What is the Waist Hip Ratio Measurement
Although waist circumference and body mass index (BMI) are interrelated, waist circumference provides an independent prediction of risk over and above that of BMI. Waist circumference measurement is particularly useful in patients who are categorized as normal or overweight on the BMI scale. At BMIs greater than or equal to 35, waist circumference has little added predictive power of disease risk beyond that of BMI. It is therefore not necessary to measure waist circumference in individuals with BMIs greater than or equal to 35 1. Given that your Body Mass Index measurement can be misleading if you have different body types and shapes, scientists and researchers have invented a more accurate measurement of your body fat distribution by measuring your waist circumference (WC) and waist-hip ratio. For example, Body Mass Index (BMI) does not take into account your age, gender or muscle mass. Nor does it distinguish between lean body mass and fat mass. As a result, some people, such as heavily muscled athletes, may have a high body mass index even though they don’t have a high percentage of body fat. In others, such as elderly people, BMI may appear normal even though muscle has been lost with aging. Take for example, basketball player Michael Jordan: When MJ was in his prime, his BMI was 27-29, classifying him as overweight, yet his waist size was less than 30. That’s one reason some experts think waist circumference can be a better overall health measurement than BMI.
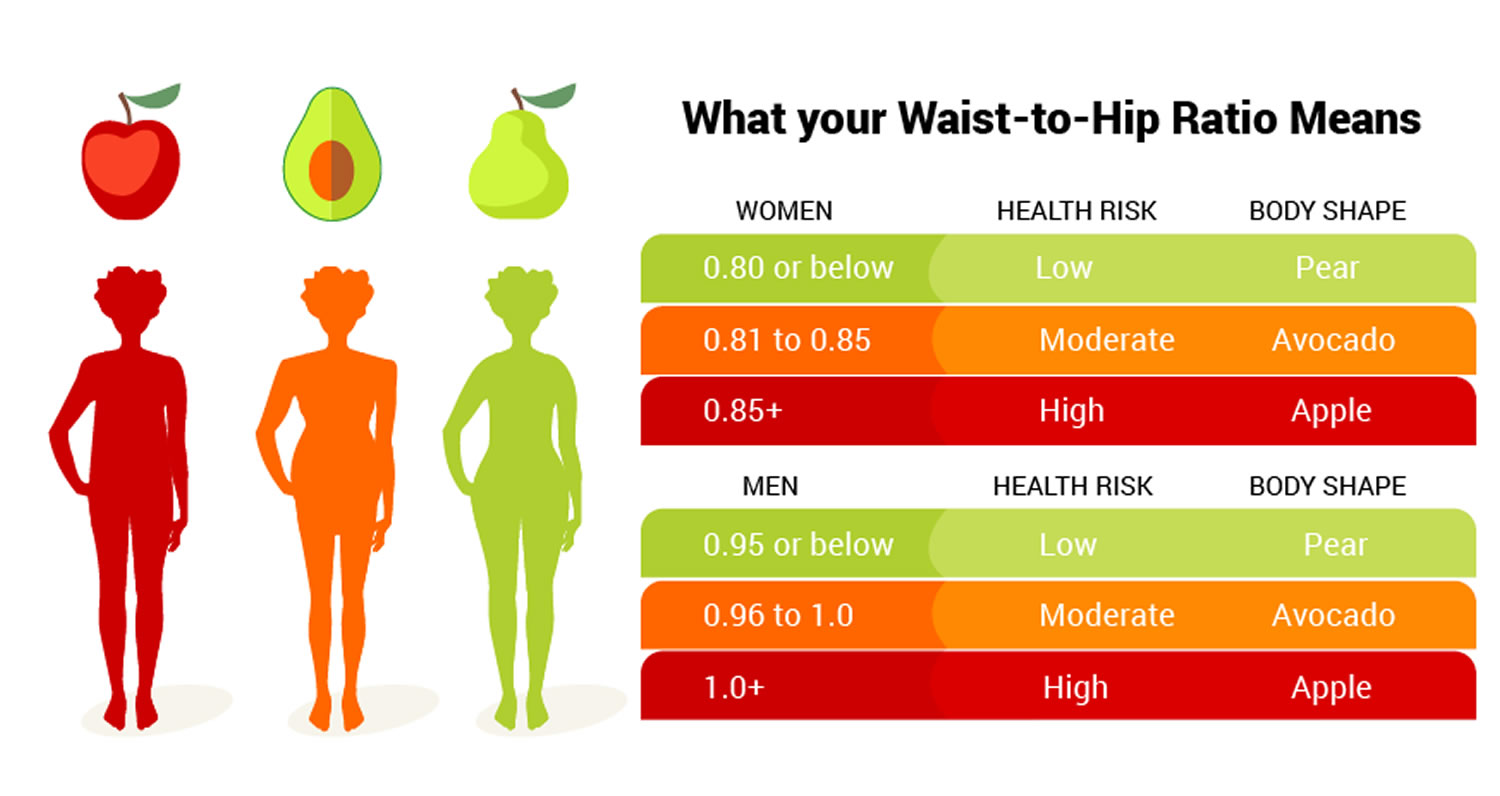
Another reason why waist-hip-ratio is important to your health is that your health is not only affected by excess body fat, but also by where the fat is located. Some people gain weight in their abdominal regions (the so-called ”apple” body shape.) Others are ”pear-shaped,” with excess weight around the hips and buttocks. The waist hip ratio has been used as an indicator or measure of health and the risk of developing serious health conditions. Research shows that people with “apple-shaped” bodies (with more weight around the waist) face more health risks associated with being overweight than those with “pear-shaped” bodies who carry more weight around the hips.
