
Contents
What is a dilated pore of Winer
A dilated pore of Winer is a commonly occurring benign hair follicle tumor (a tricho-epithelioma) that appears as an giant solitary open comedone (huge clogged hair follicle) filled with a keratin plug, with the surrounding skin remaining normal 1, 2. A dilated pore of Winer is a tumor of the intraepidermal follicle and infundibulum of a pilosebaceous apparatus 3. A dilated pore of Winer most commonly appears on the face of a middle-aged person 4. The lesion was first described by pioneering dermatologist Louis H. Winer in 1954 1. Winer suggested that an infection or an obstruction of the hair follicle opening is the stimulus for the development of a dilated pore of Winer in a process similar to those of inflammatory cystic acne or other cystic conditions 1.
Although dilated pore of Winer occurs in all sexes, a dilated pore of Winer occurs more frequently in men than women and is also more frequent in whites. Most cases occur at the age of 40 and older; however, there are reports of dilated pores occurring as early as 20.
Dilated pore of Winer lesion falls within the group of benign follicular tumors. Dilated pore of winer occurs as a small solitary papule centered by a follicular pore on the face, neck or back, mimicking a giant comedo 5. Although most commonly located on the head and neck, a dilated pore of Winer can also be found on the trunk of middle-aged and elderly individuals. These clinically present as an asymptomatic, solitary, enlarged pore with a keratin plug and normal surrounding skin. Prognosis is excellent for these lesions as they are benign and do not require any further testing or work-up. Histopathologic evaluation can confirm the diagnosis in uncertain cases. Removal can be performed via surgical excision for cosmetic purposes.
Superficial treatments, such as electrodesiccation, cauterization, coagulation, dermabrasion, or carbon dioxide laser surgery, are less effective because of the deeply invaginated base of a dilated pore of Winer.
Figure 1. Dilated pore of Winer

Figure 2. Dilated pore of Winer pathology
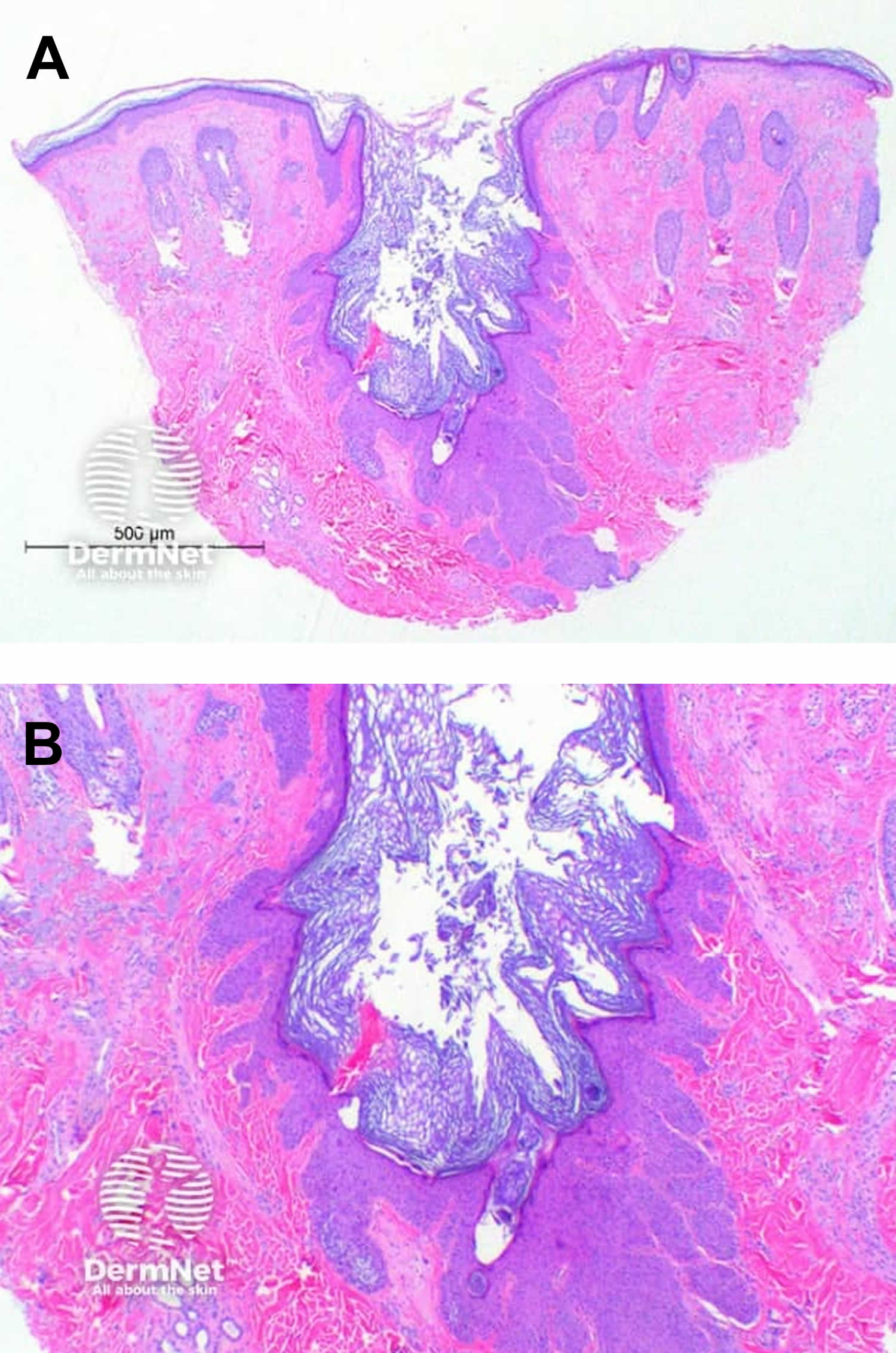
Footnotes: Scanning power view of dilated pore of Winer demonstrates a small invaginating epidermal process (Figure A). This is comprised of a widened follicular infundibulum filled with a small amount of keratinous material (Figure B). The infundibular epithelium is hyperplastic, forming small radiating strands at the base and sides of the pore (Figure B).
[Source 7 ]Dilated pore of winer causes
