
Contents
- What is acne
What is acne
Acne, pimples or zits, is a chronic inflammatory disorder of pilosebaceous (sebaceous gland a small gland in the skin which secretes a lubricating oily matter called sebum into the hair follicles to lubricate the skin and hair) units of the skin. Acne nearly always affects the face (99%), but can also affect the back (60%) and chest (15%) 1. Acne is among the most common dermatological conditions seen and acne is estimated to affect 85 to 90% of adolescents 2. Individuals of all ages can have acne, but most cases develop in adolescence 3. Acne is considered a chronic disease with up to 50% of cases persisting into adulthood 4. Acne’s impact on psychological, social, and emotional wellbeing can be devastating, and can be worse than that reported by patients with chronic asthma, epilepsy, back pain, or arthritis 5. Early and aggressive treatment is important to prevent scarring and help improve quality of life. Maintenance therapy is recommended for optimal outcomes. Treatment should target as many factors as possible in order to prevent the formation of microcomedones and prevent scarring and post-inflammatory hyperpigmentation 1.
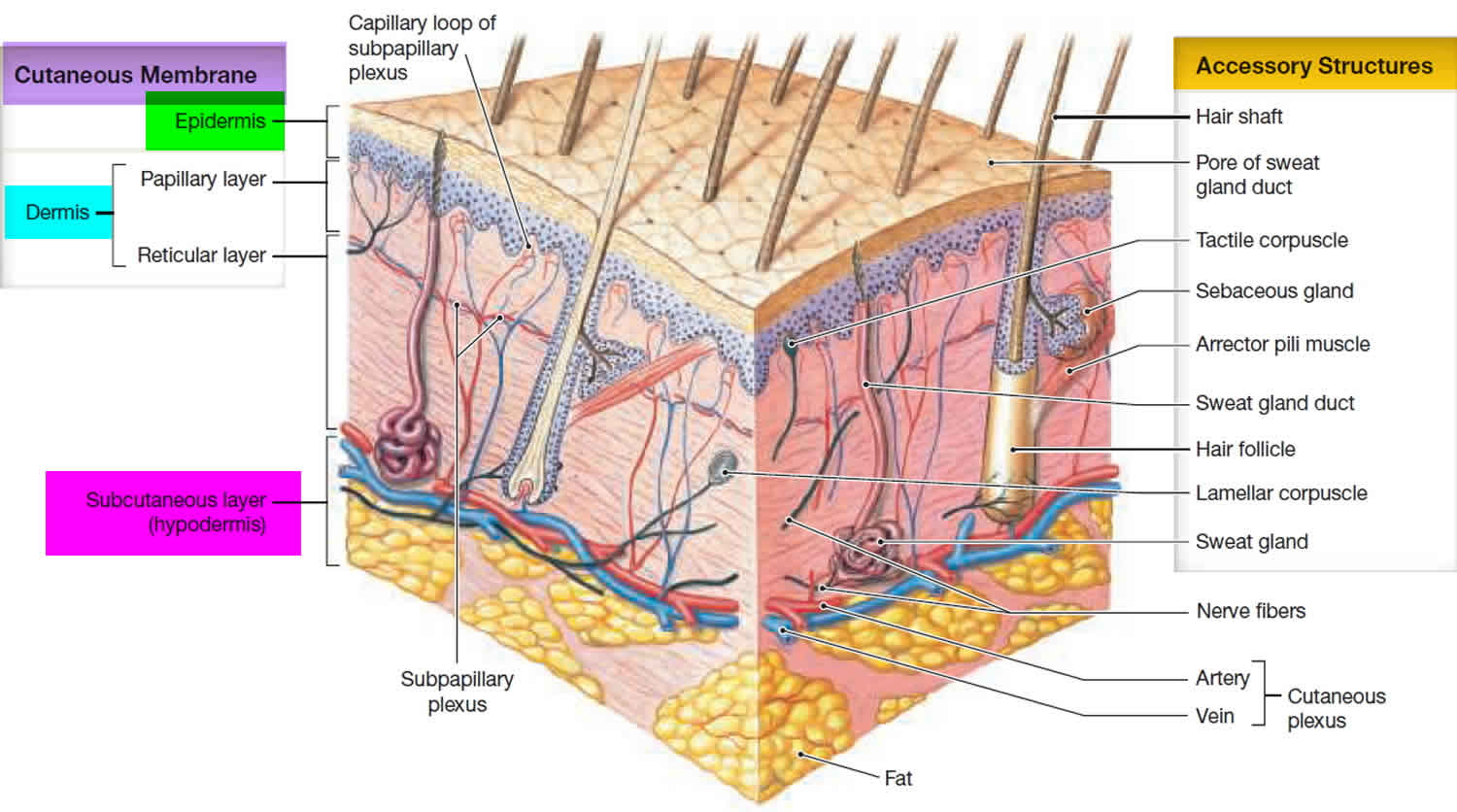
Figure 1. Skin anatomy
What causes acne?
