
Contents
What is hidradenitis suppurativa
Hidradenitis suppurativa also known as acne inversa, is a chronic painful inflammatory disease of the apocrine sweat glands in your armpits, groin, under the breasts and/or anogenital regions of the body, although other sites may be involved 1. The sweat glands become clogged due to a variety of reasons, leading to enlargement (dilatation) of the ducts behind them. This dilatation predisposes the area to inflammation and infection by a variety of bacteria. Those with hidradenitis suppurativa typically have multiple large, recurrent boil-like nodules (red bumps) and abscesses on the buttocks, breasts, groin, and armpits. The bumps gradually get larger and drain pus. After multiple bouts of this cycle of plugging, enlargement, drainage and difficult-to-heal open wounds (sinuses), there may be scarring.
Hidradenitis suppurativa onset is generally after puberty and most common between 20-24 years of age. Onset before puberty is uncommon, but does correlate with a greater severity later in life and a positive family history 2.
Potential complications of hidradenitis suppurativa include keloid scars, fistulas, lymphedema, squamous cell carcinoma (SCC), anemia of chronic disease, amyloid of the skin and/or kidney with the development of nephrotic syndrome, scarring, and limb contractures 3. Cancer, in particular squamous cell carcinoma (SCC) may rarely occur 4. Patients may die. The typical patient is one with long term, severe disease who develops a very painful nodule or lesion, often in the perianal or perineal area.
Hidradenitis suppurativa also has significant psychological impact and many patients suffer from impairment of body image, depression and anxiety.
While there is no cure for hidradenitis suppurativa, you can work with your doctor to treat existing lesions and prevent new ones.
Hidradenitis suppurativa treatment:
- Weight loss
- Smoking cessation
- Topical or oral antibiotics
- Intralesional steroids
- Low-dose prednisone
- 1064 nm nd:YAG Laser
- Laser hair removal
- Adalimumab
- Diabetic agents (e.g. metformin)
- Surgery
Figure 1. Hidradenitis suppurativa armpit

Figure 2. Hidradenitis suppurativa groin

Is hidradenitis suppurativa contagious?
No. Hidradenitis suppurativa is non-contagious and you cannot spread hidradenitis suppurativa to another person through contact.
What are apocrine sweat glands?
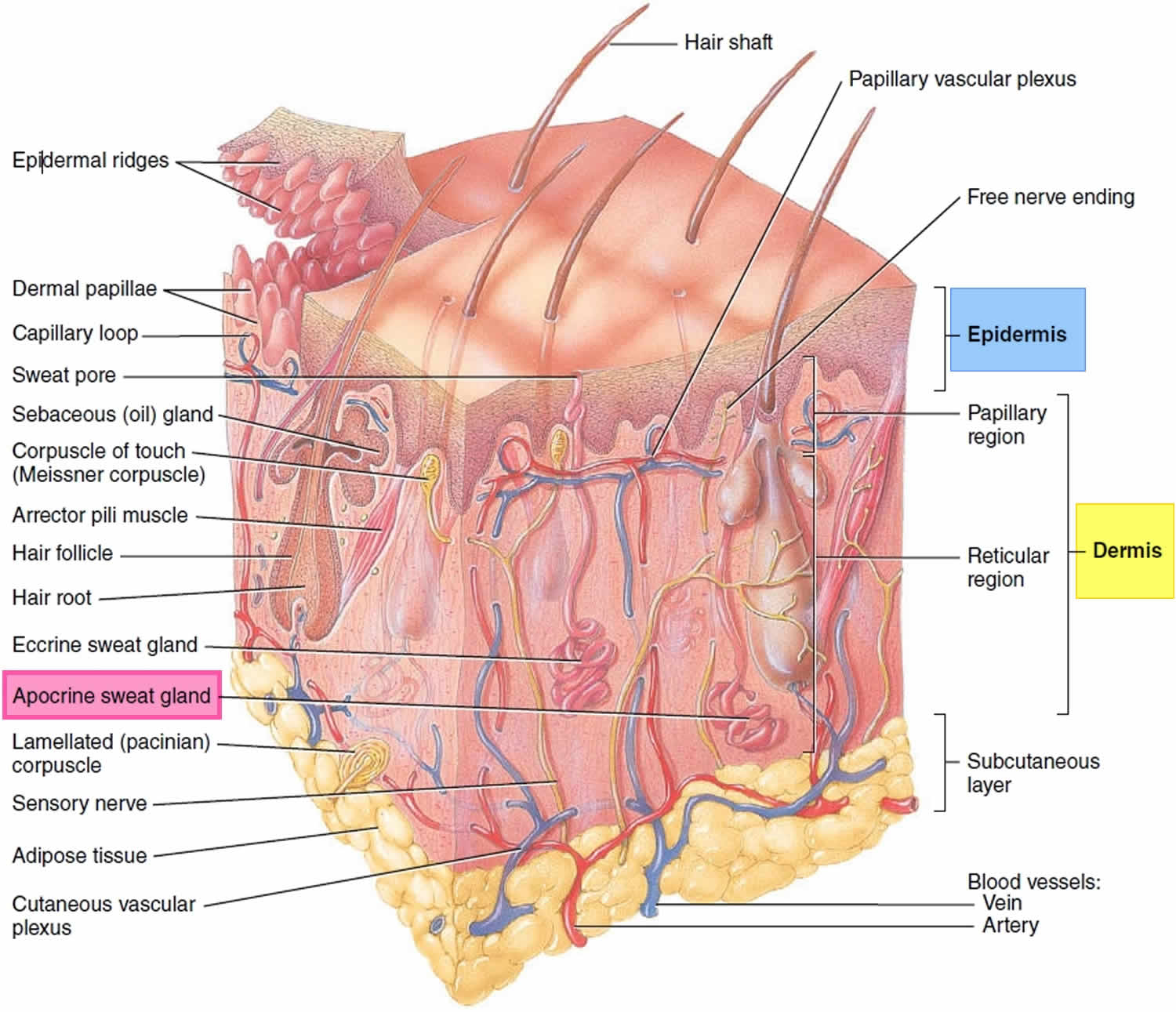
Sweating prevents overheating of your body, because sweat cools your skin as it evaporates. Only mammals have sweat glands (sudoriferous glands). Humans have more than 2.5 million sweat glands distributed over the entire skin surface, except on the nipples and parts of the external genitalia. Humans normally produce about 500 ml of sweat per day, but this amount can increase to 12 liters (over 3 gallons) on hot days during vigorous exercise. Hair interferes with the evaporation of sweat and the ability to cool the body, so the need for increased temperature regulation through sweating led to a reduction of hairiness in humans.
There are two types of sweat glands, both of which increase their secretion in response to stress as well as to heat: eccrine and apocrine glands.