The cause of a dilated pore of Winer is unknown. Some scientists have considered the dilated pore of Winer to simply be an epidermal inclusion cyst with reactive hyperplasia of its epithelial lining and others proposed it to be a variant of nevus comedonicus 5, 8. However, this lesion has been shown to be a distinct entity as an adnexal neoplasm of the follicular infundibulum 3, 9. The exact cause and pathophysiology of a dilated pore of Winer are unknown 2. Winer, in his original study, suggested that an infection or an obstruction of the follicle ostium is the stimulus for the development of a dilated pore of Winer in a process similar to those of inflammatory cystic acne or other cystic conditions 1. Sun damage has also been attributed to the development of these lesions 2.
Dilated pore of Winer histopathology
A dilated pore of Winer is characterized histopathologically by a markedly dilated follicular infundibulum extending deeply into the dermis. The cavity is filled with lamellar keratin material. It is lined by epithelium that is atrophic near the ostium and acanthotic at the deeper portion of the invagination. Radiating off of the epithelium are regularly spaced, small, finger-like epithelial projections pushing into the surrounding dermis. These finger-like projections do not contain keratin cysts, ducts, or hair shafts 10.
Dilated pore of Winer signs and symptoms
A dilated pore of Winer will present as a single, enlarged pore. The pore may be blocked by a keratin plug with softer, white, keratin material beneath. They are asymptomatic, and the surrounding skin appears normal however a background of sun damage may be noted. Inflammation or infection along with pain and swelling can occur with manipulation. Although they have a tendency for the head and neck region, particularly the face, they can also present on the trunk, most commonly the back. Patients are usually middle-aged or older and may report a past or present history of severe acne.
Most patients with dilated pore of Winer consult a dermatologist (skin specialist) after many years of dealing with an unsightly, enlarged pore on their face 11.
Patients report needing to repeatedly express a keratotic plug from the center of the dilated pore of Winer 4. The expression of this plug allows the further removal of caseous, white, soggy keratin from the deeper portion of the pore. Once the content of the dilated pore is expressed, a keratotic material similar to the original plug refills the pore within several weeks 4.
