
Contents
Eye injury
Eye injury can involve the eyelids, the bones surrounding the eye (the eye socket), and the eyeball itself. Injuries to the eye and surrounding structures can be caused by blunt trauma from sport balls, fists, or airsoft/pellet/paintball guns; sharp trauma such as a stick, projectiles or knives; or chemical trauma such as splash from a caustic substance like a cleaning material or pool supplies. Safety glasses should be worn at all times while playing with airsoft/pellet/paintball guns and these should never be pointed at anyone’s faces.
There are over 2.4 million ocular injuries in the United States every year, with about 1 million of these patients presenting to emergency departments 1. The estimated incidence of eye injuries requiring medical attention is approximately 3.2 to 9.7 per 1,000 population in the U.S 2. Traumatic eye injuries are the most common cause of monocular blindness in the U.S., with more than 40,000 new cases every year 2.
Most eye injuries are minor, like getting soap in the eye or a speck of dirt under the eyelid. Others, like those that happen during sports activities or from a fall or chemical eye injury, can be serious and need medical attention. When an eye injury does occur, have an ophthalmologist or other medical doctor examine the eye as soon as possible, even if the injury seems minor at first. DO NOT attempt to treat a serious eye injury yourself. Because eye injuries can cause serious vision loss, it’s important to be able to recognize an injury and appropriately respond to it.
A serious eye injury is not always immediately obvious. Delaying medical attention can cause the damaged areas to worsen and could result in permanent vision loss or blindness.
Eye injuries are the most common preventable cause of blindness. While many minor eye irritations can be treated at home by flushing the eye with water, more serious injuries need medical attention. So when in doubt, err on the side of caution and see your doctor for help.
The structure of your face helps protect your eyes from injury. Still, injuries can damage your eye, sometimes severely enough that you could lose your vision. Most eye injuries are preventable. If you play sports or work in certain jobs, you may need protection.
The most common type of injury happens when something irritates the outer surface of your eye. Certain jobs such as industrial jobs or hobbies such as carpentry make this type of injury more likely. It’s also more likely if you wear contact lenses.
