Contents
What is diastasis recti
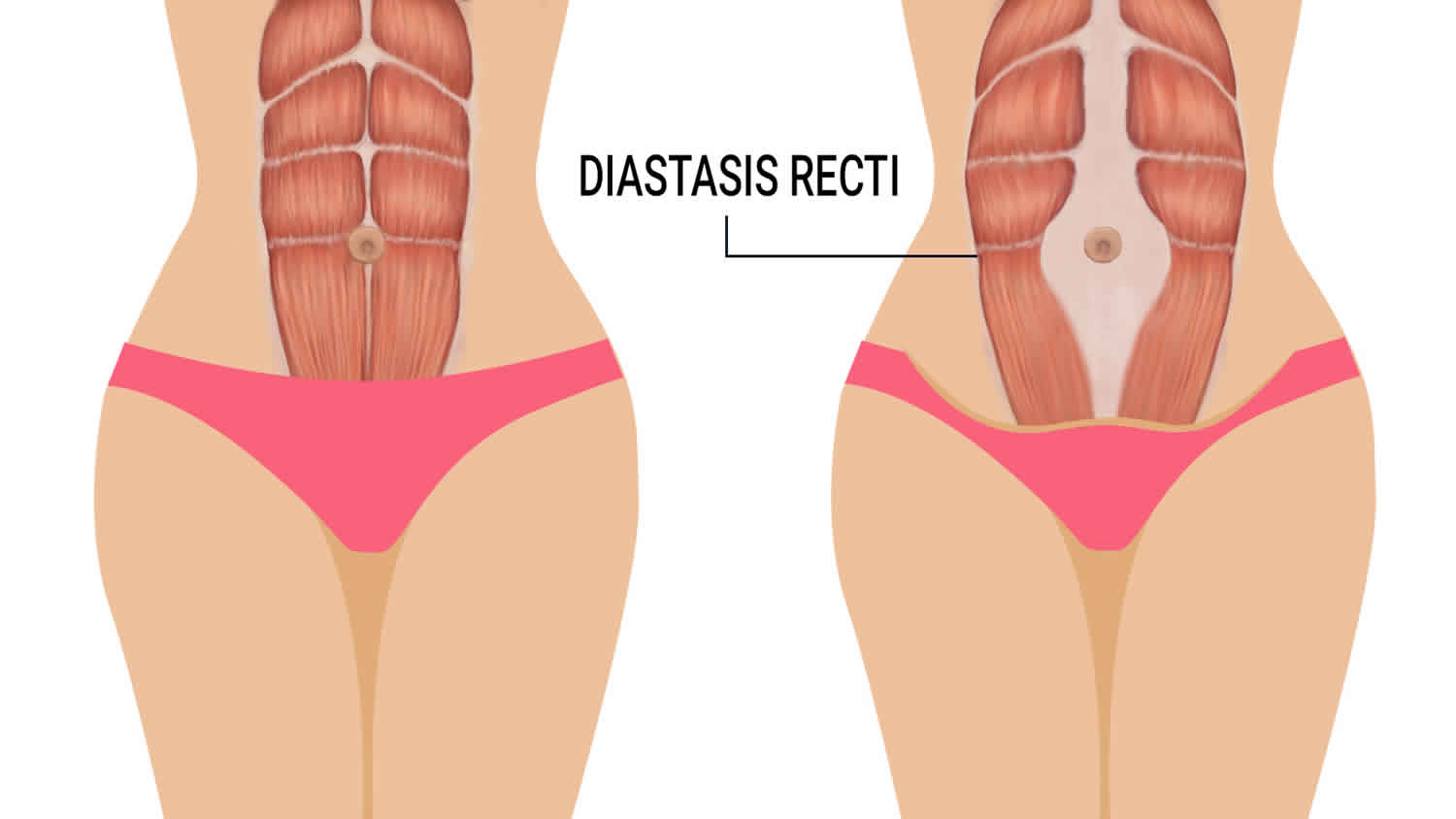
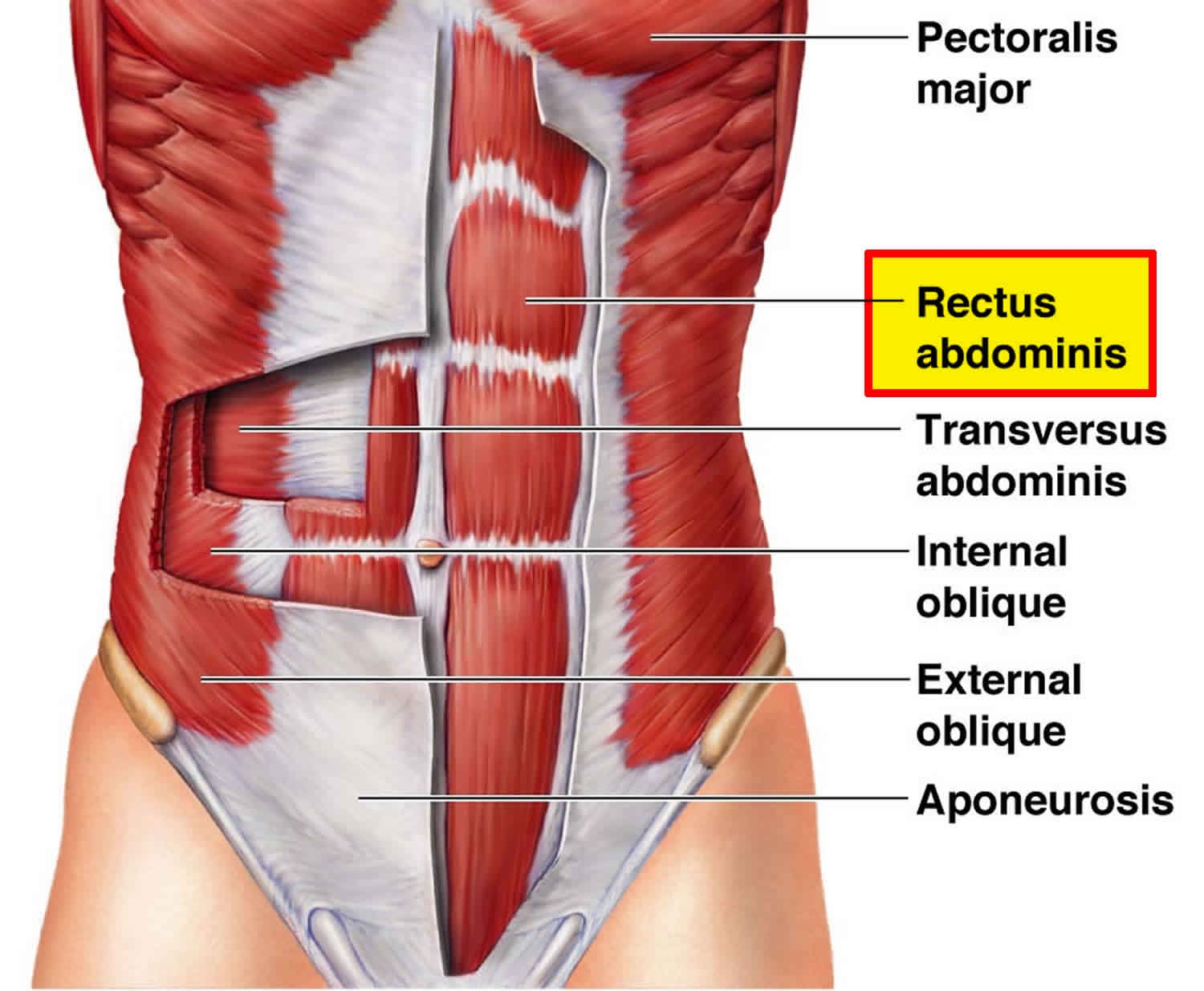
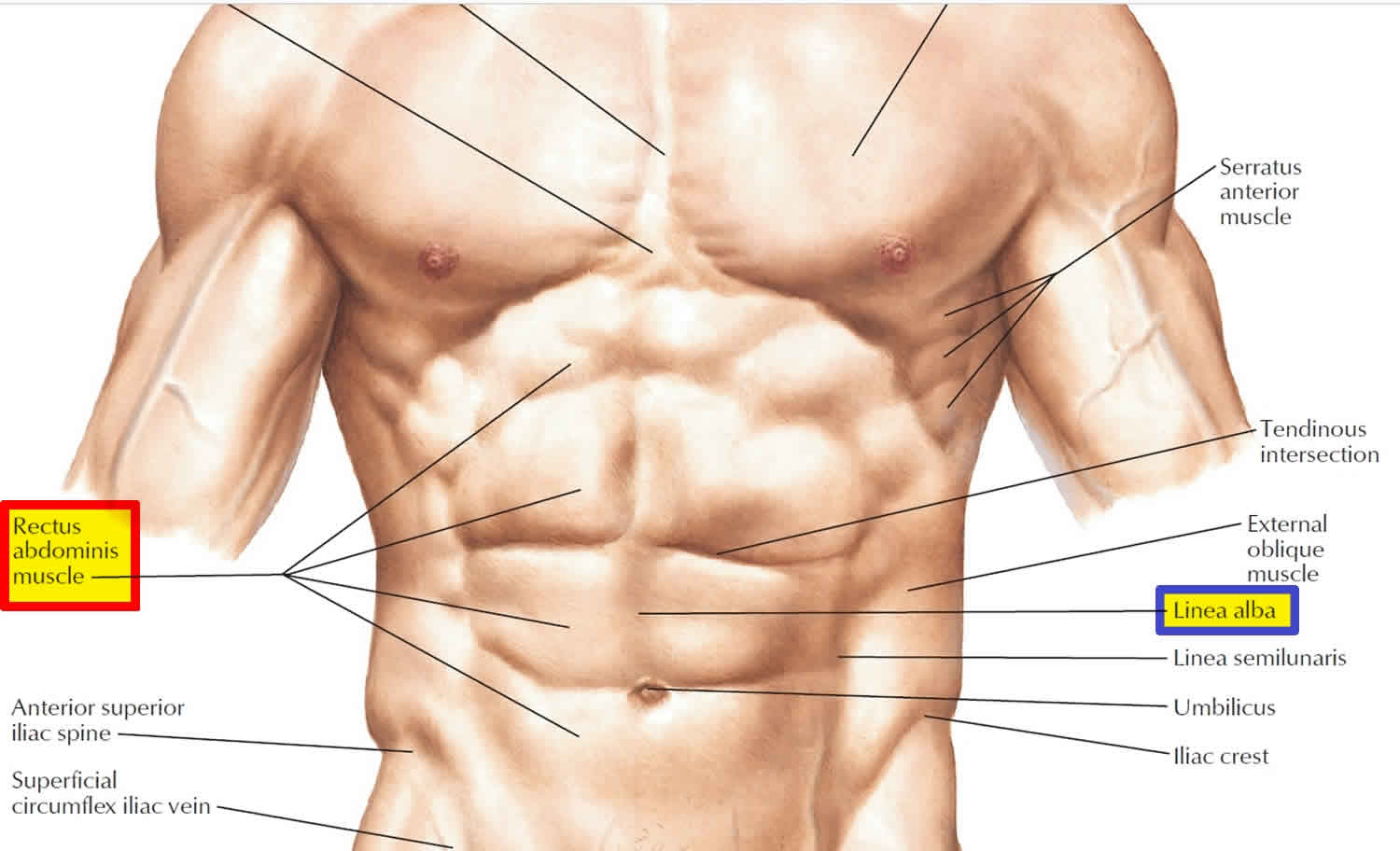
Diastasis recti also known as abdominal muscle separation or divarication, is a separation between the left and right side of the rectus abdominis muscle along the linea alba 1. The rectus abdominis muscle covers the front surface of your belly area. Some women find their stomach muscles weaken and separate during and after pregnancy.
During pregnancy, the growing uterus stretches the muscles in the abdomen. This can cause the two large parallel bands of muscles that meet in the middle of the abdomen (rectus abdominis muscles) to become separated by an abnormal distance — a condition called diastasis recti abdominis.
Diastasis recti might cause a bulge in the middle of your abdomen where the two muscles separate. Diastasis recti might be noticeable only when the abdominal muscles are tense, such as when you move from lying down to sitting up. Diastasis recti can weaken the abdominal muscles, causing lower back pain and making it difficult to lift objects or do other routine daily activities.
You might be more likely to develop diastasis recti as a result of pregnancy if you have carried multiples or a large baby to term and are of small stature and fit or are age 35 or older.
The amount of separation varies from one woman to another. Diastasis recti happens because your growing womb (uterus) pushes the muscles apart, making them longer and weaker.
Most women don’t notice any problems as their stomach muscles separate in pregnancy. But you might notice a bulge developing down the front of your bump, above and below your belly button.