A dilated pore of Winer usually appears as a solitary large comedo on the face, predominantly on the upper lip, cheek, or forehead. The lesion can also be found on the trunk, most commonly the back. A rare incidence involving external ear canal has also been reported 12.
The skin surrounding the pore appears to be unchanged, with no inflammation or induration.
Manipulation of a dilated pore of Winer may lead to infection and scarring.
Dilated pore of Winer diagnosis
A dilated pore of Winer is usually a clinical diagnosis. Histopathologic examination is not required but can be performed if the diagnosis is uncertain or in cases where the lesion is excised for cosmetic purposes. No other testing or work-up is needed.
Dermoscopic findings
Dermoscopic examination shows a pinkish nodule with peripheral vessels in a regular pattern. The individual vessels at the periphery of the lesion extend towards the center. The size of the vessels decreases with every progressive branching. The center of the lesion reveals a dilated ostium filled with terminal hairs 13.
Biopsy
Histologic examination of a biopsy specimen from the lesion is the only way to make a definitive diagnosis.
Dilated pore of Winer histopathology
A dilated pore of Winer is characterized histopathologically by a markedly dilated follicular infundibulum extending deeply into the dermis and, at times, into the subcutaneous tissue (see Figure 2 above) 14. The cavity is filled with lamellar keratin material and is lined by epithelium that is atrophic near the follicular ostium and acanthotic at the deeper portion of the invagination 14. Radiating off the epithelium are regularly spaced, small, finger-like epithelial projections pushing into the surrounding dermis. These finger-like projections do not contain keratin cysts, ducts, or hair shafts 5.
The epidermis is hypertrophic and proliferative in the deeper portion of the invagination where the numerous rete ridges project into the surrounding stroma. The cavity is filled with laminated keratin. Vellus hair follicles and small sebaceous lobules may be attached to the lower portion of the infundibulum 15. Gonzalez-Guerra et al 16 reported in 2008 that cutaneous adnexal tumors of the hair follicle can be identified using immunohistochemistry studies for calretinin, with differentiation towards cells of the outer root sheath.
Dilated pore of Winer differential diagnosis
Dilated pore of Winer differential diagnosis include 7, 17:
- Epidermoid Cyst. Epidermoid cysts also called sebaceous cysts are the most common benign skin cysts derived from the infundibulum or upper portion of a hair follicle 18, 19. Historically, epidermoid cysts have been referred to by various terms, including follicular infundibular cysts, epidermal cysts, and epidermal inclusion cysts 18. The term epidermal inclusion cyst refers specifically to an epidermoid cyst that is the result of the implantation of epidermal elements in the dermis 18. Because most lesions originate from the follicular infundibulum, the more general term epidermoid cyst is favored. The term sebaceous cyst should be avoided because it implies that the cyst is of sebaceous origin and epidermoid cysts do not involve sebaceous glands, nor do they contain sebum. Epidermoid cysts contain soft “cheesy” like material that’s composed of keratin, a protein component of skin, hair, and nails. Epidermoid cysts form when the top layer of skin (the epidermis) grows into the middle layer of the skin (the dermis) 20. This may occur due to injury or blocked hair follicles. An epidermoid cyst may have no pain or other symptoms associated with it, but if it becomes inflamed or infected, it may grow, become painful and red, and may rupture.
- Favre-Racouchot Syndrome (Nodular Elastosis With Cysts and Comedones). Favre-Racouchot syndrome is a disorder consisting of multiple open and closed comedones in the presence of sun damaged skin 21. Although the precise pathogenesis of Favre-Racouchot syndrome is unknown, it develops in individuals with a heavy smoking history and chronic exposure to UV light 22. Vogel et al 23 described a case of unilateral Favre-Racouchot syndrome indicating the etiologic role of chronic solar damage in this disease. Owing to the strong association with smoking, and the name “smokers’ comedones” has been proposed 24. Favre-Racouchot syndrome may represent as a sign of chloracne (a rare skin condition that appears as a result of exposure to dioxins or other polyhalogenated aromatic hydrocarbons), although both ultraviolet (UV) and infrared light exposure may contribute. Favre-Racouchot syndrome may also follow exposure to radiation therapy 25, 26. This was illustrated in a paper by Hoff et al 27, in which a 71-year-old man treated with radiation therapy for a malignant melanoma of the right paranasal sinus. He subsequently developed elastosis, open and closed comedones, and cysts in the radiation field 28. Lim et al 29, in a discussion of the adverse effects of UV radiation from the use of indoor tanning equipment, has cited Favre-Racouchot syndrome as one of these adverse effects.
