Contents
- Echinococcus hydatid cyst
- Hydatid cyst classification
- Hydatid cyst disease causes
- Echinococcosis life cycle
- Echinococcus geographic distribution
- Echinococcus Hosts
- Hydatid disease prevention
- Hydatid disease symptoms
- Hydatid disease complications
- Hydatid disease diagnosis
- Hydatid cyst differential diagnosis
- Hydatid cyst treatment
- Cystic echinococcosis treatment
- World Health Organization (WHO) guidelines for cystic echinococcosis treatment
- Uncomplicated liver cystic echinococcosis cysts: types CE1 or CE3a < 5 cm
- Uncomplicated liver cystic echinococcosis cysts: types CE1 or CE3a 5 cm to 10 cm
- Uncomplicated liver cystic echinococcosis cysts: types CE1 or CE3a > 10 cm
- Uncomplicated liver cystic echinococcosis cysts: types CE2 or CE3b ≤ 5 cm
- Uncomplicated liver cystic echinococcosis cysts: types CE2 or CE3b > 5 cm
- Use of praziquantel combined with albendazole post-percutaneous/surgical procedures for hepatic cyst types CE1, CE2, CE3a, CE3b
- Uncomplicated lung cystic echinococcosis cysts ≤ 5 cm
- Antiparasitic therapy
- ‘Watch and wait’ approach
- Percutaneous therapy
- Surgery
- Alveolar echinococcosis treatment
- Hydatid disease prognosis
Echinococcus hydatid cyst
Hydatid cysts result from infection by a tapeworm of either the Echinococcus granulosus or Echinococcus multilocularis and can result in cyst formation anywhere in the body. Hydatid disease also known as hydatidosis, is a zoonosis, a disease that is transmitted to humans from animals caused by a parasitic infestation by a tapeworm of the genus Echinococcus 1. Human echinococcosis or hydatid disease is caused by ingestion of Echinococcus tapeworm eggs in contaminated food, water or soil, or after direct contact with animal hosts, leading to the formation of larval cysts, primarily in your liver and lungs, that can cause symptoms after years 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13.
Six species of Echinococcus tapeworms (family Taeniidae) have been identified which infect a wide range of domestic and wild animals, but four are of human health concern: Echinococcus granulosus (which causes cystic echinococcosis), Echinococcus multilocularis (which causes alveolar echinococcosis), and two forms of neotropical echinococcosis Echinococcus vogeli (which cause polycystic echinococcosis) and Echinococcus oligarthrus (which cause unicystic echinococcosis) 3, 10, 11, 4. Two new species have recently been identified: Echinococcus shiquicus in small mammals from the Tibetan plateau and Echinococcus felidis in African lions, but their zoonotic (animal to human) transmission potential is unknown 3. Several studies have shown that echinococcus infections are an increasing public health concern and that they can be regarded as emerging or re-emerging diseases.
- Echinococcus granulosus tapeworm larvae, a 7 millimeter long tapeworm found in dogs (definitive host) and sheep, cattle, goats, and pigs (intermediate hosts) cause cystic echinococcosis, also known as hydatid disease, hydatid cyst, hydatidosis or echinococcus cysticus. Human infection with Echinococcus granulosus leads to the development of one or more hydatid cysts located most often in the liver and lungs, and less frequently in the bones, kidneys, spleen, muscles and central nervous system.
- The asymptomatic incubation period of the disease can last many years until hydatid cysts grow to an extent that triggers clinical signs, however approximately half of all patients that receive medical treatment for infection do so within a few years of their initial infection with the parasite.
- Abdominal pain, nausea and vomiting are commonly seen when hydatids occur in the liver. If the lung is affected, clinical signs include chronic cough, chest pain and shortness of breath. Other signs depend on the location of the hydatid cysts and the pressure exerted on the surrounding tissues. Non-specific signs include anorexia, weight loss and weakness.
- Echinococcus multilocularis tapeworm larvae, a 1 mm to 4 millimeter long tapeworm found in foxes, coyotes, and dogs (definitive hosts) cause alveloar echinocccosis also known as alveococcosis, echinococcus alveolaris, alveolar hydatid, alveolar hydatidosis, alveolar hydatid disease, multilocular hydatid cyst, multilocular hydatid disease or multilocular hydatidosis 14. Small rodents are intermediate hosts for Echinococcus multilocularis. Although cases of alveolar echinococcosis in animals in endemic areas are relatively common, human cases are rare. Alveolar echinococcosis (Echinococcus multilocularis) poses a much greater health threat to humans than cystic echinococcosis (Echinococcus granulosus), causing parasitic tumors that can form in your liver, lungs, brain, and other organs. If left untreated, alveolar echinococcosis can be fatal. Because the Echinococcus multilocularis cysts are slow-growing, infection with alveolar echinococcosis may not produce any symptoms for many years. Pain or discomfort in your upper abdominal region, weakness, and weight loss may occur as a result of the growing cysts. Alveolar echinococcosis (Echinococcus multilocularis) symptoms may mimic those of liver cancer and cirrhosis of the liver.
- Alveolar echinococcosis is characterized by an asymptomatic incubation period of 5–15 years and the slow development of a primary tumour-like lesion which is usually located in the liver. Clinical signs include weight loss, abdominal pain, general malaise and signs of hepatic failure.
- Larval metastases may spread either to organs adjacent to the liver (for example, the spleen) or distant locations (such as the lungs, or the brain) following dissemination of the parasite via the blood and lymphatic system. If left untreated, alveolar echinococcosis is progressive and fatal.
- Echinococcus vogeli: infections cause polycystic echinococcosis.
- Echinococcus oligarthrus: infections cause unicystic echinococcosis.
The two most important forms of echinococcosis, which are of medical and public health relevance in humans, are cystic echinococcosis (Echinococcus granulosus) and alveolar echinococcosis (Echinococcus multilocularis) caused by larval stages (metacestode) of Echinococcus multilocularis and Echinococcus granulosus respectively 4. While cystic echinococcosis (Echinococcus granulosus) is worldwide, alveolar echinococcosis (Echinococcus multilocularis) is rarer and limited to the Northern hemisphere, but the latest epidemiological data indicate an increasing incidence 5, 15. Both alveolar echinococcosis (Echinococcus multilocularis) and cystic echinococcosis (Echinococcus granulosus) are caused by infection with Echinococcus tapeworms of the Taeniidae family which have different transmission cycles and different clinical presentations. However, both progress slowly in the liver, the usual primary infection site 5, 15.
Cystic echinococcosis (hydatid disease) or Echinococcus granulosus is globally distributed and found in every continent except Antarctica. Hydatid disease (cystic echinococcosis or Echinococcus granulosus) is not endemic in the United States, but the change in the immigration patterns and the marked increase in transcontinental transportation over the past 4 decades have caused a rise in the profile of this previously unusual disease throughout North America 16. In endemic regions, human incidence rates for cystic echinococcosis (hydatid disease) can reach more than 50 per 100,000 person-years, and prevalence levels as high as 5% to 10% may occur in parts of Argentina, Peru, East Africa, Central Asia and China. In livestock, the prevalence of cystic echinococcosis found in slaughterhouses in hyperendemic areas of South America varies from 20% to 95% of slaughtered animals. The highest prevalence of cystic echinococcosis (hydatid disease) or Echinococcus granulosus is found in rural areas where older animals are slaughtered. Depending on the infected species involved, livestock production losses attributable to cystic echinococcosis result from liver condemnation and may also involve reduction in carcass weight, decrease in hide value, decrease of milk production, and reduced fertility. Human infection with Echinococcus granulosus (cystic echinococcosis) leads to the development of one or more hydatid cysts (which are slow growing fluid-filled structures that contain the larvae) located most often in the liver and lungs, and less frequently in the bones, kidneys, spleen, muscles and central nervous system including the brain and eyes. The asymptomatic incubation period of cystic echinococcosis (Echinococcus granulosus) can last many years until hydatid cysts grow to a large size that triggers clinical signs, with approximately half of all patients that receive medical treatment for cystic echinococcosis (Echinococcus granulosus) do so within a few years of their initial infection with the Echinococcus granulosus parasite. Abdominal pain, nausea and vomiting are commonly seen when hydatids occur in the liver. If the lung is affected, clinical signs include chronic cough, chest pain and shortness of breath. Other signs depend on the location of the hydatid cysts and the pressure exerted on the surrounding tissues. Non-specific signs include anorexia, weight loss and weakness.
Alveolar echinococcosis (Echinococcus multilocularis) is confined to the northern hemisphere, in particular to regions of China, the Russian Federation and countries in continental Europe and North America. Alveolar echinococcosis (Echinococcus multilocularis) is characterized by an asymptomatic incubation period of 5 to 15 years and the slow development of a primary tumor-like lesion which is usually located in the liver. Alveolar echinococcosis (Echinococcus multilocularis) clinical signs include weight loss, abdominal pain, general malaise and signs of liver failure. Alveolar echinococcosis (Echinococcus multilocularis) larval metastases may spread either to organs adjacent to the liver for example, the spleen or distant locations such as the lungs, or the brain following dissemination of the Echinococcus multilocularis parasite via the blood and lymphatic system. If left untreated, alveolar echinococcosis is progressive and fatal with mortality rates ranging between 50% and 75%.
Ultrasound imaging is the technique of choice for the diagnosis of both cystic echinococcosis and alveolar echinococcosis in humans 17. Ultrasound imaging technique is usually complemented or validated by computed tomography (CT) and/or magnetic resonance imaging (MRI) scans. Echinococcus cysts can also be incidentally discovered by x-ray.
Specific antibodies are detected by different serological tests and can support the diagnosis. Indirect hemagglutination (IHA), indirect fluorescent antibody (IFA) tests, and enzyme immunoassays (EIA) are sensitive tests for detecting antibodies in serum of patients with cystic echinococcosis (Echinococcus granulosus); sensitivity rates vary from 60% to 90%, depending on the characteristics of the cases and antigens used. At present, the best available serologic diagnosis is obtained by using combinations of tests. Enzyme immunoassays (EIA) or indirect hemagglutination (IHA) can be used for screening; positive reactions should be confirmed by immunoblot assay. As some tests may cross-react with sera from persons with cysticercosis, clinical and epidemiological information should also be used to support diagnosis. A commercial enzyme immunoassays (EIA) kit is available in the United States.
Most patients with alveolar echinococcosis (Echinococcus multilocularis) have detectable antibodies. Immunoaffinity-purified Echinococcus multilocularis antigens (Em2) used in enzyme immunoassays (EIA) allow the detection of positive antibody reactions in more than 95% of alveolar echinococcosis. Comparing serologic reactivity to Em2 antigen with that to antigens containing components of both Echinococcus multilocularis and Echinococcus granulosus permits discrimination of patients with alveolar echinococcosis from those with cystic echinococcosis. Combining two purified Echinococcus multilocularis antigens (Em2 and recombinant antigen II/3-10) in a single immunoassay improves sensitivity and specificity. These antigens are included in commercial EIA kit in Europe, but are not available in the United States. Em2 tests are more useful for postoperative follow-up than for monitoring the effectiveness of chemotherapy. Em18-ELISA is considered suitable for monitoring treatment efficacy in alveolar echinococcosis patients.
The serologic diagnosis of polycystic echinococcosis has not been extensively studied as infections with Echinococcus vogeli are very rare. One antigen has been described (Ev2) that distinguishes Echinococcus vogeli from Echinococcus granulosus but not Echinococcus multilocularis.
In seronegative patients with liver image findings compatible with echinococcosis, ultrasound guided fine needle biopsy may be useful for confirmation of diagnosis 17. During a ultrasound guided fine needle biopsy procedure, precautions must be taken to control allergic reactions or prevent secondary recurrence in the event of leakage of hydatid fluid or protoscolices.
Echinococcosis treatment in humans is complicated because the Echinococcus cysts and the disease progress in differing ways depending on the Echinococcus species, and location. For cystic echinococcosis (Echinococcus granulosus), treatment options include: (i) anti-parasitic drug treatment (albendazole or mebendazole); (ii) cyst puncture, and PAIR (Puncture, Aspiration, Injection, Re-aspiration) technique, standard catheterization or the modified catheterization technique; (iii) surgery; and (iv) the “watch and wait” approach.
Alveolar echinococcosis (Echinococcus multilocularis) requires antiparasitic drug with or without surgery; radical surgery is the preferred approach in suitable cases, although removal of the entire parasite mass is not always possible. Effective treatment involves benzimidazoles administered continuously for at least two years and patient monitoring for 10 years or more since recurrence is possible. This has inhibited progression of alveolar echinococcosis and reduced lesion size in approximately half of treated cases. Intermittent treatment with albendazole is not recommended.
Hydatid disease key facts
- Human echinococcosis is a parasitic disease caused by tapeworms of the genus Echinococcus.
- The two most important forms of the disease in humans are cystic echinococcosis (hydatidosis) and alveolar echinococcosis.
- Humans are infected through ingestion of parasite eggs in contaminated food, water or soil, or after direct contact with animal hosts.
- Echinococcosis is often expensive and complicated to treat, and may require extensive surgery and/or prolonged drug therapy.
- Prevention programmes focus on deworming of dogs, which are the definitive hosts. In the case of cystic echinococcosis, control measures also include, slaughterhouse hygiene, and public education campaigns. Vaccination of lambs is also being used as an additional intervention.
- More than 1 million people are affected with echinococcosis at any one time.
Figure 1. Echinococcus granulosus adult worm
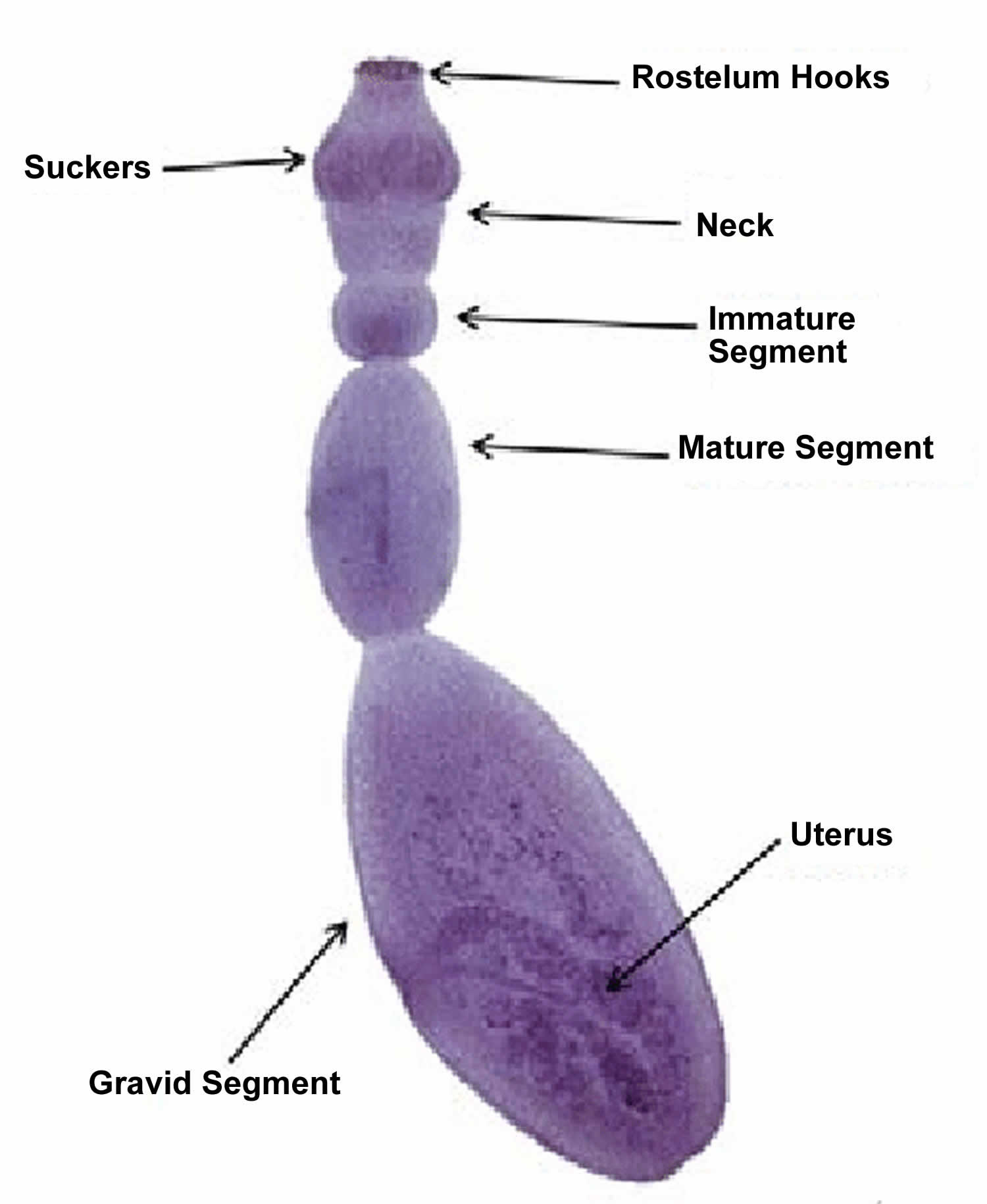
Footnotes: As dogs and other canids (animals from the dog family) are the only definitive hosts for most Echinococcus tapeworms, adult Echinococcus worms are not expected to be found in the human host. Humans are only infected by the Echinococcus larvae after ingestion of eggs from food, water or fomites contaminated with dog feces. Upon ingestion of the Echinococcus eggs by the human host, the oncospheres migrate from the intestinal lumen to other body sites where they develop into hydatid cysts. These cysts can be found in any part of the body, but are most common in the liver, lung and central nervous system (see Echincoccoosis Life Cycle below). Adult Echinococcus tapeworms range from 1.2 to 9 mm in length (depending on Echinococcus species) and usually consist of a sucker (head) and usually no more than six proglottids (segments). The terminal proglottid is gravid segment containing the uetrus and is longer than wide. The scolex (head) contains four cuplike oval suckers and a rostellum with 25 to 50 hooks. Large numbers of adult Echinococcus tapeworms may be found in the small intestines of dogs which are infected by eating the remnants of sheep, cattle or other animals containing hydatid cysts. The uterus in the gravid unit can hold up to 500 eggs, which are released into the feces through the ruptured segment. The subspherical egg is 34 to 41 micrometer in diameter, with a brown hexacanth embryo, and resembles those of other Taenia worms in appearance. Upon ingestion of eggs by the human host, the oncospheres migrate from the intestinal lumen to other body sites via circulation and develop into hydatid cysts. These cysts can be found in any part of the body, but are most common in the liver, lung and central nervous system (see Echincoccoosis Life Cycle below).
[Source 8 ]Figure 2. Echinococcus developmental stages
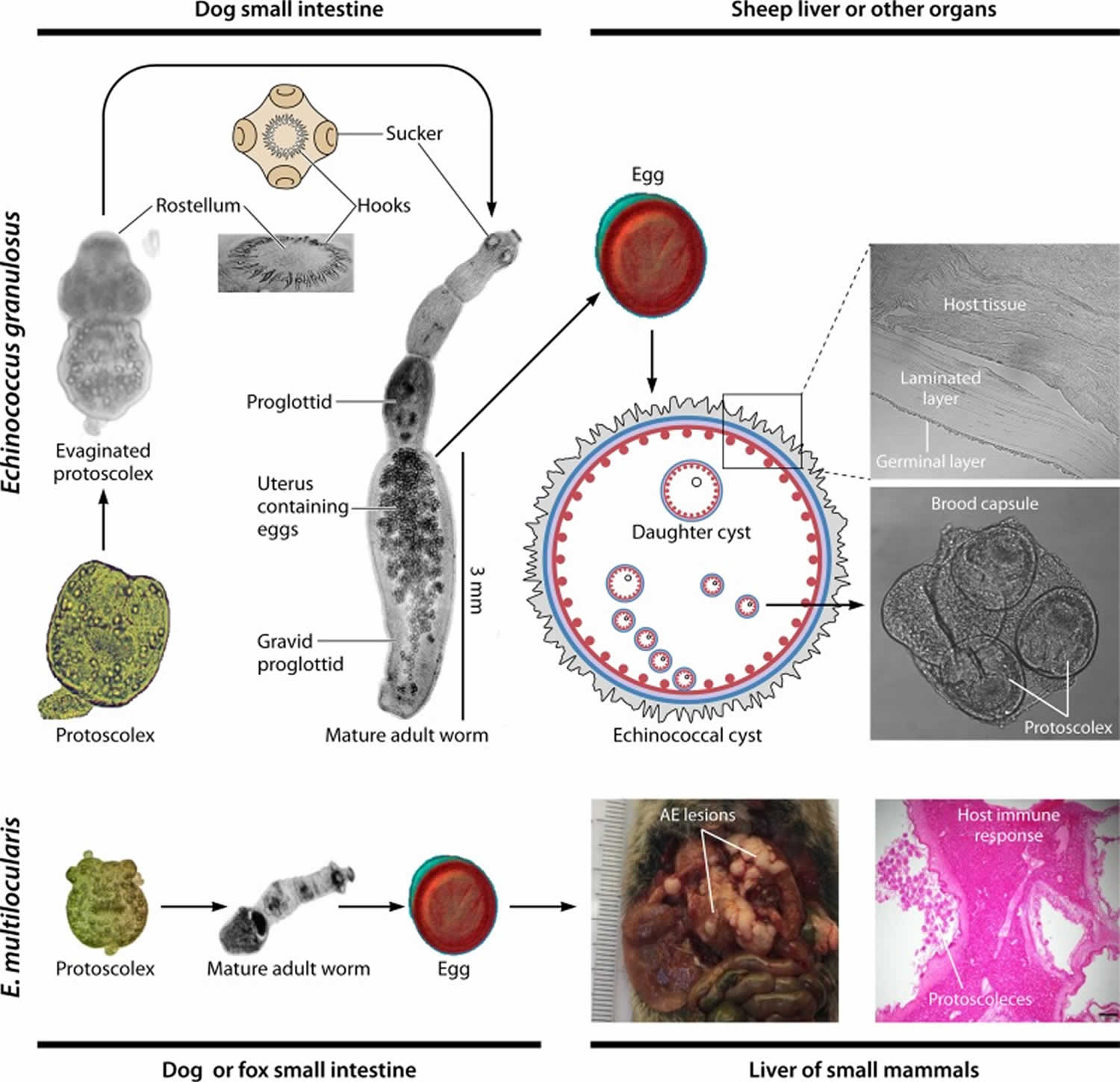
Footnotes: Different developmental stages in Echinococcus granulosus and Echinococcus multilocularis. Growth of the larval cyst is unlimited, and it can, for Echinococcus granulosus, grow to 30 cm or more in humans, while the adult worm, egg, and protoscolex are limited in size and shape. Echinococcus tapeworms have no gut, circulatory, or respiratory organs and have a highly adapted relationship with their mammalian hosts which they exploit for nutrients, signaling pathways, and neuroendocrine hormones. Strobilization is a notable feature of cestode biology, whereby proglottids (segments) bud distally from the anterior scolex, resulting in the production of tandem reproductive units (proglottids) exhibiting increasing degrees of development. Echinococcus is monoecious, and the last segment (gravid proglottid) produces diploid eggs that give rise to ovoid embryos, the oncospheres. However, a striking feature of the biology of Echinococcus is that the protoscolex has the potential to develop in either of two directions: it may develop into an adult tapeworm producing sexually produced eggs in the dog gut, or, if a hydatid cyst ruptures within the intermediate or human host, each released protoscolex is capable of differentiating asexually into a new cyst, a process termed “secondary echinococcosis”. While a unilocular fluid-filled bladder (cyst) is a feature of Echinococcus granulosus sensu lato in its larval stage, the metacestode of Echinococcus multilocularis consists of a mass of small, multilocular vesicles embedded in the immune reaction of the host (granuloma and fibrosis). These multiple and aggregated vesicles grow by proliferation of cells in the germinal layer of the metacestode.
