays have been developed and automated; but none of these tests are yet commercially available. Because antibodies are detected later, RT–PCR has become a primary tool to detect virus early in the course of illness. Current tests are between 80-90% sensitive, and more that 95% specific. A positive PCR result is a definite proof of current infection and it usually confirms the infecting serotype as well. However, a negative result is interpreted as “indeterminate”. Patients receiving negative results before 5 days of illness are usually asked to submit a second serum sample for serological confirmation after the 5th day of illness (bellow).
B) MAC ELISA
- IgM antibody capture ELISA (MAC-ELISA) format is most commonly employed in diagnostic laboratories and commercial available diagnostic kits. The assay is based on capturing human IgM antibodies on a microtiter plate using anti-human-IgM antibody followed by the addition of dengue virus specific antigen (DENV1-4). The antigens used for this assay are derived from the envelope protein of the virus. One of the limitation of this testing is the cross reactivity between other circulating flaviviruses. This limitation must be considered when working in regions where multiple flaviviruses co-circulate. IgM detection is not useful for dengue serotype determination due to cross-reactivity of the antibody.
C) IgG ELISA
- The IgG ELISA used for the detection of a past dengue infection utilizes the same viral antigens as the MAC ELISA. This assay correlates with the hemagglutination assay (HI) previously used. In general IgG ELISA lacks specificity within the flavivirus serocomplex groups. Primary versus secondary dengue infection can be determined using a simple algorithm. Samples with a negative IgG in the acute phase and a positive IgG in the convalescent phase of the infection are primary dengue infections. Samples with a positive IgG in the acute phase and a 4 fold rise in IgG titer in the convalescent phase (with at least a 7 day interval between the two samples) is a secondary dengue infection.
D) NS1 ELISA
- The non-structural protein 1 (NS1) of the dengue viral genome has been shown to be useful as a tool for the diagnosis of acute dengue infections. Dengue NS1 antigen has been detected in the serum of DENV infected patients as early as 1 day post onset of symptoms (DPO), and up to 18 DPO. The NS1 ELISA based antigen assay is commercially available for DENV and many investigators have evaluated this assay for sensitivity and specificity. The NS1 assay may also be useful for differential diagnostics between flaviviruses because of the specificity of the assay.
E) Plaque Reduction and Neutralization Test (PRNT)
- Plaque Reduction and Neutralization Test (PRNT) and the microneutralization PRNT can be used when a serological specific diagnostic is required, as this assay is the most specific serological tool for the determination of dengue antibodies The PRNT test is used to determine the infecting serotype in convalescent sera. This assay measures the titer of the neutralizing antibodies in the serum of the infected individual and determines the level of protective antibodies this individual has towards the infecting virus. The assay is a biological assay based on the principle of interaction of virus and antibody resulting in inactivation of virus such that it is no longer able to infect and replicate in cell culture. Some of the variability of this assay is differences in interpretation of the results because of the cell lines and virus seeds used as well as the dilution of the sera.
The microneutralization assay is based on the same principle however instead of counting the number of plaques per well the assay uses a colorimetric measurement of the virus induced cell lysis to determine the end-point dilution. This assay was developed to utilize less reagents and for high throughput purposes for larger number of samples for testing.
Immunological Response to Dengue Infection
Dengue can be diagnosed by isolation of the virus, by serological tests, or by molecular methods. Diagnosis of acute (on-going) or recent dengue infection can be established by testing serum samples during the first 5 days of symptoms and/or early convalescent phase (more than 5 days of symptoms). Acute infection with dengue virus is confirmed when the virus is isolated from serum or autopsy tissue specimens, or the specific dengue virus genome is identified by reverse transcription-polymerase chain reaction (RT–PCR) from serum or plasma, cerebrospinal fluid, or autopsy tissue specimens during an acute febrile illness. Methods such as one-step, real time RT–PCR or nested RT–PCR are now widely used to detect dengue viral genes in acute-phase serum samples. This detection coincides with the viremia and the febrile phase of illness onset. Acute infections can also be laboratory confirmed by identification of dengue viral antigen or RNA in autopsy tissue specimens by immunofluorescence or immunohistochemical analysis, or by seroconversion from negative to positive IgM antibody to dengue or demonstration of a fourfold or greater increase in IgG antibody titers in paired (acute and convalescent) serum specimens.