Eccrine glands (“secreting”) are by far the more numerous type (Figure 3). They are most abundant on the palms, soles, and forehead. Each is a coiled version of a simple tubular gland. The coiled, secretory base lies in the deep dermis and hypodermis, and the duct runs superficially to open at the skin surface through a funnel-shaped pore. (Although most pores on the skin surface are sweat pores, the “pores” seen on the face are openings of hair follicles.)
Apocrine glands are mostly confined to the armpits, anal, and genital areas. They are larger than eccrine glands, and their ducts open into hair follicles. Apocrine glands produce a special kind of sweat consisting of fatty substances and proteins, in addition to the components of true sweat. For this reason, apocrine sweat is viscous and sometimes has a milky or yellow color. This product is odorless when first secreted, but as its organic molecules are decomposed by bacteria on the skin, it takes on a musky smell. This is the source of body odor.
Apocrine glands start to function at puberty under the influence of androgens. Their activity is increased by sexual foreplay, and they enlarge and recede with the phases of a woman’s menstrual cycle. The secretions from the apocrine glands were identified as true human pheromones (chemical signals that convey information to a member of the same species) in the late 1990s when it was shown that they are responsible for the synchrony of the menstrual cycle that occurs in females who live together.
Apocrine glands are involved with sexual signaling and appear to function in attractiveness and mate selection. The genes that encode for the immune system, the major histocompatibility complex (MHC), also influence secretions from apocrine glands. Each person has a unique set of these genes. In experiments, the body odor scents that women selected as “sexy” or “attractive” came from men who had immune system genes most different from their own. Mates with complementary immune system genes provide their offspring with greater disease protection and decreased likelihood of recessive disorders.
Figure 3. Skin and apocrine sweat glands
Who’s at risk of hidradenitis suppurativa?
Hidradenitis suppurativa usually starts soon after puberty and continues into adult life. Hidradenitis suppurativa is most active between the ages of 20 and 40 years. Hidradenitis suppurativa is three times more common in females than in males and and in women, it can resolve at menopause. Hidradenitis suppurativa is also common in African Americans. Hair removal from shaving or using depilatories, deodorants, and irritation from anything rubbing against the affected area can worsen the condition. Hidradenitis suppurativa is often associated with smoking, obesity, and increased hormones. Additionally, it often runs in families.
Risk factors for developing hidradenitis suppurativa include:
- Other family members with hidradenitis suppurativa
- Obesity and insulin resistance/metabolic syndrome
- Cigarette smoking
- Follicular occlusion disorders: acne conglobata, dissecting cellulitis, pilonidal sinus
- Inflammatory bowel disease (Crohn disease)
- Diabetes
- Polycystic Ovarian Syndrome (PCOS)
- Spondyloarthrothopies
- Heart Disease
- Rare autoinflammatory syndromes associated with abnormalities of PSTPIP1 gene. PAPA syndrome (pyogenic arthritis, pyoderma gangrenosum and acne), PASH syndrome (pyoderma gangrenosum, acne, suppurative hidradenitis) and PAPASH syndrome (pyogenic arthritis, pyoderma gangrenosum, acne, suppurative hidradenitis).