- Trichilemmal Cyst (Pilar Cyst). Pilar cysts also called trichilemmal cysts or wens, are common growths that are filled with keratin that originates from the outer hair root sheath that form from hair follicles; they are most often found on the scalp 30, 31, 32. More than 90% of trichilemma cysts occur on the scalp, where they are the most common type of cutaneous cyst 33, 34. Pilar cysts are smooth and mobile, meaning they can be moved slightly under the skin. They are filled with keratin (a protein component found in hair, nails, and skin). They are usually painless but can be tender. There may be one or a few pilar cysts. Pilar cysts (trichilemmal cysts) are almost always benign. Very rarely, pilar cysts can become cancerous. Pilar cysts (trichilemmal cysts) may be sporadic, or they often run in the family, as they have an autosomal dominant pattern of inheritance (ie, the tendency to the cysts can be is passed on by a parent to their child of either sex, and the child has a 1 in 2 likelihood of inheriting it) 35, 31. In 2% of trichilemmal cysts, single or multiple foci of proliferating cells lead to tumors called proliferating trichilemmal cysts or malignant proliferating trichilemmal cysts 36. Proliferating trichilemmal cysts are gradually enlarging (up to 25 cm in diameter) exophytic nodules that occasionally ulcerate 33. Although these tumors are biologically benign, they may be locally aggressive 36. Recurrences and metastases have been observed, with rare malignant transformation 35, 36, 37, 38, 39.
- Trichoepithelioma. Trichoepithelioma is a rare benign skin tumor that arises from hair follicles 40, 41, 42. Trichoepithelioma is classified as a benign adnexal tumor and most commonly appears as either a solitary lesion or multiple nodules on the face. Trichoepithelioma is similar to trichoblastoma in that both are hair follicle tumors. However, trichoepitheliomas are more superficial whereas trichoblastomas tend to arise from the deep dermis 42. Trichoepithelioma do not cause ulceration or itching and are generally considered harmless 42. Multiple lesions are usually inherited. Cases associated with Brooke-Spiegler syndrome are caused by mutations of the cylindromatosis oncogene (CYLD) on chromosome 16q12-q13 43, 44, 45. A 2006 study suggested that abnormalities in CYLD gene might result in one of three syndromes: Brooke-Spiegler syndrome, familial cylindromatosis, and multiple familial trichoepithelioma 46. Furthermore, some cases of patients with multiple trichoepitheliomas appear to be sporadic and not related to familial incidence 47.
- Trichofolliculoma: Trichofolliculoma called folliculoma is an uncommon small benign tumor originating from the hair follicle tissue 48, 49, 50. Trichofolliculoma typically presents as a small, solitary flesh-colored or whitish nodule that occurs most often on the face around the nose region, scalp, or upper trunk in adults. Sometimes the lesion(s) have a central pore or black dot from which exudes sebaceous-like fluid (sebum), and is known as pore of Winer. In some cases a tuft of white hair may be growing from the central pore. Apart from its physical appearance, trichofolliculoma shows no other signs or symptoms. Trichofolliculoma is a benign follicular tumour that requires no treatment, although rare perineural invasion and reoccurrence after excision have been described. Occasionally they may be excised for cosmetic reasons or if they occur in functionally sensitive areas. Treatment options include curettage and electrodesiccation or surgical excision.
- Hair cortex comedo : This lesion demonstrates infundibular epithelium associated with a dense cornified plug with compact laminated corneocytes, and matrical and supramatrical epithelium representing attempts to form the hair cortex and shaft.
Dilated pore of Winer treatment
No treatment is required for a dilated pore of Winer 2. Removal can be performed for cosmetic concerns, and excision in an elliptical fashion or by punch biopsy and closure of the resulting surgical defect is usually curative 11. Merely removing the keratin material can be done using a comedone extractor; however, keratin gradually re-accumulates within the lesion 2. Destructive techniques such as electrodesiccation, electrocautery, laser surgery, dermabrasion, and cryotherapy are less effective due to the deeply situated base of the invagination 1. There are no effective medical treatments for these lesions.