[Source 5 ]Figure 3. Liver hydatid cyst
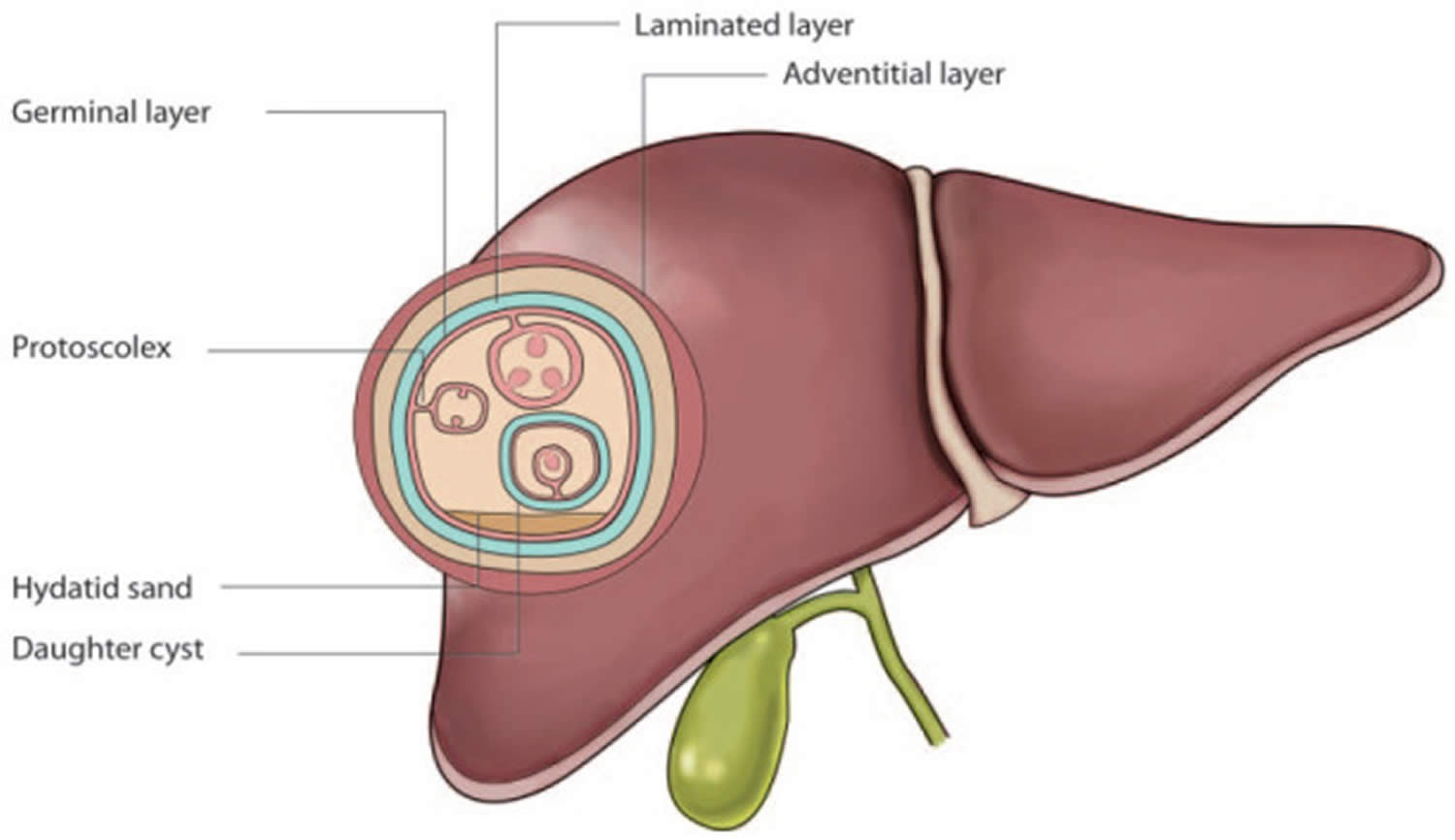
Footnotes: The hydatid cyst is characteristically a round cystic lesion that consists of an inner nucleated layer of the cyst (germinal layer) referred to as the endocyst, and an outer acellular layer of the cyst (laminated layer) referred to as the ectocyst. The inner germinal layer produces small vesicles called brood capsules that divide via asexual division and produce many protoscolices. Around the echinococcal laminated layer lies a granulomatous, adventitial layer known as the pericyst. This granulomatous layer is produced by the host’s immune system to wall off the cystic infection and is often seen in imaging studies. The protoscolex, the future head of the adult worm, is seen here budding from the germinal layer, and the daughter cyst is seen here floating within the main cyst. The hydatid sand is a sonographic finding representing a combination of cystic fluid and protoscolices.
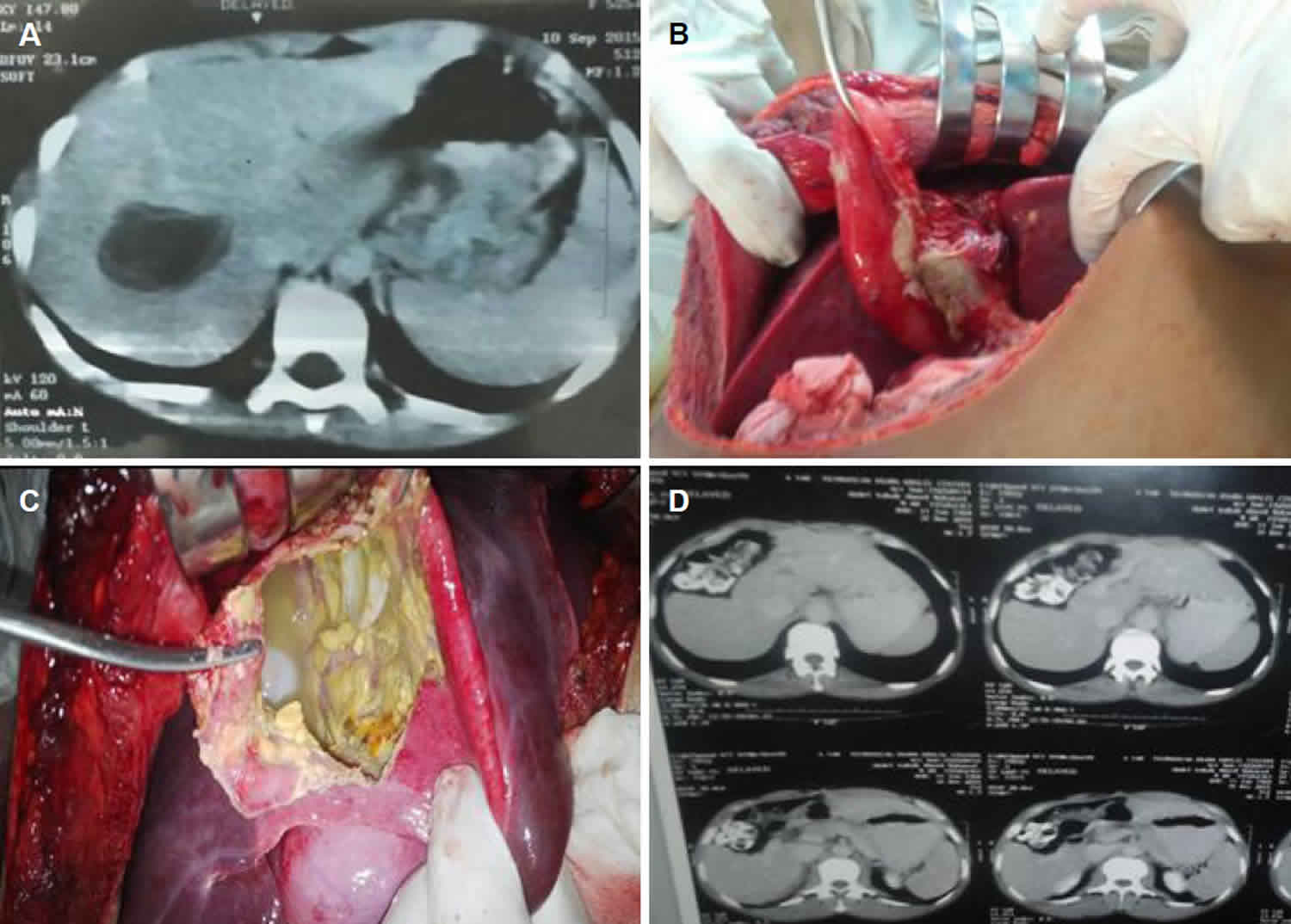
[Source 18 ]Figure 4. Alveolar echinococcosis
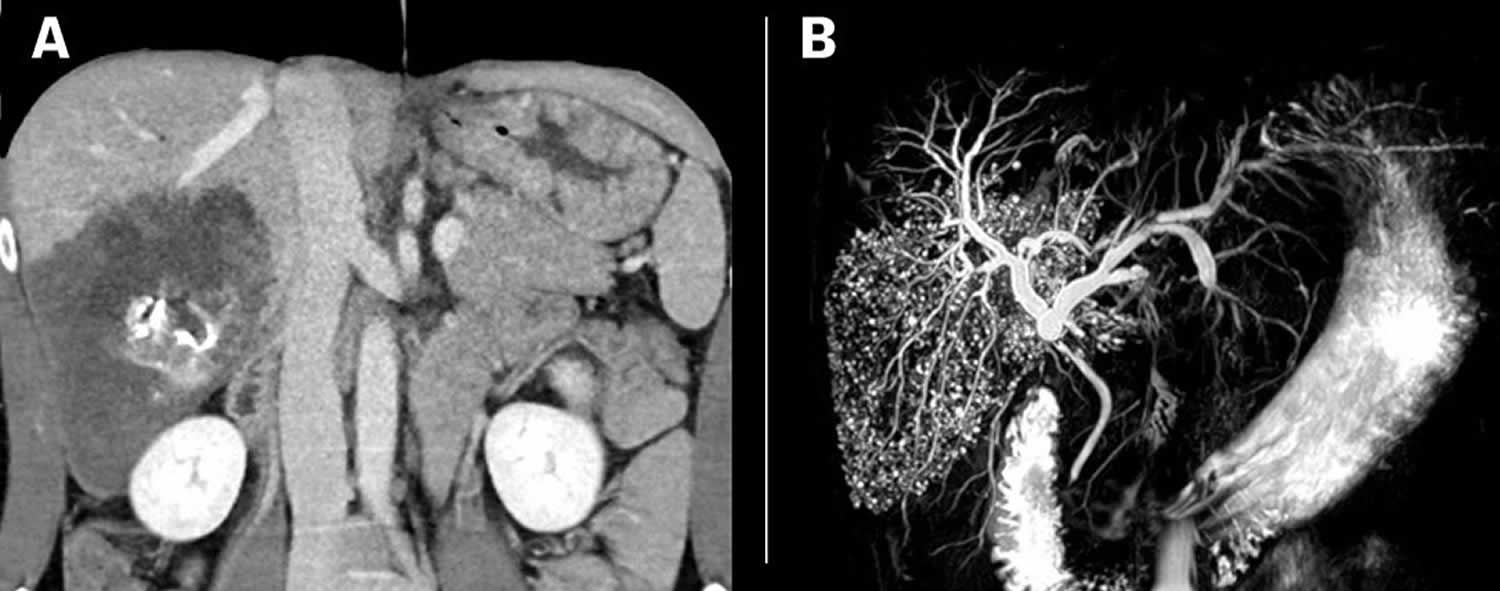
Footnotes: A man in his thirties from Eastern Europe, who had lived for several years in Norway, developed jaundice and pain below his right costal arch. (a) Patient with alveolar echinococcosis (patient 1). CT abdomen with contrast in venous phase with coronal reconstruction shows a 13 cm large irregular low attenuation lesion with central necrosis and calcification in liver segments 6 and 7. (b) MRCP sequence with coronal maximum intensity projection of liver segments 6 and 7 in the same patient shows innumerable small cysts in all involved liver segments. Serological testing detected antibodies to E. multilocularis, and treatment commenced with oral albendazole. He underwent surgery with extensive resection of the right liver. Macropathology confirmed a large, multilocular cyst (Figure 2), and histological examination showed cysts with laminated membranes, necrosis and fibrosis. Radical surgery was not technically possible, and there were residual lesions around the liver hilus and retroperitoneally. The patient is therefore expected to receive lifelong treatment with albendazole.
[Source 14 ]Figure 5. Pulmonary cystic echinococcosis
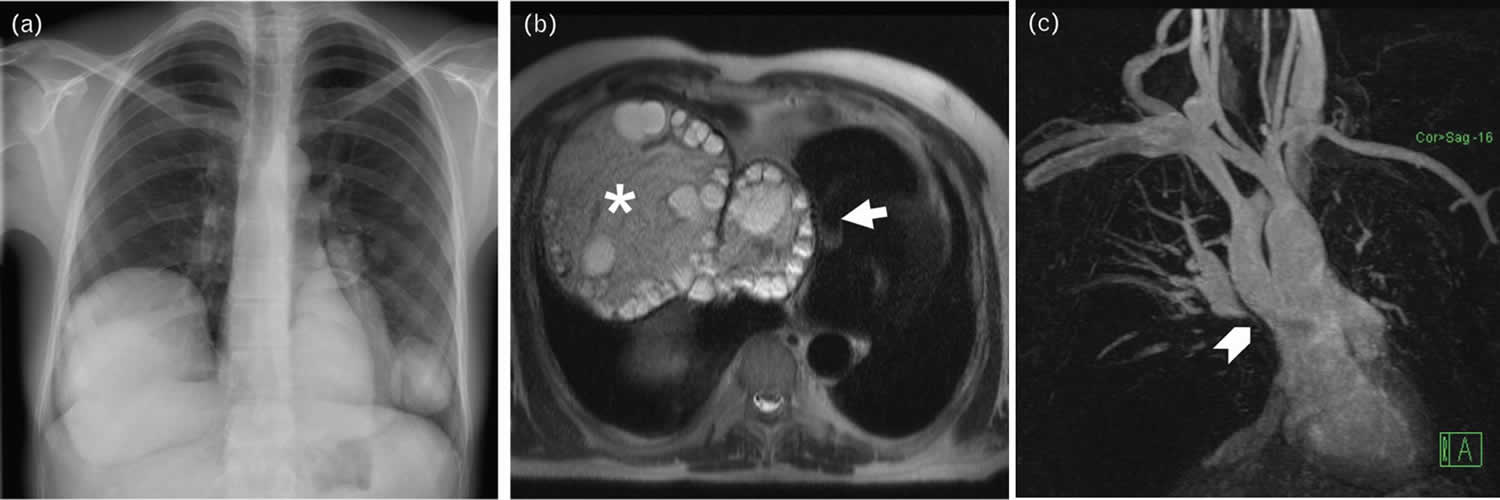
Footnotes: (a) Uncomplicated pulmonary cystic echinococcosis. The radiograph shows pulmonary cystic echinococcosis dissemination with multiple well defined masses in both lungs. As there is no evidence of intralesional air, uncomplicated unruptured cystic echinococcosis can be suggested to be present. (b and c) Pulmonary cystic echinococcosis with mass effect on heart and great vessels. T2-weighted MRI (b) shows a large CE3b cyst consisting of solid matrix and daughter cysts in the right hemithorax (asterisk) with severe compression of the heart (arrow). Magnetic resonance angiography (c) depicts severe compression, especially of the distal superior vena cava. Clinically, there was superior vena cava syndrome.
[Source 7 ]Figure 6. Lung and liver hydatid cyst
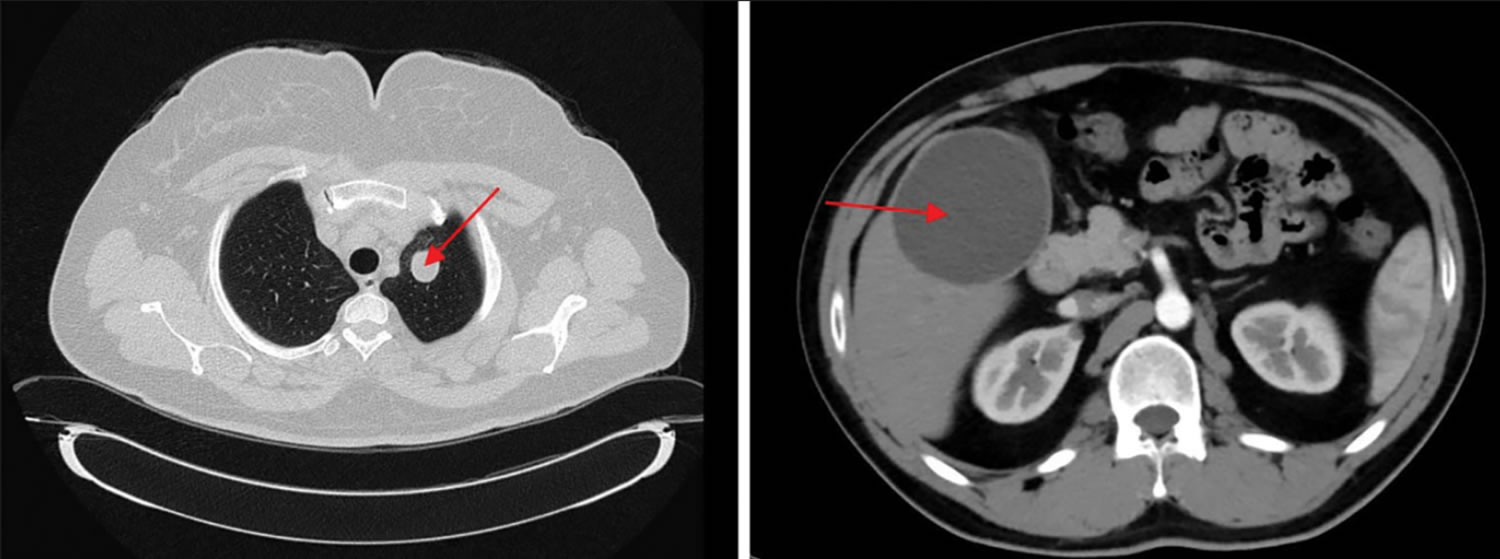
Footnotes: Cyst appearances on lung CT and abdominal CT in 2 different patients with positive Echinococcus Indirect hemagglutination (IHA).
[Source 19 ]How are dogs, cattle, sheep, and other domestic animals infected with Echinococcus?
Dogs serve as the definitive host for Echinococcus granulosus (cystic echinococcosis), and wild canids (animals from the dog family) are the main definitive hosts for Echinococcus multilocularis (alveolar echinococcosis). The definitive hosts carry adult tapeworms in their intestines (which are very small, 1.5 to 7mm long) without showing symptoms. They shed parasite eggs in feces.
For cystic echinococcosis (Echinococcus granulosus), livestock like sheep, cattle, goats, and pigs act as intermediate hosts. For alveolar echinococcosis (Echinococcus multilocularis), rodents act as intermediate hosts. Intermediate hosts get infected by ingesting Echinococcus eggs shed by the definitive hosts, from contaminated environments, which form cysts in their organs—primarily the liver and lungs. Definitive hosts get infected by eating those cysts when for example contaminated livers are fed to dogs, or when foxes eat infected rodents.
The cysts in livestock rarely cause clinical illness in animals, but infected organs (offal) are unsafe for consumption at slaughter, resulting in economic losses.
Is echinococcosis contagious and can it be transmitted from humans to humans?
Echinococcosis is zoonotic parasitic infection (parasite disease that is transmitted to humans from animals) and is not contagious between humans. The Echinococcus tapeworms requires an animal host, and human-to-human transmission is rare, except in cases like organ transplantation or accidental cyst fluid exposure during surgery (see Echinococcus Life Cycle below).
Hydatid cyst classification
Based on morphology the hydatid cyst can be classified into four different types 20:
- Type 1: simple cyst with no internal architecture
- Type 2: cyst with daughter cyst(s) and matrix
- Type 2a: round daughter cysts at periphery
- Type 2b: larger, irregularly shaped daughter cysts occupying almost the entire volume of the mother cyst
- Type 2c: oval masses with scattered calcifications and occasional daughter cysts
- Type 3: calcified cyst (dead cyst)
- Type 4: complicated cyst, e.g. ruptured cyst
World Health Organization (WHO) classification of hepatic hydatid cysts
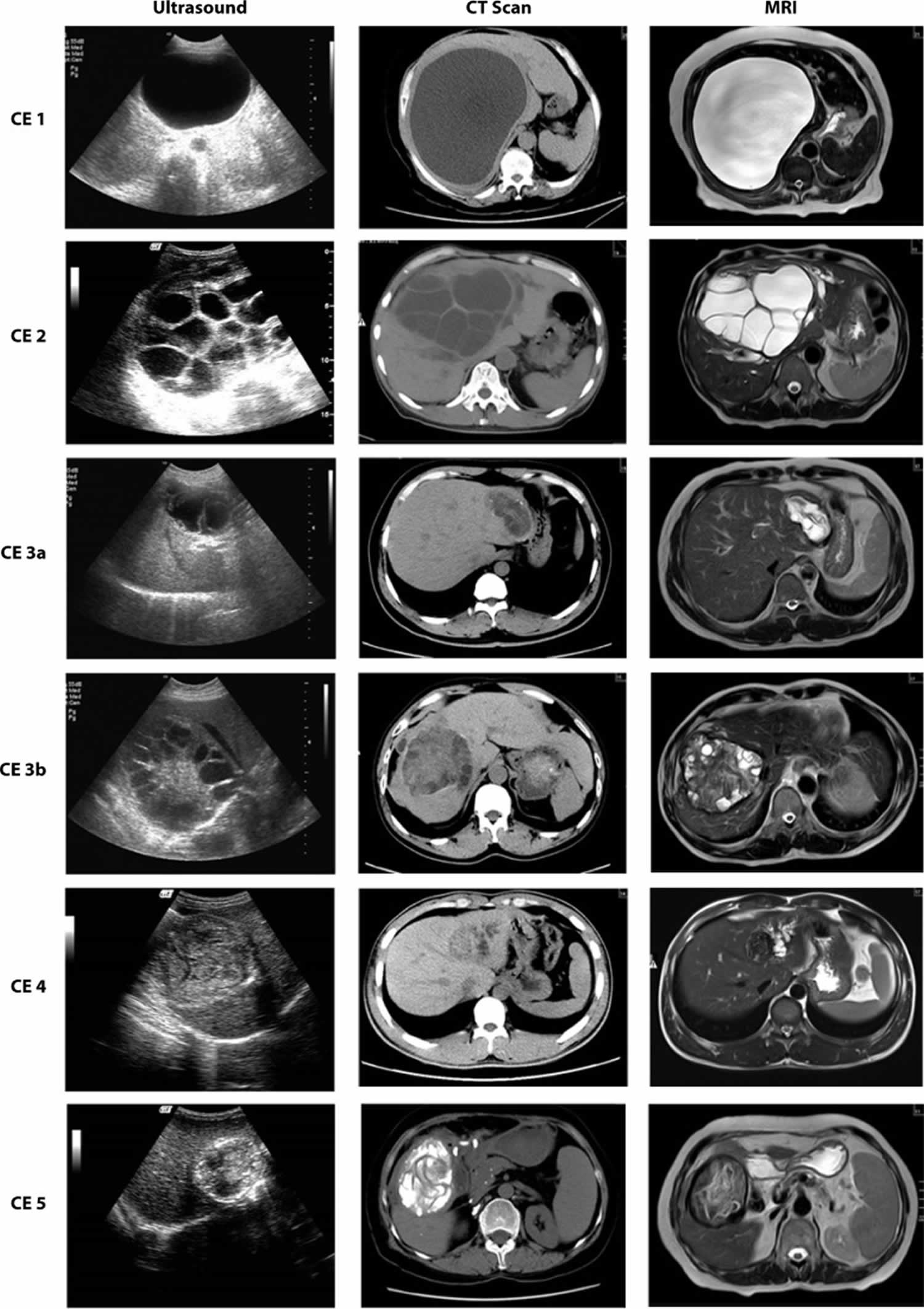
The 2001 World Health Organization (WHO) classification of hepatic hydatid cysts is used to assess the stage of hepatic hydatid cyst on ultrasound and is useful in deciding the appropriate management for it depending on the stage of the cyst 21. This classification was proposed by the WHO in 2001 remains the most widely used classification for hepatic hydatid cysts.
World Health Organization hepatic hydatid cyst classification 22:
CL: “Cystic Lesion” stage (undifferentiated).
- “Cystic Lesion” stage is not a cystic echinococcosis stage but indicates a cyst that could be a suspected young echinococcal cyst. Cystic Lesion (CL) is described as an unilocular cyst with anechoic content, without double wall sign, nor evident signs of non-parasitic aetiology (e.g. clear features of a biliary cyst). If serological and/or epidemiological criteria apply, this is a suspected cystic echinococcosis case. The etiological diagnosis of Cystic Lesion (CL) cysts (cystic echinococcosis or biliary cyst) necessitates further diagnostic steps 23, 24, 25.
Active cysts, likely to contain viable protoscoleces:
- CE1: Active, unilocular, liquid content.
- Well-defined univesicular cyst, with round or oval shape, anechoic content, posterior acoustic enhancement, with or without low intensity floating echoes upon decubitus change (moving “hydatid sand”) and with visible pathognomonic “double wall sign” consisting in the inner hyperechoic laminated layer and outer hypoechoic adventitial layer.
- CE2: Active, multivesicular, liquid content.
- Well-defined multivesicular cyst, with round or oval shape, posterior acoustic enhancement, one or more daughter cysts filling in part or completely the fluid-filled cyst; the pathognomonic “honeycomb” appearance is provided by the thin, regular, continuous and avascular clearly distinguishable adjacent walls of juxtaposed daughter cysts (giving a
septated appearance), without solid content.
