
What is gastrin
Gastrin is a peptide hormone produced and secreted by the stomach antrum “G cells” and gastrin interacts with the cholecystokinin-B receptor (CCKBR) on enterochromaffin-like and parietal cells to induce gastric hydrochloric acid (HCl) secretion 1. G-cells secrete gastrin into systemic circulation, which allows delivery of gastrin to parietal cells and enterochromaffin-like cells in the gastric fundus and cardia. When food is eaten, the antrum of the stomach becomes distended and the presence of food stimulates the release of gastrin. Gastrin in turn stimulates parietal cells to produce gastric hydrochloric acid (HCl). Acidity helps to digest food and the rise in acidity eventually suppresses gastrin release. This feedback system normally results in low concentrations of gastrin in the blood, especially in the fasting state. Rare conditions such as G-cell hyperplasia and gastrinomas, including Zollinger-Ellison syndrome, can cause an overproduction of gastrin and gastric acid. This can lead to aggressive peptic ulcers that can be difficult to treat.
Gastrin is a linear peptide that is initially synthesized as preprogastrin 2. Preprogastrin undergoes post-translation cleavage which produces a family of gastrin peptides of variable lengths, the most common being ‘Big’ gastrin, which is a peptide comprised of 34 amino acids the mature 34-amino acid, called gastrin-34. The bioactivity of gastrin is preserved in a 5 amino acid sequence called “pentagastrin,” found at the 5 C-terminal of all members of the gastrin family, regardless of the overall size of the gastrin peptide. The 5 C-terminal amino acids of gastrin and cholecystokinin (CCK) are identical 3. Gastrin-34 may be cleaved further into the shorter 17-amino acid, gastrin-17. Either may be secreted as a c-terminal amidated or unamidated isoform. A number of additional, smaller gastrin fragments, as well as gastrin molecules with atypical posttranslational modifications (eg, absent sulfation), may also be secreted in small quantities. Gastrin half-life is short, 5 minutes for amidated gastrin-17, and 20 to 25 minutes for amidated gastrin-34. Elimination occurs through peptidase cleavage and renal excretion.
Gastrin-17 I (nonsulfated form) and gastrin-17 II (sulfated) appear equipotent. Their biological effects are chiefly associated with the amidated isoforms and consist of promotion of gastric epithelial cell proliferation and differentiation to acid-secreting cells, direct promotion of acid secretion, and indirect stimulation of acid production through histamine release. In addition, gastrin stimulates gastric motility and release of pepsin and intrinsic factor. Most gastrin isoforms with atypical posttranslational modifications and most small gastrin fragments display reduced or absent bioactivity. This assay measures predominately gastrin-17. Larger precursors and smaller fragments have little or no cross-reactivity in the assay.
Intraluminal stomach pH is the main factor regulating gastrin production and secretion. Rising gastric pH levels result in increasing serum gastrin levels, while falling pH levels are associated with mounting somatostatin production in gastric D cells. Somatostatin, in turn, downregulates gastrin synthesis and release. Other weaker factors that stimulate gastrin secretion are gastric distention, protein-rich foods, and elevated secretin or serum calcium levels.
Serum gastrin levels may also be elevated in gastric distention due to gastric outlet obstruction, and in a variety of conditions that lead to real or functional gastric hypo- or achlorhydria (gastrin is secreted in an attempted compensatory response to achlorhydria). These include atrophic gastritis with or without pernicious anemia, a disorder characterized by destruction of acid-secreting (parietal) cells of the stomach; gastric dumping syndrome; and surgically excluded gastric antrum. In atrophic gastritis, the chronic cell-proliferative stimulus of the secondary hypergastrinemia may contribute to the increased gastric cancer risk observed in this condition.
Gastrin levels are pathologically increased in gastrinoma, a type of neuroendocrine tumor that can occur in the pancreas (20%-40%) or in the duodenum (50%-70%). The triad of nonbeta islet cell tumor of the pancreas (gastrinoma), hypergastrinemia, and severe ulcer disease is referred to as the Zollinger-Ellison syndrome. Over 50% of gastrinomas are malignant and can metastasize to regional lymph nodes and the liver. About 25% of gastrinomas occur as part of the multiple endocrine neoplasia type 1 (MEN 1) syndrome and are associated with hyperparathyroidism and pituitary adenomas. These MEN 1-associated tumors have been observed to occur at an earlier age than sporadic tumors and often follow a more benign course.
