Contents
- Hemophagocytic lymphohistiocytosis
- Hemophagocytic lymphohistiocytosis types
- Infection-associated hemophagocytic lymphohistiocytosis (infection-associated HLH)
- Rheumatologic hemophagocytic lymphohistiocytosis (R-HLH) or Macrophage Activation Syndrome (MAS-HLH)
- Hemophagocytic lymphohistiocytosis in patients with cancer (M-HLH)
- Hemophagocytic lymphohistiocytosis during chemotherapy (Ch-HLH)
- Hemophagocytic lymphohistiocytosis associated with receiving immune activating therapies (Rx-HLH)
- Transplant-related hemophagocytic lymphohistiocytosis (PT-HLH)
- Hemophagocytic lymphohistiocytosis in patients who are immune compromised (IC-HLH)
- Hemophagocytic lymphohistiocytosis and metabolic disorders
- Hemophagocytic lymphohistiocytosis of unknown or uncertain origin
- Hemophagocytic lymphohistiocytosis causes
- Hemophagocytic lymphohistiocytosis pathophysiology
- Hemophagocytic lymphohistiocytosis signs and symptoms
- Hemophagocytic lymphohistiocytosis differential diagnosis
- Hemophagocytic lymphohistiocytosis diagnosis
- Hemophagocytic lymphohistiocytosis treatment
- Hemophagocytic lymphohistiocytosis prognosis
- Hemophagocytic lymphohistiocytosis types
Hemophagocytic lymphohistiocytosis
Hemophagocytic lymphohistiocytosis also called HLH syndrome is a rare, life-threatening intense immune activation syndrome in which your body makes too many activated immune cells called macrophages (histiocytes) and lymphocytes (T cells, natural killer cells and B cells) 1, 2, 3, 4, 5, 6. Hemophagocytic lymphohistiocytosis (HLH) is caused by an overactive and abnormal immune response resulting in an uncontrolled excessive inflammatory and ineffective immune response resulting in progressive multi-organ damage and potentially death if untreated 7, 8. In hemophagocytic lymphohistiocytosis, the immune system responds to a stimulus or ‘trigger’, often an infection, cancer or rheumatologic disease, but the response is ineffective and abnormal. This ineffective, abnormal response, causes a variety of signs and symptoms, which, if not treated, can potentially become life-threatening.
In hemophagocytic lymphohistiocytosis (HLH) there is overactivation of T cells, natural killer (NK) cells and macrophages (histiocytes) causing an uninhibited release of pro-inflammatory cytokines (cytokine storm) resulting in a clinical presentation of fever, abnormally large spleen (splenomegaly), low fibrinogen in blood (hypofibrinogenemia) and impaired blood clotting ability (coagulopathy) 5, 6. People with HLH usually develop symptoms within the first months or years of life. Hemophagocytic lymphohistiocytosis most often affects infants from birth to 18 months, but can affect individuals of any age from childhood to adulthood 9. Symptoms may include fever, abnormally large liver (hepatomegaly) or abnormally large spleen (splenomegaly), decreased number of blood cells (cytopenia), and neurological abnormalities such as seizures, changes in mental status and irritability, paralysis (palsy) of certain cranial nerves, and problems coordinating voluntary movements (ataxia) 10, 11, 12.
Hemophagocytic lymphohistiocytosis (HLH) is not a single disease, it is a group of disorders of the immune system that can be triggered by infections, cancer or rheumatologic diseases.
Hemophagocytic lymphohistiocytosis (HLH) occurs in two major forms depending on the underlying causes 4, 13, 11, 12, 14, 5, 15, 16, 17, 18, 19, 20:
- Primary hemophagocytic lymphohistiocytosis also called Familial hemophagocytic lymphohistiocytosis is an autosomal recessively inherited version of hemophagocytic lymphohistiocytosis (HLH). This means it often runs in families and typically presents during infancy or early childhood. It is estimated that familial hemophagocytic lymphohistiocytosis (F-HLH) affects about 1 in every 50,000 births. There are five subtypes of inherited HLH which are designated as familial hemophagocytic lymphohistiocytosis types 1 to 5. Each subtype is caused by a change (mutation) in a different gene. The genetic cause of familial hemophagocytic lymphohistiocytosis type 1 is currently unknown. Familial hemophagocytic lymphohistiocytosis types 2 to 5 are caused by mutations in the PRF1 gene, the UNC13D gene, the STX11 gene and the STXBP2 gene, respectively.
- Secondary hemophagocytic lymphohistiocytosis also known as acquired hemophagocytic lymphohistiocytosis generally is diagnosed in older children and adults. Acquired hemophagocytic lymphohistiocytosis is not inherited, but rather thought to result from an inappropriate response to immune stimulation, such as severe infection, rheumatolgic disease, or cancer. Heterozygous mutations in some genes associated with primary HLH have been found in patients with secondary hemophagocytic lymphohistiocytosis, suggesting there may be a component of genetic predisposition in some patients 21. Secondary HLH is seen in all age groups, without preference for gender. The incidence of secondary hemophagocytic lymphohistiocytosis (i.e., the rate at which it occurs in the population) is not known. However, secondary HLH are more common than the familial hemophagocytic lymphohistiocytosis. An example of secondary HLH is macrophage activation syndrome (MAS). Macrophage activation syndrome (MAS) is the term used for HLH that occurs in people with an autoimmune or autoinflammatory disease. Recent consensus guidelines recommend that macrophage activation syndrome (MAS) be restricted to cases of HLH in patients with adult-onset Still’s disease, juvenile systemic arthritis (soJIA), systemic lupus erythematosus (SLE), vasculitis, and other systemic autoimmune diseases, because treatment of this condition may differ from that of other forms of HLH 22.
- Differentiation between primary and secondary hemophagocytic lymphohistiocytosis is mandatory since they share the same clinical picture but often require different therapeutic approaches 23.
Although hemophagocytic lymphohistiocytosis has various underlying causes, all subtypes of HLH are related to immune dysregulation that leads to hypercytokinemia and an accumulation of activated macrophages in organs and tissues 24. In HLH, when the white blood cells act in a dysregulated manner, they often over-produce cytokines, and the abnormally functioning white blood cells and cytokines can damage organs including the liver, spleen, bone marrow and brain. Without prompt diagnosis and treatment, HLH can lead to severe organ damage and death. Therefore, early diagnosis and prompt treatment is essential. HLH is rare, from the institution of the first international HLH registry in 1989 to the HLH-2004 therapeutic study, only approximately 700 patients have been formally evaluated worldwide 25. In Europe and Japan an HLH incidence of 1 to 2 per million was reported in 2005 26, however, there is the possibility that the diagnosis is under-reported, especially in developing countries 27. Therefore a high grade of suspicion is essential for diagnosis.
HLH should be suspected in all patients with prolonged high-grade fever associated with abnormally large spleen (splenomegaly) and multiple organ involvement 20. The clinical spectrum of hemophagocytic lymphohistiocytosis disease is wide, ranging from mild organ dysfunction to multiorgan failure requiring intensive care. Central nervous system (CNS) involvement is frequent and often severe, even though it is not included in the official diagnostic criteria 20.
Hemophagocytic lymphohistiocytosis most often affects infants or young children, but can affect individuals of any age. It affects boys and girls in equal numbers. In adults, it affects men slightly more often than women. The exact incidence and prevalence of hemophagocytic lymphohistiocytosis is unknown. Rare disorders often go misdiagnosed or undiagnosed making it difficult to determine the true frequency in the general population. About 25% of the people with hemophagocytic lymphohistiocytosis, have the familial form.
The typical patient is an infant under 1 year of age, ill-appearing (toxic aspect), occasionally with a critical sepsis-like aspect 4. A younger age at onset suggests an underlying genetic basis, as seen in familial hemophagocytic lymphohistiocytosis (F-HLH) or in HLH forms arising from genetic primary immunodeficiencies; however, familial HLH can present at any age, including adulthood 28.
Progressive splenomegaly (abnormally large spleen) is typically observed in patients, and can be associated with liver involvement, neurological signs, respiratory and kidney failure 29. Skin rashes, reddening of the skin because of inflammation (erythroderma), swelling (edema) or tiny spots on the skin due to bleeding under the skin (petechiae) have been reported 29. Atypical forms, usually seen in children older than 1 year, include isolated fever of unknown origin (FUOs), isolated central nervous system (CNS) involvement 30 or isolated acute liver failure 31, 32. Enlarged lymph node (lymphadenopathy) is uncommon in patients and indicates a potential underlying lymphoma 33.
Typical laboratory findings include cytopenias (low levels of red blood cells [anemia], white blood cells [leukopenia] or platelets [thrombocytopenia]), high level of triglycerides in blood (hypertriglyceridemia), low fibrinogen in blood (hypofibrinogenemia) are suggestive of HLH in the context of general inflammation and hyperferritinemia. Liver function tests are frequently altered 20. Leukocytosis (elevated white blood cell (WBC) count) is not typical of HLH except in HLH-associated with defined rheumatological conditions or macrophage activation syndrome-HLH (MAS-HLH) 20. Hemophagocytosis describes the pathognomonic findings where highly activated macrophages taking up different cells including lymphocytes, erythrocytes, leukocytes, and platelets in different tissues, producing excessive cytokines and an uncontrolled inflammatory reaction 7, 20, 34.
Despite great improvement in HLH diagnosis and treatment, it still represents a challenge in clinical management, with poor prognosis in the absence of an aggressive therapeutic approach 25, 20.
If HLH is diagnosed quickly and accurately at a center equipped to manage this complicated disease, a cure is possible. Often, due to the severity of the clinical picture, it is necessary to start an aggressive treatment before having clarified the primary or secondary nature of HLH syndrome 35.
Familial hemophagocytic lymphohistiocytosis are currently treated with chemotherapy as a bridge to hematopoietic stem cell transplantation (HSCT). HLH occurring in rheumatic disease (macrophage activation syndrome [MAS]) is treated with glucocorticoids, IL-1 blockade, or cyclosporine A. In other forms of HLH, addressing the underlying trigger is essential. There remains a need for safer and more effective therapies of HLH.
Figure 1. Blood cell development
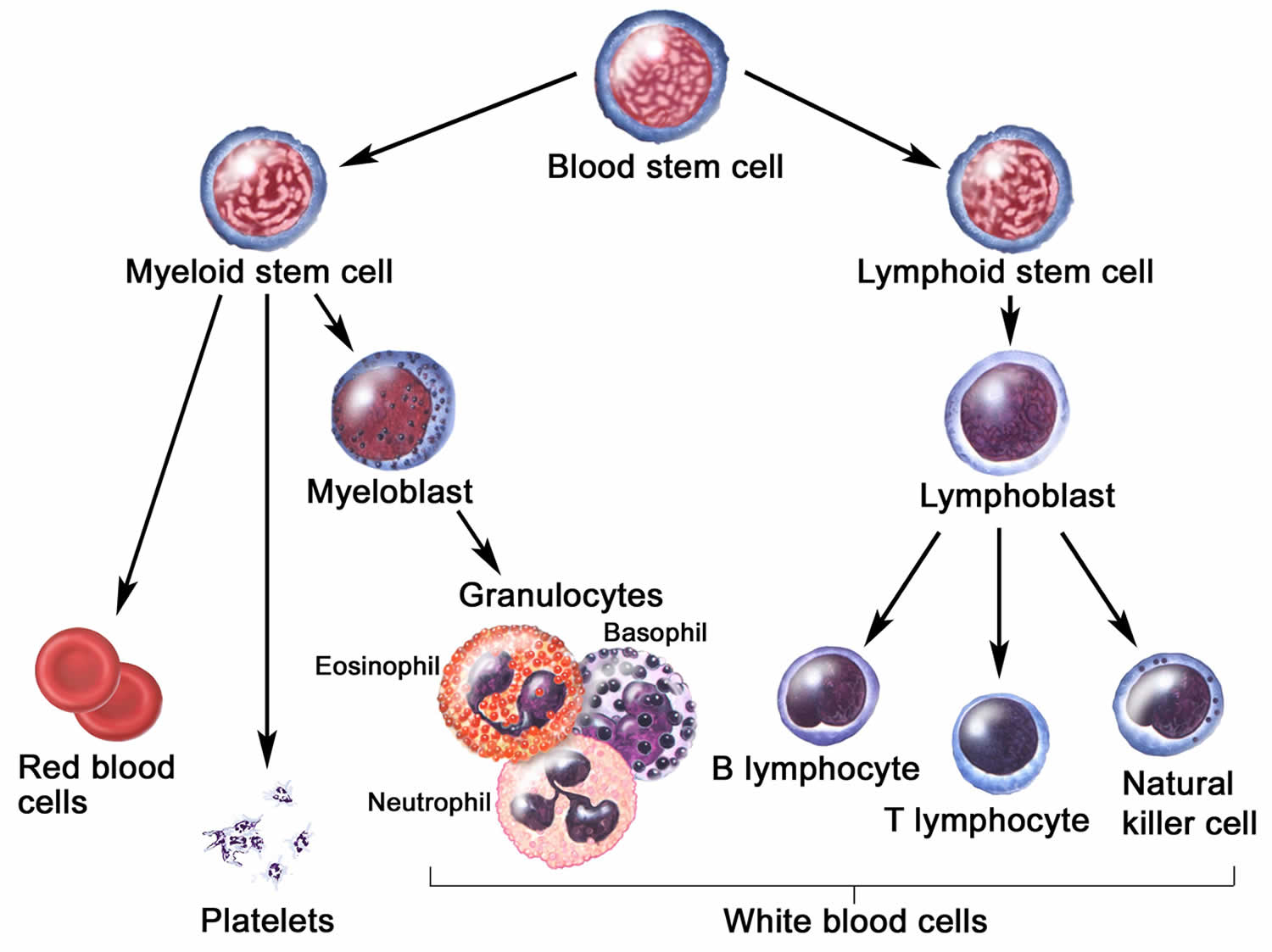
Figure 2. Hemophagocytic lymphohistiocytosis
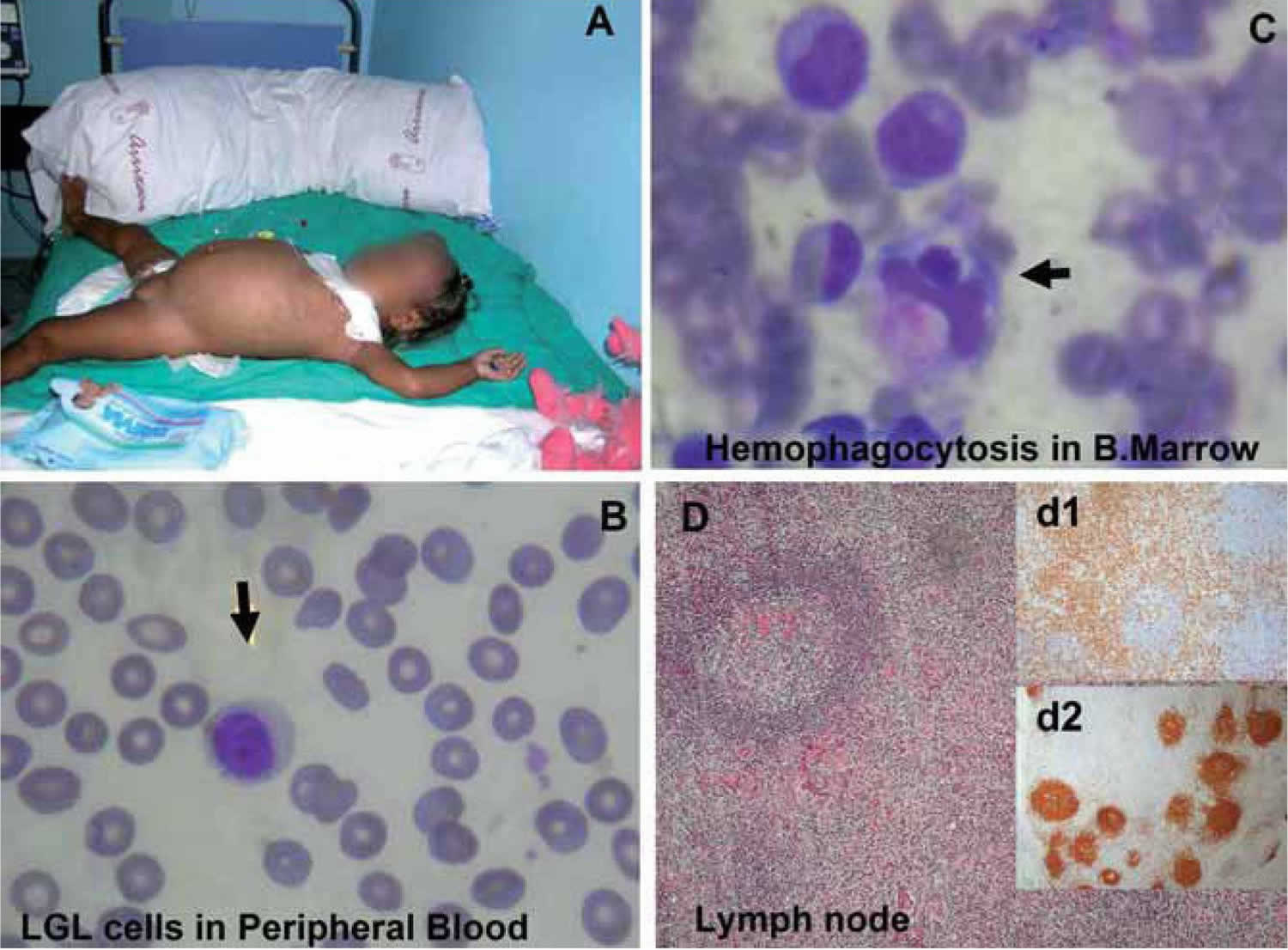
Footnotes: (A) 17-month-old Ecuatorian girl showing partial albinism and suffering from fever and cytopenias persisting over 3 weeks, splenomegaly (10 cm), hepatomegaly (5 cm), múltiple adenopathies, purpura and edema; (B) cell expansion of large granular lymphocytes (LGL cells) in peripheral blood; (C) bone marrow with erithroid, megakaryocytic, and mononuclear-phagocyte hyperplasia and scarce signs of hemophagocytosis. Arrows indicate hemophagocytosis. (D) Paracortical diffuse hyperplasia in a lymph node biopsy with no signs of hemophagocytosis or lymphoproliferative disease; d1 and d2 inserts, interfollicular/paracortical and follicular details of anti-CD3 and anti-CD20 immunohistochemistry analysis, respectively.
[Source 36 ]Figure 3. Hemophagocytic lymphohistiocytosis pathology
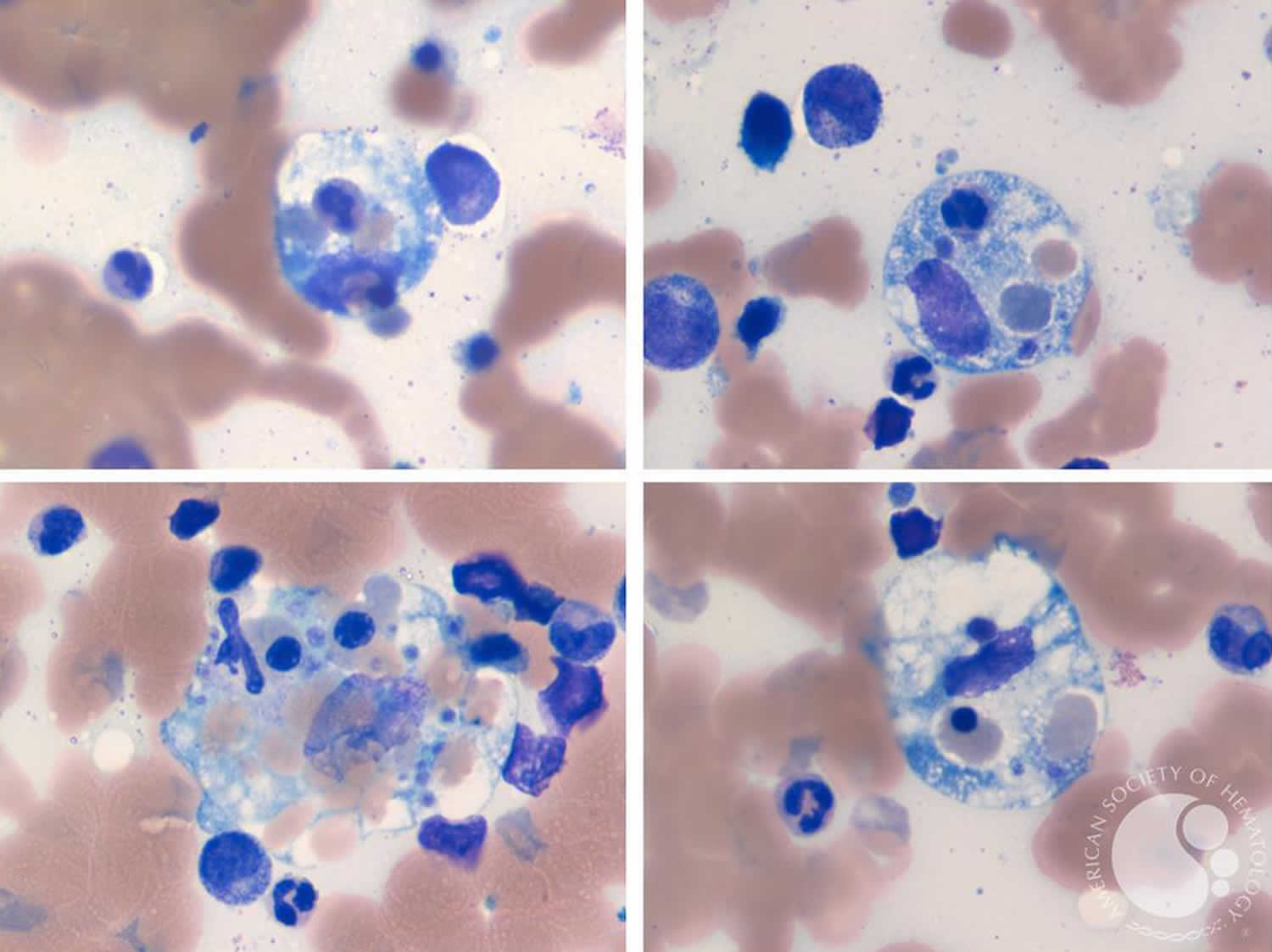
Footnotes: Hemophagocytic lymphohistiocytosis (HLH) primarily involves histiocytes (macrophages) which engulf and destroy red blood cells, a process known as erythrophagocytosis and depicted in the images. Hematologic analysis will also likely reveal increased histiocytes, hypercellular bone marrow, and pancytopenia. Cellular damage in HLH results in stimulation of inflammatory cytokines including TNF-α and IFN-γ, which suppress hematopoiesis, induce apoptosis in hematopoietic cells, and further activate histiocytes 37. If HLH is suspected, it is critical to evaluate serum ferritin, triglyceride, and fibrinogen levels. Work-up revealed positive Epstein-Barr virus (EBV) virology in this case, without morphologic or immunophenotypic evidence of lymphoma or leukemia involvement. Secondary HLH in adults is typically caused by virus or lymphoma, more commonly T cell lymphoma. Therefore, monitoring and further testing for an occult secondary lymphoma could be beneficial.
- Elevated ferritin is expected because destruction of red blood cells results in the release of iron into the serum. Additionally, histiocytes increase ferritin production secondary to increased levels of heme-oxygenase due to the inflammatory cytokines 37.
- Hypertriglyceridemia is expected in HLH, because TNF-α and IFN-γ also inhibit lipoprotein lipase activity, which decreases the breakdown of triglycerides for uptake and storage by tissues.1
- Plasmin will also be elevated due to histiocyte secretion of plasminogen activator, leading to fibrin breakdown, which decreases fibrinogen1 and increases D-dimer 38.
- In addition to elevated ferritin and triglycerides with lowered fibrinogen as key laboratory findings for HLH, elevated CD25 marks activated lymphocytes, and is the alpha subunit of the interleukin 2 receptor (IL-2R) 37.
Hemophagocytic lymphohistiocytosis types
Historically, patients with hemophagocytic lymphohistiocytosis are often split into two groups: “primary” or familial hemophagocytic lymphohistiocytosis (FHL) due to a known genetic mutation and “secondary” hemophagocytic lymphohistiocytosis triggered by an external stimulus that include infection, cancer, and rheumatologic disorders 20, 40. This classification, though widely accepted and used, fails to inform the prognosis and therapy of secondary HLH, which, as will be discussed, has many different causes 4. For this and other reasons, in 2019 the North American Consortium for Histiocytosis (NACHO) 4 introduced the concept of ‘HLH syndrome’ and proposed to categorize HLH subtypes by specific etiologic associations instead of classifying HLH as ‘primary’ or ‘secondary’. The North American Consortium for Histiocytosis favor designating subgroups of HLH by their specific etiologic associations and designates those likely benefiting from HLH-directed immunosuppressive therapies as “HLH disease” or those unlikely to benefit from these therapies (or require entirely different therapeutic strategies) as “HLH mimics” 4. In this construct, HLH disease is further broken down into clinically recognizable categories with potential for overlap between HLH disease and HLH mimics. Hemophagocytic lymphohistiocytosis (HLH) cases with clear genetic etiology should be referred to as “familial” hemophagocytic lymphohistiocytosis (F-HLH), and those seen with cancer or rheumatologic disorders associated hemophagocytic lymphohistiocytosis should be referred to as M-HLH or R-HLH respectively 4. Other notable subgroups of HLH disease include HLH associated with immune compromise (immune deficiency or immunosuppression, IC-HLH) and iatrogenic HLH (Rx-HLH, secondary to immune activating therapies) 4. All other cases of HLH disease (including those with negative or ambiguous genetic findings, with or without infectious triggers) should simply be referred to as “HLH disease-NOS” without reference to “primary” or “secondary” 4. As infection may act as a trigger for HLH in any subcategory (except iatrogenic HLH [Rx-HLH]), it is not distinguishable as a distinct category or cause. Finally, some patients develop a recognizable but incomplete or “forme fruste” HLH syndrome. “Forme fruste” HLH syndrome is important to recognize as some patients with familial hemophagocytic lymphohistiocytosis (F-HLH) or rheumatologic disorders associated hemophagocytic lymphohistiocytosis (R-HLH) may experience repeated, often self-limited episodes of this partial HLH, before developing definitive disease 4. Such a history should be a strong indicator for genetic workup/careful monitoring, and may justify treatment. Figure 4 illustrates the diversity of HLH.
Figure 4. Hemophagocytic lymphohistiocytosis syndrome
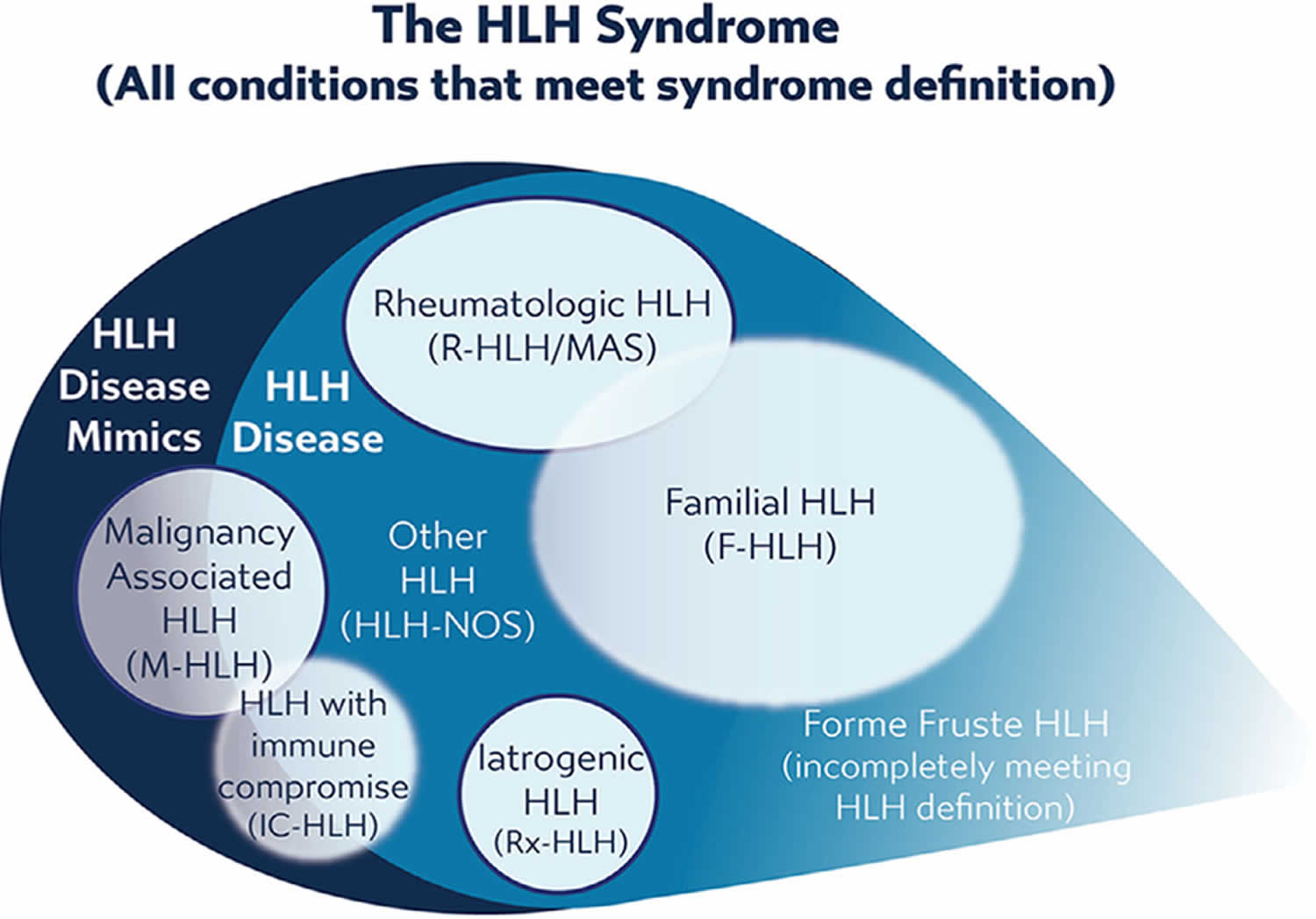
Footnote: Hemophagocytic lymphohistiocytosis syndrome includes all conditions meeting consensus diagnostic criteria. HLH syndrome includes conditions that would benefit from HLH-directed immunosuppressive therapies, which are termed “HLH disease” and those conditions that would not benefit from immunosuppressive therapy or require entirely different treatments, termed as “HLH disease mimics.” HLH disease includes recognizable subgroups: familial HLH with clear genetic origin, HLH associated with malignancy, HLH associated with rheumatologic conditions (macrophage activation syndrome [MAS]), HLH observed after immune activating therapies (iatrogenic HLH, also called cytokine release syndrome), HLH associated with immune compromise (either primary immune deficiency or treatment-related immune suppression), and HLH not associated with other specific conditions. Recognition of these subcategories is valuable as this may alter treatment, though some categories overlap with each other or have indistinct borders and may include examples of both HLH disease and HLH disease mimics. Use of these category-specific terms is preferred over the historical terms of “primary” and “secondary” because the older concepts are ambiguous due to increasing understanding of genetic complexity, involvement of infection in triggering multiple distinct variations of HLH, and varied application. Incomplete, forme fruste episodes of HLH (similar but not completely fulfilling diagnostic criteria) are also well recognized in patients with familial HLH and may occur in others, such as “mild MAS” in patients with systemic onset juvenile arthritis (soJIA).