Chemicals or heat can burn your eyes. With chemicals, the pain may cause you to close your eyes. This traps the irritant next to the eye and may cause more damage. You should wash out your eye right away while you wait for medical help.
Table 1. Urgent care eye injury
| Emergency | Initial management | Ophthalmic management |
|---|---|---|
Retinal tear or detachment | Refer to ophthalmologist immediately | Dilated fundoscopic examination; retinal laser for small retinal tear with no detachment; surgical repair with pneumatic retinopexy, scleral buckle, or vitrectomy for retinal detachment |
Mechanical globe injury | Place metal shield over eye; prescribe antiemetics and systemic antibiotics; update tetanus immunization; refer immediately to ophthalmologist or emergency department | Orbital computed tomography to evaluate for fractures and intraocular foreign bodies; immediate surgery to repair the laceration; monitor for endophthalmitis and sympathetic ophthalmia |
Chemical eye injury | Irrigate eye with normal saline or lactated Ringer’s solution with at least 2 L of fluid; continue irrigation until pH is normal, then refer immediately to ophthalmologist or emergency department | Topical antibiotics and artificial tears for mild burns; topical antibiotics, artificial tears, steroids, ascorbate, and citrate drops for severe burns |
If you notice any of these signs in yourself or someone else, get medical help right away.
- The person has obvious pain or trouble opening the eye or trouble seeing
- The person has a cut or torn eyelid.
- One eye does not move as well as the other eye.
- One eye sticks out farther or seeming more prominent than the other eye.
- The eye has an unusual pupil size or shape.
- There is blood in the white part of the eye.
- The person has something in the eye or under the eyelid that can’t be easily removed.
Get Emergency Care Immediately if you have:
- trouble seeing
- been exposed to chemicals
- something embedded in the eye
- severe eye pain
- blood in the eye
- nausea or vomiting after an eye injury
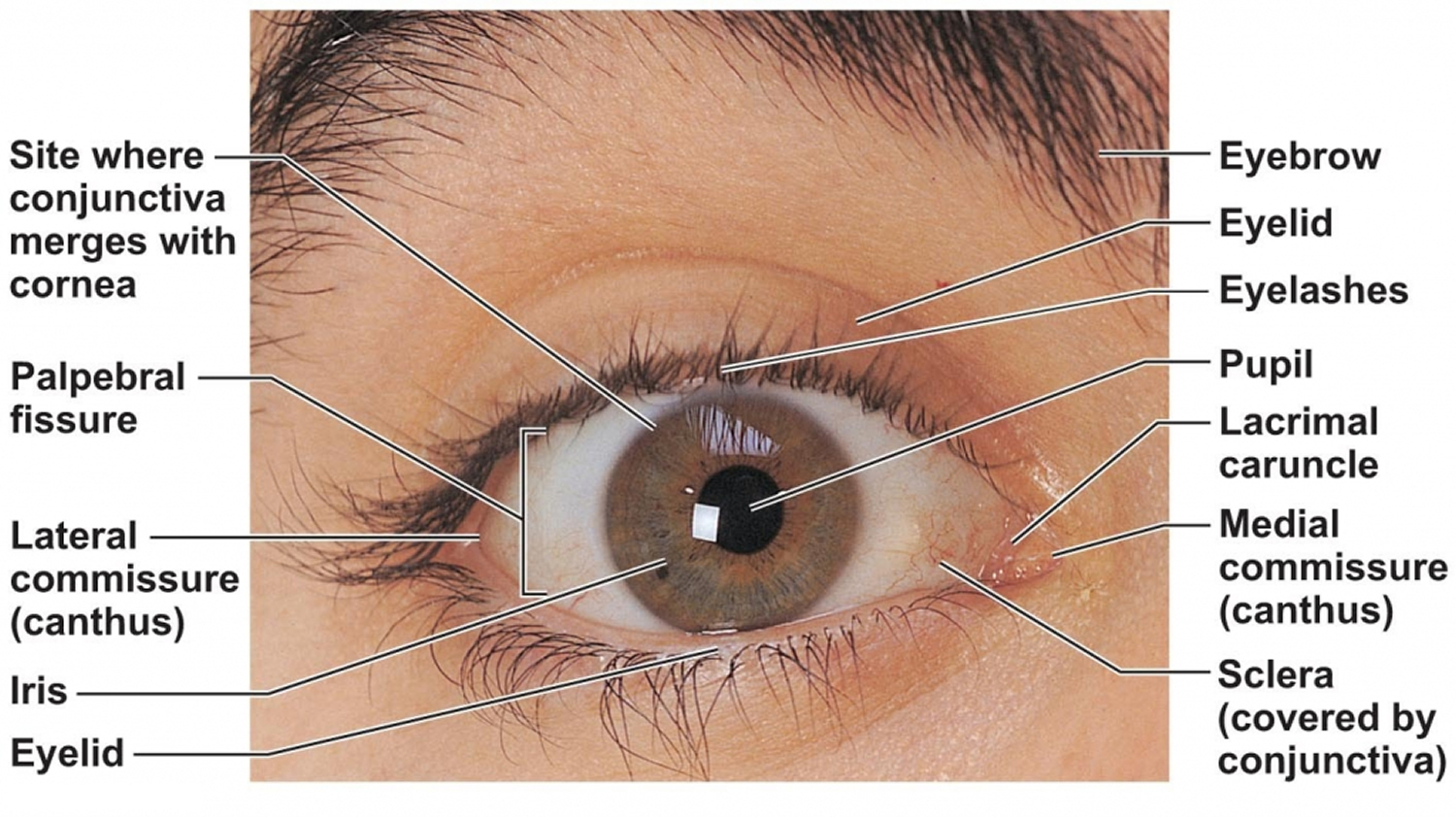
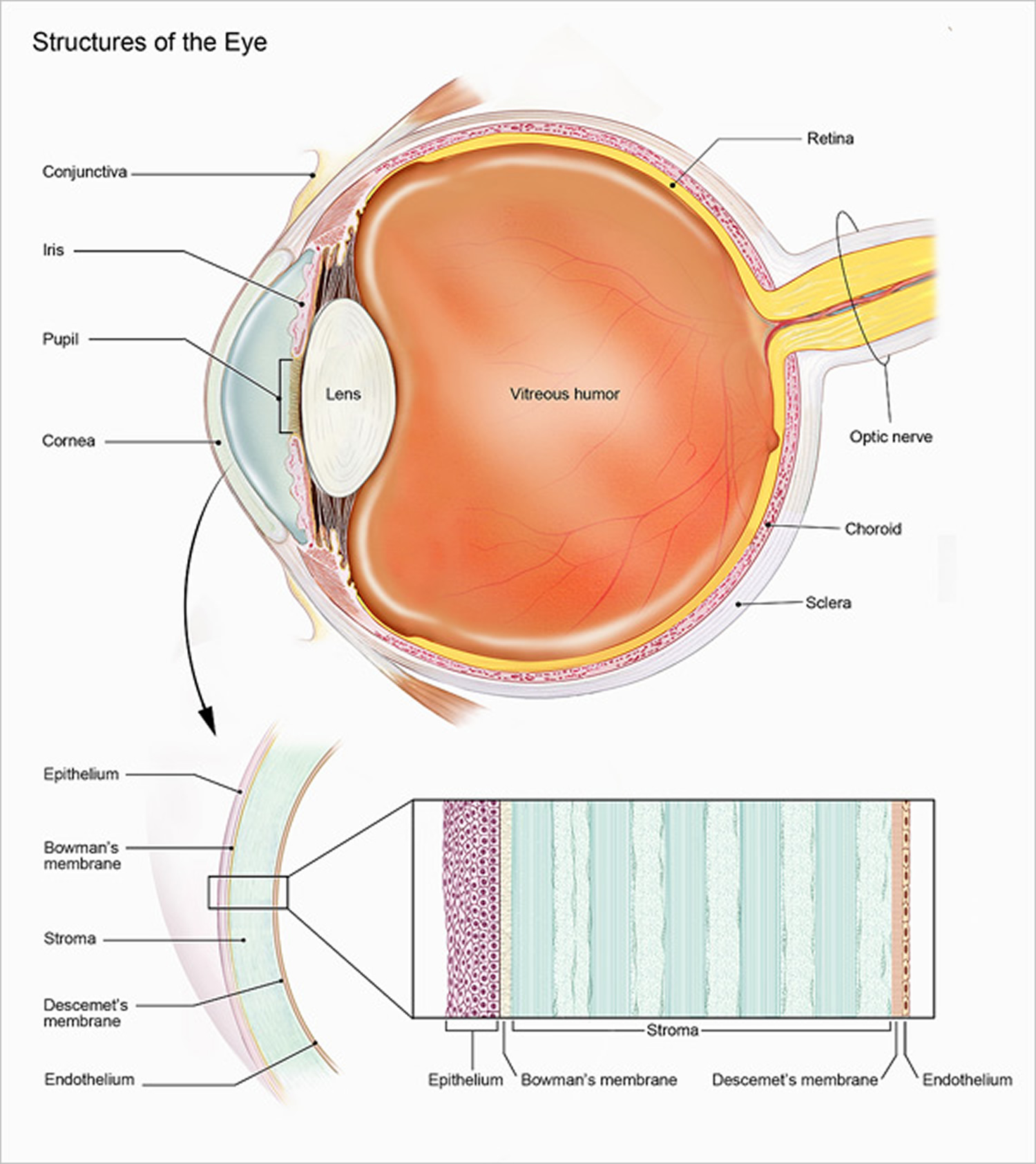
Figure 1. Human eye
Retinal Detachment
Retina separates from the underlying retinal pigment epithelium and choroid, either from accumulation of fluid between the two layers or vitreous traction on the retina.
