Contents
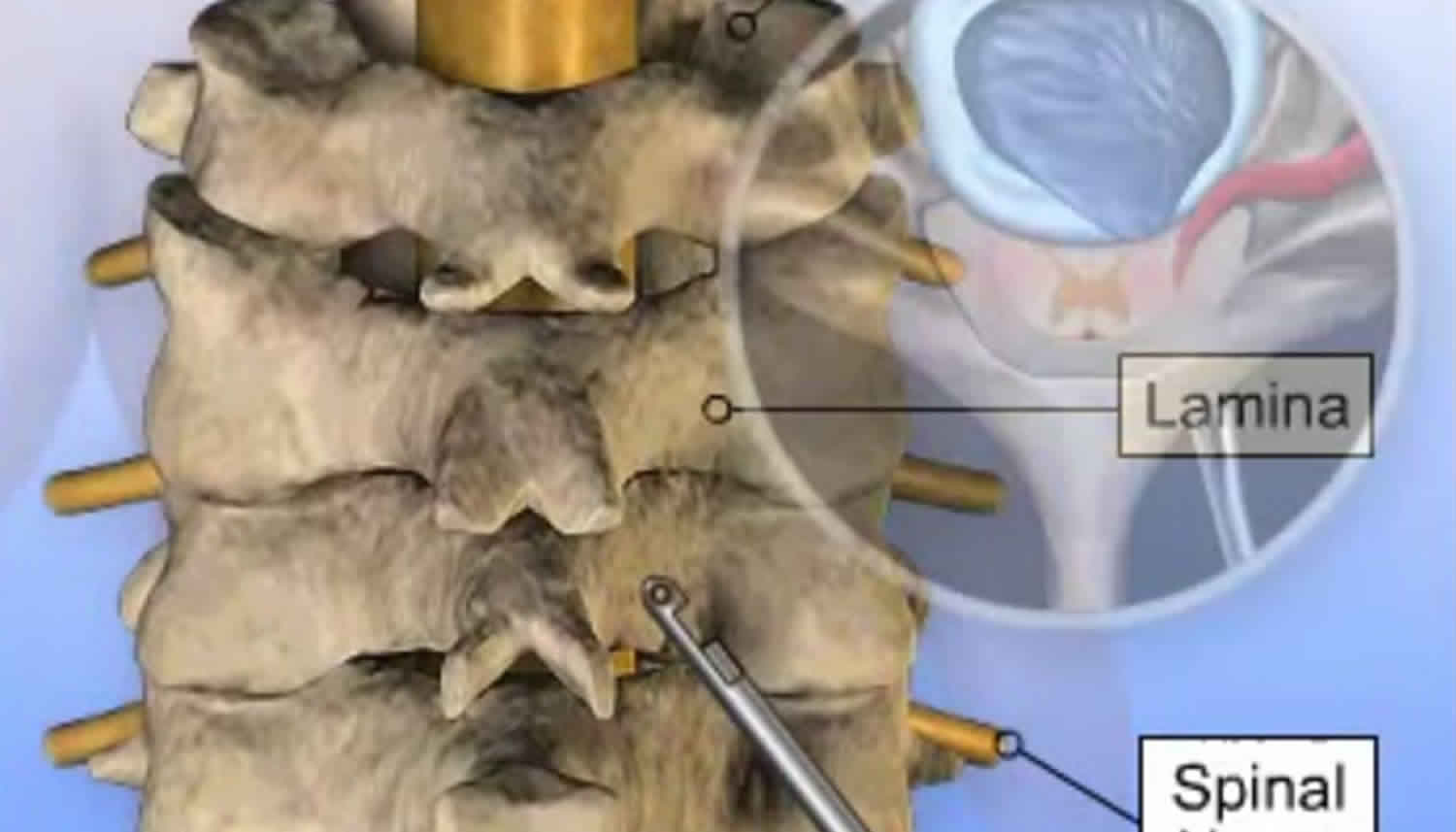
What is a foraminotomy
Foraminotomy is a decompression surgery that widens the passageway in your back where spinal nerve root leave your spinal canal. You may have a narrowing of the nerve opening (foraminal stenosis). Foramenotomies are typically performed in conjunction with a laminotomy, laminectomy or microdiscectomy.
Foraminotomy takes pressure off of the nerve coming out of your spinal column. This reduces any pain you were having. Foraminotomy can be performed on any level of the spine.
You will be asleep and feel no pain (general anesthesia).
During a foraminotomy, the spine surgeon removes bone or tissue that obstructs the passageway and pinches the spinal nerve root, which can cause inflammation and pain. The nerve passageways are called neuroforamen.
