Contents
Caffeine and Weight Loss
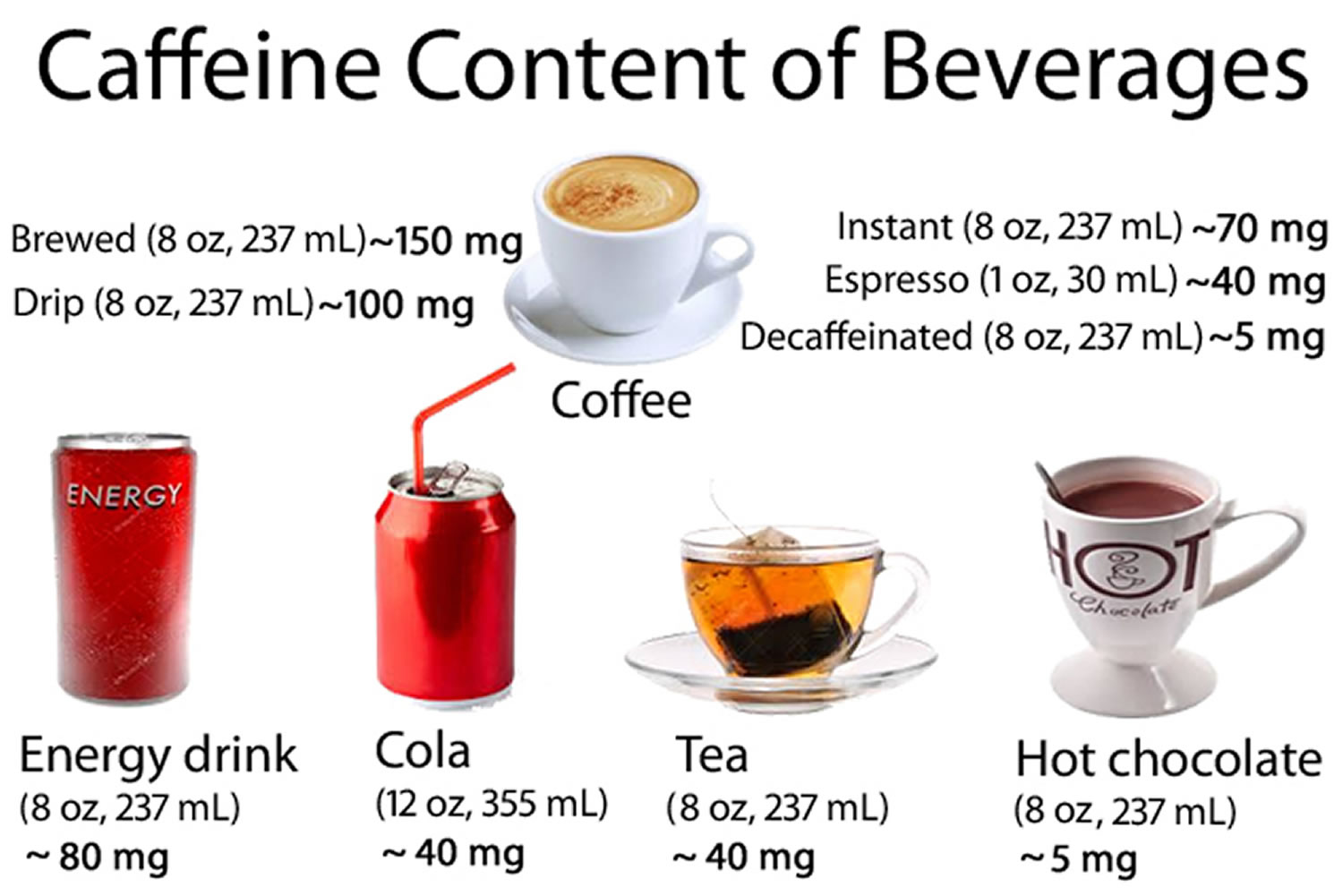
Caffeine is a widely consumed stimulant, which can be consumed in several forms (e.g. coffee, energy drinks, etc.), is one of the most commonly used psychoactive substance worldwide 1. Recent data from nationally representative samples indicate about 89% of American adults consume caffeinated products daily with virtually no difference between men and women in how frequently the products are used 2. Caffeine is a naturally occurring alkaloid substance found in numerous plant species with coffee beans, tea leaves, cocoa beans, and kola nuts are the primary natural sources of this compound 3. Caffeine is added to numerous foods and beverages (e.g., soft drinks and energy drinks). Chocolate and cocoa 4 are also sources of caffeine, as are certain dietary supplements 5 and medications 4.