Figure 1. Stomach
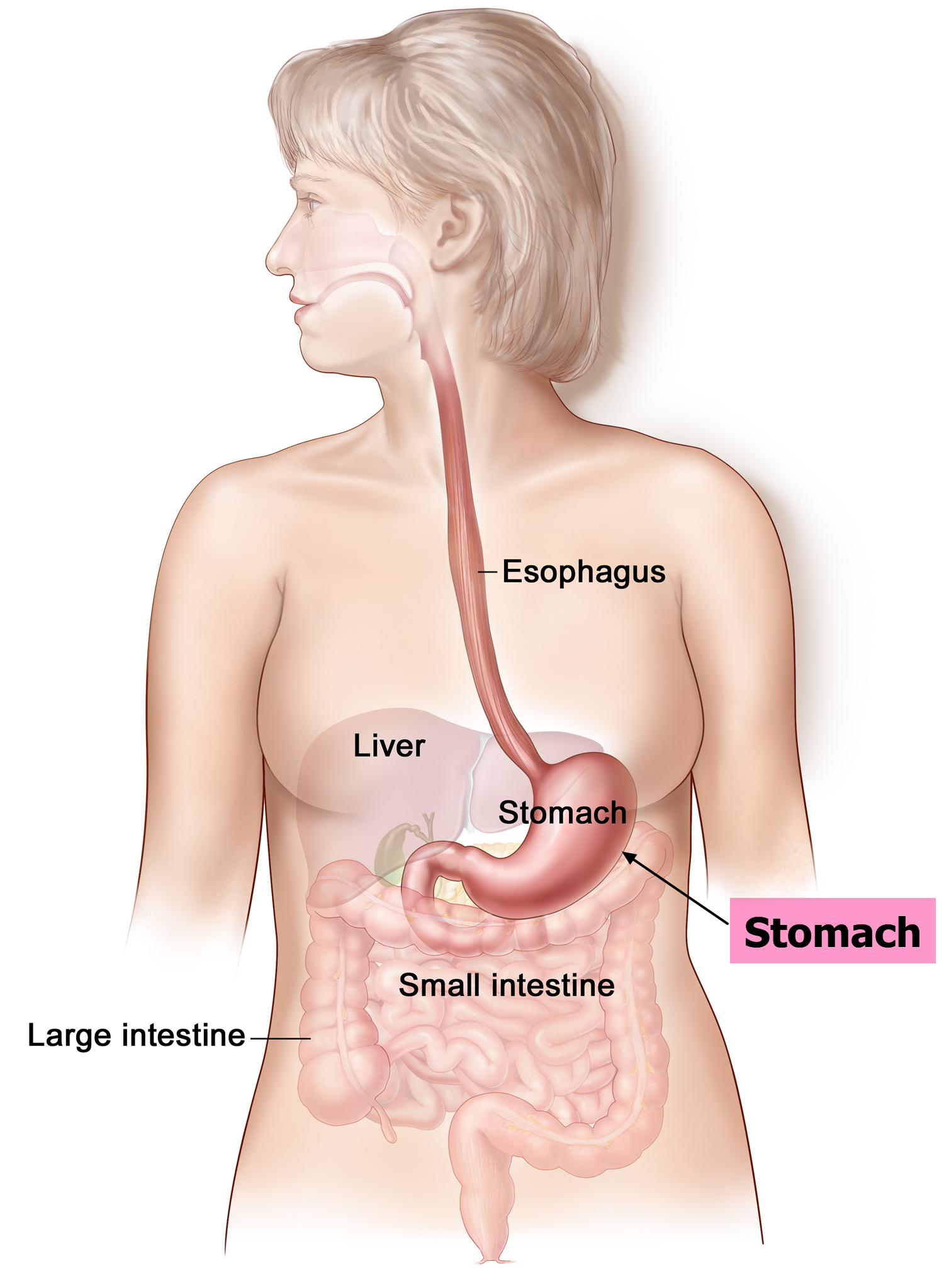
Figure 2. Parts of the stomach
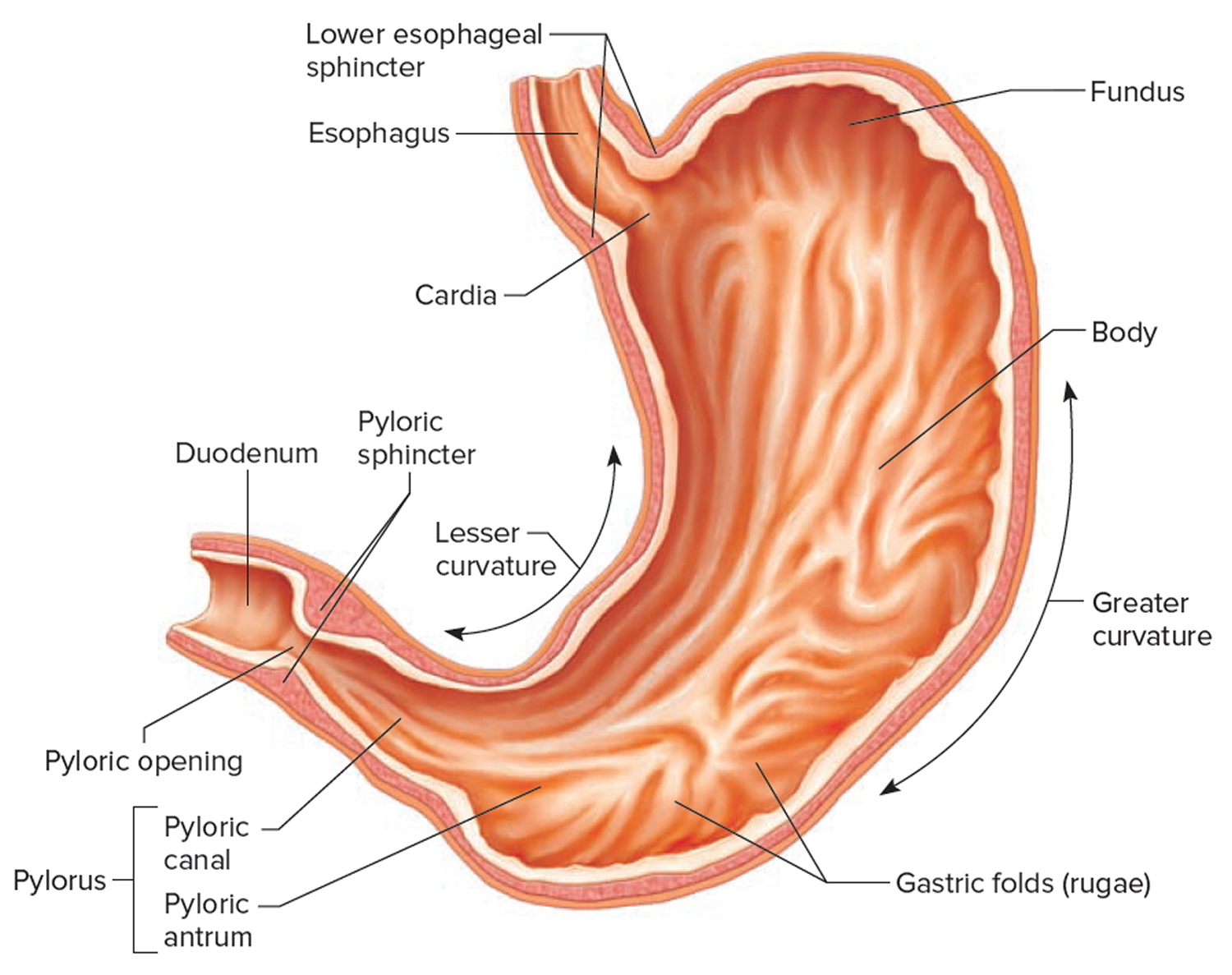
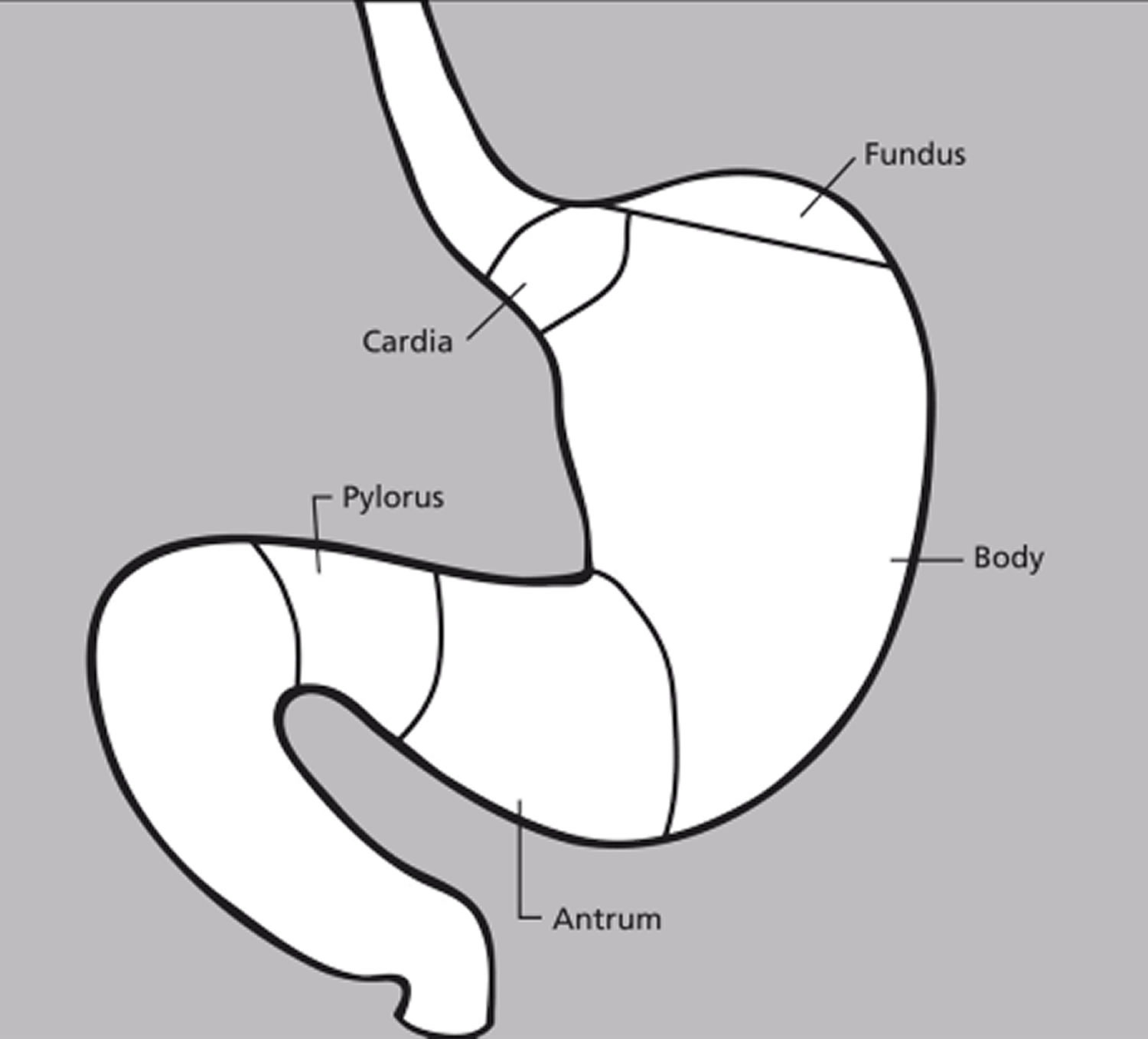
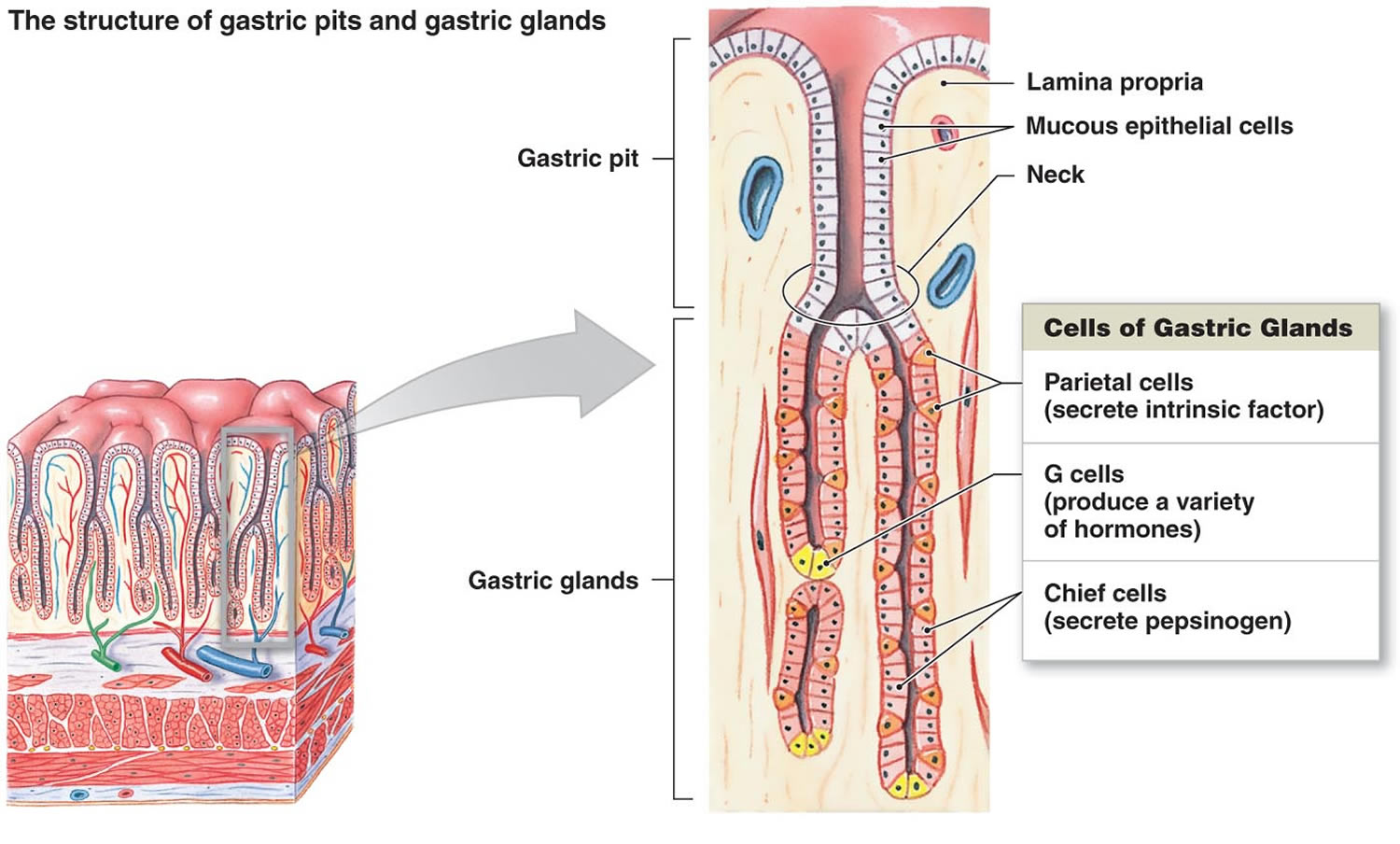
Figure 3. Stomach cells (gastric glands)
Where is gastrin produced?
Gastrin is a peptide hormone produced and secreted by the stomach antrum “G cells”.
G cells are primarily found in the pyloric antrum but can also be found in the duodenum and the pancreas. G cells secrete gastrin when stimulated directly by vagal efferent neurons as well