Complications of surgical removal include scarring, infection, and bleeding. Infection risk after surgery can be minimized by using proper aseptic or clean technique. Infection before or following surgery can be treated using topical or oral antibiotics depending on severity.
Dilated pore of Winer prognosis
Complete excision of the lesion is curative. Incomplete excision can result in the recurrence of the remaining infundibular lining. To date, there have been no reports of death associated with a dilated pore of Winer 2. Also, there have been no reports of syndromes associated with dilated pore of Winer 2. There have been rare case reports of other malignant cutaneous neoplasms, such as basal cell carcinoma and squamous cell carcinomas, arising in dilated pores of Winer 2. However, these are most likely coincidental 51, 52. There has been one case report of a trichoblastoma arising in a dilated pore of Winer 53. Inflammation or infection of the surrounding skin can result from manipulation of the lesion by the patient in an attempt to remove the keratin plug.
- WINER LH. The dilated pore, a tricho-epithelioma. J Invest Dermatol. 1954 Sep;23(3):181-8. https://www.jidonline.org/article/S0022-202X(15)48606-3/pdf[↩][↩][↩][↩][↩]
- Benedetto CJ, Riley CA, Athalye L. Dilated Pore of Winer. [Updated 2022 Sep 12]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK532967[↩][↩][↩][↩][↩][↩][↩][↩]
- Steffen C. Winer’s dilated pore: the infundibuloma. Am J Dermatopathol. 2001 Jun;23(3):246-53. doi: 10.1097/00000372-200106000-00020[↩][↩]
- Dilated Pore of Winer. https://emedicine.medscape.com/article/1061188-overview[↩][↩][↩]
- Tellechea O, Cardoso JC, Reis JP, Ramos L, Gameiro AR, Coutinho I, Baptista AP. Benign follicular tumors. An Bras Dermatol. 2015 Nov-Dec;90(6):780-96; quiz 797-8. doi: 10.1590/abd1806-4841.20154114[↩][↩][↩]
- Giant Blackheads: What Is a Dilated Pore of Winer? https://slmdskincare.com/blogs/learn/giant-blackheads-what-is-a-dilated-pore-of-winer[↩]
- Dilated pore of Winer pathology. https://dermnetnz.org/topics/dilated-pore-of-winer-pathology[↩][↩]
- Mittal RR, Sethi PS, Jha A. Dilated pore of Winer. Indian J Dermatol Venereol Leprol. 2002 Jul-Aug;68(4):239-40.[↩]
- Morikawa T, Takizawa H, Ohnishi T, Watanabe S. Dilated pore: a case report and an immunohistochemical study of cytokeratin expression. J Dermatol. 2003 Jul;30(7):556-8. doi: 10.1111/j.1346-8138.2003.tb00432.x[↩]
- Tellechea O, Cardoso JC, Reis JP, Ramos L, Gameiro AR, Coutinho I, Baptista AP. Benign follicular tumors. An Bras Dermatol. 2015 Nov-Dec;90(6):780-96; quiz 797-8.[↩]
- Jakobiec FA, Bhat P, Sutula F. Winer’s dilated pore of the eyelid. Ophthalmic Plast Reconstr Surg. 2009 Sep-Oct;25(5):411-3. doi: 10.1097/IOP.0b013e3181b3b6e3[↩][↩]
- Ayoub OM, Timms MS, Mene A. Winer’s dilated pore, rare presentation in the external ear canal. Auris Nasus Larynx. 2001 Nov;28(4):349-52. doi: 10.1016/s0385-8146(01)00089-x[↩]
- Moreira A, Menezes N, Guedes R, Tente D, Baptista A, Varela P. Dermoscopy of a dilated pore of Winer. Eur J Dermatol. 2010 Mar-Apr;20(2):229. doi: 10.1684/ejd.2010.0852[↩]