The acquired immune response following a dengue infection consists of the production of IgM and IgG antibodies primarily directed against the virus envelope proteins. The immune response varies depending on whether the individual has a primary (first dengue or other flavivirus infection) versus a secondary (had dengue or other flavivirus infection in past) dengue infection. In general, diagnosis of dengue is dependent on the phase of the infection. The general timeline of a primary infection from virus isolation or identification, to IgM detection followed by IgG detection is as follows:
Figure 6. Primary Dengue Virus Infection
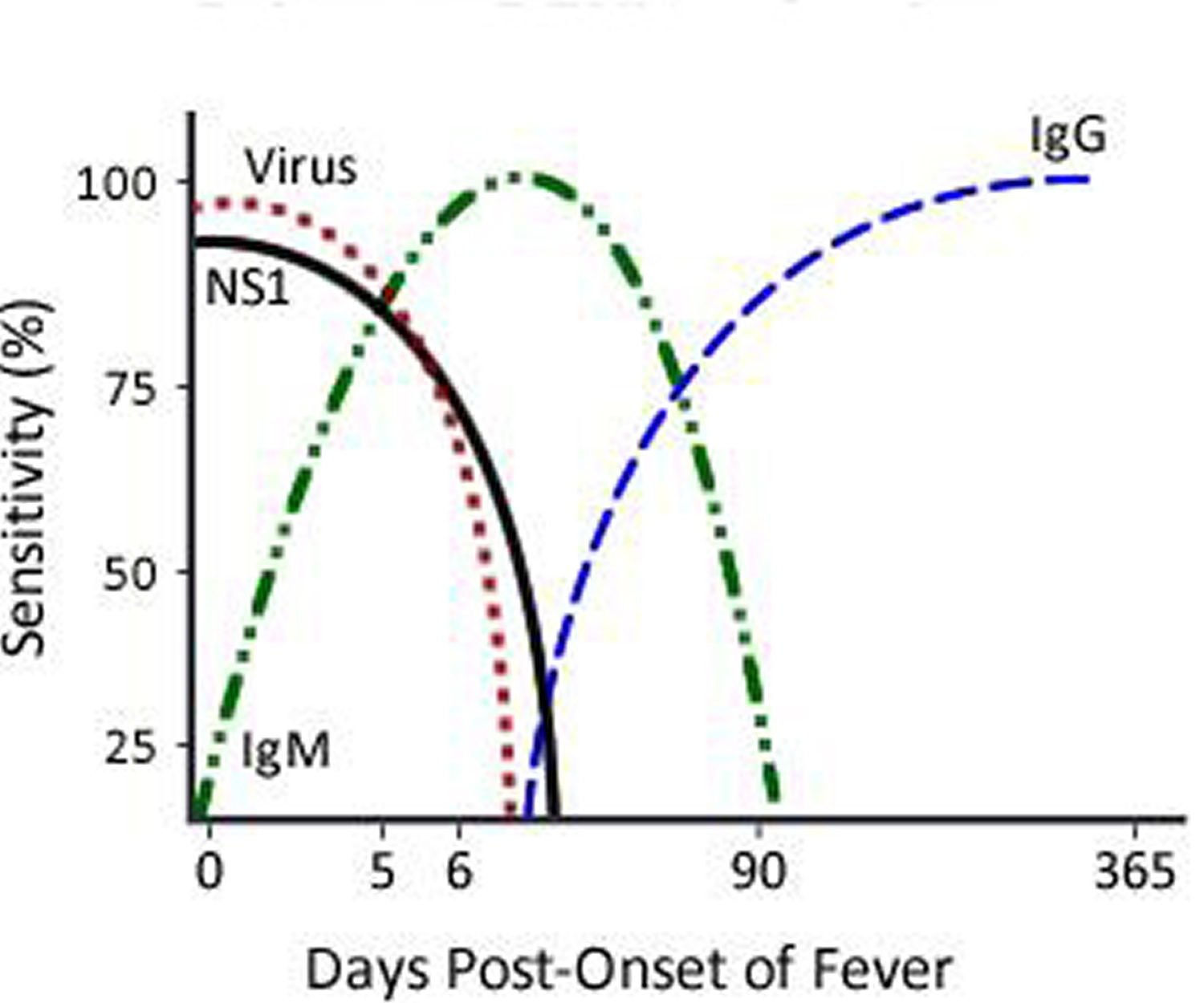 Footnotes: Dengue viral protein, NS1; Dengue Virus-reactive IgG; Dengue Virus-reactive IgM
Footnotes: Dengue viral protein, NS1; Dengue Virus-reactive IgG; Dengue Virus-reactive IgM
Figure 7. Secondary Dengue Virus Infection
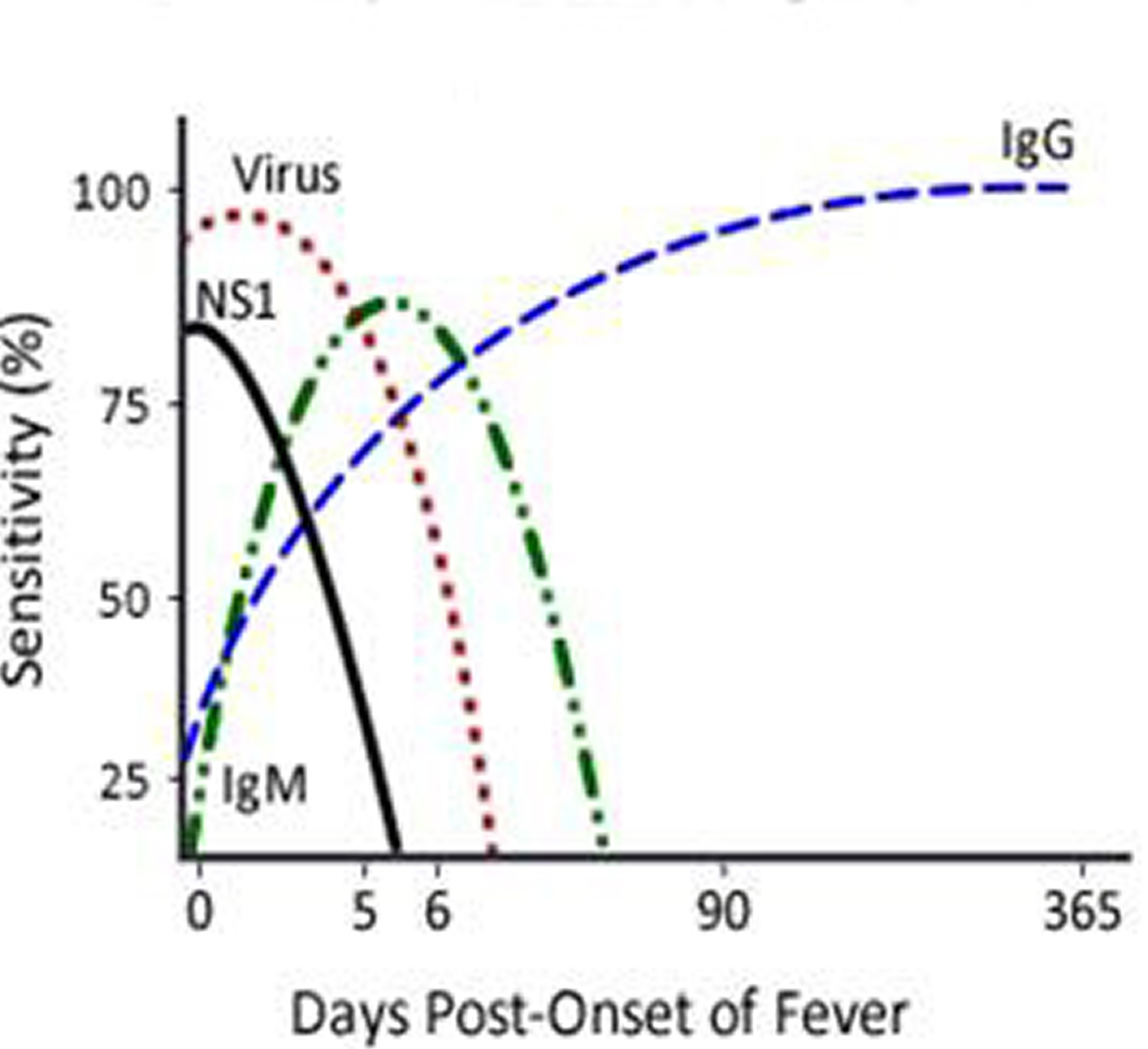 Footnotes: Dengue viral protein, NS1; Dengue Virus-reactive IgG; Dengue Virus-reactive IgM
Footnotes: Dengue viral protein, NS1; Dengue Virus-reactive IgG; Dengue Virus-reactive IgM
A primary dengue infection is characterized by a slow and low titer antibody response. IgM antibody is the first immunoglobulin isotype to appear. Anti-dengue IgG is detectable at low titer at the end of the first week of illness, and slowly increases. In contrast, during a secondary infection, antibody titers rise extremely rapidly and antibody reacts broadly with many flaviviruses. High levels of IgG are detectable even in the acute phase and they rise dramatically over the proceeding two weeks. The kinetics of the IgM response is more variable. IgM levels are significantly lower in secondary dengue infections and thus some anti-dengue IgM false-negative reactions are observed during secondary infections. According to the Pan American Health Organization (PAHO) guidelines 80% of all dengue cases have detectable IgM antibody by day five of illness, and 93-99% of cases have detectable IgM by day six to ten of illness, which may then remain detectable for over 90 days.