as gastrin-releasing peptide neurons 2. Gastrin-releasing peptide neurons are stimulated by the presence of amino acids in the stomach, gastric distention, as well as vagal efferent stimulation. Gastrin secreted by these cells primarily acts on parietal cells and enterochromaffin-like cells (ECL cells) in the gastric pits of the stomach, but also interacts with gastric smooth muscle cells, acinar cells of the pancreas, lymphocytes, polymorphonuclear leukocytes, and endothelial cells. Hence gastrin stimulates hydrochloric acid (HCl) secretion directly and by activating the enterochromaffin-like cells to secrete histamine which also results in hydrochloric acid (HCl) production.
Parietal cells, found in the pits of the gastric fundus and cardia, secrete hydrochloric acid into the lumen of the stomach via K (potassium)/H (hydrogen) ATPase on the apical (luminal) membrane. Gastrin binds cholecystokinin (CCK) B receptors on the basal membrane of parietal cells to induce expression of K/H ATPase. Increased expression and activity of the K/H ATPase results in increased secretion of hydrogen ions (gastric acid) into the stomach.
Enterochromaffin-like cells, found in the gastric pits of the fundus and cardia of the stomach, secrete histamine which then binds histamin-2 (H2) receptors on the neighboring parietal cells and further potentiate the secretion of gastric acid by the parietal cells.
Acinar cells, found in the pancreas, are responsible for the synthesis, storage, and secretion of pancreatic digestive enzymes. Gastrin binds cholecystokinin-2 receptors on the acinar cells, inducing secretion of the cell’s stored digestive enzymes 4.