Diagnosis:
- History (trauma followed by flashing lights/floaters/dark veil/curtains, or history of diabetes/sickle disease with the same complaints)
- Decreased peripheral or central visual acuity
- Direct fundoscopic exam à pale billowing parachute with a large retinal detachment
- Dilated indrect ophthalmoscopic evaluation by ophthalmologist
- Ocular ultrasound à retinal detachment seen as hyperechoic membrane is posterior part of eye, sensitivity ranges from 97% to 100%, specificity 83% to 100%.
Management:
Consult ophthalmology for surgical repair
Eye injury first aid
For ALL eye injuries:
- DO NOT touch, rub or apply pressure to the eye.
- DO NOT try to remove the object stuck in the eye.
- DO NOT apply ointment or medication to the eye.
- See a doctor as soon as possible, preferably an ophthalmologist.
If your eye has been cut or punctured:
- Gently place a shield over the eye. The bottom of a paper cup taped to the bones surrounding the eye can serve as a shield until you get medical attention.
- DO NOT rinse with water.
- DO NOT remove the object stuck in eye.
- DO NOT rub or apply pressure to eye.
- Avoid giving aspirin, ibuprofen or other non-steroidal, anti-inflammatory drugs. These drugs thin the blood and may increase bleeding.
- After you have finished protecting the eye, see a physician immediately.
If you get a particle or foreign material in your eye:
- DO NOT rub the eye.
- Lift the upper eyelid over the lashes of your lower lid.
- Blink several times and allow tears to flush out the particle.
- If the particle remains, keep your eye closed and seek medical attention.
In case of a chemical burn to the eye:
- Immediately flush the eye with plenty of clean water
- Seek emergency medical treatment right away.
To treat a blow to the eye:
- Gently apply a small cold compress to reduce pain and swelling.
- DO NOT apply any pressure.
- If a black eye, pain or visual disturbance occurs even after a light blow, immediately contact your ophthalmologist or emergency room.
- Remember that even a light blow can cause a significant eye injury.
To treat sand or small debris in the eye:
- Use eyewash to flush the eye out.
- DO NOT rub the eye.
- If the debris doesn’t come out, lightly bandage the eye and see an ophthalmologist or visit the nearest emergency room.
To treat eye scratches:
- DO rinse your eye with saline solution or clean water. If you don’t have an eyecup, use a small, clean glass. Rest the rim of the glass on the bone at the base of your eye socket, below your lower eyelid. The water or saline solution may flush the foreign object from your eye.
- DO blink. Blinking can help get rid of small bits of dust or sand in your eye.
- DO pull your upper eyelid over your lower eyelid. The lashes from your lower eyelid may be able to brush away any foreign object caught underneath your upper eye lid.
- DO wear sunglasses. If your eye is sensitive to light because of the scratch, sunglasses will lessen the symptoms while you heal.
- DO NOT rub your eye. You may be tempted to do so, but rubbing your eye can make the abrasion worse.
- DO NOT touch your eye with anything. Fingers, cotton swabs and other objects won’t help remove the foreign object and could hurt your eye more. Remember that the object that caused the scratch could be gone even though you still feel as if something is in your eye.
- DO NOT wear your contact lenses. Wearing your contact lenses will slow the healing process and could cause complications.
Eye injury prevention
While it’s true that many eye injuries happen on the job, nearly half (44.7 percent) of all eye injuries occurred in the home. More than 40 percent of eye injuries reported in by the American Academy of Ophthalmology and the American Society of Ocular Trauma were caused by projects and activities such as home repairs, yard work, cleaning and cooking. More than a third (34.2 percent) of injuries in the home occurred in living areas such as the kitchen, bedroom, bathroom, living or family room. More than 40 percent of eye injuries every year are related to sports or recreational activities. Eyes can be damaged by sun exposure, not just chemicals, dust or objects.
Among all eye injuries reported in the American Academy of Ophthalmology and the American Society of Ocular Trauma, more than 78 percent of people were not wearing eyewear at the time of injury. Of those reported to be wearing eyewear of some sort at the time of injury (including glasses or contact lenses), only 5.3 percent were wearing safety or sports glasses.
Fortunately, most eye injuries are preventable. Take simple steps to reduce the risk of an eye injury and understand when to see a doctor.
Follow these safety tips to prevent eye injuries around the home.
During DIY
- Wear protective eyewear during risky activities. Wear safety glasses with side shields anytime you might be exposed to flying particles, objects or dust.
- Wear goggles when exposed to chemicals. Take precautions even if you’re just a bystander.
- Supervise your child’s use of tools. Pencils, scissors, forks and knives can all cause serious eye injury. Keep in mind that common household items — such as paper clips, bungee cords, wire coat hangers, rubber bands and fishhooks — also can be dangerous.
In the yard
- Protect your eyes while doing yardwork. Use protective eyewear every time you operate lawnmowers, lawn trimmers and leaf blowers.
- Keep children away from flying debris. Make sure young children stay out of the yard while a lawnmower is being operated.
- Store hazardous substances out of reach. Keep fertilizers, pesticides and pool chemicals away from children at all times.
Cooking and cleaning
- Use caution with chemicals and cleaners. Carefully read the labels of chemicals and household cleaning supplies, such as bleach, before using them.
- Don’t mix products. Keep all chemicals and sprays out of a child’s reach.
- Be careful when cooking or using hot objects. Use grease shields to prevent the splattering of hot grease or oil. Avoid using a curling iron near your eyes.
- Keep sharp kitchen tools and utensils away from small children. Store them in child-proof locations, and avoid setting them down within reach of young children.
On the move
- Eliminate hazards that may cause falls. Secure rugs and railings. If a child or elderly adult lives in your home, use safety gates at the top and bottom of stairs, and consider covering sharp furniture edges and corners with a cushioning material.
