Contents
What is a dermoid cyst
A dermoid cyst is an overgrowth of normal, non-cancerous tissue in an abnormal location. Dermoid cysts can occur all over your body, such as within your skull, spine or abdominal cavity particularly the ovaries (ovarian dermoid cyst) or in your skin and may present at any time in people of all ages. The term dermoid cyst does not appear to be restricted to a single kind of lesion nor is it used in only a single medical discipline. The term dermoid cyst can be found in the vocabulary of dermatologists, dermatopathologists, general pathologists, gynecologists, neurosurgeons, or pediatricians. If asked, all of these clinicians would most probably define and describe dermoid cysts differently. For example, gynecologists and general pathologists might say that a dermoid cyst is a cystic tumor of the ovary. In contrast, neurosurgeons tend to view a dermoid cyst is associated with a congenital cyst of the spine or an intracranial congenital cyst. For pediatricians and dermatologists, dermoid cyst means subcutaneous cysts, which are usually congenital 1. In gynecology, the literature describes dermoid cysts as relatively rare tumors, a cystic teratoma that most often occurs in individuals aged 15-40 years. In neurosurgery, dermoid cysts are rare. In dermatology and pediatrics, dermoid cysts are relatively uncommon.
In all disciplines, however, the common factor is the presence of a solitary, or occasionally multiple, hamartomatous tumor 2. The tumor is covered by a thick dermis like wall that contains multiple sebaceous glands and almost all skin adnexa. Hairs and large amounts of fatty masses cover poorly to fully differentiated structures derived from the ectoderm.
Depending on the location of the lesion, dermoid cysts may contain substances such as nails and dental, cartilage-like, and bone-like structures. If limited to the skin or subcutaneous tissue, dermoid cysts are thin-walled tumors that contain different amounts of fatty masses; occasionally, they contain horny masses and hairs.
In the skin, dermoid cysts are made up of epidermal and dermal components: keratinocytes, hair follicles and hair, and sweat glands. Dermoid cyst of the skin appears in early childhood, with about 40% present at birth and most appearing by the age of 5 years. The cyst develops during skin tissue development in the embryonic stage. They occur on fusion lines. Skin dermoid cysts occur mostly on the face (outer eyebrow, eyelid, upper nose), neck, or scalp but they may occur anywhere in the body. Skin dermoid cyst is usually a solitary, firm, dough-like lump and ranges in size from 0.5–6 cm in diameter. It can be associated with a nearby pit and/or sinus tract to underlying tissues. Rarely, skin dermoid cysts can cause vision loss in the affected eye. There is a risk, however, that orbital dermoids can rupture and cause an inflammatory reaction. For this reason, ophthalmologist (eye doctor) will most often recommend that the skin dermoid cyst be removed.
Ovarian dermoid cyst is a solid ovarian cyst containing tissue such as skin, hair or even teeth instead of fluid. Dermoid cysts of the ovary are sex restricted, that is, they occur only in the female population. In other dermoid cysts, no sex predilection has been found. Ovarian dermoid cysts aren’t associated with infertility. Intra-abdominal dermoid cysts are described in females aged 15-40 years. For example, cystic teratoma is a relatively rare tumor that most often occurs in females aged 15-40 years.
Intracranial or perispinal dermoid cysts are most often found in infants, children, or young adolescents.
Most dermoid cysts on the floor of the mouth occur in individuals aged 10-30 years. There are few descriptions of oral dermoid cysts in newborns or children.
Dermoid cyst of the skin
Dermoid cysts can appear as cutaneous cysts on the head, as cysts on the floor of the mouth or elsewhere in the head, within the parotid gland 3 or as cysts in the testes or penis. Dermoid cysts of the skin can be quite large 4.
Specialists in various disciplines may consider dermoid cysts to be different entities.
Head and neck
Cutaneous cysts most commonly occur on the head (forehead), mainly around the eyes. They may be evident as a tadpole-shaped cyst on the eyebrow 5. Occasionally, they occur on the neck or in a midline region. When on the head, dermoid cysts are often adherent to the periosteum. The usual diameter of the lesions is 1-4 cm.