Gastrin function
Gastrin is a peptide hormone primarily responsible for enhancing gastric mucosal growth, gastric motility, and secretion of hydrochloric acid (HCl) into the stomach 2. Gastrin is present in the G cells of the gastric antrum and duodenum. Gastrin is secreted into the blood and carried to the gastric fundus and cardia where the majority of hydrochloric acid (HCl) secreting parietal cells are found. Hydrochloric acid (HCl) is necessary for the conversion of inactive pepsinogen to active pepsin, protein digestion in the stomach, as well as the release of cobalamin (vitamin B12) from its salivary R-protein carrier. Also, there appears to be data emerging that suggests gastrin might have a role in certain cancers such as gastric cancer.
Gastrin is primarily released in response to vagal and gastrin-releasing peptide stimulation secondary to ingestion of peptides, amino acids, gastric distention, and an elevated stomach pH 5. Conversely, gastrin release is decreased in response to paracrine inhibition by somatostatin and decreased stomach pH.
Gastrin has also been found to interact with acinar cells of the pancreas, gastric smooth muscle cells, endocrine cells, and some white blood cells (e.g., monocytes, lymphocytes) and mast cells. Gastrin stimulates the proliferation of gastric mucosal endocrine cells (parietal cells, enterochromaffin-like cells cells). This trophic quality of gastrin may be related to potentiation of some cancers.
In addition, gastrin and its derivatives stimulate cell division and inhibit apoptosis on several cell types, suggesting that gastrin and its derivatives might promote carcinogenesis 6. Gastrin and cholecystokinin (CCK) are members of a family of neuroendocrine peptides and are both physiological ligands of the cholecystokinin-B receptor (CCKBR).
Gastrin has been found to modulate immunity and inflammation via cholecystokinin-B/gastrin receptor expressing white blood cells. Specifically, cholecystokinin-B expression has been recorded in some polymorphonuclear leukocytes, mononuclear cells, and endothelial cells. It has demonstrated the ability to stimulate mast cell release of histamine, lymphocytic secretion of IL-2, endothelial expression of VCAM-1 and P-selectin, as well as endothelial secretion of IL-8 7.
What does gastrin do
The effects of gastrin are primarily mediated via binding of the cholecystokinin-B (CCKB) receptor. The cholecystokinin-B (CCKB) receptor is a G-protein coupled receptor which, upon activation by gastrin, starts downstream signaling via the phospholipase C – diacylglycerol + inositol trisphosphate – calcium – protein kinase C cascade 8.
The cholecystokinin-B (CCKB) receptor is primarily found in the central nervous system (CNS), and gastrointestinal (GI) system but is also expressed on endothelial cells and some white blood cells.
Cholecystokinin-B (CCKB) receptors can also induce signaling pathways through tyrosine kinase receptors to a more limited degree and have been demonstrated in the transactivation of epidermal growth factor receptor (EGFR).
Gastrin blood test
The gastrin blood test measures the amount of the hormone gastrin in blood to help evaluate an individual with recurrent peptic ulcers and/or other serious abdominal symptoms.
The gastrin blood test is primarily used to help detect excess production of gastrin and gastric acid. The main clinical indication for assaying gastrin is to help diagnose gastrin-producing tumors called gastrinomas, Zollinger-Ellison syndrome (a gastrin-producing tumor resulting in recurrent, treatment-refractory peptic ulcer disease and diarrhea) and hyperplasia of G-cells. G-cells are specialized cells in the stomach that produce gastrin, which in turn increases the production of gastric acid.
A gastrin blood test may also be used to monitor for recurrence following the surgical removal of a gastrinoma. Gastrinomas are gastrin-producing tumors. Zollinger-Ellison syndrome is a condition caused by the presence of one or more gastrinomas and is characterized by high gastrin levels, greatly increased gastric acid production, and by peptic ulcers. Gastrinomas usually form in the pancreas, even though the endocrine cells of the pancreas do not normally make gastrin. More than half of them are malignant, causing cancer that can spread to other parts of the body, such as the liver. Even tiny tumors can produce large quantities of gastrin.
Basal gastrin measurements is the best laboratory test for gastrinoma. A secretin-stimulated serum gastrin test may be used to provide additional information if the initial gastrin test result is moderately but not significantly elevated and the healthcare practitioner suspects that a person’s symptoms are due to a gastrinoma. This procedure involves collecting a baseline gastrin sample, giving the patient a chemical (typically the hormone secretin) to stimulate gastrin production, and then collecting additional blood samples at timed intervals for gastrin testing. The other (benign) causes of elevated gastrin will not show an increase after secretin administration.