- Dilated Pore of Winer Workup. https://emedicine.medscape.com/article/1061188-workup#c7[↩][↩]
- Lee JY, Hirsch E. Pilar Sheath Acanthoma. Arch Dermatol. 1987;123(5):569. doi:10.1001/archderm.1987.01660290033010[↩]
- Gonzalez-Guerra E, Requena L, Kutzner H. [Immunohistochemical study of calretinin in normal hair follicles and tumors with follicular differentiation]. Actas Dermosifiliogr. 2008 Jul-Aug. 99(6):456-63.[↩]
- Dilated Pore of Winer Differential Diagnoses. https://emedicine.medscape.com/article/1061188-differential[↩]
- Epidermoid Cyst. https://emedicine.medscape.com/article/1061582-overview[↩][↩][↩]
- Epidermoid cyst. https://dermnetnz.org/topics/epidermoid-cyst[↩]
- Epidermoid Cyst (Sebaceous Cyst). https://skinsight.com/skin-conditions/epidermoid-cyst-sebaceous-cyst[↩]
- Favre-Racouchot Syndrome (Nodular Elastosis With Cysts and Comedones). https://emedicine.medscape.com/article/1119362-overview[↩]
- Keough GC, Laws RA, Elston DM. Favre-Racouchot syndrome: a case for smokers’ comedones. Arch Dermatol. 1997 Jun;133(6):796-7. doi: 10.1001/archderm.133.6.796[↩]
- Vogel S, Mühlstädt M, Molin S, Ruzicka T, Schneider J, Herzinger T. Unilateral favre-racouchot disease: evidence for the etiological role of chronic solar damage. Dermatology. 2013;226(1):32-4. doi: 10.1159/000346576[↩]
- Pizzati A, Passoni E, Nazzaro G. Monolateral Favre-Racouchot Syndrome Following Long-term Exposure to Infrared Waves. JAMA Dermatol. 2018 May 1;154(5):623-625. doi: 10.1001/jamadermatol.2017.6248[↩]
- Breit S, Flaig MJ, Wolff H, Plewig G. Favre-Racouchot-like disease after radiation therapy. J Am Acad Dermatol. 2003 Jul;49(1):117-9. doi: 10.1067/mjd.2003.294[↩]
- Friedman SJ, Su WP. Favre-Racouchot syndrome associated with radiation therapy. Cutis. 1983 Mar;31(3):306-10.[↩]
- [↩]
- Hoff NP, Reifenberger J, Bölke E, Homey B, Gerber PA. Strahleninduzierter Morbus Favre-Racouchot [Radiation-induced Favre-Racouchot disease]. Hautarzt. 2012 Oct;63(10):766-7. German. doi: 10.1007/s00105-012-2444-6[↩]
- Lim HW, James WD, Rigel DS, Maloney ME, Spencer JM, Bhushan R. Adverse effects of ultraviolet radiation from the use of indoor tanning equipment: time to ban the tan. J Am Acad Dermatol. 2011 May;64(5):893-902. doi: 10.1016/j.jaad.2011.03.007[↩]
- Pilar Cyst. https://skinsight.com/skin-conditions/pilar-cyst/[↩]
- Trichilemmal cyst. https://dermnetnz.org/topics/trichilemmal-cyst[↩][↩]
- Trichilemmal Cyst (Pilar Cyst). https://emedicine.medscape.com/article/1058907-overview[↩]
- James WD, Elston DM, Treat JR, Rosenbach MA, Neuhaus IM. Epidermal nevi, neoplasms and cysts. Andrews’ Diseases of the Skin: Clinical Dermatology. 13th ed. Philadelphia: Elsevier; 2020. 636-685.[↩][↩]
- Al-Khateeb TH, Al-Masri NM, Al-Zoubi F. Cutaneous cysts of the head and neck. J Oral Maxillofac Surg. 2009 Jan;67(1):52-7. doi: 10.1016/j.joms.2007.05.023[↩]
- Cysts. Bolognia JL, Schaffer JV, Cerroni L, eds. Dermatology. 5th ed. Elsevier; 2024. Section 18: Neoplasias of the Skin: Chap 110. [↩][↩]
- Weiss J, Heine M, Grimmel M, Jung EG. Malignant proliferating trichilemmal cyst. J Am Acad Dermatol. 1995 May;32(5 Pt 2):870-3. doi: 10.1016/0190-9622(95)91550-8[↩][↩][↩]