The Waist-Hip Ratio has been shown to be a better predictor of mortality and morbidity after certain surgery than body mass index (BMI) or body surface area. According to Mayo Clinic research in 2012, people who are of normal weight but have fat concentrated in their bellies have a higher death risk than those who are obese. The researchers found those who had a normal body mass index but central obesity — a high waist-to-hip ratio — had the highest cardiovascular death risk and the highest death risk from all causes. Other researchers have found that waist, waist-to-hip ratio, and BMI are similarly strong predictors of type 2 diabetes 2, 3.
A high waist circumference is associated with an increased risk for type 2 diabetes, dyslipidemia, hypertension, and coronary heart disease in patients with a BMI in a range between 25 and 34.9 kg/m2 4. Monitoring changes in waist circumference over time may be helpful, in addition to measuring BMI, since it can provide an estimate of increased abdominal fat even in the absence of a change in BMI. Furthermore, in obese patients with metabolic complications, changes in waist circumference are useful predictors of changes in CVD risk factors 5.
There are ethnic and age-related differences in body fat distribution that modify the predictive validity of waist circumference as a surrogate for abdominal fat 6. These variations may partly explain differences between ethnic or age groups in the power of waist circumference or waist-to-hip (WHR) ratio to predict disease risks 7, 8.
In some populations, waist circumference is a better indicator of relative disease risk than is BMI: examples include Asian Americans or persons of Asian descent living elsewhere 9, 10, 11. Waist circumference also assumes greater value for estimating risk for obesity-related disease at older ages. The table below incorporates both BMI and waist circumference in the classification of overweight and obesity, and provides an indication of disease risk.
| Disease Risk* Relative to Normal Weight and Waist Circumference
|
* Disease risk for type 2 diabetes, hypertension, and CVD.
+Increased waist circumference can also be a marker for increased risk even in persons of normal weight.
Central obesity is bad and people in this group (a high waist-to-hip ratio) has the highest death rate, even higher than those who are considered obese based on body mass index. From a public health perspective, this is a significant finding. Long-term follow-up studies showed that so-called “abdominal obesity” was strongly associated with an increased risk of type 2 diabetes, cardiovascular disease and death, even after controlling for body mass index (BMI) 12, 13.
The risk of cardiovascular death was 2.75 times higher, and the risk of death from all causes was 2.08 times higher than in people of normal weight with central obesity, compared with those with a normal body mass index and waist-to-hip ratio. The high risk of death may be related to a higher visceral fat accumulation (fat stored around important internal organs such as the liver, pancreas and intestines) in this group, which is associated with insulin resistance and other risk factors.
Waist Hip Ratio is used as a measurement of obesity, abdominal fat is a marker of visceral fat causing the high waist hip ratio, which in turn is a possible indicator of other more serious health conditions. The World Health Organization states that abdominal obesity is defined as a waist–hip ratio above 0.90 for males and above 0.85 for females, or a body mass index (BMI) above 30. The National Institute of Diabetes, Digestive and Kidney Diseases states that women with waist–hip ratios of more than 0.8, and men with more than 1.0, are at increased health risk because of their fat distribution.
Waist Hip Ratio is the ratio of the circumference of your waist to that of your hips. This is calculated as waist measurement divided by hip measurement (Waist ÷ Hips). For example, a person with a 25″ (64 cm) waist and 38″ (97 cm) hips has a waist–hip ratio of about 0.66.