[Source 4 ]Infection-associated hemophagocytic lymphohistiocytosis (infection-associated HLH)
Infection-associated hemophagocytic lymphohistiocytosis (infection-associated HLH) represents a challenge in classification 1. This is because infectious diseases can trigger HLH in both primary and secondary forms, and because septic shock can either be a presentation of HLH syndrome or may mimic it, with great implications in therapeutic approach. A thorough infectious screening is thus highly recommended when facing an HLH syndrome 20, 41.
Among the case reports the most frequent infectious triggers were viruses, such as the herpetic viruses, dengue virus, Crimean Congo hemorrhagic fever virus, Eastern equine encephalitis virus, hepatitis A virus (HAV), hepatitis B virus (HBV), human immunodeficiency virus (HIV), adenovirus, parvovirus B19, measles, influenza virus and severe acute respiratory syndrome coronavirus 2 (COVID-19).
Epstein-Barr virus (EBV) has been frequently reported from all across the world, and especially from the Asian Countries 42, 43, 44, 45, 46, 47, 48, 49, 50, 51. The reason for this geographical heterogeneity may involve a higher virulence in EBV viral strains circulating in Asia 52 or a different immune predisposition in the Asian patients, but this issue has not been clarified yet. EBV typically targets B cells, but in a subset of patients with EBV-HLH, of prevalent Asian origin again, it infects T or NK cells leading to oligoclonal or monoclonal proliferation and massive cytokine production 53, 54. In extreme cases, EBV-HLH clinical picture can be difficult to differentiate from T cell lymphoproliferative disorder 54. EBV-hemophagocytic lymphohistiocytosis is usually quite aggressive, with a frequent involvement of central nervous system (CNS). Once EBV is demonstrated by serology tests or molecular biology methods, a targeted approach is recommended 52, 55. Clinical scores to differentiate low risk vs. high-risk patients have been proposed 55, but have not achieved conclusive results yet.
Cytomegalovirus (CMV) is typical of newborns and immunocompromised patients 50, 56, 57, 58, 59, 60, 51 and so is the varicella zoster virus 61. Dengue virus plays a significant role in tropical countries 51, 4, 62, 63, 64, 65, 66. Tick-borne diseases include the Crimean-Congo hemorrhagic fever nairovirus 67, 68 and the Eastern equine encephalitis virus 69. Sporadic case reports include HLH related to hepatitis A virus 66, 70, hepatitis B virus 71, human immunodeficiency virus (HIV) 65, 72, Adenovirus 50, 65, 73, 74, Parvovirus B19 50, Measles 75 and Influenza virus 76, 77, 78. Sars-Cov2 infection, causative of the recent COVID19 pandemic, has been reported to also be a HLH trigger, mostly in adults 79, 80.
Bacterial infections associated to HLH have frequently been reported in tropical countries and include Brucella 50, 81, 82, 83, Salmonella enteritidis 66, 84, 51, Tuberculosis 51, 66, 85, sepsis by streptococcal infection [group B streptococcus 86 and Streptococcus suis 87 ], by Listeria 50 or without identified pathogen 66. Orientia tsutsugamushi, the causing agent of scrub typhus, has been reported in India 65, 66, 51 and South Korea 88, 89, 90, 91. Ehrlichia chaffeensis, the agent of human monocytic ehrlichiosis, has been reported from the US 92, 93, 94, 95, 96. A case of Strep pneumoniae 23A, serotype that is not included in the pneumococcal 13-valent conjugated vaccine (PCV-13) has been reported from Japan 97.
HLH in kidney transplant recipients has been associated with Ehrlichiosis in one case 95, and with Bartonella henselae in one other case 98. A case associated with Serratia marcescens has been reported in a preterm newborn 99.
Fungal infection-associated HLH has been reported in immunocompromised hosts (being treated for aplastic anemia and preB-acute lymphoblastic leukemia, respectively), caused by Trichosporon asahii 100.
Leishmania 49, 50, 101, 102, 103, 104 and Plasmodium falciparum 105 and Plasmodium vivax 106 have been reported as parasitic triggers of HLH 66.
Rheumatologic hemophagocytic lymphohistiocytosis (R-HLH) or Macrophage Activation Syndrome (MAS-HLH)
Macrophage Activation Syndrome (MAS) is the term most commonly used to refer to an HLH or HLH-like syndrome occurring in the context of rheumatologic disorders (R-HLH) 107. While MAS and HLH are very similar and should be viewed as the same disease, regardless of differences in presentation and treatment 40, 108, 109, 110. Consensus criteria for recognizing MAS in the context of systemic onset juvenile arthritis (soJIA) have been developed, and in general, these patients with MAS are older than patients with familial hemophagocytic lymphohistiocytosis and they present with substantially higher platelet and neutrophil counts as well as higher fibrinogen levels 111 These laboratory indices are typically elevated in patients with juvenile idiopathic arthritis (JIA), so “falling” to near-normal levels is often a substantial change indicating a more severe process than would ordinarily be implied by such values. The frequency of MAS is ∼10% of patients with systemic onset juvenile arthritis (soJIA), but 30–40% may have an incomplete presentation of MAS 111, 112. MAS in adults is most commonly seen with adult-onset Still’s disease, reported in ∼15% of adult-onset Still’s disease cases 113, 114. MAS has also been reported in systemic lupus (estimated incidence of MAS in 4% of cases), dermatomyositis, Kawasaki’s disease, and rheumatoid arthritis 115, 116. Obviously, a pre-existing diagnosis of a rheumatologic disorder would define R-HLH, but unexplained rash, recurrent fever, arthralgia/arthritis in an undiagnosed patient presenting with HLH may suggest R-HLH.
Hemophagocytic lymphohistiocytosis in patients with cancer (M-HLH)
The association of hemophagocytic lymphohistiocytosis in patients with cancer (M-HLH) has been recognized for decades and it can be the initial manifestation of an underlying malignancy, it may develop during therapy as the consequence of chemotherapy or of treatment-induced mutations [treatment-induced HLH (Ch-HLH)], or it can develop as a consequence of an intercurrent infection 117, 118, 119, 120. Hemophagocytic lymphohistiocytosis in patients with cancer (M-HLH) is common in adults, where it accounts for ~50% of HLH cases 33, while it is significantly rarer in children, with a prevalence of 8-11% 117, 121.
Patients may present with the clinical syndrome of HLH associated with undiagnosed underlying malignancy (new onset), or they may develop HLH during treatment for known malignancy (on therapy), usually in the context of infection. With new onset M-HLH, this HLH syndrome is typically a “HLH disease mimic”, as the disease features appear to be driven directly by the cancer, and antineoplastic (instead of anti-HLH) treatment should be the priority, though pathophysiology is not well defined and therapy of malignancy may overlap with HLH treatment. “On therapy” M-HLH should most often be considered to be a manifestation of HLH due to infection in the context of immune compromise (IC-HLH), though it may rarely be associated with occult relapse. When considering hemophagocytic lymphohistiocytosis in patients with cancer (M-HLH), it is important to note that the presence of EBV viremia does not rule out malignancy (including B- or T-cell lymphomas) and sCD25 may be disproportionately elevated compared to other features of HLH in patients with occult lymphoma 122, 123.
The excess of proinflammatory cytokines produced by activated T cells infiltrating or surrounding the tumor or by the neoplastic T-cells in T/NK cell lymphoma is likely to cause hemophagocytic lymphohistiocytosis in patients with cancer (M-HLH) 6, 124. In rare cases, the diagnosis of HLH anticipates that of malignancy by several weeks 117, 125.
Lymphoma deserves special mention as it is the most common malignancy associated with HLH at its initial presentation. Lymphomas, though relatively uncommon at pediatric age, are frequently reported in association with HLH 117. Among the cases reviewed, HLH has been associated with Hodgkin lymphoma (73,121,140,144), anaplastic large cell lymphoma 51, 126, 127, peripheral T-cell lymphoma 126, 128, post-transplant lymphoproliferative disorder-lymphoma 129, subcutaneous panniculitis-like T-cell lymphoma 49, extranodal NK/T cell lymphoma, hepatosplenic T-cell lymphoma, systemic EBV-positive T-cell lymphoma of childhood 126. In addition, HLH and lymphoma can be alternative diagnoses as well 130, and extreme caution is required in differentiating the two conditions before starting steroid therapy. Acute leukemia (both myeloblastic and lymphoblastic) presenting as HLH syndrome has also been reported 50, 95, 126.
Because of the difficulty of distinguishing lymphoma from familial hemophagocytic lymphohistiocytosis (F-HLH) or rheumatologic disorders associated hemophagocytic lymphohistiocytosis (R-HLH), thorough imaging and aggressive biopsy, often guided by PET-CT, should be pursued or at least considered before starting corticosteroids and other therapies that may obscure diagnosis 131.
Hemophagocytic lymphohistiocytosis during chemotherapy (Ch-HLH)
Among the cases of hemophagocytic lymphohistiocytosis during chemotherapy (Ch-HLH), HLH developed on therapy or after treatment for juvenile myelomonocytic leukemia 132, acute monocytic leukemia 133, Langherhans cell histiocytosis 134 and solid tumors such as Wilms tumor 135, neuroblastoma 50, 136, rhabdomyosarcoma 119. Langerhans cell histiocytosis has been associated to HLH at presentation, during therapy or as a consequence of viral infection 119, 125, 137.
The immunosuppression induced by treatment frequently causes viral infections or reactivations, that in turn can trigger HLH. Among the cases reviewed, viral reactivation included EBV, CMV, respiratory syncytial virus, BK virus, human herpes virus 6, adenovirus and parvovirus B19 120, 138.
Hemophagocytic lymphohistiocytosis associated with receiving immune activating therapies (Rx-HLH)
Various emerging immune activating therapies such as chimeric antigen receptor T cells (CAR-T cells), immune checkpoint inhibitors and Blinatumomab a bispecific T-cell engager (BiTE, an antibody therapy that binds to two target proteins on different cells), have been associated with cytokine release syndrome (CRS) 139. Cytokine release syndrome shows major overlaps with HLH, so numerous authors classify it as a form of secondary hemophagocytic lymphohistiocytosis 140, 141, 142; some other authors, conversely, restrict the diagnosis of HLH following CAR-T infusion (car-HLH) to the cases in which a severe cytokine release syndrome is associated to the typical HLH laboratory findings, often including hemophagocitosis 143, 144.
CAR-T cells were officially licensed for use in children and young adults by the U.S. Food and Drug Administration in 2017 for the treatment of refractory B-cell acute lymphoblastic leukemia 145. Cytokine release syndrome is a common severe adverse reaction following such therapies, especially in the acute phase 139. It probably results from the high amount of IFN-γ and IL-6 produced by the constitutionally activated CAR-T cells 146 or by the subsequently activated macrophages 147, 148, 149 and by the targeted tumor cell lysis 150. Development of car-HLH seems associated with pre-infusion NK lymphopenia (although it is not associated with impaired NK function) that is further amplified by treatment 143.
The St. Jude Children’s Research Hospital group recently described a cohort of 27 pediatric patients treated with CD-19 CAR-T cells 144: 12/27 patients developed cytokine release syndrome alone, while four progressed to car-HLH despite appropriate therapy. The car-HLH subgroup showed higher and more sustained inflammation parameters and a poorer antileukemic response and survival. Blinatumomab, as well, has been associated with cytokine release syndrome and/or HLH in adults 139 and children 151.
Patients treated with T-activating therapies should be closely monitored for hemophagocytic lymphohistiocytosis, in order to optimize diagnosis and therapeutic approach.
Additional iatrogenic causes of cytokine storm include rituximab 152, gene therapies, immune checkpoint inhibitors, allogeneic hematopoietic stem cell transplantation (allo-HSCT) and heart transplantation 139.
Transplant-related hemophagocytic lymphohistiocytosis (PT-HLH) has been described in the context of hematopoietic stem cell transplantation (HSCT) 153, 154 and, more rarely, in kidney 98, 147 and liver transplant recipients 155, 156, 157. Post-transplant HLH (PT-HLH) might be triggered by a combination of tissue damage, immunosuppressive therapy 158, alloimmune response, residual malignancies or by infections 153. Viral infections or reactivations, such as EBV and CMV but also gastrointestinal viruses, represent the most frequent trigger, but bacterial and fungal infections have also occasionally been described 98, 147, 154, 159, 160, 161.
HLH post-hematopoietic stem cell transplantation (post-HSCT HLH) can occur within the first 30 days after transplantation (early onset) or later (late onset) 153. Late onset is usually related to infectious events, while for early onset the causes are not fully understood. In some cases the triggering factor may be the residual disease 153. Post transplant-related hemophagocytic lymphohistiocytosis (PT-HLH) diagnosis is extremely challenging because of the complex clinical and laboratory picture of the affected patients, for whom specific diagnostic criteria do not exist yet, and a high suspicion rate is essential 162.
In early onset post-hematopoietic stem cell transplantation (post-HSCT HLH), aspects of differential diagnosis may occur with engraftment syndrome and acute graft-vs.-host disease 153. The treatment of post-transplant HLH (PT-HLH) is also particularly complex, since we are dealing with immunosuppressed patients, often with transplant-related toxicity 153. In EBV-related forms, the use of rituximab plays an important role 44, 163.
Hemophagocytic lymphohistiocytosis in patients who are immune compromised (IC-HLH)
HLH has been reported to occur in a variety of patients who are immune compromised, including those receiving chemotherapy or those with primary immune deficiency (PID). As noted above, HLH may occur in patients with cancer who have often received chemotherapy for an extended period of time and who typically have a recent triggering infection. Similarly, a number of children (and adults) with inflammatory bowel disease (IBD), typically treated with azathioprine or mercaptopurine have been reported to develop HLH after primary infection with EBV or CMV 164. In both contexts, pathophysiology is not well understood and while it may be related to the underlying disease, HLH appears to be a dysregulated response to infection which is related to immunosuppression. It is difficult to generalize about whether IC-HLH may benefit from significant immune suppression. For patients with IBD, withdrawal of mercaptopurine, treatment of infection, supportive care, and moderate dose corticosteroids often suffice. “On therapy” M-HLH does not appear to respond well to any treatment, though corticosteroids ± etoposide are usually tried. Thus, IC-HLH ambiguously straddles the categories of HLH disease and HLH disease mimics.
A variety of PIDs have been reported to present with HLH 165, 166: severe combined immunodeficiency (SCID), Omenns syndrome, severe DiGeorge syndrome, Wiskott-Aldrich syndrome, chronic granulomatous disease (CGD), X-linked agammaglobulinemia, and autoimmune lymphoproliferative syndrome. Patients with primary immune deficiency and HLH often have unresolved, severe infections. Patients with SCID most often have viral infections, while those with chronic granulomatous disease present with bacterial infections. Thus, the presence of HLH associated with unusual or unusually severe infection should suggest undiagnosed immune deficiency. For patients with severe combined immunodeficiency (SCID) and infection, immunosuppressive therapy is generally not helpful and this condition should be considered to be a mimic of HLH disease 4. HLH in patients with chronic granulomatous disease is less clear, though typical treatment for HLH beyond corticosteroids is usually not indicated. Therefore, the constellation of HLH symptoms in the context of primary immune deficiency should usually be considered a mimic of HLH disease, though some patients may require immunosuppressive therapy 4.
Hemophagocytic lymphohistiocytosis and metabolic disorders
Among the cases reviewed in the present study, several patients were diagnosed with secondary hemophagocytic lymphohistiocytosis or HLH syndrome in the context of an inherited condition associated with metabolic diseases, such as Wolman’s disease 167, galactosemia, Gaucher disease 168, Niemann-Pick disease, methylmalonic acidemia and propionic acidemia 169. Long-chain 3-hydroxyacyl-CoA dehydrogenase deficiency 170, type 1 glycogen storage disease 171, lysosomal acid lipase deficiency 172, mucopolysaccharidosis-plus syndrome 173.
These patients fulfilled the HLH 2004 criteria, but it is possible that some HLH features, such as splenomegaly and cytopenias, were caused by the metabolic disease itself rather than by immune hyperactivation 1. On the other hand, it is possible that metabolites accumulation activated macrophages and triggered a proper secondary hemophagocytic lymphohistiocytosis. The link between metabolic disorders and HLH needs to be clarified, but an extensive screening for underlying metabolic diseases should be performed in patients presenting with HLH 167, 168.
Hemophagocytic lymphohistiocytosis of unknown or uncertain origin
HLH has recently been described in the context of febrile infection related epilepsy syndrome (FIRES) 174, an epileptic encephalopathy characterized by refractory status epilepticus following unspecific febrile illnesses. The pathophysiology of febrile infection related epilepsy syndrome (FIRES) has not been completely understood, but it likely to depend, once more, on dysfunctional activation of the innate immune system 174. Moreover, though rare, this association stresses the need of screening for patients with HLH presenting with severe CNS symptoms.
A curious case of HLH following spider bite (Loxosceles reclusa) has been reported from the US 175.
Drug reaction with eosinophilia and systemic symptoms induced by vancomycin, carbamazepine and levetiracetam has been described as an occasional trigger of HLH 50.
Hemophagocytic lymphohistiocytosis causes
Based on the underlying genetic basis and “triggers” that include infection, cancer, and rheumatologic disorders, hemophagocytic lymphohistiocytosis (HLH) is broadly broken down into primary (familial hemophagocytic lymphohistiocytosis) and secondary (acquired) HLH. Genetic mutations in PRF1, UNC13D, STXBP2, STX11, LYST, and RAB27a cause familial hemophagocytic lymphohistiocytosis (F-HLH) 4, 5, 176, 177, 178, 179. Secondary HLH is usually triggered by underlying infections, cancer, or autoimmune diseases. Epstein-Barr virus (EBV) is considered a common infectious inducer of secondary HLH (EBV-HLH) 5, 180.
Causes of primary and secondary HLH 181:
- Primary HLH (Mendelian inherited conditions leading to HLH) (see Table 1 below)
- Secondary HLH 116
- Infections (mainly viruses, such as EBV, HIV, and CMV, but also bacteria, parasites, and fungi) 186
- Malignancies (mainly malignant lymphoma) 187
- Macrophage activation syndrome in autoinflammatory or autoimmune disorders 188
- Other causes (organ or stem cell transplantation; metabolic, traumatic, iatrogenic [immunosuppression, vaccination, surgery, hemodialysis] causes; and, rarely, pregnancy) 116, 186
Hemophagocytic lymphohistiocytosis (HLH) results from an ineffective, abnormal response of the immune system to a stimulus or ‘trigger’. The underlying mechanisms that cause signs and symptoms to develop are complex. There is overproduction and overactivity of immune system cells called histiocytes (also called macrophages) and T cells (also called T-lymphocytes). These are types of white blood cells, which are the primary cell of the immune system and help the body to fight off infection.
Your immune system is complex and has many components. White blood cells comprise an important part of this system; these cells communicate with each other and other cells of the body by making chemical “messengers” called cytokines. Your immune system is your body’s natural defense system against foreign or invading organisms or substances. The immune system is a complex network of cells, tissues, organs, and proteins that work together to keep your body healthy. Macrophages are a type of white blood cells involved in the detection, phagocytosis and destruction of bacteria and other harmful organisms. Macrophages are effector cells of the innate immune system that phagocytose (a process by which certain living cells ingest or engulf other cells or particles) bacteria and secrete both pro-inflammatory and antimicrobial mediators 189. In addition, macrophages play an important role in eliminating diseased and damaged cells through their programmed cell death. Generally, macrophages ingest and degrade dead cells, debris, tumor cells, and foreign materials. Macrophages promote homeostasis by responding to internal and external changes within the body, not only as phagocytes, but also through trophic, regulatory, and repair functions 189. Furthermore, macrophages can also present antigens to T lymphocytes (T cells) and initiate inflammation by releasing molecules known as cytokines that activate other cells. On the other hand, lymphocytes are mature, infection-fighting cells that develop from lymphoblasts, a type of blood stem cell in your bone marrow (Figure 1). Lymphocytes are the main cells that make up lymphoid tissue and your lymphoid tissue is found in lymph nodes, the thymus gland, the spleen, the tonsils, and adenoids. Lymphocytes consist of several subtypes with different functions:
- B lymphocytes also called B-cells make antibodies to help fight infection. B lymphocytes (B cells) protect the body from invading germs by developing (maturing) into plasma cells, which make proteins called antibodies. The antibodies attach to the germs (bacteria, viruses, and fungi), which helps other white blood cells called granulocytes recognize and destroy them.
- T lymphocytes also called T-cells that help B lymphocytes make the antibodies that help fight infection. T lymphocytes (T cells) can also recognize cells infected by viruses and directly destroy these cells. They also help regulate your immune system.
- Natural killer cells also called NK cells that attack cancer cells and viruses. Natural killer cells serve as pivotal “watchers” or “guards” within the immune system as they respond quickly to a pathogenic infiltration and alert the host about infections. Natural killer cells are able to recognize and break down tumor cells and virus-infected cells, even without any previous sensitization. NK cells originate in the bone marrow and are released into the bloodstream upon maturation, thus being able to respond to stimuli such as pathogen molecules, cytokines, or by the interaction with any target cell that expresses ligands for activating NK cell receptors.
Histiocytes are large phagocytic cells that normally play a role in responding to infection and injury. A phagocytic cell is any “scavenger” cell that engulfs and destroys invading microorganisms or cellular debris. Macrophages also secrete cytokines, which are proteins that stimulate or inhibit other immune system cells and promote inflammation in response to disease. Excessive cytokine production will eventually cause severe tissue damage. Macrophages may also mistakenly engulf and destroy healthy tissue including healthy blood cells, which is called hemophagocytosis. Cytotoxic lymphocytes, which include T cells and natural killer cells, do not function properly. These cells eliminate other cells that are damaged, stressed, or infected. In HLH, cytotoxic lymphocytes fail to eliminate activated macrophages allowing them to abnormally build up in the organs and tissues of the body, which further activates this ineffective immune response. These immune system abnormalities cause the excessive inflammation and tissue destruction that characterizes the condition.
Familial hemophagocytic lymphohistiocytosis
Familial hemophagocytic lymphohistiocytosis (F-HLH) or primary HLH is caused by changes or mutations of specific areas within a person’s genes 190. Genes provide instructions for creating proteins that play a critical role in many functions of the body. When a mutation of a gene occurs, the protein product may be faulty, inefficient, absent, or overproduced. Depending upon the functions of the particular protein, this can affect many organ systems of the body.
Several genes have been shown to be abnormal in different people with familial hemophagocytic lymphohistiocytosis (FHL) and researchers are actively working to discover these genes. At least four different genes (i.e., PRF1, UNC13D, STX11 and STXBP2) have been identified that result in a genetic predisposition to developing hemophagocytic lymphohistiocytosis. A genetic predisposition means a person has a gene or genes for a particular disorder, but the disorder will not develop unless other factors help to trigger the disorder.
The four genes that are associated with familial hemophagocytic lymphohistiocytosis (FHL) are 191:
- Unidentified gene defect located on chromosome 9 in Familial hemophagocytic lymphocytosis type 1,
- Perforin (PRF1) gene in Familial hemophagocytic lymphocytosis type 2,
- Munc-13–4 (UNC13D) in Familial hemophagocytic lymphocytosis type 3,
- Syntaxin-11 (STX11) in Familial hemophagocytic lymphocytosis type 4,
- Syntaxin binding protein 2 (STXBP-2) in Familial hemophagocytic lymphocytosis type 5.
Table 1. Familial hemophagocytic lymphohistiocytosis genetic causes and types
| HLH type/association | Gene or locus (protein) | HLH-related dysfunction | Unique clinical features |
|---|---|---|---|
| Familial HLH | |||
| Type 1 (F-HLH 1) | 9q21.3-q22 (unknown) | Unknown | N/A |
| Type 2 (F-HLH 2) | PRF1 (perforin) | Cytolytic pore formation | None |
| Type 3 (F-HLH 3) | UNC13D (Unc-13 homolog D) | Cytolytic vesicle priming | Increased incidence of CNS disease |
| Type 4 (F-HLH 4) | STX11 (Syntaxin 11) | Cytolytic vesicle fusion | Mild, recurrent HLH, colitis |
| Type 5 (F-HLH 5) | STXBP2 (Syntaxin binding protein 2) | Cytolytic vesicle fusion | Colitis; hypogammaglobulinemia, and sensorineural hearing loss |
| Primary Immunodeficiency Syndromes | |||
| Chédiak-Higashi syndrome | LYST (Lysosomal trafficking regulator) | Cytolytic vesicle trafficking | Partial oculocutaneous albinism, recurrent pyogenic infections, and bleeding tendency |
| Hermansky-Pudlak syndrome type 2 | AP3B1 (Adaptor Related Protein Complex 3 Subunit Beta 1) | Cytolytic vesicle trafficking | Partial albinism; immunodeficiency, bleeding tendency, and platelet storage pool deficiency |
| Griscelli syndrome type 2 | RAB27A (Rab-27A protein) | Cytolytic vesicle docking | Partial albinism and silvery grey hair |
| EBV-triggered | |||
| X-linked lymphoproliferative disorder type 1 (XLP1) | SH2D1A (SH2 Domain Containing 1A) | Defective killing of EBV-infected B cells | Severe HLH; Hypogammaglobulinemia, and lymphoma |
| X-linked lymphoproliferative disorder type 2 (XLP2) | XIAP (X-linked inhibitor of apoptosis protein) | Increased inhibition of apoptosis in EBV-infected cells (gain of function) | Mild, recurrent HLH (may be triggered by non-EBV viruses) |
| IL-2-inducible T cell kinase deficiency | ITK (IL2 inducible T cell kinase) | Impaired proliferation of EBV-specific T cells | Hodgkin lymphoma |
| CD27 deficiency | CD27 | Impaired proliferation of EBV-specific T cells | Combined immunodeficiency |
| X-linked immunodeficiency with magnesium defect (XMEM) | MAGT1 (Magnesium transporter 1) | Impaired proliferation of EBV-specific T cells | Combined immunodeficiency, chronic viral infections, and lymphoma |
| Inflammasome activation | |||
| Autoinflammatory disease | NLRC4 (NLR Family CARD Domain Containing 4) | Increased inflammasome activation (gain of function) | Mild and recurrent HLH |
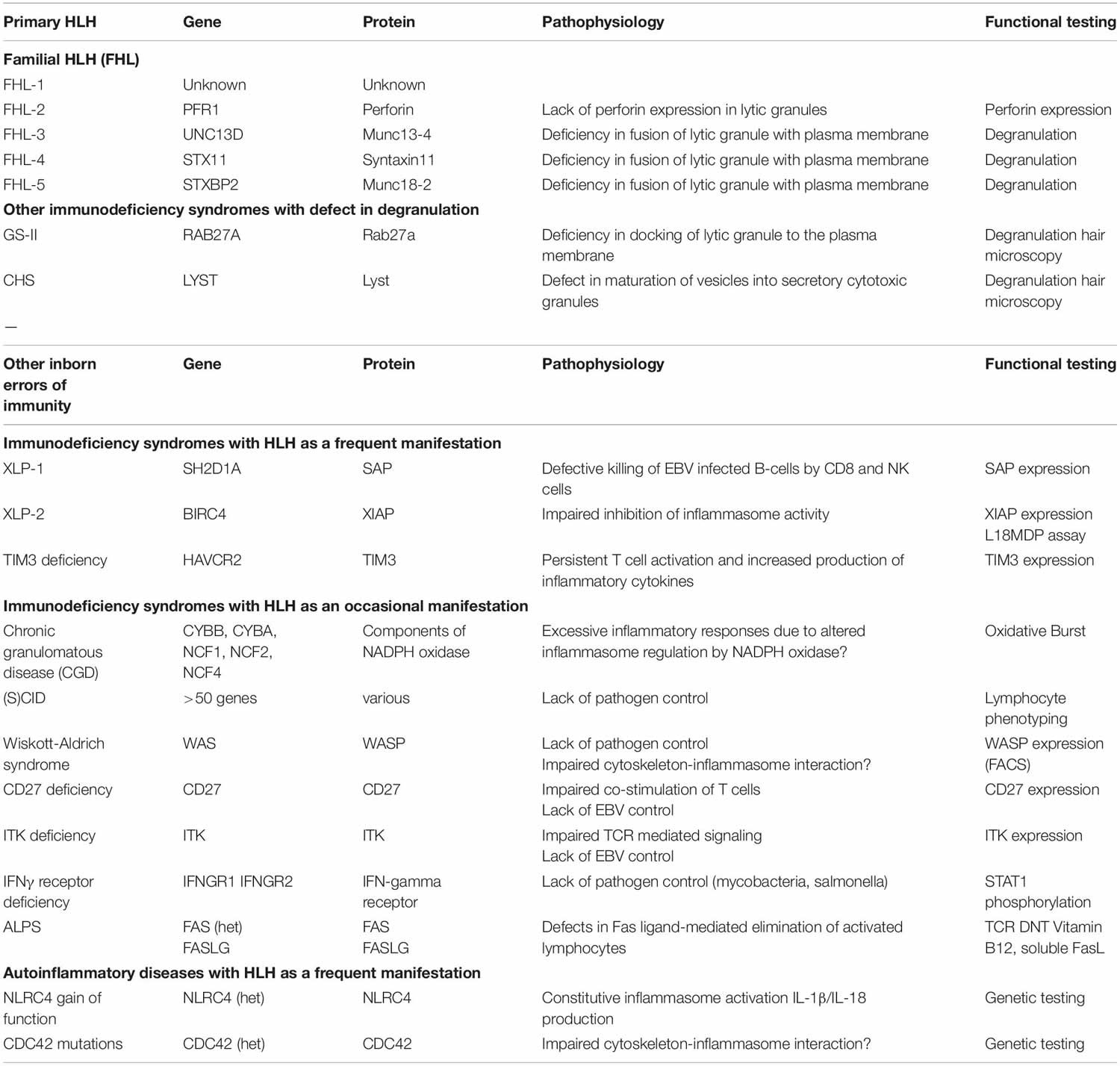
Abbreviations: CNS = central nervous system; EBV = Epstein-Barr virus.