There has been some concern regarding the potential adverse health effects of caffeine, especially with regard to cardiovascular disease and diabetes mellitus risk 6. Acute caffeine consumption increases blood pressure and plasma lipids, and these effects led to speculation that chronic caffeine consumption would increase cardiovascular disease risk 7; however, epidemiological studies have generally concluded that caffeine consumption is not associated with higher cardiovascular risk 8. Short-term metabolic studies have suggested caffeine has adverse effects on glucose tolerance and whole-body glucose management 9 which could increase diabetes risk, but longer-term investigations found that coffee consumption was associated with a lower risk of Type 2 diabetes 10. Other studies suggested there were positive effects of caffeinated products, including reduced liver dysfunction 11, slower age-related cognitive declines 12, improvement in some types of athletic performances 13, and reduced intensity of exercise-induced delayed onset muscle soreness 14. A comprehensive review of the health effects of caffeine concluded that adult consumption ≤400 mg/day (6 mg/kg body weight for a 65 kg person) was not associated with adverse effects on cardiovascular health, bone status, male reproductive systems, adult behavior, or cancer risk, although it was recommended that women of reproductive age should consume <300 mg/day because of possible effects on fertility and conception 15.
Caffeine is generally regarded as a safe substance and has a very long history of use. A comprehensive review of the effects of caffeine consumption on human health, commissioned by Health Canada, concluded that for the healthy adult population, moderate chronic intakes of caffeine up to 400 mg/d are not associated with adverse effects on cardiovascular health, calcium balance and bone status, behavior, cancer risk, and male fertility 16. Several recent meta-analyses support these conclusions 17, 18. However, it was suggested that women planning to become pregnant, as well as pregnant and lactating women, limit caffeine ingestion to ≤300 mg/d because of some evidence that caffeine consumption may adversely affect fertility and fetal growth 19.
Recommended Maximum Caffeine Intake Levels for Children and Women of Childbearing Age Children 16:
- 4 – 6 years 45 mg/day
- 7 – 9 years 62.5 mg/day
- 10 – 12 years 85 mg/day
Women who are planning to become pregnant, pregnant women and breast feeding mothers 16:
- 300 mg/day
Caffeine is considered a diuretic during periods of rest which results in a greater volume of fluid loss through urine 20. For instance, a study conducted by Neuhäuser-Berthold et al. 21 demonstrated a loss in total body water of approximately 1.1 kg following the consumption of a 321 mg serving of caffeine in the form of coffee in the morning and afternoon. Moreover, Passmore et al. 22 examined the effects of early day caffeine consumption on urine output in several doses (45, 90, 180, and 360 mg) and found a statistical difference following the highest dose. Caffeine’s role as a diuretic is relatively understood, but it is unclear if caffeine consumption truly burns more calories, and increases the breakdown of fat.
Caffeine is frequently added to dietary supplements with claims it facilitates weight loss. The labels of supplements that contain caffeine don’t always list it, so you might not know if a supplement has caffeine.
In humans, caffeine has been shown to stimulate thermogenesis and fat oxidation 23, 24, 25. In humans caffeine stimulates thermogenesis by unknown mechanisms and it is hypothesized that lactate and triglyceride production and increased vascular smooth muscle tone may be responsible for the major part of the thermogenic effect of caffeine 24. The magnitude of thermogenesis was smaller in obese (4.9 +/- 2.0%) than in lean subjects (7.6 +/- 1.3%) 25. The thermogeneic response to caffeine was prolonged during the night in lean women only. The coffee-induced stimulation of energy expenditure was mediated by a concomitant increase in lipid and carbohydrate oxidation. The magnitude of this effect was, however, blunted in obese women (lipid oxidation increased by 29 and 10% in lean and obese women, respectively) 25. Despite the high levels of urinary methylxanthine excretion, thermogenesis and lipid oxidation were less stimulated in obese than in lean subjects 25.
More recently it has been shown caffeine affects the thermogenesis by inhibiting the enzyme phosphodiesterase 26. This enzyme degrades intracellular cyclic amino mono phosphate 27. Phosphodiesterase usually hydrolyses cyclic adenosine monophosphate (cAMP) to AMP, but after consumption of caffeine, cAMP concentration rises and sympathetic nerve system activity will be increased and inactive hormone-sensitive lipase will be activated, which promotes lipolysis 28. The sympathetic nerve system activity and lipoysis are dependent on cAMP, because cAMP activates the protein kinase A 29. Besides the inhibition of phosphodiesterase, caffeine also affects the thermogenesis through the stimulation of substrate cycles such as the Cori-cycle and the free fatty acid-triglyceride cycle 30. Caffeine is a methylxanthine, which has a thermogenic impact. In the Cori cycle, lactate moves from the muscles to the liver, where it will be converted into pyruvate. The pyruvate will be converted to glucose by the enzyme lactate dehydrogenase and circulate back to the muscles through the blood 30. Acheson et al. 28 showed that free fatty acids turnover and lipid oxidation are increased after the consumption of caffeine but that it requires a large increase in free fatty acids turnover to have a small increase in lipid oxidation. Nonoxidative lipid turnover, the hydrolysis and reesterification of triacylglycerol, is greater than the increase in oxidative lipid disposal 28. They also found that caffeine antagonizes the inhibitory effects of adenosine on lipolysis by adenylyl cyclase. Nonadrenergic thermogenic mechanisms can also be involved, as caffeine antagonizes the ryanodine receptor, the calcium ion release channel of sarcoplasmatic reticulum in skeletal muscle that for instance increases glycolysis and adenosine triphosphate turnover after stimulation 28.