The causes of acne is due to a combination of factors. However, the exact mechanisms are not fully understood. The most notable pathophysiologic factors that influence its development of acne are:
- Familial tendency
- Endogenous and exogenous androgenic hormones
- Acne bacteria, Cutibacterium acnes (previously called Proprionibacterium acnes) (a part of the normal human skin gram-positive bacteria that prefers anaerobic growth conditions and is involved in the pathogenesis of acne) colonization of the hair follicle,
- Innate immune activation with inflammatory mediators
- Distension and occlusion of the hair follicles
- Hyperkeratinization (increased scaling of the skin)
- Increased sebum production
- Inflammation
Studies have also suggested that genetic, hormonal, and dietary factors may also have a role.
Flares of acne can be provoked by:
- Polycystic ovarian disease (PCOS)
- Drugs: steroids, hormones, anticonvulsants, epidermal growth factor receptor inhibitors and others
- Application of occlusive cosmetics
- High environmental humidity
- Diet high in dairy products and high glycemic foods
What are high glycemic foods?
Carbohydrate is an essential part of our diets, but not all carbohydrate foods are equal. The glycemic index (GI) was first developed by Jenkins and colleagues 6 and the Glycemic Index (GI) is a relative ranking of carbohydrate in foods according to how they affect blood glucose levels 7. Carbohydrates with a low glycemic index (GI) value (55 or less) are more slowly digested, absorbed and metabolized and cause a lower and slower rise in blood glucose and, therefore usually, insulin levels.
Research shows that both the amount and the type of carbohydrate in food affect blood glucose levels. Studies also show that the total amount of carbohydrate in food, in general, is a stronger predictor of blood glucose response than the glycemic index (GI).
The glycemic index or GI ranks carbohydrates according to their effect on blood glucose levels. The lower the glycemic index (GI), the slower the rise in blood glucose levels will be when the food is consumed. The effect may differ from person to person.
Meats and fats don’t have a GI because they do not contain carbohydrate.
Some research has shown that by eating a diet with a lower GI, people with diabetes can reduce their average blood glucose levels. This is important in reducing the risk of developing diabetes-related complications.
The GI index runs from 0–100 and usually uses glucose, which has a GI of 100, as the reference. Slowly absorbed carbohydrates have a low GI rating (55 or below), and include most fruits and vegetables, milk, some wholegrain cereals and bread, pulses and basmati rice. GI numbers are to be used as a guide only as individual foods do not have the same response in all people with diabetes.
- Low GI foods are foods with a GI less than 55.
- Intermediate GI foods are foods with a GI between 55 and 70.
- High GI foods are foods with a GI greater than 70.
Below are examples of foods based on their GI.
Low GI Foods (55 or less)
- 100% stone-ground whole wheat or pumpernickel bread
- Oatmeal (rolled or steel-cut), oat bran, muesli
- Pasta, converted rice, barley, bulgar
- Sweet potato, corn, yam, lima/butter beans, peas, legumes and lentils
- Most fruits, non-starchy vegetables and carrots
Not all low-GI foods are healthy choices – chocolate, for example, has a low-GI because of its fat content, which slows down the absorption of carbohydrate.