Hidradenitis suppurativa stages
The severity and extent of hidradenitis suppurativa should be recorded at assessment and when determining the impact of a treatment. Two scoring systems are in common use: Hurley Stages and Sartorius Hidradenitis Suppurativa Score.
The Hurley system describes three distinct clinical stages 6:
- Stage 1: Solitary or multiple, isolated abscess formation without scarring or sinus tracts
- Stage 2: Recurrent abscesses, single or multiple widely separated lesions, with sinus tract formation
- Stage 3: Diffuse or broad involvement, with multiple interconnected sinus tracts and abscesses.
- Severe hidradenitis (Hurley Stage 3) has been associated with:
- Male gender
- Armpit and perianal involvement
- Obesity
- Smoking
- Disease duration.
- Severe hidradenitis (Hurley Stage 3) has been associated with:
Hurley Staging allows medical professionals to assign a severity level to hidradenitis suppurativa, but it does not account for disease activity, measure pain, or quality of life impact.
Sartorius Hidradenitis Suppurativa Score
The Sartorius Hidradenitis Suppurativa Score is made by counting involved regions, nodules and sinus tracts 7:
- Anatomic region involved (axilla, groin, genital, gluteal, or other inflammatory region left and/or right): 3 points per region involved
- Number and scores of lesions (abscesses, nodules, fistulas, scars): 2 points for each nodule, 4 points for each fistula, 1 point for each scar, 1 point each for “other”
- Longest distance between 2 relevant lesions (ie, nodules and fistulas, in each region, or size if only 1 lesion): Less than 5 cm, 2 points; less than 10 cm, 4 points; more than 10 cm, 8 points
- Lesions clearly separated by normal skin in each region: If yes, 0 points; if no, 6 points.
Hidradenitis suppurativa symptoms
Hidradenitis can affect a single or multiple areas in the armpits, neck, submammary area, and inner thighs. Anogenital involvement most commonly affects the groin, mons pubis, vulva (in females), sides of the scrotum (in males), perineum, buttocks and perianal folds.
Signs of hidradenitis suppurativa include:
- Open and closed comedones
- Painful firm papules, larger nodules and pleated ridges
- Pustules, fluctuant pseudocysts and abscesses
- Pyogenic granulomas
- Draining sinuses linking inflammatory lesions
- Hypertrophic and atrophic scars.
Many patients with hidradenitis suppurativa also suffer from other skin disorders, including acne, hirsutism and psoriasis.
The severity and extent of hidradenitis suppurativa is recorded at assessment and when determining the impact of a treatment.
Hidradenitis suppurativa causes
The cause of hidradenitis suppurativa is unknown. It is thought that there is an exaggerated inflammatory response to the presence of bacteria trapped in obstructed hair follicles in the skin. In some cases there does seem to be a genetic component. Bacteria seem to play some role, which is why antibiotics may be used in treatment. However, bacteria are not the primary cause of hidradenitis suppurativa. Other factors such as obesity, smoking and stress also play a role.
Contributing factors include:
- Friction from clothing and body folds
- Aberrant immune response to commensal bacteria
- Abnormal cutaneous or follicular microbiome
- Follicular occlusion
- Release of pro-inflammatory cytokines
- Inflammation causing rupture of the follicular wall and destroying apocrine glands and ducts
- Secondary bacterial infection
- Certain drugs.
Follicular Occlusion
Hidradenitis suppurativa was originally thought to be caused by a defect of the sweat gland, but this view has changed and it is now widely accepted to be a problem with the hair follicle. Build-up of keratin (a type of protein) within the hair follicle eventually plugs the hair follicle, causing further build up, and eventually the hair follicle ruptures and releases this material into the surrounding skin resulting in an intense inflammatory response 8.
Bacteria
Sometimes bacteria can be isolated from hidradenitis suppurativa lesions, while other times cultures from hidradenitis suppurativa lesions are sterile (no bacteria found) 9. Those affected by hidradenitis suppurativa frequently experience the characteristic symptoms of an infection, such as pain, tenderness, warmth, and purulent drainage. It may be reasonable to assume that since symptoms tend to improve after antibiotics, that hidradenitis suppurativa is caused primarily by bacteria, however this is not the case.
Biofilms
Recently, hidradenitis suppurativa has been described as a biofilm disease. When numerous bacteria secrete a sticky material known as a polysaccharide matrix and bind to a surface they now exist in what is known as a biofilm. When bacteria exist in a biofilm they become highly resistant to antibiotics. A recent study looking at biopsy samples (pieces of skin) from patients with hidradenitis suppurativa, demonstrated that biofilms were associated with chronic hidradenitis suppurativa 10. Although, biofilms likely don’t form primarily, this may be the reason that hidradenitis suppurativa become very resistant to medical management as it becomes more severe.