Caffeine inhibit two enzymes, which interrupt the pathway of norepinephrine-activated thermogenesis 31. As sympathetic nerve system activity is determined by the concentration of norepinephrine, more norepinephrine means a higher activity and increased energy expenditure. Sympathetic nerve system activity regulates the resting metabolic rate, which is the largest component of the daily energy expenditure. Norepinephrine makes it possible to increase the usage of adenosine triphosphate (ATP) through ion pumping and substrate cycling 32. The rate of mitochondrial oxidation is also involved in the increased thermogenesis due to the poor coupling of adenosine triphosphate (ATP) synthesis, which leads to heat production. Gene expression of the uncoupling proteins also increases when cAMP activates the protein kinase A, after the inhibition of phophodiesterase by caffeine 33. The protein kinase A stimulates hormone-sensitive lipase, which increases the concentration of free fatty acids by the conversion of triglycerides. Uncoupling proteins activity will be enhanced through this 33.
Single-dose oral administration of 100 mg caffeine increased the resting metabolic rate of both lean and postobese human volunteers by 3–4% over 150 min and improved the defective diet-induced thermogenesis observed in the postobese subjects 23. Measurements of energy expenditure in a room respirometer indicate that repeated caffeine administration (100 mg) at 2-h intervals over a 12-h day period increased the energy expenditure of both subject groups by 8–11% during that period but had no influence on the subsequent 12-h night energy expenditure 23. The net effect was a significant increase in daily energy expenditure of 150 kcal in the lean volunteers and 79 kcal in the postobese subjects. Caffeine at commonly consumed doses can have a significant influence on energy balance and may promote thermogenesis in the treatment of obesity 23.
Caffeine 34, 35, 36, 37 has been shown to increase energy expenditure in humans, and weight loss has reduced risk factors for diabetes in clinical trials 38. Consequently, it seems possible that both coffee and tea consumption may decrease diabetes risk by helping individuals control their body weight. However, in a small study involving fifty healthy adults aged 18 to 50 years (42% male) where participants consumed a beverage containing 0, 1, or 3 mg/kg caffeine (order randomized). Thirty minutes later, participants consumed a buffet breakfast, ad libitum. After leaving the laboratory, participants completed hourly appetite assessments and dietary habit books until midnight or bedtime. The study results suggest caffeine has weak, transient effects on energy intake and do not support caffeine as an effective appetite suppressant 39.
Caffeine may also slightly boost weight loss or prevent weight gain, but there’s no sound evidence that increased caffeine consumption results in significant or permanent weight loss 40.
Efficacy of caffeine
For many years caffeine is known for its stimulating properties and the thermogenic effects have been extensively examined. Besides enhancing energy expenditure, caffeine also affects energy intake. However, these acute effects have not resulted into a successful long-term approach yet (Table 1) 41. Only in a prospective study from Lopez-Garcia et al.,69 who studied the effect of caffeine on long-term weight change in a cohort, it was found that people who increased the caffeine consumption over 12 years gained less weight than those who decreased the caffeine consumption. Previous studies suggest that sensitivity to caffeine may be lost over time, which means that body weight regulation cannot be sustained for a longer period of time while receiving the same dosage.