The neuroforamen are passageways that are naturally formed on either side between an upper and lower vertebra. In between each upper and lower vertebra is an intervertebral disc. The height of the disc separates the two vertebrae and creates the size of the neuroforamen.
During your foraminotomy surgery:
- You’ll lie face down or sit up on the operating table. A cut (incision) is made in the middle of the back of your spine. The length of the incision depends on how much of your spinal column will be operated on.
- Skin, muscles, and ligaments are moved to the side. Your surgeon may use a surgical microscope to see inside your back.
- Some bone is cut or shaved away to open the nerve root opening (foramen). Any disk fragments are removed.
- Other bone may also be removed at the back of the vertebrae to make more room (laminotomy or laminectomy).
- The surgeon may do a spinal fusion to make sure your spinal column is stable after surgery.
- The muscles and other tissues are put back in place. The skin is sewn together.
Figure 1. Lumbar foraminotomy
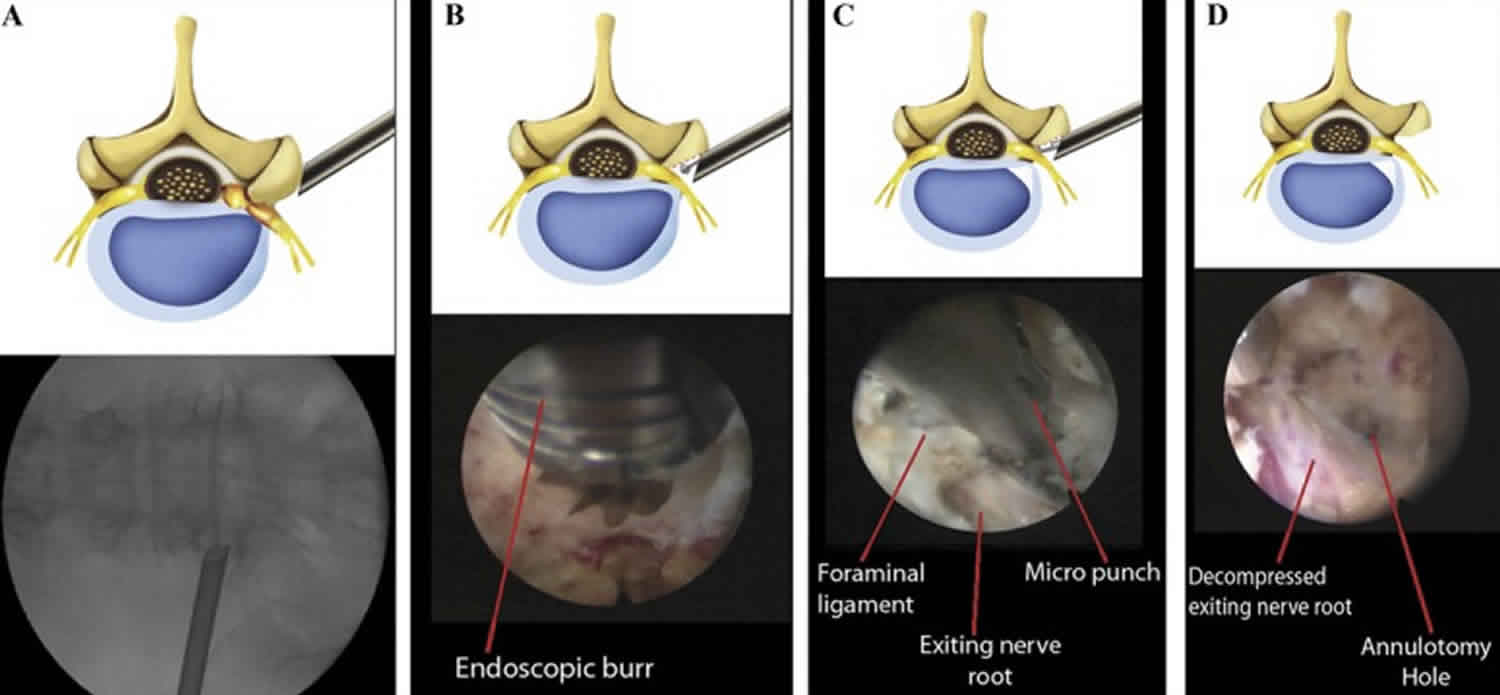
Footnote: Schematic illustrations and corresponding intraoperative fluoroscopic and endoscopic views of the surgical procedure. A, extraforaminal placement of the working cannula for foraminal decompression. B, foraminal unroofing using an endoscopic burr. C, sophisticated foraminal decompression using various instruments, including punches, forceps, and a laser. Note the exiting nerve root decompression using a micropunch. D, final view of the full-scale foraminal decompression status. Note the decompressed exiting nerve root and annulotomy site.