[Source 192, 193 ]Familial hemophagocytic lymphohistiocytosis inheritance pattern
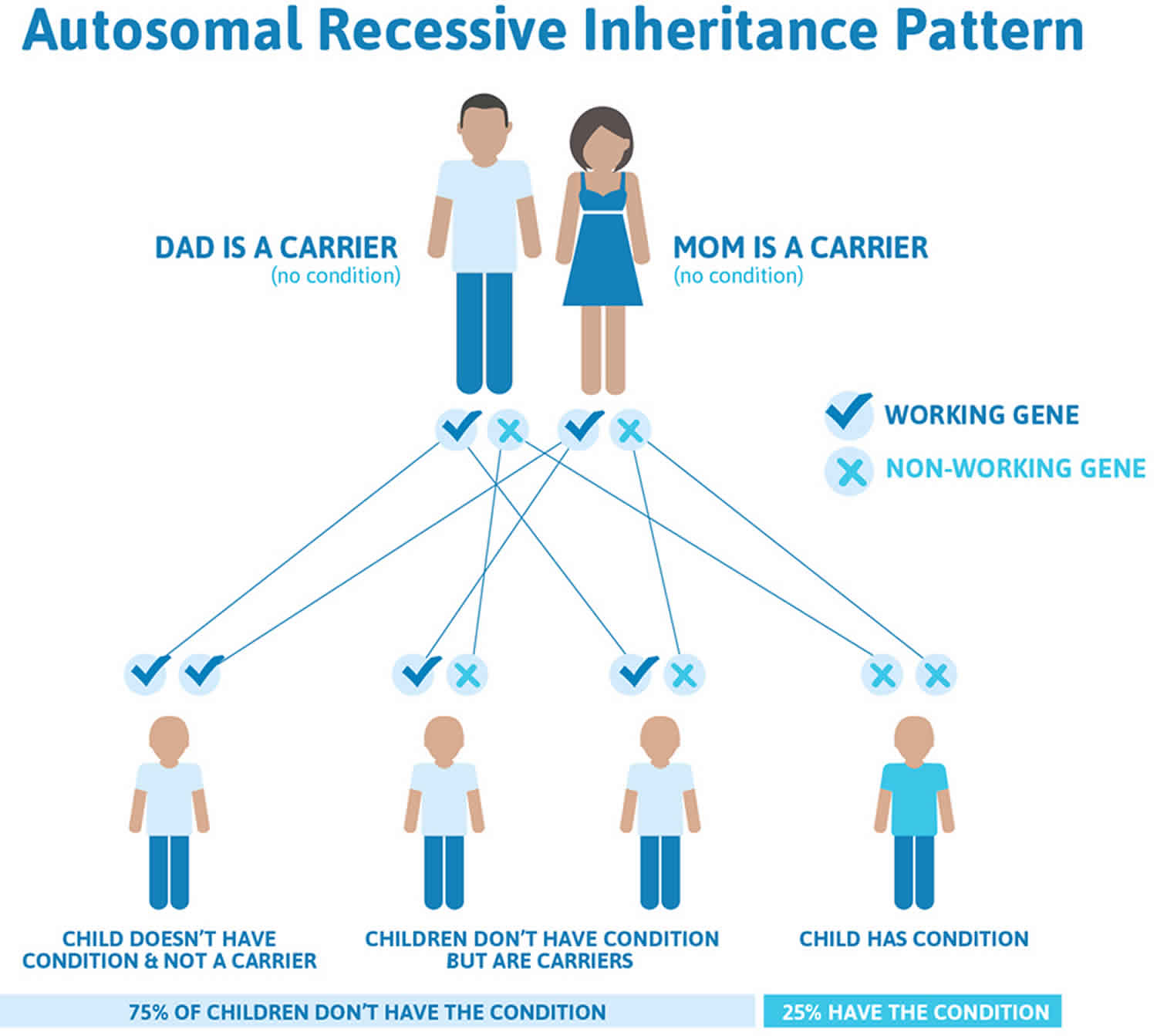
Apart from the egg and sperm cells, each cell of your body normally has two working copies of each gene. One copy of each gene comes from your biological mother, and one comes from your biological father. Most of the time, Familial hemophagocytic lymphohistiocytosis (F-HLH) or primary HLH is an autosomal recessive disorder. This means that for HLH to occur, both copies of the same HLH-associated genes must be mutated. In this situation, the parents are considered HLH “carriers” because they carry one normal and one altered copy of an HLH-associated gene in the cells of their bodies. Although they carry an altered gene copy, HLH carriers usually remain healthy and do not develop the signs and symptoms of HLH. However, they have a 50% chance of passing on the defective gene to their children.
Familial hemophagocytic lymphohistiocytosis autosomal recessive inheritance pattern means that a person must inherit two changed copies of the same gene (one abnormal gene from each parent) in order to have the condition. If a person inherits one abnormal gene and one normal gene, then in most cases that person will be a healthy carrier because the normal gene compensates for the abnormal gene. Being a carrier means that you do not have the condition, but carry a changed copy of the gene on one of a pair of genes.
- If both partners are carriers of the same abnormal gene, they may pass on either their normal gene or their abnormal gene to their child. This occurs randomly.
- Each child of parents who both carry the same abnormal gene therefore has a 25% (1 in 4) chance of inheriting a abnormal gene from both parents and being affected by the condition.
- This also means that there is a 75% ( 3 in 4) chance that a child will not be affected by the condition. This chance remains the same in every pregnancy and is the same for boys or girls.
- There is also a 50% (2 in 4) chance that the child will inherit just one copy of the abnormal gene from a parent. If this happens, then they will be healthy carriers like their parents.
- Lastly, there is a 25% (1 in 4) chance that the child will inherit both normal copies of the gene. In this case the child will not have the condition, and will not be a carrier.
These possible outcomes occur randomly. The chance remains the same in every pregnancy and is the same for boys and girls.
Figure 5 illustrates autosomal recessive inheritance. The example below shows what happens when both dad and mum is a carrier of the abnormal gene, there is only a 25% chance that they will both pass down the abnormal gene to the baby, thus causing a genetic condition.
Key points to remember
- A person must inherit two copies of a abnormal gene, one from each parent, in order to be affected by the condition (25% chance). If a person inherits only one abnormal gene then they will be a carrier (50% chance). These outcomes occur randomly. They remain the same in every pregnancy and are the same for boys and girls.
- A abnormal gene cannot be corrected – it is present for life.
- A abnormal gene is not something that can be caught from other people. They can still be a blood donor, for example.
- People often feel guilty about a genetic condition which runs in the family. It is important to remember that it is no-one’s fault and no-one has done anything to cause it to happen.
Figure 5. Familial hemophagocytic lymphohistiocytosis autosomal recessive inheritance pattern
Secondary hemophagocytic lymphohistiocytosis
Individuals with secondary HLH or acquired hemophagocytic lymphohistiocytosis develop the disorder because of a heightened, abnormal immune system response that occurs for unknown reasons. There is no family history of the disorder and no known genetic factors can be identified. Conditions that can lead to secondary hemophagocytic lymphohistiocytosis include viral infections especially Epstein-Barr virus, other infections including bacterial, viral and fungal infections, a weakened or depressed immune system, autoimmune diseases, autoinflammatory diseases, rheumatological diseases such as juvenile idiopathic arthritis, metabolic disorders, and cancer such as non-Hodgkin lymphoma.
Secondary HLH may occur at any age, and the first clinical symptoms are usually associated with an infectious episode, rheumatic condition, or malignancy 116. The clinical course may be severe, and the mortality is still significant 194. Recently, some cases of “secondary” HLH have been linked to mutations that confer a partial impairment of cytolytic function 116. These findings make the distinction between primary and secondary HLH increasingly difficult. Symptoms of HLH developing in a patient with an underlying rheumatic condition are historically called Macrophage Activation Syndrome (MAS). Suggestions to replace the term MAS with “secondary HLH” first appeared in the literature in 2002 195, 196. Emile et al 197 suggest using the term MAS-HLH for this subset of HLH.
Secondary hemophagocytic lymphohistiocytosis causes 197:
- Infection-associated HLH
- Virus-associated HLH
- Epstein-Barr virus (EBV)-associated HLH
- Cytomegalovirus (CMV)-associated HLH
- HLH associated with other defined herpes virus infections
- HIV-associated HLH
- Influenza-associated HLH
- HLH associated with other defined virus infections
- Bacteria-associated HLH
- Parasite-associated HLH
- Fungal-associated HLH
- Virus-associated HLH
- Malignancy-associated HLH
- Malignancy-triggered HLH (HLH at onset of malignancy)
- Hematological malignancies
- T-cell lymphoblastic lymphoma/leukemia
- T-cell non-lymphoblastic lymphomas
- B-cell leukemias
- B-cell lymphomas (non-Hodgkin)
- Hodgkin lymphomas
- Natural killer (NK)-cell lymphomas/leukemias
- Myeloid neoplasia
- Other hematological malignancies
- Solid tumors
- Unclassified malignancies
- Hematological malignancies
- HLH occurring during chemotherapy (not associated with initial diagnosis of malignancy)
- HLH associated with a malignancy, but not further defined
- Malignancy-triggered HLH (HLH at onset of malignancy)
- HLH associated with defined rheumatologic conditions (R-HLH or MAS-HLH)
- HLH associated with systemic-onset juvenile idiopathic arthritis (SoJIA)
- HLH associated with adult-onset Still disease
- HLH associated with SLE
- HLH associated with vasculitis
- HLH associated with other defined autoimmune conditions
- HLH associated with a not defined autoimmune condition
- Transplant-related HLH
- HLH associated with iatrogenic immune activation
- HLH associated with iatrogenic immune suppression
- HLH associated with other apparently non-Mendelian conditions
- HLH of unknown/uncertain origin
The exact manner that these predisposing conditions cause the signs and symptoms, and specifically how they cause an ineffective, abnormal immune response, in hemophagocytic lymphohistiocytosis are not fully understood and continue to be investigated.
Hemophagocytic lymphohistiocytosis disease triggers
Infection and cancer, acting alone or in concert with the above-mentioned genetic susceptibility factors, are common HLH triggers 186, 198. HLH that occurs in a patient who has a strong immunologic trigger such as infection or cancer, in the absence of a genetic disease which features HLH, are often said to have secondary HLH (acquired HLH).
Hemophagocytic lymphohistiocytosis can occur with virtually any infection or cancer. More common infections include DNA viruses (Epstein-Barr virus (EBV), cytomegalovirus, and adenovirus) and intracellular pathogens (eg, Leishmania), but the list of infections that have been reported to occur with HLH is extensive and influenced by geographic region (leishmaniasis and tick-borne illnesses), season (influenza viruses, tick-borne illnesses), and socioeconomic status (tuberculosis) 5. Immune reconstitution inflammatory syndrome occurring when newly treated HIV patients are coinfected with (usually) tuberculosis bears striking similarity to HLH and has been associated with high interleukin-18 (IL-18) 199. Features of HLH should be considered in all serious infections, and infectious disease consultation may be appropriate in many/most HLH patients.
Lymphoma and leukemia are common malignancies associated with HLH, particularly T-cell and NK-cell lymphomas or leukemias, diffuse large B-cell lymphoma, and Hodgkin lymphoma 200. Solid tumors can also trigger HLH. It is important to realize that hemophagocytic lymphohistiocytosis is due to an underlying cancer in >50% of adult cases 201, 202. Aggressive evaluations should be performed to evaluate for cancer in adult patients with HLH.
Hemophagocytic lymphohistiocytosis can also occur during the course of chemotherapy and is often associated with an infection 200. Treatment with chimeric antigen receptor–modified T cells called CAR T-cell therapy or bispecific T-cell–engaging antibodies can be associated with a cytokine release syndrome that mimics hemophagocytic lymphohistiocytosis 203, 204.
Hemophagocytic lymphohistiocytosis pathophysiology
The cellular and molecular mechanisms underlying HLH are incompletely understood. HLH is not one disease, but rather a distinct state of sustained immune system activation that may be engaged through a number of different pathways, depending on an individual’s predispositions and environmental triggers. Three major observations can be distilled from decades of clinical observation, genetic analysis, and basic science research 4:
- Disease in HLH is driven primarily by the aberrant immune response, not underlying triggers;
- Immune responses in HLH do not appear to target self-antigens, as seen in autoimmune diseases; and
- Uncontrolled activation of T cells (especially CD8+ cytotoxic T cells), not macrophages, is the root abnormality in most forms of HLH.
Genetic susceptibility to HLH clusters around genes whose products are involved in cell-mediated cytotoxicity and lymphocyte activation/survival. Immunosuppression and chronic inflammation also predispose to HLH; in these settings, HLH is often triggered by infection, most often viruses, but also other intracellular pathogens. Certain hematological malignancies and cancer-related therapies may trigger and drive HLH in the absence of identifiable genetic or infectious factors. Clinical and laboratory features of HLH reflect tissue infiltration by activated immune cells (especially T cells, macrophages, and neutrophils) and the local and systemic effects of inflammatory cytokines such as IFN-γ, tumor necrosis factor (TNF)-α, IL-1β, IL-6, IL-10, and IL-18 205, 206. Perpetuation of HLH immunopathology appears to involve feed-forward amplification loops whereby activated CD8+ T cells and macrophages stimulate each other in a so-called “cytokine storm.”
The pathogenesis of HLH has mostly been studied in familial hemophagocytic lymphohistiocytosis (FHL). An inherited defect in the perforin/granzyme pathway or in the fusion of cytotoxic lytic granules with the surface of natural killer (NK) cells causes, in the presence of an external trigger, an over-response by cytotoxic CD8+ T lymphocytes 1. Viral infections are the most common triggers 207.
Cytotoxic CD8+ T cells produce large amounts of interferon gamma (IFN-γ), which in turn activates macrophages 1. Overstimulated macrophages release large amounts of inflammatory cytokines, such as interleukin-1 beta (IL-1β), interleukin-6 (IL-6), interleukin-12 (IL-12), interleukin-18 (IL-18) and tumor necrosis factor alpha (TNFα). There is also an increased production of interleukin-10 (IL-10), with inhibitory activity, but not sufficient to limit the phenomenon 1. IL-12 and IL-18 produced by macrophages in turn stimulate CD8+ T cells, amplifying the inflammatory response 6. The resulting tissue damage causes a release of interleukin-33 (IL-33) and IL-1β, which further activates the macrophages. Activated macrophages engulf blood cells and produce large amounts of ferritin. The ‘cytokine storm’ causes all the clinical manifestations of HLH, from endothelial damage to coagulopathy and multi-organ failure 6, 28, 208, 209, 210. The central role of interferon gamma (IFN-γ) in the pathogenesis of familial hemophagocytic lymphohistiocytosis has been demonstrated in a perforin-deficient mouse model 211.
A similar pathogenesis of HLH can also be observed in patients with primary immunodeficiencies involving granule trafficking or exocytosis, such as Hermansky-Pudlak syndrome type 2, Griscelli syndrome type 2 and Chediak-Higashi syndrome 2, all with reduced cytotoxic T lymphocytes (CTL) cytotoxicity 11, 12. Advances in genetic diagnosis suggest that cell killing by cytotoxic T lymphocytes (CTLs) and NK cells can be affected from mildly to severely, thus explaining the different HLH phenotypes as a continuum 212. The known mutations in genes related to granule-mediated killing account for familial hemophagocytic lymphohistiocytosis (FHL) and primary forms in general 20. Minor alterations of the cytotoxic T lymphocytes (CTL) and NK cells activity, together with an external trigger, account for secondary HLH, severe sepsis, multi-organ failure and HLH in the context of rheumatologic diseases 212.
In all cases, a cytokine storm causing a devastating inflammation is the primal agent of the multiorgan failure, regardless of the underlying defect 213, 212, 214, 215, 216, 139 and HLH should be considered a clinical syndrome of hyperinflammation with different phenotypes 23. Moreover, this finding likely explains the numerous similarities and overlaps between HLH and other systemic inflammatory syndromes, such as septic shock, cytokine release syndrome following viral infections 139 and acute liver failure 217.
The case of malignancy-associated HLH includes two completely heterogeneous mechanisms. Firstly, when HLH is a manifestation of the underlying malignancy, particularly in the case of lymphomas, the overproduction of inflammatory cytokines such as INF-γ and TNF-α is likely caused by neoplastic cells 6, 124. Secondly, when HLH develops as the consequence of chemotherapy, the process is more likely to be caused by the association of drug-induced cytotoxic T lymphocytes (CTL) suppression and infection 187.
Figure 6. Hemophagocytic lymphohistiocytosis pathophysiology
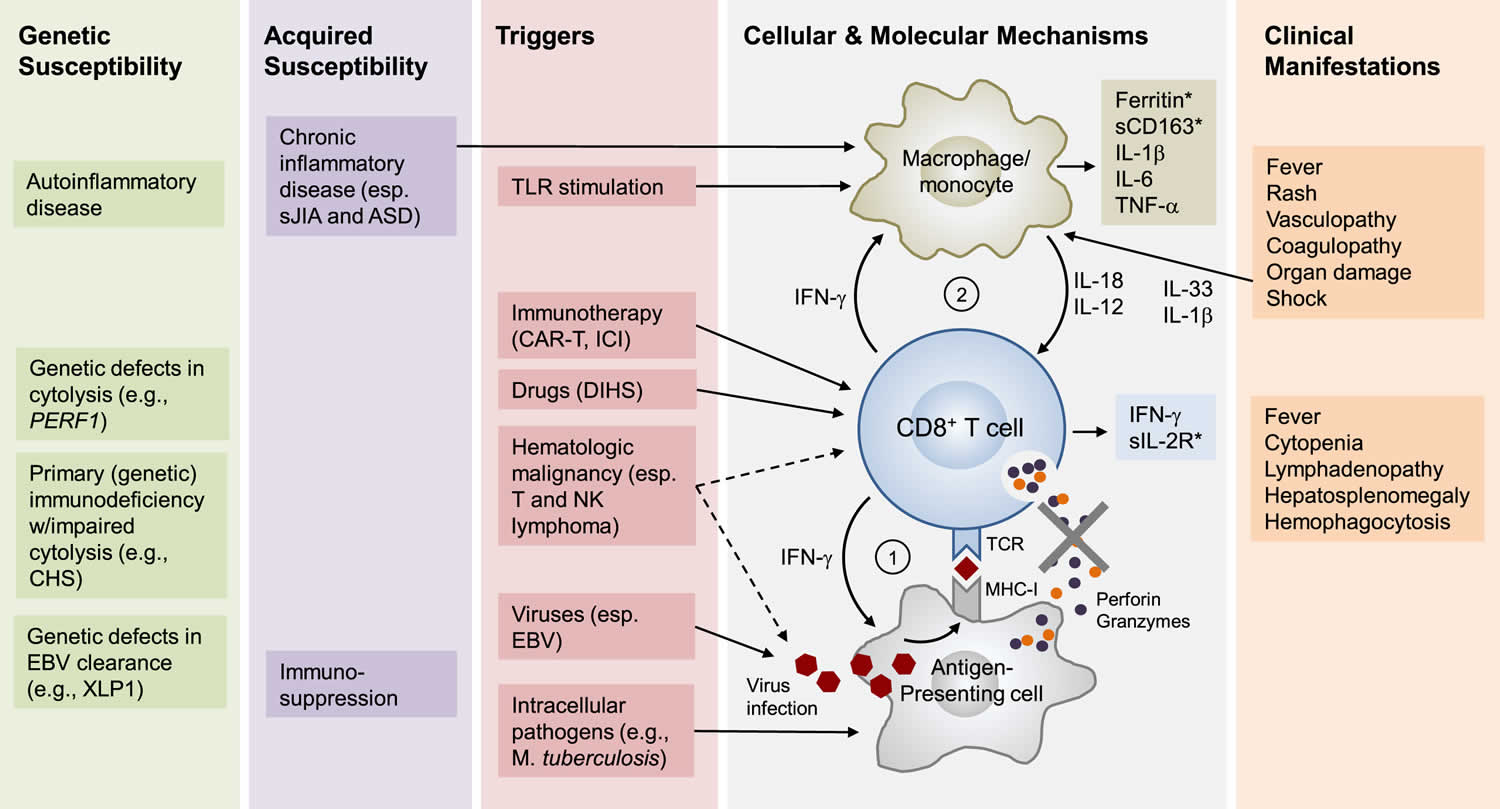
Footnotes: HLH is not one disease but rather a highly distinct state of immunological hyperactivation that has many different causes. A sustained and uncontrolled activation of CD8+ T cells is a core immunological feature of HLH; and in most forms of HLH, this activation is sustained by amplification loops involving antigen-presenting cells (APCs) and macrophages/monocytes. Depending on the individual, the development of HLH involves genetic and/or acquired risk factors. In familial HLH (F-HLH), genetic defects in cytolysis are the primary determinants of risk. In HLH associated with systemic juvenile idiopathic arthritis (sJIA), risk is determined by genetic and acquired factors, particularly chronic inflammation. In adults, HLH most often occurs in the settings of untreated hematological malignancy, chronic rheumatic disease, or immunosuppression. In many patients with HLH, a proximate inciting event or agent (trigger) is identified, most often an infection (particularly viral), occult hematological malignancy (particularly T or NK lymphoma), recent/ongoing immune-activating therapy (e.g., CAR-T therapy), or certain drugs associated with drug-induced hypersensitivity syndromes (DIHS). In F-HLH and certain forms of HLH associated with primary EBV infection, genetic defects in the killing of virally infected cells (e.g., PERF1 deficiency) results in sustained antigen presentation to, and activation of, CD8+ T cells, which is amplified by IFN-g release and subsequent MHC-I upregulation (Loop #1). Sustained IFN-g release from activated CD8+ T cells is believed to drive the activation of tissue macrophages/monocytes, which results in the release of inflammatory mediators such as IL-1b, IL-6, IL-18, and IL-12. IL-18 and IL-12 may serve to enhance IFN-g production by CD8+ T cells (Loop #2). Macrophages/monocytes are further activated by chronic inflammation, tissue injury (through Il-1b and IL-33), and TLR stimulation from infection. In malignancy-associated HLH, transformed cells may drive HLH through autonomous cytokine release and/or sustained presentation of EBV antigen. HLH after CAR-T therapy likely reflects exuberant activation of therapeutic CD8+ CAR-T cells. In HLH associated with DIHS, drug-MHC-I complexes may drive CD8+ T cell hyperactivation. Important clinical and laboratory abnormalities appear to be driven by macrophage/monocyte- and T-cell-derived molecules, several of which serve as important disease biomarkers (∗). Abbreviations: ASD, adult onset Stills disease; CAR-T, chimeric antigen receptor T cell; CHS, Chédiak-Higashi syndrome; DIHS, drug-induced hypersensitivity syndrome; EBV, Epstein-Barr virus; ICI, immune checkpoint inhibitor; MHC-I, major histocompatibility complex I; PERF-1, perforin-1; sIL-2 R, soluble Il-2 receptor; sJIA, systemic juvenile idiopathic arthritis; TCR, T cell antigen receptor; TLR, toll-like receptor; XLP1, and X-linked lymphoproliferative disorder type 1.
[Source 193 ]Hemophagocytic lymphohistiocytosis signs and symptoms
The onset and severity of hemophagocytic lymphohistiocytosis can vary greatly from one person to another 218. The specific symptoms that develop can also vary greatly, although HLH often causes multiorgan involvement. Generally, affected individuals develop fevers, a rash, an abnormally large liver (hepatomegaly), and an abnormally large spleen (splenomegaly). Fevers of unknown origin may be prolonged and persistent, often failing to respond to antibiotics 218. Sometimes, the lymph nodes are also abnormally large (lymphadenopathy). Lymph nodes are part of your lymphatic system, a circulatory network of vessels, ducts, and nodes that filter and distribute certain protein-rich (lymph) and blood cells throughout the body. Lymph nodes are small structures, found in groups throughout the body, that help to filter or drain out harmful substances from the body.
These initial sign and symptoms are described as nonspecific. This means that these signs and symptoms are common to many other different disorders or conditions, which can make getting a correct diagnosis difficult.
Affected individuals may also have low levels circulating red blood cells (anemia) and low levels of circulating platelets (thrombocytopenia). Red blood cells deliver oxygen to the body and platelets allow the body to form clots to stop bleeding. Individuals with anemia may experience tiredness, increased need for sleep, weakness, lightheadedness, dizziness, irritability, headaches, pale skin color, difficulty breathing (dyspnea), and cardiac symptoms. Individuals with thrombocytopenia (low levels of circulating platelets) are more susceptible to excessive bruising following minimal injury and to spontaneous bleeding from the mucous membranes, especially those of the gums and nose.
Some affected individuals may develop neurological symptoms including seizures, changes in mental status and irritability, paralysis (palsy) of certain cranial nerves, and problems coordinating voluntary movements (ataxia). Affected individuals are at risk of developing posterior reversible encephalopathy syndrome, which causes a rapid onset of headaches, altered consciousness, seizures, and disturbances in vision. Neurological problems are most common with familial hemophagocytic lymphohistiocytosis.
Additional symptoms can occur depending upon the specific organ system involved in an individual. These symptoms can include significant problems breathing (lung dysfunction), severe low blood pressure (hypotension), liver inflammation (hepatitis), kidney dysfunction, yellowing of the skin and whites of the eyes (jaundice), swelling due to fluid accumulation (edema), abdominal swelling due to fluid accumulation (ascites), and a variety of skin problems including widespread, reddening of the skin because of inflammation (erythroderma), rashes, blood spots (purpura), and tiny spots on the skin due to bleeding under the skin (petechiae).
Infant with fever
While “classic” familial hemophagocytic lymphohistiocytosis may present at almost any age, it most commonly presents in infants under 1 year of age, and neonatal or in utero presentations are well described 219. This “typical” patient with HLH usually presents with fever and is then noted to have cytopenias and splenomegaly. Further investigation reveals an illappearing patient, sometimes with a critical sepsis-like appearance. Marrow biopsy is often obtained to evaluate for leukemia and may (variably) reveal hemophagocytosis, while not displaying malignancy. Though infection and malignancy must be carefully considered, a triggering infection may not be identified 220. While these patients are well described by current diagnostic criteria, their most striking features are typically the degree of cytopenias, hypofibrinogenemia (in the face of inflammation), and hepatosplenomegaly. This patient population is capable of sudden, severe, and unpredictable worsening, necessitating rapid diagnosis and aggressive intervention.
Older children with infection
Children over the age of 1 year with hemophagocytic lymphohistiocytosis typically have definable triggers, most commonly viral infection. Epstein-Barr virus (EBV) is the most frequently identified infection triggering HLH, followed by cytomegalovirus (CMV), though numerous other viral, bacterial, parasitic, and fungal infections have been reported 19, 221, 222. Though underlying genetic mutations may not be found in patients with EBV-HLH, disease is often responsive to standard treatments and rituximab may be a helpful adjunct, as it may decrease viral burden 223. EBV-associated HLH is usually seen with primary infection, though some patients may present with HLH (or HLH recurrence) associated with chronic active EBV infection 224. These patients typically have predominant EBV infection of T cells (less often NK cells), instead of B cells. Overall, clinical presentations in older patients are similar to those in younger patients, though they may vary widely in severity. While patients presenting with relatively milder acuity may only require corticosteroids or intravenous immune globulin, aggressive treatment may be appropriate, as early initiation of etoposide is associated with improved survival in severe EBV-HLH 225, 226, 227. Ferritin values are consistently high in older patients, and sCD25 is always elevated, though often not to the degree seen in infants.
Sepsis-like presentations
Patients with hemophagocytic lymphohistiocytosis (pediatric and adult) stand out as some of the most critically ill patients in the ICU 228, 229, 230. While HLH can be very difficult to discern from typical sepsis or multiple organ dysfunction syndrome (MODS), there are often clues that the severity of inflammation may be more than expected for critical illness and further investigation for possible HLH needs to be considered. These patients tend to be persistently febrile with significant cytopenias, especially thrombocytopenia, and require multiple transfusions 228, 230. Hypofibrinogenemia may be helpful to discern HLH from sepsis, though disseminated intravascular coagulation (DIC) may lead to a similar appearance 231, 232. Hepatosplenomegaly often seen in HLH but not in sepsis can aid in the diagnosis. If present, hemophagocytosis in tissue and bone marrow can be suggestive of HLH, but hemophagocytosis can be found in critically ill patients with no other HLH features 233, 234. Beyond patients with clear HLH disease, there is a growing body of evidence to support a macrophage activation syndrome (MAS) like phenotype in some patients with sepsis.55–58 Unfortunately, there are multiple definitions that have been used for MAS-like sepsis, but in general these patients are described as having MODS characterized by hyperferritinemia, hepatobiliary dysfunction, and DIC with or without bone marrow failure 235, 236, 237, 238. Whether these patients may benefit from immunosuppressive therapy is an active area of investigation.
Central nervous system involvement
Patients with familial hemophagocytic lymphohistiocytosis present with central nervous system (CNS) involvement about one-third of the time with symptoms including seizures, meningismus, signs of cranial nerve involvement, ataxia, dysarthria, and encephalopathy 239, 240. However, patients may also rarely present with isolated central nervous system (CNS) inflammation, without complete or even any systemic signs of HLH. Though rare, this isolated disease is an important forme fruste of HLH, which often presents insidiously with patients experiencing substantial delays in diagnosis 241. Cerebrospinal fluid analysis shows pleocytosis and hyperproteinemia, and brain biopsy reveals T-cell and histiocytic infiltrates. MRI findings in isolated or non-isolated CNS HLH typically include increased signal in T2-weighted images of widespread areas, with symmetric periventricular white matter hyperintensity, meningeal enhancement, diffusion restriction, and may progress to include necrosis 242, 243, 244. Age of onset of isolated CNS HLH varies greatly, but is most often seen in children over a year of age, as younger children will usually have accompanying systemic HLH 4.
Hemophagocytic lymphohistiocytosis differential diagnosis
Infections
Many infections may trigger hemophagocytic lymphohistiocytosis 4. Search for common HLH associated viruses by polymerase chain reaction (not serology) should be performed, as concurrent disseminated infection, not prior exposure, is the principal concern 4. Atypical infections that may lead to cytopenias, elevations of inflammatory markers, and other features of HLH include visceral leishmaniasis, atypical/tuberculous mycobacteria, histoplasmosis, ehrlichia, bartonella and Brucella species, disseminated adenovirus, and disseminated herpes simplex 4. In most cases, these infections should be considered as mimics of HLH disease as direct treatment of the infection is preferable to HLH-directed immune suppression, and the HLH syndrome does not appear to have a largely immune-mediated etiology in these patients.
Other hematologic disorders
Hematologic diseases that may present with a clear pattern of HLH include Langerhans cell histiocytosis involving the marrow and/or visceral organs; multicentric Castleman disease, especially the thrombocytopenia, anasarca, myelofibrosis, renal dysfunction, and organomegaly variant (TAFRO) 4. In both cases, therapy should be directed toward the underlying disorder, ±additional corticosteroids.
Drug reactions
Drug rash with eosinophilia and systemic symptoms (DRESS) may present as HLH, but should be treated by withdrawal of the offending agent, ±corticosteroids 4.
Storage and metabolic disorders
Patients with storage diseases including Wolman’s disease (infantile lysosomal acid lipase deficiency), Gaucher’s, and other disorders have been reported to fulfill HLH diagnostic criteria 245, 246, 247, 248. In most cases, these disorders should be considered as mimics of HLH disease, as they develop features of HLH (eg, splenomegaly, cytopenias) due to processes not involving immune hyperactivation. However, inflammation in these patients remains poorly studied and there is evidence of abnormal immune regulation in some contexts 249, 250. Similarly, patients with metabolic disorders including lysinuric protein intolerance (LPI) and others have also been reported to develop HLH 251, 252. Though these disorders should be also be considered as mimics of HLH disease, as they require different, specific treatment, the inflammatory features of lysinuric protein intolerance (LPI) in particular are notable and may benefit from immune suppression 253.
Newborns
The differential in newborns with fulminant liver failure includes gestational alloimmune liver disease (GALD), also called neonatal hemochromatosis 4. While patients with GALD present with hyperferritinemia and coagulopathy, hemophagocytosis, and other signs of inflammation are absent and extrahepatic siderosis is typically present 254. Disseminated HSV presenting with the syndrome of HLH should be viewed as a mimicker of HLH disease, and immune suppression may be more harmful than beneficial to patients.
Isolated CNS disease
Differential diagnosis includes autoimmune disseminated encephalomyelitis (ADEM), CNS vasculitis, multiple sclerosis, Rasmussen’s encephalitis, febrile infection–related epilepsy syndrome (FIRES), and acute necrotizing encephalopathy (ANE), or interferonopathies 240. Rasmussen’s encephalitis is usually recognized based on single hemispheric involvement; ANE may be distinguished from isolated CNS HLH due to its typical presentation with symmetric thalamic necrosis and an absence of extensive white matter changes; and interferonopathies may present with cerebral calcifications 255. Febrile infection–related epilepsy syndrome (FIRES) remains poorly defined and in some cases may actually represent undiagnosed HLH 256.