Table 1: Short-term and long-term studies with caffeine
| Author | Year | Duration (hours or weeks) | Sample size (n) | BMI (kg/ m2) | Gender | Age (years) | Dosage (mg) | Outcome |
|---|---|---|---|---|---|---|---|---|
| Short-term study | ||||||||
| Acheson et al.42 | 1980 | 3 | CAF=27 | 18–30 | M/F | 21–35 | CAF=300–600 | Increase in EE in normal weight (10–16%) and obese subjects; however, only increase in fat oxidation in normal weight subjects |
| Tremblay et al 43 | 1988 | 1.5 | CAF=20 | 21.5 | M/F | 20.8 | CAF=300 | Decrease in energy intake in men (21.7%) |
| Dulloo et al.44 | 1989 | 2.5/24 | CAF=18 and 11 | 26.1–29.6 | M/F | 20–35 | CAF=100 and 600 | Increase in EE after 2.5 h (3–4%) and 24 h (8–11%); net increase in lean subjects 150 kcal and postobese 79 kcal |
| Astrup et al.30 | 1990 | 3 | CAF=6 | 21.9 | M/F | 20–32 | CAF=100, 200 and 400 | Net increase in EE after 100 and 400 mg of 27.6 and 97.2 kcal |
| Bracco et al.45 | 1995 | 24 | CAF=20 | <25 and 25> | F | 20–35 | CAF=500 | Increase in EE and lipid oxidation in lean (7.6; 29%) and obese subjects (4.9; 10%) |
| Arciero et al.46 | 1995 | 1.5 | CAF=20 | 25.1 | M | 19–80 | CAF=300–350 | Increase in EE of 9.5–11% |
| Dulloo et al.47 | 1999 | 24 | CAF=10 | 25.1 | M | 25 | CAF=150 | No difference in EE between caffeine and placebo group |
| Hollands et al 48 | 2001 | 2 | CAF=12 | 22.3 | M/F | 20–46 | CAF=100 | Increase in EE of 16% |
| Rumpler et al.49 | 2001 | 23 | CAF=12 | 18–30 | M | 25–60 | CAF=270 | Increase in EE of 3.4%=331 kJ day−1 |
| Acheson et al.28 | 2004 | 4 | CAF=8 | 25.5 | M | 23.1 | CAF=770 | Increase in EE of 13.3% |
| Gregersen et al.50 | 2009 | 13.5 | CAF=15 | 22.4 | M | 23.6 | CAF=150 | No significant difference in EE between caffeine and placebo group |
| Long-term study | ||||||||
| Pasman et al.41 | 1997 | 56 | CAF=13 | 31.2 | F | 34.8 | CAF=100 per day | No weight maintenance (+66.1% body weight regain) |
Abbreviations: CAF = caffeine; EE = energy expenditure; BMI = body mass index; M = male; F = female.
[Source 51]Caffeine Supplements
Caffeine is one of the ingredients now being included in many of the weight loss supplements. It’s added for its energy enhancement, appetite suppressant, and “fat-burning” properties.
On September 1, 2015, the FDA issued warning letters to five distributors of pure powdered caffeine because these products are dangerous and present a significant or unreasonable risk of illness or injury to consumers. (Source 52). Pure powdered caffeine products are potentially dangerous and have contributed to at least two deaths 53. The FDA advises consumers to avoid pure powdered caffeine. It is nearly impossible to accurately measure pure powdered caffeine with common kitchen measuring tools and you can easily consume a lethal amount.
The difference between a safe amount and a toxic dose of caffeine in these pure powdered products is very small. Safe quantities of these products can be nearly impossible to measure accurately with common kitchen measuring tools. Volume measures, such as teaspoons, are not precise enough to calculate how many milligrams of caffeine are in the serving size. Pre-existing conditions can intensify the effects of caffeine and make the product more dangerous for these individuals.
One teaspoon of pure powdered caffeine (100 percent caffeine) is equivalent to the amount of caffeine in about 28 cups of regular coffee. While consumers of caffeinated products such as coffee, tea, and soda may be aware of caffeine’s less serious effects – such as nervousness and tremors – they may not be aware that these pure powdered caffeine products are much more potent and can cause serious health effects, including rapid or dangerously erratic heartbeat, seizures and death. Vomiting, diarrhea, stupor and disorientation are also symptoms of caffeine toxicity.

Does caffeine work ?
In a prospective cohort study 54 to assess the effect of weight change on the relationship between coffee and tea consumption and diabetes risk. The finding of that study found that for less than or equal to 60-years-old subjects, the risk of diabetes was significantly, negatively and independently associated with the consumption of ground-caffeinated coffee, ground-decaffeinated coffee and regular tea offers clues to the underlying causes of the reduction in diabetes risk. It suggests that each of these beverages contains constituents that are involved in reducing diabetes risk, and that are not contained, or not active, in the other two beverages. Caffeine appears to have been involved in the reduction of diabetes risk, possibly by inducing weight loss, because: (1) caffeine accounted for the significance of the negative association between diabetes risk and ground-caffeinated coffee, after the effects of ground-decaffeinated coffee and regular tea had been considered; (2) caffeine also accounted for the significance of the negative association between weight gain and ground-caffeinated coffee, after the effects of ground-decaffeinated coffee had been considered; and (3) the negative association between caffeine intake and diabetes risk was only significant for subjects with prior weight loss. These findings are consistent with the finding in several previously-published studies that caffeine induces thermogenesis 34, 55, 36 and stimulates lipid oxidation 34, 36, 37 in humans. Caffeine might thereby help individuals control their weight, and hence decrease diabetes-risk.
In addition, some studies found that even decaffeinated coffee may contribute to modest weight loss, suggesting that substances or factors besides caffeine may play a role in weight loss.
