Contents
Fetal hydantoin syndrome
Fetal hydantoin syndrome also known as hydantoin embryopathy, phenytoin embryopathy or dilantin embryopathy, is a spectrum of birth defects seen in babies born to mothers who use of the anti-seizure (antiepileptic or anticonvulsant) drug phenytoin (Dilantin) during their pregnancy 1, 2, 3, 4. Dilantin also known as phenytoin is a medication used to treat epilepsy (seizure disorder). However, not all infants exposed to phenytoin (Dilantin) will be affected with fetal hydantoin syndrome 5, 6. If phenytoin (Dilantin) is taken by the mother in the first three months of pregnancy (the first trimester), there is approximately a 5 to 10 percent chance that the baby could be born with Fetal Hydantoin Syndrome 7. Phenytoin (Dilantin) crosses the placenta in such a way that the developing fetus receives a much higher dose of the medication than the mother is taking (the drug is broken down differently by the fetus). This is especially true when phenytoin (Dilantin) is used during the first three months of pregnancy (the first trimester). A few authors have suggested that phenytoin interferes with the body’s ability to absorb folic acid 2, 8, 9. And without an adequate supply of folic acid, infants have a significantly increased risk of developing major birth injuries. Genetic factors like defects in the detoxification of phenytoin arene oxide, complex interactions between multiple antiepileptic drugs, maternal age and period of gestation have also been implicated in contributing to phenytoin teratogenicity 10.
Fetal hydantoin syndrome signs and symptoms in affected babies can vary greatly from one infant to another. Symptoms may not be noticeable at birth (congenital), but will become apparent as an affected child grows older. Although researchers have been able to establish a clear fetal hydantoin syndrome with characteristic abnormalities or “core” symptoms, much about the disorder is not fully understood 11. Several factors including the small number of identified cases, the lack of large clinical studies, and the possibility of genes or other factors influencing the disorder prevent physicians from developing an accurate picture of associated symptoms and prognosis 11. Therefore, it is important to note that affected individuals may not have all of the symptoms. Parents should talk to their child’s doctor and medical team about their specific case, associated symptoms and overall prognosis.
Fetal hydantoin syndrome physical features may include abnormalities of the skull and facial features, growth deficiencies, underdeveloped (hypoplastic) nails of the fingers and toes, and/or mild developmental delays. Other findings occasionally associated with fetal hydantoin syndrome include cleft lip and palate, having an abnormally small head (microcephaly) and brain malformations with more significant developmental delays and skeletal malformations particularly of the fingers or hands.
There is no diagnostic testing that can identify fetal hydantoin syndrome. A diagnosis is made clinically based upon identification of characteristic symptoms in an affected infant in conjunction with a history of phenytoin exposure during gestation. It is important to note that the majority of infants born to women who take phenytoin during pregnancy will not develop fetal hydantoin syndrome.
The treatment of fetal hydantoin syndrome is directed toward the specific symptoms that are apparent in each individual. Treatment may require the coordinated efforts of a team of specialists. Pediatricians, oral surgeons, plastic surgeons, neurologists, psychologists, and other healthcare professionals may need to systematically and comprehensively plan an affect child’s treatment.