If obesity is redefined using waist hip ratio instead of BMI, the proportion of people categorized as at risk of heart attack worldwide increases threefold. The body fat percentage is considered to be an even more accurate measure of relative weight. Of these three measurements, only the waist–hip ratio takes account of the differences in body structure. Hence, it is possible for two women to have vastly different body mass indices but the same waist–hip ratio, or to have the same body mass index but vastly different waist–hip ratios.
Waist hip ratio has been shown to be a better predictor of cardiovascular disease than waist circumference and body-mass index (BMI). However, other studies have found waist circumference, not waist hip ratio, to be a good indicator of cardiovascular risk factors, body fat distribution, and hypertension in type 2 diabetes.
Figure 1. How To Measure Waist Hip Ratio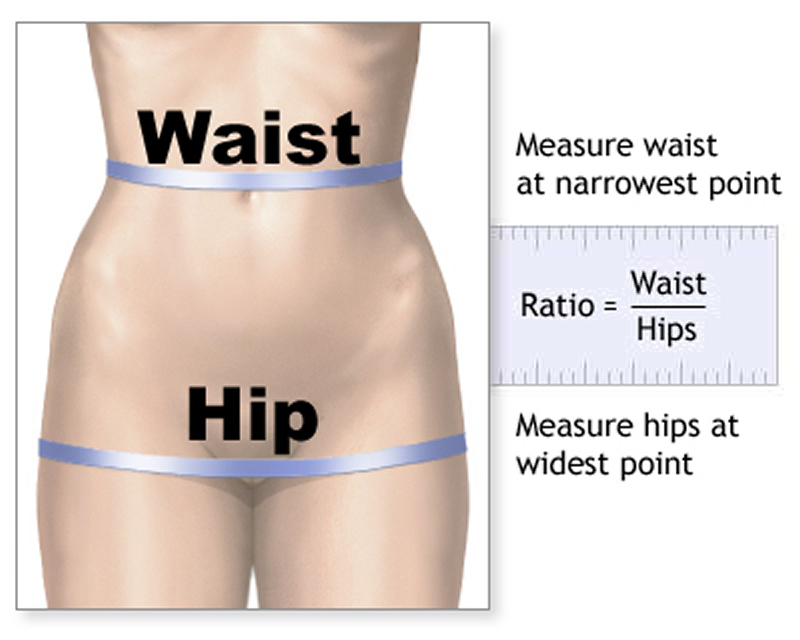
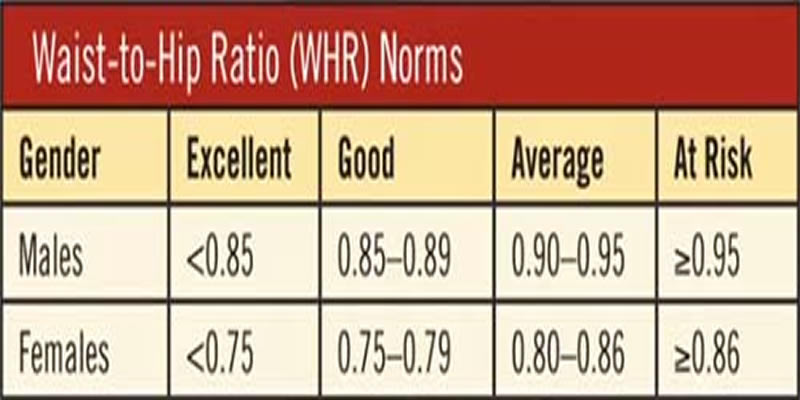
Figure 2. Waist Hip Ratio Chart
Abdominal obesity results in an “apple-shaped” body type, which is more common among men. Women typically accumulate fat around the hips and thighs to develop a “pear shaped” body type (although they can certainly develop “apple-shaped” body types as well).
- The two most common ways to measure abdominal obesity are waist circumference and waist size compared to hip size, also known as the waist-to-hip ratio. Several organizations have defined cut-points for abdominal obesity around one or both of these measurements, with different cut-points for men and women (see Figure 1 and 2).
In people who are not overweight, having a large waist may mean that they are at higher risk of health problems than someone with a trim waist.
- The Nurses’ Health Study, one of the largest and longest studies to date that has measured abdominal obesity, looked at the relationship between waist size and death from heart disease, cancer, or any cause in middle-aged women 14. At the start of the study, all 44,000 study volunteers were healthy, and all of them measured their waist size and hip size.
- After 16 years, women who had reported the highest waist sizes — 35 inches or higher –had nearly double the risk of dying from heart disease, compared to women who had reported the lowest waist sizes (less than 28 inches) 14.
- Women in the group with the largest waists had a similarly high risk of death from cancer or any cause, compared with women with the smallest waists. The risks increased steadily with every added inch around the waist 14.