Medium GI (56-69)
- Whole wheat, rye and pita bread
- Quick oats
- Brown, wild or basmati rice, couscous
High GI (70 or more)
- White bread or bagel
- Corn flakes, puffed rice, bran flakes, instant oatmeal
- Shortgrain white rice, rice pasta, macaroni and cheese from mix
- Russet potato, pumpkin
- Pretzels, rice cakes, popcorn, saltine crackers
- melons and pineapple
Table 1. The average GI of 62 common foods derived from multiple studies by different laboratories 8
| High-carbohydrate foods | Breakfast cereals | Fruit and fruit products | Vegetables | ||||
|---|---|---|---|---|---|---|---|
| White wheat bread* | 75 ± 2 | Cornflakes | 81 ± 6 | Apple, raw† | 36 ± 2 | Potato, boiled | 78 ± 4 |
| Whole wheat/whole meal bread | 74 ± 2 | Wheat flake biscuits | 69 ± 2 | Orange, raw† | 43 ± 3 | Potato, instant mash | 87 ± 3 |
| Specialty grain bread | 53 ± 2 | Porridge, rolled oats | 55 ± 2 | Banana, raw† | 51 ± 3 | Potato, french fries | 63 ± 5 |
| Unleavened wheat bread | 70 ± 5 | Instant oat porridge | 79 ± 3 | Pineapple, raw | 59 ± 8 | Carrots, boiled | 39 ± 4 |
| Wheat roti | 62 ± 3 | Rice porridge/congee | 78 ± 9 | Mango, raw† | 51 ± 5 | Sweet potato, boiled | 63 ± 6 |
| Chapatti | 52 ± 4 | Millet porridge | 67 ± 5 | Watermelon, raw | 76 ± 4 | Pumpkin, boiled | 64 ± 7 |
| Corn tortilla | 46 ± 4 | Muesli | 57 ± 2 | Dates, raw | 42 ± 4 | Plantain/green banana | 55 ± 6 |
| White rice, boiled* | 73 ± 4 | Peaches, canned† | 43 ± 5 | Taro, boiled | 53 ± 2 | ||
| Brown rice, boiled | 68 ± 4 | Strawberry jam/jelly | 49 ± 3 | Vegetable soup | 48 ± 5 | ||
| Barley | 28 ± 2 | Apple juice | 41 ± 2 | ||||
| Sweet corn | 52 ± 5 | Orange juice | 50 ± 2 | ||||
| Spaghetti, white | 49 ± 2 | ||||||
| Spaghetti, whole meal | 48 ± 5 | ||||||
| Rice noodles† | 53 ± 7 | ||||||
| Udon noodles | 55 ± 7 | ||||||
| Couscous† | 65 ± 4 |
| Dairy products and alternatives | Legumes | Snack products | Sugars | ||||
|---|---|---|---|---|---|---|---|
| Milk, full fat | 39 ± 3 | Chickpeas | 28 ± 9 | Chocolate | 40 ± 3 | Fructose | 15 ± 4 |
| Milk, skim | 37 ± 4 | Kidney beans | 24 ± 4 | Popcorn | 65 ± 5 | Sucrose | 65 ± 4 |
| Ice cream | 51 ± 3 | Lentils | 32 ± 5 | Potato crisps | 56 ± 3 | Glucose | 103 ± 3 |
| Yogurt, fruit | 41 ± 2 | Soya beans | 16 ± 1 | Soft drink/soda | 59 ± 3 | Honey | 61 ± 3 |
| Soy milk | 34 ± 4 | Rice crackers/crisps | 87 ± 2 | ||||
| Rice milk | 86 ± 7 |
Note: The GI should not be used in isolation; the energy density and macronutrient profile of foods should also be considered 9.
Fat and fiber tend to lower the GI of a food. As a general rule, the more cooked or processed a food, the higher the GI; however, this is not always true.
Below are a few specific examples of other factors that can affect the GI of a food 10:
- The type of starch present.
- The type of sugar present – fructose (fruit sugar) and lactose (milk sugar) both have a lower GI than sucrose (table sugar).
- Ripeness and storage time — the more ripe a fruit or vegetable is, the higher the GI.
- Processing — juice has a higher GI than whole fruit; mashed potato has a higher GI than a whole baked potato, stone ground whole wheat bread has a lower GI than whole wheat bread.
- Cooking methods — how long a food is cooked (al dente pasta has a lower GI than soft-cooked pasta), frying, boiling and baking. Cooking and processing food will usually increase the GI as there is less work required by the body to break the carbohydrates down.
- Fibre: wholegrains and high-fibre foods act as a physical barrier that slows down the absorption of carbohydrate. This is not the same as ‘wholemeal’, where, even though the whole of the grain is included, it has been ground up instead of left whole. For example, some mixed grain breads that include wholegrains have a lower GI than wholemeal or white bread.