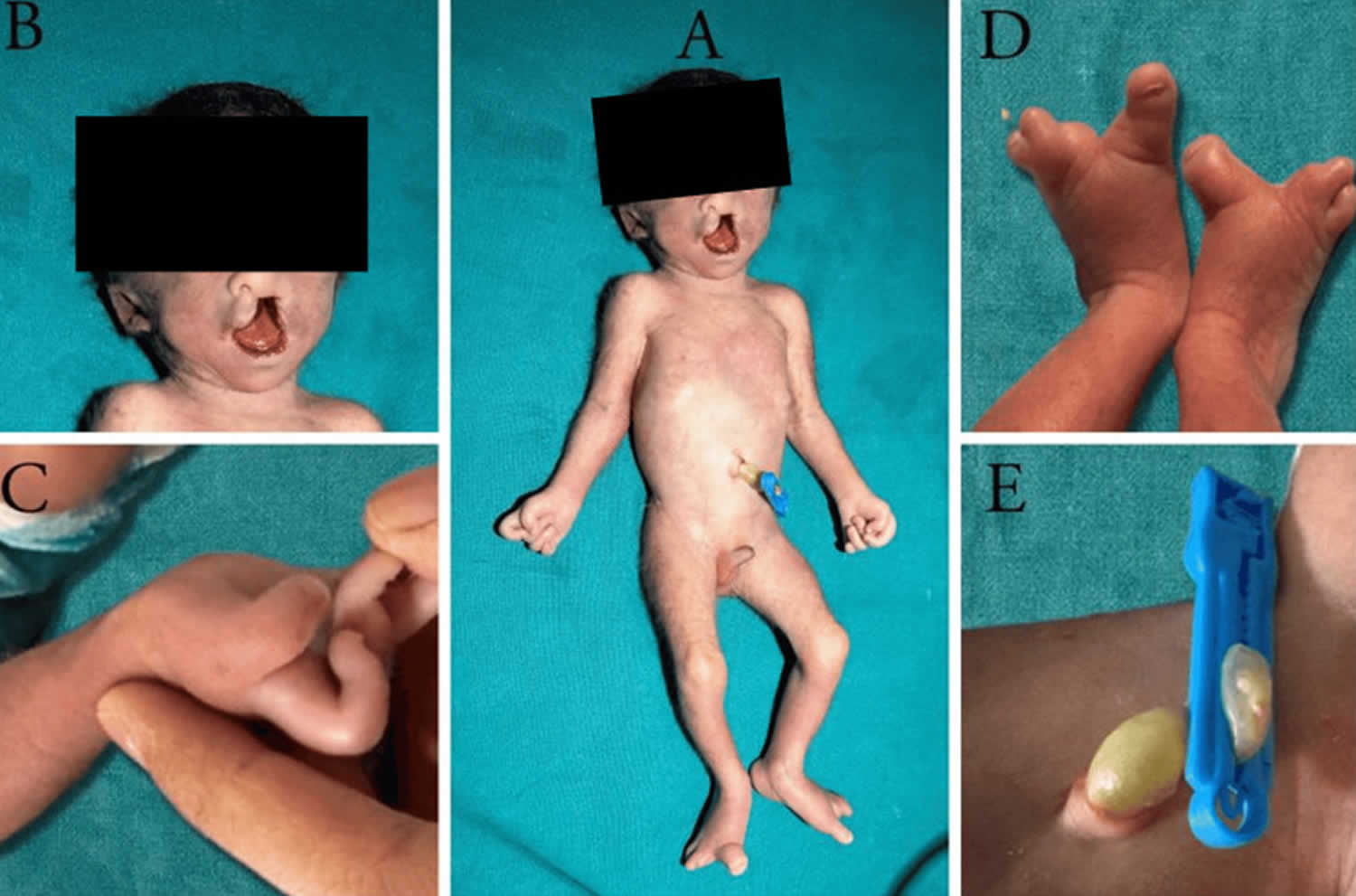
Figure 1. Facial features and limb abnormalities of fetal hydantoin syndrome

Footnotes: Clinical photographs of the patient showing (A) hypertelorism, flat and broad nasal bridge; (B) short upturned nose, long philtrum, thin upper lip; (C) stiff tapered fingers with hypoplastic fingernails; and (D) hypoplastic toenails and digitalized great toe.
[Source 3 ]Figure 2. Fetal hydantoin syndrome
Footnotes: Clinical photographs of the patient showing characteristic features of fetal hydantoin syndrome: (A) hypertelorism, broad nasal bridge, cleft lip and low-set ears. (B) Hypoplastic distal phalanges in the right hand with contractures. (C) Oligosyndactyly. (D) Absent distal phalanges in bilateral feet. (E) Single umbilical artery.
[Source 7 ]Fetal hydantoin syndrome causes
The exact risk of a fetus developing fetal hydantoin syndrome is not fully understood, but only approximately 5 to 10% of fetuses exposed to phenytoin (Dilantin) develop the disorder 10. Phenytoin (Dilantin) crosses the placenta in such a way that the developing fetus receives a much higher dose of the medication than the mother is taking (the drug is broken down differently by the fetus). This is especially true when phenytoin (Dilantin) is used during the first three months of pregnancy (the first trimester). A few authors have suggested that phenytoin interferes with the body’s ability to absorb folic acid 2, 8, 9. And without an adequate supply of folic acid, infants have a significantly increased risk of developing major birth injuries.