Hemophagocytic lymphohistiocytosis diagnosis
Diagnosing hemophagocytic lymphohistiocytosis can be challenging because many of its initial symptoms mimic other common conditions. Symptoms such as persistent fevers, respiratory issues, rash, anemia, seizures and enlarged liver, spleen or lymph nodes may be cause other conditions. Because the symptoms of hemophagocytic lymphohistiocytosis are nonspecific and may overlap with other inflammatory or hematopoietic diseases, affected individuals may often have been through a prolonged illness and be hospitalized before a diagnosis is made.
Figure 7 displays a hemophagocytic lymphohistiocytosis diagnostic algorithm in newly presenting patients.
Hemophagocytic lymphohistiocytosis diagnosis is based upon identification of characteristic symptoms, a detailed patient history, a thorough clinical evaluation and a variety of specialized tests. Guidelines have been published that detail the criteria necessary for a diagnosis of hemophagocytic lymphohistiocytosis (see Table 2).
HLH is diagnosed when an individual meets established HLH-2004 diagnostic criteria 231. HLH-2004 criteria for diagnosis of HLH requires either 1 or 2.
- The presence of a known HLH-causing genetic mutation, OR
- Has five or more of the clinical or laboratory findings listed below:
- High and often prolonged periods of fever (more than 7 days);
- Rash, irritability and/or seizures;
- An abnormally large spleen (splenomegaly);
- Low blood cells (cytopenias): red blood cells (hemoglobin less than 9 g/dL in adults, hemoglobin less than 10 g/dL in infants <4 wk), white blood cells (neutrophils less than 1 × 109/L), or platelets (platelets count less than 100 × 109/L);
- Abnormally high levels of a type of fat called a triglyceride in the blood (hypertriglyceridemia) triglyceride ≥ 3.0 mmol/L (≥ 265 mg/dl);
- Abnormally low levels of fibrinogen (a specific blood clotting protein) (hypofibrinogenemia) serum fibrinogen < 150 mg/dL;
- Destruction of blood cells by macrophages (hemophagocytosis) in the bone marrow, spleen, or lymph nodes and/or cerebrospinal fluid with no evidence of malignancy;
- Low or absent natural killer (NK) cell activity;
- Abnormal high levels of ferritin (a protein that binds to iron) in the blood (ferritin ≥ 500mcg/L); and
- Elevated soluble interleukin-2 receptor alpha chain (sCD25 ≥ 2400 U/mL), a specialized protein that builds up in the blood when the immune system is stimulated.
- Reduced expression of proteins such as perforin, signaling lymphocytic activation molecule-associated protein (SAP), X-linked inhibitor of apoptosis protein (XIAP), and/or depressed cell functions
On occasion, HLH may be strongly considered, and HLH-directed therapy may be initiated, even though the 5 HLH-2004 diagnostic criteria are not fulfilled 257.
If hemophagocytic activity is not proven at the time of presentation, further search for hemophagocytic activity is encouraged. If the bone marrow specimen is not conclusive, material may be obtained from other organs. Serial marrow aspirates over time may also be helpful. The following findings may provide strong supportive evidence for the diagnosis: spinal fluid pleocytosis (mononuclear cells) and/or elevated spinal fluid protein and histological picture in the liver resembling chronic persistent hepatitis (biopsy). Other abnormal clinical and laboratory findings consistent with the diagnosis are cerebromeningeal symptoms, lymph node enlargement, jaundice, edema, skin rash, hepatic enzyme abnormalities, hypoproteinemia, hyponatremia, and elevated very low-density lipoprotein (VLDL↑)/low high-density lipoprotein (HDL↓).
Figure 7. Hemophagocytic lymphohistiocytosis diagnostic algorithm
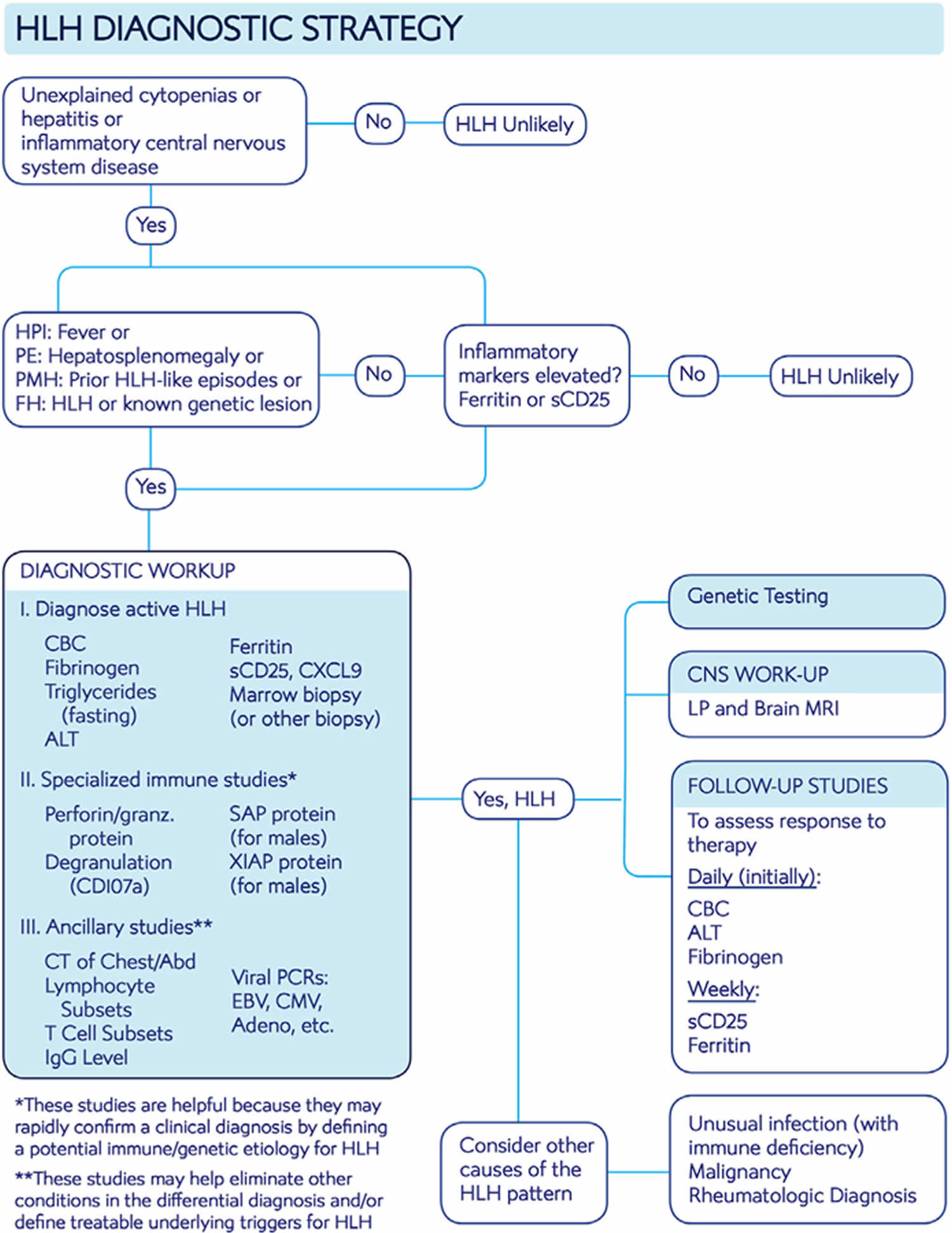
Table 2. Hemophagocytic lymphohistiocytosis diagnostic criteria
| HLH 2004 criteria | Comment |
|---|---|
| A. Molecular diagnosis consistent with HLH: Pathologic mutations of PRF1, UNC13D, STXBP2, Rab27a, STX11, SH2D1A, or XIAP or | In a patient with known genetic defects, treatment before full development of HLH may be appropriate, but genetic studies usually just help to define HLH recurrence risk, not the presence of an active disease state. |
| B. Five of the eight criteria listed below are fulfilled | |
| 1. Fever ≥38.3°C | Nearly universal in untreated HLH. |
| 2. Splenomegaly | While splenomegaly and hepatomegaly are very common in HLH, adenopathy is not. |
| 3. Cytopenias (affecting at least two of three lineages in the peripheral blood): Hemoglobin <9 g/dL (in infants <4 weeks: hemoglobin <10 g/dL) Platelets <100 × 10³/mL Neutrophils < 1 × 10³/mL | Cytopenias are ubiquitous in HLH. Lack of cytopenias should make one doubt a diagnosis of HLH, except in the special case of isolated, CNS-only disease. |
| 4. Hypertriglyceridemia (>265 mg/dL) and/or hypofibrinogenemia (<150 mg/dL) | Low fibrinogen in the context of inflammation is paradoxical and one of the more distinctive features of HLH. |
| 5. Hemophagocytosis in bone marrow or spleen or lymph nodes or liver | Not specific to HLH, or essential for the diagnosis, but helpful as a disease marker. Of note, it is often not evident early after disease onset. |
| 6. Low or absent NK-cell activity | More modern and robust assays measuring perforin levels and its degranulation should replace this assay for reliable diagnosis of HLH. This assay is not specific for primary HLH. |
| 7. Ferritin >500 ng/mL | Most patients have much higher levels than this threshold suggests. |
| 8. Elevated Soluble CD25 (soluble IL-2 receptor alpha) | As HLH is a T-cell driven disease, this assay is extremely informative for diagnosis and response to therapy. See Clinical Testing and Workup for patients with suspected HLH disease for more information. |
Clinical testing and workup for patients with suspected HLH disease
The initial workup is two-pronged and aims (a) to establish the diagnosis of HLH promptly and (b) to identify mimickers of HLH disease (if present), or potentially treatable underlying HLH disease triggers.
Common laboratory studies
- Complete blood count (CBC), hepatic panel, fibrinogen, triglycerides. Essential to define typical features of HLH. Though not part of diagnostic criteria, hepatitis is extremely common in HLH.
- Ferritin. Usually (but not always) very elevated
- Search for triggering infection with cultures, viral PCRs: EBV, CMV, adenovirus
Specialized laboratory studies
- Markers of immune activation: soluble interleukin-2 receptor alpha chain (sCD25), granzyme B expression and CXCL9. Essentially always elevated in untreated HLH; very sensitive, but not specific. sCD25, and perhaps CXCL9, are also useful for monitoring response to therapy
- Interlukin-18 (IL-18) level. Elevated in HLH associated with inflammasome-opathies (XIAP, NLRC4, systemic onset juvenile arthritis)
- Measurement of proteins affected in familial HLH: perforin, SAP, XIAP. Helpful to quickly confirm a suspected familial HLH diagnosis
- Functional studies: lymphocyte degranulation (CD107a mobilization), NK cell function. May help to fulfill diagnostic criteria. Degranulation is the preferred functional assay over NK cell function 259.
- Lymphocyte subsets, T-cell subsets, immune globulin levels. Screening studies for primary immune deficiency
- Genetic testing (multigene panel or whole exome). Essential for defining HLH recurrence risk
Imaging studies (should be routinely performed to help rule out malignancy, or unusual infections if trigger is unknown)
- Body cavity CT’s (chest/abdomen/pelvis)
- Consider 18F-fluorodeoxyglucose (FDG) positron emission tomography-computed tomography (PET-CT) if suspicion of lymphoma
- MRI of brain. Brain MRI complements lumbar puncture for central nervous system (CNS) assessment
Tissue sampling (essential to rule out malignancy, identify hemophagocytosis, and identify central nervous system (CNS) involvement)
- Bone marrow biopsy
- Lumbar puncture
- Other tissue biopsies as appropriate: liver, lymph node, masses
Physicians may order blood tests to take a complete blood cell count, which will measure the levels of red cells, white cells and platelets. Blood tests can also reveal abnormally high ferritin levels, or abnormal high levels of triglycerides. Physicians may also use blood tests to look for signs of infection in the blood and conduct tests to determine how well the blood clots (coagulation studies). Physicians may also order tests that can assess the health and function of the liver.
Sometimes, a bone marrow biopsy (the surgical removal and microscopic examination of a tissue sample) may be taken and studied for signs of hemophagocytosis, signs of infection or infectious organisms, and the accumulation of macrophages.
Molecular genetic testing can confirm a diagnosis of hemophagocytic lymphohistiocytosis in certain people. Molecular genetic testing can detect mutations in one of the four specific genes known to cause familial forms of this disorder, but is available only as a diagnostic service at specialized laboratories.
It should be emphasized that since T-cell activation is central to HLH pathogenesis, elevated soluble IL2 receptor alpha chain (sCD25) should always be observed in untreated HLH 123, 260, 261. If sCD25 is not elevated, then one should doubt a diagnosis of HLH 4. Similarly, though not as well established because HLH appears to be largely driven by interferon gamma (IFN-γ), elevations of CXCL9 (a sensitive indicator of IFN-γ bioactivity) should be seen in untreated cases of HLH disease 109, 262, 263. Additionally, elevated expression of granzyme B in NK cells has been shown to be similarly ubiquitous in HLH; normal expression levels would suggest that HLH is not the correct diagnosis 264. Ferritin levels above 10,000 ng/mL appear to be relatively specific for HLH but are not very sensitive 265. While specialized immunologic testing may facilitate diagnosis, if a diagnosis can be made without them then treatment should not be delayed pending these results. Likewise, treatment should not be delayed for assessment of central nervous system (CNS) involvement, though this should always be conducted (once a lumbar puncture may be safely performed).
Practical examples of when to not diagnose HLH disease
Certain clinical features may suggest mimics of HLH disease 4:
- Despite the common presence of splenomegaly, prominent or abnormal lymphadenopathy is not typically seen in HLH. This finding strongly suggests lymphoma, Castleman disease, or unusual infection such as HIV, histoplasmosis or mycobacterial disease 131. Similarly, leukocytosis is not typical of HLH (except in R-HLH/MAS) and should prompt a search for an alternative diagnosis.
- An extremely elevated sCD25 (>10- to 20-fold above normal) in a noninfantile patient suggests undiagnosed lymphoma, especially when ferritin is not similarly elevated 131, 266.
- The early occurrence of isolated and aggressive “CNS relapse” during treatment of systemic HLH may suggest an undiagnosed malignant disorder relapsing in the CNS.
- A normal or only modestly elevated sCD25, despite extremely elevated ferritin, suggests disseminated infection in the context of primary immune deficiency, especially in an infant 267.
Other diagnostic tools
Other features supporting an HLH diagnosis that are not part of the HLH-2004 diagnostic criteria include hyperbilirubinemia, hepatomegaly, transaminitis (present in the vast majority of patients with HLH), and elevated lactate dehydrogenase and d-dimer levels, with the latter usually elevated even when international normalized ratio, partial thromboplastin time, and fibrinogen are normal 181. These findings may help to discriminate HLH from septic shock and conditions such as autoimmune hemolytic anemia, and they are also useful in assessing response to therapy.
H Score
The HLH-probability calculator (HScore), with graded clinical and laboratory parameters, is a Web-based online calculator developed retrospectively in adult patients that may be a helpful diagnostic tool (Table 3) 268. The pattern of inflammatory cytokines (elevated levels of interferon-γ [IFN-γ] and IL-10, with only modestly elevated IL-6 levels) has high diagnostic accuracy for secondary hemophagocytic lymphohistiocytosis and may be a useful approach to differentiate HLH from infection and to monitor patients; however, the utility of this pattern of changes needs to be verified in children and adults outside of China 269, 270, 271.
Table 3. Parameters and points in the HScore
| Parameter | No. of points (criteria for scoring) |
|---|---|
| Known underlying immunosuppression* | 0 (no) or 18 (yes) |
| Temperature (°C) | 0 (<38.4), 33 (38.4–39.4), or 49 (>39.4) |
| Organomegaly | 0 (no), 23 (hepatomegaly or splenomegaly), or 38 (hepatomegaly and splenomegaly) |
| No. of cytopenias† | 0 (1 lineage), 24 (2 lineages), or 34 (3 lineages) |
| Ferritin (μg/L) | 0 (<2000), 35 (2000-6000), or 50 (>6000) |
| Triglyceride (mmol/L) | 0 (<1.5), 44 (1.5-4), or 64 (>4) |
| Fibrinogen (g/L) | 0 (>2.5) or 30 (≤2.5) |
| Aspartate aminotransferase (U/L) | 0 (<30) or 19 (≥30) |
| Hemophagocytosis on bone marrow aspirate | 0 (no) or 35 (yes) |
Footnote:
* HIV positive or receiving long-term immunosuppressive therapy (ie, glucocorticoids, cyclosporine A, azathioprine).
† Defined as a hemoglobin level of 9.2 g/L and/or a leukocyte count ≤5 × 109/L and/or a platelet count ≤110 × 109/L.
Hemophagocytic lymphohistiocytosis treatment
The treatment of hemophagocytic lymphohistiocytosis is directed toward the specific symptoms that are apparent in each individual. Treatment may require the coordinated efforts of a team of specialists. Pediatricians, specialists in diagnosing and treating blood disorders (hematologists), specialists in diagnosing and treating cancer (oncologists), specialists in diagnosing and treating immune system diseases (immunologists), geneticists (for familial forms), social workers, and other healthcare professionals may need to systematically and comprehensively plan treatment. Psychosocial support for the entire family is essential as well. Genetic counseling may be of benefit for affected individuals and their families. A useful algorithm for medical managements of adults with HLH is presented in Figure 8 below.
The aim of hemophagocytic lymphohistiocytosis treatment is to suppress the life-threatening inflammation that leads to organ damage 210. Specific therapeutic procedures and interventions may vary, depending upon numerous factors, such as the underlying cause; the presence or absence of certain symptoms; the overall severity of the symptoms and the disorder; an individual’s age and general health; and/or other elements. Decisions concerning the use of particular drug regimens and/or other treatments should be made by physicians and other members of the health care team in careful consultation with the patient based upon the specifics of his or her case; a thorough discussion of the potential benefits and risks, including possible side effects and long-term effects; patient preference; and other appropriate factors.
Affected individuals whose overall health is strong enough may undergo treatment for the underlying condition such as medications to treat an underlying infection, or appropriate treatment for autoimmune disorders or cancer. Treating the underlying condition may remove the “trigger” that has led to the abnormal immune system response.
The first goal is to induce disease remission by controlling the hyper-activated T cells and the cytokine storm they generate 20, 272. The second step, instead, may differ according to the underlying condition: in familial hemophagocytic lymphohistiocytosis and HLH cases, due to primary immunodeficiency, allogeneic hematopoietic stem cell transplantation (allo-HSCT) is the only curative treatment that is currently known, while there is no consensus on secondary hemophagocytic lymphohistiocytosis best treatment 1.
Affected individuals who health is deteriorating require treated specific for hemophagocytic lymphohistiocytosis immediately. In 1994, the Histiocyte Society published treatment recommendations for this disorder (HLA-94). There were also published studies from 2004 (HLA-2004) that were slightly different. In 1994, the Histiocyte Society introduced an etoposide-based treatment protocol for HLH, which is still the gold standard in the therapy of hemophagocytic lymphohistiocytosis disease 273. Etoposide, dexamethasone and cyclosporine act on the pathogenetic mechanisms of HLH, inhibiting T cells and the release of inflammatory cytokines 257. In this respect, etoposide has a very high immunosuppressive activity 274. These treatment regimens target and destroy the hyperactive immune system cells and reduce the life-threatening inflammation that characterizes hemophagocytic lymphohistiocytosis.
After initial treatment, which lasts about 8 weeks, affected individuals are gradually weaned off the drugs onto different medications. If affected individuals have not responded well to this treatment, an allogeneic stem cell transplant may be recommended. This treatment is also recommended for individuals with an abnormal variant in a known HLH gene, central nervous system involvement, and blood cancer (hematologic malignancy) that cannot be treated.
An allogeneic stem cell transplant is a procedure in which stem cells from an affected individual is replaced with the stem cells from a matched, healthy donor. Stem cells are special cells found in bone marrow that manufacture different types of blood cells (e.g. red blood cells, white blood cells, platelets).
Affected individuals undergo high-doses of chemotherapy or radiation to wipe out their stem cells. The stem cells are then replaced with those from a donor. Allogeneic stem cell transplant is a high-risk procedure with the potential for side effects.
Some affected individuals may need blood transfusion because they have low levels of circulating red blood cells or platelets. Some physicians may recommend antibiotics to prevent the development of an infection (prophylactic therapy).
Emapalumab (GAMIFANT) an anti-IFN-γ monoclonal antibody has been used successfully in children with refractory or previously untreated familial hemophagocytic lymphohistiocytosis 275, 276. In 2018, emapalumab was approved by the FDA for the treatment of children and adult patients with primary HLH who have refractory, recurrent or progressive disease or cannot tolerate conventional HLH therapy 277. Due to the risk of serious infections (frequent during therapy of primary HLH patients and observed in 32% of patients in the trial) patients should receive prophylaxis for Herpes Zoster, Pneumocystis jirovecii, and fungal infections and should be monitored for tuberculosis, adenovirus, EBV and CMV.
Another treatment capable of acting on HLH is anti-thymocyte globulin (ATG)-based immuno-therapy which has shown efficacy as a first-line therapy for familial hemophagocytic lymphohistiocytosis (F-HLH) 278. Epstein-Barr virus (EBV)-associated HLH can occur in X-linked lymphoproliferative type (XLP)1 and XLP2, where it is caused by signaling lymphocytic activation molecule-associated protein (SAP) or X-linked inhibitor of apoptosis protein (XIAP) deficiency and by the subsequent uncontrolled EBV infection 279, or in individuals without obvious immune defects. In the latter case, activation of cytotoxic CD8+ cells by EBV-infected B cells or a direct activation of CD8+ cells or NK cells by the virus has been hypothesized 280, 281. The addition of rituximab to an etoposide-based therapy is effective in the treatment of Epstein-Barr virus (EBV)-associated HLH, reducing the infected B lymphocyte population and EBV load 44.
Figure 8. Hemophagocytic lymphohistiocytosis treatment algorithm
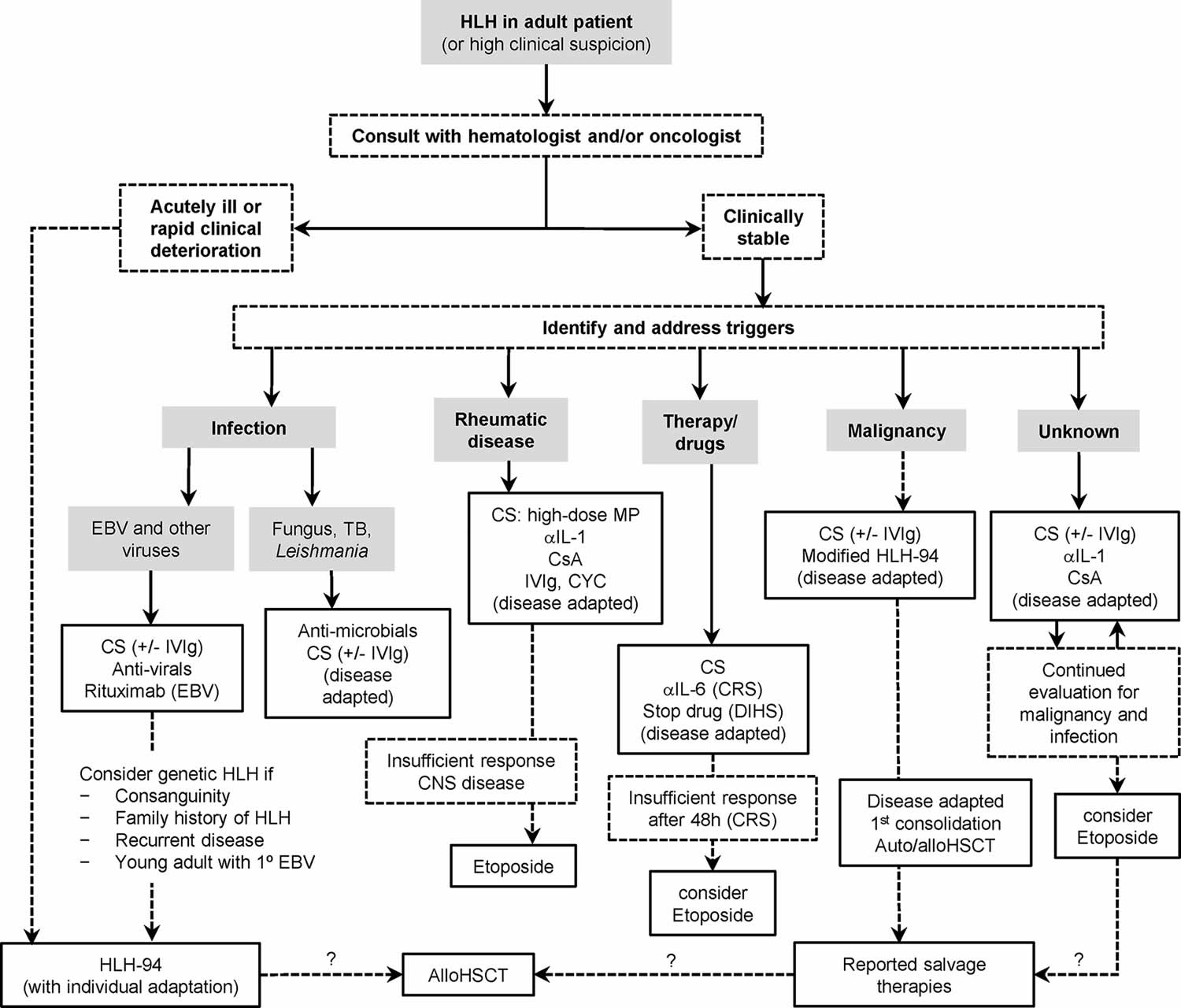
Footnotes: Management algorithm for adults with HLH or suspected HLH. The HLH-94 treatment protocol is consensus therapy for familial hemophagocytic lymphohistiocytosis (F-HLH). Medical treatment of adults with HLH is not standardized and should be adapted to severity of illness and underlying triggers (infection, rheumatic disease, drugs, and malignancy). Hematologists/oncologists should be involved early in care, because the treatment of severe, refractory, or relapsed disease involves chemotherapy (dashed lines) and case-by-case consideration of allogenic stem cell transplant or highly experimental therapies (question marks). Shown here are frequently encountered clinical scenarios (shaded boxes), major assessment nodes (dashed line boxes), and treatment options (solid line boxes).
Abbreviations: aIL-1, anti-IL-1 (e.g., anakinra); aIL-6, anti-IL-6 (e.g., tocilizumab); Allo-HSCT = allogeneic hematopoietic stem cell transplant; Auto-HSCT = autologous hematopoietic stem cell transplant; CNS = central nervous system; CRS = cytokine release syndrome; CS = corticosteroids; CsA = cyclosporine A; CYC = cyclophosphamide; DIHS = drug-induced hypersensitivity syndrome; EBV = Epstein-Barr virus; IVIg = intravenous immunoglobulin; MP = methylprednisolone; TB = Mycobacterium tuberculosis.
[Source 193 ]Figure 9. HLH-94 protocol
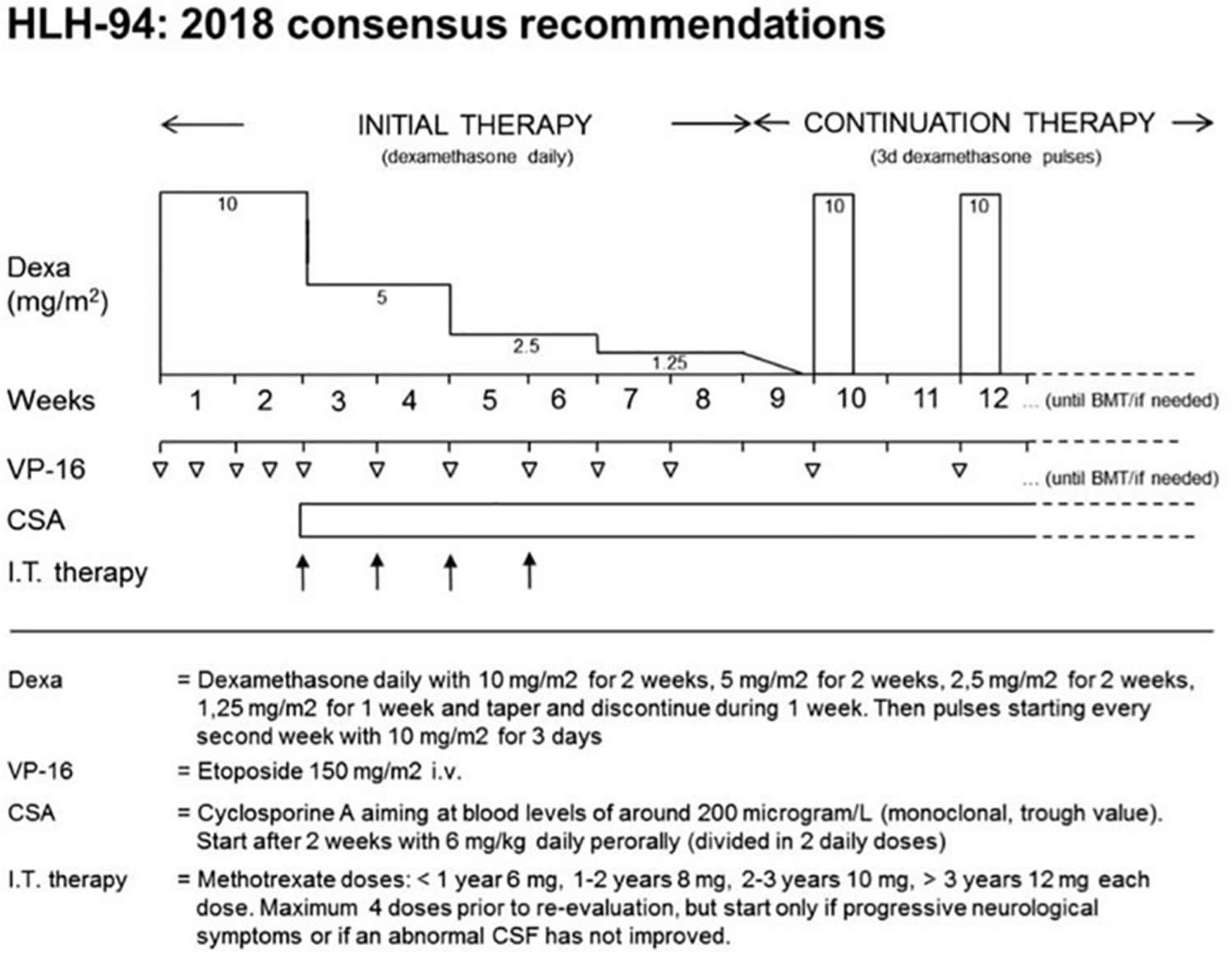
Footnotes: The HLH-94 protocol is based on immunochemotherapy including dexamethasone, etoposide, and cyclosporine A (CSA). After an intensive phase of 2 weeks with high doses of dexamethasone and twice weekly administration of etoposide, dexamethasone is tapered until week nine. Cyclosporine A (CSA) is used from week three onward to prevent reactivation. Intrathecal therapy with methotrexate is recommended in patients with central nervous system (CNS) involvement. Immunological testing and genetic confirmation of the underlying genetic disease is required in all patients and should provide the basis for hematopoietic stem cell transplantation (HSCT) within 8 weeks.