Aberrant Immunity
Several markers of inflammation exist in the blood and skin and can be used to assess the inflammatory state of the body. Abnormal levels of these markers have been implicated in the development of several diseases and similarly found to be abnormal in hidradenitis suppurativa. Additional research is needed to determine the implications of these abnormal levels, but these findings have led to the use of biologic medications, such as adalimumab and infliximab for the treatment of hidradenitis suppurativa.
Diet
Nutrition is an understudied and notoriously difficult topic to research in medicine. The majority of evidence is based on individual experience with few published articles in the literature, but the impact of diet on hidradenitis suppurativa infiltrates through social media and online message boards with reports of improvement that ranges from minimal or no effect to complete resolution. In one survey study involving 47 patients who followed dairy free diets, no patients experienced disease progression and 83% improved to various degrees 11. In another study, 12 subjects underwent surgical excision followed by diet modification with no wheat or brewers yeast consumption with immediate disease stabilization during a 12 month period of follow up 12.
Additional research is needed in order to allow for comprehensive diet counseling. Some patients have reported improvement after exclusion of nightshades, simple carbohydrates, and dairy, but the impact of diet modification appears to be highly individual and should be discussed with your physician or nutritionist. Dieticians can provide individualized meal plans to make sure that you are getting all of the required nutrients.
Other Factors
Several other factors have been implicated in the development of hidradenitis suppurativa. Smoking is more common among people with hidradenitis suppurativa than among the general population, and the components of smoke are known to promote hyperkeratosis (causing follicular occlusion) and also increases inflammation potentially worsening hidradenitis suppurativa 13. Mechanical factors caused by skin to skin contact and obesity may also contribute to the overall inflammatory state of hidradenitis suppurativa and the development or progression of hidradenitis suppurativa.
Lastly, hormones are potentially implicated in hidradenitis suppurativa. It is known that more women are affected by hidradenitis suppurativa than men and therefore a hormonal component has been hypothesized. Androgens, a type of hormone, can increase proliferation of the keratinocytes (skin cells), however the hormonal profile of patients with hidradenitis suppurativa is usually found to be normal 13.
With numerous factors implicated in the development of hidradenitis suppurativa, it is clear that additional research is needed and the trigger for one patient may not be consistent across the entire population.
Hidradenitis suppurativa treatment
General measures
Friction and moisture in the affected areas should be reduced as much as possible. Weight loss can greatly improve the condition if the patient is overweight 14. Topical clindamycin may be helpful (or benzoyl peroxide 10% wash). Bleach baths and Hibiclens may have some benefit. Smokers should stop. Bacterial cultures may occasionally be done to rule out other causes or secondary infection.