After you have had your baby, you can check the size of the diastasis recti separation with this simple technique:
- Lie on your back with your legs bent and your feet flat on the floor.
- Raise your shoulders off the floor slightly and look down at your tummy. Using the tips of your fingers, feel between the edges of the muscles, above and below your belly button. See how many fingers you can fit into the gap between your muscles.
- Do this regularly to check that the gap is gradually decreasing.
The separation between your stomach muscles will usually go back to normal by the time your baby is eight weeks old. If the gap is still obvious at eight weeks, the muscles may still be long and weak. This can put you at risk of back problems.
If you think you have diastasis recti, talk to your health care provider. Your doctor can refer you to a physiotherapist, who will give you some specific exercises to do.
Regular pelvic floor and deep stomach muscle exercises can help to reduce the size of the separation between your stomach muscles. It’s also important to stand up tall and be aware of your posture now you’re no longer pregnant.
If abdominal muscle weakness associated with diastasis recti is interfering with your daily activities, surgery might be recommended to repair the muscle separation. If you’re bothered by the bulge in your abdomen, you might also consider surgery for cosmetic reasons.
Figure 1. Rectus abdominis muscles
Does diastasis recti go away by itself?
Diastasis recti usually goes away after the birth of the baby in about 8 weeks. That said, up to 1 in 3 women still report problems with diastasis recti abdominis 12 months after the birth of their baby.
What causes diastasis recti?
Pregnant women may develop the condition because of increased tension on the abdominal wall. Diastasis recti is more common in women who have had more than one child, are aged over 35 or who are having twins or triplets (or more). Diastasis recti can also occur in a small-statured woman who is having a larger-than-average baby. To date, there is no consensus about risk factors for development of diastasis recti during pregnancy and in the postpartum period 1. Older age, multiparity, caesarean section, gestational weight gain, high birth weight, multiple pregnancy, and child care have been proposed 2. There is also scant knowledge on the consequences of diastasis recti 3. It has been hypothesized that diastasis recti, in addition to being a cosmetic concern for many women, may reduce low back and pelvic stability, cause low back and pelvic girdle pain, and be related to pelvic floor dysfunctions such as urinary incontinence, anal incontinence, and pelvic organ prolapse 4.
Diastasis recti is also common in newborns. It is seen most often in premature and African American infants.
Diastasis recti prevention during pregnancy
Strengthening your core muscles before you get pregnant or in the early stages of pregnancy might help prevent diastasis recti.
It’s best to avoid putting excess strain on your abdominal muscles while pregnant. Avoid sit-ups or planks. Try to avoid constipation and if you have a cough, get it treated.
Diastasis recti symptoms
A diastasis recti looks like a ridge, which runs down the middle of the belly area. It stretches from the bottom of the breastbone to the belly button. It increases with muscle straining. If you have diastasis recti after the birth of your baby, you may be able to see a gap between the two bands of abdominal muscles. You can see this gap more clearly if you lie flat on your back and lift your head up. You might also notice a physical bulge in the middle of your stomach, especially when your abdominal muscles are active. Some women with diastasis recti also get lower back pain, as the separation prevents the stomach muscles from supporting the back.
Diastasis recti is commonly seen in women who have multiple pregnancies. This is because the muscles have been stretched many times. Extra skin and soft tissue in the front of the abdominal wall may be the only signs of this condition in early pregnancy. In the later part of pregnancy, the top of the pregnant uterus can be seen bulging out of the abdominal wall. An outline of parts of the unborn baby may be seen in some severe cases.
In infants, diastasis recti is most easily seen when the baby tries to sit up. When the infant is relaxed, you can often feel the edges of the rectus muscles.
Diastasis recti test
After you have had your baby, you can check the size of the diastasis recti separation with this simple technique:
- Lie on your back with your legs bent and your feet flat on the floor.
- Raise your shoulders off the floor slightly and look down at your tummy. Using the tips of your fingers, feel between the edges of the muscles, above and below your belly button. See how many fingers you can fit into the gap between your muscles.
- Do this regularly to check that the gap is gradually decreasing.
How is diastasis recti diagnosed?
Your doctor, midwife or physiotherapist can check how big your diastasis recti is by measuring it with their fingers or a measuring tape, or by doing an ultrasound.
Diastasis recti treatment
It’s important to stop the separation from getting worse. Try these tips:
- Avoid lifting anything heavier than your baby.
- Roll onto your side when getting out of bed or sitting up.