[Source 1 ]Posterior cervical foraminotomy
Posterior cervical foraminotomy is a surgical solution performed to relieve the painful symptoms of compromised spinal nerves. Your spine surgeon performs this procedure through an incision in your back to make more space for the spinal nerve to pass through.
Posterior cervical foraminotomy surgery removes bone and/or portions of a herniated or diseased disc to relieve the symptoms described above. Neck pain and radiating arm pain often result when parts of a disc press against nerve roots in your spine. The procedure is described below. Ask your physician about the risks that apply to your case, as well as what you can expect from the recovery.
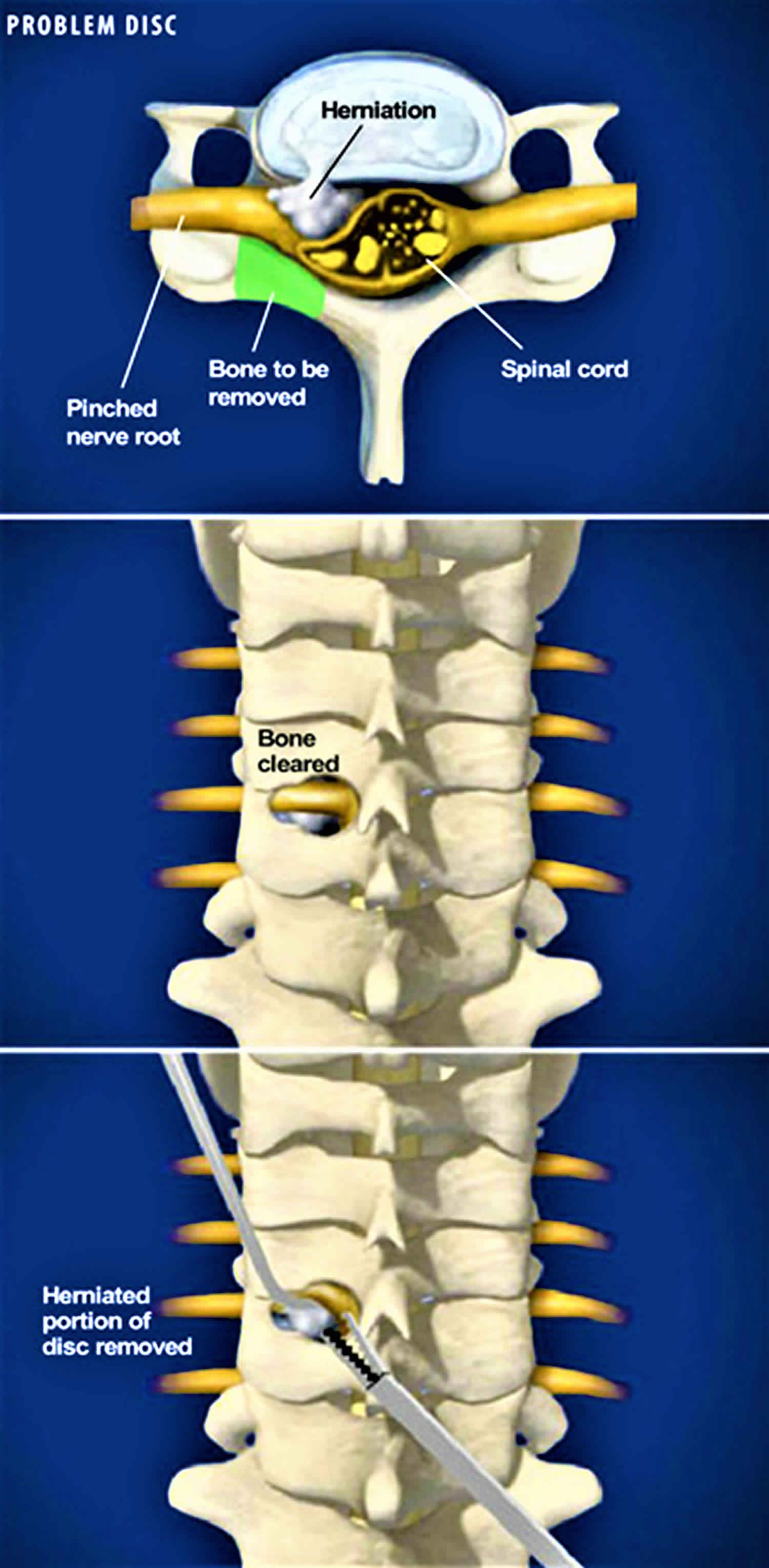
Figure 2. Posterior cervical foraminotomy
1. Preparing for the posterior cervical foraminotomy surgery
You are placed face down on the operating table. After the anesthesia has taken effect, your board certified surgeon performs this procedure through an incision in the back of your neck to expose the bony roof of the spine. This incision leaves a minimal scar.