- Weight loss; follow an anti-inflammatory, low-sugar, low-grain, low-dairy diet (mainly plants)
- Smoking cessation: this can lead to improvement within a few months
- Loose fitting clothing
- Daily unfragranced antiperspirants
- If prone to secondary infection, wash with antiseptics or take bleach baths
- Apply hydrogen peroxide solution or medical grade honey to reduce malodour
- Use peeling agents such as resorcinol 15% cream to de-roof nodules
- Apply simple dressings to draining sinuses
- Analgesics, such as paracetamol (acetaminophen), for pain control
- Seek help to manage anxiety and depression.
Figure 4. Hidradenitis suppurativa treatment algorithm
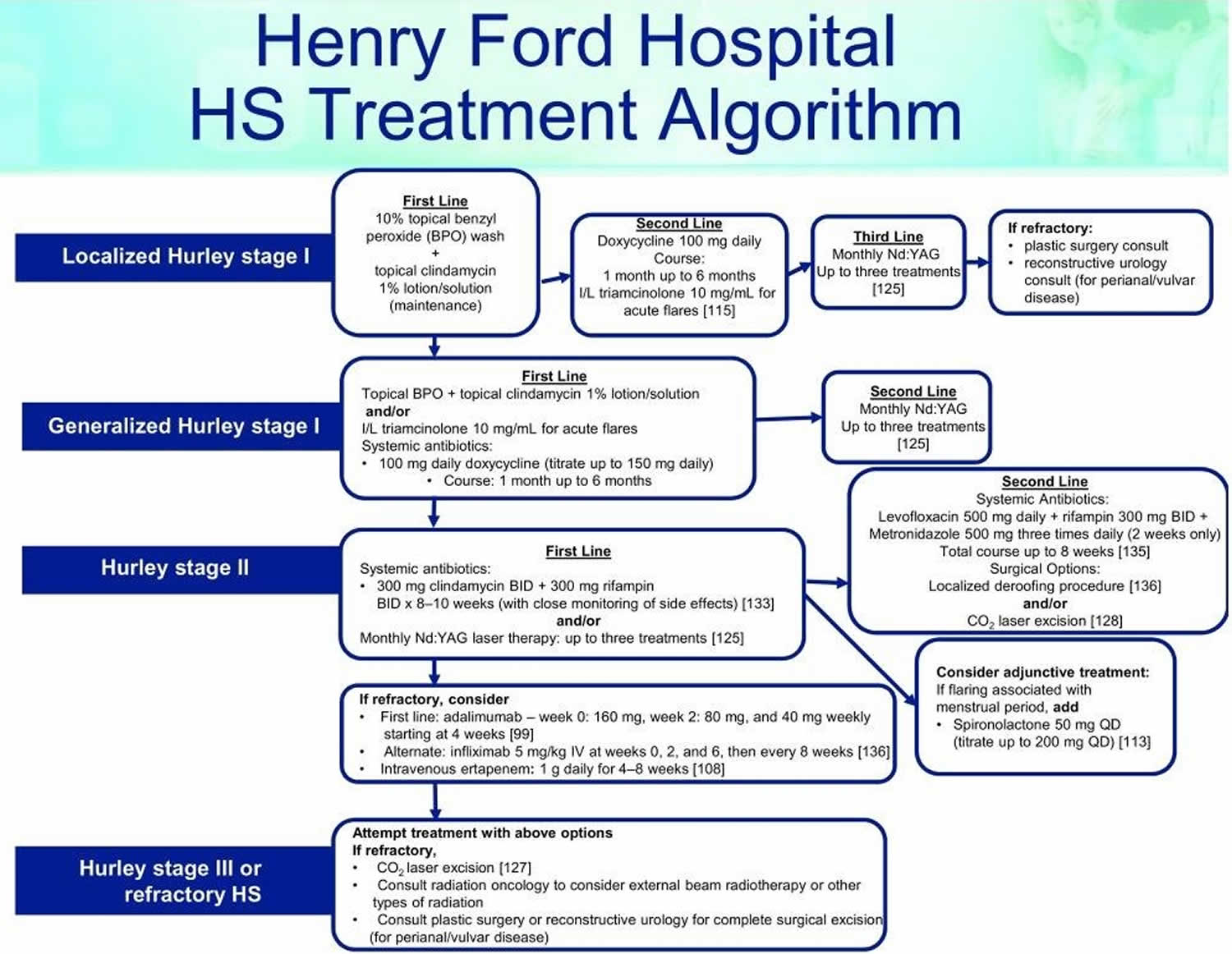
Footnote: This treatment algorithm is used in the Henry Ford Dermatology Clinic, which provides care to more than 1,000 patients with HS. The algorithm is based on a combination of evidence-based research and provider experience.
Abbreivations: HS = hidradenitis suppurativa; BID = bis in die (twice daily); I/L = intralesional; IV = intravenously; Nd:YAG = neodymium-doped yttrium aluminum garnet; QD = quaque die (once daily)
[Source 1]Medical management of hidradenitis suppurativa
Medical management of hidradenitis suppurativa is difficult. Treatment is required long term. Effective options are listed below.
Antibiotics
- Topical clindamycin, with benzoyl peroxide to reduce bacterial resistance
- Short course of oral antibiotics for acute staphylococcal abscesses, eg flucloxacillin
- Oral antibiotics can be very helpful. Prolonged courses (minimum 3 months) of tetracycline, metronidazole, trimethoprim + sulphamethoxazole, fluoroquinolones, ertapenem or dapsone for their anti-inflammatory action.
- Doxycycline 100 mg oral twice daily ongoing can be beneficial.
- Dapsone, 5-200 mg/day, may be helpful.
- 6–12 week courses of the combination of clindamycin (or doxycycline) and rifampicin for severe disease.
- Several experts recommend treatment for more severe, unstable hidradenitis suppurativa, with the combination of clindamycin 300 mg and rifampicin 300 mg both twice daily for 10 weeks. On the plus side, rifampicin acts against Clostridium difficule infections, decreasing the risk of colitis. On the down side, rifampicin can inactivate birth control pills. Also, it can turn bodily secretions orange, e.g. tears, sweat and urine.
- Other options include amoxicillin with clavulanic acid or fluoroquinolones (e.g., ciprofloxacin). Trimethoprim with sulfamethoxazole may also be beneficial. One study showed Staphylococcus epidermidis, Proteus mirabilis, and Staphylococcus aureus to be the most common isolates 15.
Antiandrogens
- Long-term oral contraceptive pill; antiandrogenic progesterones drospirenone or cyproterone acetate may be more effective than standard combined pills. These are more suitable than progesterone-only pills or devices.
- Spironolactone. Some women experience a premenstrual flare. For them, antiandrogen therapy (e.g., spironolactone) may be helpful.
- Finasteride has been used in children with hidradenitis suppurativa with success 16, 17. Three female patients, ages six, seven, and 15 who had failed standard therapy including isotretinoin, were treated with finasteride 1.25-10 mg/day for up to six years. Adjunctive birth control pills were given if the patient was a menstruating female. Treatment resulted in decreased frequency and severity of disease flares with no significant adverse effects.