- Use car seats. Make sure your child is properly secured in a car seat and that the seat belt or shoulder belt fits tightly. Don’t allow a child age 12 or younger to ride in the front seat. Store loose items in your trunk or secure them to the floor of your vehicle.
At play
- Avoid certain children’s toys. Don’t allow your child to play with non-powder rifles, such as pellet guns or BB guns. Avoid projectile toys, such as darts, bows and arrows, and missile-firing toys.
- DO NOT allow your children to use laser pointers. Laser pointers, especially those with short wave lengths such as green laser pointers, can permanently damage the retina and cause visual loss with exposures as short as a few seconds. As an adult, be cautious when using laser pointers. Avoid directing the beam toward anyone’s eyes.
- Wear protective eyewear during sports. Any sport featuring a ball, puck, stick, bat, racket or flying object, is a potential risk of eye injury. Choose sports protective eyewear labeled as ASTM F803-approved. Eyewear that hasn’t been tested for sports use, such as sunglasses, can cause more harm than no eyewear at all.
- Keep small children safe around dogs. When young children are bitten by dogs, eye injuries frequently occur.
Celebrating
- Forgo backyard fireworks. Leave fireworks to trained professionals.
- Use caution when opening a champagne bottle. Don’t shake the bottle. Point the bottle at a 45-degree angle away from yourself and any bystanders. Firmly place your palm over the cork while removing the wire hood. Place a towel over the entire top of the bottle, grasp the cork and slowly twist the bottle until the cork is almost out of the neck. To prevent the cork from being discharged like a missile, maintain slight downward pressure on the cork just as it comes out of the bottle.
Protective Eyewear
The type of eye protection needed will depend on the activity you are involved in. Your regular eyeglasses do not protect your eyes from impact, debris or damage. In fact, some eye glasses can shatter if damaged, causing even more eye injury.
For most repair projects and activities around the home, standard ANSI-approved protective eyewear will be sufficient. For many work situations, the same protection you use at home will suffice, but there are important exceptions you need to know about. Sports eye protection should meet the specific requirements of that sport; these requirements are usually established and certified by the sport’s governing body and/or the American Society for Testing and Materials (ASTM).
Eye Protection in the Home
The American Academy of Ophthalmology and the American Society of Ocular Trauma recommend that every household have at least one pair of ANSI-approved protective eyewear to be worn when doing projects or activities that could create a risk for eye injuries at home.
Choose protective eyewear with “ANSI Z87.1” marked on the lens or frame. This means the glasses, goggles or face shield meets the American National Standards Institute (ANSI) Z87.1 safety standard. ANSI-approved protective eyewear can be easily purchased from most hardware stores nationwide.
You should use eye protection of the activity involves:
- Hazardous chemicals or other substances that could damage your eyes upon contact
- Flying debris or other small particles that could hit participants or bystanders
- Projectiles or objects that could become projectiles and fly into the eyes unexpectedly
Bottom line: use common sense, especially if there are children around. You should protect them, and set an example by making a smart choice.
Eye Protection at Sports
The eye protection needed to prevent eye injuries in your sport is determined by various standards set by ASTM (American Society for Testing and Materials). Some eye-safety standards by sport are listed below. This is not a comprehensive list.
- ASTM F803: Eye protectors for selected sports (racket sports, women’s lacrosse [see the U.S. Lacrosse website for more details], field hockey, baseball, basketball);
- ASTM F513: Eye and face protective equipment for hockey players;
- ASTM F1776: Eye protectors for use by players of paintball sports;
- ASTM F2879: Eye protectors for use by players of airsoft sports;
- ASTM F1587: Head and face protective equipment for ice hockey goaltenders;
- ASTM F910: Face guards for youth baseball; and
- ASTM F659: High-impact resistant eye protective devices for Alpine skiing.
Protective glasses or goggles with UV protection should be worn when snow or water skiing. They will help shield the eyes from sunburn and glare.
Eye Protection at Work
The eye protection needed to do your job safely is determined by the Occupational Safety and Health Administration (OSHA). To find out what standards apply, check with your company’s human resources department, or whoever is charged with overseeing OSHA compliance.
With the exception of welding, which requires additional eye and face protection, OSHA standards may often require the same ANSI-certified eye protection at work that you should use at home.
Eye Protection for Children
Each year thousands of children sustain eye damage or even blindness from accidents at home, at play or in the car. More than 90 percent of all eye injuries can be prevented through use of suitable protective eyewear.
Sports deserve particular attention, because eye injuries occur fairly often in children and young adult athletes: between the ages of five and 14, most sports-related injuries in the U.S. occur while playing baseball.
Preventing Injuries
- Children should wear sports eye protectors made with polycarbonate lenses for baseball, basketball, football, racquet sports, soccer, hockey, lacrosse, paintball.
- All chemicals and sprays must be kept out of reach of small children.
- Parents and others who provide care and supervision for children need to practice safe use of common items that can cause serious eye injury, such as paper clips, pencils, scissors, bungee cords, wire coat hangers and rubber bands.
- Teach your children to be EyeSmart by safeguarding your own sight with ANSI-approved protective eyewear during potentially dangerous yard work and household repairs or projects.
- Only purchase age-appropriate toys.
- Avoid projectile toys such as darts, bows and arrows, and missile-firing toys.
- Look for toys marked with “ASTM”, which means the product meets the national safety standards set by the American Society for Testing and Materials.
- Use safety gates at the top and bottom of stairs. Pad or cushion sharp corners. Put locks on all cabinets and drawers that kids can reach.
- DO NOT allow your children to play with non-powder rifles, pellet guns or BB guns. They are extremely dangerous and have been reclassified as firearms and removed from toy departments.
- DO NOT allow children anywhere near fireworks, especially bottle rockets. These fireworks pose a serious risk of eye injury and have been banned in several states.