- Well-defined multivesicular cyst, with round or oval shape, posterior acoustic enhancement, one or more daughter cysts filling in part or completely the fluid-filled cyst; the pathognomonic “honeycomb” appearance is provided by the thin, regular, continuous and avascular clearly distinguishable adjacent walls of juxtaposed daughter cysts (giving a
- CE3a: Transitional unilocular, liquid content with detached parasitic layers.
- Well-defined univesicular cyst with round or oval shape, posterior acoustic enhancement, and with partial or complete detachment of the laminated layer, visible as a hyperechoic thin and regular layer floating in the anechoic cyst content, giving a pathognomonic appearance, referred to as the “water lily sign”. The whole layer must be identified as a continuous hyperechogenic structure, in different views. Low-intensity floating echoes upon decubitus change (moving “hydatid sand”) may be present.
- CE3b: Active multivesicular cyst, with partially solid content with daughter cysts.
- Well-defined multivesicular cyst with round or oval shape, posterior acoustic enhancement, and heterogeneous structure, encompassing avascular solid components and hypoechoic folded structures deriving from degenerating layers and one or more round daughter cysts with anechoic content, giving the pathognomonic “Swiss cheese” appearance.
Inactive Stages:
- CE4: Solid content.
- Well-defined round or oval mass with or without posterior acoustic enhancement and with heterogeneous avascular solid content formed by the degenerated cyst layers, and hypoechoic folded structures deriving from degenerating layers in the mass and giving the pathognomonic “ball of wool” or “canalicular” or “cerebroid” appearance. Unlikely to contain viable protoscoleces.
- CE5: Solid content with eggshell calcified wall.
- Well-defined round or oval mass with posterior acoustic shadow deriving from a complete or nearly complete egg-shell calcified wall, and heterogeneous avascular solid content (when acoustic shadow allows visualization) formed by the degenerated cyst layers and hypoechoic folded structures deriving from degenerating layers in the mass and giving the pathognomonic “ball of wool” or” canalicular” appearance. Non-viable.
Note: All cystic echinococcosis cyst stages can show some wall calcification, so this feature, per se, does not indicate viability or non-viability of the cyst.
Stages CE1 and CE2 indicate active disease; stage CE3 indicates a transitional stage where the cyst has suffered a compromise, whereas CE4 and CE5 indicate inactive disease.
Radiography can be used to detect calcifications in up to 30% of cases. The calcifications are typically ring-like and can progress throughout all stages of the disease 26.
CT imaging is highly sensitive and serves a vital role in cases where ultrasonography is difficult (e.g., obese patients). It’s also crucial in the perioperative period, as it’s excellent at detecting complications, including cyst rupture, underlying infection, and biliary or vascular involvement 27.
Other modalities used for diagnosis include ultrasound-guided fine needle aspiration (in seronegative cases with inconclusive imaging) and endoscopic retrograde cholangiopancreatography (both diagnostic and therapeutic for cases affecting the biliary tree) 28.
Figure 7. World Health Organization echinococcosis ultrasound classification
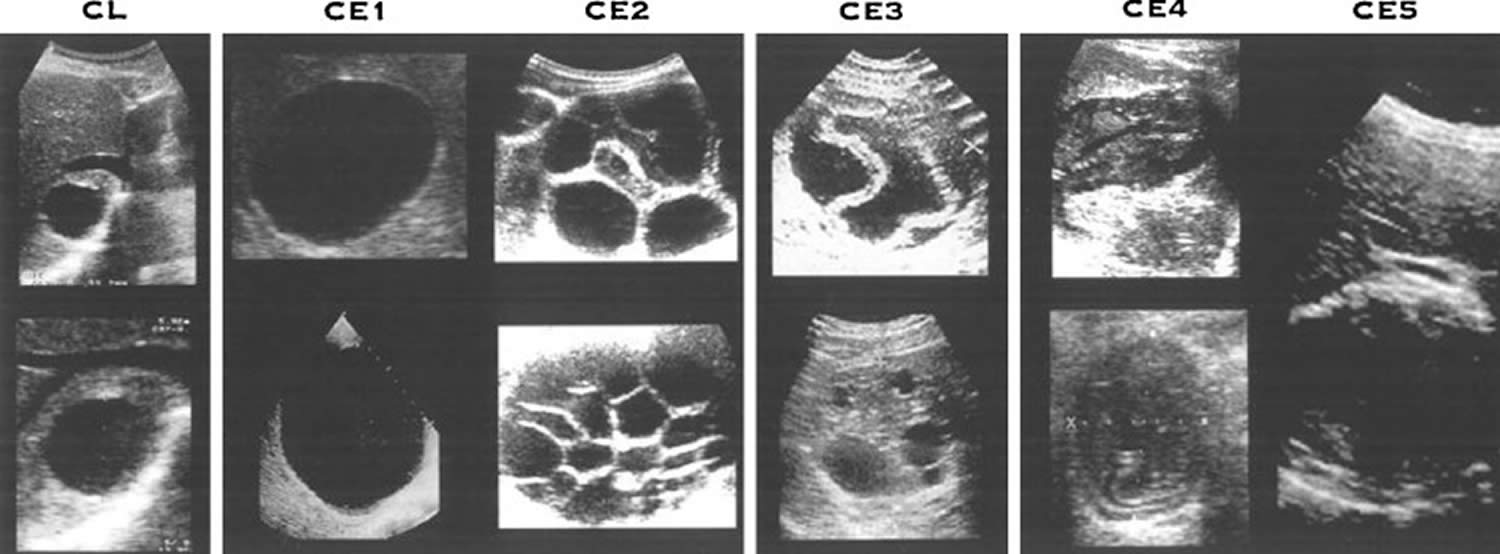
Figure 8. New Echinococcosis Imaging and Classification
Footnotes: New classification of ultrasound images and the associated classification of computed tomography (CT) images in alveolar echinococcosis have been proposed and are currently being tested on patients at European and Chinese centers in order to evaluate their usefulness for diagnosis and follow-up 29, 30.
[Source 5 ]Hydatid cyst disease causes
Humans become infected when they swallow the Echinococcus tapeworm eggs in contaminated food, shed in the feces of infected definitive hosts—primarily dogs for Echinococcus granulosus (cystic echinococcosis) or foxes/coyotes for Echinococcus multilocularis (alveolar echinococcosis). The Echinococcus eggs can be present on contaminated animals’ fur, soil, food, water, or other surfaces (e.g., unwashed vegetables, untreated water). The eggs then form cysts inside the body. A hydatid cyst is a closed pocket or pouch. The hydatid cysts keep growing, which leads to symptoms.
The three primary human echinococcosis types are cystic echinococcosis (Echinococcus granulosus), alveolar echinococcosis (Echinococcus multilocularis), and neotropical echinococcosis (Echinococcus vogeli and Echinococcus oligarthrus) 31. They are caused by different Echinococcus species, and differ on their geographical distribution, transmission cycles and clinical presentation.
- Echinococcus granulosus (sensu lato) is the cause of cystic echinococcosis or hydatid disease and is the type most frequently encountered. Echinococcus granulosus has a worldwide distribution, and the highest prevalence is observed in pastoral communities. It is the most common cause of echinococcosis in humans in which typically forms slow-growing fluid-filled cysts in the liver or lungs, causing symptoms like abdominal pain or cough.
- Echinococcus multilocularis causes alveolar echinococcosis. Echinococcus multilocularis is only present in the northern hemisphere but it’s becoming increasingly more common. It behaves aggressively, invading tissues like a malignant tumor, primarily in the liver and spreading to other organs, often leading to fatal liver failure if untreated.
- Neotropical echinococcosis is quite rare and includes two subtypes: Echinococcus vogeli which causes polycystic growths mainly in the liver and Echinococcus oligarthrus causes the extremely rare unicystic form, which has only been identified in very few human cases. Neotropical echinococcosis have only been reported in rural areas of the tropics in Central and South America. Since neotropical echinococcosis is so rare it is not well understood how long it can remain without symptoms.
Mitochondrial DNA sequencing has identified 10 distinct genotypes of Echinococcus granulosus (G1 to G10) that differ in their distribution, host range, and some morphological features; these are often grouped into separate species in modern literature 32, 33. The known zoonotic genotypes within the Echinococcus granulosus sensu lato complex include the “classical” Echinococcus granulosus sensu stricto (G1–G3 genotypes), Echinococcus ortleppi (G5), and the Echinococcus canadensis group (usually considered G6, G7, G8, and G10) 34, 35, 36, 5, 4. These include two sheep strains (G1 and G2), two bovid strains (G3 and G5), a horse strain (G4), a camelid strain (G6), a pig strain (G7), and a cervid strain (G8). A ninth genotype (G9) has been described in swine in Poland and a tenth strain (G10) in reindeer in Eurasia 36. The sheep strain (G1) is the worldwide form and is most commonly associated with human infections 32. Certain human activities (e.g. the widespread rural practice of feeding dogs the organs of home-butchered sheep) facilitate transmission of the sheep strain and consequently raise the risk that humans will become infected 33.
There are two hosts in the life-cycle of the Echinococcus granulosus tapeworm. The first one is the “primary host” or “definitive host” and the second one is the “intermediate host” in which the illness occurs. Adult Echinococcus granulosus tapeworms are present in the intestines of primary hosts including cats, dogs, wolfs and foxes, and they only cause intestinal parasitosis but not organ disease. Adult Echinococcus granulosus tapeworm lives approximately for 5 months in dog intestines 37, 38. “Definitive hosts” spread millions of Echinococcus granulosus eggs on defecation. Sheep and other herbivorous animals becomes “intermediate host” for the parasite when they eat herbs contaminated with these eggs, or humans become “intermediate host” for the Echinococcus granulosus tapeworm when they eat food contaminated with these eggs. Embryo (oncosphere) which comes out of the egg taken via gastrointestinal tract, adheres to intestinal wall with its hooks, then enters into circulation and reaches firstly to the liver. Therefore, liver is the most common site of disease in humans accounting for 50–70% of cases, followed by the lungs (20–30%), and less frequently the spleen, kidneys, heart, bones, central nervous system, and other organs 38. The Echinococcus granulosus tapeworm embryo loses its scolex (head) when it settles in an organ, and takes the cyst form consisting of cuticula (exocyst) and germinal membrane (endocyst). The cyst has sterile, clear fluid inside, and this cystic structure is wrapped with a fibrous capsule “pericyst”. When alive hydatid cysts are eaten by the last host dog, the infection chain is completed, and the life cycle returns to beginning 39, 40.
Cystic echinocccosis
Cystic echinocccosis also known as hydatid disease, hydatid cyst, hydatidosis or echinococcus cysticus is caused by infection with cyst-like Echinococcus granulosus tapeworm larvae, a 7 millimeter long tapeworm found in dogs (definitive host) and sheep, cattle, goats, and pigs (intermediate hosts). The incubation period of cystic echinococcosis (Echinococcus granulosus) is often prolonged for several years and most cases of cystic echinococcosis remain asymptomatic until the Echinococcus granulosus cysts reach a large enough size to cause dysfunction. Most primary Echinococcus granulosus infections in humans consist of a single cyst. The liver is the most common site of the hydatid cysts, followed by the lungs. Echinococcus granulosus cysts in the spleen, kidneys, heart, bone and central nervous system are less common. In secondary echinococcosis, Echinococcus granulosus larval tissue spreads from the primary site and new cysts develop after spontaneous or trauma-induced cyst rupture or after release of viable parasite material during invasive treatment procedures.
Although most infections in humans are asymptomatic, cystic echinococcosis causes harmful, slowly enlarging cysts in your liver, lungs, and other organs of your body that often grow unnoticed and neglected for years. Because the Echinococcus granulosus cysts are slow-growing, infection with cystic echinococcosis (Echinococcus granulosus) may not produce any symptoms for many years. Signs and symptoms may include liver enlargement with or without a palpable mass in the right upper quadrant, right epigastric pain, chest pain, coughing, nausea, and vomiting as a result of the growing cysts. Rupture or leakage of cyst fluid can lead to allergic reactions or even death.
You get cystic echinococcosis or hydatid disease by swallowing the eggs of the Echinococcus granulosus tapeworm. Dogs that eat home-slaughtered sheep and other livestock become infected with the tapeworm Echinococcus granulosus and the tapeworm eggs can be found in their stool. Direct contact with infected dogs, particularly intimate contact between children and their pet dogs, may lead to human infection. Ingestion of soil, water and vegetables contaminated with infected dog feces may also lead to Echinococcus granulosus infections. Echinococcus granulosus eggs can survive snow and freezing conditions.
People at highest risk of cystic echinococcosis (Echinococcus granulosus) include pastoral communities where livestock and dogs interact (dogs are the main definitive host), and those in areas with poor sanitation. Children are particularly vulnerable due to close contact with dogs and poor hygiene.
Humans can also be exposed to these Echinococcus granulosus tapeworm eggs by “hand-to-mouth” transfer or contamination.
- By ingesting food, water or soil contaminated with stool from infected dogs. This might include grass, herbs, greens, or berries gathered from fields.
- By petting or handling dogs infected with the Echinococcus granulosus tapeworm. These dogs may shed the tapeworm eggs in their stool, and their fur may be contaminated.
See your doctor if you think you may have cystic echinococcosis (hydatid disease). Cystic echinococcosis (Echinococcus granulosus) can be diagnosed with imaging studies such as X-rays or MRI scans, which are helpful to see the Echinococcus granulosus cysts in most of your organs. Blood tests are available to help diagnose an Echinococcus granulosus infection but may not always be accurate. If surgery is necessary, confirmation of the diagnosis can be made by the laboratory.
Alveolar echinococcosis
Alveolar echinococcosis also known as alveococcosis, echinococcus alveolaris, alveolar hydatid, alveolar hydatidosis, alveolar hydatid disease, multilocular hydatid cyst, multilocular hydatid disease or multilocular hydatidosis is caused by parasitic tapeworm infection with the larval stage of Echinococcus multilocularis, a 1 mm to 4 millimeter long tapeworm found in foxes, coyotes, and dogs (definitive hosts) 14. Small rodents are intermediate hosts for Echinococcus multilocularis. Although cases of alveolar echinococcosis in animals in endemic areas are relatively common, human cases are rare. Alveolar echinococcosis (Echinococcus multilocularis) poses a much greater health threat to humans than cystic echinococcosis (Echinococcus granulosus), causing parasitic tumors that can form in your liver, lungs, brain, and other organs. If left untreated, alveolar echinococcosis can be fatal. Because the Echinococcus multilocularis cysts are slow-growing, infection with alveolar echinococcosis may not produce any symptoms for many years. Pain or discomfort in your upper abdominal region, weakness, and weight loss may occur as a result of the growing cysts. Alveolar echinococcosis (Echinococcus multilocularis) symptoms may mimic those of liver cancer and cirrhosis of the liver.
People who accidentally swallow the eggs of the Echinococcus multilocularis tapeworm are at risk for alveolar echinococcosis (Echinococcus multilocularis) infection. People at high risk of alveolar echinococcosis (Echinococcus multilocularis) are people in contact with the definitive hosts (mainly wild carnivores, for example foxes, coyotes, wolves) such as hunters, trappers, veterinarians, or others who have contact with wild foxes, or coyotes, or their stool, or household dogs and cats that have the opportunity to eat wild rodents infected with alveolar echinococcosis (Echinococcus multilocularis).
Humans can be exposed to Echinococcus multilocularis eggs by “hand-to-mouth” transfer or contamination.
- By directly ingesting food items contaminated with stool from foxes or coyotes. This might include grass, herbs, greens, or berries gathered from fields.
- By petting or handling household dogs or cats infected with the Echinococcus multilocularis tapeworm. These pets may shed the tapeworm eggs in their stool, and their fur may be contaminated. Some dogs “scent roll” in foreign material (such as wild animal feces) and may become contaminated this way.
The primary infection of alveolar echinococcosis (Echinococcus multilocularis) is in your liver, usually the right lobe, but direct extension to nearby organs, as well as spread via blood to your lungs and brain is common. Alveolar echinococcosis (Echinococcus multilocularis) is inhibited by the host from completing its development and remains in the proliferative stage indefinitely. The larval mass resembles a cancer in appearance and behavior. In chronic alveolar hydatid infections, the lesion consists of a central necrotic cavity filled with a white amorphous material that is covered with a thin peripheral layer of dense fibrous tissue. Host tissue is directly invaded by extension of the budding and proliferating cyst wall, causing a pressure necrosis of surrounding host tissue. A vigorous inflammatory and fibrous tissue reaction usually surrounds the larval mass. Diagnosis is often delayed until an advanced and inoperable stage; mortality rates have traditionally been high, ranging between 50% and 75%.
See your doctor if you think you may have alveolar echinococcosis (Echinococcus multilocularis). Diagnosis of alveolar echinococcosis (Echinococcus multilocularis) can be made by a blood test that looks for the presence of antibodies to Echinococcus multilocularis.
Echinococcosis life cycle
Echinococcosis life cycle life cycle involves two animals. A carnivore is the definitive host – where the adult worms live in the intestines – and almost any mammal, including humans, can be the intermediate host – where the worms form cysts in various organs.
Echinococcosis also known as hydatid disease or hydatidosis is a parasitic tapeworm disease caused by the ingestion of Echinococcus tapeworm eggs in contaminated food, water or soil, or after direct contact with animal hosts, leading to the formation of larval cysts, primarily in your liver and lungs, that can cause symptoms after years 2, 3, 4, 5, 8, 9, 10. Echinococcosis is a zoonosis, a disease that is transmitted to humans from animals. Six species of Echinococcus tapeworms (family Taeniidae) have been identified which infect a wide range of domestic and wild animals, but four are of human health concern: Echinococcus granulosus (which causes cystic echinococcosis), Echinococcus multilocularis (which causes alveolar echinococcosis), and two forms of neotropical echinococcosis Echinococcus vogeli (which cause polycystic echinococcosis) and Echinococcus oligarthrus (which cause unicystic echinococcosis) 3, 10. Two new species have recently been identified: Echinococcus shiquicus in small mammals from the Tibetan plateau and Echinococcus felidis in African lions, but their zoonotic (animal to human) transmission potential is unknown 3. Several studies have shown that echinococcus infections are an increasing public health concern and that they can be regarded as emerging or re-emerging diseases.
The two most important forms of echinococcosis, which are of medical and public health relevance in humans, are cystic echinococcosis (Echinococcus granulosus) and alveolar echinococcosis (Echinococcus multilocularis) caused by larval stages (metacestode) of Echinococcus multilocularis and Echinococcus granulosus respectively 4. While cystic echinococcosis (Echinococcus granulosus) is worldwide, alveolar echinococcosis (Echinococcus multilocularis) is rarer and limited to the Northern hemisphere, but the latest epidemiological data indicate an increasing incidence 5, 15. Both alveolar echinococcosis (Echinococcus multilocularis) and cystic echinococcosis (Echinococcus granulosus) are caused by infection with Echinococcus tapeworms of the Taeniidae family which have different transmission cycles and different clinical presentations. However, both progress slowly in the liver, the usual primary infection site 5, 15.
Neotropical Echinococcosis (Echinococcus vogeli and Echinococcus oligarthrus) follow the same life cycle although with differences in hosts, morphology, and cyst structure. Adults of Echinococcus vogeli reach up to 5.6 mm long, and Echinococcus oligarthrus up to 2.9 mm. Neotropical Echinococcosis (Echinococcus vogeli and Echinococcus oligarthrus) cysts are generally similar to those found in cystic echinocccosis but are multi-chambered.
A number of herbivorous and omnivorous animals act as intermediate hosts of Echinococcus. They become infected by ingesting the Echinococcus eggs in contaminated food and water, and the parasite then develops into larval stages in the organs of definitive host (e.g., foxes, coyotes, and dogs). Carnivores act as definitive hosts for the parasite, and harbour the mature tapeworm in their intestine. The definitive hosts are infected through the consumption of organs of intermediate hosts (e.g., sheeps, cattle, goats, pigs and rodentts) that contain the parasite larvae.
Humans act as so-called accidental intermediate hosts in the sense that humans acquire infection in the same way as other intermediate hosts, but are not involved in transmitting the infection to the definitive host (e.g., foxes, coyotes, and dogs).
Several distinct genotypes of Echinococcus granulosus are recognized, some having distinct intermediate host preferences. Some genotypes are considered species distinct from Echinococcus granulosus. Not all Echinococcus granulosus genotypes cause infections in humans. The Echinococcus granulosus genotype causing the great majority of cystic echinococcosis infections in humans is principally maintained in a dog–sheep–dog cycle, yet several other domestic animals may also be involved, including goats, swine, cattle, camels and yaks.
Alveolar echinococcosis usually occurs in a wildlife cycle between foxes or other carnivores with small mammals (mostly rodents) acting as intermediate hosts. Domesticated dogs and cats can also act as definitive hosts.
Figure 9. Echinococcus life cycle
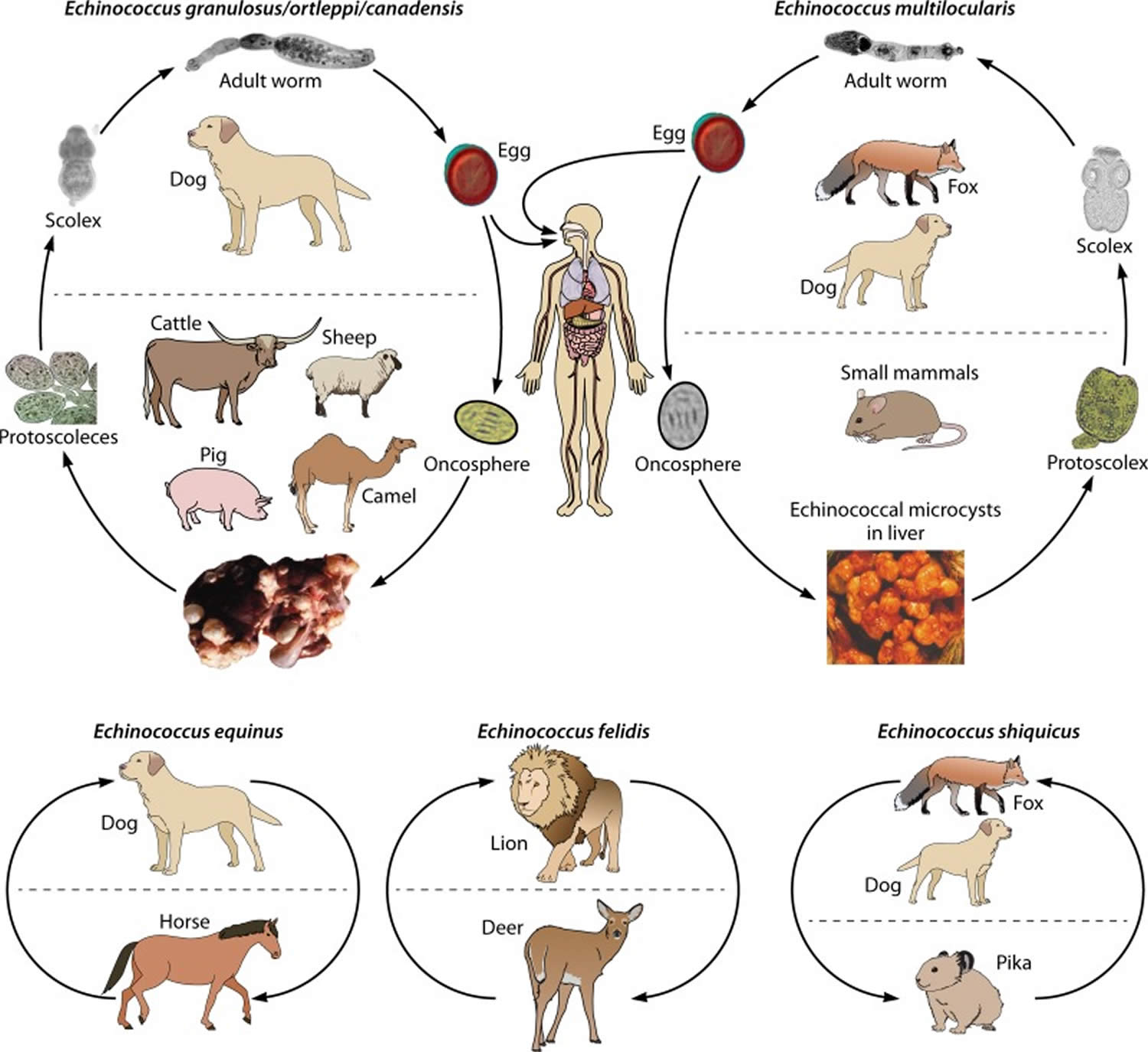
Footnotes: Life cycles of Echinococcus species. Species responsible for human infection (Echinococcus granulosus sensu stricto, Echinococcus ortleppi, and Echinococcus canadensis [belonging to Echinococcus granulosus sensu lato] and Echinococcus multilocularis) are shown at the top. Species at the bottom (Echinococcus shiquicus, a species close to Echinococcus multilocularis, and Echinococcus equinus and Echinococcus felidis, belonging to Echinococcus granulosus sensu lato) are not known to cause disease in humans. Only the most common definitive and intermediate hosts which play a major role in life cycle/transmission are shown; other hosts may be encountered (especially wildlife hosts for Echinococcus granulosus sensu lato and domestic hosts for Echinococcus multilocularis). Echinococcus vogeli and Echinococcus oligarthra, which are responsible for polycystic echinococcosis in humans in Central and South America, are not represented in the figure.