[Source 192 ]HLH-94 protocol
2018 consensus statements by the HLH Steering Committee of the Histiocyte Society recommending the use of HLH-94. The HLH-94 protocol is based on immuno-chemotherapy including dexamethasone, etoposide and cyclosporine A to achieve remission of the hyperinflammatory state and to maintain remission until hematopoietic stem cell transplantation (HSCT) can be performed 282. Functionally, all agents target lymphocytes, macrophages and antigen presenting cells. The cytostatic agent etoposide induces cell death mainly in activated T cells 283, but also in macrophages and dendritic cells. The use of the calcineurin inhibitor cyclosporine A leads to an inhibition of the transcription factor NFAT (nuclear factor of activated T-cells) and thus to a reduced activation and proliferation of T cells. Steroids slow down inflammation by reducing cytokine secretion, but in addition, they have a moderate cytotoxic effect on activated T cells. It is recommended to treat patients with central nervous system (CNS) involvement also with intrathecal methotrexate 284, although there is no clear evidence of benefit. The protocol has a 2-week intensive phase with dexamethasone and twice weekly administration of etoposide, followed by 6 weeks of weekly etoposide and steroid tapering. In this second phase, cyclosporine A is used to prevent reactivation 285. Rapid immunological testing followed by genetic confirmation of the underlying genetic disease is required in all patients and should provide the basis for hematopoietic stem cell transplantation (HSCT) within these 8 weeks. In the international multicenter registry-based HLH-2004 study, 5-year probability of survival for children with genetically verified familial HLH treated with this protocol was 59% 286. Dexamethasone/etoposide-based protocols have been successfully used in X-linked lymphoproliferative disorder or patients with TIM3 deficiency. It remains an ultimate choice also in other inborn errors of immunity, but the toxicity and immunosuppression associated with etoposide asks for more targeted therapies in these conditions.
Familial hemophagocytic lymphohistiocytosis treatment
For children with familial hemophagocytic lymphohistiocytosis, the first step in treatment is generally to suppress the overactive immune system. This is often done using a combination of steroids and chemotherapy, with the goal of putting the disease into remission. The Histiocyte Society first published international treatment protocol for HLH in 1994 (HLH-94), which combined chemotherapy and immunotherapy (etoposide and cyclosporine A [CsA]) for 8 weeks with or without intrathecal methotrexate in select patients to control the inflammatory response as a bridge to hematopoietic stem cell transplantation (HSCT) 287, 20. The HLH-94 protocol was reserved for patients with familial, relapsing, or severe/persistent HLH 239. HLH-94 dramatically improved survival in familial hemophagocytic lymphohistiocytosis from an estimated 5-year rate of 22% to an estimated 3-year rate of 51% ±20 239. The HLH-94 protocol (minus HSCT) was also found to be beneficial in secondary forms of HLH 288. For this reason, HLH-94 is often recommended by oncologists for the treatment of nonfamilial forms of HLH that are severe or relapsing 193.
Based on experience with HLH-94, the Histiocyte Society in 2004 modified the protocol (HLH-2004) in several ways, most notably by adding early and continuous cyclosporine A (CsA) therapy 231. During therapy with either protocol (HLH-94 or HLH-2004), patients should be monitored closely for clinical and laboratory response, and relapses should be expected as steroids are weaned (around week 6 in HLH-94) 4. HSCT remains the only long-term curative treatment, and achieving disease remission of HLH prior to transplant is essential for good prognosis, because HSCT complications (infection, excessive bleeding, organ failure, graft rejection, and graft versus host disease) and mortality are associated with HLH disease activity 289.
The HLH-94 induction chemotherapy is based on steroids and etoposide administration for 8 weeks with or without intrathecal methotrexate, followed by maintenance with cyclosporine A (CSA), etoposide and dexamethasone pulses while waiting for allogeneic hematopoietic stem cell transplantation (allo-HSCT) 287, 20. Chemotherapy might be suspended after 8 weeks of treatment once clinical remission is obtained and a clear genetic base is excluded 287. Otherwise, if a clear genetic base is proved, or in case of reactivation, hematopoietic stem cell transplantation (HSCT) is recommended 287.
After initial treatment, children with familial hemophagocytic lymphohistiocytosis usually undergo an allogeneic stem cell transplant (allo-HSCT), which replaces their defective immune system with a healthy one from a donor. Donor cells may come from a sibling, a parent or an unrelated donor. A stem cell transplant offers familial hemophagocytic lymphohistiocytosis patients the best chance for a cure 20, 287.
For disease refractory to HLH-94/2004, an anti-CD52 monoclonal antibody called alemtuzumab (which depletes T and B cells) has shown effectiveness as a salvage therapy 4, 290. Salvage therapy should be directed by oncologists and hematologists 193.
Secondary (acquired) hemophagocytic lymphohistiocytosis treatment
For children with secondary hemophagocytic lymphohistiocytosis, the aim is to identify and treat the underlying cause of HLH such as an infection, cancer or rheumatologic disease. In many cases, by treating the underlying cause, HLH will go into remission. In some cases, however, it will be necessary to use steroids and/or chemotherapy to treat the condition – similar to treatment for familial hemophagocytic lymphohistiocytosis.
Treatment for secondary HLH is determined more by the severity of the disorder and its symptoms, rather than its classification.
Treatment of infection-associated HLH depends on the underlying infection, since some forms respond to anti-infectious treatment such as Leishmania 291, 102, 103, Ehrlichiosis 96, scrub typhus 65, 66 and other tropical diseases-associated forms, while reaction to some other pathogens displays intermediate features and benefits of standard aggressive immunosuppression.
Several studies 291, 103, 292, 293 have reported complete response of Leishmania-associated HLH to amphotericin B therapy +/- steroids, with an excellent prognosis (3 year overall survival rate 24% in pHLH vs. 100% in visceral leishmaniasis-associated HLH in Iranian cohort of 60 children 102. A Chinese retrospective study 104 reported good results with antiparasitic therapy associated with chemotherapy according to the HLH94 protocol in patients with visceral leishmaniosis-HLH; however, the cohort includes children and adults and it is impossible to discriminate whether treatment intensification depends on age.
Human monocytic ehrlichiosis, can also trigger an HLH form that has proved to respond to antimicrobial therapy alone (doxycycline) 96.
Scrub typhus, dengue fever and tropical infections in general respond to steroids alone or to regimens without cytotoxic drugs in cases with mild to moderate disease activity 65, 66.
The hepatitis-associated HLH cases reviewed in the present study have experienced complete recovery on antiviral therapy and ruxolitinib in the case of a patient with hepatitis B virus infection 71 and after IVIG-infusion in the cases of patients with hepatitis A virus infection 70.
A patient developing HLH after HIV diagnosis has required both antiretroviral therapy and chemotherapy according to HLH94 protocol 72.
The Crimean Congo hemorrhagic fever-associated HLH has been resolved using antiviral therapy combined with IVIG therapy and plasma exchange 67.
The case of EBV-HLH is more complex. EBV-HLH standard treatment is by the HLH94 protocol, and early initiation of etoposide-based regimens improves survival in severe EBV-HLH 41, 52, 294. Chemotherapy can be combined with targeted therapies such as Rituximab 44, 163 or Ruxolitinib 295. Treatment intensification with the L-DEP regimen (PEG-asparaginase in combination with liposomal doxorubicin, etoposide and high-dose methylprednisolone) has been reported as salvage therapy and bridge to allo-HSCT for children with refractory disease 296. Blood purification techniques (plasma exchange and continuous renal replacement therapy) have proved to be safe and effective in addition to standard chemotherapy in severe cases 297. On the other hand, patients presenting with mild-to-moderate disease activity may only require immunomodulating therapies, such as IVIGs, cyclosporine A and steroids 54. A Japanese group 298 described a cohort of 22 patients aged 6 months to 41 years in which >60% recovered after immunotherapy (IVIG, cyclosporine A 6 mg/kg/day, prednisone); they suggest that early immunotherapy may modulate T-cell activation and reduce the chance of unnecessary chemotherapy. Sporadic cases of spontaneous resolution have been reported: An American group 299 reported the cases of two adolescents who fulfilled the HLH2004 diagnostic criteria in the context of an acute EBV infection. In both cases, treatment was planned according to HLH94 protocol, but the patients spontaneously improved before the initiation of therapy. The authors recommend caution in starting aggressive treatment, especially when patients experience mild-to-moderate symptoms. These differences in treatment approaches and outcomes underline the need for evidence-based risk stratification criteria in patients with EBV-HLH.
Cancer associated HLH (M-HLH) treatment
Malignancy-triggered forms should be distinguished from the forms that occur after chemotherapy (Ch-HLH) to optimize the therapeutic approach.
Hemophagocytic lymphohistiocytosis during chemotherapy (Ch-HLH) is often caused by infections related to immunosuppression, and benefits of anti-infectious therapy, steroids and IVIGs.
HLH as a manifestation of underlying malignancy. Cancer associated HLH (M-HLH) is associated with increased mortality and the early detection of malignancy can favorably influence the prognosis. Treatment is not homogeneous, and can address the underlying malignancy first, be focused on HLH or a combination of the two 300, 117, 126, 301, 302, 303. The published series refer to small numbers and suggest an individualized therapeutic approach. Aggressive HLH-directed therapy at the onset of malignancy-associated HLH can delay or complicate anticancer treatment 300, 187.
Rheumatologic HLH (MAS-HLH) treatment
MAS-HLH usually responds to steroid therapy or to anakinra (recombinant human IL-1 receptor antagonist), especially when given in the early course of therapy 304, 305. The present study refers to specific international guidelines for more detailed considerations on MAS-HLH 107, 306, 307.
HLH associated with iatrogenic immune activation treatment
The cytokine release syndrome following CAR-T or Blinatumomab administration usually responds to Tocilizumab, steroids, Anakinra or to a combination of such molecules 139, 147, 151. Whether carHLH should be differentiated from a severe form of cytokine-release syndrome is still an open question, and a more precise definition of both conditions is essential in order to guide therapeutic choices in the most complex cases 144, 308.
Post-transplant HLH requires prompt and aggressive treatment because of the high risk of graft failure, but no international consensus exists on treatment protocol. Reported therapeutic approaches range from corticosteroids, IVIGs and low-dose etoposide 309, 310, 311 to standard HLH-94 protocol with eventual rescue HSCT 154. Ruxolitinib was recently reported as salvage therapy in 2 children, with alternating results 312. Outcome is unclear, usually compromised by graft failure.
Emerging new treatments
Despite their success, the HLH-94 and HLH-2004 treatment protocols that involve the use of etoposide, cyclosporine A (CsA) and sustained high-dose corticosteroids carry significant risk of toxicity, infection, and long term adverse effects 193. Therefore, more targeted and less toxic treatments are needed, particularly for nongenetic forms of HLH where controlling aberrant inflammation and addressing underlying triggers can be curative 193. The most recent consensus guidelines on recognition, diagnosis and management of HLH in critically ill children 313 stress the importance of aggressive treatment. Steroids, in particular, should not be delayed as part of first-line treatment in different protocols (HLH-94 and ATG-based protocols) and are effective in both primary and secondary HLH.
A Canadian group reported nine cases of pediatric liver transplantation in acute liver failure secondary to acquired hemophagocytic lymphohistiocytosis, suggesting that HLH might not be an absolute contraindication to transplantation and instead play a role in a very restricted subgroup of patients 32.
A recently published Phase 2/3 trial 314 of the IFN-γ-blocking antibody, emapalumab, plus IV dexamethasone for the treatment of young children with presumed familial hemophagocytic lymphohistiocytosis (some resistant to HLH-94 protocol) showed remarkable efficacy (26% complete response, 30% partial response, and 7.4% some improvement); this led to the US FDA’s approval of emapalumab for the treatment of familial hemophagocytic lymphohistiocytosis in late 2018. Trials of emapalumab are being planned or underway in adult HLH (NCT03985423) and systemic Juvenile Idiopathic Arthritis (sJIA)-MAS/HLH (NCT03311854). There is increasing interest in the use of recombinant IL-18 binding protein (IL-18BP) in the treatment of HLH driven by IL-18, e.g., systemic Juvenile Idiopathic Arthritis (sJIA)-MAS/HLH and HLH associated with NLRC4 mutations 206. Similarly, IL-33, a member of the IL-1 family of cytokines, may be an important therapeutic target 206. Combination cytokine blockade has not been well studied in humans, but this strategy is likely to prove highly effective based on what is known about HLH amplification loops 193. Blockade of IL-1 with high-dose anakinra is often used when treating children with systemic Juvenile Idiopathic Arthritis (sJIA)-MAS/HLH, and related clinical trials are being planned or underway (NCT02780583).
Small molecule inhibitors of Janus kinases (JAKs), which transduce signals through various cytokine receptors, offer the ability to inhibit simultaneously multiple cytokine pathways with limited toxicity. Consistent with this concept, in a study of mouse models of both primary and secondary HLH 315, treatment with ruxolitinib, a small molecule JAK1/2 inhibitor (which inhibits IFN-γ and IL-6 signals), provided efficacy and broader effects than did treatment with IFN-γ-neutralizing antibodies. Wang et al. 316 conducted a study of ruxolitinib for salvage therapy, treating 34 patients with refractory/relapsed HLH (in addition to low-dose methylprednisolone in patients who were already on long-term high-dose corticosteroids). Complete remission was achieved in 15% of patients, and partial remission in 59% of patients 316. Currently, a prospective multicenter large-scale clinical trial is underway in China to evaluate combined ruxolitinib and doxorubicin for refractory/relapsed HLH (NCT03533790). JAK inhibition was also noted to be beneficial in the treatment of IL-18 pulmonary alveolar proteinosis-MAS patients 317.
Antibody-mediated ablation of lymphocytes, especially B cells, T cells, and NK cells, can be helpful in cases of severe or relapsed HLH, particularly EBV-HLH and M-HLH 22. Other salvage therapies include plasma exchange, splenectomy, and cytokine adsorption. Prescription and management of these highly experimental approaches should be directed by an oncologist or hematologist.
The most recent clinical trials focus on hybrid immunotherapy (ATG + etoposide + dexamethasone; NCT01104025), monoclonal antibodies such as Alemtuzumab 318 (NCT02472054) and tyrosine-kinase inhibitors such as ruxolitinib 319 and zanubrutinib (NCT05320575). Studies on selectively cytokine-targeting molecules include Tocilizumab 320 (NCT02007239), Anakinra (NCT02780583) and Emapalumab 276. In the subset of EBV-HLH patients, the ongoing clinical trials focus on Rituximab (NCT05384743), anti CD20 monoclonal antibody Sintilimab and Lenalidomide (NCT05258136), Tabelecleucel (NCT04554914), programmed cell death protein 1 antibody alone (NCT05039580) or in association with Lenalidomide (NCT04084626).
In intensive care settings, nonspecific physical therapies showed interesting results, at least in the acute phase 297, 321. If a massive release of cytokines/a cytokine storm is responsible for organ damage, blood purification techniques can blunt the process with a rapid non-selective effect, potentially translating into survival benefit 297. These techniques include plasma exchange, which has been successfully applied in medium resource contexts such as Turkey and India 322, 323, and hemofiltration combined with highly immune adsorbent cartridges 93, 272, 321. HLH recommendations have recognized blood purification as a potential salvage treatment in adults 324. Furthermore, these non-specific therapies might be combined with targeted therapies 325, but do not replace appropriate treatment of the underlying trigger of HLH, especially in patients with refractory disease 326.
Hemophagocytic lymphohistiocytosis prognosis
Hemophagocytic lymphohistiocytosis prognosis is related to the cause that induced secondary hemophagocytic lymphohistiocytosis, with the worst outcomes in cancer associated HLH (M-HLH) 1. In the 1980s, long-term survival in hemophagocytic lymphohistiocytosis was less than 5% 327. The HLH-94 protocol improved life expectancy up to 54% of 5-year survival, with similar results in familial hemophagocytic lymphohistiocytosis and secondary hemophagocytic lymphohistiocytosis patients. Unfortunately, the subsequent HLH-2004 treatment protocol failed to further improve the outcome 25.
An alternative therapeutic approach consisting of steroids, antithymocyte globulin (ATG) and cyclosporin has obtained satisfactory results, with a 70% remission rate 278. In general, in HLH the highest mortality is in the first weeks of therapy. In patients with familial hemophagocytic lymphohistiocytosis who underwent hematopoietic stem cell transplantation, a 5-year probability of overall survival of ~70% has been observed 328. Overall, hemophagocytic lymphohistiocytosis still carries a heavy burden of mortality up to the present day 1.
- Benevenuta C, Mussinatto I, Orsi C, Timeus FS. Secondary hemophagocytic lymphohistiocytosis in children (Review). Exp Ther Med. 2023 Jul 17;26(3):423. doi: 10.3892/etm.2023.12122[↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Janka GE. Familial and acquired hemophagocytic lymphohistiocytosis. Annu Rev Med. 2012;63:233-46. doi: 10.1146/annurev-med-041610-134208[↩]
- Bergsten E, Horne A, Aricó M, Astigarraga I, Egeler RM, Filipovich AH, Ishii E, Janka G, Ladisch S, Lehmberg K, McClain KL, Minkov M, Montgomery S, Nanduri V, Rosso D, Henter JI. Confirmed efficacy of etoposide and dexamethasone in HLH treatment: long-term results of the cooperative HLH-2004 study. Blood. 2017 Dec 21;130(25):2728-2738. doi: 10.1182/blood-2017-06-788349[↩]
- Jordan MB, Allen CE, Greenberg J, Henry M, Hermiston ML, Kumar A, Hines M, Eckstein O, Ladisch S, Nichols KE, Rodriguez-Galindo C, Wistinghausen B, McClain KL. Challenges in the diagnosis of hemophagocytic lymphohistiocytosis: Recommendations from the North American Consortium for Histiocytosis (NACHO). Pediatr Blood Cancer. 2019 Nov;66(11):e27929. doi: 10.1002/pbc.27929[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Canna SW, Marsh RA. Pediatric hemophagocytic lymphohistiocytosis. Blood. 2020 Apr 16;135(16):1332-1343. doi: 10.1182/blood.2019000936[↩][↩][↩][↩][↩][↩]
- Griffin G, Shenoi S, Hughes GC. Hemophagocytic lymphohistiocytosis: An update on pathogenesis, diagnosis, and therapy. Best Pract Res Clin Rheumatol. 2020;34(101515) doi: 10.1016/j.berh.2020.101515[↩][↩][↩][↩][↩][↩]
- Janka GE, Lehmberg K. Hemophagocytic syndromes – An update. Blood Rev. 2014;28(4):135–42. doi: 10.1016/j.blre.2014.03.002[↩][↩]
- Madkaikar M, Shabrish S, Desai M. Current Updates on Classification, Diagnosis and Treatment of Hemophagocytic Lymphohistiocytosis (HLH) Indian J Pediatr. 2016;83(5):434–43. doi: 10.1007/s12098-016-2037-y[↩]
- Farquhar JW, Claireaux AE. Familial haemophagocytic reticulosis. Arch Dis Child. 1952;27:519–525. doi: 10.1136/adc.27.136.519[↩]
- Price B, Lines J, Lewis D, Holland N. Haemophagocytic lymphohistiocytosis: A fulminant syndrome associated with multiorgan failure and high mortality that frequently masquerades as sepsis and shock. S Afr Med J. 2014;104:401–406. doi: 10.7196/samj.7810[↩]
- Brisse E, Wouters CH, Matthys P. Advances in the pathogenesis of primary and secondary haemophagocytic lymphohistiocytosis: Differences and similarities. Br J Haematol. 2016;174:203–217. doi: 10.1111/bjh.14147[↩][↩][↩]
- Brisse E, Matthys P, Wouters CH. Understanding the spectrum of haemophagocytic lymphohistiocytosis: Update on diagnostic challenges and therapeutic options. Br J Haematol. 2016;174:175–187. doi: 10.1111/bjh.14144[↩][↩][↩]
- George MR. Hemophagocytic lymphohistiocytosis: review of etiologies and management. J Blood Med. 2014 Jun 12;5:69-86. doi: 10.2147/JBM.S46255[↩]
- Shamriz O, Kumar D, Shim J, Briones M, Quarmyne MO, Chonat S, Lucas L, Edington H, White MH, Mahajan A, Park S, Chandrakasan S. T Cell-Epstein-Barr Virus-Associated Hemophagocytic Lymphohistiocytosis (HLH) Occurs in Non-Asians and Is Associated with a T Cell Activation State that Is Comparable to Primary HLH. J Clin Immunol. 2021 Oct;41(7):1582-1596. doi: 10.1007/s10875-021-01073-9. Epub 2021 Jun 26. Erratum in: J Clin Immunol. 2021 Aug 11[↩]
- Ladisch S, Poplack DG, Holiman B, Blaese RM. Immunodeficiency in familial erythrophagocytic lymphohistiocytosis. Lancet. 1978 Mar 18;1(8064):581-3. doi: 10.1016/s0140-6736(78)91028-0[↩]
- Jaffe ES, Costa J, Fauci AS, Cossman J, Tsokos M. Malignant lymphoma and erythrophagocytosis simulating malignant histiocytosis. Am J Med. 1983 Nov;75(5):741-9. doi: 10.1016/0002-9343(83)90402-3[↩]
- Hadchouel M, Prieur AM, Griscelli C. Acute hemorrhagic, hepatic, and neurologic manifestations in juvenile rheumatoid arthritis: possible relationship to drugs or infection. J Pediatr. 1985 Apr;106(4):561-6. doi: 10.1016/s0022-3476(85)80072-x[↩]
- Goldberg J, Nezelof C. Lymphohistiocytosis: a multi-factorial syndrome of macrophagic activation clinico-pathological study of 38 cases. Hematol Oncol. 1986 Oct-Dec;4(4):275-89. doi: 10.1002/hon.2900040405[↩]
- Risdall RJ, McKenna RW, Nesbit ME, Krivit W, Balfour HH Jr, Simmons RL, Brunning RD. Virus-associated hemophagocytic syndrome: a benign histiocytic proliferation distinct from malignant histiocytosis. Cancer. 1979 Sep;44(3):993-1002. doi: 10.1002/1097-0142(197909)44:3<993::aid-cncr2820440329>3.0.co;2-5[↩][↩]
- Henter JI, Horne A, Aricó M, Egeler RM, Filipovich AH, Imashuku S, Ladisch S, McClain K, Webb D, Winiarski J, Janka G. HLH-2004: Diagnostic and therapeutic guidelines for hemophagocytic lymphohistiocytosis. Pediatr Blood Cancer. 2007;48:124–131. doi: 10.1002/pbc.21039[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Allen CE, McClain KL. Pathophysiology and epidemiology of hemophagocytic lymphohistiocytosis. Hematology Am Soc Hematol Educ Program. 2015;2015:177-82. doi: 10.1182/asheducation-2015.1.177[↩]
- La Rosée P, Horne A, Hines M, von Bahr Greenwood T, Machowicz R, Berliner N, Birndt S, Gil-Herrera J, Girschikofsky M, Jordan MB, Kumar A, van Laar JAM, Lachmann G, Nichols KE, Ramanan AV, Wang Y, Wang Z, Janka G, Henter JI. Recommendations for the management of hemophagocytic lymphohistiocytosis in adults. Blood. 2019 Jun 6;133(23):2465-2477. doi: 10.1182/blood.2018894618[↩][↩]
- Freeman HR, Ramanan AV. Review of haemophagocytic lymphohistiocytosis. Arch Dis Child. 2011;96:688–693. doi: 10.1136/adc.2009.176610[↩][↩]
- Henter JI, Elinder G, Söder O, Hansson M, Andersson B, Andersson U. Hypercytokinemia in familial hemophagocytic lymphohistiocytosis. Blood. 1991 Dec 1;78(11):2918-22. https://doi.org/10.1182/blood.V78.11.2918.2918[↩]
- Bergsten E, Horne A, Aricó M, Astigarraga I, Egeler RM, Filipovich AH, Ishii E, Janka G, Ladisch S, Lehmberg K, et al. Confirmed efficacy of etoposide and dexamethasone in HLH treatment: Long-term results of the cooperative HLH-2004 study. Blood. 2017;130:2728–2738. doi: 10.1182/blood-2017-06-788349[↩][↩][↩]
- Ishii E, Ohga S, Imashuku S, Yasukawa M, Tsuda H, Miura I, Yamamoto K, Horiuchi H, Takada K, Ohshima K, et al. Nationwide survey of hemophagocytic lymphohistiocytosis in Japan. Int J Hematol. 2007;86:58–65. doi: 10.1532/IJH97.07012[↩]
- Cleves D, Lotero V, Medina D, Perez PM, Patiño JA, Torres-Canchala L, Olaya M. Pediatric hemophagocytic lymphohistiocytosis: A rarely diagnosed entity in a developing country. BMC Pediatr. 2021;21(411) doi: 10.1186/s12887-021-02879-7[↩]
- Sieni E, Cetica V, Piccin A, Gherlinzoni F, Sasso FC, Rabusin M, Attard L, Bosi A, Pende D, Moretta L, Aricò M. Familial hemophagocytic lymphohistiocytosis may present during adulthood: Clinical and genetic features of a small series. PLoS One. 2012;7(e44649) doi: 10.1371/journal.pone.0044649[↩][↩]
- Malinowska I, Machaczka M, Popko K, Siwicka A, Salamonowicz M, Nasiłowska-Adamska B. Hemophagocytic syndrome in children and adults. Arch Immunol Ther Exp (Warsz) 2014;62:385–394. doi: 10.1007/s00005-014-0274-1[↩][↩]
- Benson LA, Li H, Henderson LA, Solomon IH, Soldatos A, Murphy J, Bielekova B, Kennedy AL, Rivkin MJ, Davies KJ, et al. Pediatric CNS-isolated hemophagocytic lymphohistiocytosis. Neurol Neuroimmunol Neuroinflamm. 2019;6(e560) doi: 10.1212/NXI.0000000000000560[↩]
- de Kerguenec C, Hillaire S, Molinié V, Gardin C, Degott C, Erlinger S, Valla D. Hepatic manifestations of hemophagocytic syndrome: A study of 30 cases. Am J Gastroenterol. 2001;96:852–857. doi: 10.1111/j.1572-0241.2001.03632.x[↩]