A series of four trials 56 was carried out to investigate the effects of caffeine and coffee on the metabolic rate and substrate utilization in normal weight and obese individuals. In the first trial 8 mg/kg caffeine was compared with a placebo in normal weight subjects. Metabolic rate increased significantly during the 3 hr after caffeine ingestion. While plasma glucose, insulin, and carbohydrate oxidation did not change significantly, plasma free fatty acid levels rose from 432 +/- 31 to 848 +/- 135 muEq/liter and were accompanied by significant increases in fat oxidation during the last hour of the test. In the second and third trials the effects of coffee providing 4 mg/kg caffeine were studied in control and obese subjects. Metabolic rate increased significantly in both groups; however, significant increases in fat oxidation were only observed in the control group. Plasma free fatty acids did not change in the obese. In the fourth trial, coffee was taken with a 3080 kJ meal. The thermic effect of the meal was significantly greater after coffee than after decaffeinated coffee and again fat oxidation was significantly greater after coffee. In conclusion caffeine/coffee stimulates the metabolic rate in both control and obese individuals; however, this is accompanied by greater oxidation of fat in normal weight subjects. Weight-loss dietary supplements with caffeine might help you lose a little weight or gain less weight over time. But when you use caffeine regularly, you develop a tolerance to it. This tolerance might lessen any effect of caffeine on body weight over time.
Although research about the connection between caffeine and weight isn’t definitive, there are a few theories about how caffeine might affect weight, including:
- Appetite suppression. Caffeine may reduce your desire to eat for a brief time, but there’s not enough evidence to show that long-term consumption aids weight loss.
- Calorie burning. Caffeine may stimulate thermogenesis — one way your body generates heat and energy from digesting food. But this probably isn’t enough to produce significant weight loss.
It is possible that subjects with weight loss, and hence lower diabetes risk, were also, coincidentally, prone to drinking ground coffee and regular tea, and that the prior weight loss caused the negative association between these beverages and diabetes risk. However, given that previous studies have yielded evidence supporting the weight-reduction potential of both regular tea 34 and caffeine 34, 36, 37 it seems more likely that the beverages themselves promoted the weight loss and hence the reduction in diabetes risk. In addition, some studies found that even decaffeinated coffee may contribute to modest weight loss, suggesting that substances or factors besides caffeine may play a role in weight loss.
The bottom line: Be cautious about using caffeine products to help with weight loss. When used in moderation (400 milligrams or less) by healthy adults, caffeine is generally safe. But too much caffeine might cause nervousness, insomnia, nausea, increased blood pressure and other problems.
Also keep in mind that some caffeinated beverages, such as specialty coffees, are high in calories and fat. So instead of losing weight, you might actually gain weight if you drink too many of these.
Safety of caffeine
Caffeine is safe at low doses. But it can make you feel nervous, jittery, and shaky. It can also affect your sleep. At high doses (above about 400 milligrams [mg] a day for adults), it can cause nausea, vomiting, rapid heartbeat, and seizures. Combining caffeine with other stimulant ingredients can increase caffeine’s effects.
Caffeine is found in many beverages, including coffee, tea, energy drinks and colas; in products containing cocoa or chocolate; and in a variety of medications and dietary supplements, including supplements aimed at weight loss.
Caffeine appears to be a safe thermogenic agent for weight control. In adults, the short-term lethal dose for caffeine is estimated at 5–10 g per day (either intravenously or orally), which is equivalent to 75 cups of coffee, 125 cups of tea or 200 cola beverages 57. Long-term ingestion of caffeine has been suggested to have some minor adverse effects on human health. Astrup et al. 30 observed only small and insignificant changes in blood pressure and pulse rate after 100 and 200 mg caffeine. In contrast, 400 mg caffeine significantly increased systolic and diastolic blood pressure by an average value of 6.3 mmHg. Furthermore, after 400 mg caffeine, significantly more subjects reported side effects such as palpitation, anxiety, headache, restlessness, dizziness compared with placebo 30. Robertson et al. 58 administrated 250 mg oral caffeine to nine subjects who were not used to coffee. Systolic blood pressure increased 10 mmHg 1 hour after caffeine consumption. Heart rate showed a decrease after the first hour followed by an increase above baseline after 2 hours 58. However, in a subsequent study that examined the chronic effects of caffeine ingestion (150 mg day−1 for 7 days), tolerance to these effects was developed after 1–4 days 59. Thus no long-term effects of caffeine on blood pressure, heart rate or plasma rennin activity were demonstrated. Furthermore, in the short term, Bracco et al. 45 did not find a significantly altered heart rate during the day after 4 mg caffeine per kg body weight was consumed five times daily. Accordingly, the use of caffeine is relatively safe, as it is quite certain that, although acute caffeine consumption may alter some cardiovascular variables, chronic ingestion of caffeine has little or no health consequences.