- When very small children (age 4 and younger) are bitten by dogs, eye injuries occur about 15 percent of the time. The dog is usually one the child is familiar with, and second attacks by the same dog are likely to cause more serious injury. It is recommended that any dog that bites a child be removed from the household.
- On the road, make sure children are properly secured in baby carriers and child safety seats and that the seat and shoulder belts fit well. Children age 12 and younger should never ride in the front seat. Store loose items in the trunk or secured on the floor, as any loose object can become a dangerous projectile in a crash.
Chemical eye injury
Chemical eye injuries occur after exposure of the eye surface to an acid or alkali in the form of a liquid, powder, or gas 3. Both acids and alkalis can cause severe chemical burns to the eye. Table 2 contains a list of chemicals that commonly cause these burns. Alkali substances lead to very rapid and deep eye injury by a process called liquefactive necrosis, in which cells are completely digested by the chemical and turn into liquid. Irreversible damage to the eye can occur within a few minutes of alkali exposure. Acid burns tend to be less severe, but still can result in significant eye damage, especially if the chemical is not rapidly removed. Hydrofluoric acid—commonly found in etchant, rust-removing compounds and wheel-cleaning agents—is an exception to this rule, behaving like an alkali with rapid penetration and damage to the eye 4.
The severity of the eye injury depends on the pH concentration of the chemical and the duration of contact with the ocular surface 5. Chemical burns damage the conjunctival and corneal epithelium and may cause ischemic damage to the conjunctival and scleral vessels, potentially affecting the entire anterior segment of the eye.
Chemical burns account for nearly 3% of all ocular trauma cases; alkali burns are more common and more severe than acid burns 6. Most of these injuries occur in the workplace, but they can also occur at home or during an assault 7.
Table 2: Chemicals that commonly cause eye burns
| Chemical | Common Products |
| Acids | |
| Sulfuric acid | Toilet cleaner, battery fluid |
| Sodium hypochlorite | Pool cleaners, bleach |
| Acetic acid | Vinegar |
| Hydrofluoric acid | Glass polishers, rust removal agents |
| Hydrochloric acid | Food and leather processing agents |
| Alkalis | |
| Calcium carbonate/Magnesium carbonate | Lime (building material) |
| Calcium hydroxide | Plaster, mortar |
| Sodium hydroxide/Potassium hydroxide | Lye (oven and drain cleaner) |
| Magnesium hydroxide | Fireworks |
| Ammonium hydroxide | Ammonia (cleaning agents, fertilizers) |
| Sodium tripolyphosphate | Dishwasher detergent |
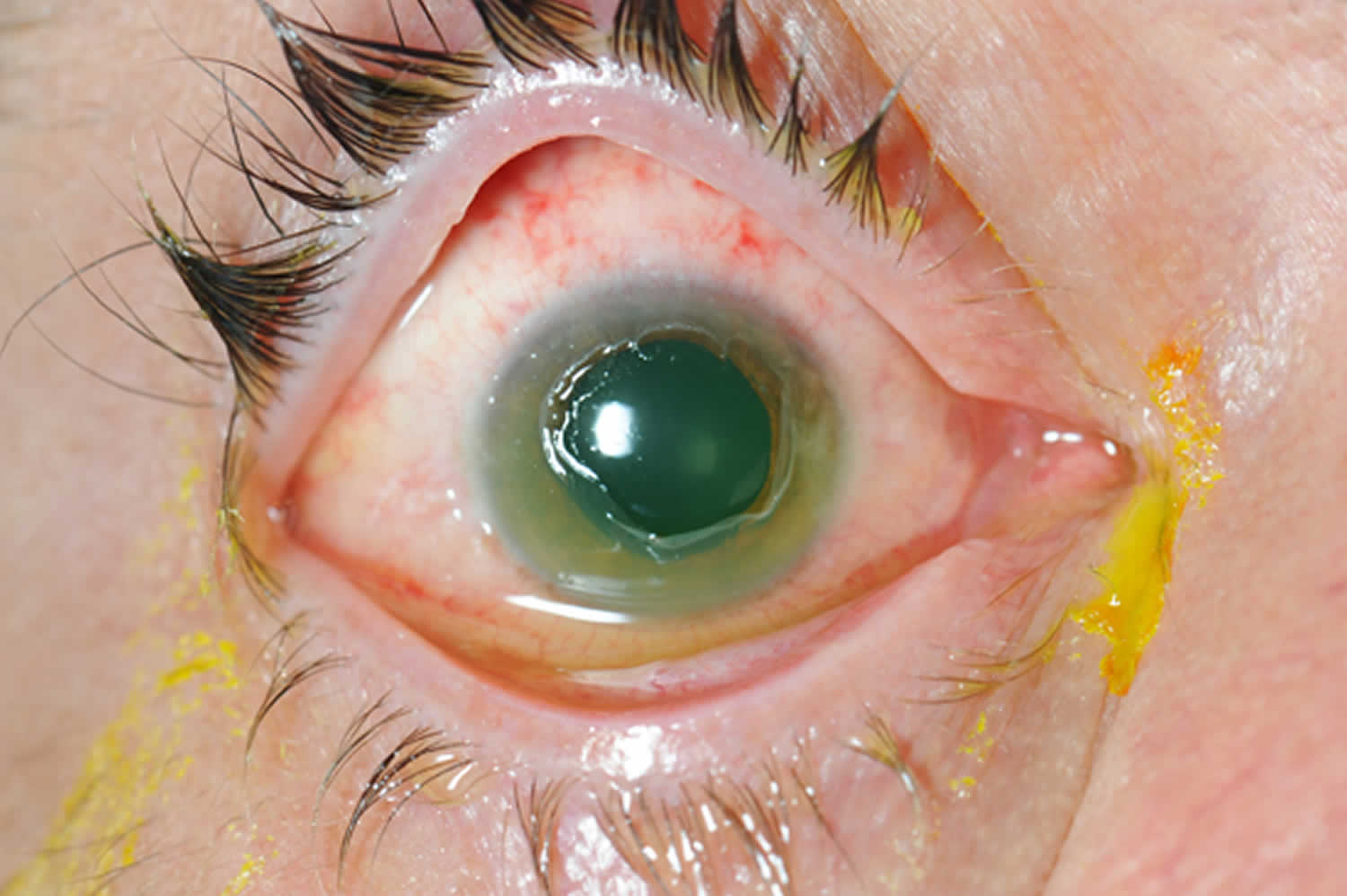
Patients with a chemical eye injury typically complain of severe eye pain, redness, watery eyes, sensitivity to light, decreased vision and blepharospasm (inability to open the eyelids) 4. However, exposure to some alkali substances may not be painful at first due to the local inhibition of sensation. In severe cases of alkali injury, the eye may appear white due to conjuctival ischemia or a large cornea defect may be visible (see Figure 2). To assess the severity of the injury, the physician should attempt to identify the type of chemical involved and how much of it came in contact with the eye.