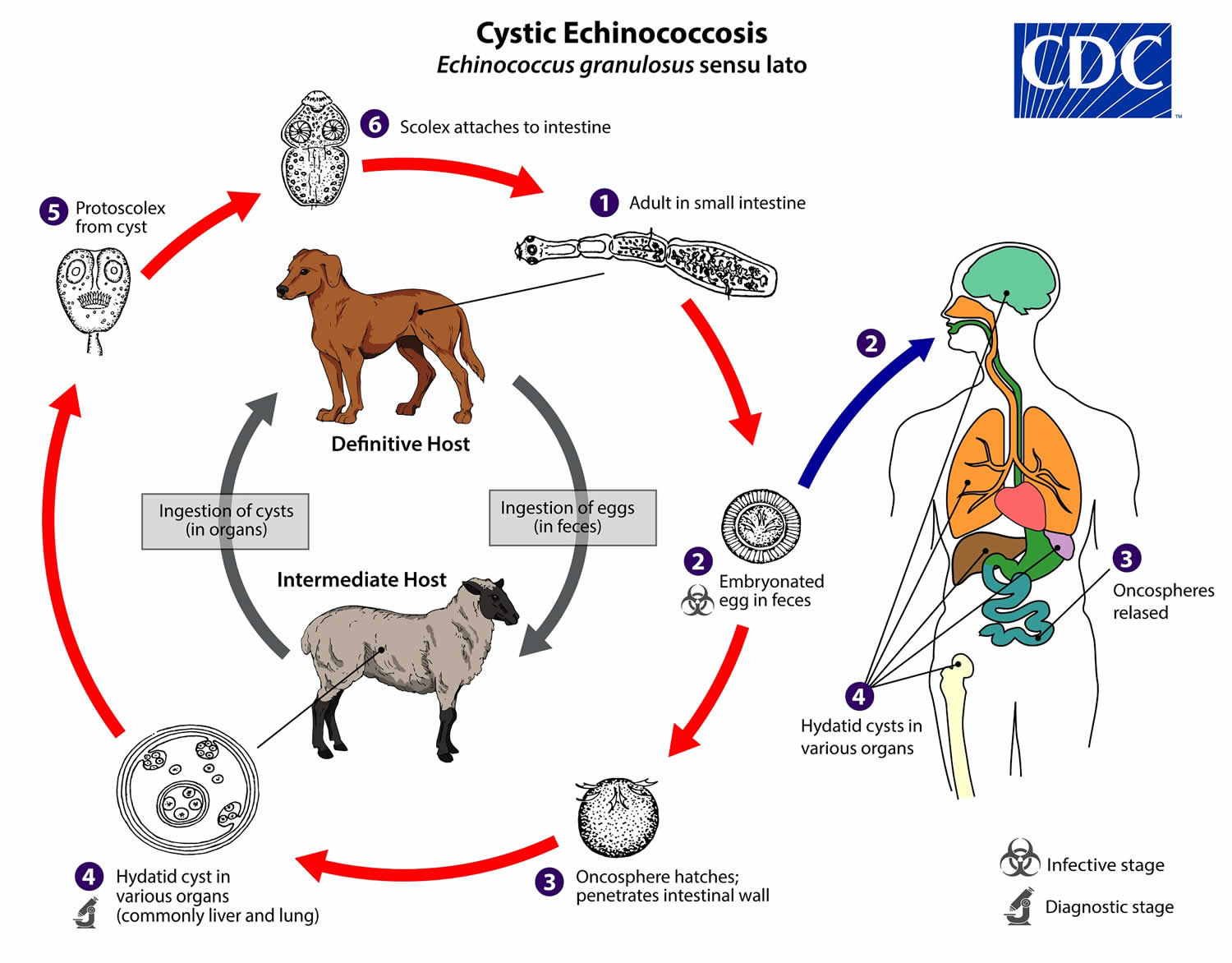
[Source 5 ]Cystic Echinococcosis Life Cycle
The adult Echinococcus granulosus sensu lato (2mm to 7 mm long) resides in the small intestine of the definitive host (dogs, wolves, jackals, domestic cats, and reindeer etc) (number 1). Gravid proglottids (each proglottid contains hundreds of eggs) release eggs (number 2) that are passed in the feces, and are immediately infectious. After ingestion by a suitable intermediate host (sheep, cattle, pigs and humans), eggs hatch in the small intestine and release six-hooked oncospheres (number 3) that penetrate the intestinal wall and migrate through the circulatory system into various organs, especially the liver and lungs. In these organs, the oncosphere develops into a thick-walled hydatid cyst (number 4) that enlarges gradually, producing protoscolices and daughter cysts that fill the cyst interior. The definitive host becomes infected by ingesting the cyst-containing organs of the infected intermediate host. After ingestion, the protoscolices (number 5) evaginate, attach to the intestinal mucosa (number 6), and develop into adult stages (number 1) in 32 to 80 days.
Humans are accidental intermediate hosts, and become infected by direct contact with a dog contaminated with egg-bearing feces or by ingesting water, food, or soil contaminated with egg-bearing feces (number 2). In human infection, the first stage is the asymptomatic incubation period, during which the ingested Echinococcus granulosus sensu lato eggs release oncospheres that are able to penetrate the human intestinal wall (number 3). These oncospheres enter the portal venous system, which provides access to the liver, lungs, and various other organs 41, 42, 43. Next, the oncospheres begin cyst development in a variety of organs (number 4). Cysts are usually unilocular, and can range anywhere from 1 cm to 15 cm in diameter. In hydatid disease, cyst growth ranges from 1–2 mm to 10 mm per year. They also tend to affect the right lobe of the liver more frequently than the left lobe of the liver due to the nature of portal blood flow. The cysts are composed of two layers of membrane: an inner, nucleated, germinal membrane, and an outer, acellular, laminated layer. The immune system responds to the cyst by forming a calcified fibrous capsule around it, which is the layer that is most often visualized on imaging studies 36. The cyst enlarges to form a combination of protoscolices and daughter cysts. The combination of many protoscolices and cystic fluid appears grain-like on ultrasound imaging, and is termed “hydatid sand” 36. If cysts rupture, the liberated protoscolices may create secondary cysts in other sites within the body (secondary echinococcosis). Animals that consume organs infected with protoscolices will become definitive hosts (number 5), as the protoscolices attach firmly to the host’s intestine (number 6), and then develop into an adult worm with a scolex (head), neck, and proglottids 44. Echinococcus granulosus infections usually present as solitary cysts, and have single-organ involvement. In 10–15% of patients, there can be involvement of two organs depending on the specific geographic region and strain of parasite 36.
Figure 10. Echinococcus granulosus life cycle
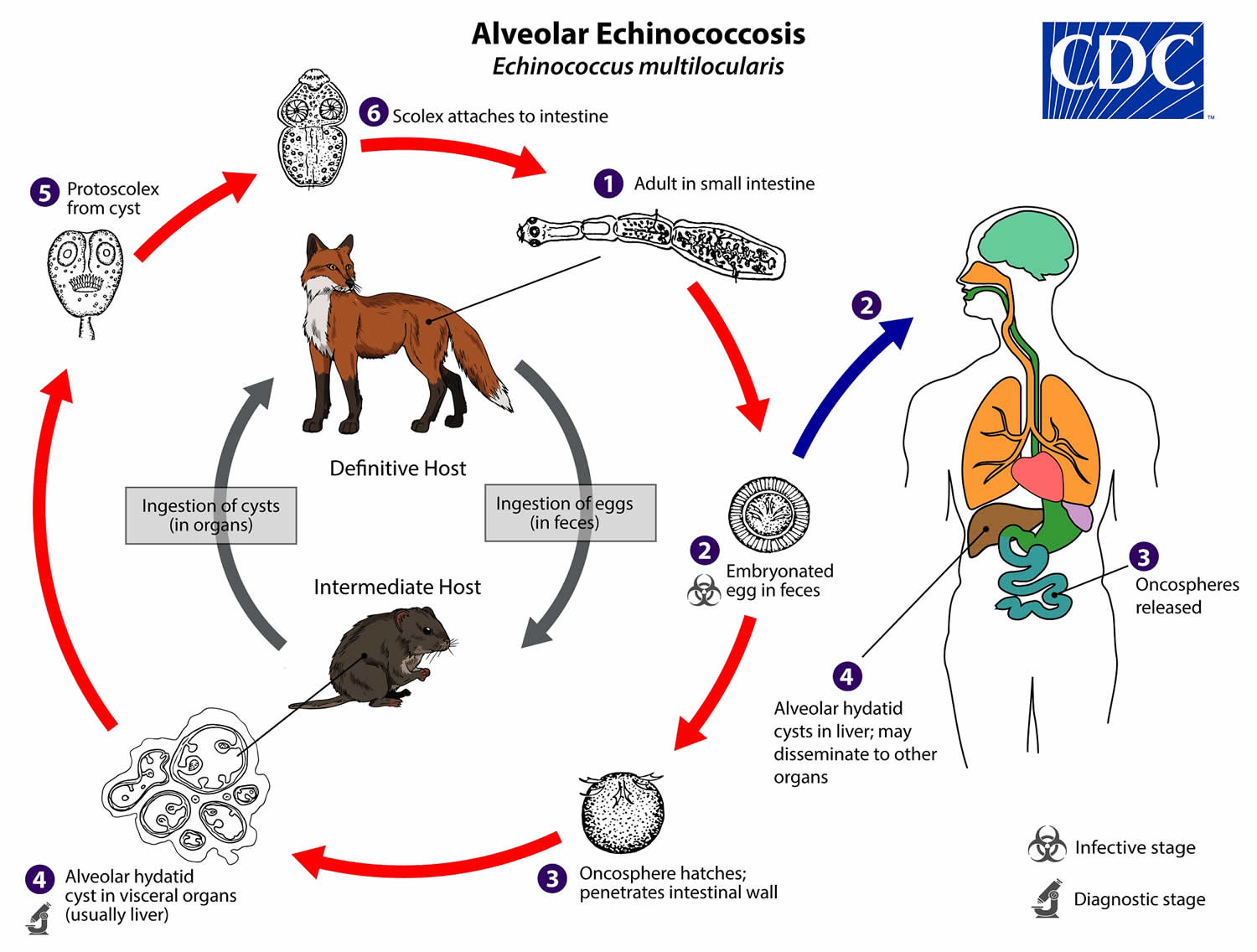
Alveolar echinococcosis life cycle
The adult Echinococcus multilocularis (1.2—4.5 mm long) (number 1) resides in the small intestine of the definitive host. Gravid proglottids release eggs (number 2) that are passed in the feces, and are immediately infectious. After ingestion by a suitable intermediate host, eggs hatch in the small intestine and releases a six-hooked oncosphere (number 3) that penetrates the intestinal wall and migrates through the circulatory system into various organs (primarily the liver for Echinococcus multilocularis). The oncosphere develops into a multi-chambered (“multilocular”), thin-walled (alveolar) hydatid cyst (number 4) that proliferates by successive outward budding. Numerous protoscolices develop within these cysts. The definitive host becomes infected by ingesting the cyst-containing organs of the infected intermediate host. After ingestion, the protoscolices (number 5) evaginate, attach to the intestinal mucosa (number 6), and develop into adult stages (number 1) in 32 to 80 days.
Humans are aberrant intermediate hosts, and become infected by ingesting eggs (number 2). Oncospheres (number 3) are released in the intestine and cysts develop within in the liver (number 4). Metastasis or dissemination to other organs (e.g., lungs, brain, heart, bone) may occur if protoscolices are released from cysts, sometimes called “secondary echinococcosis”.
Figure 11. Alveolar echinococcosis life cycle
Hydatid disease transmission
A number of herbivorous and omnivorous animals act as intermediate hosts of Echinococcus. They become infected by ingesting the parasite eggs in contaminated food and water, and the parasite then develops into larval stages in the viscera.
Carnivores act as definitive hosts for the parasite, and harbour the mature tapeworm in their intestine. The definitive hosts are infected through the consumption of viscera of intermediate hosts that contain the parasite larvae.
Humans act as so-called accidental intermediate hosts in the sense that they acquire infection in the same way as other intermediate hosts, but are not involved in transmitting the infection to the definitive host.
Several distinct genotypes of Echinococcus granulosus are recognised, some having distinct intermediate host preferences. Some genotypes are considered species distinct from Echinococcus granulosus. Not all genotypes cause infections in humans. The genotype causing the great majority of cystic echinococcosis infections in humans is principally maintained in a dog–sheep–dog cycle, yet several other domestic animals may also be involved, including goats, swine, cattle, camels and yaks.
Alveolar echinococcosis usually occurs in a wildlife cycle between foxes, other carnivores and small mammals (mostly rodents). Domesticated dogs and cats can also act as definitive hosts.
Hydatid cyst location
- Hepatic hydatid infection: most common organ, 76% of cases involve the liver 46
- Alveolar hydatid infection: second most common organ
- Splenic hydatid infection
- Central nervous system (brain and spinal cord) hydatid infection
- Spinal hydatid infection
- Retroperitoneal hydatid infection
- Renal hydatid infection
- Musculoskeletal hydatid infection.
Echinococcus geographic distribution
Echinococcosis is common in:
- Africa
- Central Asia
- Southern South America
- The Mediterranean
- The Middle East
In rare cases, the infection is seen in the United States. It has been reported in California, Arizona, New Mexico, and Utah.
Hydatid disease (Echinococcus granulosus sensu lato) occurs worldwide (except Antarctica) and more frequently in rural, grazing areas where dogs ingest organs from infected animals. The pattern of distribution for cystic echinococcosis has remained essentially unchanged over the past 2 decades, with areas of high endemicity, including western China, Central Asia, South America, Mediterranean countries and eastern Africa and the main risk factors being contact with dogs and raising livestock 47, 48, 49. However, studies in Africa have revealed a significant number of human cases and active transmission in animals, including wildlife, in countries up to now considered not to be areas of endemicity 50, 51. In endemic regions, human incidence rates for cystic echinococcosis (Echinococcus granulosus) can reach more than 50 per 100,000 person-years, and prevalence levels as high as 5% to 10% may occur in parts of Argentina, Peru, East Africa, Central Asia and China. Five thousand new cystic echinococcosis cases are still diagnosed annually in Argentina, Brazil, Chile, Peru, and Uruguay 52, 53. Thirty years of dosing dogs with the anthelmintic drug praziquantel 8 times annually has significantly decreased transmission to humans, but cystic echinococcosis is still present in a number of areas in South America 52, 54. In livestock, the prevalence of cystic echinococcosis (Echinococcus granulosus) found in slaughterhouses in hyperendemic areas of South America varies from 20% to 95% of slaughtered animals. The highest prevalence of cystic echinococcosis (Echinococcus granulosus) is found in rural areas where older animals are slaughtered. Depending on the infected species involved, livestock production losses attributable to cystic echinococcosis result from liver condemnation and may also involve reduction in carcass weight, decrease in hide value, decrease of milk production, and reduced fertility.
The geographic distribution of individual Echinococcus granulosus genotypes is variable and an area of ongoing research. The lack of accurate Echinococcus granulosus case reporting and genotyping currently prevents any precise mapping of the true epidemiologic picture. However, Echinococcus granulosus genotypes G1 and G3 (associated with sheep) are the most commonly reported at present and broadly distributed. In North America, Echinococcus granulosus is rarely reported in Canada and Alaska, and a few human cases have also been reported in Arizona and New Mexico in sheep-raising areas. In the United States, most infections are diagnosed in immigrants from counties where cystic echinococcosis (Echinococcus granulosus) is endemic. Some Echinococcus granulosus genotypes designated “Echinococcus canadensis” occur broadly across Eurasia, the Middle East, Africa, North and South America (G6, G7) while some others seem to have a northern holarctic distribution (G8, G10).
Hydatid disease has been declared eliminated from New Zealand, and Tasmania in Australia is considered to be provisionally free of the disease 55; nevertheless, Echinococcus granulosus is present on the Australian mainland and is still found in Tasmanian wild and rural dogs, but at low prevalence 56. In Western Europe and North America, most human cases are imported, although an indigenous cycle of various genotypes within the species group E. granulosus sensu lato is present. However, the lack of accurate case recording currently prevents any precise mapping of the true epidemiological picture; a European Registry of cystic echinococcosis (the Heracles project) has been launched to improve this situation 57.
Alveolar echinococcosis (Echinococcus multilocularis) is confined to the northern hemisphere, including central and northern Europe, Central Asia, regions of China, northern Russia, northern Japan, north-central United States, northwestern Alaska, and northwestern Canada. Alveolar echinococcosis has been a public health concern in northern Japan for the past 40 years 58, 59, 60. Mass screening with ultrasound and serology in China have confirmed a high incidence of alveolar echinococcosis on the Tibetan plateau (in Qinghai, Sichuan, and Tibet) and show that alveolar echinococcosis prevalence, especially in children, is higher than that of cystic echinococcosis in several areas 61, 62. Among the 18,235 estimated new alveolar echinococcosis cases per year globally, 91% occur in China 63, with human prevalence of >3% in some areas 64. Alveolar echinococcosis is also endemic in Central Asia, with high endemicity of both Echinococcus multilocularis and Echinococcus granulosus in Kazakhstan and Kyrgyzstan 65, 66, 67, 68. In Europe, the prevalence of Echinococcus multilocularis in definitive and intermediate hosts increased markedly within the first 15 years of this century, and the geographic distribution of fox infections is far broader than earlier reported; urban foxes may be involved in transmission 51, 55, 69, 70. Human cases have been found in European countries previously considered to be free of alveolar echinococcosis, and the situation in the Baltic region has become worrisome; in addition, alveolar echinococcosis incidence has doubled in the previously recognized areas of endemicity of France, Switzerland, Germany, and Austria 51, 71, 72, 73.
In regard to North America, the north-central United States, northwestern Alaska, and northwestern Canada have long been areas of Echinococcus multilocularis endemicity, but the parasite’s geographic range appears to be expanding due, at least in part, to increased and improved sampling efforts and the targeting of definitive hosts other than foxes (such as coyotes [Canis latrans]) 51. Alveolar echinococcosis had not been considered a mainstream human health issue in North America other than in Alaska until recently, and Echinococcus multilocularis has not been reported from Mexico or the southern United States 51. However, human cases were reported in Alberta, Canada as well as in Quebec and Manitoba (unpublished reports to a WHO Collaborating Centre) in the past decade 74. Molecular analysis of Echinococcus multilocularis in Alberta suggests that coyotes are important definitive hosts and that a European strain is involved, perhaps through carnivores imported from Europe, and not the local endemic “Alaskan” strains 75, 76. Only a single indigenous inhabitant case in the United States (Minnesota) has been confirmed.
The distribution of Neotropical Echinococcosis (Echinococcus vogeli and Echinococcus oligarthrus) remains limited to Central and South America 77; newly recognized human cases of Echinococcus vogeli infection in new areas, such as French Guyana in eastern South America 78, 79, are likely the result of improved diagnosis and molecular identification of the disease 80.
Figure 12. Echinococcosis Geographic Distribution
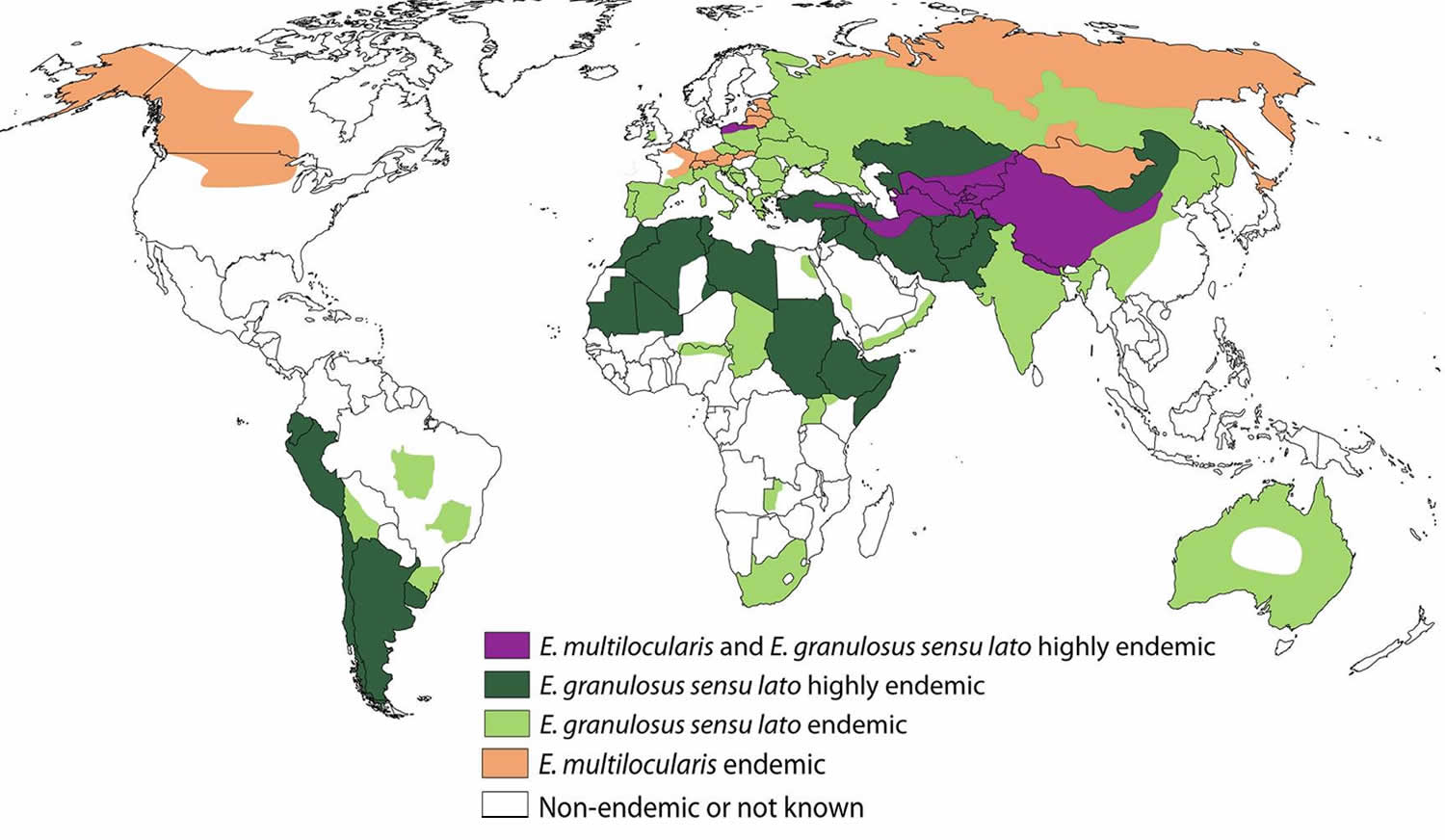
Footnotes: Global distribution of Echinococcus granulosus sensu lato responsible for cystic echinococcosis (CE), and Echinococcus multilocularis responsible for alveolar echinococcosis (AE). The map is based on recent epidemiological studies as far as the current situation has been studied in a given area 81, 51, 57, 82. The different colors represent a proxy for human prevalence and infection in animal hosts in a given area (to take indigenous human cases into account only). For alveolar echinococcosis (Echinococcus multilocularis), the represented disease density is based mainly on the presence of autochthonous alveolar echinococcosis cases in humans, Echinococcus multilocularis metacestodes in small mammals, and Echinococcus multilocularis adult worms in foxes and dogs. For cystic echinococcosis (Echinococcus granulosus sensu lato), the represented disease density is based mainly on the presence of indigenous human cases of cystic echinococcosis and of Echinococcus granulosus sensu lato metacestodes (irrespective of species or genotype) in intermediate hosts, including sheep, cattle, equids, and camels.
[Source 5 ]Echinococcus Hosts
Cystic echinococcosis (Echinococcus granulosus) definitive hosts are wild and domestic canids (animals from the dog family). Natural intermediate hosts depend on genotype. Intermediate hosts for zoonotic species/genotypes are usually ungulates, including sheep and goats (Echinococcus granulosus sensu stricto), cattle (“Echinococcus ortleppi”/G5), camels (“Echinococcus canadensis”/G6), and cervids (“Echinococcus canadensis”/G8, G10).