A measurement of gastric acid pH level may sometimes be ordered along with or following a gastrin test to help diagnose Zollinger-Ellison syndrome.
Is any test preparation needed to ensure the quality of the sample?
You should fast for 12 hours and avoid alcohol for 24 hours prior to the test. Your healthcare practitioner may also ask you to refrain from taking certain stomach medications for several days prior to the test. Medications that can increase gastrin levels include antacids, H2-blocking agents (such as cimetidine), and proton pump inhibitors (such as omeprazole). These prevent the normal negative feedback in which acidity suppresses gastrin production.
When is gastrin blood test ordered?
A gastrin blood test may be ordered when a person has diarrhea, abdominal pain, and/or recurrent peptic ulcers that do not respond to treatment and that the healthcare practitioner suspects are due to excess gastrin production. A gastrin stimulation test may be ordered when a gastrin level is moderately elevated and the healthcare practitioner suspects that a person has a gastrinoma.
When a gastrin-producing tumor has been removed, a gastrin blood test may be ordered periodically as a screening test to monitor for recurrence.
Normal gastrin level
Normal gastrin level are generally less than 100 pg/mL (48.1 pmol/L).
Normal value ranges may vary slightly among different laboratories. Some labs use different measurements or test different samples. Talk to your provider about the meaning of your specific test result.
There is no evidence that fasting serum gastrin levels differ between adults and children. Although 8-hour fasts are difficult or impossible to enforce in small children, serum gastrin levels after shorter fasting periods (3-8 hours) may be 50% to 60% higher than the 8-hour fasting value.
Low or normal blood levels of gastrin are not typically of concern.
High gastrin levels
Too much gastrin can causes severe peptic ulcer disease. A higher than normal level may also be due to:
- Chronic kidney disease
- Long-term gastritis
- Over-activity of the gastrin-producing cells in the stomach (G-cell hyperplasia)
- Helicobacter pylori infection of the stomach
- Use of antacids or medicines to treat heartburn
- Zollinger-Ellison syndrome, a gastrin-producing tumor that may develop in the stomach or pancreas
- Decreased acid production in the stomach
- Previous stomach surgery
Moderately elevated levels may be seen with a variety of conditions such as Zollinger-Ellison syndrome, G-cell hyperplasia, chronic atrophic gastritis (a condition resulting from long-term inflammation of the stomach lining that leads to the loss of acid-producing cells), pernicious anemia, a pyloric obstruction (blockage at the junction of the stomach and duodenum), and chronic kidney failure.
Greatly elevated levels of gastrin in symptomatic individuals and concentrations of gastrin that increase significantly during a gastrin stimulation test indicate the likelihood that a person has Zollinger-Ellison syndrome and one or more gastrinomas. Imaging tests may be ordered as a follow up to high gastrin concentrations to locate the gastrinoma(s). The quantity of gastrin produced is not related to either the tumor size or to the number of tumors. Even tiny tumors can produce large amounts of gastrin.
Gastrin levels that were initially low after the surgical removal of a gastrinoma and then increase may signal a recurrence of the tumor. Concentrations that do not decrease after treatment may indicate that the treatment has not been fully effective.
Is there anything else I should know?
Gastrinomas can affect anyone, but people who have an inherited condition called MEN-1 (Multiple Endocrine Neoplasia, type 1) are at an increased risk. These people have genetic alterations that increase their lifetime risk of developing tumors in their pancreas or in another of their endocrine glands.
It is important to note that most stomach ulcers are not due to gastrinomas. They are commonly associated with Helicobacter pylori infections and sometimes with the use of nonsteroidal anti-inflammatory drugs (NSAIDs) such as ibuprofen.
Gastrin levels commonly increase with age and with prolonged use of medications such as antacids and proton pump inhibitors that neutralize or inhibit the production of stomach acid. They will also typically be elevated in people who are not fasting. Increases in gastrin concentration with age may reflect a general decrease in the ability to produce stomach acid.
Gastrin blood levels follow a circadian rhythm. This means that they will be at their lowest between about 3 to 7 AM. Concentrations will be higher during the day and will fluctuate in response to meals.
What is Zollinger-Ellison syndrome?