- Fat lowers the GI of a food. For example, chocolate has a medium GI because of it’s fat content, and crisps will actually have a lower GI than potatoes cooked without fat.
- Protein lowers the GI of food. Milk and other diary products have a low GI because they are high in protein and contain fat.
- Adding acidity to the food will lower the GI (e.g. adding lemon juice).
- Variety — converted long-grain white rice has a lower GI than brown rice but short-grain white rice has a higher GI than brown rice.
Low-GI foods in your healthy, balanced diet
It’s easy to include low-GI carbs in everyday meals:
- Choose basmati or easy cook rice, pasta or noodles. Or, try plantain, quinoa or bulgur wheat for a change.
- Eat wholemeal roti and include dhal in your meals.
- Use new potatoes instead of old potatoes – try sweet potatoes for a change.
- Instead of white and wholemeal bread, choose granary, pumpernickel or rye bread.
- Swap frozen chips for pasta or noodles.
- Try porridge, natural muesli or wholegrain breakfast cereals.
Fruits
Most fruits have a low glycemic index (GI) because of their fructose and fiber content. Melons and pineapple have medium GI values as do some dried fruits such as dates, raisins, and sweetened cranberries.
Fruit – all types such as apples, oranges, peaches, bananas, melons. Fruit is a good source of fiber; try to eat the whole fruit rather than drinking the juice. Include at least 2 serves of fruit a day (1 serve = 1 medium piece apple, orange or pear OR 2 small kiwifruit or plums).
Suitable food if you have acne
Some people with acne have reported improvement in their skin when they follow a low-glycemic index diet and increase their consumption of whole grains, fresh fruits and vegetables, fish, olive oil, garlic, while keeping their wine consumption moderate.
It’s a good idea to drink less milk and eat less of high glycemic index foods such as sugar, biscuits, cakes, ice creams and bottled drinks. Reducing your intake of meat and amino acid supplements may also help.
Seek medical help if you are concerned about your skin, as changing diet does not always help.
Do certain foods cause acne?
Some studies suggest there is a link between the food you eat and acne. It is very difficult to study the role of diet and acne.
Acne is reported to be less common in people that have a diet with lower glycemic index (GI), e.g., natives from Kitava and Papua New Guinea, the Ache people of Paraguay, Inuits and rural residents of Kenya, Zambia and Bantu. These people tend to become sexually mature at a later age than in the cities where higher glycemic index foods are consumed. Early puberty is associated with earlier onset and more severe acne that tends to peak at the time of full maturity (age 16 to 18).
Several studies, criticized for their quality, have shown benefits in acne from a low-glycemic (low GI), low-protein, low-fat and low-dairy diet. The reasons for these benefits are thought to relate to the effects of these foods on insulin and insulin-like growth factor-1 (IGF-1).
Insulin induces male hormones (androgens), glucocorticoids and growth factors. These provoke keratinization (scaling) of the hair follicle and sebum production. An increase in sebum production and keratinisation is a factor in the appearance of acne.
Foods that increase insulin production
Foods that increase insulin levels have a high glycemic index (high GI). The glycaemic index is a measurement of how carbohydrates have an effect on your blood sugar levels. When you eat foods with a high glycemic index (high GI), such as white bread and baked goods, your blood sugar level rises. This increases the amount of insulin produced in your body.
Although cow’s milk has a low glycemic index, it contains androgens, estrogen, progesterone and glucocorticoids, which also provoke keratinization and sebum (skin oil) production. Milk also contains amino acids (e.g., arginine, leucine, and phenylalanine) that produce insulin when combined with carbohydrates. Other components of milk that might induce comedones include whey proteins and iodine.
Caffeine, theobromine, and serotonin found in chocolate may also increase insulin production.
Food containing fatty acids
Fatty acids are needed to form sebum. Studies show that some monounsaturated fatty-acids, such as sapienic acid and some vegetable oils, can increase sebum production. However, the essential fatty acids linoleic, linolenic and gamma linolenic acid can unblock the follicles and reduce sebum production.
Why is acne often most severe during teenage years?
The precise reasons that acne is most severe during the teenage years are being studied. There are several theories.