Examination of the external and anterior segment of the eye may reveal swelling and burns to the eyelids; a cloudy cornea; corneal epithelial defect; conjunctival injection; or a white eye, which indicates conjunctival ischemia. Initial testing of the ocular surface should be performed by placing a strip of litmus paper in the conjunctival fornix. The Roper-Hall classification system 8 is used to describe the extent of injury; it is based on the degree of ischemia to the limbus (i.e., the junction between the cornea and sclera) and the degree of corneal haze (Table 3).
Table 3. Roper-Hall Classification of Ocular Surface Burns
| Grade | Corneal findings | Limbal ischemia | Prognosis |
|---|---|---|---|
I | Mild epithelial damage | None | Good |
II | Stromal haze with visible iris details | Less than one-third of limbus | Good |
III | Stromal haze that obscures iris details | One-third to one-half of limbus | Guarded |
IV | Opaque, no view of the iris | More than one-half of limbus | Poor |
Figure 2. Severe chemical eye burns
Chemical eye injury treatment
A chemical burn to the eye is an ocular emergency 3. The essential aspect of managing chemical eye burns is immediate and copious irrigation of the eye to dilute and remove as much of the chemical as possible. Treatment should be initiated immediately because of the potential for permanent damage and vision loss. Irrigation should begin in the prehospital setting. Delays in initiating irrigation by as little as 20 seconds have been associated with more severe injury in animal models of alkali eye burns 9. If possible, the patient should be placed on his/her side with the affected eye down, and irrigation should be directed from the nasal corner outward to wash away chemicals from the lacrimal punctum 10. The patient should be asked to look in all directions during irrigation to ensure complete removal of chemicals from the entire surface of the eye.
Initial treatment involves administering topical anesthetics to the eye, followed by copious irrigation with lactated Ringer’s solution, normal saline, or water if other irrigation solutions are not available 5. The eye should be irrigated with at least 2 L of fluid using a lens irrigation system or intravenous tubing. The pH of the ocular surface should be remeasured five minutes after initial irrigation, and a wet cotton swab should be used to sweep the upper and lower fornices to remove any retained crystallized chemical particles. Further irrigation is necessary if the ocular surface has not been neutralized (pH of 7.0 to 7.5).
- Start irrigation IMMEDIATELY with Normal Saline or Lactated Ringers Solution (2 liters)—wait 5 minutes and check pH.
- Additional irrigation as needed until pH is 7.0-7.5.
- Continue irrigation until pH is normal—compare pH to that of the other eye because often pH paper will read either too alkaline or acidic.
- Sweep for particulate matter and examine fornices.
- Check intraocular pressure (IOP).
- Note limbal ischemia, epithelial defect, stromal loss/haze, edema, anterior chamber depth, inflammation, and lens clouding.
Once the ocular surface has been neutralized, the patient should be referred immediately to an ophthalmologist. Subsequent care depends on the extent of the injury. For mild burns (grades I and II), treatment with antibiotic eye drops and preservative-free artificial tears may suffice to promote corneal and conjunctival epithelial healing 11. Severe burns (grades III and IV) require topical antibiotics and artificial tears, as well as topical steroid, ascorbate, and citrate drops to reduce inflammation and promote epithelialization 11.
Chemical eye injury prognosis
The prognosis depends on how quickly the eye is irrigated after a chemical injury; immediate irrigation results in less damage to the ocular surface and better visual outcomes 12. The prognosis also depends on the grade of the initial injury. In a retrospective study of patients with alkali burns, visual acuity was 20/40 or better in 100% of patients with grade I or II injuries, compared with 86% and 60% of patients with grade III or IV injuries, respectively 11. Long-term complications may occur, and follow-up is necessary to monitor for elevated intraocular pressure, corneal opacities, and eyelid abnormalities.
Penetrating eye injury
Penetrating eye injury in which a foreign object enters the eye and creates a hole in the cornea/sclera (“globe laceration”), with a retained intraocular foreign body. No attempts to remove intraocular foreign bodies should be made in the prehospital setting. The distal end of an intraocular foreign body may be lodged deep within the eye, in a paranasal sinus or even in the intracranial space. Manipulation of the object can increase the severity of injury by further damaging surrounding structures and inducing agitation and vomiting 13.