- Response takes 6 months or longer.
Immunomodulatory treatments for severe disease
- Intralesional corticosteroids into nodules (e.g., Triamcinolone 5-10 mg/mL) can give the patient great relief. In one study utilizing triamcinolone 10 mg/mL 18, pain was reduced after 1 day and signs of inflammation after 7 days.
- Systemic corticosteroids short-term for flares. In one report 19, 13 patients were treated initially with prednisone 10 mg/day (ultimate dose varied from 5-15 mg/day). This was given in addition to existing therapy when that was not sufficient for control (e.g., acitretin, adalimumab, dapsone, clindamycin, doxycycline). All patients received calcium (1200 mg/day) and vitamin D (1000 IU/day) and monthly glucose monitoring. Overall, 11/13 patients showed a clinical response with the addition of low-dose prednisone. Side effects were minor and included hyperglycemia, sleep disturbance, and mild psychomotor agitation.
- Methotrexate, cyclosporin, and azathioprine. A few case reports highlight the benefit of cyclosporin. One patient did well on long-term cyclosporin 5 mg/kg/day, then 3 mg/kg/day 20.
- If oral and topical antibiotics plus general measures are not sufficient, a biologic agent is often added. TNF-α inhibitors adalimumab and infliximab, used in higher dose than required for psoriasis, are the most successful treatments to date. Note that paradoxically, they may sometimes induce new-onset hidradenitis suppurativa
- Other biologics are under investigation, such as the IL-1β antagonist, canakinumab
Adalimumab
Adalimumab is FDA-approved for moderate to severe hidradenitis suppurativa that is resistant to conventional therapies, but the dosing is weekly (for psoriasis, it is every other week). Adalimumab for hidradenitis suppurativa is given as a subcutaneous injection as follows: 160 mg day 1; 80 mg day 15; 40 mg day 29; and then weekly ongoing. Combining adalimumab with oral antibiotics, e.g., doxycycline increases efficacy. Interestingly, the incidence of serious infections is not higher than placebo.
In one randomized double blind controlled trial, adalimumab weekly was superior to both adalimumab every other week and placebo 21.
Other biologic agents
In comparing all the biologic agents, one review put the percent responders at 89% infliximab, 79% adalimumab, and 56% for etanercept 22. Ustekinumab has also been used in a few patients. Infliximab seems to be most effective but in one study 22% experienced serious adverse events, the most common being infusion reactions, and one patient died of pneumococcal sepsis. In one study 23 of 11 patients with severe hidradenitis suppurativa unresponsive to more than three prior therapies, infliximab 5 mg/kg every four weeks was given. Nine of the 11 patients remain well-controlled on this regimen. Secukinumab has been helpful anecdotally.
Canakinumab is a human IgGk monoclonal antibody targeting IL-1B. It was beneficial in two patients with severe hidradenitis suppurativa 24.
Other medical treatments
- Metformin in patients with insulin resistance. Metformin 25 and more recently liragutide 26 have shown benefit in difficult to control hidradenitis suppurativa. In overweight or obese patients with recalcitrant disease, these agents may be beneficial.
- Acitretin (unsuitable for females of childbearing potential). Acitretin in one study of 12 patients did incredibly well 27. The average dose was 0.67 mg/kg/day. Nine patients achieved marked or complete remission after one course. The improvement generally started within two months and further improvement was achieved within the first six months of therapy. Isotretinoin has not shown analogous results.
- Isotretinoin — effective for acne but appears unhelpful for most cases of hidradenitis suppurativa
- Colchicine
- Anakinra (IL-1 receptor antagonist) showed benefit in a study of five patients 28. Another study randomized 20 patients to receive either anakinra or placebo for 12 weeks. The disease activity score was decreased at the end of treatment in 20% (2 of 10) of the placebo arm compared with 67% (6 of 9) of the anakinra arm 29
- Medical management of anxiety and depression
- Nd:YAG laser hair removal. For axillary involvement, laser hair removal can be quite helpful. In addition, the 1064 nm nd:YAG laser has been used ongoing with benefit in uncontrolled studies 30.
Hidradenitis suppurativa surgery
If medical therapy is not successful and the patient desires a “cure,” a surgical approach may be considered 31. This usually consists of excision of all diseased tissue in the area. Limited excisions usually result in recurrence adjacent to the scar. In one study, limited excision of diseased tissue had a 43% recurrence rate whereas radical excision had only a 27% recurrence rate 32. With appropriate patient selection, patient satisfaction with surgery is high 33.
There are both localized and extensive surgical interventions. Although there is no consensus on the best approach, procedures are carried out based on disease severity and location, with the overall goal of removing lesional tissue and sparing healthy skin to optimize outcomes.
- Incision and drainage of acute abscesses
- Curettage and deroofing of nodules, abscesses and sinuses. Incision and drainage is usually not helpful as lesions invariably recur. Deroofing an inflammatory nodule, curetting the base, and letting it heal by secondary intention is recommended 34.