There are higher levels of sex hormones after puberty than in younger children.
- Sex hormones are converted in the skin to dihydrotestosterone (DHT), which stimulates sebaceous (oil) glands at the base of hair follicles to enlarge.
- The sebaceous glands produce sebum. Changes in sebum composition may lead to acne lesions.
- The activated sebaceous gland cells (sebocytes) also produce proinflammatory factors, including lipid peroxides, cytokines, peptidases and neuropeptides.
- Hair follicles are tiny canals that open into skin pores (tiny holes) on the skin surface. The follicles normally carry sebum and keratin (scale) from dead skin cells to the surface. Inflammation and debris leads to blockage of the skin pores – forming comedones.
- The wall of the hair follicle may then rupture, increasing an inflammatory response.
- Bacteria within the hair follicle may enhance inflammatory lesions.
While acne is most common in adolescents, acne can affect people of all ages and all races. It usually becomes less of a problem after the age of 25 years, although about 15% of women and 5% of men continue to have acne as adults. It may also start in adult life.
Why is acne worse in some people?
Some people have particularly severe acne. This may be because of:
- Genetic factors (family members have bad acne)
- Hormonal factors (higher levels of male/androgenic hormones) due to:
- Polycystic ovaries (common). Hyperinsulinaemia and insulin resistance are characteristically found in women with polycystic ovarian syndrome (PCOS), who are prone to acne among other problems
- Psychological stress and depression
- Excessive corticosteroids eg Cushing disease (rare)
- Enzyme deficiency e.g., sterol hydroxylase deficiency (very rare)
- Environmental factors such as:
- High humidity causing swelling of the skin
- Cosmetics especially certain moisturisers, foundation and pomades. Watch out for products that contain lanolin, petrolatum, vegetable oils, butyl stearate, lauryl alcohol and oleic acid.
- Pressure from headbands and chin straps (e.g., “fiddler’s neck”, a condition seen in violin or viola players, where continual pressure from the violin against the neck causes skin irritation)
- Excessive dairy products, meat protein and sugars in the diet. Diets low in zinc or high in iodine can worsen pustular acne.
- Certain medications may provoke acne.
- Much of the individual variation in acne severity is due to variation in the innate immune system and the production of inflammatory mediators such as cytokines, defensins, peptidases, sebum lipids, and neuropeptides. Evidence has emerged that inflammation leads to distension and occlusion of the hair follicle, which then ruptures.
Why does acne eventually clear up?
Scientists do not understand why acne eventually clears up. Acne going away does not always coincide with a reduction in sebum production or with a reduction in the number of bacteria. It may relate to changes in the sebaceous glands themselves or to the activity of your immune system.
Acne Lesions
- Microcomedones are microscopic plugged follicular openings that are not visible to the naked eye. They are the precursors for all acne lesions.
- Noninflammatory lesions include:
- Closed comedones (whiteheads) are small, skin-colored papules that lack an obvious follicular opening.
- Open comedones (blackheads) have a dilated follicular opening filled with a keratin plug, which has a black color due to oxidized lipids and melanin.
- Inflammatory lesions include:
- Erythematous (red) papules and pustules.
- Nodules and cysts, which may contain pus or serosanguinous fluid.
- Inflammation has been demonstrated to some degree, in all acne lesions.
- Inflammation localized to the pilosebaceous unit can be considered the defining feature of acne and should be addressed via multiple therapeutic pathways 11.
Acne Clinical Severity and Treatments
Acne is commonly described as mild, moderate or severe. A descriptive scale, known as the Physician’s Global Assessment, is also used to categorize acne 12. The determination depend on types, severity, and number of lesions.
Figure 2. Acne severity grades

Grade 1 (Comedonal) Acne:
- Grade 1 acne consists of only comedones (blackheads and whiteheads). No inflammation (i.e. no pimples or pustules) is present.
The best topical treatment options are retinoids or fixed-dose combination as per guidelines.