Penetrating eye injury management:
- Prevent increased intraocular pressure (IOP)
- Raise head of bed at 30 degrees
- Avoid eye manipulation (do not measure eye pressure, retract lid, or perform ocular ultrasound)
- Cover with an eye shield (do not place eye patch as it exerts pressure on globe) – A paper cup can be used if an eye shield is not available
- Administer topical and systemic broad-spectrum antibiotics
- Update tetanus
- Give antiemetics to prevent nausea (which increases IOP)
- Give pain medicine
The goal of management for penetrating eye injuries in the prehospital setting is to avoid secondary injury by preventing any increase in intraocular pressure (IOP). It’s crucial to avoid applying any external pressure to the eye. A protective shield should be placed over the eye for transport, being especially careful not to place any pressure points of the shield onto the eye itself, but instead onto the bones surrounding the eye. If a commercial metal or plastic eye shield is not available, a Styrofoam or plastic cup can be taped over the eye for protection. The head of the bed should be elevated to 30° if possible to prevent increased intraocular pressure. Because pain, agitation, uncontrolled hypertension and Valsalva maneuvers can elevate intraocular pressure, appropriate analgesic, antiemetic and sedative therapy should be provided. Narcotics are preferred to non-steroidal anti-inflammatory drugs (NSAIDs) due to the latter’s platelet-inhibiting properties. Treatment in the hospital typically includes continued protection of the globe to prevent worsening injury, intravenous antibiotics to prevent post-traumatic endophthalmitis, tetanus prophylaxis and emergent ophthalmology consultation for surgical repair of the injury.
In the hospital setting, radiographic imaging, such as computed tomography (CT scan), is often used to identify the precise location of the foreign body. The objects are usually removed by ophthalmologists in an operating room, where damage to surrounding structures can be minimized.
Prognosis of penetrating eye injuries is very poor, with over one-third of patients requiring enucleation or having no light perception. Only about one-third of patients have visual acuity of greater than 20/200 at hospital discharge 14.
Figure 3. Penetrating eye injury

Retrobulbar hematoma
Retrobulbar hematoma is a bleeding posterior to the eye causing the eye to push forward. Retrobulbar hematoma occurs when veins draining the posterior of the eye are injured and bleed into the space between the eye and skull. Blunt trauma to the face is the typical mechanism of injury, but retrobulbar hematoma can also occur as a complication of orbital or sinus surgery. Displaced orbital wall fractures can protect against retrobulbar hematoma, because bleeding inside the orbit can drain through the fracture. Rarely, reduction of these fractures can lead to a retrobulbar hematoma if bleeding into the orbit isn’t controlled prior to reduction 15.
Symptoms of a retrobulbar hematoma typically develop over a few hours as the expanding hemorrhage exerts increasing pressure on the eye, resulting in elevated intraocular pressure (IOP) 16. This elevation in pressure results in ischemia to the retina and optic nerve by decreasing blood flow through the central retinal artery.17 Animal models have shown permanent eye damage within 90–120 minutes of sustaining a retrobulbar hematoma 16. Signs and symptoms include decreased visual acuity, painful proptosis (anterior displacement of the eye), a dilated pupil and restricted extraocular movements.
Principles of prehospital management include rapid transport and minimizing intraocular pressure (IOP). Vomiting and Valsalva maneuvers can lead to increased intraocular pressure, so prevention with antiemetics and pain control is especially important with retrobulbar hematomas. It’s prudent to avoid medications that can increase the risk of further bleeding, including NSAIDs and other antiplatelet agents.
Definitive treatment in the hospital involves surgical drainage of the hematoma. This procedure is typically performed by an ophthalmologist in an operating room. If an ophthalmologist is not immediately available, experienced emergency physicians or surgeons may perform an emergency lateral canthotomy and cantholysis in the emergency department in attempt to relieve the elevated intraocular pressure (IOP) and prevent permanent blindness16. In this procedure, the tendon positioned immediately laterally to the globe is incised, allowing blood to flow anteriorly and laterally out of the retro-orbital space.
Consider lateral canthotomy if any of the following 17
- Decreased visual acuity
- Restricted extraocular movement
- Afferent pupillary defect
- Proptosis
- Intraocular pressure > 40 mmHg
Figure 4. Retrobulbar hematoma

Toddler eye injury
An ophthalmologist, primary care doctor, school nurse or children’s health service should examine the eye as soon as possible, even if the injury seems minor at first, as a serious injury is not always immediately obvious.
- Delaying medical attention can cause the damaged areas to worsen and could result in permanent vision loss or blindness.
While seeking medical help, care for the child as follows:
- DO NOT touch, rub or apply pressure to the eye.
- DO NOT try to remove any object stuck in the eye. For small debris, lift eye lid and ask child to blink rapidly to see if tears will flush out the particle. If not, close the eye and seek treatment.
- DO NOT apply ointment or medication to the eye.
- A cut or puncture wound should be gently covered.
- Only in the event of chemical exposure, flush with plenty of water.
Eye injury signs and symptoms
It’s not always easy to identify an eye injury — especially in a child.
Signs and symptoms of an eye injury may include:
- redness around or in the eye
- stinging or burning
- watering
- sensitivity to light
- blurred vision
- swelling of the eyelids
- discoloration around the eye
Seek medical care immediately if you notice any of these signs or symptoms:
- Obvious pain, trouble opening the eye or trouble seeing
- A cut or torn eyelid
- One eye not moving as well as the other eye
- One eye sticking out farther or seeming more prominent than the other
- An unusual pupil size or shape
- Blood in the white part of the eye
- An object on the eye or under the eyelid that can’t easily be removed
Eye injury treatment
When an eye injury occurs, seek medical help from an ophthalmologist or another doctor as soon as possible — even if the injury seems minor. Delaying care could lead to permanent vision loss or blindness. In addition, take simple steps to prevent further damage. For example:
- DO NOT touch, rub or apply pressure to the eye
- DO NOT try to remove an object that appears stuck on the surface of the eye or an object that appears to have penetrated the eye
- DO NOT apply ointment or medication to the eye
- Flush out any chemicals the eye has been exposed to with plenty of clean water
- Gently place a shield or gauze patch over the eye until you can get medical attention
An accident can happen in the blink of an eye. Being prepared — both through prevention and quick action in case of an emergency — can help keep you and your loved ones seeing clearly.
Routine Irritations
Sand, dirt, and other foreign bodies on the eye surface.
- Wash your hands thoroughly before touching the eyelids to examine or flush the eye.
- DO NOT touch, press, or rub the eye itself, and do whatever you can to keep your child from touching it (a baby can be swaddled to prevent this).