Zollinger-Ellison syndrome is a condition in which the body produces too much of the hormone gastrin. Most of the time, a small tumor (gastrinoma) in the pancreas or small intestine is the source of the extra gastrin in the blood. Zollinger-Ellison syndrome is characterized by severe recurrent peptic ulcers in the stomach, duodenum and/or the upper portion of the small intestine. The ulcers are caused by a greatly increased amount of stomach acid due to high levels of gastrin, the hormone that stimulates stomach acid production. In Zollinger-Ellison syndrome, high gastrin levels are caused by gastrin-producing tumors called gastrinomas, which usually form in the duodenum but can be found in the head of the pancreas and rarely in other parts of the body. More than half of them are malignant and can metastasize to other parts of the body, such as the liver. The tumors must be removed surgically, and sometimes total removal of the stomach is necessary to control the acid production.
Gastrinomas occur as single tumors or several tumors. One half to two thirds of single gastrinomas are cancerous (malignant) tumors. These tumors often spread to the liver and nearby lymph nodes.
Many people with gastrinomas have several tumors as part of a condition called multiple endocrine neoplasia type I (MEN I). Tumors may develop in the pituitary gland (brain) and parathyroid gland (neck) as well as in the pancreas.
Zollinger-Ellison syndrome complications may include:
- Failure to locate the tumor during surgery
- Intestinal bleeding or hole (perforation) from ulcers in the stomach or duodenum
- Severe diarrhea and weight loss
- Spread of the tumor to other organs
Zollinger-Ellison syndrome treatment
Drugs called proton pump inhibitors (omeprazole, lansoprazole, and others) are used for treating this problem. These drugs reduce acid production by the stomach. This helps the ulcers in the stomach and small intestine heal. These medicines also relieve abdominal pain and diarrhea.
Surgery to remove a single gastrinoma may be done if the tumors have not spread to other organs. Surgery on the stomach (gastrectomy) to control acid production is rarely needed.
Zollinger-Ellison syndrome prognosis
The cure rate is low, even when it is found early and the tumor is removed. However, gastrinomas grow slowly. People with this condition may live for many years after the tumor is found. Acid-suppressing medicines work well to control the symptoms.
Can’t I just take stomach medicines to address my excess gastrin and stomach acid?
Stomach medications such as proton pump inhibitors may be prescribed as part of your treatment, but it is important to diagnose your underlying condition e.g., gastrinomas. Although gastrinomas are rare, more than half of them are cancerous and can spread to other parts of your body.
- Chueca E, Lanas A, Piazuelo E. Role of gastrin-peptides in Barrett’s and colorectal carcinogenesis. World J Gastroenterol. 2012;18(45):6560-70. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3516208/[↩]
- Prosapio JG, Jialal I. Physiology, Gastrin. [Updated 2018 Nov 26]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2018 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK534822[↩][↩][↩]
- Grozinsky-Glasberg S, Alexandraki KI, Angelousi A, Chatzellis E, Sougioultzis S, Kaltsas G. Gastric Carcinoids. Endocrinol. Metab. Clin. North Am. 2018 Sep;47(3):645-660.[↩]
- Majumdar AP, Johnson LR. Gastric mucosal cell proliferation during development in rats and effects of pentagastrin. Am. J. Physiol. 1982 Feb;242(2):G135-9.[↩]
- Al-Ezzy AIA. Immunopathological and Modulatory Effects of Cag A+ Genotype on Gastric Mucosa, Inflammatory Response, Pepsinogens, and Gastrin-17 Secretion in Iraqi Patients infected with H. pylori. Open Access Maced J Med Sci. 2018 May 20;6(5):794-802[↩]
- Glycine-extended gastrin inhibits apoptosis in Barrett’s oesophageal and oesophageal adenocarcinoma cells through JAK2/STAT3 activation. Beales IL, Ogunwobi OO. J Mol Endocrinol. 2009 Apr; 42(4):305-18.[↩]
- Vinik A, Perry RR, Hughes MS, Feliberti E. Multiple Endocrine Neoplasia Type 1. In: De Groot LJ, Chrousos G, Dungan K, Feingold KR, Grossman A, Hershman JM, Koch C, Korbonits M, McLachlan R, New M, Purnell J, Rebar R, Singer F, Vinik A, editors. Endotext [Internet]. MDText.com, Inc.; South Dartmouth (MA): Oct 7, 2017.[↩]
- Smith JP, Shih AH, Wotring MG, McLaughlin PJ, Zagon IS. Characterization of CCK-B/gastrin-like receptors in human gastric carcinoma. Int. J. Oncol. 1998 Feb;12(2):411-9.[↩]





{kind=link}