- Choose gentle exercises (rather than intense ones) that strengthen the deeper stomach muscles.
- Skip activities and movements that can make abdominal separation worse, such as sit-ups (crunches), oblique curls and some yoga poses (ask your yoga teacher for advice).
You can also wear a supportive brace or compression underwear to help support your back and resolve the muscle separation.
There is a good chance that with time and care, the rectus abdominis muscles will come back together. If that doesn’t work as well as you’d like, surgery after you’ve had your baby is an option.
Surgery often involves using stitches to repair the abdominal wall and reduce the gap between the rectus abdominis muscles. This can improve quality of life and muscle strength, especially when separation is wider than 3 cm.
Diastasis recti exercises
Deep stomach exercises can help you tone up your stomach muscles:
- Lie on your side with your knees slightly bent
- Let your tummy relax and breathe in gently
- As you breathe out, gently draw in the lower part of your stomach like a corset, narrowing your waistline
- Squeeze your pelvic floor muscles at the same time
- Hold for a count of 10, breathing normally, then gently release
- Repeat up to 10 times
Diastasis recti surgery
There is no consensus on the surgical technique or indications for the treatment of diastasis recti 5. Different options have been proposed such as conventional surgery, with abdominoplasty or laparoscopic approach. The most common surgical technique used is by the way of an abdominoplasty in patients with excess abdominal skin and subcutaneous cellular tissue 6. However, a mini-invasive approach presents as an alternative procedure to the most commonly used surgical technique for diastasis recti treatment. For this endoscopic approach, the patient is positioned in supine position with both legs open and the surgeon is located between them. A 10 mm incision is made in the suprapubic midline and a space is created between the subcutaneous cellular tissue and the superficial aponeurosis with blunt dissection. A 10 mm trocar is introduced for the optic and then 5 mm trocars are placed under direct vision on each side of the midline by around 5 cm. 12 mmHg CO2 was used to maintain a correct work space. Under endoscopic vision the supra-aponeurotic space is dissected exposing the linea alba and superficial aponeurosis until we reach the umbilical region. The umbilicus was desinserted above the hernia sac, reintroducing it into the intra-abdominal compartment. Dissection continued until reaching the subcostal incisional hernia. Where the hernia is also dissected. The plication of the aponeurosis of the recti muscles was done with two continuous non-absorbable barbed sutures from the subxiphoid to suprapubic region. Then, a polypropylene of 15 cm × 10 cm mesh prosthesis was introduced in the supra-aponeurotic space (onlay) and fixed with securestrap. Finally, the umbilicus was reinserted to its normal position to the plicated fascia with an intracorporeal knotting.
- Gluppe SL, Hilde G, Tennfjord MK, Engh ME, Bø K. Effect of a Postpartum Training Program on the Prevalence of Diastasis Recti Abdominis in Postpartum Primiparous Women: A Randomized Controlled Trial. Phys Ther. 2018;98(4):260-268. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5963302/[↩][↩]
- Mahalakshmi V, Sumathi G, Chitra TV, Ramamoorthy V. Effect of exercise on diastasis recti abdominis among the primiparous women: a quasi-experimental study. Int J Reprod Contracept Obstet Gynecol. 2016;5(12):4441–4446.[↩]
- Mota PG, Pascoal AG, Carita AI, Bø K. Prevalence and risk factors of diastasis recti abdominis from late pregnancy to 6 months postpartum, and relationship with lumbo-pelvic pain. Man Ther. 2015;20(1):200–205.[↩]
- Parker MA, Millar LA, Dugan SA. Diastasis rectus abdominis and lumbo-pelvic pain and dysfunction—are they related? J Womens Health Phys Therap. 2009;33(2):15–22.[↩]
- Nardi WS, Busnelli GL, Tchercansky A, Pirchi DE, Medina PJ. Diastasis recti associated with midline hernias: Totally subcutaneous video-endoscopic repair. J Minim Access Surg. 2018;14(2):161-163. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5869979/[↩]
- Totally endoscopic surgery on diastasis recti associated with midline hernias. The advantages of a minimally invasive approach. Prospective cohort study. Bellido Luque J, Bellido Luque A, Valdivia J, Suarez Gráu JM, Gomez Menchero J, García Moreno J, Guadalajara Jurado J. Hernia. 2015 Jun; 19(3):493-501.[↩]





{kind=link}