For alveolar echinococcosis (Echinococcus multilocularis), foxes, particularly red foxes (Vulpes vulpes), are the primary definitive host species. Other canids including domestic dogs, wolves, and raccoon dogs (Nyctereutes procyonoides) are also competent definitive hosts. Many rodents can serve as intermediate hosts, but members of the subfamily Arvicolinae (voles, lemmings, and related rodents) are the most typical.
The natural definitive host of Echinococcus vogeli is the bush dog (Speothos venaticus), and possibly domestic dogs. Pacas (Cuniculus paca) and agoutis (Dasyprocta spp.) are known intermediate hosts. Echinococcus oligarthrus uses wild neotropical felids (e.g. ocelots, puma, jaguarundi) as definitive hosts, and a broader variety of rodents and lagomorphs as intermediate hosts.
Risk factors for hydatid disease include being exposed to:
- Cattle
- Deer
- Feces of dogs, foxes, wolves, or coyotes
- Pigs
- Sheep
- Camels
Hydatid disease prevention
The main tools for prevention of echinococcosis transmission are the regular deworming of dogs with praziquantel (at least 4 times per year) and vaccination of sheep with the EG95 vaccine 83. Infected livestock organs should be disposed of safely and should not be fed to dogs or other canids.
Strategies for the prevention of infection in humans include proper sanitation and hygiene practices, emphasizing thorough handwashing after contact with dogs, with their faeces or with soil contaminated with the parasite’s eggs. In at-risk areas, it is important to wash vegetables that are eaten raw and to use safe water.
You can help prevent cystic echinococcosis (Echinococcus granulosus) by limiting areas where your dogs are allowed and don’t let your animals eat meat infected with Echinococcus granulosus cysts. To prevent alveolar echinococcosis (Echinococcus multilocularis), limit contact with wild animals like foxes, coyotes, and dogs, and limit your dog’s contact with rodents.
If you live in an area where Echinococcus granulosus (cystic echinococcosis) or hydatid disease is found in sheep or cattle, take the following precautions to avoid infection:
- Wash your hands with soap and warm water after handling dogs, and before handling food.
- Teach children the importance of washing hands to prevent infection.
- Do not consume any food or water that may have been contaminated by fecal matter from dogs. This might include grass, herbs, greens, or berries gathered from fields.
- Don’t allow your dogs to wander freely or to capture and eat raw meat from sheep, cattle, pigs, and goats.
- Control stray dog populations.
- Don’t home slaughter sheep and other livestock.
- Prevent dogs from feeding on the carcasses of infected sheep.
- If you think your pet may have eaten infected meat, consult your veterinarian about the possible need for preventive treatments.
Cystic echinococcosis / hydatid disease prevention
The main tools for prevention of hydatid disease or cystic echinococcosis (Echinococcus granulosus) transmission are the regular deworming of dogs with praziquantel (at least 4 times per year) and vaccination of sheep with the EG95 vaccine 83. Recent trials in Australia and Argentina using EG95 recombinant vaccine have reported that 86% of vaccinated sheep were completely free of viable hydatid cysts when examined 1 year after immunization. Vaccination reduced the number of viable cysts by 99.3% 84. A vaccine has also been developed against the dog tapeworm stage, which conferred 97–100% protection against worm growth and egg production 85.
Strategies for the prevention of Echinococcus granulosus infection in humans include proper sanitation and hygiene practices, emphasizing thorough handwashing after contact with dogs, with their feces or with soil contaminated with the parasite’s eggs. In at-risk areas, it is important to wash vegetables that are eaten raw and to use safe water. Infected livestock organs should be disposed of safely and should not be fed to dogs or other canids.
You can help prevent hydatid disease (Echinococcus granulosus) by limiting areas where your dogs are allowed and don’t let your animals eat meat infected with Echinococcus granulosus cysts.
If you live in an area where Echinococcus granulosus (cystic echinococcosis) or hydatid disease is found in sheep or cattle, take the following precautions to avoid infection:
- Wash your hands with soap and warm water after handling dogs, and before handling food.
- Teach children the importance of washing hands to prevent infection.
- Do not consume any food or water that may have been contaminated by fecal matter from dogs. This might include grass, herbs, greens, or berries gathered from fields.
- Don’t allow your dogs to wander freely or to capture and eat raw meat from sheep, cattle, pigs, and goats.
- Control stray dog populations.
- Don’t home slaughter sheep and other livestock.
- Prevent dogs from feeding on the carcasses of infected sheep.
- If you think your pet may have eaten infected meat, consult your veterinarian about the possible need for preventive treatments.
Alveolar echinococcosis
Alveolar echinococcosis (Echinococcus multilocularis) can be prevented by avoiding contact with wild animals such as foxes, coyotes, and dogs and their fecal matter and by limiting the interactions between dogs and rodent populations.
If you live in an area where Echinococcus multilocularis (alveolar echinococcosis) is found in rodents and wild canines, take the following precautions to avoid infection:
- Don’t touch a fox, coyote, stray dogs or other wild canine, dead or alive, unless you are wearing gloves. Hunters and trappers should use plastic gloves to avoid exposure.
- Don’t keep wild animals, especially wild canines, as pets or encourage them to come close to your home.
- Don’t allow your dogs and cats to wander freely or to capture and eat rodents.
- Do not allow dogs to feed on rodents and other wild animals.
- If you think that your pet may have eaten rodents, consult your veterinarian about possible preventive treatments.
- Wash your hands with soap and warm water after handling dogs or cats, and before handling food.
- Teach children the importance of washing hands to prevent infection.
- Do not collect or eat wild fruits or vegetables picked directly from the ground. All wild-picked foods should be washed carefully or cooked before eating.
Prevention and control of alveolar echinococcosisis more complex as the cycle involves wild animal species as both definitive and intermediate hosts. Regular deworming of domestic carnivores that have access to wild rodents should help to reduce the risk of infection in humans.
Deworming of wild and stray definitive hosts with anthelminthic baits resulted in significant reductions in alveolar echinococcosis prevalence in European and Japanese studies. Culling of foxes and unowned free-roaming dogs appears to be highly inefficient. The sustainability and cost–benefit effectiveness of such campaigns are controversial.
Hydatid disease symptoms
People with hydatid disease or cystic echinococcosis (Echinococcus granulosus) often remain asymptomatic for 10 years or more until the hydatid cysts containing the larval parasites grow large enough to cause discomfort, pain, nausea, and vomiting.
Hydatid disease or Echinococcus granulosus infections often remain asymptomatic for years before the cysts grow large enough to cause symptoms in the affected organs. The rate at which symptoms appear typically depends on the location of the cyst. The Echinococcus granulosus cysts are mainly found in your liver and lungs, but can also appear in your spleen, kidneys, heart, bone, and central nervous system, including your brain and eyes. Liver and lung signs/symptoms are the most common clinical manifestations, as these are the most common sites for cysts to develop. In addition to the liver and lungs, other organs (spleen, kidneys, heart, bone, and central nervous system, including the brain and eyes) can also be involved with resulting symptoms. Rupture of the cysts can produce a host reaction manifesting as fever, urticaria, eosinophilia, and potentially anaphylactic reactions, even death as a result of the release of cystic fluid. Rupture of the cyst may also lead to cyst dissemination.
As the hydatid disease advances and the hydatid cysts get larger, symptoms may include:
- Pain in the upper right part of the abdomen (liver cyst)
- Increase in size of the abdomen due to swelling (liver cyst)
- Bloody sputum (lung cyst)
- Chest pain (lung cyst)
- Cough (lung cyst)
- Severe allergic reaction (anaphylaxis) when cysts break open.
Echinococcus multilocularis or alveolar echinococcosis is characterized by slow growing, destructive parasitic tumor in your liver that may spread to other organs including your lungs and brain. In humans, the larval forms of Echinococcus multilocularis do not fully mature into cysts but cause vesicles that invade and destroy surrounding tissues and causing abdominal pain and biliary obstruction, weight loss, and malaise being the only manifestations evident in early infection. This may be misdiagnosed as liver cancer. Rarely, alveolar echinococcosis (Echinococcus multilocularis) can cause liver failure and death because of the spread into nearby tissues (e.g., lungs, spleen) and, rarely, your brain. Alveolar echinococcosis (Echinococcus multilocularis) is a dangerous disease that can result in a mortality rate of between 50% and 75%, especially because most affected people live in remote locations and have limited access to health care.
Echinococcus vogeli affects mainly the liver, where it acts as a slow growing tumor; secondary cystic development is common. Too few cases of E. oligarthrus have been reported for characterization of its clinical presentation.
Hydatid disease complications
Rupture of hydatid cyst may either be spontaneous or more usually after blunt trauma can cause site-specific complications. Cyst may rupture into the biliary system (leading to cholangitis with or without obstructive jaundice and marked eosinophilia), into the peritoneum (leading to anaphylaxis and/or peritoneal dissemination causing secondary hydatidosis) or into the pleura or lung (causing pleural hydatidosis, bronchial fistula, pneumonitis, pneumothorax, pleural effusion, and secondary pleuritis) 86, 87, 88, 89.
Hydatid cyst rupture can be of three types 90:
- Contained rupture – only endocyst is torn and cyst contents are confined within pericyst. The size of cyst does not decrease on imaging.
- Communicating rupture – there is tearing of endocyst and cyst contents escape via biliary radicals or bronchioles that have been incorporated in pericyst. On imaging, cyst becomes smaller with undulating membrane.
- Direct rupture – both endocyst and pericyst rupture causing spillage of contents into peritoneum or pleural space and dissemination of disease.
Hydatid cysts may become infected following bacteremia or via communicating bile ducts, especially when endoscopic retrograde cholangio-pancreatography (ERCP) has been performed. These patients present with high fever, sepsis syndrome and a tender liver. Pressure or mass effect on the bile ducts, portal veins, hepatic veins and inferior vena cava can cause cholestasis, portal hypertension and the Budd-Chiari Syndrome, respectively.
Rupture of echinococcosis cyst can induce an IgE-mediated hypersensitivity reaction in patients, presenting as hives, mucous membrane swelling, and flushing. The hypersensitivity reaction can be life-threatening 91.
Hydatid disease diagnosis
Your doctor will perform a physical exam and ask you about your symptoms.
If your health care provider suspects cystic echinococcosis or alveolar hydatid disease (alveolar echinococcosis), tests that may be done to find the cysts include:
- X-ray, echocardiogram, CT scan, PET scan, or ultrasound to view the cysts
- Blood tests, such as enzyme-linked immunoassay (ELISA), liver function tests
- Fine needle aspiration biopsy
Most often, echinococcosis cysts are found when an imaging test is done for another reason.
The diagnosis of echinococcosis varies depending on the infecting Echinococcus species. The primary infection of alveolar echinococcosis (Echinococcus multilocularis) is in the liver, usually the right lobe. The liver is the most common site of hydatid cysts, followed by the lungs, in patients with cystic echinococcosis (Echinococcus granulosus).
The diagnosis of echinococcosis relies mainly on findings by ultrasound imaging and/or other imaging techniques (magnetic resonance imaging [MRI] should be preferred to computed tomography [CT] due to better visualization of liquid areas within the matrix) supported by positive serologic tests 17, 92. Ultrasound surveys have shown that cysts may grow 1 mm to 50 mm per year or persist without changes for years. They may also spontaneously rupture or collapse or disappear 93, 94, 95, 96. The sequence of cyst changes during the natural history is still unclear 97. Liver cysts appear to grow at a lower rate than lung cysts 98. Clinical symptoms usually occur when the cyst compresses or ruptures into neighbouring structures.
In seronegative patients with liver image findings compatible with echinococcosis, ultrasound guided fine needle biopsy may be useful for confirmation of diagnosis 17. During a ultrasound guided fine needle biopsy procedure, precautions must be taken to control allergic reactions or prevent secondary recurrence in the event of leakage of hydatid fluid or protoscolices.
Serum liver enzyme tests have low sensitivities, and are frequently unreliable in determining the underlying severity of the infection. Moreover, liver enzyme tests are abnormal in only 40% of hydatid disease infected patients 36. When present, alkaline phosphatase (ALP) is commonly elevated, while aspartate/alanine transaminase ratio and bilirubin levels typically remain within the normal limits 36.
Possible versus probable versus confirmed cystic echinococcosis case
- Possible case. Any patient with a clinical or epidemiological history, and imaging findings or serology positive for cystic echinococcosis.
- Probable case. Any patient with the combination of clinical history, epidemiological history, imaging findings and serology positive for cystic echinococcosis on two tests.
- Confirmed case. The above, plus either (1) demonstration of protoscoleces or their components, using direct microscopy or molecular biology, in the cyst contents aspirated by percutaneous puncture or at surgery, or (2) changes in ultrasound appearance, e. g. detachment of the endocyst in a CE1 cyst, thus moving to a CE3a stage, or solidification of a CE2 or CE3b, thus changing to a CE4 stage, after administration of albendazole (at least 3 months) or spontaneous.
Figure 13. Hydatid cyst ultrasound
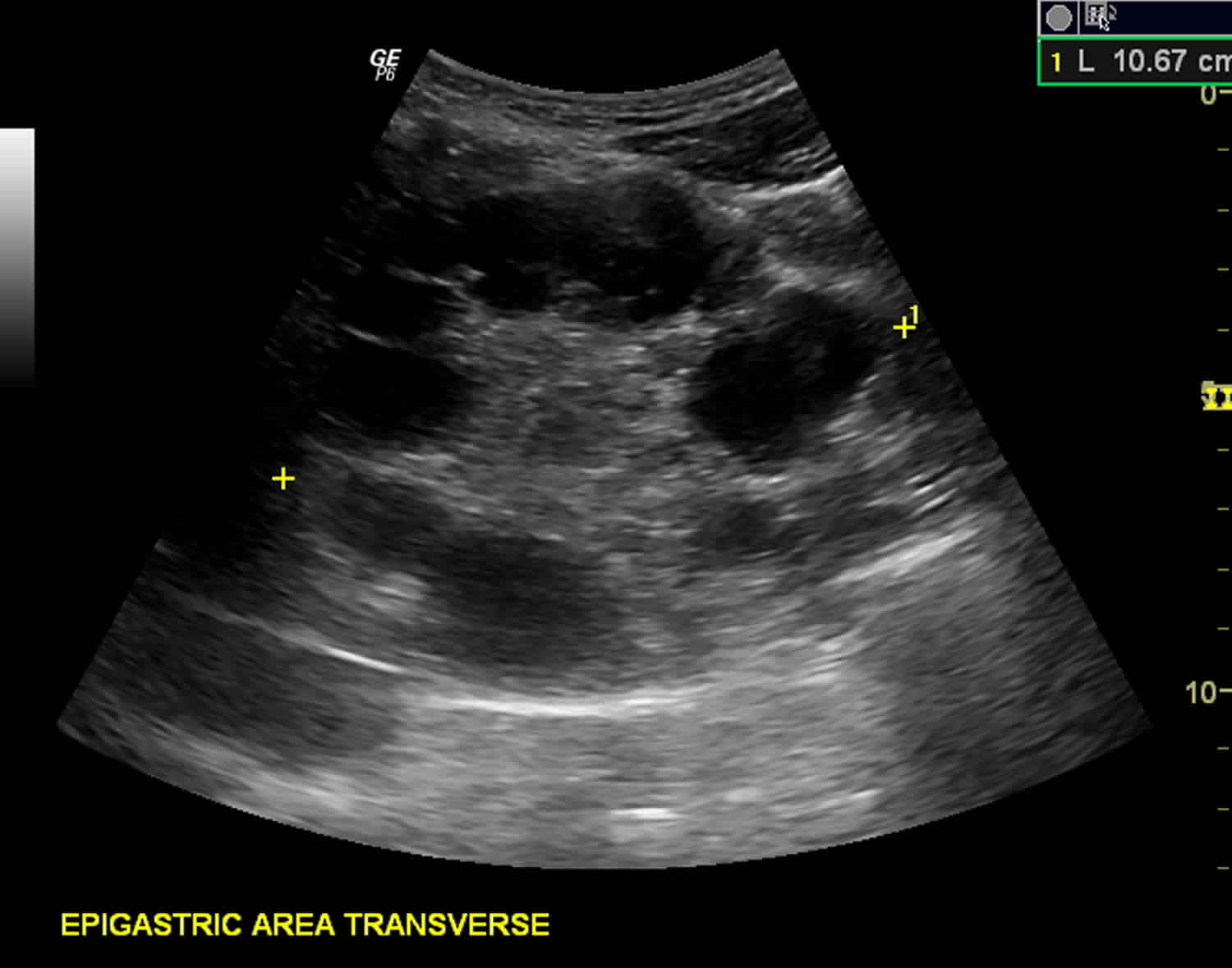
Footnote: Multiple hydatid cysts of variable sizes, sonographic appearance and stages seen in the liver, spleen, epigastric area (possibly retroperitoneal), pelvic cavity and anterior to the left psoas muscle (possibly retroperitoneal). Unilocular anechoic cyst (stage cystic lesion [CL]) according to WHO classification seen anterior to left psoas muscle at retroperitoneum. Unilocular mother cyst with honeycomb appearance (stage cystic echinococcosis [CE 2]) (according to WHO classification) seen in the pelvis, just cranially to the urinary bladder.
Cystic Echinococcosis diagnosis
The diagnosis of Echinococcus granulosus infection or cystic echinococcosis is suggested by identification of a cyst-like mass in a person with a history of exposure to sheepdogs in areas where the Echinococcus granulosus taperworm is endemic. Cystic echinococcosis (Echinococcus granulosus) must be differentiated from benign cysts, cavitary tuberculosis, mycoses, abscesses, and benign or malignant neoplasms. Noninvasive imaging techniques such as CT scans, MRI, and ultrasound imaging are all used for detecting and defining the extent and condition of avascular fluid-filled cysts in most organs. These techniques have proved valuable for diagnosis and preoperative evaluation by staging the condition of the lesion, the extent of the lesion in reference to other organs and vital structures, and identifying the presence of additional occult lesions. Radiography permits the detection of hydatid cysts in the lungs; however, in other organ sites, calcification is necessary for visualization. Ultrasonography has been widely used for screening, clinical diagnosis, and monitoring of treatment of liver and intra-abdominal cysts. Cyst viability cannot be reliably determined with radiography or parasite antigen detection; calcification can be present in all stages of cysts.
Serologic tests, such as enzyme-linked immunosorbent assay (ELISA) and indirect hemagglutination test, are highly sensitive methods for detecting infection. Specific confirmation can be obtained by demonstrating echinococcal antigens by immunodiffusion (arc 5) procedures or immunoblot assays (8-, 21 –kD bands).
Possible versus probable versus confirmed cystic echinococcosis case
- Possible case. Any patient with a clinical or epidemiological history, and imaging findings or serology positive for cystic echinococcosis.
- Probable case. Any patient with the combination of clinical history, epidemiological history, imaging findings and serology positive for cystic echinococcosis on two tests.
- Confirmed case. The above, plus either (1) demonstration of protoscoleces or their components, using direct microscopy or molecular biology, in the cyst contents aspirated by percutaneous puncture or at surgery, or (2) changes in ultrasound appearance, e. g. detachment of the endocyst in a CE1 cyst, thus moving to a CE3a stage, or solidification of a CE2 or CE3b, thus changing to a CE4 stage, after administration of albendazole (at least 3 months) or spontaneous.
Alveolar Echinococcosis diagnosis
Alveolar echinococcosis or Echinococcus multilocularis infection closely mimics liver cancer or cirrhosis and is more commonly diagnosed in people of an advanced age. Plain radiographs show hepatomegaly and characteristic scattered areas of radiolucency outlined by calcific rings 2 to 4 mm in diameter. The usual CT image of E. multilocularis infection is that of indistinct solid tumors with central necrotic areas and perinecrotic plaque-like calcifications. Serologic test results are usually positive at high titers. Comparing a patient’s titers with both purified-specific and shared antigens permits the serologic discrimination between patients infected with Echinococcus multilocularis and those infected with Echinococcus granulosus.
Antibody detection
Immunodiagnostic tests can be very helpful in the diagnosis of echinococcosis, particularly in conjunction with imaging, and should be used before invasive methods. However, the clinician must have some knowledge of the characteristics of the available tests and the patient and parasite factors in order to interpret assay results. False-positive reactions may occur in persons with other tapeworm (cestode) infections, some other helminth infections, cancer, and liver cirrhosis. Negative test results do not rule out echinococcosis because some cyst carriers do not have detectable antibodies. Whether the patient has detectable antibodies depends on the physical location, integrity, and vitality of the larval cyst.
Sensitivity of serum antibody detection using indirect hemagglutination, ELISA, or latex agglutination, with hydatid cyst fluid antigens, ranges between 85 and 98% for liver cysts, 50–60% for lung cysts and 90–100% for multiple organ cysts 99, 100, 101. Specificity of all tests is limited by cross-reactions due to other cestode infections (Echinococcus multilocularis and Taenia solium), some other helminth diseases, cancers, liver cirrhosis and presence of anti-P1 antibodies.
Confirmatory tests must be used (arc-5 test; Antigen B (AgB) 8 kDa/12 kDa subunits or EgAgB8/1 immunoblotting) in dubious cases 99, 100. Immunoblotting may be used as a first-line test and is best for differential diagnosis 102. Mass screening in populations at risk optimally deploys ultrasound and serology 103.
Detection of parasite-specific IgE or IgG4 has no significant diagnostic advantage. Both parasite-specific IgE or IgG4, as well as eosinophil count, are more elevated after rupture/leakage of cysts 104.
Cystic echinococcosis (Echinococcus granulosus)
Indirect hemagglutination (IHA), indirect fluorescent antibody (IFA) tests, and enzyme immunoassays (EIA) are sensitive tests for detecting antibodies in serum of patients with cystic echinococcosis (Echinococcus granulosus); sensitivity rates vary from 60% to 90%, depending on the characteristics of the cases and antigens used. At present, the best available serologic diagnosis is obtained by using combinations of tests. Enzyme immunoassays (EIA) or indirect hemagglutination (IHA) can be used for screening; positive reactions should be confirmed by immunoblot assay. As some tests may cross-react with sera from persons with cysticercosis, clinical and epidemiological information should also be used to support diagnosis. A commercial enzyme immunoassays (EIA) kit is available in the United States.
Alveolar echinococcosis (Echinococcus multilocularis)
Most patients with alveolar echinococcosis (Echinococcus multilocularis) have detectable antibodies. Immunoaffinity-purified Echinococcus multilocularis antigens (Em2) used in enzyme immunoassays (EIA) allow the detection of positive antibody reactions in more than 95% of alveolar echinococcosis. Comparing serologic reactivity to Em2 antigen with that to antigens containing components of both Echinococcus multilocularis and Echinococcus granulosus permits discrimination of patients with alveolar echinococcosis from those with cystic echinococcosis. Combining two purified Echinococcus multilocularis antigens (Em2 and recombinant antigen II/3-10) in a single immunoassay improves sensitivity and specificity. These antigens are included in commercial EIA kit in Europe, but are not available in the United States. Em2 tests are more useful for postoperative follow-up than for monitoring the effectiveness of chemotherapy. Em18-ELISA is considered suitable for monitoring treatment efficacy in alveolar echinococcosis patients.
Polycystic echinococcosis (Echinococcus vogeli)
The serologic diagnosis of polycystic echinococcosis has not been extensively studied as infections with Echinococcus vogeli are very rare. One antigen has been described (Ev2) that distinguishes Echinococcus vogeli from Echinococcus granulosus but not Echinococcus multilocularis.
Hydatid cyst differential diagnosis
Hydatid cyst can mimic a large number of conditions, depending on the site of the cyst.
Liver echinococcosis differential diagnoses include:
- Liver abscess
- Liver cysts
- Budd-Chiari syndrome
- Biliary colic
- Biliary cirrhosis
- Tuberculosis
- Primary hepatic carcinoma
A detailed history and physical exam, alongside proper workup including serology and imaging, is key in making the diagnosis and ruling out diseases that may mimic hydatidosis.
Hydatid cyst treatment
Echinococcosis treatment varies depending on the infecting Echinococcus species. Treatment options for cystic echinococcosis (Echinococcus granulosus) include antiparasitic drugs (albendazole or mebendazole), cyst puncture, and PAIR (Puncture, Aspiration, Injection of protoscolecide, Reaspiration). In some cases, no treatment but a conservative “watch and wait” approach is best.
Alveolar echinococcosis (Echinococcus multilocularis) requires antiparasitic drug with or without surgery.
There are 4 options for the treatment of cystic echinococcosis (Echinococcus granulosus):
- Percutaneous treatment of the hydatid cysts with the PAIR (Puncture, Aspiration, Injection, Re-aspiration) technique;
- Surgery
- Anti-parasitic drug treatment
- “Watch and wait”.