In one study, 25 benign tumors on the forehead and brow of children and adolescents were successfully removed by means of endoscopic excision. Of these, 6 were classified as dermoid cysts. Dermoid cysts on the forehead and brow are known to cause pressure-related erosion of the underlying bony tissue, and surgical intervention may be helpful.
In 191 children treated for congenital cysts and fistulas of the neck in 1984-1999, 21 dermoid cysts were found. Periauricular fistulas and cystic hygromas were not included in this study 6.
Occasionally, skin-related dermoid cysts are multiple and develop over periods as long as 20 years. In one unusual case, multiple subcutaneous dermoid cysts were present in the frontal region of a 41-year-old man, none with evident intracranial extension.
In many patients, dermoid cysts occur on the floor of the mouth or elsewhere in the mouth 7.
Because the term dermoid is frequently used in the literature, some authors believe that this term should be used for all congenital cysts on the floor of the mouth. Three subclasses of congenital mouth cysts are described in the literature: epidermoid (simple) cysts, dermoid (complex) cysts, and teratoid (complex) cysts. Most of these lesions occur in individuals aged 10-30 years. Only a few cases describe dermoid cysts of the mouth in newborns or children.
An unusual case of a carcinomatous transformation of a long-standing sublingual dermoid cyst has been described 8.
Other rare dermoid cysts in the oral cavity are those on the tongue 9. As of early 2000, 17 patients with intralingual dermoid cysts are described in the English-language literature. All cases occurred in young patients. Magnetic resonance imaging (MRI) was helpful in establishing the differential diagnosis. Surgical excision corrected deglutition and speech problems in all of these patients.
Dermoid cysts in the eustachian tube are rare 10. Only 12 patients have been described. In most cases reviewed, cysts affected female patients on the left side. MRI was useful in establishing the correct diagnosis and in selecting the surgical approach.
Reports of nasal dermoid cysts were recently published. Of 36 children with nasal dermoid sinus cysts that were treated from 1974-1994, 10 had only a midline cyst, 8 had only nasal pits, and 18 had combined cysts. Meningeal adherences have been found in only 2 patients 11. Nasal dermoid cysts may be evident as a midline nasal pit, fistula, or infected mass from the glabella to nasal columella, sometimes as a midline nasal punctum at birth 12.
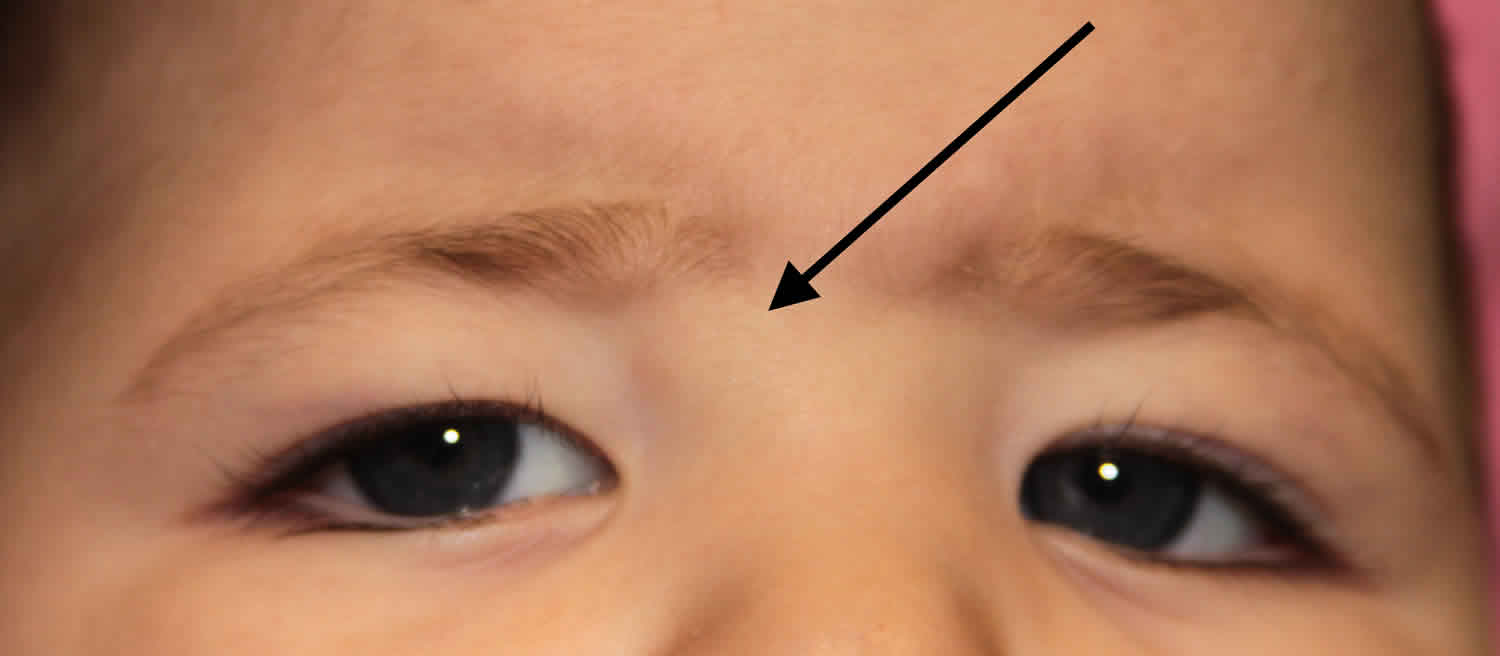
Figure 1. Dermoid cyst eye

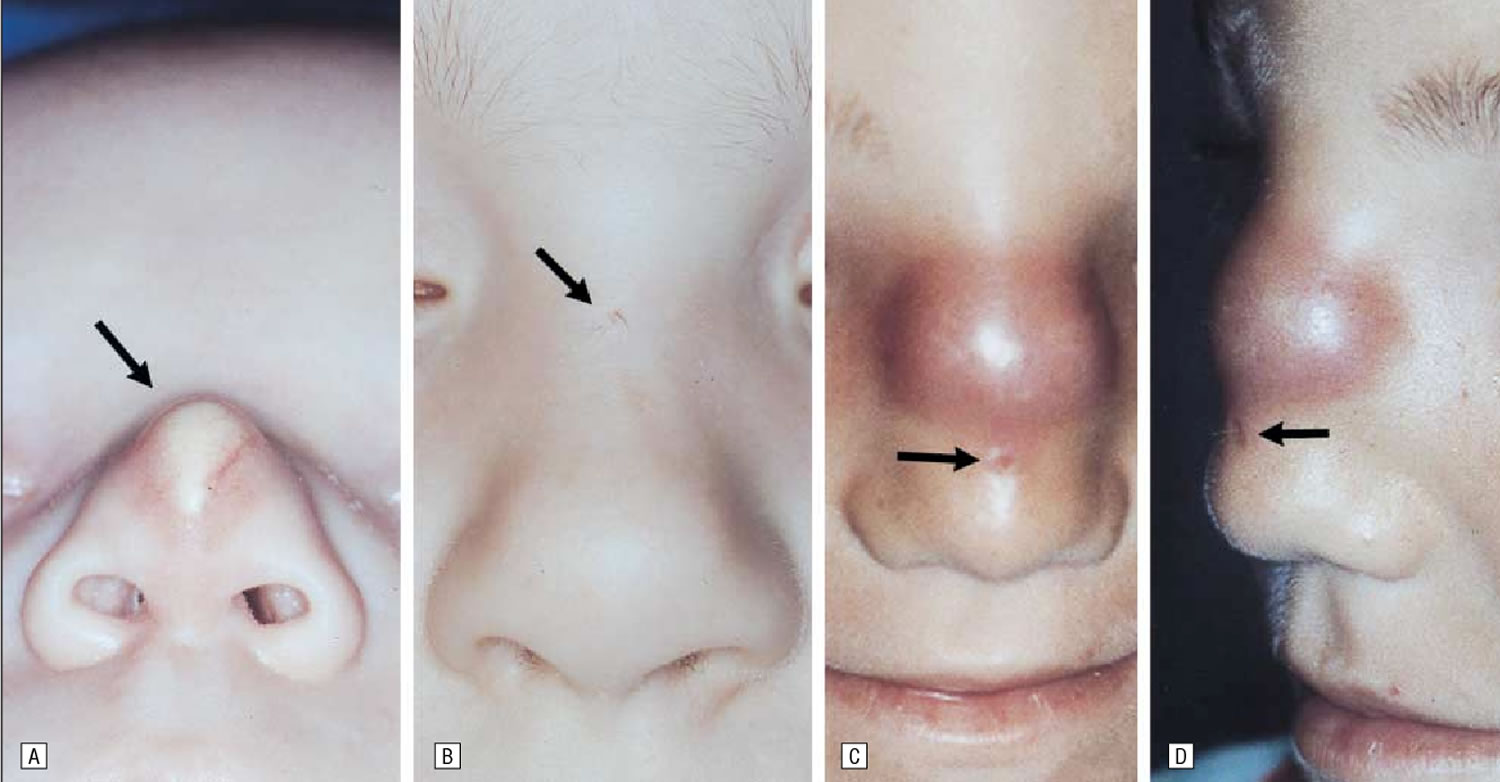
Figure 2. Nasal dermoid cyst
Testes or penis
Dermoid cysts can occur in the testes or penis.