The specific amount of phenytoin ingestion required to cause fetal hydantoin syndrome has not been determined. Phenytoin (Dilantin) is often given with other anti-seizure drugs and other ‘add-on’ medications that may influence development of fetal hydantoin syndrome. Fetal hydantoin syndrome may be caused by a combination of specific genetic and environmental factors. Genetic factors like defects in the detoxification of phenytoin arene oxide, complex interactions between multiple antiepileptic drugs, maternal age and period of gestation have also been implicated in contributing to phenytoin teratogenicity 10.
Fetal hydantoin syndrome affects males and females in equal numbers. Studies have suggested that approximately 5% to 10% of infants exposed to phenytoin during pregnancy will develop fetal hydantoin syndrome.
Anti-seizure medications, also known as antiepileptic or anticonvulsant medications, are among the most common teratogens prescribed to women of childbearing age. A teratogen is a drug that interferes with the development of a fetus. Affected infants often develop similar symptoms regardless of the associated drug, particularly symptoms affecting the head and face region (craniofacial abnormalities).
It is not known whether the adverse effects of phenytoin during fetal development are due to the drug itself or if they are caused by one of phenytoin’s by-products (metabolites). In addition, the potential role of other factors remains unclear, such as genetic influences that affect phenytoin metabolism or additional environmental factors (e.g. smoking). There have been reports in the medical literature that women with mutations in the methylenetetrahydrofolate reductase (MTHFR) gene are at an increased risk of having an infant with fetal hydantoin syndrome. Researchers believe that the protein product of this gene plays a role in the proper breakdown (metabolism) of phenytoin or one of its metabolites.
Another theory speculates that intermediate metabolites of phenytoin are responsible for its teratogenesis. These intermediate metabolites are free radicals that bind to DNA, proteins and lipids adversely affecting neurodevelopment. Genetic differences in formation of these free radicals, drug clearance, and repair mechanisms may explain different susceptibility across individuals.
Determining the precise, underlying reasons why fetal hydantoin syndrome develops, requires further research to discover the specific genetic and environmental factors that play a role in the development of the disorder.
Other anti-seizure medications can cause a characteristic pattern of mental and physical birth defects similar to those seen in infants exposed to phenytoin during pregnancy. Such drugs include valproate, carbamazepine, primidone, and phenobarbital. Studies have indicated that fetal valproate syndrome is associated with greater risk of neurological and cognitive abnormalities than other anti-seizure medications. Fetal valproate syndrome is a rare condition that is caused by exposure of the unborn baby to valproic acid or sodium valproate during the first three months of pregnancy (the first trimester). Valproic acid or sodium valproate is a medication used to treat certain types of seizures (epilepsy), bipolar disorder (BPD) and migraines. Although many babies exposed to valproic acid or sodium valproate are born healthy, a small percentage of pregnant women who take this medication can have a baby born with fetal valproate syndrome. The exact prevalence of this condition remains to be established. Symptoms of fetal valproate syndrome may include neural tube defects such as spina bifida, distinctive facial features, congenital heart defects and other musculoskeletal abnormalities.
Fetal hydantoin syndrome prevention
The International League Against Epilepsy recommends that all women with epilepsy be managed in close association with a neurologist and obstetrician 12. Counseling is recommended for women to discuss the need to control seizures, the adverse effects and the teratogenicity of anti-epileptic drugs during pregnancy. Therapeutic drug monitoring in the antenatal period is a must when phenytoin and phenobarbitone are being used and should be done monthly. Also, it is recommended that women taking phenytoin take folic acid supplements, both before conception and during pregnancy as a preventive measure against malformations. According to the U.S. Centers for Disease Control and Prevention (CDC), the use of pre-conception folate of 4 mg (4,000 microgram folic acid) per day beginning 1 month prior to conception in planned pregnancies and all women with epilepsy in childbearing age and continuing for 3 months into pregnancy 13. If you’re not planning to become pregnant, you should get 400 mcg (400 microgram) of folic acid daily.
It is recommended that women be treated with a single anti-seizure (antiepileptic or anticonvulsant) medication prior to becoming pregnant and throughout pregnancy, since it appears that children exposed to multiple anticonvulsants may be at a greater risk for significant birth defects 11. The International League Against Epilepsy also performed a questionnaire-based global survey of guidelines on the management of epilepsy in pregnant females and found that almost two-thirds of their national chapters had guidelines for such patients, although a significant proportion of these were last reviewed prior to 2014 14. Also, there was a wide variation in the folate dose recommended for women with epilepsy.