2. Identifying a herniated disc
Identifying the cause of your pain. If the cause is a herniated disc, your surgeon first confirm the location of the damaged disc. A disc herniation may compress the nerve root against the roof of the spinal canal. The highlighted area in the illustration (Figure 2) represents the bone section the surgeon will remove during this procedure.
3. Accessing the nerve root
The surgeon clears away bone and soft tissue to access the pinched nerve root and the herniated disc in your spinal canal. This procedure also reduces pressure on the nerve root. In a cervical posterior foraminotomy, the surgeon chisels away the bone to widen the passageway for the nerve.
4. Checking the nerve
Once he has cleared the bone away from the nerve, the surgeon checks to ensure that the nerve has freedom from impingement, as shown in the second illustration (Figure 2).
5. Removing the fragment
If your surgeon finds a fragment of herniated disc beneath the nerve root, he removes it. A successful cervical posterior foraminotomy results in an uncompressed nerve root, freeing you from pain.
Why foraminotomy surgery is performed
A bundle of nerves (nerve root) leaves your spinal cord through openings in your spinal column. These openings are called the neural foramens. When the openings for the nerve root become narrow, it can put pressure on your nerve. This condition is called foraminal spinal stenosis.
Foraminotomy surgery may be considered if you have severe symptoms that interfere with your daily life. Symptoms include:
- Pain that may be felt in your thigh, calf, lower back, shoulder, arms or hands. The pain is often deep and steady
- Pain when doing certain activities or moving your body a certain way
- Numbness, tingling, and muscle weakness
Who are good candidates for foraminotomy?
Ideal candidates for a foraminotomy may experience varying symptoms and may have diverse spinal conditions, but most have foraminal stenosis. Candidates should have neck or back pain for at least 3 months and experience one or more of the following symptoms:
- Acute or chronic pain in the neck or back that is dull, deep, constant, shooting, throbbing, sharp, or radiating to the extremities
- Pain that radiates from the lower back to the buttocks, legs, calves, feet, and/or toes
- Pain that radiates from the neck to the shoulders, arms, hands, and/or fingers
- Weakness, numbness, or tingling sensation felt in the muscles and/or the extremities
- Limited motor functions
- Difficulty performing daily activities or partaking in physical activity
- Difficulty standing, walking, or sitting for varying periods of time
- Past failed attempts at relieving pain with conservative methods of treatment
Additionally, ideal candidates should acknowledge the possibility of physical therapy as part of their recovery. Patients should also be optimistic towards successful pain improvement and management.
Foraminotomy surgery risks
Risks of anesthesia and surgery in general are:
- Reactions to medicines or breathing problems
- Bleeding, blood clots, or infection
Risks of foraminotomy are:
- Infection in wound or vertebral bones
- Damage to a spinal nerve, causing weakness, pain, or loss of feeling
- Partial or no relief of pain after surgery
- Return of back pain in the future
Before the foraminotomy procedure
You will have an MRI to make sure foraminal stenosis is causing your symptoms.
Tell your health care provider what medicines you are taking. This includes medicines, supplements, or herbs you bought without a prescription.
During the days before the foraminotomy surgery:
- Prepare your home for when you leave the hospital after surgery.
- If you are a smoker, you need to stop. Your recovery will be slower and possibly not as good if you continue to smoke. Ask your doctor for help.
- Two weeks before surgery, your doctor or nurse may ask you to stop taking medicines that make it harder for your blood to clot. These include aspirin, ibuprofen (Advil, Motrin), naproxen (Aleve, Naprosyn).
- If you have diabetes, heart disease, or other medical problems, your surgeon will ask you to see your regular doctor.
- Talk with your doctor if you have been drinking a lot of alcohol.
- Ask your doctor which medicines you should still take on the day of the surgery.
- Let your doctor know right away if you get a cold, flu, fever, herpes breakout, or other illnesses.
- You may want to visit a physical therapist to learn exercises to do before surgery and to practice using crutches.