- Effects of caffeine and coffee consumption on cardiovascular disease and risk factors. Mattioli AV. Future Cardiol. 2007 Mar; 3(2):203-12. https://www.ncbi.nlm.nih.gov/pubmed/19804249/[↩]
- Trends in intake and sources of caffeine in the diets of US adults: 2001-2010. Fulgoni VL 3rd, Keast DR, Lieberman HR. Am J Clin Nutr. 2015 May; 101(5):1081-7. https://www.ncbi.nlm.nih.gov/pubmed/25832334/[↩]
- Institute of Medicine, Committee on Military Nutrition Research, Food and Nutrition Board. Caffeine for the sustainment of mental task performance. Washington (DC): National Academies Press; 2001.[↩]
- Heckman MA, Weil J, Gonzalez de Mejia E. Caffeine (1, 3, 7-trimethylxanthine) in foods: a comprehensive review on consumption, functionality, safety, and regulatory matters. J Food Sci 2010;75:R77–87.[↩][↩]
- Andrews KW, Schweitzer A, Zhao C, Holden JM, Roseland JM, Brandt M, Dwyer JT, Picciano MF, Saldanha LG, Fisher KD, et al. The caffeine contents of dietary supplements commonly purchased in the US: analysis of 53 products with caffeine-containing ingredients. Anal Bioanal Chem 2007;389:231–9.[↩]
- Knapik JJ, Trone DW, McGraw S, Steelman RA, Austin KG, Lieberman HR. Caffeine Use among Active Duty Navy and Marine Corps Personnel. Nutrients. 2016;8(10):620. doi:10.3390/nu8100620 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5084008/[↩]
- Cai L., Ma D., Zhang Y., Lui Z., Wang P. The effect of coffee consumption on serum lipids: A meta-analysis of randomized controlled trials. Eur. J. Clin. Nutr. 2012;66:872–877. doi: 10.1038/ejcn.2012.68[↩]
- Wilson P.W.F., Bloom H.L. Caffeine consumption and cardiovascular risk: Little cause for concern. J. Am. Heart Assoc. 2016;5:e003089. doi: 10.1161/JAHA.115.003089[↩]
- Shearer J., Graham T.E. Performance effects and metabolic consequences of caffeine and caffeinated energy drink consumption on glucose disposal. Nutr. Rev. 2014;72:121–136. doi: 10.1111/nure.12124[↩]
- Ding M., Bhupathiraju S.N., Chen M., VanDam R.M., Hu F.B. Caffeinated and decaffeinated coffee consumption and risk of Type 2 diabetes: A systematic review and a dose-response meta-analysis. Diabetes Care. 2014;37:569–586. doi: 10.2337/dc13-1203 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3898757/[↩]
- Feld J.J., Lavoie E.G., Fausther M., Dranoff J.A. I drink for my liver, doc: Emerging evidence that coffee prevents cirrhosis. F1000Research. 2015;4:95. doi: 10.12688/f1000research.6368.2[↩]
- Arab L., Khan F., Lam H. Epidemiological evidence of a relationship between tea, coffee, or caffeine consumption and cognitive decline. Adv. Nutr. 2013;4:115–122. doi: 10.3945/an.112.002717[↩]
- Spriet L.L. Exercise and sports performance with low doses of caffeine. Sports Med. 2014;44:S175–S184. doi: 10.1007/s40279-014-0257-8[↩]
- Kim J., Lee J. A review of nutritional intervention on delayed onset muscle soreness. Part 1. J. Exerc. Rehabil. 2014;10:349–356. doi: 10.12965/jer.140179[↩]
- Nawrot P., Jordan S., Eastwood J., Rotstein J., Hugenholtz A., Feeley M. Effects of caffeine on human health. Food Addit. Contam. 2003;20:1–30. doi: 10.1080/0265203021000007840[↩]
- Caffeine in Food. https://www.canada.ca/en/health-canada/services/food-nutrition/food-safety/food-additives/caffeine-foods/foods.html[↩][↩][↩]
- Crippa A, Discacciati A, Larsson SC, Wolk A, Orsini N. Coffee consumption and mortality from all causes, cardiovascular disease and cancer: a dose-response meta-analysis. Am J Epidemiol 2014;180:763–5.[↩]
- Je Y, Giovannucci E. Coffee consumption and total mortality: a meta-analysis of twenty prospective cohort studies. Br J Nutr 2014;111:1162–73.[↩]
- Nawrot P, Jordan S, Eastwood J, Rotstein J, Hugenholtz A, Feeley M. Effects of caffeine on human health. Food Addit Contam 2003;20:1–30.[↩]
- Goldstein ER, Ziegenfuss T, Kalman D, Kreider R, Campbell B, Wilborn C, Taylor L, Willoughby D, Stout J, Graves BS. International society of sports nutrition position stand: caffeine and performance. J Int Soc Sports Nutr. 2010;7(1):5. doi: 10.1186/1550-2783-7-5[↩]