In a review of cystic testicular lesions in the pediatric population, dermoid cysts were noted 13. Other diagnoses for these cysts include epidermoid cyst, prepubertal teratoma, juvenile granulosa cell tumor, cystic dysplasia of the rete testis, testicular cystic lymphangioma, simple cyst, and cystic degeneration after torsion. An understanding of potentially cystic testicular lesions in children leads to the best treatment choices and often to the preservation of a substantial portion of the affected testis.
Dermoid cysts in the penis are extremely rare. Tomasini et al 14 described the first in 1997. The patient was a young white male who had significant penile swelling for several months.
Spine and cranium
For neurosurgeons, dermoid cysts are associated with congenital cysts of the spine or intracranial cysts.
Several cases involve ruptured cysts and generalized subarachnoid and ventricular spread of the contents (mostly fatty masses) 15.
In some patients, spinal dermoid cysts, especially those connected to dermal sinus tract, lead to severe neurologic complications such as secondary spinal subdural abscesses caused by the spread of the infection in the dermoid cyst. Bilateral orbital abscesses were described as a result of an infected nasal dermoid cyst 16.
Dermoid cyst ovary
For gynecologists and general pathologists a dermoid cyst is primarily associated with a cystic tumor of the female ovary.
Cystic teratoma is a relatively rare tumor that most often occurs in females aged 15-40 years. A cystic teratoma consists of a thick leather-like capsule that covers amorphous fatty masses and poorly to fully differentiated structures derived from the ectoderm. Most ovarian dermoid cysts contain skin and skin adnexa, including prominent sebaceous glands, hairs, and nails, but also teeth or eyes. Melanotic changes may also occur. Rare cases of multiple dermoid cysts of the omentum have been reported 17. Dermoid cysts of the ovary are usually benign and easy to remove.
Malignant melanomas may originate from melanocytes in ovarian cystic teratomas. Two new cases and 17 older cases in the literature (reported from 1903-1995) are described and were critically reviewed. The present authors found 17 additional cases of benign and malignant melanotic ovarian lesions that were not associated with a dermoid cyst, including 4 melanomas, 3 benign nevi, 5 benign melanosis, and 4 benign and malignant retinal anlage tumors. The extremely rare primary ovarian melanoma was differentiated from the more common melanoma metastatic cyst of the ovary by its unilaterality, the presence of junctional change, and detailed history taking and physical examination, the findings of which excluded other primary sites 18.
Three patients with metastasizing squamous cell carcinoma from a dermoid cyst of the ovary are described 19. Malignant transformation in a dermoid cyst is a rare complication and mainly occurs in older individuals. Although the prognosis is poor, aggressive therapy may result in long-term remission.