- Amir AZ, Ling SC, Naqvi A, Weitzman S, Fecteau A, Grant D, Ghanekar A, Cattral M, Nalli N, Cutz E, et al. Liver transplantation for children with acute liver failure associated with secondary hemophagocytic lymphohistiocytosis. Liver Transpl. 2016;22:1245–1253. doi: 10.1002/lt.24485[↩][↩]
- Ramos-Casals M, Brito-Zerón P, López-Guillermo A, Khamashta MA, Bosch X. Adult haemophagocytic syndrome. Lancet. 2014;383:1503–1516. doi: 10.1016/S0140-6736(13)61048-X[↩][↩]
- Macheta M, Will AM, Houghton JB, Wynn RF. Prominent dyserythropoiesis in four cases of haemophagocytic lymphohistiocytosis. J Clin Pathol. 2001;54:961–963. doi: 10.1136/jcp.54.12.961[↩]
- Ehl S, Astigarraga I, von Bahr Greenwood T, Hines M, Horne A, Ishii E, Janka G, Jordan MB, La Rosée P, Lehmberg K, et al. Recommendations for the use of etoposide-based therapy and bone marrow transplantation for the treatment of HLH: Consensus statements by the HLH steering committee of the histiocyte society. J Allergy Clin Immunol Pract. 2018;6:1508–1517. doi: 10.1016/j.jaip.2018.05.031[↩]
- Hemophagocytic lymphohistiocytosis: Overview and diagnostic procedure. A case induced by an expansion of monoclonal EBV-negative NK cells. Inmunología Vol. 28, Núm 3, Julio-Septiembre 2009: 135-146. https://www.elsevier.es/es-revista-inmunologia-322-pdf-S021396260970037X[↩]
- Rosado FG, Kim AS. Hemophagocytic lymphohistiocytosis: an update on diagnosis and pathogenesis. Am J Clin Pathol. 2013 Jun;139(6):713-27. doi: 10.1309/AJCP4ZDKJ4ICOUAT[↩][↩][↩]
- Grzybowski B, Vishwanath VA. Hemophagocytic Lymphohistiocytosis: A Diagnostic Conundrum. J Pediatr Neurosci. 2017 Jan-Mar;12(1):55-60. doi: 10.4103/jpn.JPN_140_16[↩]
- Hemophagocytic Lymphohistiocytosis. https://imagebank.hematology.org/image/63563/hemophagocytic-lymphohistiocytosis[↩]
- Emile JF, Abla O, Fraitag S, Horne A, Haroche J, Donadieu J, Requena-Caballero L, Jordan MB, Abdel-Wahab O, Allen CE, et al. Revised classification of histiocytoses and neoplasms of the macrophage-dendritic cell lineages. Blood. 2016;127:2672–2681. doi: 10.1182/blood-2016-01-690636[↩][↩]
- Jordan MB, Allen CE, Greenberg J, Henry M, Hermiston ML, Kumar A, Hines M, Eckstein O, Ladisch S, Nichols KE, et al. Challenges in the diagnosis of hemophagocytic lymphohistiocytosis: Recommendations from the North American consortium for histiocytosis (NACHO) Pediatr Blood Cancer. 2019;66(e27929) doi: 10.1002/pbc.27929[↩][↩]
- Kawa K, Sawada A, Sato M, Okamura T, Sakata N, Kondo O, Kimoto T, Yamada K, Tokimasa S, Yasui M, Inoue M. Excellent outcome of allogeneic hematopoietic SCT with reduced-intensity conditioning for the treatment of chronic active EBV infection. Bone Marrow Transplant. 2011 Jan;46(1):77-83. doi: 10.1038/bmt.2010.122[↩]
- Fujiwara S, Kimura H, Imadome K, Arai A, Kodama E, Morio T, Shimizu N, Wakiguchi H. Current research on chronic active Epstein-Barr virus infection in Japan. Pediatr Int. 2014 Apr;56(2):159-66. doi: 10.1111/ped.12314[↩]
- Balamuth NJ, Nichols KE, Paessler M, Teachey DT. Use of rituximab in conjunction with immunosuppressive chemotherapy as a novel therapy for Epstein Barr virus-associated hemophagocytic lymphohistiocytosis. J Pediatr Hematol Oncol. 2007;29:569–573. doi: 10.1097/MPH.0b013e3180f61be3[↩][↩][↩][↩]
- Mărginean MO, Molnar E, Chinceşan MI. Epstein-Barr virus-associated hemophagocytic lymphohistiocytosis in a small child: A case report. Medicine (Baltimore) 2020;99(e18759) doi: 10.1097/MD.0000000000018759[↩]
- Fałkowska A, Prądzyńska K, Drabko K. Difficult balance between EBV treatment and posttransplant immunosuppression: A successful transplant in a child with recurrent Epstein-Barr virus-induced hemophagocytic lymphohistiocytosis. Transplant Proc. 2021;53:2035–2039. doi: 10.1016/j.transproceed.2021.03.044[↩]
- Pan H, Feng DN, Song L, Sun LR. Acute myeloid leukemia following etoposide therapy for EBV-associated hemophagocytic lymphohistiocytosis: A case report and a brief review of the literature. BMC Pediatr. 2016;16(116) doi: 10.1186/s12887-016-0649-z[↩]
- DomInguez-Pinilla N, Baro-Fernández M, González-Granado LI. Hemophagocytic lymphohistiocytosis secondary to Epstein Barr virus and Leishmania co-infection in a toddler. J Postgrad Med. 2015;61:44–45. doi: 10.4103/0022-3859.147052[↩]
- Gera A, Misra A, Tiwari A, Singh A, Mehndiratta S. A hungry Histiocyte, altered immunity and myriad of problems: Diagnostic challenges for Pediatric HLH. Int J Lab Hematol. 2021;43:1443–1450. doi: 10.1111/ijlh.13626[↩][↩][↩]
- Oguz MM, Sahin G, Altinel Acoglu E, Polat E, Yucel H, Oztek Celebi FZ, Unsal H, Akcaboy M, Sari E, Senel S. Secondary hemophagocytic lymphohistiocytosis in pediatric patients: A single center experience and factors that influenced patient prognosis. Pediatr Hematol Oncol. 2019;36:1–16. doi: 10.1080/08880018.2019.1572253[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Paul T, Kalra M, Danewa A, Sachdeva P, Thatikonda KB, Sachdeva D, Sachdeva A. Pediatric Hemophagocytic Lymphohistiocytosis – A Single Center Study. Indian Pediatr. 2022 Apr 15;59(4):283-286. https://www.indianpediatrics.net/apr2022/283.pdf[↩][↩][↩][↩][↩][↩][↩]
- Imashuku S, Tabata Y, Teramura T, Hibi S. Treatment strategies for Epstein-Barr virus-associated hemophagocytic lymphohistiocytosis (EBV-HLH) Leuk Lymphoma. 2000;39:37–49. doi: 10.3109/10428190009053537[↩][↩][↩]
- Kawaguchi H, Miyashita T, Herbst H, Niedobitek G, Asada M, Tsuchida M, Hanada R, Kinoshita A, Sakurai M, Kobayashi N, et al. Epstein-Barr virus-infected T lymphocytes in Epstein-Barr virus-associated hemophagocytic syndrome. J Clin Invest. 1993;92:1444–1450. doi: 10.1172/JCI116721[↩]
- Lin MT, Chang HM, Huang CJ, Chen WL, Lin CY, Lin CY, Chuang SS. Massive expansion of EBV+ monoclonal T cells with CD5 down regulation in EBV-associated haemophagocytic lymphohistiocytosis. J Clin Pathol. 2007;60:101–103. doi: 10.1136/jcp.2005.034371[↩][↩][↩]
- Imashuku S. Clinical features and treatment strategies of Epstein-Barr virus-associated hemophagocytic lymphohistiocytosis. Crit Rev Oncol Hematol. 2002;44:259–272. doi: 10.1016/s1040-8428(02)00117-8[↩][↩]
- Lohana C, Jhatial MA, Bokhari SWI. A challenging case of haemophagocytic lymphohistiocytosis (HLH) secondary to CMV infection in an adolescent with B-acute lymphoblastic leukemia. J Coll Physicians Surg Pak. 2021;31:1011–1012. doi: 10.29271/jcpsp.2021.08.1011[↩]
- Pessoa FS, Gonçalves VC, Lacerda EMDCB. Haemophagocytic lymphohistiocytosis secondary to intrauterine cytomegalovirus infection. Rev Inst Med Trop Sao Paulo. 2021;63(e15) doi: 10.1590/S1678-9946202163015[↩]
- Eldem İ, Al-Rahawan MM, Levent F. How to treat cytomegalovirus-induced hemophagocytic lymphohistiocytosis in a child with leukemia. J Pediatr Hematol Oncol. 2020;42:313–315. doi: 10.1097/MPH.0000000000001547[↩]
- Silwedel C, Frieauff E, Thomas W, Liese JG, Speer CP. Secondary haemophagocytic lymphohistiocytosis triggered by postnatally acquired cytomegalovirus infection in a late preterm infant. Infection. 2017;45:355–359. doi: 10.1007/s15010-016-0970-3[↩]
- Hasan MR, Sundaram MS, Sundararaju S, Tsui KM, Karim MY, Roscoe D, Imam O, Janahi MA, Thomas E, Dobson S, et al. Unusual accumulation of a wide array of antimicrobial resistance mechanisms in a patient with cytomegalovirus-associated hemophagocytic lymphohistiocytosis: A case report. BMC Infect Dis. 2020;20(237) doi: 10.1186/s12879-020-04966-z[↩]
- Gur G, Cakar N, Uncu N, Ayar G, Basaran O, Taktak A, Koksoy AY, Acar B, Caycı FS. Hemophagocytic lymphohistiocytosis secondary to Varicella zoster infection in a child with Henoch-Schönlein purpura. Pediatr Int. 2015;57:e37–e38. doi: 10.1111/ped.12523[↩]
- Agrawal G, Wazir S, Sachdeva A, Kumar S. Primary dengue infection triggered haemophagocytic lymphohistiocytosis in a neonate. BMJ Case Rep. 2020;13(e236881) doi: 10.1136/bcr-2020-236881[↩]
- Krithika MV, Amboiram P, Latha SM, Ninan B, Suman FR, Scott J. Neonate with haemophagocytic lymphohistiocytosis secondary to dengue infection: A case report. Trop Doct. 2017;47:253–255. doi: 10.1177/0049475516644102[↩]
- Jasmine YSY, Lee SL, Kan FK. Infection associated haemophagocytic syndrome in severe dengue infection-a case series in a district hospital. Med J Malaysia. 2017;72:62–64.[↩]
- Nandhakumar D, Loganatha A, Sivasankaran M, Sivabalan S, Munirathnam D. Hemophagocytic lymphohistiocytosis in children. Indian J Pediatr. 2020;87:526–531. doi: 10.1007/s12098-020-03190-6[↩][↩][↩][↩][↩][↩]
- Simon AC, Delhi Kumar CG, Basu D, Ramesh Kumar R. Hemophagocytic lymphohistiocytosis in children: Clinical profile and outcome. J Pediatr Hematol Oncol. 2020;42:e281–e285. doi: 10.1097/MPH.0000000000001791[↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Gayretli Aydin ZG, Yesilbas O, Reis GP, Guven B. The first pediatric case of hemophagocytic lymphohistiocytosis secondary to Crimean-Congo haemorrhagic fever successfully treated with therapeutic plasma exchange accompanying ribavirin and intravenous immunoglobulin. J Clin Apher. 2021;36:780–784. doi: 10.1002/jca.21915[↩][↩]
- Bıçakçı Z, Tavil B, Tezer H, Olcay L. Hemophagocytosis in a case with Crimean-Congo hemorrhagic fever and an overview of possible pathogenesis with current evidence. Turk J Pediatr. 2013 May-Jun;55(3):344-8.[↩]
- Mancao MY, Imran H, Chandra S, Estrada B, Figarola M, Sosnowski J, Vidal R. Eastern equine encephalitis virus infection and hemophagocytic lymphohistiocytosis in a 5-month-old infant. Pediatr Infect Dis J. 2009;28:543–545. doi: 10.1097/INF.0b013e3181950e99[↩]
- Bay A, Bosnak V, Leblebisatan G, Yavuz S, Yilmaz F, Hizli S. Hemophagocytic lymphohistiocytosis in 2 pediatric patients secondary to hepatitis A virus infection. Pediatr Hematol Oncol. 2012;29:211–214. doi: 10.3109/08880018.2012.666783[↩][↩]
- Jianguo L, Zhixuan Z, Rong L, Xiaodong S. Ruxolitinib in alleviating the cytokine storm of hemophagocytic lymphohistiocytosis. Pediatrics. 2020;146(e20191301) doi: 10.1542/peds.2019-1301[↩][↩]
- Chiperi LE, Ionescu AD, Marcu CT, Itu-Mureşan C, Pantelemon C. Hemophagocytic lymphohistiocytosis in a child with human immunodeficiency virus infection-a case report. Rom J Morphol Embryol. 2021;62:279–282. doi: 10.47162/RJME.62.1.29[↩][↩]
- Censoplano N, Gorga S, Waldeck K, Stillwell T, Rabah-Hammad R, Flori H. Neonatal adenovirus infection complicated by hemophagocytic lymphohistiocytosis syndrome. Pediatrics. 2018;141 (Suppl 5):S475–S480. doi: 10.1542/peds.2017-2061[↩]
- Otto WR, Behrens EM, Teachey DT, Lamson DM, Barrett DM, Bassiri H, Lambert MP, Mount S, Petrosa WL, Romberg N, et al. Human adenovirus 7-associated hemophagocytic lymphohistiocytosis-like illness: Clinical and virological characteristics in a cluster of five pediatric cases. Clin Infect Dis. 2021;73:e1532–e1538. doi: 10.1093/cid/ciaa1277[↩]
- Joshi R, Phatarpekar A, Currimbhoy Z, Desai M. Haemophagocytic lymphohistiocytosis: A case series from Mumbai. Ann Trop Paediatr. 2011;31:135–140. doi: 10.1179/1465328111Y.0000000009[↩]
- Zhang XY, Ye XW, Feng DX, Han J, Li D, Zhang C. Hemophagocytic lymphohistiocytosis induced by severe pandemic influenza A (H1N1) 2009 virus infection: A case report. Case Rep Med. 2011;2011(951910) doi: 10.1155/2011/951910[↩]
- Shrestha B, Omran A, Rong P, Wang W. Report of a fatal pediatric case of hemophagocytic lymphohistiocytosis associated with pandemic influenza A (H1N1) infection in 2009. Pediatr Neonatol. 2015;56:189–192. doi: 10.1016/j.pedneo.2013.03.006[↩]
- Ozdemir H, Çiftçi E, Ince EU, Ertem M, Ince E, Doğru U. Hemophagocytic lymphohistiocytosis associated with 2009 pandemic influenza A (H1N1) virus infection. J Pediatr Hematol Oncol. 2011;33:135–137. doi: 10.1097/MPH.0b013e3181f46baf[↩]
- Tholin B, Hauge MT, Aukrust P, Fehrle L, Tvedt TH. Hemophagocytic lymphohistiocytosis in a patient with COVID-19 treated with tocilizumab: A case report. J Med Case Rep. 2020;14(187) doi: 10.1186/s13256-020-02503-9[↩]
- Hakim NN, Chi J, Olazagasti C, Liu JM. Secondary hemophagocytic lymphohistiocytosis versus cytokine release syndrome in severe COVID-19 patients. Exp Biol Med (Maywood) 2021;246:5–9. doi: 10.1177/1535370220962043[↩]
- Mittal J, Kumar P, Goyal JP, Purohit A. Haemophagocytic lymphohistiocytosis secondary to brucellosis in a young child. BMJ Case Rep. 2021;14(e240759) doi: 10.1136/bcr-2020-240759[↩]
- Pekpak E, Sirvan Cetin B. Secondary hemophagocytic lymphohistocytosis in a child with brucellosis. J Pediatr Hematol Oncol. 2017;39:e501–e503. doi: 10.1097/MPH.0000000000000849[↩]
- Yaman Y, Gözmen S, Özkaya AK, Oymak Y, Apa H, Vergin C, Devrim İ. Secondary hemophagocytic lymphohistiocytosis in children with brucellosis: Report of three cases. J Infect Dev Ctries. 2015;9:1172–1176. doi: 10.3855/jidc.6090[↩]
- Banday AZ, Mehta R, Vignesh P, Kanaujia R, Durgadevi S, Angrup A, Kumar N, Ray P, Suri D. Case Report: Ceftriaxone-resistant invasive Salmonella enteritidis infection with secondary hemophagocytic lymphohistiocytosis: A contrast with enteric fever. Am J Trop Med Hyg. 2020;103:2515–2517. doi: 10.4269/ajtmh.20-0566[↩]
- Maheshwari P, Chhabra R, Yadav P. Perinatal tuberculosis associated hemophagocytic lymphohistiocytosis. Indian J Pediatr. 2012;79:1228–1229. doi: 10.1007/s12098-011-0675-7[↩]
- Choi YB, Yi DY. Fatal case of hemophagocytic lymphohistiocytosis associated with group B streptococcus sepsis: A case report. Medicine (Baltimore) 2018;97(e12210) doi: 10.1097/MD.0000000000012210[↩]
- Liu SS, Wang Y, Xue L, Ma C, Li CH. Hemophagocytic lymphohistiocytosis due to Streptococcus suis in a 12-year-old girl: A case report. Medicine (Baltimore) 2019;98(e15136) doi: 10.1097/MD.0000000000015136[↩]
- Sahu SK, Behera JR, Yadav SK. Scrub typhus with secondary hemophagocytic lymphohistiocytosis in a 3-month-old child from a tertiary care hospital of Odisha. Indian J Public Health. 2021;65:85–86. doi: 10.4103/ijph.IJPH_565_20[↩]
- Han DK, Baek HJ, Shin MG, Kim JW, Kook H, Hwang TJ. Scrub typhus-associated severe hemophagocytic lymphohistiocytosis with encephalomyelitis leading to permanent sequelae: A case report and review of the literature. J Pediatr Hematol Oncol. 2012;34:531–533. doi: 10.1097/MPH.0b013e318257a442[↩]
- Agrwal S, Dabas A, Mantan M, Yadav S. Hemophagocytic lymphohistiocytosis with neurological manifestations in an infant with scrub typhus: A rare fatal occurrence. Trop Doct. 2019;49:52–53. doi: 10.1177/0049475518804696[↩]
- Pazhaniyandi S, Lenin R, Sivathanu S. Hemophagocytic lymphohistiocytosis with a leukemoid reaction in an infant with scrub typhus. J Infect Public Health. 2015;8:626–629. doi: 10.1016/j.jiph.2015.05.012[↩]
- Otrock ZK, Gonzalez MD, Eby CS. Ehrlichia-induced hemophagocytic lymphohistiocytosis: A case series and review of literature. Blood Cells Mol Dis. 2015;55:191–193. doi: 10.1016/j.bcmd.2015.06.009[↩]
- Cheng A, Williams F, Fortenberry J, Preissig C, Salinas S, Kamat P. Use of extracorporeal support in hemophagocytic lymphohistiocytosis secondary to ehrlichiosis. Pediatrics. 2016;138(e20154176) doi: 10.1542/peds.2015-4176[↩][↩]
- Burns S, Saylors R, Mian A. Hemophagocytic lymphohistiocytosis secondary to Ehrlichia chaffeensis infection: A case report. J Pediatr Hematol Oncol. 2010;32:e142–143. doi: 10.1097/MPH.0b013e3181c80ab9[↩]
- Singh NS, Pagano AL, Hays AJ, Kats A, Dahl SM, Warady BA, Beins NT, Yin DE. Ehrlichia-induced hemophagocytic lymphohistiocytosis in a pediatric kidney transplant recipient. Pediatr Transplant. 2022;26(e14134) doi: 10.1111/petr.14134[↩][↩][↩]
- Cabler SS, Hogan PG, Fritz SA, Bednarski JJ, Hunstad DA. Incidence and treatment of hemophagocytic lymphohistiocytosis in hospitalized children with Ehrlichia infection. Pediatr Blood Cancer. 2020;67(e28436) doi: 10.1002/pbc.28436[↩][↩][↩]
- Tsuge M, Miyamoto M, Miyawaki R, Kondo Y, Tsukahara H. Hemophagocytic lymphohistiocytosis complicating invasive pneumococcal disease: A pediatric case report. BMC Pediatr. 2020;20(15) doi: 10.1186/s12887-020-1915-7[↩]
- Poudel A, Lew J, Slayton W, Dharnidharka VR. Bartonella henselae infection inducing hemophagocytic lymphohistiocytosis in a kidney transplant recipient. Pediatr Transplant. 2014;18:E83–E87. doi: 10.1111/petr.12235[↩][↩][↩]
- Edner J, Rudd E, Zheng C, Dahlander A, Eksborg S, Schneider EM, Edner A, Henter JI. Severe bacteria-associated hemophagocytic lymphohistiocytosis in an extremely premature infant. Acta Paediatr. 2007;96:1703–1706. doi: 10.1111/j.1651-2227.2007.00505.x[↩]
- Karapinar DY, Karadaş N, Yazici P, Polat SH, Karapinar B. Trichosporon asahii, sepsis, and secondary hemophagocytic lymphohistiocytosis in children with hematologic malignancy. Pediatr Hematol Oncol. 2014;31:282–284. doi: 10.3109/08880018.2013.851754[↩]
- Guo F, Kang L, Xu M. A case of pediatric visceral leishmaniasis-related hemophagocytic lymphohistiocytosis diagnosed by mNGS. Int J Infect Dis. 2020;97:27–29. doi: 10.1016/j.ijid.2020.05.056[↩]
- Mottaghipisheh H, Kalantar K, Amanati A, Shokripour M, Shahriari M, Zekavat OR, Zareifar S, Karimi M, Haghpanah S, Bordbar M. Comparison of the clinical features and outcome of children with hemophagocytic lymphohistiocytosis (HLH) secondary to visceral leishmaniasis and primary HLH: A single-center study. BMC Infect Dis. 2021;21(732) doi: 10.1186/s12879-021-06408-w[↩][↩][↩]
- de Carvalho FHG, Lula JF, Teles LF, Caldeira AP, de Carvalho SFG. Hemophagocytic lymphohistiocytosis secondary to visceral leishmaniasis in an endemic area in the north of Minas Gerais, Brazil. Rev Soc Bras Med Trop. 2020;53(e20190491) doi: 10.1590/0037-8682-0491-2019[↩][↩][↩]
- Shi Q, Huang M, Li X, Zheng X, Wang F, Zou Y, Wang L, Jia J. Clinical and laboratory characteristics of hemophagocytic lymphohistiocytosis induced by Leishmania infantum infection. PLoS Negl Trop Dis. 2021;15(e0009944) doi: 10.1371/journal.pntd.0009944[↩][↩]
- Srivatsav S, Mahalingam S, Ramineni P, Manya S. Dengue and Plasmodium falciparum coinfection with secondary hemophagocytic lymphohistiocytosis in a 3-year-old boy: A clinical conundrum. J Pediatr Hematol Oncol. 2022;44:e253–e254. doi: 10.1097/MPH.0000000000002018[↩]
- Padhi S, Varghese RGB, Ramdas A, Phansalkar MD, Sarangi R. Hemophagocytic lymphohistiocytosis: Critical reappraisal of a potentially under-recognized condition. Front Med. 2013;7:492–498. doi: 10.1007/s11684-013-0292-0[↩]
- Henderson LA, Cron RQ. Macrophage activation syndrome and secondary hemophagocytic lymphohistiocytosis in childhood inflammatory disorders: Diagnosis and management. Paediatr Drugs. 2020;22:29–44. doi: 10.1007/s40272-019-00367-1[↩][↩]
- Vastert SJ, van Wijk R, D’Urbano LE, de Vooght KM, de Jager W, Ravelli A, Magni-Manzoni S, Insalaco A, Cortis E, van Solinge WW, Prakken BJ, Wulffraat NM, de Benedetti F, Kuis W. Mutations in the perforin gene can be linked to macrophage activation syndrome in patients with systemic onset juvenile idiopathic arthritis. Rheumatology (Oxford). 2010 Mar;49(3):441-9. doi: 10.1093/rheumatology/kep418[↩]
- Bracaglia C, de Graaf K, Pires Marafon D, Guilhot F, Ferlin W, Prencipe G, Caiello I, Davì S, Schulert G, Ravelli A, Grom AA, de Min C, De Benedetti F. Elevated circulating levels of interferon-γ and interferon-γ-induced chemokines characterise patients with macrophage activation syndrome complicating systemic juvenile idiopathic arthritis. Ann Rheum Dis. 2017 Jan;76(1):166-172. doi: 10.1136/annrheumdis-2015-209020[↩][↩]
- Bleesing J, Prada A, Siegel DM, Villanueva J, Olson J, Ilowite NT, Brunner HI, Griffin T, Graham TB, Sherry DD, Passo MH, Ramanan AV, Filipovich A, Grom AA. The diagnostic significance of soluble CD163 and soluble interleukin-2 receptor alpha-chain in macrophage activation syndrome and untreated new-onset systemic juvenile idiopathic arthritis. Arthritis Rheum. 2007 Mar;56(3):965-71. doi: 10.1002/art.22416[↩]
- Minoia F, Bovis F, Davì S, et al. Pediatric Rheumatology International Trials Organization, the Childhood Arthritis and Rheumatology Research Alliance, the Pediatric Rheumatology Collaborative Study Group, and the Histiocyte Society. Development and Initial Validation of the Macrophage Activation Syndrome/Primary Hemophagocytic Lymphohistiocytosis Score, a Diagnostic Tool that Differentiates Primary Hemophagocytic Lymphohistiocytosis from Macrophage Activation Syndrome. J Pediatr. 2017 Oct;189:72-78.e3. doi: 10.1016/j.jpeds.2017.06.005[↩][↩]
- Ravelli A, Davì S, Minoia F, Martini A, Cron RQ. Macrophage Activation Syndrome. Hematol Oncol Clin North Am. 2015 Oct;29(5):927-41. doi: 10.1016/j.hoc.2015.06.010[↩]
- Efthimiou P, Kadavath S, Mehta B. Life-threatening complications of adult-onset Still’s disease. Clin Rheumatol. 2014 Mar;33(3):305-14. doi: 10.1007/s10067-014-2487-4[↩]
- Lenert A, Yao Q. Macrophage activation syndrome complicating adult onset Still’s disease: A single center case series and comparison with literature. Semin Arthritis Rheum. 2016 Jun;45(6):711-6. doi: 10.1016/j.semarthrit.2015.11.002[↩]
- Ravelli A, Minoia F, Davì S, et al. Paediatric Rheumatology International Trials Organisation; Childhood Arthritis and Rheumatology Research Alliance; Pediatric Rheumatology Collaborative Study Group; Histiocyte Society. 2016 Classification Criteria for Macrophage Activation Syndrome Complicating Systemic Juvenile Idiopathic Arthritis: A European League Against Rheumatism/American College of Rheumatology/Paediatric Rheumatology International Trials Organisation Collaborative Initiative. Ann Rheum Dis. 2016 Mar;75(3):481-9. doi: 10.1136/annrheumdis-2015-208982[↩]
- Ramos-Casals M, Brito-Zerón P, López-Guillermo A, Khamashta MA, Bosch X. Adult haemophagocytic syndrome. Lancet. 2014 Apr 26;383(9927):1503-1516. doi: 10.1016/S0140-6736(13)61048-X. Epub 2013 Nov 27. Erratum in: Lancet. 2014 Apr 26;383(9927):1464.[↩][↩][↩][↩][↩]
- Lehmberg K, Sprekels B, Nichols KE, Woessmann W, Müller I, Suttorp M, Bernig T, Beutel K, Bode SF, Kentouche K, et al. Malignancy-associated haemophagocytic lymphohistiocytosis in children and adolescents. Br J Haematol. 2015;170:539–549. doi: 10.1111/bjh.13462[↩][↩][↩][↩][↩]
- O’Brien MM, Lee-Kim Y, George TI, McClain KL, Twist CJ, Jeng M. Precursor B-cell acute lymphoblastic leukemia presenting with hemophagocytic lymphohistiocytosis. Pediatr Blood Cancer. 2008;50:381–383. doi: 10.1002/pbc.20950[↩]
- Celkan T, Berrak S, Kazanci E, Ozyürek E, Unal S, Uçar C, Yilmaz S, Gürgey A. Malignancy-associated hemophagocytic lymphohistiocytosis in pediatric cases: A multicenter study from Turkey. Turk J Pediatr. 2009;51:207–213.[↩][↩][↩]
- Strenger V, Merth G, Lackner H, Aberle SW, Kessler HH, Seidel MG, Schwinger W, Sperl D, Sovinz P, Karastaneva A, et al. Malignancy and chemotherapy induced haemophagocytic lymphohistiocytosis in children and adolescents-a single centre experience of 20 years. Ann Hematol. 2018;97:989–998. doi: 10.1007/s00277-018-3254-4[↩][↩]
- Chinn IK, Eckstein OS, Peckham-Gregory EC, Goldberg BR, Forbes LR, Nicholas SK, Mace EM, Vogel TP, Abhyankar HA, Diaz MI, et al. Genetic and mechanistic diversity in pediatric hemophagocytic lymphohistiocytosis. Blood. 2018;132:89–100. doi: 10.1182/blood-2017-11-814244[↩]
- Tabata C, Tabata R. Possible prediction of underlying lymphoma by high sIL-2R/ferritin ratio in hemophagocytic syndrome. Ann Hematol. 2012 Jan;91(1):63-71. doi: 10.1007/s00277-011-1239-7[↩]
- Hayden A, Lin M, Park S, Pudek M, Schneider M, Jordan MB, Mattman A, Chen LYC. Soluble interleukin-2 receptor is a sensitive diagnostic test in adult HLH. Blood Adv. 2017 Dec 6;1(26):2529-2534. doi: 10.1182/bloodadvances.2017012310[↩][↩]
- Daver N, McClain K, Allen CE, Parikh SA, Otrock Z, Rojas-Hernandez C, Blechacz B, Wang S, Minkov M, Jordan MB, et al. A consensus review on malignancy-associated hemophagocytic lymphohistiocytosis in adults. Cancer. 2017;123:3229–3240. doi: 10.1002/cncr.30826[↩][↩]
- Chellapandian D, Hines MR, Zhang R, Jeng M, van den Bos C, Santa-María López V, Lehmberg K, Sieni E, Wang Y, Nakano T, et al. A multicenter study of patients with multisystem Langerhans cell histiocytosis who develop secondary hemophagocytic lymphohistiocytosis. Cancer. 2019;125:963–971. doi: 10.1002/cncr.31893[↩][↩]
- Huang Z, Jia Y, Zuo Y, Wu J, Lu A, Zhang L. Malignancy-associated hemophagocytic lymphohistiocytosis in children: A 10-year experience of a single pediatric hematology center. Hematology. 2020;25:389–399. doi: 10.1080/16078454.2020.1833505[↩][↩][↩][↩][↩]
- Sakamoto K, Osumi T, Yoshimura S, Shimizu S, Kato M, Tomizawa D, Fukuda A, Sakamoto S, Nakano N, Yoshioka T, et al. Living-donor liver transplantation providing an adequate chemotherapy for a pediatric patient with anaplastic large cell lymphoma complicated with liver failure due to the aggravation of biliary hepatopathy by secondary hemophagocytic lymphohistiocytosis. Int J Hematol. 2020;112:900–905. doi: 10.1007/s12185-020-02949-z[↩]
- Teshigawara S, Katada Y, Maeda Y, Yoshimura M, Kudo-Tanaka E, Tsuji S, Harada Y, Matsushita M, Ohshima S, Watanabe K, et al. Hemophagocytic lymphohistiocytosis with leukoencephalopathy in a patient with dermatomyositis accompanied with peripheral T-cell lymphoma: A case report. J Med Case Rep. 2016;10(212) doi: 10.1186/s13256-016-0986-4[↩]
- Sinno MG, Rosen D, Wittler R. Concomitant presentation of hemophagocytic lymphohistiocytosis and posttransplant lymphoproliferative disease-like lymphoma in a mildly immunosuppressed leukemia patient: An unusual association. Pediatr Blood Cancer. 2016;63:1474–1476. doi: 10.1002/pbc.26033[↩]
- McCall CM, Mudali S, Arceci RJ, Small D, Fuller S, Gocke CD, Vuica-Ross M, Burns KH, Borowitz MJ, Duffield AS. Flow cytometric findings in hemophagocytic lymphohistiocytosis. Am J Clin Pathol. 2012;137:786–794. doi: 10.1309/AJCPP40MEXWYRLPN[↩]
- Gurunathan A, Boucher AA, Mark M, Prus KM, O’Brien MM, Breese EH, Mizukawa BE, Absalon MJ, Nelson AS, Jordan MB, Grimley MS, Lorsbach RB, Rotz SJ, Mathanda R, Kumar AR. Limitations of HLH-2004 criteria in distinguishing malignancy-associated hemophagocytic lymphohistiocytosis. Pediatr Blood Cancer. 2018 Dec;65(12):e27400. doi: 10.1002/pbc.27400[↩][↩][↩]