Fetal hydantoin syndrome signs and symptoms
The range and severity of associated mental and physical birth defects associated with fetal hydantoin syndrome can vary greatly from one infant to another. Symptoms may not be noticeable at birth (congenital), but will become apparent as an affected child grows older. Babies with fetal hydantoin syndrome may be born with some of the following health problems 15, 1, 2, 5, 6:
- Growth deficiency
- Developmental delay
- Cleft palate
- Certain facial characteristics
- Heart defects
- Genitourinary abnormalities
- Abnormalities of the fingers and nails
Microcephaly (baby’s head is smaller than expected), growth restriction, impaired cognition, hernias and hypospadias have also been reported in a few patients 1. Affected infants may be small at birth due to growth deficiency during development (prenatal growth deficiency) 11. Growth deficiency may be mild to moderate in severity and can continue during the newborn period (postnatal growth deficiency). Congenital heart diseases have also been reported in such newborns and include valvular stenosis, coarctation of the aorta and ventricular septal defects 16.
Distinctive facial features may be present including a flat, broad bridge of the nose; a short nose; eyes that are farther apart from each other than usual (hypertelorism); crossed eyes (strabismus); eyelids that droop (ptosis); a large, wide mouth; malformed ears; mild webbing of the neck (pterygium colli); and microcephaly. Affected infants often have a gap or cleft of missing tissue of the upper lip (cleft lip) and/or a gap or cleft of missing tissue on the roof of the mouth (cleft palate).
Affected infants may also exhibit stiff, tapered fingers, underdeveloped fingers and toes, toes that resembled fingers (digitalized toes), and malformed, underdeveloped fingernails and toenails. An increased number of fingerprint arches have also been noted. Some infants may have increased hair on the body and face.
Some infants and children may experience delays in reaching developmental milestones such as learning to sit up or crawl (developmental delays). As affected children grow older, the developmental delays improve, but studies suggest that children may remain slightly behind unexposed siblings. The neurological effects of phenytoin exposure in utero have not been clearly established by studies, which have demonstrated conflicting results. Borderline to mild intellectual disability has been reported in some cases, and some studies have suggested that children exposed to phenytoin in the womb have a greater risk of developing learning disabilities, particularly in verbal skills. Reports in the medical literature disagree as to the likelihood of infants with fetal hydantoin syndrome experiencing developmental delays or intellectual disability. The exact risk of these findings in these children is not fully understood. More research is necessary to determine the specific long-term risks in neurological development of infants and children exposed to phenytoin in utero.
Additional symptoms occurring with varying frequencies have been reported in the medical literature including congenital heart defects, cardiac rhythm disturbances, behavioral abnormalities such as attention deficit hyperactivity disorder, ocular defects including nearsightedness (myopia), joint laxity, kidney abnormalities, and inguinal and umbilical hernia. Inguinal hernia is when a portion of the intestines pushes through the muscular layers of the abdominal wall. An umbilical hernia is when the intestines or fatty tissue pushes through the area near the bellybutton.
Case reports in the medical literature have suggested that infants with fetal hydantoin syndrome may be at an increased risk for the occurrence of certain benign or malignant tumors such as neuroblastoma, Wilm’s tumor, or ectodermal tumors, but such an increased risk is not proven 11.
Fetal hydantoin syndrome diagnosis
There is no diagnostic testing that can identify fetal hydantoin syndrome 11. Fetal hydantoin syndrome diagnosis is made clinically based upon identification of characteristic symptoms in an affected infant in combination with a history of phenytoin exposure during pregnancy. It is important to note that the majority of infants born to women who take phenytoin during pregnancy will not develop fetal hydantoin syndrome 11.
Fetal hydantoin syndrome treatment
The treatment of fetal hydantoin syndrome is directed toward the specific symptoms that are apparent in each individual. Treatment may require the coordinated efforts of a team of specialists. Pediatricians, oral surgeons, plastic surgeons, neurologists, psychologists, and other healthcare professionals may need to systematically and comprehensively plan an affect child’s treatment 11.
Infants with fetal hydantoin syndrome can benefit from early developmental intervention to ensure that affected children reach their potential. Affected children may benefit from occupational, physical and speech therapy. Various methods of rehabilitative and behavioral therapy may be beneficial. Additional medical, social and/or vocational services may be necessary. Psychosocial support for the entire family is essential as well.