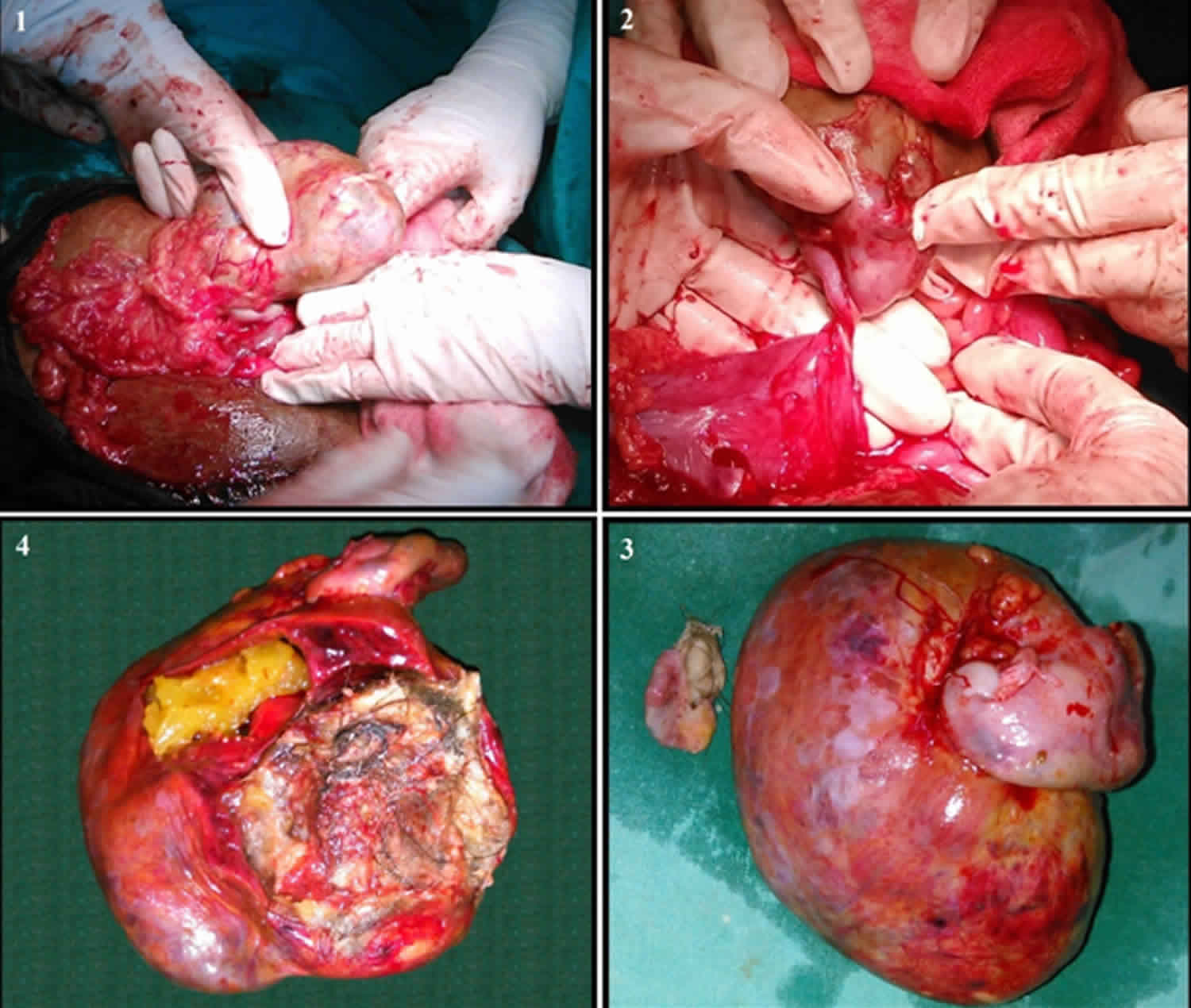
Figure 3. Ovarian dermoid cyst
Dermoid cyst causes
Dermoid cysts are true hamartomas or benign (not cancer) growths made up of an abnormal mixture of cells and tissues normally found in the area of the body where the growth occurs. Dermoid cysts occur when skin and skin structures become trapped during fetal development.
Histogenetically, dermoid cysts are a result of the sequestration of the skin along the lines of embryonic closure. If connected with the ovary, dermoid cysts are true teratomas. Scalp cysts may be evaluated using fine-needle aspiration cytology 20.
In contrast to epidermal inclusion cysts, dermoid cysts in the skin are lined by an epidermis that possesses various epidermal appendages. As a rule, these appendages are fully mature. Hair follicles containing hairs that project into the lumen of the cyst are often present. The dermis of dermoid cysts usually contains sebaceous glands, eccrine glands, and, in many patients, apocrine glands. Occasionally, the lining epithelium may proliferate as papillary boundaries extend externally or inward toward the lumen of the cyst. This proliferation may have some superficial resemblance to epidermal carcinomatous proliferation, and the growth may be misclassified as a cancer.