- Retinoids:
- Tretinoin – 0.025%, 0.05%, 0.1% cream or gel
Tretinoin gel microsphere – 0.04% gel or 0.1% gel
Adapalene – 0.1% or 0.3% gel, 0.1% cream
Tazarotene – 0.1% cream or gel
- Tretinoin – 0.025%, 0.05%, 0.1% cream or gel
- Fixed-dose combinations:
- Clindamycin 1%/ benzoyl peroxide 5%
- Clindamycin 1.2% / Tretinoin 0.025%
- Adapalene 0.1% / benzoyl peroxide 2.5% gel pump
- Adapalene 0.3% / benzoyl peroxide 2.5% gel pump
- Erythromycin 3% / benzoyl peroxide 5%
Grade 2 (Inflammatory) Acne
- Grade 2 acne presents with inflammatory papules (pimples) with or without comedones.
The best topical treatment options include:
- Clindamycin 1.2% / Tretinoin 0.025%
- Clindamycin 1% / benzoyl peroxide 5% gel pump
- Adapalene 0.1% / benzoyl peroxide 2.5% gel pump
- Adapalene 0.3% / benzoyl peroxide 2.5% gel pump
Grade 3 (Inflammatory) Acne
- Grade 3 acne presents with more intense or widespread inflammatory papules (pimples) as well as pustules. Comedones may or may not be involved.
The best topical treatment options include the following:
- Clindamycin 1.2% / Tretinoin 0.025%
- Clindamycin 1% / benzoyl peroxide 5% gel pump
- Adapalene 0.1% / benzoyl peroxide 2.5% gel pump
- Adapalene 0.3% / benzoyl peroxide 2.5% gel pump
- An oral antibiotic such as doxycyline, minocycline, tetracycline, trimethoprim-sulfamethoxazole, or erythromycin can be used in combination with benzoyl peroxide.
Grade 4 (Nodulocystic) Acne
Grade 4 acne presents with nodules and/or cysts; inflammatory papules (pimples), pustules. Comedones and textural scarring may or may not be involved.
The best treatment options include the following:
- Oral isotretinoin
- Systemic antibiotics in combination with topical benzoyl peroxide, with or without a topical retinoid for patients unwilling or unable to use oral isotretinoin and those with intolerance 13.
Hormonal Acne
- Hormonal acne is typically seen in females on the lower face (cheeks, chin, jawline), submental region and presents with monomorphic inflammatory papules and cysts that are deep-seated and tender.
The best topical treatment options include:
- Dapsone 5% gel or Clindamycin 1%/benzoyl peroxide 5% gel pump
- WITH an oral anti-hormonal medication such as an oral contraceptive or spironolactone.
Perioral Dermatitis
- Perioral dermatitis is typically seen in females. It presents around the mouth, nose and/or eyes with acneiform or eczematous papules that are superficial and deep.
The best topical treatment options include:
- Pimecrolimus 1% cream
- Tacrolimus 0.1% ointment
- WITH oral antibiotic such as doxycyline, minocycline, tetracycline, trimethoprim-sulfamethoxazole, or erythromycin and or in combination with benzoyl peroxide.
Does chocolate give you acne
Some evidence is beginning to show that chocolate might increase acne symptoms, but it is too soon to say for sure.
The role of chocolate in acne has been controversial for decades. Chocolate is typically made with milk, cocoa butter, and sugar, all of which might hypothetically increase acne lesions. However, the science is still not complete in any of these areas.
On the flip side, chocolate contains flavonoids, and this might hypothetically help decrease the severity of acne.
The best way to determine whether chocolate affects acne is to look at the scientific studies. One initial and flawed study in 1969 found no connection, and the conclusion that no connection existed continued until 2011, when research resumed and several newer studies began finding a weak connection.
Let’s start by looking at the initial 1969 study that got the whole world saying chocolate does not affect acne, and why you should not give as much credibility to its findings.
The first study on chocolate and acne, published in 1969 14, the study included 35 young adult male prisoner volunteers in addition to 30 male and female adolescents. The participants were given either a chocolate bar or a placebo bar. The placebo bar was a bar that looked and tasted like chocolate but contained no chocolate. At the end of the study 14, the researchers concluded that chocolate had no effect on acne severity and despite several serious design flaws 15 in the study, this was generally accepted as fact for decades.
A closer inspection of the 1969 study’s design and methods discovered many worrying limitations, including:
- Differences in gender composition between the group that received the chocolate bar and the group that received the placebo bar.
- Excluding the age of participants. Neither the “young adult male prisoners” nor the “adolescent boys and girls” mean age was stated.