Figure 14. Liver hydatid disease surgical approaches
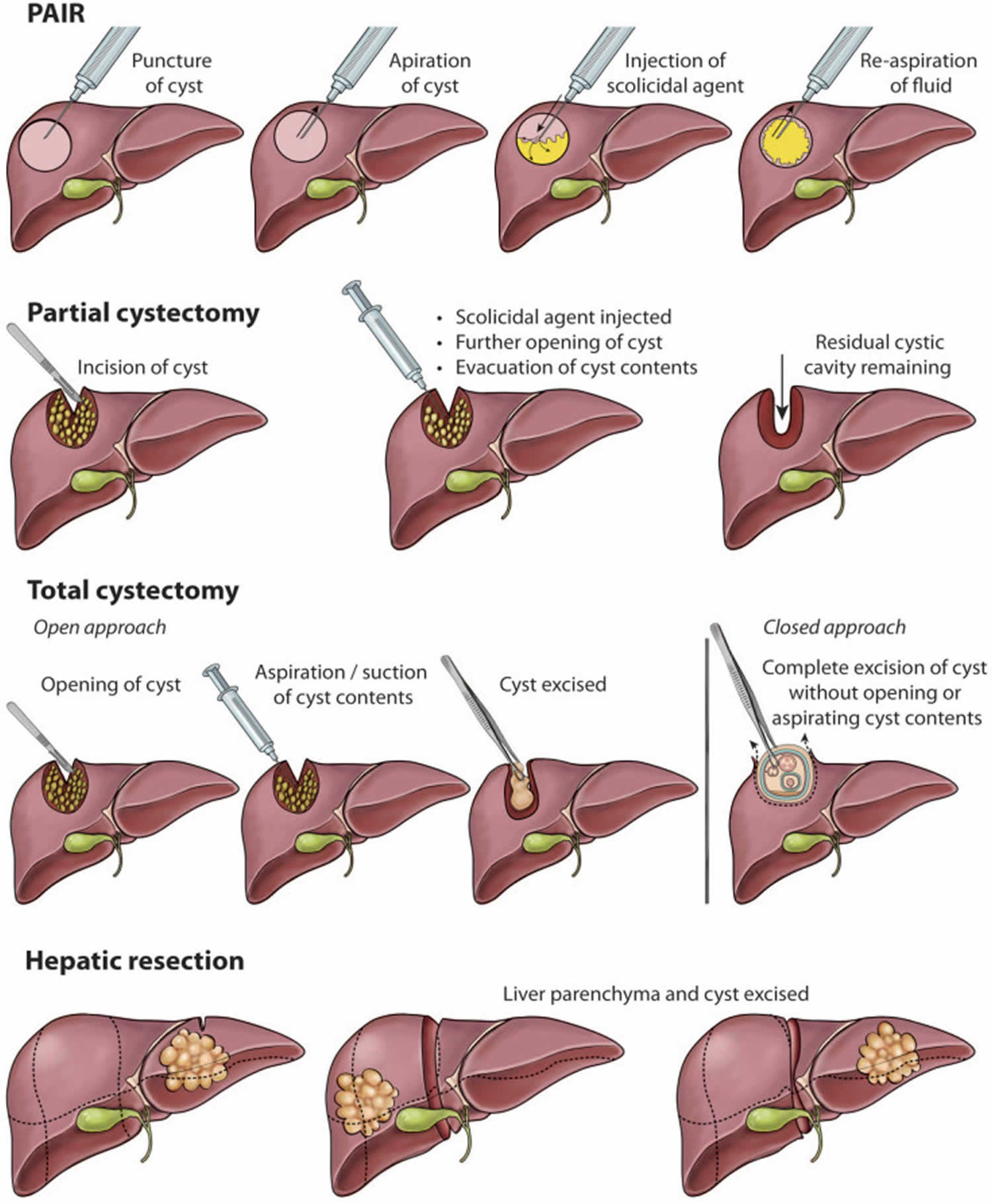
Footnotes: Surgical approaches for liver cystic echinococcosis vary from minimally invasive percutaneous approaches (PAIR) to more invasive surgical treatment options, which include partial cystectomy, total cystectomy and hepatic resection.
[Source 18 ]Cystic echinococcosis treatment
In the past, surgery was the only treatment for cystic echinococcal (Echinococcus granulosus) cysts. Antiparasitic drugs (albendazole or mebendazole), cyst puncture, and PAIR (percutaneous aspiration, injection of chemicals and reaspiration) have been used to replace surgery as effective treatments for cystic echinococcosis (Echinococcus granulosus) and, for some cases, no treatment but a conservative “watch and wait” approach is best. Treatment indications vary with cyst characteristics, including cyst type, location, size, and complications. Surgery may be the best treatment for liver cysts that are secondarily infected, or cysts located in the brain, lungs, or kidney. Liver cysts larger than 7.5 cm are likely to have biliary communication; surgery may be the best option for these cysts. Many abdominal cysts can be treated by injection of protoscolicidal chemical solutions into the cyst, followed by evacuation, prior to further manipulations and extirpation of cysts.
For some patients, drug treatment with benzimidazoles is the preferred treatment. Approximately one third of patients treated with benzimidazole drugs have been cured of cystic echinococcosis (Echinococcus granulosus) and even higher proportions, between 30 – 50%, have responded with significant regression of the cyst size and alleviation of symptoms.
Patients with small cysts or multiple cysts in several organs can be treated successfully with albendazole.
Both albendazole 10 – 15 mg/kg body weight per day (max 800 mg orally in two doses) and, as a second choice for treatment, mebendazole 40 – 50 mg/kg body weight per day continuously for several months have been highly effective. Additionally, antiparasitic drugs can be very effective when used in conjunction with surgery. Albendazole has been administered to patients prior to surgery for the intended purpose of facilitating the safe surgical manipulation of the cysts by inactivating protoscolices, altering the integrity of the cyst’s membranes, and reducing the turgidity of the cysts.
Praziquantel may be useful preoperatively or in case of spillage of cyst contents during surgery 105.
A third treatment option, PAIR (percutaneous aspiration, injection of chemicals and reaspiration), has been shown to be effective. This option is indicated for patients with relapse after surgery, failure of antiparasitic drug alone, or who refuse surgery.
World Health Organization (WHO) guidelines for cystic echinococcosis treatment
World Health Organization (WHO) 2025 guidelines for cystic echinococcosis treatment 106, 107:
- The “Watch and wait” approach can be an option in cases in which the cysts are uncomplicated (stages CE4 and CE5), given that long-term follow-up with ultrasonography can be ensured.
- Medical treatment with benzimidazoles is indicated for CE1 and CE3a cysts smaller than 5 cm in the liver and lung, patients with cysts in two or more organs, and inoperable patients. Benzimidazoles are also used following surgery or percutaneous procedures to prevent recurrence. Albendazole is currently the drug of choice at a dose of 10 to 15 mg/kg/day. Mebendazole at a dose of 40 to 50 mg/kg/day is another therapeutic option. Medical treatment with benzimidazole is contraindicated in cysts vulnerable to rupture and early pregnancy. Duration of treatment is based on the clinical situation and can range from 1 to 6 months.
- Surgery is the modality of choice for complicated cysts. It is necessary for the removal of large CE2-CE3b cysts, superficial cysts that may rupture with trauma or spontaneously, infected cysts, cysts with biliary tree communication, and cysts exerting pressure on adjacent organs.
- PAIR (Puncture, Aspiration, Injection, Re-aspiration) procedure is an ultrasound-guided, minimally invasive modality used in hepatic and other abdominal cysts. Indications include inoperable patients, relapsing cases after surgery, and failure to respond to medical treatment. It provides the best results in CE1 and CE3a cysts over 5 cm and is used in combination with medical therapy (benzimidazole). It is contraindicated in for CE2, CE3b, CE4, and CE5 cysts. Physicians performing this procedure must be equipped to deal with the potential anaphylactic shock. Other percutaneous treatments can be used but are usually reserved for CE2 and CE3b cysts.
Uncomplicated liver cystic echinococcosis cysts: types CE1 or CE3a < 5 cm
- In patients with uncomplicated hepatic cyst types CE1 or CE3a < 5 cm, treatment with albendazole is suggested. This recommendation is applicable in any tier (see Tier footnotes below).
- Albendazole should be given orally, at a dosage of 10–15 mg/kg/day in two divided doses (up to 400 mg twice a day), with a fat rich meal to increase its bioavailability 28. It should be administered continuously, without the monthly treatment interruptions recommended in the 1980s. The treatment duration depends on the individual situation, stage and size of the cystic echinococcosis cyst. Current recommendations suggest continuous treatment for 3–6 months 108. It is important to use high-quality albendazole that contains the required amount of bioavailable drug.
- Albendazole is contraindicated in cysts at risk of rupture and in the first trimester of pregnancy 28. Later in pregnancy, potential benefits may warrant use of albendazole despite potential risks. Contraceptive measures are necessary for women of reproductive age while on long-term albendazole. Benzimidazoles must be used with caution in patients with chronic hepatic disease and avoided in those with bone-marrow depression. Monitoring of side-effects is based on liver enzymes for hepatotoxicity and blood cell count.
- Follow-up imaging at 3–6 months and thereafter once a year for a minimum of 5 consecutive years after inactivation may help evaluate the success of treatment and monitor for any recurrence of the cysts.
- A lack of response is defined as an absence of cyst changes after 3 months of treatment (detachment of the parasitic layers from the outer cyst wall, size reduction, or stage modification). Complete response should be evaluated not earlier than 12 months after treatment end.
- Based on expert opinion, if there is a lack of response to an initial course of albendazole, a repeat course of albendazole could be considered.
Uncomplicated liver cystic echinococcosis cysts: types CE1 or CE3a 5 cm to 10 cm
- In patients with uncomplicated hepatic cyst types CE1 or CE3a 5cm to 10cm, PAIR (Puncture, Aspiration, Injection, Re-aspiration) combined with albendazole is suggested. PAIR (Puncture, Aspiration, Injection, Re-aspiration) should not be used if biliary communication is present. This recommendation requires tier 3 or tier 4 settings (see Tier footnotes below).
- PAIR (Puncture, Aspiration, Injection, Re-aspiration) is only recommended where there is no biliary communication. If bile-stained cyst fluid is aspirated (the assessment is made through visual inspection of aspirate for bile contamination and checking for bilirubin in the aspirated cyst fluid) or contrast is observed in the biliary tract after having been injected into the cyst during a planned PAIR procedure, it is strongly recommended that injection of a protoscolecidal agent after aspiration is not performed. An alternative treatment is percutaneous drainage (S-CAT) without injection of protoscolecidal agent and prolonging administration of albendazole to 6 months. Surgery or medical management can also be considered.
- Standard practice is to give albendazole for 1–7 days prior to PAIR (Puncture, Aspiration, Injection, Re-aspiration) and then continue for 1–3 months post-PAIR 109, at a dose of 10–15 mg/kg/day (up to 400 mg twice a day) in two divided doses with a fat-rich meal to increase its bioavailability; duration can be extended if considered appropriate. It is important to use high-quality albendazole (branded or generic) that contains the required amount of bioavailable drug. A two-week post-procedure course of praziquantel in addition to albendazole may be considered if there is spillage of cyst contents.
- For larger hepatic cystic echinococcosis cysts, especially for CE1 cyst types which are more prone to albendazole-related perforation, albendazole should be given for a shorter period before procedure (sometimes only once) to reduce the risk of perforation.
- After PAIR, patients must be closely monitored for potential complications including anaphylaxis, infection or bleeding. Monitoring of adverse events to albendazole treatment should also be implemented.
- Albendazole is contraindicated in cysts at risk of rupture and in the first trimester of pregnancy 28. Later in pregnancy, potential benefits may warrant use of albendazole despite potential risks. Contraceptive measures are necessary for women of reproductive age while on long-term albendazole. Benzimidazoles must be used with caution in patients with chronic hepatic disease and avoided in those with bone-marrow depression. Monitoring of side-effects is based on liver enzymes for hepatotoxicity and blood cell-count.
- In cases where surgical intervention is chosen for individuals with uncomplicated CE1 or CE3a cysts 5–10 cm in size, the surgical procedure can be performed either through an open or laparoscopic approach, depending on the location of the cyst, the expertise of the surgical team and the availability of resources. For any patient in which surgery is an option, individual patient factors such as general health, comorbidities and age should be considered before the final decision is made.
- Follow-up imaging at 3–6 months and thereafter once a year for a minimum of 5 consecutive years after inactivation may help evaluate the success of treatment and monitor for any recurrence of the cysts.
- A lack of response is defined as an absence of cyst changes after 3 months of treatment (detachment of the parasitic layers from the outer cyst wall, size reduction, or stage modification). Complete response should be evaluated not earlier than 12 months after treatment end.
Uncomplicated liver cystic echinococcosis cysts: types CE1 or CE3a > 10 cm
- In patients with uncomplicated hepatic cyst types CE1 or CE3a > 10 cm, percutaneous treatment combined with albendazole is suggested. PAIR (Puncture, Aspiration, Injection, Re-aspiration) is suggested rather than standard catheterization or surgery. PAIR (Puncture, Aspiration, Injection, Re-aspiration) should not be used if biliary communication is present. This recommendation requires tier 3 or tier 4 settings (see Tier footnotes below).
- Many health care settings may not have the appropriate expertise and resources available to safely deliver PAIR (Puncture, Aspiration, Injection, Re-aspiration), Standard Catheterization (S-CAT) or surgery. In these settings, the safest treatment option utilizing available expertise and resources with consideration of patient treatment preferences is recommended.
- PAIR (Puncture, Aspiration, Injection, Re-aspiration) is only recommended where there is no biliary communication, and cysts > 10 cm have high risk of such fistulas, so special care should be taken. If bile-stained cyst fluid is aspirated (the assessment is made through visual inspection of aspirate for bile contamination and checking for bilirubin in the aspirated cyst fluid) or contrast is observed in the biliary tract after having been injected into the cyst during a planned PAIR procedure, it is strongly recommended that injection of a protoscolecidal agent after aspiration is not performed. An alternative treatment is percutaneous drainage (S-CAT) without injection of protoscolecidal agent and prolonging the administration of albendazole to 6 months. Surgery or medical management can also be considered.
- Standard practice is to give albendazole for 1–7 days prior to the percutaneous treatment and then continue for 1–3 months post percutaneous treatment 109, at a dose of 10–15 mg/kg/day (up to 400 mg twice a day) in two divided doses with a fat-rich meal to increase its bioavailability; duration can be extended if considered appropriate. It is important to use high-quality albendazole (branded or generic) that contains the required amount of bioavailable drug. A 2-week post-procedure course of praziquantel in addition to albendazole may be considered if there is spillage of cyst contents.
- For larger hepatic cystic echinococcosis cysts, especially for CE1 cyst types which are more prone to albendazole- related perforation, albendazole should be given for a shorter period before procedure (sometimes only once) to reduce the risk of perforation.
- After percutaneous treatments, patients must be closely monitored for potential complications including anaphylaxis, infection or bleeding. Monitoring of adverse events to albendazole should also be implemented.
- Albendazole is contraindicated in cysts at risk of rupture and in the first trimester of pregnancy 28. Later in pregnancy, potential benefits may warrant use of albendazole despite potential risks. Contraceptive measures are necessary for women of reproductive age while on long-term albendazole. Benzimidazoles must be used with caution in patients with chronic hepatic disease and avoided in those with bone-marrow depression. Monitoring of side-effects is based on liver enzymes for hepatotoxicity and blood cell count.
- In cases where surgical intervention is chosen for individuals with uncomplicated CE1 or CE3a cysts > 10 cm in size, the surgical procedure can be performed either through an open or laparoscopic approach, depending on the location of the cyst, the expertise of the surgical team and the availability of resources. For any patient in which surgery is an option, individual patient factors such as general health, co-morbidities and age should be considered before the final decision is made.
- Follow-up imaging at 3–6 months and thereafter once a year for a minimum of 5 consecutive years after inactivation may help evaluate the success of treatment and monitor for any recurrence of the cysts.
- A lack of response is defined as an absence of cyst changes after 3 months of treatment (detachment of the parasitic layers from the outer cyst wall, size reduction, or stage modification). Complete response should be evaluated not earlier than 12 months after treatment end.
Uncomplicated liver cystic echinococcosis cysts: types CE2 or CE3b ≤ 5 cm
- In patients with uncomplicated hepatic cyst types CE2 or CE3b ≤ 5 cm, initial treatment with albendazole alone is suggested. This recommendation is applicable in any tier (see Tier footnotes below).
- Albendazole should be given orally, at a dosage of 10–15 mg/kg/day in two divided doses (up to 400 mg twice a day), with a fat-rich meal to increase its bioavailability 28. Albendazole should be administered continuously, without the monthly treatment interruptions recommended in the 1980s. The treatment duration depends on the individual situation, stage and size of the cystic echinococcosis cyst. Current recommendations suggest continuous treatment for 3–6 months 108. It is important to use high-quality albendazole that contains the required amount of bioavailable drug.
- Albendazole is contraindicated in cysts at risk of rupture and in the first trimester of pregnancy 28. Later in pregnancy, potential benefits may warrant use of albendazole despite potential risks. Contraceptive measures are necessary for women of reproductive age while on long-term albendazole. Benzimidazoles must be used with caution in patients with chronic hepatic disease and avoided in those with bone-marrow depression. Monitoring of side-effects is based on liver enzymes for hepatotoxicity and blood cell count.
- Follow-up imaging at 3–6 months and thereafter once a year for a minimum of 5 consecutive years after inactivation may help evaluate the success of treatment and monitor for any recurrence of the cysts.
- A lack of response is defined as an absence of cyst changes after 3 months of treatment (detachment of the parasitic layers from the outer cyst wall, size reduction or stage modification). Complete response should be evaluated not earlier than 12 months after end of treatment.
- Since albendazole alone is known to have a higher risk of relapse, in the event of non-response at 3 months, based on expert opinion, surgery (non-radical or radical approaches) should be offered along with continued albendazole. For any patient in which surgery is an option, individual patient factors such as general health, comorbidities and age should be considered before the final decision is made.
Uncomplicated liver cystic echinococcosis cysts: types CE2 or CE3b > 5 cm
- In patients with uncomplicated hepatic cyst types CE2 or CE3b > 5 cm, surgery combined with albendazole is suggested. This can be open surgery (in tiers 2–4) or laparoscopy (in tiers 3–4) (see Tier footnotes below).
- For any patient in which an invasive procedure, especially surgery, is an option, individual patient factors such as general health, comorbidities and age should be considered before the final decision is made.
- The choice between open or laparoscopic surgery will depend on the setting infrastructure, availability of laparoscopy, site of the cyst and cyst characteristics, expertise and experience of the local clinical team, surgeon’s preference and patient choice. Laparoscopy is favoured for peripheral, superficial cysts, especially in paediatric cases, and open surgery should be chosen when a cyst is deep or in other complicated scenarios.
- Surgical challenges include inaccessibility when dealing with small cysts deep within the liver parenchyma, particularly in segments 7 and 8, and in individuals with underlying comorbidities.
If opting for Mo-CAT, it is crucial to reduce the risk of recurrence by ensuring thorough removal of all cyst content and the germinal layer. T2-weighted MRI in addition to ultrasound and cavitography can be used to monitor the efficacy of treatment between sessions. - Standard practice is to give albendazole for 1–7 days prior to the surgical procedure and then continue for 1–3 months post procedure, at a dose of 10–15 mg/kg/day (up to 400 mg twice a day) in two divided doses with a fat-rich meal to increase its bioavailability; duration can be extended if considered appropriate. It is important to use high-quality albendazole that contains the required amount of bioavailable drug. A two-week post-procedure course of praziquantel in addition to albendazole may be considered if there is spillage of cyst contents.
- For the larger hepatic cystic echinococcosis cysts, albendazole should be given for a shorter period before procedure (sometimes only once) to reduce the risk of perforation.
- After surgery, patients must be closely monitored for potential complications including anaphylaxis, infection or bleeding. Monitoring of adverse events to albendazole should also be implemented.
- Albendazole is contraindicated in cysts at risk of rupture and in the first trimester of pregnancy 28. Later in pregnancy, potential benefits may warrant use of albendazole despite potential risks. Contraceptive measures are necessary for women of reproductive age while on long-term albendazole. Benzimidazoles must be used with caution in patients with chronic hepatic disease and avoided in those with bone-marrow depression. Monitoring of side-effects is based on liver enzymes for hepatotoxicity and blood cell count.
- Follow-up imaging at 3–6 months and thereafter once a year for a minimum of 5 consecutive years after inactivation may help evaluate the success of treatment and monitor for any recurrence of the cysts.
- A lack of response is defined as an absence of cyst changes after 3 months of treatment (detachment of the parasitic layers from the outer cyst wall, size reduction or stage modification). Complete response should be evaluated not earlier than 12 months after treatment end.
Use of praziquantel combined with albendazole post-percutaneous/surgical procedures for hepatic cyst types CE1, CE2, CE3a, CE3b
- In cystic echinococcosis patients undergoing percutaneous or surgical interventions, when spillage is suspected or has occurred, the combination praziquantel and albendazole is suggested.
- In case of suspected or ascertained cyst fluid spillage, albendazole should be given at a dose of 10–15 mg/kg/day in two divided doses (up to 400 mg twice a day) for a minimum of 3 months, usually, 6–12 months after the intervention, as considered appropriate by the clinician.
- Praziquantel should be given at a dose of 40–50 mg/kg/day divided into two daily doses for 2 weeks after the intervention. Because praziquantel does not have an effect on the cyst (as compared to albendazole), 2 weeks are suggested. However, the period can be increased to a maximum of 4 weeks if considered appropriate by the clinician.
- Albendazole and praziquantel can be given simultaneously during a fat-rich meal to increase their bioavailability.
- Some clinicians use praziquantel in combination with albendazole for 2 weeks prior to procedure 110. More evidence is needed to make this practice a recommendation.
Uncomplicated lung cystic echinococcosis cysts ≤ 5 cm
- In patients with uncomplicated active lung cystic echinococcosis cysts < 5 cm, surgery is suggested. Albendazole should not be given before surgery. When spillage is suspected or has occurred, albendazole after surgery is suggested. Lung surgery requires tier 4 settings (see Tier footnotes below).
- Medical treatment with albendazole should only be contemplated if surgery is medically contraindicated or not feasible due to specific patient circumstances. During medical treatment, regular monitoring for secondary infection, or expectoration of laminated layer, is mandated. T2-weighted MRI can be applied to monitor the inactivation of the cyst over time.
- For any patient in which an invasive procedure, especially surgery, is an option, individual patient factors such as general health, comorbidities and age should be considered before the final decision is made.
- Standard practice is not to give albendazole prior to the surgical procedure due to the perceived risk of rupture in the case of lung cysts. If there are concerns of intraoperative spillage, then give albendazole for 1–3 months post procedure, at a dose of 10–15 mg/kg/day (up to 400 mg twice a day) in two divided doses with a fat-rich meal to increase its bioavailability; duration can be extended if considered appropriate. It is important to use high-quality albendazole, that contains the required amount of bioavailable drug. A 2-week post-procedure course of praziquantel in addition to albendazole may be considered if there is spillage of cyst contents.
- After surgery, patients must be closely monitored for potential complications including anaphylaxis, infection, prolonged air leak or bleeding. Monitoring of adverse events to albendazole should also be implemented.
- Albendazole is contraindicated in the first trimester of pregnancy 28. Later in pregnancy, potential benefits may warrant use of albendazole despite potential risks. Contraceptive measures are necessary for women of reproductive age while on long-term albendazole. Benzimidazoles must be used with caution in patients with chronic hepatic disease and avoided in those with bone-marrow depression. Monitoring of side-effects is based on liver enzymes for hepatotoxicity and blood cell count.
- Follow-up imaging at 3–6 months and thereafter once a year for a minimum of 5 years after inactivation may help evaluate the success of treatment and monitor for any recurrence of the cysts.
A lack of response is defined as an absence of cyst changes after 3 months of treatment (detachment of the parasitic layers from the surrounding lung tissue, size reduction or morphological change). Complete response should be evaluated not earlier than 12 months after treatment end.
Uncomplicated inactive liver cysts are not covered in these guidelines. Current practice is to “watch and wait”, that is, to follow-up with imaging (ultrasonography or MRI). Surgery should be avoided as far as possible unless the inactive cyst is causing complications (e.g. cyst causing portal hypertension).
Patients with multiple hepatic cysts, with hepatic cysts in different stages, and with two or more organs involved (multi-organ involvement) will require individualized management 106, 107.
Tiers Footnotes:
- Tier 1: Medical doctor, basic laboratory capacity, ultrasound referral availability.
- Tier 2: Tier 1 plus general surgeon, anaesthetic and operating theatre capacity, on-site ultrasonography.
- Tier 3: Tier 2 plus laparoscopic surgeon, physician trained in PAIR, Standard Catheterization (S-CAT), CT and fluoroscopy capacity.
- Tier 4: Tier 3 plus thoracic surgery and interventional radiology capacity, MRI and MRCP capacity, advanced laboratory capacity.