Dermoid cysts in the ovary (cystic teratomas) or those disseminated intra-abdominally may contain other structures such as nails, hairs, or cartilage and bone fragments. These cysts have cell walls that are almost identical to those of the skin, and they may contain multiple adnexal skin structures such as hair follicles, sweat glands, and occasionally, hair, teeth, or nerves.
A congenital dermoid together with a bronchogenic cyst of the tongue is extremely rare but has been described in a few patients 21.
Dermoid cyst symptoms
Dermoid cysts that are congenital and localized on the neck, head, or trunk are usually visible at birth. In some instances, careful medical examination may be necessary to identify a dermoid cyst. A tuft of hairs emanating from a midline nasal depression or nodule may represent a nasal dermoid cyst 22. Unilateral upper eyelid swelling may be the first sign, with imaging studies demonstrating a soft tissue orbital dermoid cyst arising from the lacrimal gland 14. An eyelid dermoid cyst attached to a tarsus may be evident as a firmly adherent nontender upper-eyelid nodule 23. A dermoid cyst of the lower lid may be evident as a painless, gradually enlarging swelling of the lower eyelid 24. Dermoid tumors in the medial canthal area may present as masses adherent to the lacrimal canaliculi 25. Rarely, a dermoid cyst evident during the newborn period clinically appears, only to become evident years later with full-thickness bone erosion and transcranial extension 26.
Intracranial, intraspinal, or intra-abdominal dermoid cysts may be suspected after specific or nonspecific neurologic or gynecologic symptoms occur. In these instances, imaging studies may help in distinguishing dermoid cysts from other tumors or organ malformations. A congenital intracranial frontotemporal dermoid cyst may be first evident as a cutaneous fistula, although intracranial extension and cutaneous sinus tract formation are rarely seen with these dermoid cysts 27.
Dermoid cyst complications
Several possible complications of spontaneous or posttraumatic rupture and surgical procedures have been described. In patients with a ruptured spinal dermoid cyst, fatty droplets can disseminate in the cerebrospinal fluid or in a dilated central canal of the spinal cord. In other patients, subarachnoid and ventricular fat dissemination can occur after the cerebellopontine angle dermoid cyst is resected. Spinal subdural abscesses are a possible complication because of the bacterial infection of spinal dermoid cysts in a dermal sinus tract. A ruptured intracranial dermoid cyst be an incidental finding on an MRI performed for other purposes or because of a persistent headache 28.
Pay special attention to intralingual dermoid cysts because deglutition and speech problems may occur.
Nasal dermoid cysts in a nasal tip location are rare, but they may produce social and psychologic problems in children 29.
Malignant transformation is an unusual complication that may occur in patients with long-standing dermoid cysts. Carcinomatous transformation to a squamous cell carcinoma is described in sublingual and intra-abdominal dermoid cysts, most often dermoid cysts of the ovary. Metastatic malignant melanomas arising from dermoid cysts have been reported in the literature.
Dermoid cyst treatment
A dermoid cyst is usually removed by surgical excision. Surgically remove dermoid cysts. The average age at the time of surgery can vary widely; in one retrospective study of 159 patients, it ranged from age 1 month to 63 years 30.
In some patients, surgery should be performed even more carefully than usual because the fatty content of the cyst may spread to the surrounding tissues or anatomic structures, especially if the cyst is infected with bacteria. The spread of these contents can cause foreign body reactions and severe complications.
Minimally invasive surgical techniques have been successful in removing dermoid cysts from difficult locations, such as those on the tongue or the floor of the mouth. Intralingual dermoid cysts lead to lingual motility defects and speech problems. These cysts should be surgically removed to restore normal lingual function and to correct speech problems.
Intracranial, intramedullary, and ovarian dermoid cysts are difficult to treat. Sophisticated neurosurgical or gynecologic surgical techniques are often needed to remove the dermoid cyst and prevent possible complications. High-definition fiber tracking guidance may be beneficial in the resection of an intraparenchymal dermoid cyst by means of a minimally invasive endoscopic port 31.