- Laser ablation of nodules, abscesses and sinuses
- Wide local excision of persistent nodules
- Radical excisional surgery of entire affected area
Many approaches exist to manage hidradenitis suppurativa, including local destruction, incision and drainage, standard unroofing, and wide excision techniques 35. Local destruction is used to ablate hidradenitis suppurativa lesions and may be carried out with electrosurgery, cryotherapy, or laser removal. Incision and drainage may be used for decompression in acute episodes of unbearable pain. However, incision and drainage does not assist in the long-term resolution of disease, as the inflamed tissue remains and infection is almost certain to recur 36. Unroofing techniques are effective for both small and large lesional units and are carried out by opening the surface of all connected abscesses and tracts within an hidradenitis suppurativa lesion. The contents are removed by curettage, often leaving the site open to heal by secondary intention 37. Unroofing techniques are preferred for Hurley stage I/II, whereas skin-tissue-saving excision with electrosurgical peeling (STEEP) is preferred for Hurley stage II/III. Skin-tissue-saving excision with electrosurgical peeling (STEEP) similarly removes diseased, fibrotic tissue via electrosurgical loop while sparing healthy skin to decrease sequelae following the surgical procedure 38. Lesions that cannot be unroofed may be excised, which includes the removal of the entire diseased area up to the margins of normal-appearing subcutaneous tissue 35.
The best surgical approach for long-term outcomes is controversial and is dependent on the patient’s disease severity and location of the lesions. A recent systematic review and meta-analysis assessed for recurrence rates with varying methods of surgical management. The lowest rates of recurrence occurred following wide excision therapy when compared to local excision and deroofing procedures. This study also indicated that recurrence rates were lowest with skin grafts and skin flaps compared to primary closure, although this was limited by retrospective analysis and lack of randomization of closures 39. Wide excision followed by secondary intention healing was also shown to be functional and aesthetically acceptable to patients 40. Bias may exist in the discrepancy between recurrence rates and type of closure owing to the fact that primary closure is possible only with smaller wound sizes compared to larger excisions that simply cannot be closed by primary intention. Although this has not been formally assessed, the size of the wound may play a role.
The use of lasers in hidradenitis suppurativa management has gained recent popularity. The 1064 nm neodymium-doped yttrium aluminum garnet (Nd:YAG) laser appears to be an effective, novel modality in hidradenitis suppurativa management. After a series of treatments, two trials reported decreases in hidradenitis suppurativa-associated inflammation, scarring, and fibrosis, indicating successful, selective photothermolysis to manage the disease 41. It is best used in recalcitrant Hurley stage I and II patients.
Another type of laser used in the treatment of hidradenitis suppurativa is the carbon dioxide (CO2) laser, which is used to excise hidradenitis suppurativa lesions and ablate pathologic tissues. CO2 laser has been used since the late 1980s for hidradenitis suppurativa, although it is now increasing in popularity. Laser excision followed by marsupialization has been shown to be effective for the management of persistent or late-stage cases of hidradenitis suppurativa, with overall patient satisfaction in post-operative quality of life and pain measures 42. Additionally, a retrospective study (n = 58) of CO 2 laser evaporation techniques reported a 29% recurrence rate of disease within 12.2 months of the procedure (noted around the borders of treated regions), while 95% of patients reported some or great improvement in disease status 43. A reported complication of CO2 excision is scar contracture, restricted range of motion, and delayed wound healing. Nicholson et al. determined that fractional CO 2 therapy could be a helpful adjunct in these cases 44.