Antiparasitic therapy
Antiparasitic therapy confers numerous benefits for the patient. It can be used as monotherapy for the uncomplicated CE1 and CE3a liver cysts less than 5 cm in diameter and multiple liver cysts or multiorgan involvement in the inoperable candidate 5, 111, 31. Antiparasitic therapy is also used as a neoadjuvant agent before percutaneous or surgical therapy to chemically sterilize the parasite to render the cyst inactive, reduce the cystic wall tension and reduce the risk of intra-operative viable cyst rupture 36, 31. Due to the increased bioavailability and improved absorption from the gut, albendazole is the preferred anthelmintic agent of choice for liver hydatid disease 5, 111, 112, 113. Albendazole is administered at a 12-hourly dosage of 10–15 mg/kg/day 5, 31. There has been no consensus on the schedule and length of anthelmintic in the neoadjuvant and adjuvant setting, with various authors making different recommendations 5. Akhan et al 114 recommended albendazole therapy be given for Puncture, Aspiration, Injection and Re-aspiration (PAIR), 1 week before and 1 month after treatment. Velasco-Tirado et al 113 recommended that albendazole be used pre-operatively anytime from 3 months to 1 day before surgical or percutaneous intervention and continued 1–3 months after the procedure. Wen et al 5 suggested initiating albendazole therapy 1 week before intervention and continuing for up to 2 months after the procedure. A comprehensive regime to administer for uncomplicated cysts is albendazole therapy, administered at least 3 days pre-operatively and continued post-operatively for 4–8 weeks. In complicated cysts or intra-operative spillage, the post-operative duration may be extended to 3–6 months 34, 36, 31.
A continuous treatment regime should be administered with the previous regime of cyclical administration avoided in current practice 34, 31. Clinicians must be prudent about the side effects of albendazole, such as hepatic dysfunction, alopecia and agranulocytosis. Patients should be monitored regularly with white cell count and liver function tests 115, 31. Blood tests should be done on days 5, 14 and 28 after initiation, biweekly and monthly, if therapy is ongoing 34, 36, 115. It should be noted that albendazole is contraindicated in early pregnancy as it is teratogenic in rats and rabbits 116, 31.
Some authors have postulated that combination therapy with praziquantel increases the albendazole metabolite’s serum and cystic fluid levels compared with patients receiving albendazole monotherapy 113, 34. However, due to the lack of more robust evidence with further randomized control trials, it is not a widely accepted practice 113, 31, 112.
Albendazole
- Adult dosage 400 mg orally twice a day for 1-6 months
- Children dosage 10-15 mg/kg/day (max 800 mg) orally in two doses for 1-6 months
Albendazole treatment during pregnancy
- Albendazole is a pregnancy category C drug. There are limited data on the use of albendazole in pregnant women. The available evidence suggests no difference in congenital abnormalities in the children of women accidentally treated with albendazole during mass drug administration (MDA) campaigns compared with those who were not. In MDA campaigns for which the World Health Organization (WHO) has determined that the benefits of treatment outweigh the risks, WHO allows use of albendazole in the 2nd and 3rd trimesters of pregnancy. However, healthcare providers should balance the risks of treatment for the fetus with the risks of disease progression in the woman in the absence of treatment.
- Pregnancy Category C: Either studies in animals have revealed adverse effects on the fetus (teratogenic or embryocidal, or other) plus there are no controlled studies in women, or studies in women and animals are not available. Prescribe albendazole only if the potential benefits to the woman justify the potential risks to the fetus.
Treatment during lactation - Albendazole is minimally excreted in human milk. WHO has concluded that a single oral dose of albendazole can be given to lactating women.
Albendazole treatment in children
The safety of albendazole in children less than 6 years old is not certain. Studies of the use of albendazole in children as young as one year old suggest that it is safe. According to WHO guidelines for Mass Drug Administration campaigns, children as young as one year of age (able to safely swallow tablets) can take albendazole. These Mass Drug Administration campaigns have treated many children under six years old with albendazole, albeit at a reduced dose.
Mebendazole
- Adult dosage 40 – 50 mg/kg body weight per day continuously for several months. Duration of treatment is based on the clinical situation and can range from 1 to 6 months.
Mebendazole treatment during pregnancy
- Mebendazole is a pregnancy category C drug. Data on the use of mebendazole in pregnant women are limited. The available evidence suggests no difference in congenital anomalies in the children of women treated with mebendazole during mass drug administration (MDA) campaigns compared with those who were not. In MDA campaigns in countries where soil-transmitted helminths are common, World Health Organization (WHO) has determined that the benefits of treatment outweigh the risks and WHO allows use of mebendazole in the 2nd and 3rd trimesters of pregnancy. However, in a pregnant woman infected with a soil-transmitted helminth, balance the risks of treatment for the fetus with the risks of disease progression in the woman in the absence of treatment.
- Pregnancy Category C: Either studies in animals have revealed adverse effects on the fetus (teratogenic or embryocidal, or other) plus there are no controlled studies in women, or studies in women and animals are not available. Prescribe mebendazole only if the potential benefits to the woman justify the potential risks to the fetus.
Treatment during lactation
Mebendazole is minimally excreted in breast milk. WHO classifies mebendazole as compatible with breastfeeding and allows its use in lactating women.
Mebendazole treatment in children
The safety of mebendazole in children is unclear. There are limited data in children under 2 years old. The WHO Model List of Essential Medicines for Children lists mebendazole as an intestinal antihelminthic medicine that can be used for children older than 2 years of age.
‘Watch and wait’ approach
Inactive, degenerating CE4 and all CE5 cysts can be observed with interval ultrasound monitoring without pharmacological or surgical intervention 35, 5, 117.
Percutaneous therapy
Percutaneous approaches for the treatment of liver hydatid disease include PAIR (Puncture, Aspiration, Injection, Re-aspiration), standard catheterization (S-CAT) and modified catheterization technique (MoCat) 34, 118, 119, 120, 121.
PAIR (Puncture, Aspiration, Injection, Re-aspiration) therapy is successfully used for single-compartment cysts, such as CE1 and CE3a cysts less than 10 cm in diameter. Deterrence of PAIR use includes CE2 and CE3b cysts, cases where safe percutaneous cyst localisation with ultrasound guidance is unavailable, and when there is evidence of cysto-biliary communication 120, 122, 35, 31, 119.
Standard catheterization (S-CAT) technique is also used for CE1 and CE3a cysts but includes cysts with a diameter greater than 10 cm or those with cystic fluid content of more than 1,000 ml 123, 31. If a cysto-biliary communication is found during PAIR, a standard catheterization (S-CAT) technique may be utilised to control biliary drainage 123. One of the drawbacks is the increased duration of hospital stay. Akhan et al 114 reported a median duration of hospital stay of 2.5 days in 26 patients with standard catheterisation. The catheterization and hospital stay may be prolonged if cysto-biliary communication or cystic infection occurs 124, 125, 126, 123.
A modification to PAIR, the modified catheterization (MoCat) technique, has been utilized for uncomplicated CE2 and CE3b cysts and cysts larger than 10 cm in diameter. As with standard catheterization (S-CAT) technique, modified catheterization (MoCat), results in a longer hospital stay. The modified catheterization (MoCat) approach uses a drainage catheter placed via the Seldinger technique, wherein the cyst contents and membranes can be aspirated. At the end of the procedure, the catheter can be left in place for any ongoing fluid drainage 127, 5, 128, 31, 119, 121.
The first step in the standard PAIR technique is to puncture and aspirate the cyst under ultrasound guidance. A scolicidal agent is then injected into the cystic cavity to sterilise the cyst of any viable protoscoleces and destroy the germinal layer. Various scolicidal agents have been adopted in the use of hydatid disease. Either 20% hypertonic saline or 95% alcohol is recommended with the PAIR technique. The fluid is re-aspirated approximately 15–20 minutes later 129, 117, 5, 35. If bile is aspirated, initially after the first puncture, it is suggestive of cysto-biliary communication. Scolicidal injection into the cyst may result in a devastating risk of chemical sclerosing cholangitis and subsequent biliary stricturing and thus should be avoided 111, 129. There are limited recommendations regarding the management of cysto-biliary communication noted during PAIR. Khuroo 122 recommends aborting PAIR if ‘yellow cyst fluid’ or ‘positive bilirubin dipstick’ on fluid aspiration occurs. Öztürk et al 119 Turkish consensus report recommends catheterisation after percutaneous therapy can be done for cysts larger than 10 cm and those with biliary content. Catheterization should be left in place for roughly 1 week, with removal only once the fistula output is less than 10 cc. If there is an ongoing or increasing biliary leak, endoscopic retrograde cholangiopancreatography (ERCP) is recommended 119.
Surgery
Surgical options for liver hydatid disease can be divided into conservative and radical approaches 130. The radical approach, which includes total cystectomy and hepatic resection, has been criticised as an aggressive form of therapy associated with significant morbidity for a relatively benign disease process 130, 131. It is also a technically demanding surgery and usually requires patients to be operated on in a specialised hepatobiliary unit 116, 111. For these reasons, the conservative approach with partial cystectomy is more widely adopted. This involves the removal of the cyst content and sterilisation of the residual cavity, together with partial cyst resection, under albendazole cover 132, 133, 5.
The partial cystectomy approach uses an appropriate incision to gain access to and expose the liver cyst(s). The surgical field is protected by abdominal swabs soaked in a scolicidal agent (20% hypertonic saline). This helps to prevent contamination in the event of spillage during cyst-content evacuation. The cyst is then punctured, aspirated and instilled with a chosen scolicidal agent. As with PAIR, if bile is aspirated within the cyst, biliary communication is present and the scolicidal agent is avoided. After 15 minutes, the contents are re-aspirated, and the cyst is opened to evacuate the endocyst contents with suction. The cyst is then unroofed by excising the cyst wall outside the liver parenchyma. If a cysto-biliary fistula is noted intra-operatively, it can be managed by suture placement. Once the cystic cavity is evacuated of its contents, the cavity needs to be obliterated either with capitonnage or omentoplasty 34, 133, 129.
Follow-up period
Follow-up is recommended initially every six months for the first two years, and then once a year depending on the appropriate clinical setting. In hydatid disease, it is difficult to assess the frequency of relapses. Therefore, monitoring with ultrasound is sometimes performed for up to ten years, a duration for which recurrences have been reported despite treatment. In the post-treatment phase, serologic studies, often with Ig levels, are difficult to interpret because they may indicate residual disease as opposed to a disease recurrence. In many cases, they remain elevated despite appropriate therapy or complete resection, which is why they are often used in combination with imaging studies during follow-up to detect cystic activity 134.
Alveolar echinococcosis treatment
Alveolar echinococcosis (Echinococcus multilocularis) requires antiparasitic drug with or without surgery; radical surgery is the preferred approach in suitable cases, although removal of the entire parasite mass is not always possible. Effective treatment involves benzimidazoles administered continuously for at least two years and patient monitoring for 10 years or more since recurrence is possible. This has inhibited progression of alveolar echinococcosis and reduced lesion size in approximately half of treated cases. Intermittent treatment with albendazole is not recommended.
Follow-up after surgical treatment
Follow-up after surgical treatment is best performed by MRI of the chest 7. This can be done without contrast enhancement and requires heavily T2-weighted sequences. This technique has the highest sensitivity to detect postoperative recurrence very early (small fluid filled cysts). Its biggest disadvantage being lack of availability and affordability in most cystic echinococcosis endemic regions of the world.
Computed tomography of the chest is a less sensitive alternative and implies radiation exposure. Patients should be followed for at least 5 years after surgery. In patients with remaining cysts, long-term follow-up is needed.
Hydatid disease prognosis
Hydatid disease prognosis prognosis is considered generally good with appropriate treatment and if the cysts respond to oral antiparasitic medicines. However, hydatid cysts that develop in difficult sites for surgery, such as the heart and spine, have a poorer prognosis 11. Only 30% to 40% of patients with spinal cystic echinococcosis (Echinococcus granulosus) make a full recovery and the Echinococcosis has high rates of morbidity and mortality 135. Complete cure is possible with total surgical excision without spillage for cystic echinococcosis. Spillage occurs in 2%-25% of cases (depends on the location and surgeon’s experience), and the operative mortality rate varies from 0.5%-4% for the same reasons. Recurrence at the site of the cyst or in other sites occurs in some cases 136, 137, 138, 139. Recurrence rates for those with spinal cystic echinococcosis at 24 months was 48% 135. It is for this reason that close follow-up with serial imaging is required.
In alveolar echinococcosis, the prognosis is much worse. Cure is only possible with early detection and complete surgical excision. In patients in whom the latter is not possible, the addition of long-term chemotherapy has decreased the 10-year mortality rates from 94% to 10%.
Morbidity and mortality
Morbidity is usually secondary to free rupture of the echinococcal cyst (with or without anaphylaxis), infection of the cyst, or dysfunction of affected organs. Examples of dysfunction of affected organs are biliary obstruction, cirrhosis, bronchial obstruction, renal outflow obstruction, increased intracranial pressure secondary to a mass, and hydrocephalus secondary to cerebrospinal fluid outflow obstruction.
In cystic echinococcosis, mortality is secondary to anaphylaxis, systemic complications of the cysts (eg, sepsis, cirrhosis, respiratory failure), or operative complications.
In clinical cases of alveolar echinococcosis, the mortality rate is 50%-60%. This figure reaches 100% for untreated or poorly treated alveolar echinococcosis. Sudden death has been reported with alveolar echinococcosis in asymptomatic patients (autopsy diagnosis).
- Ravis E, Theron A, Lecomte B, Gariboldi V. Pulmonary cyst embolism: a rare complication of hydatidosis. Eur J Cardiothorac Surg. 2018 Jan 1. 53(1):286-7.[↩]
- Rinaldi F, Brunetti E, Neumayr A, Maestri M, Goblirsch S, Tamarozzi F. Cystic echinococcosis of the liver: A primer for hepatologists. World J Hepatol. 2014 May 27;6(5):293-305. doi: 10.4254/wjh.v6.i5.293.[↩][↩]
- Moro P, Schantz PM. Echinococcosis: a review. Int J Infect Dis. 2009 Mar;13(2):125-33. https://doi.org/10.1016/j.ijid.2008.03.037[↩][↩][↩][↩][↩][↩]
- Vuitton DA, McManus DP, Rogan MT, Romig T, Gottstein B, Naidich A, Tuxun T, Wen H, Menezes da Silva A; World Association of Echinococcosis. International consensus on terminology to be used in the field of echinococcoses. Parasite. 2020;27:41. doi: 10.1051/parasite/2020024[↩][↩][↩][↩][↩][↩]
- Wen H, Vuitton L, Tuxun T, Li J, Vuitton DA, Zhang W, McManus DP. Echinococcosis: Advances in the 21st Century. Clin Microbiol Rev. 2019 Feb 13;32(2):e00075-18. doi: 10.1128/CMR.00075-18[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Autier B, Gottstein B, Millon L, Ramharter M, Gruener B, Bresson-Hadni S, Dion S, Robert-Gangneux F. Alveolar echinococcosis in immunocompromised hosts. Clin Microbiol Infect. 2023 May;29(5):593-599. https://www.clinicalmicrobiologyandinfection.org/article/S1198-743X(22)00630-9/fulltext[↩]
- Weber TF, Junghanss T, Stojković M. Pulmonary cystic echinococcosis. Curr Opin Infect Dis. 2023 Oct 1;36(5):318-325. doi: 10.1097/QCO.0000000000000962[↩][↩][↩]
- Pal, Mahendra & Alemu, Habtamu & Megersa, Lencho & Garedo, Derartu & Bodena, Ebisa. (2022). Cystic Echincoccoosis: A Comprehensive Review on Life Cycle, Epidemiology, Pathogenesis, Clinical Spectrum, Diagnosis, Public Health and Economic Implications, Treatment, and Control. International Journal of Clinical and Experimental Medicine Research. 6. 10.26855/ijcemr.2022.04.005. https://www.researchgate.net/publication/359576923_Cystic_Echincoccoosis_A_Comprehensive_Review_on_Life_Cycle_Epidemiology_Pathogenesis_Clinical_Spectrum_Diagnosis_Public_Health_and_Economic_Implications_Treatment_and_Control[↩][↩][↩]
- About Echinococcosis. https://www.cdc.gov/echinococcosis/about[↩][↩]
- Echinococcosis. https://www.who.int/news-room/fact-sheets/detail/echinococcosis[↩][↩][↩][↩]
- Almulhim AM, John S. Echinococcus Granulosus. [Updated 2023 Aug 7]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK539751[↩][↩][↩]
- Ghasemirad H, Bazargan N, Shahesmaeili A, Harandi MF. Echinococcosis in immunocompromised patients: A systematic review. Acta Trop. 2022 Aug;232:106490. doi: 10.1016/j.actatropica.2022.106490[↩]
- Monge-Maillo B, Lopez-Velez R. Cystic echinococcosis of the bone. Curr Opin Infect Dis. 2023 Oct 1;36(5):341-347. doi: 10.1097/QCO.0000000000000951[↩]
- Jensenius M, Mørch K, Yaqub S, Halvorsen DS, Reims HM, Björk IG, Røsok BI, Oltmanns G, Helbak K, Øines Ø, Lier T. Alveolar echinococcosis. Tidsskr Nor Laegeforen. 2024 Sep 9;144(10). https://tidsskriftet.no/en/2024/09/clinical-review/alveolar-echinococcosis[↩][↩][↩]
- Bresson-Hadni S, Spahr L, Chappuis F. Hepatic Alveolar Echinococcosis. Semin Liver Dis. 2021 Aug;41(3):393-408. doi: 10.1055/s-0041-1730925[↩][↩][↩][↩]
- Hydatid Cysts. https://emedicine.medscape.com/article/178648-overview[↩]
- Echinococcosis Laboratory Diagnsosi. https://www.cdc.gov/dpdx/echinococcosis/index.html#tabs-1-2[↩][↩][↩][↩]
- Govindasamy A, Bhattarai PR, John J. Liver cystic echinococcosis: a parasitic review. Ther Adv Infect Dis. 2023 May 11;10:20499361231171478. doi: 10.1177/20499361231171478[↩][↩]
- Şahin S, Kaya B. Evaluation of Hydatid Cyst Cases: A Single-center Retrospective Study. Turkiye Parazitol Derg. 2025 Jan 22;48(4):222-227. https://www.turkiyeparazitolderg.org/articles/evaluation-of-hydatid-cyst-cases-a-single-center-retrospective-study/doi/tpd.galenos.2024.79553[↩]
- Hydatid Disease from Head to Toe. Pinar Polat, Mecit Kantarci, Fatih Alper, Selami Suma, Melike Bedel Koruyucu, and Adnan Okur. RadioGraphics 2003 23:2, 475-494 https://doi.org/10.1148/rg.232025704[↩]
- Brunetti E, Kern P, Vuitton DA. Writing Panel for the WHO-IWGE. Expert consensus for the diagnosis and treatment of cystic and alveolar echinococcosis in humans. Acta Trop. 2010;114:1–16. doi: 10.1016/j.actatropica.2009.11.00[↩]
- WHO Informal Working Group. Expert consensus for the diagnosis and treatment of cystic and alveolar echinococcosis in humans. International classification of ultrasound images in cystic echinococcosis for application in clinical and field epidemiological settings. Acta Trop. 2010 Apr;114(1):1-16. https://doi.org/10.1016/j.actatropica.2009.11.001[↩][↩]
- Caremani M, Lapini L, Caremani D, Occhini U. Sonographic diagnosis of hydatidosis: the sign of the cyst wall. Eur J Ultrasound. 2003;16(3):217-23. doi: 10.1016/s0929-8266(02)00076-9[↩]
- Tamarozzi F, Akhan O, Cretu CM, Vutova K, Akinci D, Chipeva R, et al. Prevalence of abdominal cystic echinococcosis in rural Bulgaria, Romania, and Turkey: a cross-sectional, ultrasound-based, population study from the HERACLES project. Lancet Infect Dis. 2018;18(7):769-78. doi: 10.1016/S1473-3099(18)30221-4[↩]
- Solomon N, Kachani M, Zeyhle E, Macpherson CNL. The natural history of cystic echinococcosis in untreated and albendazole-treated patients. Acta Trop. 2017;171:52–7. doi: 10.1016/j.actatropica.2017.03.018[↩]
- Beggs I. The radiology of hydatid disease. AJR Am J Roentgenol. 1985 Sep;145(3):639-48. doi: 10.2214/ajr.145.3.639[↩]
- Stojkovic M, Rosenberger K, Kauczor HU, Junghanss T, Hosch W. Diagnosing and staging of cystic echinococcosis: how do CT and MRI perform in comparison to ultrasound? PLoS Negl Trop Dis. 2012;6(10):e1880. doi: 10.1371/journal.pntd.0001880[↩]
- Brunetti E, Kern P, Vuitton DA; Writing Panel for the WHO-IWGE. Expert consensus for the diagnosis and treatment of cystic and alveolar echinococcosis in humans. Acta Trop. 2010 Apr;114(1):1-16. doi: 10.1016/j.actatropica.2009.11.001[↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Kratzer W, Gruener B, Kaltenbach TE, Ansari-Bitzenberger S, Kern P, Fuchs M, Mason RA, Barth TF, Haenle MM, Hillenbrand A, Oeztuerk S, Graeter T. 2015. Proposal of an ultrasonographic classification for hepatic alveolar echinococcosis: Echinococcosis multilocularis Ulm classification-ultrasound. World J Gastroenterol 21:12392–12402. doi: 10.3748/wjg.v21.i43.12392[↩]