- Zheng F, Jia Y, Zhang L, Qin J. Hemophagocytic lymphohistiocytosis secondary to juvenile myelomonocytic leukemia: A case report and review of the literature. J Pediatr Hematol Oncol. 2022;44:e580–e584. doi: 10.1097/MPH.0000000000002273[↩]
- Farias MG, Freitas PAC, Spagnol F, Souza MV, Alegretti AP, Riegel M, Taniguchi ANR, Daudt LE. Hemophagocytosis by blasts in a child with acute monocytic leukemia after chemotherapy. Rev Paul Pediatr. 2021;39(e2019290) doi: 10.1590/1984-0462/2021/39/2019290[↩]
- Dokmanovic L, Krstovski N, Jankovic S, Janic D. Hemophagocytic lymphohistiocytosis arising in a child with Langerhans cell histiocytosis. Turk J Pediatr. 2014;56:452–457.[↩]
- Murphy EP, Mo J, Yoon JM. Secondary hemophagocytic lymphohistiocytosis in a patient with favorable histology wilms tumor. J Pediatr Hematol Oncol. 2015;37:e494–e496. doi: 10.1097/MPH.0000000000000433[↩]
- Nascimento FA, Nery J, Trennepohl J, Pianovski MAD. Hemophagocytic lymphohistiocytosis after initiation of chemotherapy for bilateral adrenal neuroblastoma. J Pediatr Hematol Oncol. 2016;38:e13–e15. doi: 10.1097/MPH.0000000000000469[↩]
- Tang X, Guo X, Gao J, Sun JJ, Wan Z. Hemophagocytic lymphohistiocytosis in langerhans cell histiocytosis: A case series and literature review. J Pediatr Hematol Oncol. 2022;44:e20–e25. doi: 10.1097/MPH.0000000000002212[↩]
- Devecioglu O, Anak S, Atay D, Aktan P, Devecioglu E, Ozalp B, Saribeyoglu E. Pediatric acute lymphoblastic leukemia complicated by secondary hemophagocytic lymphohistiocytosis. Pediatr Blood Cancer. 2009;53:491–492. doi: 10.1002/pbc.22064[↩]
- Fajgenbaum DC, June CH. Cytokine storm. N Engl J Med. 2020;383:2255–2273. doi: 10.1056/NEJMra2026131[↩][↩][↩][↩][↩][↩][↩]
- Sandler RD, Tattersall RS, Schoemans H, Greco R, Badoglio M, Labopin M, Alexander T, Kirgizov K, Rovira M, Saif M, et al. Diagnosis and management of secondary HLH/MAS following HSCT and CAR-T cell therapy in adults; A review of the literature and a survey of practice within EBMT centres on behalf of the autoimmune diseases working party (ADWP) and transplant complications working party (TCWP) Front Immunol. 2020;11(524) doi: 10.3389/fimmu.2020.00524[↩]
- Teachey DT, Lacey SF, Shaw PA, Melenhorst JJ, Maude SL, Frey N, Pequignot E, Gonzalez VE, Chen F, Finklestein J, et al. Identification of predictive biomarkers for cytokine release syndrome after chimeric antigen receptor T-cell therapy for acute lymphoblastic leukemia. Cancer Discov. 2016;6:664–679. doi: 10.1158/2159-8290.CD-16-0040[↩]
- Neelapu SS, Tummala S, Kebriaei P, Wierda W, Gutierrez C, Locke FL, Komanduri KV, Lin Y, Jain N, Daver N, et al. Chimeric antigen receptor T-cell therapy-assessment and management of toxicities. Nat Rev Clin Oncol. 2018;15:47–62. doi: 10.1038/nrclinonc.2017.148[↩]
- Lichtenstein DA, Schischlik F, Shao L, Steinberg SM, Yates B, Wang HW, Wang Y, Inglefield J, Dulau-Florea A, Ceppi F, et al. Characterization of HLH-like manifestations as a CRS variant in patients receiving CD22 CAR T cells. Blood. 2021;138:2469–2484. doi: 10.1182/blood.2021011898[↩][↩]
- Hines MR, Keenan C, Maron Alfaro G, Cheng C, Zhou Y, Sharma A, Hurley C, Nichols KE, Gottschalk S, Triplett BM, Talleur AC. Hemophagocytic lymphohistiocytosis-like toxicity (carHLH) after CD19-specific CAR T-cell therapy. Br J Haematol. 2021;194:701–707. doi: 10.1111/bjh.17662[↩][↩][↩]
- Maude SL, Laetsch TW, Buechner J, Rives S, Boyer M, Bittencourt H, Bader P, Verneris MR, Stefanski HE, Myers GD, et al. Tisagenlecleucel in children and young adults with B-cell lymphoblastic leukemia. N Engl J Med. 2018;378:439–448. doi: 10.1056/NEJMoa1709866[↩]
- Xu XJ, Tang YM. Cytokine release syndrome in cancer immunotherapy with chimeric antigen receptor engineered T cells. Cancer Lett. 2014;343:172–178. doi: 10.1016/j.canlet.2013.10.004[↩]
- Singh N, Hofmann TJ, Gershenson Z, Levine BL, Grupp SA, Teachey DT, Barrett DM. Monocyte lineage-derived IL-6 does not affect chimeric antigen receptor T-cell function. Cytotherapy. 2017;19:867–880. doi: 10.1016/j.jcyt.2017.04.001[↩][↩][↩][↩]
- Giavridis T, van der Stegen SJC, Eyquem J, Hamieh M, Piersigilli A, Sadelain M. CAR T cell-induced cytokine release syndrome is mediated by macrophages and abated by IL-1 blockade. Nat Med. 2018;24:731–738. doi: 10.1038/s41591-018-0041-7[↩]
- Norelli M, Camisa B, Barbiera G, Falcone L, Purevdorj A, Genua M, Sanvito F, Ponzoni M, Doglioni C, Cristofori P, et al. Monocyte-derived IL-1 and IL-6 are differentially required for cytokine-release syndrome and neurotoxicity due to CAR T cells. Nat Med. 2018;24:739–748. doi: 10.1038/s41591-018-0036-4[↩]
- Liu Y, Fang Y, Chen X, Wang Z, Liang X, Zhang T, Liu M, Zhou N, Lv J, Tang K, et al. Gasdermin E-mediated target cell pyroptosis by CAR T cells triggers cytokine release syndrome. Sci Immunol. 2020;5(eaax7969) doi: 10.1126/sciimmunol.aax7969[↩]
- Teachey DT, Rheingold SR, Maude SL, Zugmaier G, Barrett DM, Seif AE, Nichols KE, Suppa EK, Kalos M, Berg RA, et al. Cytokine release syndrome after blinatumomab treatment related to abnormal macrophage activation and ameliorated with cytokine-directed therapy. Blood. 2013;121:5154–5157. doi: 10.1182/blood-2013-02-485623[↩][↩]
- Winkler U, Jensen M, Manzke O, Schulz H, Diehl V, Engert A. Cytokine-release syndrome in patients with B-cell chronic lymphocytic leukemia and high lymphocyte counts after treatment with an anti-CD20 monoclonal antibody (rituximab, IDEC-C2B8). Blood. 1999 Oct 1;94(7):2217-24.[↩]
- Asano T, Kogawa K, Morimoto A, Ishida Y, Suzuki N, Ohga S, Kudo K, Ohta S, Wakiguchi H, Tabuchi K, et al. Hemophagocytic lymphohistiocytosis after hematopoietic stem cell transplantation in children: A nationwide survey in Japan. Pediatr Blood Cancer. 2012;59:110–114. doi: 10.1002/pbc.23384[↩][↩][↩][↩][↩][↩]
- Noguchi M, Inagaki J. Hemophagocytic lymphohistiocytosis and graft failure following unrelated umbilical cord blood transplantation in children. J Pediatr Hematol Oncol. 2020;42:e440–e444. doi: 10.1097/MPH.0000000000001795[↩][↩][↩]
- Jarchin L, Chu J, Januska M, Merola P, Arnon R. Autoimmune hemolytic anemia: An unusual presentation of hemophagocytic lymphohistiocytosis in a pediatric post-liver transplant patient. Pediatr Transplant. 2018;22(e13281) doi: 10.1111/petr.13281[↩]
- Nakajima K, Hiejima E, Nihira H, Kato K, Honda Y, Izawa K, Kawabata N, Kato I, Ogawa E, Sonoda M, et al. Case report: A case of Epstein-Barr virus-associated acute liver failure requiring hematopoietic cell transplantation after emergent liver transplantation. Front Immunol. 2022;13(825806) doi: 10.3389/fimmu.2022.825806[↩]
- Jha B, Mohan N, Gajendra S, Sachdev R, Goel S, Sahni T, Raina V, Soin A. Prompt diagnosis and management of Epstein-Barr virus-associated post-transplant lymphoproliferative disorder and hemophagocytosis: A dreaded complication in a post-liver transplant child. Pediatr Transplant. 2015;19:E177–E180. doi: 10.1111/petr.12558[↩]
- Matsuda K, Toyama K, Toya T, Ikemura M, Nakamura F, Kurokawa M. Reactivation of hemophagocytic lymphohistiocytosis triggered by antithymocyte globulin. Intern Med. 2018;57:583–586. doi: 10.2169/internalmedicine.9226-17[↩]
- Ali S, AlThubaiti S, Renzi S, Krueger J, Chiang KY, Naqvi A, Schechter T, Punnett A, Ali M. Hemophagocytic lymphohistiocytosis is a sign of poor outcome in pediatric Epstein-Barr virus-associated post-transplant lymphoproliferative disease after allogeneic hematopoietic stem cell transplantation. Pediatr Transplant. 2019;23(e13319) doi: 10.1111/petr.13319[↩]
- Park M, Yun YJ, Woo SI, Lee JW, Chung NG, Cho B. Rotavirus-associated hemophagocytic lymphohistiocytosis (HLH) after hematopoietic stem cell transplantation for familial HLH. Pediatr Int. 2015;57:e77–e80. doi: 10.1111/ped.12567[↩]
- Salvador C, Meister B, Larcher H, Crazzolara R, Kropshofer G. Hemophagocytic lymphohistiocytosis after allogeneic bone marrow transplantation during chronic norovirus infection. Hematol Oncol. 2014;32:102–106. doi: 10.1002/hon.2052[↩]
- Hattori N, Sato M, Uesugi Y, Nakata A, Sasaki Y, Shimada S, Watanuki M, Fujiwara S, Kawaguchi Y, Arai N, et al. Characteristics and predictors of post-transplant-associated hemophagocytic lymphohistiocytosis in adults. Int J Hematol. 2021;113:693–702. doi: 10.1007/s12185-020-03067-6[↩]
- Stefanou C, Tzortzi C, Georgiou F, Timiliotou C. Combining an antiviral with rituximab in EBV-related haemophagocytic lymphohistiocytosis led to rapid viral clearance; and a comprehensive review. BMJ Case Rep. 2016;2016(bcr2016216488) doi: 10.1136/bcr-2016-216488[↩][↩]
- Fitzgerald MP, Armstrong L, Hague R, Russell RK. A case of EBV driven haemophagocytic lymphohistiocytosis complicating a teenage Crohn’s disease patient on azathioprine, successfully treated with rituximab. J Crohns Colitis. 2013 May;7(4):314-7. doi: 10.1016/j.crohns.2012.05.002[↩]
- Bode SF, Ammann S, Al-Herz W, Bataneant M, Dvorak CC, Gehring S, Gennery A, Gilmour KC, Gonzalez-Granado LI, Groß-Wieltsch U, Ifversen M, Lingman-Framme J, Matthes-Martin S, Mesters R, Meyts I, van Montfrans JM, Pachlopnik Schmid J, Pai SY, Soler-Palacin P, Schuermann U, Schuster V, Seidel MG, Speckmann C, Stepensky P, Sykora KW, Tesi B, Vraetz T, Waruiru C, Bryceson YT, Moshous D, Lehmberg K, Jordan MB, Ehl S; Inborn Errors Working Party of the EBMT. The syndrome of hemophagocytic lymphohistiocytosis in primary immunodeficiencies: implications for differential diagnosis and pathogenesis. Haematologica. 2015 Jul;100(7):978-88. doi: 10.3324/haematol.2014.121608[↩][↩]
- Schultz KA, Neglia JP, Smith AR, Ochs HD, Torgerson TR, Kumar A. Familial hemophagocytic lymphohistiocytosis in two brothers with X-linked agammaglobulinemia. Pediatr Blood Cancer. 2008 Aug;51(2):293-5. doi: 10.1002/pbc.21573[↩]
- Alabbas F, Elyamany G, Alanzi T, Ali TB, Albatniji F, Alfaraidi H. Wolman’s disease presenting with secondary hemophagocytic lymphohistiocytosis: A case report from Saudi Arabia and literature review. BMC Pediatr. 2021;21(72) doi: 10.1186/s12887-021-02541-2[↩][↩]
- Schüller S, Attarbaschi A, Berger A, Hutter C, Klebermass-Schrehof K, Steiner M. Hemophagocytic lymphohistiocytosis triggered by Gaucher disease in a preterm neonate. Pediatr Hematol Oncol. 2016;33:462–467. doi: 10.1080/08880018.2016.1234011[↩][↩]
- Gokce M, Unal O, Hismi B, Gumruk F, Coskun T, Balta G, Unal S, Cetin M, Kalkanoglu-Sivri HS, Dursun A, Tokatlı A. Secondary hemophagocytosis in 3 patients with organic acidemia involving propionate metabolism. Pediatr Hematol Oncol. 2012;29:92–98. doi: 10.3109/08880018.2011.601402[↩]
- Erdol S, Ture M, Baytan B, Yakut T, Saglam H. An unusual case of LCHAD deficiency presenting with a clinical picture of hemophagocytic lymphohistiocytosis: Secondary HLH or coincidence? J Pediatr Hematol Oncol. 2016;38:661–662. doi: 10.1097/MPH.0000000000000626[↩]
- Düzenli Kar Y, Özdemir ZC, Kiral E, Kiliç Yildirim G, Dinleyici EÇ, Bör Ö. Hemophagocytic lymphohystiocytosis associated with type Ia glycogen storage disease. J Pediatr Hematol Oncol. 2019;41:e260–e262. doi: 10.1097/MPH.0000000000001208[↩]
- Santos Silva E, Klaudel-Dreszler M, Bakuła A, Oliva T, Sousa T, Fernandes PC, Tylki-Szymańska A, Kamenets E, Martins E, Socha P. Early onset lysosomal acid lipase deficiency presenting as secondary hemophagocytic lymphohistiocytosis: Two infants treated with sebelipase alfa. Clin Res Hepatol Gastroenterol. 2018;42:e77–e82. doi: 10.1016/j.clinre.2018.03.012[↩]
- Faraguna MC, Musto F, Crescitelli V, Iascone M, Spaccini L, Tonduti D, Fedeli T, Kullmann G, Canonico F, Cattoni A, et al. Mucopolysaccharidosis-plus syndrome, a rapidly progressive disease: Favorable impact of a very prolonged steroid treatment on the clinical course in a child. Genes (Basel) 2022;13(442) doi: 10.3390/genes13030442[↩]
- Farias-Moeller R, LaFrance-Corey R, Bartolini L, Wells EM, Baker M, Doslea A, Suslovic W, Greenberg J, Carpenter JL, Howe CL. Fueling the FIRES: Hemophagocytic lymphohistiocytosis in febrile infection-related epilepsy syndrome. Epilepsia. 2018;59:1753–1763. doi: 10.1111/epi.14524[↩][↩]
- Dandoy C, Grimley M. Secondary hemophagocytic lymphohistiocytosis (HLH) from a presumed brown recluse spider bite. J Clin Immunol. 2014;34:544–547. doi: 10.1007/s10875-014-0036-1[↩]
- Janka GE, Lehmberg K. Hemophagocytic lymphohistiocytosis: pathogenesis and treatment. Hematology Am Soc Hematol Educ Program. 2013;2013:605–611. doi: 10.1182/asheducation-2013.1.605[↩]
- Chandrakasan S, Filipovich AH. Hemophagocytic lymphohistiocytosis: advances in pathophysiology, diagnosis, and treatment. J Pediatr. 2013;163(5):1253–1259. doi: 10.1016/j.jpeds.2013.06.053[↩]
- Malinowska I, Machaczka M, Popko K, Siwicka A, Salamonowicz M, Nasilowska-Adamska B. Hemophagocytic syndrome in children and adults. Arch Immunol Ther Exp (Warsz) 2014;62(5):385–394. doi: 10.1007/s00005-014-0274-1[↩]
- Jordan MB, Allen CE, Weitzman S, Filipovich AH, McClain KL. How I treat hemophagocytic lymphohistiocytosis. Blood. 2011 Oct 13;118(15):4041-52. doi: 10.1182/blood-2011-03-278127[↩]
- Chellapandian D, Das R, Zelley K, Wiener SJ, Zhao H, Teachey DT, et al. Treatment of Epstein Barr virus-induced haemophagocytic lymphohistiocytosis with rituximab-containing chemo-immunotherapeutic regimens. Br J Haematol. 2013;162(3):376–382. doi: 10.1111/bjh.12386[↩]
- La Rosée P, Horne A, Hines M, von Bahr Greenwood T, Machowicz R, Berliner N, Birndt S, Gil-Herrera J, Girschikofsky M, Jordan MB, Kumar A, van Laar JAM, Lachmann G, Nichols KE, Ramanan AV, Wang Y, Wang Z, Janka G, Henter JI. Recommendations for the management of hemophagocytic lymphohistiocytosis in adults. Blood. 2019 Jun 6;133(23):2465-2477. https://doi.org/10.1182/blood.2018894618[↩][↩][↩]
- Sepulveda FE, de Saint Basile G. Hemophagocytic syndrome: primary forms and predisposing conditions. Curr Opin Immunol. 2017 Dec;49:20-26. doi: 10.1016/j.coi.2017.08.004[↩]
- Cetica V, Sieni E, Pende D, Danesino C, De Fusco C, Locatelli F, Micalizzi C, Putti MC, Biondi A, Fagioli F, Moretta L, Griffiths GM, Luzzatto L, Aricò M. Genetic predisposition to hemophagocytic lymphohistiocytosis: Report on 500 patients from the Italian registry. J Allergy Clin Immunol. 2016 Jan;137(1):188-196.e4. doi: 10.1016/j.jaci.2015.06.048[↩]
- Romberg N, Al Moussawi K, Nelson-Williams C, Stiegler AL, Loring E, Choi M, Overton J, Meffre E, Khokha MK, Huttner AJ, West B, Podoltsev NA, Boggon TJ, Kazmierczak BI, Lifton RP. Mutation of NLRC4 causes a syndrome of enterocolitis and autoinflammation. Nat Genet. 2014 Oct;46(10):1135-1139. doi: 10.1038/ng.3066[↩]
- Canna SW, Girard C, Malle L, de Jesus A, Romberg N, Kelsen J, Surrey LF, Russo P, Sleight A, Schiffrin E, Gabay C, Goldbach-Mansky R, Behrens EM. Life-threatening NLRC4-associated hyperinflammation successfully treated with IL-18 inhibition. J Allergy Clin Immunol. 2017 May;139(5):1698-1701. doi: 10.1016/j.jaci.2016.10.022[↩]
- Rouphael NG, Talati NJ, Vaughan C, Cunningham K, Moreira R, Gould C. Infections associated with haemophagocytic syndrome. Lancet Infect Dis. 2007 Dec;7(12):814-22. doi: 10.1016/S1473-3099(07)70290-6[↩][↩][↩]
- Lehmberg K, Nichols KE, Henter JI, Girschikofsky M, Greenwood T, Jordan M, Kumar A, Minkov M, La Rosée P, Weitzman S; Study Group on Hemophagocytic Lymphohistiocytosis Subtypes of the Histiocyte Society. Consensus recommendations for the diagnosis and management of hemophagocytic lymphohistiocytosis associated with malignancies. Haematologica. 2015 Aug;100(8):997-1004. doi: 10.3324/haematol.2015.123562[↩][↩][↩]
- Carter SJ, Tattersall RS, Ramanan AV. Macrophage activation syndrome in adults: recent advances in pathophysiology, diagnosis and treatment. Rheumatology (Oxford). 2019 Jan 1;58(1):5-17. doi: 10.1093/rheumatology/key006[↩]
- Hirayama D, Iida T, Nakase H. The Phagocytic Function of Macrophage-Enforcing Innate Immunity and Tissue Homeostasis. Int J Mol Sci. 2017 Dec 29;19(1):92. doi: 10.3390/ijms19010092[↩][↩]
- Pachlopnik Schmid J, Côte M, Ménager MM, Burgess A, Nehme N, Ménasché G, Fischer A, de Saint Basile G. Inherited defects in lymphocyte cytotoxic activity. Immunol Rev. 2010 May;235(1):10-23. doi: 10.1111/j.0105-2896.2010.00890.x. Erratum in: Immunol Rev. 2010 Jul;236(1):276. Schmid, Jana P (corrected to Pachlopnik Schmid, Jana].[↩]
- Gholam C, Grigoriadou S, Gilmour KC, Gaspar HB. Familial haemophagocytic lymphohistiocytosis: advances in the genetic basis, diagnosis and management. Clin Exp Immunol. 2011 Mar;163(3):271-83. doi: 10.1111/j.1365-2249.2010.04302.x[↩]
- Wegehaupt O, Wustrau K, Lehmberg K, Ehl S. Cell Versus Cytokine – Directed Therapies for Hemophagocytic Lymphohistiocytosis (HLH) in Inborn Errors of Immunity. Front Immunol. 2020 May 8;11:808. doi: 10.3389/fimmu.2020.00808[↩][↩]
- Griffin G, Shenoi S, Hughes GC. Hemophagocytic lymphohistiocytosis: An update on pathogenesis, diagnosis, and therapy. Best Pract Res Clin Rheumatol. 2020 Aug;34(4):101515. https://doi.org/10.1016/j.berh.2020.101515[↩][↩][↩][↩][↩][↩][↩][↩]
- Imashuku S. Treatment of Epstein-Barr virus-related hemophagocytic lymphohistiocytosis (EBV-HLH); update 2010. J Pediatr Hematol Oncol. 2011 Jan;33(1):35-9. doi: 10.1097/MPH.0b013e3181f84a52[↩]
- Athreya BH. Is macrophage activation syndrome a new entity? Clin Exp Rheumatol. 2002 Mar-Apr;20(2):121-3.[↩]
- Ramanan AV, Baildam EM. Macrophage activation syndrome is hemophagocytic lymphohistiocytosis–need for the right terminology. J Rheumatol. 2002 May;29(5):1105; author reply 1105.[↩]
- Emile JF, Abla O, Fraitag S, Horne A, Haroche J, Donadieu J, Requena-Caballero L, Jordan MB, Abdel-Wahab O, Allen CE, Charlotte F, Diamond EL, Egeler RM, Fischer A, Herrera JG, Henter JI, Janku F, Merad M, Picarsic J, Rodriguez-Galindo C, Rollins BJ, Tazi A, Vassallo R, Weiss LM; Histiocyte Society. Revised classification of histiocytoses and neoplasms of the macrophage-dendritic cell lineages. Blood. 2016 Jun 2;127(22):2672-81. doi: 10.1182/blood-2016-01-690636[↩][↩]
- Chesshyre E, Ramanan AV, Roderick MR. Hemophagocytic Lymphohistiocytosis and Infections: An Update. Pediatr Infect Dis J. 2019 Mar;38(3):e54-e56. doi: 10.1097/INF.0000000000002248[↩]
- Tan HY, Yong YK, Andrade BB, Shankar EM, Ponnampalavanar S, Omar SF, Narendran G, Kamarulzaman A, Swaminathan S, Sereti I, Crowe SM, French MA. Plasma interleukin-18 levels are a biomarker of innate immune responses that predict and characterize tuberculosis-associated immune reconstitution inflammatory syndrome. AIDS. 2015 Feb 20;29(4):421-31. doi: 10.1097/QAD.0000000000000557[↩]
- Lehmberg K, Sprekels B, Nichols KE, Woessmann W, Müller I, Suttorp M, Bernig T, Beutel K, Bode SF, Kentouche K, Kolb R, Längler A, Minkov M, Schilling FH, Schmid I, Vieth S, Ehl S, Zur Stadt U, Janka GE. Malignancy-associated haemophagocytic lymphohistiocytosis in children and adolescents. Br J Haematol. 2015 Aug;170(4):539-49. doi: 10.1111/bjh.13462[↩][↩]
- Rivière S, Galicier L, Coppo P, Marzac C, Aumont C, Lambotte O, Fardet L. Reactive hemophagocytic syndrome in adults: a retrospective analysis of 162 patients. Am J Med. 2014 Nov;127(11):1118-1125. doi: 10.1016/j.amjmed.2014.04.034[↩]
- Parikh SA, Kapoor P, Letendre L, Kumar S, Wolanskyj AP. Prognostic factors and outcomes of adults with hemophagocytic lymphohistiocytosis. Mayo Clin Proc. 2014 Apr;89(4):484-92. doi: 10.1016/j.mayocp.2013.12.012[↩]
- Namuduri M, Brentjens RJ. Medical management of side effects related to CAR T cell therapy in hematologic malignancies. Expert Rev Hematol. 2016 Jun;9(6):511-3. doi: 10.1080/17474086.2016.1183479[↩]
- Teachey DT, Rheingold SR, Maude SL, Zugmaier G, Barrett DM, Seif AE, Nichols KE, Suppa EK, Kalos M, Berg RA, Fitzgerald JC, Aplenc R, Gore L, Grupp SA. Cytokine release syndrome after blinatumomab treatment related to abnormal macrophage activation and ameliorated with cytokine-directed therapy. Blood. 2013 Jun 27;121(26):5154-7. doi: 10.1182/blood-2013-02-485623[↩]
- Al-Samkari H, Berliner N. Hemophagocytic Lymphohistiocytosis. Annu Rev Pathol. 2018 Jan 24;13:27-49. doi: 10.1146/annurev-pathol-020117-043625[↩]
- Crayne CB, Albeituni S, Nichols KE, Cron RQ. The Immunology of Macrophage Activation Syndrome. Front Immunol. 2019 Feb 1;10:119. doi: 10.3389/fimmu.2019.00119[↩][↩][↩]
- Al-Samkari H, Berliner N. Hemophagocytic lymphohistiocytosis. Annu Rev Pathol. 2018;13:27–49. doi: 10.1146/annurev-pathol-020117-043625[↩]
- Ishii E. Hemophagocytic lymphohistiocytosis in children: Pathogenesis and treatment. Front Pediatr. 2016;4(47) doi: 10.3389/fped.2016.00047[↩]
- Skinner J, Yankey B, Shelton BK. Hemophagocytic lymphohistiocytosis. AACN Adv Crit Care. 2019;30:151–164. doi: 10.4037/aacnacc2019463[↩]
- Morimoto A, Nakazawa Y, Ishii E. Hemophagocytic lymphohistiocytosis: Pathogenesis, diagnosis, and management. Pediatr Int. 2016;58:817–825. doi: 10.1111/ped.13064[↩][↩]
- Jordan MB, Hildeman D, Kappler J, Marrack P. An animal model of hemophagocytic lymphohistiocytosis (HLH): CD8+ T cells and interferon gamma are essential for the disorder. Blood. 2004;104:735–743. doi: 10.1182/blood-2003-10-3413[↩]
- Castillo L, Carcillo J. Secondary hemophagocytic lymphohistiocytosis and severe sepsis/systemic inflammatory response syndrome/multiorgan dysfunction syndrome/macrophage activation syndrome share common intermediate phenotypes on a spectrum of inflammation. Pediatr Crit Care Med. 2009;10:387–392. doi: 10.1097/PCC.0b013e3181a1ae08[↩][↩][↩]
- Jordan MB, Hildeman D, Kappler J, Marrack P. An animal model of hemophagocytic lymphohistiocytosis (HLH): CD8+ T cells and interferon gamma are essential for the disorder. Blood. 2004 Aug 1;104(3):735-43. doi: 10.1182/blood-2003-10-3413[↩]
- Grom AA, Horne A, De Benedetti F. Macrophage activation syndrome in the era of biologic therapy. Nat Rev Rheumatol. 2016;12:259–268. doi: 10.1038/nrrheum.2015.179[↩]
- Canna SW, Behrens EM. Making sense of the cytokine storm: A conceptual framework for understanding, diagnosing, and treating hemophagocytic syndromes. Pediatr Clin North Am. 2012;59:329–344. doi: 10.1016/j.pcl.2012.03.002[↩]
- Jordan MB. Emergence of targeted therapy for hemophagocytic lymphohistiocytosis. Hematologist. 2018;15[↩]
- Alonso EM, Horslen SP, Behrens EM, Doo E. Pediatric acute liver failure of undetermined cause: A research workshop. Hepatology. 2017;65:1026–1037. doi: 10.1002/hep.28944[↩]
- Hemophagocytic Lymphohistiocytosis. https://rarediseases.org/rare-diseases/hemophagocytic-lymphohistiocytosis[↩][↩]
- Shah AJ, Kapoor N, Cooper RM, Crooks GM, Lenarsky C, Abdel-Azim H, Wu SQ, Wilson K, Weinberg KI, Parkman R, Kohn DB. Pre- and post-natal treatment of hemophagocytic lymphohistiocytosis. Pediatr Blood Cancer. 2009 Jan;52(1):139-42. doi: 10.1002/pbc.21778[↩]
- Heeg M, Ammann S, Klemann C, Panning M, Falcone V, Hengel H, Lehmberg K, Zur Stadt U, Wustrau K, Janka G, Ehl S. Is an infectious trigger always required for primary hemophagocytic lymphohistiocytosis? Lessons from in utero and neonatal disease. Pediatr Blood Cancer. 2018 Nov;65(11):e27344. doi: 10.1002/pbc.27344[↩]
- Marsh RA, Vaughn G, Kim MO, Li D, Jodele S, Joshi S, Mehta PA, Davies SM, Jordan MB, Bleesing JJ, Filipovich AH. Reduced-intensity conditioning significantly improves survival of patients with hemophagocytic lymphohistiocytosis undergoing allogeneic hematopoietic cell transplantation. Blood. 2010 Dec 23;116(26):5824-31. doi: 10.1182/blood-2010-04-282392[↩]
- Xu XJ, Wang HS, Ju XL, Xiao PF, Xiao Y, Xue HM, Shi HY, Gao YJ, Jia GC, Li XR, Zhao WH, Wang NL, Tang YM; Histiocytosis Study Group of the Chinese Pediatric Society. Clinical presentation and outcome of pediatric patients with hemophagocytic lymphohistiocytosis in China: A retrospective multicenter study. Pediatr Blood Cancer. 2017 Apr;64(4). doi: 10.1002/pbc.26264[↩]
- Balamuth NJ, Nichols KE, Paessler M, Teachey DT. Use of rituximab in conjunction with immunosuppressive chemotherapy as a novel therapy for Epstein Barr virus-associated hemophagocytic lymphohistiocytosis. J Pediatr Hematol Oncol. 2007 Aug;29(8):569-73. doi: 10.1097/MPH.0b013e3180f61be3[↩]
- Imashuku S. Clinical features and treatment strategies of Epstein-Barr virus-associated hemophagocytic lymphohistiocytosis. Crit Rev Oncol Hematol. 2002 Dec;44(3):259-72. doi: 10.1016/s1040-8428(02)00117-8[↩]
- Shiraishi A, Ohga S, Doi T, Ishimura M, Takimoto T, Takada H, Miyamoto T, Abe Y, Hara T. Treatment choice of immunotherapy or further chemotherapy for Epstein-Barr virus-associated hemophagocytic lymphohistiocytosis. Pediatr Blood Cancer. 2012 Aug;59(2):265-70. doi: 10.1002/pbc.24039[↩]
- Arca M, Fardet L, Galicier L, Rivière S, Marzac C, Aumont C, Lambotte O, Coppo P. Prognostic factors of early death in a cohort of 162 adult haemophagocytic syndrome: impact of triggering disease and early treatment with etoposide. Br J Haematol. 2015 Jan;168(1):63-8. doi: 10.1111/bjh.13102[↩]
- Imashuku S, Kuriyama K, Teramura T, Ishii E, Kinugawa N, Kato M, Sako M, Hibi S. Requirement for etoposide in the treatment of Epstein-Barr virus-associated hemophagocytic lymphohistiocytosis. J Clin Oncol. 2001 May 15;19(10):2665-73. doi: 10.1200/JCO.2001.19.10.2665[↩]
- Leow EH, Soh SY, Tan AM, Mok YH, Chan MY, Lee JH. Critically Ill Children With Hemophagocytic Lymphohistiocytosis: A Case Series of 14 Patients. J Pediatr Hematol Oncol. 2017 Aug;39(6):e303-e306. doi: 10.1097/MPH.0000000000000916[↩][↩]
- Rajagopala S, Singh N, Agarwal R, Gupta D, Das R. Severe hemophagocytic lymphohistiocytosis in adults-experience from an intensive care unit from North India. Indian J Crit Care Med. 2012 Oct;16(4):198-203. doi: 10.4103/0972-5229.106501[↩]
- Buyse S, Teixeira L, Galicier L, Mariotte E, Lemiale V, Seguin A, Bertheau P, Canet E, de Labarthe A, Darmon M, Rybojad M, Schlemmer B, Azoulay E. Critical care management of patients with hemophagocytic lymphohistiocytosis. Intensive Care Med. 2010 Oct;36(10):1695-1702. doi: 10.1007/s00134-010-1936-z[↩][↩]
- Henter JI, Horne A, Aricó M, Egeler RM, Filipovich AH, Imashuku S, Ladisch S, McClain K, Webb D, Winiarski J, Janka G. HLH-2004: Diagnostic and therapeutic guidelines for hemophagocytic lymphohistiocytosis. Pediatr Blood Cancer. 2007 Feb;48(2):124-31. doi: 10.1002/pbc.21039[↩][↩][↩]