- Neuhäuser-Berthold M, Beine S, Verwied SC, Lührmann PM. Coffee consumption and total body water homeostasis as measured by fluid balance and bioelectrical impedance analysis. Ann Nutr Metab. 1997;41(1):29–36. doi: 10.1159/000177975[↩]
- Passmore A, Kondowe G, Johnston G. Renal and cardiovascular effects of caffeine: a dose–response study. Clin Sci. 1987;72(6):749–756. doi: 10.1042/cs0720749[↩]
- A G Dulloo, C A Geissler, T Horton, A Collins, D S Miller; Normal caffeine consumption: influence on thermogenesis and daily energy expenditure in lean and postobese human volunteers, The American Journal of Clinical Nutrition, Volume 49, Issue 1, 1 January 1989, Pages 44–50, https://doi.org/10.1093/ajcn/49.1.44[↩][↩][↩][↩]
- A Astrup, S Toubro, S Cannon, P Hein, L Breum, J Madsen; Caffeine: a double-blind, placebo-controlled study of its thermogenic, metabolic, and cardiovascular effects in healthy volunteers, The American Journal of Clinical Nutrition, Volume 51, Issue 5, 1 May 1990, Pages 759–767, https://doi.org/10.1093/ajcn/51.5.759[↩][↩]
- American Journal of Physiology-Endocrinology and Metabolism October 1995. Volume 269, Issue 4, Pages E671-E678 https://doi.org/10.1152/ajpendo.1995.269.4.E671[↩][↩][↩][↩]
- Thermogenic ingredients and body weight regulation. nternational Journal of Obesity volume 34, pages 659–669 (2010). https://www.nature.com/articles/ijo2009299[↩]
- Cornelis MC, El-Sohemy A, Campos H. Genetic polymorphism of the adenosine A2A receptor is associated with habitual caffeine consumption. Am J Clin Nutr 2007; 86: 240–244.[↩]
- Acheson KJ, Gremaud G, Meirim I, Montigon F, Krebs Y, Fay LB et al. Metabolic effects of caffeine in humans: lipid oxidation or futile cycling? Am J Clin Nutr 2004; 79: 40–46.[↩][↩][↩][↩][↩]
- Belza A, Frandsen E, Kondrup J. Body fat loss achieved by stimulation of thermogenesis by a combination of bioactive food ingredients: a placebo-controlled, double-blind 8-week intervention in obese subjects. Int J Obes (2005) 2007; 31: 121–130.[↩]
- Astrup A, Toubro S, Cannon S, Hein P, Breum L, Madsen J. Caffeine: a double-blind, placebo-controlled study of its thermogenic, metabolic, and cardiovascular effects in healthy volunteers. Am J Clin Nutr 1990; 51: 759–767.[↩][↩][↩][↩][↩]
- Kao YH, Hiipakka RA, Liao S. Modulation of obesity by a green tea catechin. Am J Clin Nutr 2000; 72: 1232–1234.[↩]
- Dulloo AG, Seydoux J, Girardier L, Chantre P, Vandermander J. Green tea and thermogenesis: interactions between catechin-polyphenols, caffeine and sympathetic activity. Int J Obes Relat Metab Disord 2000; 24: 252–258.[↩]
- Lowell BB, Spiegelman BM. Towards a molecular understanding of adaptive thermogenesis. Nature 2000; 404: 652–660.[↩][↩]
- Dulloo AG, Duret C, Rohrer D, Girardier L, Mensi N, Fathi M, Chantre P & Vendermander J. Efficacy of a green tea extract rich in catechin polyphenols and caffeine in increasing 24-hr energy expenditure and fat oxidation in humans. Am J Clin Nutr 1999; 70: 1040−1045. – https://www.ncbi.nlm.nih.gov/pubmed/10584049?dopt=Abstract&holding=npg[↩][↩][↩][↩][↩]
- Arciero PJ, Bougopoulos CL, Nindl BC & Benowitz NL. Influence of age on the thermic response to caffeine in women. Metabolism 2000; 49: 101−107. – http://www.metabolismjournal.com/article/S0026-0495(00)90888-6/pdf[↩]
- Astrup A & Toubro S. Thermogenic, metabolic, and cardiovascular responses to ephedrine and caffeine in man. Int J Obes Relat Metab Disord 1993; 17 Suppl 1: S41−S43. – https://www.ncbi.nlm.nih.gov/pubmed/8384179?dopt=Abstract&holding=npg[↩][↩][↩][↩]
- Bracco D, Ferrarra JM, Arnaud MJ Jequier E & Schutz Y. Effects of caffeine on energy metabolism, heart rate, and methylxanthine metabolism in lean and obese women. Am J Physiol 1995; 269: E671−E678. – https://www.ncbi.nlm.nih.gov/pubmed/7485480?dopt=Abstract&holding=npg[↩][↩][↩]
- Katzel LI, Bleecker ER, Colman EG, Rogus EM, Sorkin JD & Goldberg AP. Effects of weight loss vs aerobic exercise training on risk factors for coronary disease in healthy, obese, middle-aged and older men. JAMA 1995; 274: 1915−1921. – https://www.ncbi.nlm.nih.gov/pubmed/8568984?dopt=Abstract&holding=npg[↩]