In some patients with dermoid cysts on the forehead and brow, successful excision with endoscopy-assisted surgery have been described 32. In the reported cases, no complications (eg, paresthesia or numbness on the scalp) occurred. The absence of visible scarring is an additional advantage of endoscopy-assisted surgery.
Angular dermoid cyst excision using an eyelid crease approach may yield excellent cosmesis 33. External angular dermoid cysts can be excised using a minimally invasive subcutaneoscopic technique that involves placing incisions above the hairline to avoid scarring on the face 34.
Frontozygomatic removal through a blepharoplasty incision has been advocated for frontozygomatic dermoid cysts 35.
Dermoid cyst prognosis
If dermoid cysts are diagnosed early and treated with complete surgical excision, the prognosis is good, and no further complications are expected.
In patients with cancerous transformation, the prognosis depends on the stage of the malignant disease (locally limited or spreading) and the success of therapy.
Although dermoid cysts are located in connection with the spinal channel (as described in neurosurgery literature), no deaths are directly linked to ruptures of the cyst or to the spreading of fatty and occasionally, infected masses in subarachnoid, ventricular, or subdural compartments. However, rupture or spread can lead to severe neurologic complications such as secondary spinal subdural abscesses.
- Yan J, Li Y, Chen Q, Ye X, Li J. Rare orbital cystic lesions in children. J Craniomaxillofac Surg. 2015 Mar. 43(2):238-43.[↩]
- Dermoid Cyst. https://emedicine.medscape.com/article/1112963-overview[↩]
- Tas A, Yagiz R, Altaner S, Karasalihoglu AR. Dermoid cyst of the parotid gland: first pediatric case. Int J Pediatr Otorhinolaryngol. 2010 Feb. 74(2):216-7.[↩]
- Kahraman A, Kahveci R. A giant dermoid cyst. Dermatol Surg. 2008 Sep. 34(9):1273-5.[↩]
- Choi HJ, Kim SH, Lee JH. Unusual Presenting Tadpole-Shaped Dermoid Cyst on Eyebrow. J Craniofac Surg. 2016 May. 27 (3):e281-2.[↩]
- Nicollas R, Guelfucci B, Roman S, Triglia JM. Congenital cysts and fistulas of the neck. Int J Pediatr Otorhinolaryngol. 2000 Sep 29. 55(2):117-24.[↩]
- Vargas Fernandez JL, Lorenzo Rojas J, Aneiros Fernandez J, Sainz Quevedo M. [Dermoid cyst of the floor of the mouth]. Acta Otorrinolaringol Esp. 2007 Jan. 58(1):31-3.[↩]
- Devine JC, Jones DC. Carcinomatous transformation of a sublingual dermoid cyst. A case report. Int J Oral Maxillofac Surg. 2000 Apr. 29(2):126-7.[↩]
- Myssiorek D, Lee J, Wasserman P, Lustrin E. Intralingual dermoid cysts: a report of two new cases. Ear Nose Throat J. 2000 May. 79(5):380-3.[↩]
- Sichel JY, Dano I, Halperin D, Chisin R. Dermoid cyst of the eustachian tube. Int J Pediatr Otorhinolaryngol. 1999 Apr 25. 48(1):77-81.[↩]
- Carroll CM, Gaffney R, McShane D. Congenital nasal dermoids in children. Ir J Med Sci. 1997 Jul-Sep. 166(3):149-51.[↩]
- Min HJ, Hong SC, Kim KS. The Usefulness of Three-Dimensional Reconstruction Computed Tomography in the Nasal Dermoid Cyst. J Craniofac Surg. 2016 May. 27 (3):819-20.[↩]
- Garrett JE, Cartwright PC, Snow BW, Coffin CM. Cystic testicular lesions in the pediatric population. J Urol. 2000 Mar. 163(3):928-36.[↩]
- Kiratli H, Bilgic S, Sahin A, Tezel GG. Dermoid cyst of the lacrimal gland. Orbit. 2005 Jun. 24(2):145-8.[↩][↩]