- DO NOT try to remove any foreign body except by flushing. Other methods can scratch the surface of the eye, especially the cornea.
- Tilt your head over a basin or sink with the affected eye down and gently pull down the lower lid. Open the eyes as wide as possible. For an infant or small child, it’s helpful to have a second person hold the child’s eyes open while you flush.
- Gently pour a steady stream of clean water from a pitcher or faucet over the eye. (DO NOT heat the water)
- Flush for up to 15 minutes, checking the eye every 5 minutes to see if the foreign body has been flushed out.
- Because a particle can scratch the cornea and cause an infection, the eye should be examined by a doctor if irritation continues after flushing.
- A foreign body that remains after flushing probably will require removal by a trained medical professional.
Embedded Foreign Body
An object penetrates or enters the globe of the eye.
If an object, such as a piece of glass or metal, is sticking out of the eye, take the following steps:
- Call for emergency medical help or go to the emergency room.
- Cover the affected eye with a small cup taped in place. The point is to keep all pressure off the eye.
- Keep as calm and comfortable as possible until help arrives.
Chemical Exposure
- Many chemicals, even those found around the house, can damage an eye. If you or your child gets a chemical in the eye and you know what it is, look on the product’s container for an emergency number to call for instructions.
- Flush the eye (see Routine Irritations above) immediately with clean water for 15 to 30 minutes. If both eyes are affected, flush them in the shower.
- Call for emergency medical help.
- Call your local poison control center for specific instructions. Be prepared to give the exact name of the chemical, if you have it. However, do not delay flushing the eye first.
Black Eyes and Blunt Injuries
A black eye is often a minor injury. But this bruising also can be the result of a significant eye injury or head trauma. A visit to the doctor or an eye specialist might be needed to rule out serious injury, particularly if you’re not sure what caused the black eye.
For a black eye:
- Apply cold compresses intermittently: 5 to 10 minutes on, 10 to 15 minutes off. If you use ice, make sure it’s covered with a towel or sock to protect the delicate skin on the eyelid.
- Use cold compresses for 24 to 48 hours, then switch to applying warm compresses intermittently. This will help the body reabsorb the leakage of blood and may help reduce discoloration.
- For pain, take acetaminophen — not aspirin or ibuprofen, which can increase bleeding.
- Prop your head with an extra pillow at night, and encourage him or her to sleep on the uninjured side of the face (pressure can increase swelling).
- See your doctor, who may recommend an in-depth evaluation to rule out damage to the eye. Call immediately if you see any of these problems:
- increased redness
- drainage from the eye
- lasting eye pain
- any changes in vision
- any visible abnormality of the eyeball
- visible bleeding on the white part (sclera) of the eye, especially near the cornea
If the injury happened during one of your routine activities, such as a sport, follow up by investing in an ounce of prevention — protective goggles or unbreakable glasses are vitally important.
- McGwin G Jr, Owsley C. The incidence of emergency department-treated eye injury in the United States. Arch Ophthalmol. 2005;123(5):662–666.[↩]
- McGwin G, Xie A, Owsley C. The rate of eye injury in the United States. Arch Ophthalmol. 2005;123(9):970–976.[↩][↩]
- Common Eye Emergencies. Am Fam Physician. 2013 Oct 15;88(8):515-519. https://www.aafp.org/afp/2013/1015/p515.html[↩][↩]
- Fish R, Davidson RS. Management of ocular thermal and chemical injuries, including amniotic membrane therapy. Curr Opin Ophthalmol. 2010;21(4):317–321.[↩][↩]
- Kuckelkorn R, Schrage N, Keller G, Redbrake C. Emergency treatment of chemical and thermal eye burns. Acta Ophthalmol Scand. 2002;80(1):4–10.[↩][↩]
- Macewen CJ. Eye injuries: a prospective survey of 5671 cases. Br J Ophthalmol. 1989;73(11):888–894.[↩]
- Morgan SJ. Chemical burns of the eye: causes and management. Br J Ophthalmol. 1987;71(11):854–857.[↩]
- Roper-Hall MJ. Thermal and chemical burns. Trans Ophthalmol Soc U K. 1965;85:631–653.[↩][↩]
- Spector J, Fernandez WG. Chemical, thermal, and biological ocular exposures. Emerg Med Clin North Am. 2008;26(1):125–136.[↩]
- Duffy B. Managing chemical eye injuries. Emerg Nurse. 2008;16(1):25–29.[↩]
- Brodovsky SC, McCarty CA, Snibson G, et al. Management of alkali burns: an 11-year retrospective review. Ophthalmology. 2000;107(10):1829–1835.[↩][↩][↩]
- Saari KM, Leinonen J, Aine E. Management of chemical eye injuries with prolonged irrigation. Acta Ophthalmol Suppl. 1984;161:52–59.[↩]
- Morley MG, Nguyen JK, Heier JS, et al. Blast eye injuries: A review for first responders. Disaster Med Public Health Prep. 2010;4(2):154–160.[↩]
- Smith D, Wrenn K, Stack LB. The epidemiology and diagnosis of penetrating eye injuries. Acad Emerg Med.2002;9(3):209–213.[↩]
- Colletti G, Valassina D, Rabbiosi D, et al. Traumatic and iatrogenic retrobulbar hemorrhage: An 8-patient series. J Oral Maxillofac Surg. 2012;70(8):e464–e468.[↩]
- Chen YA, Singhal D, Chen YR, et al. Management of acute traumatic retrobulbar hematomas: A 10-year retrospective review. J Plast Reconstr Aesthet Surg. 2012;65(10):1325–1330.[↩][↩][↩]
- Lateral canthotomy and cantholysis: emergency management of orbital compartment syndrome. J Emerg Med. 2015 Mar;48(3):325-30. doi: 10.1016/j.jemermed.2014.11.002. Epub 2014 Dec 16. https://escholarship.org/uc/item/0zn3n1dd[↩]





{kind=link}