- Caffeine Transiently Affects Food Intake at Breakfast. Journal of the Academy of Nutrition and Dietetics, Volume 0, Issue 0. https://jandonline.org/article/S2212-2672(18)30768-8/fulltext[↩]
- National Institutes of Health Office of Dietary Supplements – Dietary Supplements for Weight Loss Fact Sheet for Consumers – https://ods.od.nih.gov/pdf/factsheets/WeightLoss-Consumer.pdf[↩]
- Pasman WJ, Westerterp-Plantenga MS, Saris WH. The effectiveness of long-term supplementation of carbohydrate, chromium, fibre and caffeine on weight maintenance. Int J Obes Relat Metab Disord 1997; 21: 1143–1151.[↩][↩]
- Arciero PJ, Gardner AW, Calles-Escandon J, Benowitz NL, Poehlman ET. Effects of caffeine ingestion on NE kinetics, fat oxidation, and energy expenditure in younger and older men. Am J Physiol 1995; 268: E1192–E1198.[↩]
- Acheson KJ, Zahorska-Markiewicz B, Pittet P, Anantharaman K, Jequier E. Caffeine and coffee: their influence on metabolic rate and substrate utilization in normal weight and obese individuals. Am J Clin Nutr 1980; 33: 989–997.[↩]
- Dulloo AG, Geissler CA, Horton T, Collins A, Miller DS. Normal caffeine consumption: influence on thermogenesis and daily energy expenditure in lean and postobese human volunteers. Am J Clin Nutr 1989; 49: 44–50.[↩]
- Bracco D, Ferrarra JM, Arnaud MJ, Jequier E, Schutz Y. Effects of caffeine on energy metabolism, heart rate, and methylxanthine metabolism in lean and obese women. Am J Physiol 1995; 269: E671–E678.[↩][↩]
- Tremblay A, Masson E, Leduc S, Houde A, Despres JP. Caffeine reduces spontaneous energy intake in men but not in women. Nutr Res 1988; 8: 553–558.[↩]
- Dulloo AG, Duret C, Rohrer D, Girardier L, Mensi N, Fathi M et al. Efficacy of a green tea extract rich in catechin polyphenols and caffeine in increasing 24-h energy expenditure and fat oxidation in humans. Am J Clin Nutr 1999; 70: 1040–1045.[↩]
- Hollands MA, Arch JR, Cawthorne MA. A simple apparatus for comparative measurements of energy expenditure in human subjects: the thermic effect of caffeine. Am J Clin Nutr 1981; 34: 2291–2294.[↩]
- Rumpler W, Seale J, Clevidence B, Judd J, Wiley E, Yamamoto S et al. Oolong tea increases metabolic rate and fat oxidation in men. J Nutr 2001; 131: 2848–2852.[↩]
- Boschmann M, Thielecke F. The effects of epigallocatechin-3-gallate on thermogenesis and fat oxidation in obese men: a pilot study. J Am Coll Nutr 2007; 26: 389S–395S.[↩]
- Thermogenic ingredients and body weight regulation. International Journal of Obesity volume 34, pages 659–669 (2010). https://www.nature.com/articles/ijo2009299[↩]
- U.S. Food and Drug Administration – Pure Powdered Caffeine – https://www.fda.gov/food/dietarysupplements/productsingredients/ucm460095.htm[↩]
- FDA Voice December 16, 2014 – Tragic Deaths Highlight the Dangers of Powdered Pure Caffeine – https://blogs.fda.gov/fdavoice/index.php/2014/12/tragic-deaths-highlight-the-dangers-of-powdered-pure-caffeine/[↩]
- International Journal of Obesity (2005) 29, 1121–1129. doi:10.1038/sj.ijo.0802999 – Coffee, tea and diabetes: the role of weight loss and caffeine – http://www.nature.com/ijo/journal/v29/n9/full/0802999a.html[↩]
- Arciero PJ, Bougopoulos CL, Nindl BC & Benowitz NL. Influence of age on the thermic response to caffeine in women. Metabolism 2000; 49: 101−107. – https://www.ncbi.nlm.nih.gov/pubmed/10647072?dopt=Abstract&holding=npg[↩]
- Am J Clin Nutr. 1980 May;33(5):989-97.Caffeine and coffee: their influence on metabolic rate and substrate utilization in normal weight and obese individuals.- https://www.ncbi.nlm.nih.gov/pubmed/7369170[↩]
- Curatolo PW, Robertson D. The health consequences of caffeine. Ann Intern Med 1983; 98: 641–653.[↩]
- Robertson D, Frolich JC, Carr RK, Watson JT, Hollifield JW, Shand DG et al. Effects of caffeine on plasma renin activity, catecholamines and blood pressure. N Engl J Med 1978; 298: 181–186.[↩][↩]
- Robertson D, Wade D, Workman R, Woosley RL, Oates JA. Tolerance to the humoral and hemodynamic effects of caffeine in man. J Clin Invest 1981; 67: 1111–1117.[↩]


{kind=link}