- Janka GE. Familial and acquired hemophagocytic lymphohistiocytosis. Eur J Pediatr. 2007 Feb;166(2):95-109. doi: 10.1007/s00431-006-0258-1[↩]
- Strauss R, Neureiter D, Westenburger B, Wehler M, Kirchner T, Hahn EG. Multifactorial risk analysis of bone marrow histiocytic hyperplasia with hemophagocytosis in critically ill medical patients–a postmortem clinicopathologic analysis. Crit Care Med. 2004 Jun;32(6):1316-21. doi: 10.1097/01.ccm.0000127779.24232.15[↩]
- Stéphan F, Thiolière B, Verdy E, Tulliez M. Role of hemophagocytic histiocytosis in the etiology of thrombocytopenia in patients with sepsis syndrome or septic shock. Clin Infect Dis. 1997 Nov;25(5):1159-64. doi: 10.1086/516086[↩]
- Shakoory B, Carcillo JA, Chatham WW, Amdur RL, Zhao H, Dinarello CA, Cron RQ, Opal SM. Interleukin-1 Receptor Blockade Is Associated With Reduced Mortality in Sepsis Patients With Features of Macrophage Activation Syndrome: Reanalysis of a Prior Phase III Trial. Crit Care Med. 2016 Feb;44(2):275-81. doi: 10.1097/CCM.0000000000001402[↩]
- Kyriazopoulou E, Leventogiannis K, Norrby-Teglund A, Dimopoulos G, Pantazi A, Orfanos SE, Rovina N, Tsangaris I, Gkavogianni T, Botsa E, Chassiou E, Kotanidou A, Kontouli C, Chaloulis P, Velissaris D, Savva A, Cullberg JS, Akinosoglou K, Gogos C, Armaganidis A, Giamarellos-Bourboulis EJ; Hellenic Sepsis Study Group. Macrophage activation-like syndrome: an immunological entity associated with rapid progression to death in sepsis. BMC Med. 2017 Sep 18;15(1):172. doi: 10.1186/s12916-017-0930-5[↩]
- Carcillo JA, Podd B, Simon DW. From febrile pancytopenia to hemophagocytic lymphohistiocytosis-associated organ dysfunction. Intensive Care Med. 2017 Dec;43(12):1853-1855. doi: 10.1007/s00134-017-4853-6[↩]
- Carcillo JA, Sward K, Halstead ES, Telford R, Jimenez-Bacardi A, Shakoory B, Simon D, Hall M; Eunice Kennedy Shriver National Institute of Child Health and Human Development Collaborative Pediatric Critical Care Research Network Investigators. A Systemic Inflammation Mortality Risk Assessment Contingency Table for Severe Sepsis. Pediatr Crit Care Med. 2017 Feb;18(2):143-150. doi: 10.1097/PCC.0000000000001029[↩]
- Trottestam H, Horne A, Aricò M, Egeler RM, Filipovich AH, Gadner H, Imashuku S, Ladisch S, Webb D, Janka G, Henter JI; Histiocyte Society. Chemoimmunotherapy for hemophagocytic lymphohistiocytosis: long-term results of the HLH-94 treatment protocol. Blood. 2011 Oct 27;118(17):4577-84. doi: 10.1182/blood-2011-06-356261[↩][↩][↩]
- Horne A, Wickström R, Jordan MB, Yeh EA, Naqvi A, Henter JI, Janka G. How to Treat Involvement of the Central Nervous System in Hemophagocytic Lymphohistiocytosis? Curr Treat Options Neurol. 2017 Jan;19(1):3. doi: 10.1007/s11940-017-0439-4[↩][↩]
- Benson LA, Li H, Henderson LA, Solomon IH, Soldatos A, Murphy J, Bielekova B, Kennedy AL, Rivkin MJ, Davies KJ, Hsu AP, Holland SM, Gahl WA, Sundel RP, Lehmann LE, Lee MA, Alexandrescu S, Degar BA, Duncan CN, Gorman MP. Pediatric CNS-isolated hemophagocytic lymphohistiocytosis. Neurol Neuroimmunol Neuroinflamm. 2019 Apr 8;6(3):e560. doi: 10.1212/NXI.0000000000000560[↩]
- Haddad E, Sulis ML, Jabado N, Blanche S, Fischer A, Tardieu M. Frequency and severity of central nervous system lesions in hemophagocytic lymphohistiocytosis. Blood. 1997 Feb 1;89(3):794-800.[↩]
- Lounder DT, Khandelwal P, Chandra S, Jordan MB, Kumar AR, Grimley MS, Davies SM, Bleesing JJ, Marsh RA. Incidence and Outcomes of Central Nervous System Hemophagocytic Lymphohistiocytosis Relapse after Reduced-Intensity Conditioning Hematopoietic Stem Cell Transplantation. Biol Blood Marrow Transplant. 2017 May;23(5):857-860. doi: 10.1016/j.bbmt.2017.02.011[↩]
- Rego I, Severino M, Micalizzi C, Faraci M, Pende D, Dufour C, Aricò M, Rossi A. Neuroradiologic findings and follow-up with magnetic resonance imaging of the genetic forms of haemophagocytic lymphohistiocytosis with CNS involvement. Pediatr Blood Cancer. 2012 May;58(5):810-4. doi: 10.1002/pbc.23405[↩]
- Rabah F, Al-Hashmi N, Beshlawi I. Wolman’s disease with secondary hemophagocytic lymphohistiocytosis. Pediatr Hematol Oncol. 2014 Sep;31(6):576-8. doi: 10.3109/08880018.2014.920942[↩]
- Karaman S, Urgancı N, Kutluk G, Çetinkaya F. Niemann – Pick disease associated with hemophagocytic syndrome. Turk J Haematol. 2010 Dec 5;27(4):303-7. English. doi: 10.5152/tjh.2010.54[↩]
- Düzenli Kar Y, Özdemir ZC, Kiral E, Kiliç Yildirim G, Dinleyici EÇ, Bör Ö. Hemophagocytic Lymphohystiocytosis Associated With Type Ia Glycogen Storage Disease. J Pediatr Hematol Oncol. 2019 May;41(4):e260-e262. doi: 10.1097/MPH.0000000000001208[↩]
- Gholamreza B, Ghasem MA. Hemophagocytic lymphohistiocytosis syndrome associated with Gaucher disease type 2. Turk J Haematol. 2014 Sep 5;31(3):307-8. doi: 10.4274/tjh.2014.0037[↩]
- Sotiropoulos C, Theodorou G, Repa C, Marinakis T, Verigou E, Solomou E, Karakantza M, Symeonidis A. Severe impairment of regulatory T-cells and Th1-lymphocyte polarization in patients with Gaucher disease. JIMD Rep. 2015;18:107-15. doi: 10.1007/8904_2014_357[↩]
- Aflaki E, Borger DK, Grey RJ, Kirby M, Anderson S, Lopez G, Sidransky E. Efferocytosis is impaired in Gaucher macrophages. Haematologica. 2017 Apr;102(4):656-665. doi: 10.3324/haematol.2016.155093[↩]
- Duval M, Fenneteau O, Doireau V, Faye A, Emilie D, Yotnda P, Drapier JC, Schlegel N, Sterkers G, de Baulny HO, Vilmer E. Intermittent hemophagocytic lymphohistiocytosis is a regular feature of lysinuric protein intolerance. J Pediatr. 1999 Feb;134(2):236-9. doi: 10.1016/s0022-3476(99)70423-3[↩]
- Gokce M, Unal O, Hismi B, Gumruk F, Coskun T, Balta G, Unal S, Cetin M, Kalkanoglu-Sivri HS, Dursun A, Tokatlı A. Secondary hemophagocytosis in 3 patients with organic acidemia involving propionate metabolism. Pediatr Hematol Oncol. 2012 Feb;29(1):92-8. doi: 10.3109/08880018.2011.601402[↩]
- Bader-Meunier B, Parez N, Muller S. Treatment of hemophagocytic lymphohistiocytosis with cyclosporin A and steroids in a boy with lysinuric protein intolerance. J Pediatr. 2000 Jan;136(1):134. doi: 10.1016/s0022-3476(00)90072-6[↩]
- Feldman AG, Whitington PF. Neonatal hemochromatosis. J Clin Exp Hepatol. 2013 Dec;3(4):313-20. doi: 10.1016/j.jceh.2013.10.004[↩]
- Neilson DE. The interplay of infection and genetics in acute necrotizing encephalopathy. Curr Opin Pediatr. 2010 Dec;22(6):751-7. doi: 10.1097/MOP.0b013e3283402bfe[↩]
- Farias-Moeller R, LaFrance-Corey R, Bartolini L, Wells EM, Baker M, Doslea A, Suslovic W, Greenberg J, Carpenter JL, Howe CL. Fueling the FIRES: Hemophagocytic lymphohistiocytosis in febrile infection-related epilepsy syndrome. Epilepsia. 2018 Sep;59(9):1753-1763. doi: 10.1111/epi.14524[↩]
- Ehl S, Astigarraga I, von Bahr Greenwood T, Hines M, Horne A, Ishii E, Janka G, Jordan MB, La Rosée P, Lehmberg K, Machowicz R, Nichols KE, Sieni E, Wang Z, Henter JI. Recommendations for the Use of Etoposide-Based Therapy and Bone Marrow Transplantation for the Treatment of HLH: Consensus Statements by the HLH Steering Committee of the Histiocyte Society. J Allergy Clin Immunol Pract. 2018 Sep-Oct;6(5):1508-1517. doi: 10.1016/j.jaip.2018.05.031[↩][↩]
- Henter, J.-I., Horne, A., Aricó, M., Egeler, R.M., Filipovich, A.H., Imashuku, S., Ladisch, S., McClain, K., Webb, D., Winiarski, J. and Janka, G. (2007), HLH-2004: Diagnostic and therapeutic guidelines for hemophagocytic lymphohistiocytosis. Pediatr. Blood Cancer, 48: 124-131. https://doi.org/10.1002/pbc.21039[↩]
- Rubin TS, Zhang K, Gifford C, Lane A, Choo S, Bleesing JJ, Marsh RA. Perforin and CD107a testing is superior to NK cell function testing for screening patients for genetic HLH. Blood. 2017 Jun 1;129(22):2993-2999. doi: 10.1182/blood-2016-12-753830[↩]
- Lin M, Park S, Hayden A, Giustini D, Trinkaus M, Pudek M, Mattman A, Schneider M, Chen LYC. Clinical utility of soluble interleukin-2 receptor in hemophagocytic syndromes: a systematic scoping review. Ann Hematol. 2017 Aug;96(8):1241-1251. doi: 10.1007/s00277-017-2993-y[↩]
- Meeths M, Horne A, Sabel M, Bryceson YT, Henter JI. Incidence and clinical presentation of primary hemophagocytic lymphohistiocytosis in Sweden. Pediatr Blood Cancer. 2015 Feb;62(2):346-352. doi: 10.1002/pbc.25308[↩]
- Buatois V, Chatel L, Cons L, Lory S, Richard F, Guilhot F, Johnson Z, Bracaglia C, De Benedetti F, de Min C, Kosco-Vilbois MH, Ferlin WG. Use of a mouse model to identify a blood biomarker for IFNγ activity in pediatric secondary hemophagocytic lymphohistiocytosis. Transl Res. 2017 Feb;180:37-52.e2. doi: 10.1016/j.trsl.2016.07.023[↩]
- Prencipe G, Caiello I, Pascarella A, Grom AA, Bracaglia C, Chatel L, Ferlin WG, Marasco E, Strippoli R, de Min C, De Benedetti F. Neutralization of IFN-γ reverts clinical and laboratory features in a mouse model of macrophage activation syndrome. J Allergy Clin Immunol. 2018 Apr;141(4):1439-1449. doi: 10.1016/j.jaci.2017.07.021[↩]
- Mellor-Heineke S, Villanueva J, Jordan MB, Marsh R, Zhang K, Bleesing JJ, Filipovich AH, Risma KA. Elevated Granzyme B in Cytotoxic Lymphocytes is a Signature of Immune Activation in Hemophagocytic Lymphohistiocytosis. Front Immunol. 2013 Mar 22;4:72. doi: 10.3389/fimmu.2013.00072[↩]
- Allen CE, Yu X, Kozinetz CA, McClain KL. Highly elevated ferritin levels and the diagnosis of hemophagocytic lymphohistiocytosis. Pediatr Blood Cancer. 2008 Jun;50(6):1227-35. doi: 10.1002/pbc.21423[↩]
- Tsuji T, Hirano T, Yamasaki H, Tsuji M, Tsuda H. A high sIL-2R/ferritin ratio is a useful marker for the diagnosis of lymphoma-associated hemophagocytic syndrome. Ann Hematol. 2014 May;93(5):821-6. doi: 10.1007/s00277-013-1925-8[↩]
- Bode SF, Ammann S, Al-Herz W, et al. Inborn Errors Working Party of the EBMT. The syndrome of hemophagocytic lymphohistiocytosis in primary immunodeficiencies: implications for differential diagnosis and pathogenesis. Haematologica. 2015 Jul;100(7):978-88. doi: 10.3324/haematol.2014.121608[↩]
- Fardet L, Galicier L, Lambotte O, Marzac C, Aumont C, Chahwan D, Coppo P, Hejblum G. Development and validation of the HScore, a score for the diagnosis of reactive hemophagocytic syndrome. Arthritis Rheumatol. 2014 Sep;66(9):2613-20. doi: 10.1002/art.38690[↩]
- Xu XJ, Tang YM, Song H, Yang SL, Xu WQ, Zhao N, Shi SW, Shen HP, Mao JQ, Zhang LY, Pan BH. Diagnostic accuracy of a specific cytokine pattern in hemophagocytic lymphohistiocytosis in children. J Pediatr. 2012 Jun;160(6):984-90.e1. doi: 10.1016/j.jpeds.2011.11.046[↩]
- Han XC, Ye Q, Zhang WY, Tang YM, Xu XJ, Zhang T. Cytokine profiles as novel diagnostic markers of Epstein-Barr virus-associated hemophagocytic lymphohistiocytosis in children. J Crit Care. 2017 Jun;39:72-77. doi: 10.1016/j.jcrc.2017.02.018[↩]
- Zondag TC, Rokx C, van Lom K, van den Berg AR, Sonneveld P, Dik WA, van Doornum GJ, Lam KH, van Laar JA. Cytokine and viral load kinetics in human herpesvirus 8-associated multicentric Castleman’s disease complicated by hemophagocytic lymphohistiocytosis. Int J Hematol. 2016 Apr;103(4):469-72. doi: 10.1007/s12185-015-1928-4[↩]
- Merli P, Quintarelli C, Strocchio L, Locatelli F. The role of interferon-gamma and its signaling pathway in pediatric hematological disorders. Pediatr Blood Cancer. 2021;68(e28900) doi: 10.1002/pbc.28900[↩][↩]
- Henter JI, Aricò M, Egeler RM, Elinder G, Favara BE, Filipovich AH, Gadner H, Imashuku S, Janka-Schaub G, Komp D, et al. HLH-94: A treatment protocol for hemophagocytic lymphohistiocytosis. HLH study group of the histiocyte society. Med Pediatr Oncol. 1997;28:342–347. doi: 10.1002/(sici)1096-911x(199705)28:5<342::aid-mpo3>3.0.co;2-h[↩]
- Johnson TS, Terrell CE, Millen SH, Katz JD, Hildeman DA, Jordan MB. Etoposide selectively ablates activated T cells to control the immunoregulatory disorder hemophagocytic lymphohistiocytosis. J Immunol. 2014;192:84–91. doi: 10.4049/jimmunol.1302282[↩]
- Jordan M, Prof FL, Allen C, De Benedetti F, Grom AA, Ballabio M, Ferlin WG, De Min C. A novel targeted approach to the treatment of hemophagocytic lymphohistiocytosis (HLH) with an anti-interferon gamma (IFNγ) monoclonal antibody (mAb), NI-0501: First results from a pilot phase 2 study in children with primary HLH. Blood. 2015;126:LBA–3.[↩]
- Locatelli F, Jordan MB, Allen C, Cesaro S, Rizzari C, Rao A, Degar B, Garrington TP, Sevilla J, Putti MC, et al. Emapalumab in children with primary hemophagocytic lymphohistiocytosis. N Engl J Med. 2020;382:1811–1822. doi: 10.1056/NEJMoa1911326[↩][↩]
- FDA approves emapalumab for hemophagocytic lymphohistiocytosis. https://www.fda.gov/drugs/fda-approves-emapalumab-hemophagocytic-lymphohistiocytosis[↩]
- Mahlaoui N, Ouachée-Chardin M, de Saint Basile G, Neven B, Picard C, Blanche S, Fischer A. Immunotherapy of familial hemophagocytic lymphohistiocytosis with antithymocyte globulins: A single-center retrospective report of 38 patients. Pediatrics. 2007;120:e622–e628. doi: 10.1542/peds.2006-3164[↩][↩]
- Latour S, Fischer A. Signaling pathways involved in the T-cell-mediated immunity against Epstein-Barr virus: Lessons from genetic diseases. Immunol Rev. 2019;291:174–189. doi: 10.1111/imr.12791[↩]
- Kasahara Y, Yachie A. Cell type specific infection of Epstein-Barr virus (EBV) in EBV-associated hemophagocytic lymphohistiocytosis and chronic active EBV infection. Crit Rev Oncol Hematol. 2002;44:283–294. doi: 10.1016/s1040-8428(02)00119-1[↩]
- Moss DJ, Burrows SR, Khanna R, Misko IS, Sculley TB. Immune surveillance against Epstein-Barr virus. Semin Immunol. 1992 Apr;4(2):97-104.[↩]
- Henter JI, Samuelsson-Horne A, Aricò M, Egeler RM, Elinder G, Filipovich AH, et al. Treatment of hemophagocytic lymphohistiocytosis with HLH-94 immunochemotherapy and bone marrow transplantation. Blood. (2002) 100:2367–73. 10.1182/blood-2002-01-0172[↩]
- Johnson TS, Terrell CE, Millen SH, Katz JD, Hildeman DA, Jordan MB. Etoposide selectively ablates activated T cells to control the immunoregulatory disorder hemophagocytic lymphohistiocytosis. J Immunol. (2014) 192:84–91. 10.4049/jimmunol.1302282[↩]
- Horne A, Wickström R, Jordan MB, Ann Yeh E, Naqvi A, Henter JI, et al. How to treat involvement of the central nervous system in hemophagocytic lymphohistiocytosis? Curr Treat Options Neurol. (2017) 19:3 10.1007/s11940-017-0439-4[↩]
- Ehl S, Astigarraga I, von Bahr Greenwood T, Hines M, Horne A, Ishii E, et al. Recommendations for the use of etoposide-based therapy and bone marrow transplantation for the treatment of HLH: consensus statements by the HLH steering committee of the histiocyte society. J Allergy Clin Immunol Pract. (2018) 6:1508–17. 10.1016/j.jaip.2018.05.031[↩]
- Bergsten E, Horne A, Aricó M, Astigarraga I, Egeler RM, Filipovich AH, et al. Confirmed efficacy of etoposide and dexamethasone in HLH treatment: long-term results of the cooperative HLH-2004 study. Blood. (2017) 130:2728–38. 10.1182/blood-2017-06-788349[↩]
- Henter JI, Samuelsson-Horne A, Aricò M, Egeler RM, Elinder G, Filipovich AH, Gadner H, Imashuku S, Komp D, Ladisch S, et al. Treatment of hemophagocytic lymphohistiocytosis with HLH-94 immunochemotherapy and bone marrow transplantation. Blood. 2002;100:2367–2373. doi: 10.1182/blood-2002-01-0172[↩][↩][↩][↩][↩]
- Henter JI, Samuelsson-Horne A, Aricò M, Egeler RM, Elinder G, Filipovich AH, Gadner H, Imashuku S, Komp D, Ladisch S, Webb D, Janka G; Histocyte Society. Treatment of hemophagocytic lymphohistiocytosis with HLH-94 immunochemotherapy and bone marrow transplantation. Blood. 2002 Oct 1;100(7):2367-73. doi: 10.1182/blood-2002-01-0172[↩]
- Jordan MB, Filipovich AH. Hematopoietic cell transplantation for hemophagocytic lymphohistiocytosis: a journey of a thousand miles begins with a single (big) step. Bone Marrow Transplant. 2008 Oct;42(7):433-7. doi: 10.1038/bmt.2008.232[↩]
- Marsh RA, Allen CE, McClain KL, Weinstein JL, Kanter J, Skiles J, Lee ND, Khan SP, Lawrence J, Mo JQ, Bleesing JJ, Filipovich AH, Jordan MB. Salvage therapy of refractory hemophagocytic lymphohistiocytosis with alemtuzumab. Pediatr Blood Cancer. 2013 Jan;60(1):101-9. doi: 10.1002/pbc.24188[↩]
- Rajagopala S, Dutta U, Chandra KSP, Bhatia P, Varma N, Kochhar R. Visceral leishmaniasis associated hemophagocytic lymphohistiocytosis-case report and systematic review. J Infect. 2008;56:381–388. doi: 10.1016/j.jinf.2008.02.013[↩][↩]
- Cançado GGL, Freitas GG, Faria FHF, de Macedo AV, Nobre V. Hemophagocytic lymphohistiocytosis associated with visceral leishmaniasis in late adulthood. Am J Trop Med Hyg. 2013;88:575–577. doi: 10.4269/ajtmh.12-0563[↩]
- Ay Y, Yildiz B, Unver H, Karapinar DY, Vardar F. Hemophagocytic lymphohistiocytosis associated with H1N1 virus infection and visceral leishmaniasis in a 4.5-month-old infant. Rev Soc Bras Med Trop. 2012 Jun;45(3):407-9.[↩]
- Imashuku S, Kuriyama K, Teramura T, Ishii E, Kinugawa N, Kato M, Sako M, Hibi S. Requirement for etoposide in the treatment of Epstein-Barr virus-associated hemophagocytic lymphohistiocytosis. J Clin Oncol. 2001;19:2665–2673. doi: 10.1200/JCO.2001.19.10.2665[↩]
- Huang Z, Xie J. Ruxolitinib in conjunction with the HLH-94 protocol for Epstein-Barr virus-related hemophagocytic lymphohistiocytosis in the intensive care unit: A case report. Medicine (Baltimore) 2021;100(e25188) doi: 10.1097/MD.0000000000025188[↩]
- Zhao Y, Li Z, Zhang L, Lian H, Ma H, Wang D, Zhao X, Zhang Q, Wang T, Zhang R. L-DEP regimen salvage therapy for paediatric patients with refractory Epstein-Barr virus-associated haemophagocytic lymphohistiocytosis. Br J Haematol. 2020;191:453–459. doi: 10.1111/bjh.16861[↩]
- Huang P, Huang C, Xu H, Lu J, Tian R, Wang Z, Chen Y. Early use of blood purification in severe Epstein-Barr virus-associated hemophagocytic syndrome. Pediatrics. 2020;145(e20193197) doi: 10.1542/peds.2019-3197[↩][↩][↩]
- Shiraishi A, Ohga S, Doi T, Ishimura M, Takimoto T, Takada H, Miyamoto T, Abe Y, Hara T. Treatment choice of immunotherapy or further chemotherapy for Epstein-Barr virus-associated hemophagocytic lymphohistiocytosis. Pediatr Blood Cancer. 2012;59:265–270. doi: 10.1002/pbc.24039[↩]
- Belyea B, Hinson A, Moran C, Hwang E, Heath J, Barfield R. Spontaneous resolution of Epstein-Barr virus-associated hemophagocytic lymphohistiocytosis. Pediatr Blood Cancer. 2010;55:754–756. doi: 10.1002/pbc.22618[↩]
- Gurunathan A, Boucher AA, Mark M, Prus KM, O’Brien MM, Breese EH, Mizukawa BE, Absalon MJ, Nelson AS, Jordan MB, et al. Limitations of HLH-2004 criteria in distinguishing malignancy-associated hemophagocytic lymphohistiocytosis. Pediatr Blood Cancer. 2018;65(e27400) doi: 10.1002/pbc.27400[↩][↩]
- Lackner H, Seidel MG, Strenger V, Sovinz P, Schwinger W, Benesch M, Sperl D, Urban C. Hemophagocytic syndrome in children with acute monoblastic leukemia-another cause of fever of unknown origin. Support Care Cancer. 2013;21:3519–3523. doi: 10.1007/s00520-013-1937-x[↩]
- Han L, Li L, Wu J, Li X, Zhang L, Wang X, Fu X, Ma W, Sun Z, Zhang X, et al. Clinical features and treatment of natural killer/T cell lymphoma associated with hemophagocytic syndrome: comparison with other T cell lymphoma associated with hemophagocytic syndrome. Leuk Lymphoma. 2014;55:2048–2055. doi: 10.3109/10428194.2013.876629[↩]
- Chi MS, Chang YC, Chi KH. In Reply to Roos et al. Int J Radiat Oncol Biol Phys. 2018 Jul 15;101(4):1003. doi: 10.1016/j.ijrobp.2018.03.042[↩]
- Eloseily EM, Weiser P, Crayne CB, Haines H, Mannion ML, Stoll ML, Beukelman T, Atkinson TP, Cron RQ. Benefit of anakinra in treating pediatric secondary hemophagocytic lymphohistiocytosis. Arthritis Rheumatol. 2020;72:326–334. doi: 10.1002/art.41103[↩]
- Bami S, Vagrecha A, Soberman D, Badawi M, Cannone D, Lipton JM, Cron RQ, Levy CF. The use of anakinra in the treatment of secondary hemophagocytic lymphohistiocytosis. Pediatr Blood Cancer. 2020;67(e28581) doi: 10.1002/pbc.28581[↩]
- Bagri NK, Gupta L, Sen ES, Ramanan AV. Macrophage activation syndrome in children: Diagnosis and management. Indian Pediatr. 2021;58:1155–1161. doi: 10.1007/s13312-021-2399-8[↩]
- Ravelli A, Minoia F, Davì S, Horne A, Bovis F, Pistorio A, Aricò M, Avcin T, Behrens EM, De Benedetti F, et al. 2016 Classification criteria for macrophage activation syndrome complicating systemic juvenile idiopathic arthritis: A European league against rheumatism/American college of rheumatology/paediatric rheumatology international trials organisation collaborative initiative. Arthritis Rheumatol. 2016;68:566–576. doi: 10.1002/art.39332[↩]
- Shalabi H, Gust J, Taraseviciute A, Wolters PL, Leahy AB, Sandi C, Laetsch TW, Wiener L, Gardner RA, Nussenblatt V, et al. Beyond the storm-subacute toxicities and late effects in children receiving CAR T cells. Nat Rev Clin Oncol. 2021;18:363–378. doi: 10.1038/s41571-020-00456-y[↩]
- Ishida H, Yoshida H, Yoshihara T, Ito M, Morimoto A. Origin of macrophages involved in the development of allogeneic hematopoietic stem cell transplantation-associated hemophagocytic syndrome: Observations on a patient with juvenile myelomonocytic leukemia. Bone Marrow Transplant. 2007;40:701–703. doi: 10.1038/sj.bmt.1705783[↩]
- Ostronoff M, Ostronoff F, Coutinho M, Calixto R, Souto Maior AP, Sucupira A, Florencio R, Tagliari C. Hemophagocytic syndrome after autologous peripheral blood stem cell transplantation for multiple myeloma; successful treatment with high-dose intravenous immunoglobulin. Bone Marrow Transplant. 2006;37:797–798. doi: 10.1038/sj.bmt.1705329[↩]
- Koyama M, Sawada A, Yasui M, Inoue M, Kawa K. Encouraging results of low-dose etoposide in the treatment of early-onset hemophagocytic syndrome following allogeneic hematopoietic stem cell transplantation. Int J Hematol. 2007;86:466–467. doi: 10.1007/BF02984009[↩]
- Ono R, Ashiarai M, Hirabayashi S, Mizuki K, Hosoya Y, Yoshihara H, Ohtake J, Mori S, Manabe A, Hasegawa D. Ruxolitinib for hematopoietic cell transplantation-associated hemophagocytic lymphohistiocytosis. Int J Hematol. 2021;113:297–301. doi: 10.1007/s12185-020-02999-3[↩]
- Hines MR, von Bahr Greenwood T, Beutel G, Beutel K, Hays JA, Horne A, Janka G, Jordan MB, van Laar JAM, Lachmann G, et al. Consensus-based guidelines for the recognition, diagnosis, and management of hemophagocytic lymphohistiocytosis in critically Ill children and adults. Crit Care Med. 2022;50:860–872. doi: 10.1097/CCM.0000000000005361[↩]
- Vallurupalli M, Berliner N. Emapalumab for the treatment of relapsed/refractory hemophagocytic lymphohistiocytosis. Blood. 2019 Nov 21;134(21):1783-1786. doi: 10.1182/blood.2019002289[↩]
- Albeituni S, Verbist KC, Tedrick PE, Tillman H, Picarsic J, Bassett R, Nichols KE. Mechanisms of action of ruxolitinib in murine models of hemophagocytic lymphohistiocytosis. Blood. 2019 Jul 11;134(2):147-159. doi: 10.1182/blood.2019000761[↩]
- Wang J, Wang Y, Wu L, Wang X, Jin Z, Gao Z, Wang Z. Ruxolitinib for refractory/relapsed hemophagocytic lymphohistiocytosis. Haematologica. 2020 May;105(5):e210-e212. doi: 10.3324/haematol.2019.222471[↩][↩]
- de Jesus AA, Hou Y, Brooks S, et al. Distinct interferon signatures and cytokine patterns define additional systemic autoinflammatory diseases. J Clin Invest. 2020 Apr 1;130(4):1669-1682. doi: 10.1172/JCI129301[↩]
- Marsh RA, Allen CE, McClain KL, Weinstein JL, Kanter J, Skiles J, Lee ND, Khan SP, Lawrence J, Mo JQ, et al. Salvage therapy of refractory hemophagocytic lymphohistiocytosis with alemtuzumab. Pediatr Blood Cancer. 2013;60:101–109. doi: 10.1002/pbc.24188[↩]
- Das R, Guan P, Sprague L, Verbist K, Tedrick P, An QA, Cheng C, Kurachi M, Levine R, Wherry EJ, et al. Janus kinase inhibition lessens inflammation and ameliorates disease in murine models of hemophagocytic lymphohistiocytosis. Blood. 2016;127:1666–1675. doi: 10.1182/blood-2015-12-684399[↩]
- De Benedetti F, Brunner HI, Ruperto N, Kenwright A, Wright S, Calvo I, Cuttica R, Ravelli A, Schneider R, Woo P, et al. Randomized trial of tocilizumab in systemic juvenile idiopathic arthritis. N Engl J Med. 2012;367:2385–2395. doi: 10.1056/NEJMoa1112802[↩]
- Bottari G, Murciano M, Merli P, Bracaglia C, Guzzo I, Stoppa F, Pardeo M, Nunziata J, Bufalo FD, Genuini L, et al. Hemoperfusion with cytosorb to manage multiorgan dysfunction in the spectrum of hemophagocytic lymphohistiocytosis syndrome in critically Ill children. Blood Purif. 2022;51:417–424. doi: 10.1159/000517471[↩][↩]
- Matsumoto Y, Naniwa D, Banno S, Sugiura Y. The efficacy of therapeutic plasmapheresis for the treatment of fatal hemophagocytic syndrome: Two case reports. Ther Apher. 1998;2:300–304. doi: 10.1111/j.1744-9987.1998.tb00127.x[↩]
- Demirkol D, Yildizdas D, Bayrakci B, Karapinar B, Kendirli T, Koroglu TF, Dursun O, Erkek N, Gedik H, Citak A, et al. Hyperferritinemia in the critically ill child with secondary hemophagocytic lymphohistiocytosis/sepsis/multiple organ dysfunction syndrome/macrophage activation syndrome: What is the treatment? Crit Care. 2012;16(R52) doi: 10.1186/cc11256[↩]
- La Rosée P, Horne A, Hines M, von Bahr Greenwood T, Machowicz R, Berliner N, Birndt S, Gil-Herrera J, Girschikofsky M, Jordan MB, et al. Recommendations for the management of hemophagocytic lymphohistiocytosis in adults. Blood. 2019;133:2465–2477. doi: 10.1182/blood.2018894618[↩]
- Yan WL, Yang SL, Zhao FY, Xu XJ. Ruxolitinib is an alternative to etoposide for patient with hemophagocytic lymphohistiocytosis complicated by acute renal injury: A case report. J Oncol Pharm Pract. 2022;28:222–227. doi: 10.1177/10781552211020821[↩]
- Broglie L, Pommert L, Rao S, Thakar M, Phelan R, Margolis D, Talano J. Ruxolitinib for treatment of refractory hemophagocytic lymphohistiocytosis. Blood Adv. 2017;1:1533–1536. doi: 10.1182/bloodadvances.2017007526[↩]
- Janka GE. Familial hemophagocytic lymphohistiocytosis. Eur J Pediatr. 1983;140:221–230. doi: 10.1007/BF00443367[↩]
- Messina C, Zecca M, Fagioli F, Rovelli A, Giardino S, Merli P, Porta F, Aricò M, Sieni E, Basso G, et al. Outcomes of children with hemophagocytic lymphohistiocytosis given allogeneic hematopoietic stem cell transplantation in italy. Biol Blood Marrow Transplant. 2018;24:1223–1231. doi: 10.1016/j.bbmt.2018.01.022[↩]





{kind=link}