The study found that even women at a “normal weight” BMI less than 25 were at a higher risk, if they were carrying more of that weight around their waist:
- Normal-weight women with a waist of 35 inches or higher had three times the risk of death from heart disease, compared to normal-weight women whose waists were smaller than 35 inches 14.
The Shanghai Women’s Health study found a similar relationship between abdominal fatness and risk of death from any cause in normal-weight women 15.
What is it about abdominal fat that makes it strong marker of disease risk ?
The fat surrounding the liver and other abdominal organs, so-called visceral fat, is very metabolically active. It releases fatty acids, inflammatory agents, and hormones that ultimately lead to higher LDL cholesterol, triglycerides, blood glucose, and blood pressure 16.
- National Heart, Lung and Blood Institute. According to Waist Circumference. https://www.nhlbi.nih.gov/health-pro/guidelines/current/obesity-guidelines/e_textbook/txgd/4142.htm[↩]
- Vazquez G, Duval S, Jacobs DR, Jr., Silventoinen K. Comparison of body mass index, waist circumference, and waist/hip ratio in predicting incident diabetes: a meta-analysis. Epidemiol.Rev. 2007;29:115-28. https://www.ncbi.nlm.nih.gov/pubmed/17494056[↩]
- Qiao Q, Nyamdorj R. Is the association of type II diabetes with waist circumference or waist-to-hip ratio stronger than that with body mass index? Eur J Clin Nutr. 2009. https://www.ncbi.nlm.nih.gov/pubmed/19724291[↩]
- Chan JM, Rimm EB, Colditz GA,Stampfer MJ, Willett WC. Obesity, fat distribution, and weight gain as risk factors for clinical diabetes in men. Diabetes Care. 1994;17:961-969.[↩]
- Lemieux S, Prud’homme D, Bouchard C, Tremblay A, Despres J. A single threshold value of waist girth identifies normal-weight and overweight subjects with excess visceral adipose tissue. Am J Clin Nutr. 1996;64:685-693.[↩]
- Gallagher D, Visser M, Sepulveda D, Pierson RN, Harris T, Heymsfield SB. How useful is body mass index for comparison of body fatness across age, sex, and ethnic groups? Am J Epidemiol. 1996;143:228-239.[↩]
- Dowling HJ, Pi-Sunyer FX. Race-dependent health risks of upper body obesity. Diabetes. 1993;42:537-543.[↩]
- Conway JM, Yanovski SZ, Avila NA, Hubbard VS. Visceral adipose tissue differences in black and white women. Am J Clin Nutr. 1995;61:765-771.[↩]
- Klatsky AL, Armstrong MA. Cardiovascular risk factors among Asian Americans living in northern California. Am J Public Health. 1991;81:1423-1428.[↩]
- Fujimoto WY, Newell-Morris LL, Grote M, Bergstrom RW, Shuman WP. Visceral fat obesity and morbidity: NIDDM and atherogenic risk in Japanese-American men and women. Int J Obes. 1991;15 (Suppl2):41-44.[↩]
- Potts J, Simmons D. Sex and ethnic group differences in fat distribution in young United Kingdom South Asians and Europids. J Clin Epidemiol. 1994;47:837-841.[↩]
- Ohlson LO, Larsson B, Svardsudd K, et al. The influence of body fat distribution on the incidence of diabetes mellitus. 13.5 years of follow-up of the participants in the study of men born in 1913. Diabetes. 1985;34:1055-8. http://diabetes.diabetesjournals.org/content/34/10/1055.long[↩]
- Larsson B, Svardsudd K, Welin L, Wilhelmsen L, Bjorntorp P, Tibblin G. Abdominal adipose tissue distribution, obesity, and risk of cardiovascular disease and death: 13 year follow up of participants in the study of men born in 1913. Br Med J (Clin Res Ed). 1984;288:1401-4. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1441047/pdf/bmjcred00500-0007.pdf[↩]
- Zhang C, Rexrode KM, van Dam RM, Li TY, Hu FB. Abdominal obesity and the risk of all-cause, cardiovascular, and cancer mortality: sixteen years of follow-up in US women. Circulation. 2008;117:1658-67. http://circ.ahajournals.org/content/117/13/1658.long[↩][↩][↩][↩]
- Zhang X, Shu XO, Yang G, et al. Abdominal adiposity and mortality in Chinese women. Arch Intern Med. 2007;167:886-92. http://jamanetwork.com/journals/jamainternalmedicine/fullarticle/412396[↩]
- Despres JP. Health consequences of visceral obesity. Ann Med. 2001;33:534-41. https://www.ncbi.nlm.nih.gov/pubmed/11730160[↩]


{kind=link}