MAC-ELISA has become an important tool for routine dengue diagnosis, MAC-ELISA has a sensitivity and specificity of approximately 90% and 98%, respectively but only when used five or more days after onset of fever (i.e., in convalescent phase). Different formats such as capture ELISA, capture ultramicroELISA, dot-ELISA, AuBioDOT IgM capture and dipsticks have been developed. Serums, blood on filter paper, and saliva (but not urine) are useful for IgM detection if samples are taken in convalescent phase of illness (Vasquez et al., 2006). A variety of different commercial kits is available with variable sensitivity and specificity. Dengue diagnosis becomes even more challenging because dengue IgM antibodies also cross-react to some extent with other flaviviruses such asJEV, SLE, WNV and YFV.
Dengue fever treatment
There’s no cure or specific medication for treatment of a dengue infection. Treatment involves relieving your symptoms while the infection runs its course. Persons who think they have dengue should use analgesics (pain relievers) with acetaminophen and AVOID those containing ibuprofen, naproxen, aspirin or aspirin containing drugs. They should also rest, drink plenty of fluids to prevent dehydration, avoid mosquito bites while febrile and consult a physician.
You can usually look after yourself at home.
The following can help:
- take paracetamol to relieve pain and fever – avoid aspirin or ibuprofen, as these can cause bleeding problems in people with dengue
- drink plenty of fluids to prevent dehydration – if you’re currently abroad, only drink bottled water from properly sealed bottles
- get plenty of rest
You should start to feel better in around a week, although it may be a few weeks before you feel your normal self again. Get medical advice if your symptoms don’t improve.
As with dengue, there is no specific medication for Dengue hemorrhagic fever. If a clinical diagnosis is made early, a health care provider can effectively treat Dengue hemorrhagic fever using fluid replacement therapy. Adequate management of Dengue hemorrhagic fever generally requires hospitalization.
- Dengue Epidemiology. https://www.cdc.gov/dengue/epidemiology/index.html[↩][↩][↩][↩]
- Dengue vaccine: WHO position paper – July 2016 http://www.who.int/wer/2016/wer9130.pdf[↩][↩]
- Dengue Frequently Asked Questions. https://www.cdc.gov/dengue/faqfacts/index.html[↩]
- Messina JP, et al. Global spread of dengue virus types: mapping the 70 year history. Trends Microbiol. 2014;22(3):138–146.[↩]
- Guzman MG, et al. Dengue. Lancet. 2015;385(9966):453–465.[↩]
- Background Paper on Dengue Vaccines. World Health Organization, Geneva, Switzerland, 2016. Available at http://www.who.int/entity/immunization/sage/meetings/2016/april/1_Background_Paper_Dengue_Vaccines_2016_03_17.pdf[↩][↩]
- Villar L, et al. Efficacy of a tetravalent dengue vaccine in children in Latin America. N Engl J Med. 2015;372(2):113–123.[↩]
- Thomas EA, John M, Kanish B. MUCOCUTANEOUS MANIFESTATIONS OF DENGUE FEVER. Indian Journal of Dermatology. 2010;55(1):79-85. doi:10.4103/0019-5154.60359. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2856380/[↩]
- Hunsperger EA, et al. The Performance of Dengue Diagnostic Tests in a Single-Specimen Diagnostic Algorithm. J Infect Dis. 2016.[↩]
- Dengue Laboratory Guidance and Diagnostic Testing. https://www.cdc.gov/Dengue/clinicalLab/laboratory.html[↩]





{kind=link}