On the day of the foraminotomy surgery:
- You will likely be asked not to drink or eat anything for 6 to 12 hours before the procedure.
- Take the medicines your doctor told you to take with a small sip of water.
- Bring your cane, walker, or wheelchair if you have one already. Also bring shoes with flat, nonskid soles.
- Arrive at the hospital on time.
Foraminotomy procedure
A foraminotomy usually takes about 1 to 2 hours to complete, depending on the patient’s spinal conditions and its complexity. The patient will be under general anesthesia during the procedure.
The following are the general steps of the foraminotomy procedure:
- The procedure begins with the prepping of area on the back or neck for the incision. After creating a small one to three inch incision, the skin, muscles, and tissues are separated so the surgeon can operate.
- A small amount of bone (a laminotomy) may be removed to expose the foraminal canal. Any abnormal spinal structures present like disc material or excessive ligaments are removed to decompress the nerve roots.
- If a herniated or bulging disc is present, then a microdiscectomy or a discectomy may be performed to remove part or most of the disc material. A fusion may also be performed if instability may become an issue.
- The nerves are now decompressed, and the procedure ends when the surgeon closes the incision with sutures.
Foraminotomy recovery time
You will likely wear a soft neck collar afterward if the foraminotomy surgery was on your neck. Most people are able to get out of bed and sit up within 2 hours after foraminotomy surgery. You will need to move your neck carefully.
You should be able to leave the hospital the day after the foraminotomy surgery. At home, follow instructions on how to care for your wound and back.
You should be able to drive within a week or two and resume light work after 4 weeks.
Foraminotomy prognosis
Foraminotomy for spinal foraminal stenosis will often provide full or some relief of symptoms.
Future spine problems are possible for people after spine surgery. If you had foraminotomy and spinal fusion, the spinal column above and below the fusion could have problems in the future.
You may have more of a chance of future problems if you needed more than one kind of procedure in addition to the foraminotomy (laminotomy, laminectomy, or spinal fusion).
Foraminotomy success rate
Studies on posterior foraminotomy reported good outcomes in 64% to 96% of patients and re-operation rates of around 4% to 7% 2. The few studies exclusively investigating anterior cervical foraminotomy and fusion reported 83% to 91% good results and re-operation rates of 4% to 14% 3.
Other studies have reported for the success rates for open paraspinal foraminotomy are as high as 72% to 83% 4 and this technique has been considered the gold standard for the surgical treatment of lumbar foraminal or far lateral stenosis 1. However, some patients experience postoperative leg pain or dysesthesia, which are the primary causes of unfavorable outcomes 5. Excessive manipulation of the dorsal root ganglion is thought to cause dysesthesia 6. Moreover, a limited field of view in the paraspinal approach may lead to incomplete decompression. To solve the above problems, various minimally invasive techniques have been developed. Some authors have reported the use of a technique known as percutaneous endoscopic foraminal discectomy and/or foraminoplasty 7.
- Ahn Y, Oh HK, Kim H, Lee SH, Lee HN. Percutaneous endoscopic lumbar foraminotomy: an advanced surgical technique and clinical outcomes. Neurosurgery. 2014;75(2):124-33; discussion 132-3. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4086756/[↩][↩]
- Schöggl A, Reddy M, Saringer W, Ungersböck K. Social and economic outcome after posterior microforaminotomy for cervical spondylotic radiculopathy. Wien Klin Wochenschr. 2002;114:200–204.[↩]
- Brigham CD, Tsahakis PJ. Anterior cervical foraminotomy and fusion: surgical technique and results. Spine (Phila Pa 1976) 1995;20:766. doi: 10.1097/00007632-199504000-00004[↩]
- Chang HS, Zidan I, Fujisawa N, Matsui T. Microsurgical posterolateral transmuscular approach for lumbar foraminal stenosis. J Spinal Disord Tech. 2011;24(5):302-307[↩]
- Epstein NE. Foraminal and far lateral lumbar disc herniations: surgical alternatives and outcome measures. Spinal Cord. 2002;40(10):491-500[↩]
- Hodges SD, Humphreys SC, Eck JC, Covington LA. The surgical treatment of far lateral L3-L4 and L4-L5 disc herniations. A modified technique and outcomes analysis of 25 patients. Spine (Phila Pa 1976). 1999;24(12):1243-1246[↩]
- Schubert M, Hoogland T. Endoscopic transforaminal nucleotomy with foraminoplasty for lumbar disk herniation. Oper Orthop Traumatol. 2005;17(6):641-661[↩]





{kind=link}