- Smith MK, Nicholson CL, Parks-Miller A, Hamzavi IH. Hidradenitis suppurativa: an update on connecting the tracts. F1000Research. 2017;6:1272. doi:10.12688/f1000research.11337.1. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5538037/[↩][↩]
- JAAD 2015;72;485[↩]
- JEADV 2016;230;174[↩]
- Ann R Coll Surg Engl. 2007 Oct; 89: 709–712[↩]
- Zarchi K, Dufour DN, Jemec GBE. Successful Treatment of Severe Hidradenitis Suppurativa With Anakinra. JAMA Dermatol. 2013;149(10):1192–1194. doi:10.1001/jamadermatol.2013.5377[↩]
- Hurley H. Axillary hyperhidrosis, apocrine bromhidrosis, hidradenitis suppurativa, and familial benign pemphigus: surgical approach. In: Roenigh R, Roenigh H, eds. Dermatologic surgery. New York: Marcel Dekker; 1989:729-739.[↩]
- Sartorius K, Emtestam L, Jemec GB et al. Objective scoring of hidradenitis suppurativa reflecting the role of tobacco smoking and obesity. Br J Dermatol 2009; 161: 831–839.[↩]
- Jemec GB, Hansen U. Histology of hidradenitis suppurativa. J Am Acad Dermatol. 1996;34(6):994-999.[↩]
- Ring HC, Riis Mikkelsen P, Miller IM, et al. The bacteriology of hidradenitis suppurativa: a systematic review. Exp Dermatol. 2015;24(10):727-731.[↩]
- Ring HC, Bay L, Nilsson M, et al. Bacterial Biofilm in Chronic Lesions of Hidradenitis Suppurativa. Br J Dermatol. 2016.[↩]
- Danby FW. Diet in the prevention of hidradenitis suppurativa (acne inversa). J Am Acad Dermatol. 2015;73(5 Suppl 1):S52-54.[↩]
- Cannistra C, Finocchi V, Trivisonno A, Tambasco D. New perspectives in the treatment of hidradenitis suppurativa: surgery and brewer’s yeast-exclusion diet. Surgery. 2013;154(5):1126-1130.[↩]
- Prens E, Deckers I. Pathophysiology of hidradenitis suppurativa: An update. J Am Acad Dermatol. 2015;73(5 Suppl 1):S8-11.[↩][↩]
- Acta Derm Vener 2014;94;553[↩]
- Acta Derm Venereol 2014; 94: 699–702[↩]
- JAMA Derm 2013;149(6):732-35[↩]
- PD 2017;34;578[↩]
- JAAD 2016;75;1151[↩]
- JAAD 2016;75;1061[↩]
- JAAD Dec 2012[↩]
- J Drugs Dermatol 2016;15;1192[↩]
- BJD 2013;168;243-52[↩]
- BJD April 2014[↩]
- JAMA Derm 2017;153;1195[↩]
- JEADV 2012;27;1101[↩]
- Br J Dermatol 2017;177;858[↩]
- Br J Dermatol Jan 2011[↩]
- J Am Acad Dermatol. 2014;70:243-51[↩]
- JAMA Derm 2016;152;52[↩]
- Semin Cutan Med Surg. 2017;36:67-74[↩]
- Dermatol Surg. 2016 Sep;42(9):1030-40[↩]
- Int J Colorectal Dis 1998;13;164[↩]
- Dermatol Surg. 2017 Jan;43(1):125-133[↩]
- BJD July 2012[↩]
- Danby FW, Hazen PG, Boer J: New and traditional surgical approaches to hidradenitis suppurativa. J Am Acad Dermatol. 2015;73(5 Suppl 1):S62–5. 10.1016/j.jaad.2015.07.043[↩][↩]
- Jemec GB: Clinical practice. Hidradenitis suppurativa. N Engl J Med. 2012;366(2):158–64. 10.1056/NEJMcp1014163[↩]
- Danby FW: Commentary: unroofing for hidradenitis suppurativa, why and how. J Am Acad Dermatol. 2010;63(3):481.e1–3. 10.1016/j.jaad.2010.01.033[↩]
- Blok JL, Spoo JR, Leeman FW, et al. : Skin-Tissue-sparing Excision with Electrosurgical Peeling (STEEP): a surgical treatment option for severe hidradenitis suppurativa Hurley stage II/III. J Eur Acad Dermatol Venereol. 2015;29(2):379–82. 10.1111/jdv.12376[↩]
- Mehdizadeh A, Hazen PG, Bechara FG, et al. : Recurrence of hidradenitis suppurativa after surgical management: A systematic review and meta-analysis. J Am Acad Dermatol. 2015;73(5 Suppl 1):S70–7. 10.1016/j.jaad.2015.07.044[↩]
- Humphries LS, Kueberuwa E, Beederman M, et al. : Wide excision and healing by secondary intent for the surgical treatment of hidradenitis suppurativa: A single-center experience. J Plast Reconstr Aesthet Surg. 2016;69(4):554–66. 10.1016/j.bjps.2015.12.004[↩]
- Xu LY, Wright DR, Mahmoud BH, et al. : Histopathologic study of hidradenitis suppurativa following long-pulsed 1064-nm Nd:YAG laser treatment. Arch Dermatol. 2011;147(1):21–8. 10.1001/archdermatol.2010.245[↩]
- Hazen PG, Hazen BP: Hidradenitis suppurativa: successful treatment using carbon dioxide laser excision and marsupialization. Dermatol Surg. 2010;36(2):208–13. 10.1111/j.1524-4725.2009.01427.x[↩]
- Mikkelsen PR, Dufour DN, Zarchi K, et al. : Recurrence rate and patient satisfaction of CO2 laser evaporation of lesions in patients with hidradenitis suppurativa: a retrospective study. Dermatol Surg. 2015;41(2):255–60. 10.1097/DSS.0000000000000264[↩]
- Nicholson CL, Hamzavi I, Ozog DM: Rapid healing of chronic ulcerations and improvement in range of motion after fractional carbon dioxide (CO 2) treatment after CO 2 excision of hidradenitis suppurativa axillary lesions: A case report. JAAD Case Rep. 2016;2(1):4–6. 10.1016/j.jdcr.2015.11.001[↩]





{kind=link}