- Calabrò F, Capellini C, Jinkins JR. Rupture of spinal dermoid tumors with spread of fatty droplets in the cerebrospinal fluid pathways. Neuroradiology. 2000 Aug. 42(8):572-9.[↩]
- Carvalho GA, Cervio A, Matthies C, Samii M. Subarachnoid fat dissemination after resection of a cerebellopontine angle dysontogenic cyst: case report and review of the literature. Neurosurgery. 2000 Sep. 47(3):760-3; discussion 763-4.[↩]
- Mazumdar A, Vaiphei K, Verma GR. Multiple dermoid cysts of omentum. J Postgrad Med. 1997 Apr-Jun. 43(2):41-2.[↩]
- Davis GL. Malignant melanoma arising in mature ovarian cystic teratoma (dermoid cyst). Report of two cases and literature analysis. Int J Gynecol Pathol. 1996 Oct. 15(4):356-62.[↩]
- Ayhan A, Tuncer ZS, Bilgin F, Kucukali T. Squamous cell carcinoma arising in dermoid cyst. Eur J Gynaecol Oncol. 1996. 17(2):144-7.[↩]
- Sharma P, Pathak P, Goyal A, Sharma S. Cytomorphological spectrum of scalp lesions in the population of a developing country: A retrospective study. Diagn Cytopathol. 2019 Feb 13.[↩]
- Gleizal A, Abouchebel N, Lebreton F, Beziat JL. Dermoid cyst of the tongue: an association of dermoid cyst with bronchogenic epithelium. J Craniomaxillofac Surg. 2006 Mar. 34(2):113-6.[↩]
- Madke B, Nayak C, Giri A, Jain M. Nasal dermoid sinus cyst in a young female. Indian Dermatol Online J. 2013 Oct. 4(4):380-1.[↩]
- Koreen IV, Kahana A, Gausas RE, Potter HD, Lemke BN, Elner VM. Tarsal dermoid cyst: clinical presentation and treatment. Ophthal Plast Reconstr Surg. 2009 Mar-Apr. 25(2):146-7.[↩]
- Gonsalves SR, Lobo GJ, Mendonca N. Dermoid cyst: an unusual location. BMJ Case Rep. 2013 Nov 8. 2013[↩]
- Kim NJ, Choung HK, Khwarg SI. Management of dermoid tumor in the medial canthal area. Korean J Ophthalmol. 2009 Sep. 23(3):204-6.[↩]
- Maurice SM, Burstein FD. Disappearing dermoid: fact or fiction?. J Craniofac Surg. 2012 Jan. 23(1):e31-3.[↩]
- Scolozzi P, Lombardi T, Jaques B. Congenital intracranial frontotemporal dermoid cyst presenting as a cutaneous fistula. Head Neck. 2005 May. 27(5):429-32.[↩]
- Jacquin A, Bejot Y, Hervieu M, et al. [Rupture of intracranial dermoid cyst with disseminated lipid droplets.]. Rev Neurol (Paris). 2009 Oct 19.[↩]
- Tatlidede S, Egemen O, Ozkaya O, Erol O. Witch nose: an embarassing metaphor for nasal tip dermoid cysts. J Craniofac Surg. 2011 Sep. 22(5):1948-51.[↩]
- Khalid S, Ruge J. Considerations in the management of congenital cranial dermoid cysts. J Neurosurg Pediatr. 2017 Apr 21. 1-5.[↩]
- Fernandez-Miranda JC, Engh JA, Pathak SK, et al. High-definition fiber tracking guidance for intraparenchymal endoscopic port surgery. J Neurosurg. 2009 Nov 27.[↩]
- Lin SD, Lee SS, Chang KP, Lin TM, Lu DK, Tsai CC. Endoscopic excision of benign tumors in the forehead and brow. Ann Plast Surg. 2001 Jan. 46(1):1-4.[↩]
- Cozzi DA, Mele E, d’Ambrosio G, Totonelli G, Frediani S, Spagnol L. The eyelid crease approach to angular dermoid cysts in pediatric general surgery. J Pediatr Surg. 2008 Aug. 43(8):1502-6.[↩]
- Agrawal V, Acharya H, Agarwal P, Sekhon V, Sharma D. Subcutaneoscopic excision of external angular dermoid cyst in children without conspicuous scarring. Asian J Endosc Surg. 2013 Aug. 6(3):241-4.[↩]
- Nelson KE, Mishra A, Duncan C. Upper blepharoplasty approach to frontozygomatic dermoid cysts. J Craniofac Surg. 2011 Nov. 22(6):e41-4.[↩]





{kind=link}