When cleft lip and/or palate are present, the coordinated efforts of a team of specialists may be used to plan an affected child’s treatment and rehabilitation. Cleft lip may be surgically corrected. Generally surgeons repair the lip when the child is still an infant. A second surgery is sometimes necessary for cosmetic purposes when the child is older. Cleft palate may be repaired by surgery or covered by an artificial device (prosthesis) that closes or blocks the opening. Surgical repair can be carried out in stages or in a single operation, according to the nature and severity of the defect. The first palate surgery is usually scheduled during the toddler period.
- Hanson JW, Smith DW. The fetal hydantoin syndrome. J Pediatr. 1975 Aug;87(2):285-90. doi: 10.1016/s0022-3476(75)80604-4[↩][↩][↩]
- Singh R, Kumar N, Arora S, Bhandari R, Jain A. Fetal hydantoin syndrome and its anaesthetic implications: a case report. Case Rep Anesthesiol. 2012;2012:370412. doi: 10.1155/2012/370412[↩][↩][↩][↩]
- Hegde A, Kaur A, Sood A, Dhanorkar M, Varma HT, Singh G, Saini AG, Kumar P. Fetal Hydantoin Syndrome. J Pediatr. 2017 Sep;188:304. https://www.jpeds.com/article/S0022-3476(17)30639-X/fulltext[↩][↩]
- Easton JD. Potential hazards of hydantoin use. Ann Intern Med. 1972 Dec;77(6):998-9. doi: 10.7326/0003-4819-77-6-998[↩]
- Jones K I, editor. Smith’S Recognizable Patterns of Human Malformation. 5th edition. Philadelphia, Pa, USA: W.B. Saunders; 1997.[↩][↩]
- Hanson JW. Teratogen update: fetal hydantoin effects. Teratology. 1986 Jun;33(3):349-53. doi: 10.1002/tera.1420330314[↩][↩]
- Aggarwal S, Barman M, Poudel B, Joshi K, Devi R, Singh P, Priyadarshi M, Chaurasia S, Basu S. Fetal Hydantoin Syndrome: A Case Report. Cureus. 2023 Nov 29;15(11):e49663. doi: 10.7759/cureus.49663[↩][↩]
- Speidel BD, Meadow SR. Maternal epilepsy and abnormalities of the fetus and newborn. Lancet. 1972 Oct 21;2(7782):839-43. doi: 10.1016/s0140-6736(72)92209-x[↩][↩]
- Hernández-Díaz S, Werler MM, Walker AM, Mitchell AA. Folic acid antagonists during pregnancy and the risk of birth defects. N Engl J Med. 2000 Nov 30;343(22):1608-14. doi: 10.1056/NEJM200011303432204[↩][↩]
- Oguni M, Osawa M. Epilepsy and pregnancy. Epilepsia. 2004;45 Suppl 8:37-41. doi: 10.1111/j.0013-9580.2004.458008.x[↩][↩][↩]
- Fetal Hydantoin Syndrome. https://rarediseases.org/rare-diseases/fetal-hydantoin-syndrome[↩][↩][↩][↩][↩][↩][↩][↩]
- Tomson T, Battino D, Bromley R, Kochen S, Meador K, Pennell P, Thomas SV. Management of epilepsy in pregnancy: a report from the International League Against Epilepsy Task Force on Women and Pregnancy. Epileptic Disord. 2019 Dec 1;21(6):497-517. doi: 10.1684/epd.2019.1105[↩]
- About Folic Acid. https://www.cdc.gov/folic-acid/about/[↩]
- Tomson T, Battino D, Bromley R, Kochen S, Meador KJ, Pennell PB, Thomas SV. Global Survey of Guidelines for the Management of Epilepsy in Pregnancy: A report from the International League Against Epilepsy Task Force on Women and Pregnancy. Epilepsia Open. 2020 Aug 5;5(3):366-370. doi: 10.1002/epi4.12420[↩]
- Phenytoin (Dilantin). https://www.chop.edu/conditions-diseases/phenytoin-dilantin[↩]
- Godbole KG, Gambhir PS, Deshpande AS, Kurlekar SU, Phadke MA. Fetal hydantoin syndrome with rheumatic valvular heart disease. Indian J Pediatr. 1999 Mar-Apr;66(2):290-3. doi: 10.1007/BF02761222[↩]





{kind=link}