- Variations in menstrual cycle, weight, stress, lifestyle, and the use of caffeine, tobacco, or medications amongst participants, all of which may affect acne severity, were not mentioned.
- Differences in composition of the chocolate bars and the placebo bars. The placebo bars contained more hydrogenated fats.
- The short duration of the study (4 weeks).
- Not including a description of the statistical methods.
- A conflict of interest. The study was sponsored by the Chocolate Manufacturers Association of the USA 15.
Due to the design flaws of the study, it was concluded that its conclusion that chocolate did not affect acne was unreliable.
After almost 50 years of no further research, interest in the potential effects of chocolate and acne resumed in earnest in 2011. However, as you read, remember that studying the effect of diet on any disease is difficult, and so conclusions are still tentative.
In 2011, a study published in the Journal of the American Academy of Dermatology 16 found that 100% chocolate increased the number of acne lesions in a group of 10 men between the ages of 18 and 35.
However, this study 16 also had limitations, including:
- No control group.
- Small sample size (only 10 people)
- Exclusion of females.
- Limited follow-up time.
- Variables such as diet (sugar and calorie intake), weight, or smoking status, all of which may influence the development of acne, were not mentioned 16.
Since then researchers have performed 5 more studies, with all of them demonstrating a weak relationship between chocolate consumption and an increase in acne.
In 2014, another study 17 was performed that expanded on the 2011 study. Thirteen male subjects with mild acne took either capsules filled with 100% cocoa, capsules filled with only hydrolyzed gelatin (placebo), or a combination of both. The results showed an increase in acne on day 4 and day 7. The authors concluded that there was a correlation between the consumption of chocolate and an increase in acne lesions observed during their study 17.
However, there were considerable limitations to this study, including:
- Small sample size (only 13 people).
- Exclusion of females.
- Variables such as he amount of dairy or sugar consumed, were not mentioned 17.
- Very short one-week study.
- Acne lesions can take 2-6 weeks to form.
- Therefore, it is unclear whether other factors or the consumption of chocolate played a role in the results observed.
In 2015 18, a survey of 2,266 French adolescents and young adults, of which 1,375 participants had acne and 891 participants had no acne, found that the consumption of chocolate and sweets was associated with participants who reported having acne.
However, once again, this study had limitations, including:
- Variables such as sugar, milk, and chocolate were not separately investigated.
- Self-reported data.
- The study relied on survey answers from participants, which is not the most robust method of gathering data 18.
In 2016 19, a study of 25 men from ages 18 to 30 years old found that 99% dark chocolate increased existing acne. After a 4-week period of abstaining from any food containing chocolate, the researchers asked participants to consume 25 grams of 99% dark chocolate daily for an additional 4 weeks. The study 19 stated that the participants’ diets did not change significantly throughout the study period, and concluded that the dark chocolate caused the increase in acne.
However, limitations to the study included:
- No placebo group.
- A small sample size (only 25 people).
- The exclusion of females.
- Lifestyle variables such as the participants’ consumption of alcohol, dairy, and sugar, were not controlled during the study.
In 2016, a study 20 found that the consumption of milk chocolate appeared to increase acne lesions among 54 college students with an average age of 21.4 years. In this study, 54 students were divided into two groups. One group was given a 1.55-ounce Hershey’s milk chocolate bar, and the other group was given 15 Jelly Belly jellybeans. Both types of candy had the same glycemic load. Neither group was allowed to eat chocolate other than the chocolate provided during the study.
Researchers assessed the number of acne lesions 48 hours after participants ate the candy. Then, four weeks after the first trial, the type of candy each group consumed was switched, and acne lesions were again assessed 48 hours later.
In both trials, the researchers observed an increase in acne lesions among participants consuming milk chocolate compared to those consuming jellybeans 20.
However, as with all of the other studies, there were several limitations to this study, including:
- A small sample size (only 54 people).
- The variable of dairy, which is present in milk chocolate, was not controlled for. Some weak evidence shows may aggravate acne, and researchers did not take dairy under consideration.
- Extremely short study. Since acne can take 2 to 6 weeks to form, observing acne formation after 48 hours may not be enough time to determine whether chocolate caused the observed increases 19.
Overall, all of these more recent studies also had their own limitations, so it is still too soon to say for sure whether chocolate increases acne.