- Liu L, Long T, Wei N, Zhang H, Tang C, Gao J. Successful treatment of trichilemmal carcinoma with distant metastasis using pembrolizumab: a case report and review. Immunotherapy. 2024;16(10):659-667. doi: 10.1080/1750743X.2024.2353535[↩]
- Ibrahim AE, Barikian A, Janom H, Kaddoura I. Numerous recurrent trichilemmal cysts of the scalp: differential diagnosis and surgical management. J Craniofac Surg. 2012 Mar;23(2):e164-8. doi: 10.1097/SCS.0b013e31824cdbd2[↩]
- Satyaprakash AK, Sheehan DJ, Sangüeza OP. Proliferating trichilemmal tumors: a review of the literature. Dermatol Surg. 2007 Sep;33(9):1102-8. doi: 10.1111/j.1524-4725.2007.33225.x[↩]
- Trichoepithelioma in Adult. https://www.visualdx.com/visualdx/diagnosis/?moduleId=101&diagnosisId=52428[↩]
- Trichoepithelioma. https://emedicine.medscape.com/article/1060049-overview[↩]
- Trichoepithelioma. https://dermnetnz.org/topics/trichoepithelioma[↩][↩][↩]
- Guardoli D, Argenziano G, Ponti G, Nasti S, Zalaudek I, Moscarella E, Lallas A, Piana S, Specchio F, Martinuzzi C, Raucci M, Pellacani G, Longo C. A novel CYLD germline mutation in Brooke-Spiegler syndrome. J Eur Acad Dermatol Venereol. 2015 Mar;29(3):457-62. doi: 10.1111/jdv.12578[↩]
- Vanecek T, Halbhuber Z, Kacerovska D, Martinek P, Sedivcova M, Carr RA, Slouka D, Michal M, Kazakov DV. Large germline deletions of the CYLD gene in patients with Brooke-Spiegler syndrome and multiple familial trichoepithelioma. Am J Dermatopathol. 2014 Nov;36(11):868-74. doi: 10.1097/DAD.0000000000000068[↩]
- Bowen S, Gill M, Lee DA, Fisher G, Geronemus RG, Vazquez ME, Celebi JT. Mutations in the CYLD gene in Brooke-Spiegler syndrome, familial cylindromatosis, and multiple familial trichoepithelioma: lack of genotype-phenotype correlation. J Invest Dermatol. 2005 May;124(5):919-20. doi: 10.1111/j.0022-202X.2005.23688.x[↩]
- Young AL, Kellermayer R, Szigeti R, Tészás A, Azmi S, Celebi JT. CYLD mutations underlie Brooke-Spiegler, familial cylindromatosis, and multiple familial trichoepithelioma syndromes. Clin Genet. 2006 Sep;70(3):246-9. doi: 10.1111/j.1399-0004.2006.00667.x[↩]
- Sehrawat M, Jairath V, Jain VK. Nonfamilial Multiple Trichoepithelioma: Few and Far Between. Indian J Dermatol. 2016 Jan-Feb;61(1):78-80. doi: 10.4103/0019-5154.174030[↩]
- Trichofolliculoma. https://dermnetnz.org/topics/trichofolliculoma[↩]
- Trichofolliculoma. https://www.visualdx.com/visualdx/diagnosis/?moduleId=101&diagnosisId=52429[↩]
- Hamartoma. https://emedicine.medscape.com/article/1254012-overview[↩]
- Carlson-Sweet KL, Weigand DA, MacFarlane DF. Trichoid basal cell carcinoma found in a dilated pore on the nose. Dermatol Surg. 2000 Sep;26(9):874-6. doi: 10.1046/j.1524-4725.2000.00083.x[↩]
- Zhao L, Xu J, Fang F, Qian G, Wang Y, Wang QQ. Squamous cell carcinoma found in a dilated pore. J Eur Acad Dermatol Venereol. 2007 Feb;21(2):277-8. doi: 10.1111/j.1468-3083.2006.01849.x[↩]
- Misago N, Sada A, Narisawa Y. Trichoblastoma with a dilated pore. J Am Acad Dermatol. 2006 Feb;54(2):357-8. doi: 10.1016/j.jaad.2005.07.033[↩]





{kind=link}