All things in moderation: Eliminating chocolate from the diet is unlikely to result in a noticeable decrease in acne. It is likely safe to enjoy the occasional chocolate treat based on the evidence we currently have, but it may be best not to overdo it. All things in moderation.
Summary
Research on the effects of chocolate on acne is conflicting. While the bulk of studies since 2011 show a correlation between chocolate consumption and acne, all of these studies have limitations, and other studies on the components of acne have shown that some components of chocolate may increase acne, while others may decrease it, or have no effect. Until more research is done, we cannot say for certain what effect reducing or eliminating your chocolate intake will have on your acne. In the meantime, a proper treatment regimen can greatly improve the health of your skin and reduce acne lesions.
- Nast A et al. J Eur Acad Dermatol Venereol. 2016 Aug;30(8):1261-8.[↩][↩]
- Lynde C et al. J Cutan Med Surg. 2014 Jul-Aug;18(4):243-55.[↩]
- James WD. N Engl J Med. 2005 Apr 7;352(14):1463-72.[↩]
- Thiboutot D et al. J Am Acad Dermatol. 2009 May;60(5 Suppl):S1-50.[↩]
- Mallon E et al. Br J Dermatol. 1999 Apr;140(4):672-6.[↩]
- Glycemic index of foods: a physiological basis for carbohydrate exchange. Jenkins DJ, Wolever TM, Taylor RH, Barker H, Fielden H, Baldwin JM, Bowling AC, Newman HC, Jenkins AL, Goff DV. Am J Clin Nutr. 1981 Mar; 34(3):362-6. https://www.ncbi.nlm.nih.gov/pubmed/6259925/[↩]
- American Diabetes Association. Glycemic Index and Diabetes. http://www.diabetes.org/food-and-fitness/food/what-can-i-eat/understanding-carbohydrates/glycemic-index-and-diabetes.html[↩]
- Atkinson FS, Foster-Powell K, Brand-Miller JC. International Tables of Glycemic Index and Glycemic Load Values: 2008 . Diabetes Care. 2008;31(12):2281-2283. doi:10.2337/dc08-1239. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2584181/[↩]
- FAO/WHO scientific update on carbohydrates in human nutrition: conclusions. Mann J, Cummings JH, Englyst HN, Key T, Liu S, Riccardi G, Summerbell C, Uauy R, van Dam RM, Venn B, Vorster HH, Wiseman M. Eur J Clin Nutr. 2007 Dec; 61 Suppl 1:S132-7. https://www.ncbi.nlm.nih.gov/pubmed/17992184/[↩]
- Glycemic Index International Database, University of Sydney. http://www.glycemicindex.com[↩]
- Pascoe VL et al. J Am Acad Dermatol. 2015 Apr;151(4):375-81.[↩]
- Berger R et al. Clin Ther. Jun;29(6):1086-97.[↩]
- Asai Y. CMAJ. 2016 Feb 2;188(2):118-26.[↩]
- Fulton, J. E., Plewig, G. & Kligman, A. M. Effect of chocolate on acne vulgaris. JAMA. 1969, 210, 20171- 2074[↩][↩]
- Goh, W, et al. Chocolate and acne: how valid was the original study? Clin. Dermatol. 2011, 29, 459-460[↩][↩]
- Block, S. G. et al. Exacerbation of facial acne vulgaris after consuming pure chocolate. J. Am. Acad. Dermatol. 2011, 65, e114-e115[↩][↩][↩]
- Caperton, C., Block, S., Viera, M., Keri, J. & Berman, B. Double-blind, placebo-controlled study assessing the effect of chocolate consumption in subjects with a history of acne vulgaris. J. Clin. Aesth. Dermatol. 2014, 7, 19-23[↩][↩][↩]
- Wolkenstein P. et al. Smoking and dietary factors associated with moderate-to-sever acne in French adolescents and young adults: results of a survey using a representative sample. Dermatology 2015, 230, 34-39[↩][↩]
- Vongraviopap, S. & Asawanonda P. Dark chocolate exacerbates acne. Int. J. Dermatol. 2016, 55, 587-591[↩][↩][↩]
- Delost, G. R., Delost, M. E. & Lloyd, J. The impact of chocolate consumption on acne vulgaris in college students: a randomized crossover study. J. Am. Acad. Dermatol. 2016, 75, 220-221[↩][↩]





{kind=link}