- Graeter T, Kratzer W, Oeztuerk S, Haenle MM, Mason RA, Hillenbrand A, Kull T, Barth TF, Kern P, Gruener B. 2016. Proposal of a computed tomography classification for hepatic alveolar echinococcosis. World J Gastroenterol 22:3621–3631. doi: 10.3748/wjg.v22.i13.3621[↩]
- Kern P, Menezes da Silva A, Akhan O, Müllhaupt B, Vizcaychipi KA, Budke C, Vuitton DA. The Echinococcoses: Diagnosis, Clinical Management and Burden of Disease. Adv Parasitol. 2017;96:259-369. doi: 10.1016/bs.apar.2016.09.006[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- McManus D.P., Thompson R.C. Molecular epidemiology of cystic echinococcosis. Parasitology. 2003;127:37–51. doi: 10.1017/s0031182003003524[↩][↩]
- Thompson R.C., McManus D.P. Towards a taxonomic revision of the genus Echinococcus. Trends Parasitol. 2002;18:452–457. doi: 10.1016/s1471-4922(02)02358-9[↩][↩]
- Tsoulfas G, Hoballah JJ, Velmahos GC, et al. The surgical management of parasitic diseases. Cham: Springer, 2020.[↩][↩][↩][↩][↩][↩][↩]
- Fadel SA, Asmar K, Faraj W, Khalife M, Haddad M, El-Merhi F. Clinical review of liver hydatid disease and its unusual presentations in developing countries. Abdom Radiol (NY). 2019 Apr;44(4):1331-1339. doi: 10.1007/s00261-018-1794-7[↩][↩][↩][↩]
- Bhutani N, Kajal P. Hepatic echinococcosis: A review. Ann Med Surg (Lond). 2018 Nov 2;36:99-105. doi: 10.1016/j.amsu.2018.10.032[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Yang Y.R., Sun T., Li Z., Zhang J., Teng J., Liu X. Community surveys and risk factor analysis of human alveolar and cystic echinococcosis in Ningxia Hui Autonomous Region, China. Bull. World Health Organ. 2006;84:714–721. doi: 10.2471/blt.05.025718[↩]
- Kammerer WS, Schantz PM. Echinococcal disease. Infect Dis Clin North Am. 1993 Sep;7(3):605-18.[↩][↩]
- Carrim Z.I., Murchison J.T. The prevalence of simple renal and hepatic cysts detected by spiral computed tomography. Clin. Radiol. 2003;58:626–629. doi: 10.1016/s0009-9260(03)00165-x[↩]
- Karaman U, Mıman O, Kara M, Gicik Y, Aycan OM, Atambay M. Kars bölgesinde hidatik kist prevalansı [Hydatid cyst prevalence in the region of Kars.]. Turkiye Parazitol Derg. 2005;29(4):238-40. Turkish.[↩]
- Lewall D.B. Hydatid disease: biology, pathology, imaging and classification. Clin. Radiol. 1998;52:863–874. doi: 10.1016/s0009-9260(98)80212-2[↩]
- Gottstein B. Hydatid disease, major tropical syndromes by body system. Syst. Infect. 2000;169 section 6.[↩]
- Siracusano A., Delunardo F., Teggi A., Ortona E. Host-parasite relationship in cystic echinococcosis: an evolving story. Clin. Dev. Immunol. 2012:639362. doi: 10.1155/2012/639362[↩]
- Lissandrin R., Tamarozzi F., Piccoli L., Tinelli C., Silvestri A., Mariconti M. Factors influencing the serological response in hepatic Echinococcus granulosus infection. Am. J. Trop. Med. Hyg. 2016;94:166–171. doi: 10.4269/ajtmh.15-0219[↩]
- Echinococcosis. https://www.cdc.gov/dpdx/echinococcosis/index.html[↩][↩]
- Hydatid Disease: Radiologic and Pathologic Features and Complications. Iván Pedrosa, Antonio Saíz, Juan Arrazola, Joaquín Ferreirós, and César S. Pedrosa. RadioGraphics 2000 20:3, 795-817 https://doi.org/10.1148/radiographics.20.3.g00ma06795[↩]
- Craig PS, McManus DP, Lightowlers MW, Chabalgoity JA, Garcia HH, Gavidia CM, Gilman RH, Gonzalez AE, Lorca M, Naquira C, Nieto A, Schantz PM. 2007. Prevention and control of cystic echinococcosis. Lancet Infect Dis 7:385–394. doi: 10.1016/S1473-3099(07)70134-2[↩]
- Zhang W, Zhang Z, Wu W, Shi B, Li J, Zhou X, Wen H, McManus DP. 2015. Epidemiology and control of echinococcosis in central Asia, with particular reference to the People’s Republic of China. Acta Trop 141:235–243. doi: 10.1016/j.actatropica.2014.03.014[↩]
- Craig PS, Li T, Qiu J, Zhen R, Wang Q, Giraudoux P, Ito A, Heath D, Warnock B, Schantz P, Yang W. 2008. Echinococcosis and Tibetan communities. Emerg Infect Dis 14:1674–1675. doi: 10.3201/eid1410.071636[↩]
- Alvarez Rojas CA, Romig T, Lightowlers MW. 2014. Echinococcus granulosus sensu lato genotypes infecting humans—review of current knowledge. Int J Parasitol 44:9–18. doi: 10.1016/j.ijpara.2013.08.008[↩]
- Deplazes P, Rinaldi L, Alvarez Rojas CA, Torgerson PR, Harandi MF, Romig T, Antolova D, Schurer JM, Lahmar S, Cringoli G, Magambo J, Thompson RC, Jenkins EJ. 2017. Global distribution of alveolar and cystic echinococcosis. Adv Parasitol 95:315–493. doi: 10.1016/bs.apar.2016.11.001[↩][↩][↩][↩][↩][↩]
- Larrieu E, Zanini F. 2012. Critical analysis of cystic echinococcosis control programs and praziquantel use in South America, 1974-2010. Rev Panam Salud Publica 31:81–87. doi: 10.1590/S1020-49892012000100012[↩][↩]
- Pavletic CF, Larrieu E, Guarnera EA, Casas N, Irabedra P, Ferreira C, Sayes J, Gavidia CM, Caldas E, Lise MLZ, Maxwell M, Arezo M, Navarro AM, Vigilato MAN, Cosivi O, Espinal M, Vilas V. 2017. Cystic echinococcosis in South America: a call for action. Rev Panam Salud Publica 41:e42[↩]
- Cucher MA, Macchiaroli N, Baldi G, Camicia F, Prada L, Maldonado L, Avila HG, Fox A, Gutierrez A, Negro P, Lopez R, Jensen O, Rosenzvit M, Kamenetzky L. 2016. Cystic echinococcosis in South America: systematic review of species and genotypes of Echinococcus granulosus sensu lato in humans and natural domestic hosts. Trop Med Int Health 21:166–175. doi: 10.1111/tmi.12647[↩]
- Craig PS, Hegglin D, Lightowlers MW, Torgerson PR, Wang Q. 2017. Echinococcosis: control and prevention. Adv Parasitol 96:55–158. doi: 10.1016/bs.apar.2016.09.002[↩][↩]
- Jenkins DJ, Lievaart JJ, Boufana B, Lett WS, Bradshaw H, Armua-Fernandez MT. 2014. Echinococcus granulosus and other intestinal helminths: current status of prevalence and management in rural dogs of eastern Australia. Aust Vet J 92:292–298. doi: 10.1111/avj.12218[↩]
- Rossi P, Tamarozzi F, Galati F, Pozio E, Akhan O, Cretu CM, Vutova K, Siles-Lucas M, Brunetti E, Casulli A. 2016. The first meeting of the European Register of Cystic Echinococcosis (ERCE). Parasit Vectors 9:243. doi: 10.1186/s13071-016-1532-3[↩][↩]
- Kawamura N, Kamiyama T, Sato N, Nakanishi K, Yokoo H, Kamachi H, Tahara M, Yamaga S, Matsushita M, Todo S. 2011. Long-term results of hepatectomy for patients with alveolar echinococcosis: a single-center experience. J Am Coll Surg 212:804–812. doi: 10.1016/j.jamcollsurg.2011.02.007[↩]
- Irie T, Mukai T, Yagi K. 2018. Echinococcus multilocularis surveillance using copro-DNA and egg examination of shelter dogs from an endemic area in Hokkaido, Japan. Vector Borne Zoonotic Dis 18:390–392. doi: 10.1089/vbz.2017.2245[↩]
- Vuitton DA, Wang Q, Zhou HX, Raoul F, Knapp J, Bresson-Hadni S, Wen H, Giraudoux P. A historical view of alveolar echinococcosis, 160 years after the discovery of the first case in humans: part 1. What have we learnt on the distribution of the disease and on its parasitic agent? Chin Med J (Engl). 2011 Sep;124(18):2943-53. DOI: 10.3760/cma.j.issn.0366-6999.2011.18.027[↩]
- Feng X, Qi X, Yang L, Duan X, Fang B, Gongsang Q, Bartholomot B, Vuitton DA, Wen H, Craig PS. 2015. Human cystic and alveolar echinococcosis in the Tibet Autonomous Region (TAR), China. J Helminthol 89:671–679. doi: 10.1017/S0022149X15000656[↩]
- Cai H, Guan Y, Ma X, Wang L, Wang H, Su G, Zhang X, Han X, Ma J, Liu YF, Li J, Zhang J, Wang Y, Wang W, Du R, Lei W, Wu W. 2017. Epidemiology of echinococcosis among schoolchildren in Golog Tibetan Autonomous Prefecture, Qinghai, China. Am J Trop Med Hyg 96:674–679. doi: 10.4269/ajtmh.16-0479[↩]
- Torgerson PR, Keller K, Magnotta M, Ragland N. 2010. The global burden of alveolar echinococcosis. PLoS Negl Trop Dis 4:e722. doi: 10.1371/journal.pntd.0000722[↩]
- Craig P. 2003. Echinococcus multilocularis. Curr Opin Infect Dis 16:437–444. doi: 10.1097/01.qco.0000092815.64370.39[↩]
- Abdybekova A, Sultanov A, Karatayev B, Zhumabayeva A, Shapiyeva Z, Yeshmuratov T, Toksanbayev D, Shalkeev R, Torgerson PR. 2015. Epidemiology of echinococcosis in Kazakhstan: an update. J Helminthol 89:647–650. doi: 10.1017/S0022149X15000425[↩]
- Torgerson PR. 2013. The emergence of echinococcosis in central Asia. Parasitology 140:1667–1673. doi: 10.1017/S0031182013000516[↩]
- Counotte MJ, Minbaeva G, Usubalieva J, Abdykerimov K, Torgerson PR. 2016. The burden of zoonoses in Kyrgyzstan: a systematic review. PLoS Negl Trop Dis 10:e0004831. doi: 10.1371/journal.pntd.0004831[↩]
- Usubalieva J, Minbaeva G, Ziadinov I, Deplazes P, Torgerson PR. 2013. Human alveolar echinococcosis in Kyrgyzstan. Emerg Infect Dis 19:1095–1097. doi: 10.3201/eid1907.121405[↩]
- Beerli O, Guerra D, Baltrunaite L, Deplazes P, Hegglin D. 2017. Microtus arvalis and Arvicola scherman: key players in the Echinococcus multilocularis life cycle. Front Vet Sci 4:216. doi: 10.3389/fvets.2017.00216[↩]
- Berke O, Romig T, von Keyserlingk M. 2008. Emergence of Echinococcus multilocularis among red foxes in northern Germany, 1991-2005. Vet Parasitol 155:319–322. doi: 10.1016/j.vetpar.2008.05.017[↩]
- Vuitton DA, Demonmerot F, Knapp J, Richou C, Grenouillet F, Chauchet A, Vuitton L, Bresson-Hadni S, Millon L. 2015. Clinical epidemiology of human AE in Europe. Vet Parasitol 213:110–120. doi: 10.1016/j.vetpar.2015.07.036[↩]
- Marcinkutė A, Šarkūnas M, Moks E, Saarma U, Jokelainen P, Bagrade G, Laivacuma S, Strupas K, Sokolovas V, Deplazes P. 2015. Echinococcus infections in the Baltic region. Vet Parasitol 213:121–131. doi: 10.1016/j.vetpar.2015.07.032[↩]
- Gottstein B, Stojkovic M, Vuitton DA, Millon L, Marcinkute A, Deplazes P. 2015. Threat of alveolar echinococcosis to public health—a challenge for Europe. Trends Parasitol 31:407–412. doi: 10.1016/j.pt.2015.06.001[↩]
- Massolo A, Liccioli S, Budke C, Klein C. 2014. Echinococcus multilocularis in North America: the great unknown. Parasite 21:73. doi: 10.1051/parasite/2014069[↩]
- Catalano S, Lejeune M, Liccioli S, Verocai GG, Gesy KM, Jenkins EJ, Kutz SJ, Fuentealba C, Duignan PJ, Massolo A. 2012. Echinococcus multilocularis in urban coyotes, Alberta, Canada. Emerg Infect Dis 18:1625–1628. doi: 10.3201/eid.1810.120119[↩]
- Romig T, Deplazes P, Jenkins D, Giraudoux P, Massolo A, Craig PS, Wassermann M, Takahashi K, de la Rue M. 2017. Ecology and life cycle patterns of Echinococcus species. Adv Parasitol 95:213–314. doi: 10.1016/bs.apar.2016.11.002[↩]
- Eckert J, Thompson RC. 2017. Historical aspects of echinococcosis. Adv Parasitol 95:1–64. doi: 10.1016/bs.apar.2016.07.003[↩]
- Debourgogne A, Blanchet D, Fior A, Umhang G, Simon S, Aznar C. 2017. Neotropical echinococcosis caused by Echinococcus vogeli in a 6-year-old child: the second case report in humans in French Guiana. Paediatr Int Child Health 37:63–65. doi: 10.1179/2046905515Y.0000000054[↩]
- Knapp J, Chirica M, Simonnet C, Grenouillet F, Bart JM, Sako Y, Itoh S, Nakao M, Ito A, Millon L. 2009. Echinococcus vogeli infection in a hunter, French Guiana. Emerg Infect Dis 15:2029–2031. doi: 10.3201/eid1512.090940[↩]
- Siles-Lucas M, Casulli A, Conraths FJ, Müller N. 2017. Laboratory diagnosis of Echinococcus spp. in human patients and infected animals. Adv Parasitol 96:159–257. doi: 10.1016/bs.apar.2016.09.003[↩]
- McManus DP, Gray DJ, Zhang W, Yang Y. 2012. Diagnosis, treatment, and management of echinococcosis. BMJ 344:e3866. doi: 10.1136/bmj.e3866[↩]
- Romig T, Omer RA, Zeyhle E, Huttner M, Dinkel A, Siefert L, Elmahdi IE, Magambo J, Ocaido M, Menezes CN, Ahmed ME, Mbae C, Grobusch MP, Kern P. 2011. Echinococcosis in sub-Saharan Africa: emerging complexity. Vet Parasitol 181:43–47. doi: 10.1016/j.vetpar.2011.04.022[↩]
- Craig PS, Hegglin D, Lightowlers MW, Torgerson PR, Wang Q. Echinococcosis: control and prevention. Adv Parasitol. 2017;96:55-158. doi: 10.1016/bs.apar.2016.09.002[↩][↩]
- Heath D.D., Jensen O., Lightowlers M.W. Progress in control of echinococcosis using vaccination–—a review of formulation and delivery of the vaccine and recommendations for practical use in control programs. Acta Trop. 2003;85:133–143. doi: 10.1016/s0001-706x(02)00219-x[↩]
- Zhang W., Zhang Z., Shi B., Li J., You H., Tulson G. Vaccination of dogs against Echinococcus granulosus, the cause of cystic hydatid disease in humans. J. Infect. Dis. 2006;194:966–974. doi: 10.1086/506622[↩]
- Symeonidis N, Pavlidis T, Baltatzis M, Ballas K, Psarras K, Marakis G, Sakantamis A. Complicated liver echinococcosis: 30 years of experience from an endemic area. Scand J Surg. 2013;102(3):171-7. doi: 10.1177/1457496913491877[↩]
- Ammann R., Eckert J. Cestodes. Echinococcus. Gastroenterol. Clin. North Am. 1996;25:655–689. doi: 10.1016/s0889-8553(05)70268-5[↩]
- McManus DP, Zhang W, Li J, Bartley PB. Echinococcosis. Lancet. 2003 Oct 18;362(9392):1295-304. doi: 10.1016/S0140-6736(03)14573-4[↩]
- Moro P, Schantz PM. Echinococcosis: a review. Int J Infect Dis. 2009 Mar;13(2):125-33. doi: 10.1016/j.ijid.2008.03.037[↩]
- Lewall D.B., Mc Corkell S.J. Rupture of echinococcal cysts:diagnosis, classification and clinical implications. Am. J. Roentgenol. 1986;146:391–394. doi: 10.2214/ajr.146.2.391[↩]
- Langer JC, Rose DB, Keystone JS, Taylor BR, Langer B. Diagnosis and management of hydatid disease of the liver. A 15-year North American experience. Ann Surg. 1984 Apr;199(4):412-7. https://pmc.ncbi.nlm.nih.gov/articles/instance/1353359/pdf/annsurg00122-0050.pdf[↩]
- Hosch W, Junghanss T, Stojkovic M, Brunetti E, Heye T, Kauffmann GW, Hull WE. Metabolic viability assessment of cystic echinococcosis using high-field 1H MRS of cyst contents. NMR Biomed. 2008 Aug;21(7):734-54. doi: 10.1002/nbm.1252[↩]
- Romig T, Zeyhle E, Macpherson CN, Rees PH, Were JB. Cyst growth and spontaneous cure in hydatid disease. Lancet. 1986 Apr 12;1(8485):861. doi: 10.1016/s0140-6736(86)90974-8[↩]
- Frider B, Larrieu E, Odriozola M. Long-term outcome of asymptomatic liver hydatidosis. J Hepatol. 1999 Feb;30(2):228-31. doi: 10.1016/s0168-8278(99)80066-x[↩]
- Wang Y, He T, Wen X, Li T, Waili A, Zhang W, Xu X, Vuitton DA, Rogan MT, Wen H, Craig PS. Post-survey follow-up for human cystic echinococcosis in northwest China. Acta Trop. 2006 Apr;98(1):43-51. doi: 10.1016/j.actatropica.2006.01.009[↩]
- Müfit K, Nejat I, Mercan S, Ibrahim K, Mete UY, Yüksel K. Growth of multiple hydatid cysts evaluated by computed tomography. J Clin Neurosci. 1998 Apr;5(2):215-7. doi: 10.1016/s0967-5868(98)90042-x[↩]
- Rogan MT, Hai WY, Richardson R, Zeyhle E, Craig PS. Hydatid cysts: does every picture tell a story? Trends Parasitol. 2006 Sep;22(9):431-8. doi: 10.1016/j.pt.2006.07.003[↩]
- Larrieu EJ, Frider B. Human cystic echinococcosis: contributions to the natural history of the disease. Ann Trop Med Parasitol. 2001 Oct;95(7):679-87. doi: 10.1080/00034980120094730[↩]
- Siracusano A, Bruschi F. Cystic echinococcosis: progress and limits in epidemiology and immunodiagnosis. Parassitologia. 2006 Jun;48(1-2):65-6.[↩][↩]
- Ito A, Craig PS. Immunodiagnostic and molecular approaches for the detection of taeniid cestode infections. Trends Parasitol. 2003 Sep;19(9):377-81. doi: 10.1016/s1471-4922(03)00200-9[↩][↩]
- Siles-Lucas MM, Gottstein BB. Molecular tools for the diagnosis of cystic and alveolar echinococcosis. Trop Med Int Health. 2001 Jun;6(6):463-75. doi: 10.1046/j.1365-3156.2001.00732.x[↩]
- Akisu C, Delibas SB, Bicmen C, Ozkoc S, Aksoy U, Turgay N. Comparative evaluation of western blotting in hepatic and pulmonary cystic echinococcosis. Parasite. 2006 Dec;13(4):321-6. doi: 10.1051/parasite/2006134321[↩]
- Macpherson CN, Milner R. Performance characteristics and quality control of community based ultrasound surveys for cystic and alveolar echinococcosis. Acta Trop. 2003 Feb;85(2):203-9. doi: 10.1016/s0001-706x(02)00224-3[↩]
- Khabiri AR, Bagheri F, Assmar M, Siavashi MR. Analysis of specific IgE and IgG subclass antibodies for diagnosis of Echinococcus granulosus. Parasite Immunol. 2006 Aug;28(8):357-62. doi: 10.1111/j.1365-3024.2006.00837.x[↩]
- Bygott JM, Chiodini PL. Praziquantel: neglected drug? Ineffective treatment? Or therapeutic choice in cystic hydatid disease? Acta Trop. 2009 Aug;111(2):95-101. doi: 10.1016/j.actatropica.2009.04.006[↩]
- WHO guidelines for the treatment of patients with cystic echinococcosis. Geneva: World Health Organization; 2025. Licence: CC BY-NC-SA 3.0 IGO https://iris.who.int/server/api/core/bitstreams/9f8adf1f-7f84-4d05-a13a-9c1adb503020/content[↩][↩]
- WHO guidelines for the treatment of patients with cystic echinococcosis [Internet]. Geneva: World Health Organization; 2025. Executive summary. Available from: https://www.ncbi.nlm.nih.gov/books/NBK616284[↩][↩]
- Kern P, Menezes da Silva A, Akhan O, Mullhaupt B, Vizcaychipi KA, Budke C, et al. The echinococcoses: diagnosis, clinical management and burden of disease. Adv Parasitol. 2017;96:259–369. doi: 10.1016/bs.apar.2016.09.006[↩][↩]
- Akhan O, Yildiz AE, Akinci D, Yildiz BD, Ciftci T. Is the adjuvant albendazole treatment really needed with PAIR in the management of liver hydatid cysts? A prospective, randomized trial with short-term follow-up results. Cardiovasc Intervent Radiol. 2014;37(6):1568–74. doi: 10.1007/s00270-014-0840-2[↩][↩]
- Cobo F, Yarnoz C, Sesma B, Fraile P, Aizcorbe M, Trujillo R, Diaz-de-Liaño A, Ciga MA. Albendazole plus praziquantel versus albendazole alone as a pre-operative treatment in intra-abdominal hydatisosis caused by Echinococcus granulosus. Trop Med Int Health. 1998 Jun;3(6):462-6. doi: 10.1046/j.1365-3156.1998.00257.x[↩]
- Keong B, Wilkie B, Sutherland T, Fox A. Hepatic cystic echinococcosis in Australia: an update on diagnosis and management. ANZ J Surg. 2018 Jan;88(1-2):26-31. doi: 10.1111/ans.14117[↩][↩][↩][↩]
- Dehkordi AB, Sanei B, Yousefi M, Sharafi SM, Safarnezhad F, Jafari R, Darani HY. Albendazole and Treatment of Hydatid Cyst: Review of the Literature. Infect Disord Drug Targets. 2019;19(2):101-104. doi: 10.2174/1871526518666180629134511[↩][↩]
- Velasco-Tirado V, Alonso-Sardón M, Lopez-Bernus A, Romero-Alegría Á, Burguillo FJ, Muro A, Carpio-Pérez A, Muñoz Bellido JL, Pardo-Lledias J, Cordero M, Belhassen-García M. Medical treatment of cystic echinococcosis: systematic review and meta-analysis. BMC Infect Dis. 2018 Jul 5;18(1):306. doi: 10.1186/s12879-018-3201-y[↩][↩][↩][↩]
- Akhan O, Yildiz AE, Akinci D, Yildiz BD, Ciftci T. Is the adjuvant albendazole treatment really needed with PAIR in the management of liver hydatid cysts? A prospective, randomized trial with short-term follow-up results. Cardiovasc Intervent Radiol. 2014 Dec;37(6):1568-74. doi: 10.1007/s00270-014-0840-2[↩][↩]
- Stojković M, Weber TF, Junghanss T. Clinical management of cystic echinococcosis: state of the art and perspectives. Curr Opin Infect Dis. 2018 Oct;31(5):383-392. doi: 10.1097/QCO.0000000000000485[↩][↩]
- Rashid MM, Rabbi H, Ahmed AT, et al. Outcome of surgically treated 79 patients of hepatic hydatidosis: a single center tertiary care hospital experience in Bangladesh. J Surg Sci 2020; 22: 118–124.[↩][↩]
- Mönnink GLE, Stijnis C, van Delden OM, Spijker R, Grobusch MP. Percutaneous Versus Surgical Interventions for Hepatic Cystic Echinococcosis: A Systematic Review and Meta-Analysis. Cardiovasc Intervent Radiol. 2021 Nov;44(11):1689-1696. doi: 10.1007/s00270-021-02911-4[↩][↩]
- Turgut B, Öncü F. The conversion time of cysts to inactive form after percutaneous treatment of hepatic hydatid disease and predisposing factors in this process. Haseki Tip Bul 2020; 58: 286–292.[↩]
- Öztürk G, Uzun MA, Özkan ÖF, Kayaalp C, Tatlı F, Eren S, Aksungur N, Çoker A, Bostancı EB, Öter V, Kaya E, Taşar P. Turkish HPB Surgery Association consensus report on hepatic cystic Echinococcosis (HCE). Turk J Surg. 2022 Jun 29;38(2):101-120. doi: 10.47717/turkjsurg.2022.5757[↩][↩][↩][↩][↩]
- Köroğlu M, Erol B, Gürses C, Türkbey B, Baş CY, Alparslan AŞ, Köroğlu BK, Toslak İE, Çekiç B, Akhan O. Hepatic cystic echinococcosis: percutaneous treatment as an outpatient procedure. Asian Pac J Trop Med. 2014 Mar;7(3):212-5. doi: 10.1016/S1995-7645(14)60023-7[↩][↩]
- Kahriman G, Ozcan N, Dogan S, Karaborklu O. Percutaneous treatment of liver hydatid cysts in 190 patients: a retrospective study. Acta Radiol. 2017 Jun;58(6):676-684. doi: 10.1177/0284185116664226[↩][↩]
- Khuroo MS. Percutaneous Drainage in Hepatic Hydatidosis-The PAIR Technique: Concept, Technique, and Results. J Clin Exp Hepatol. 2021 Sep-Oct;11(5):592-602. doi: 10.1016/j.jceh.2021.05.005[↩][↩]
- Balli O, Balli G, Cakir V, Gur S, Pekcevik R, Tavusbay C, Akhan O. Percutaneous Treatment of Giant Cystic Echinococcosis in Liver: Catheterization Technique in Patients with CE1 and CE3a. Cardiovasc Intervent Radiol. 2019 Aug;42(8):1153-1159. doi: 10.1007/s00270-019-02248-z[↩][↩][↩]
- Akhan O, Salik AE, Ciftci T, Akinci D, Islim F, Akpinar B. Comparison of Long-Term Results of Percutaneous Treatment Techniques for Hepatic Cystic Echinococcosis Types 2 and 3b. AJR Am J Roentgenol. 2017 Apr;208(4):878-884. doi: 10.2214/AJR.16.16131[↩]
- Akhan O, Erdoğan E, Ciftci TT, Unal E, Karaağaoğlu E, Akinci D. Cystobiliary Fistula of Liver CE Treatment as a Major Problem. Cardiovasc Intervent Radiol. 2020 Nov;43(11):1718-1719. doi: 10.1007/s00270-020-02631-1[↩]
- Akhan O, Erdoğan E, Ciftci TT, Unal E, Karaağaoğlu E, Akinci D. Comparison of the Long-Term Results of Puncture, Aspiration, Injection and Re-aspiration (PAIR) and Catheterization Techniques for the Percutaneous Treatment of CE1 and CE3a Liver Hydatid Cysts: A Prospective Randomized Trial. Cardiovasc Intervent Radiol. 2020 Jul;43(7):1034-1040. doi: 10.1007/s00270-020-02477-7[↩]
- Akhan O, Gumus B, Akinci D, Karcaaltincaba M, Ozmen M. Diagnosis and percutaneous treatment of soft-tissue hydatid cysts. Cardiovasc Intervent Radiol. 2007 May-Jun;30(3):419-25. doi: 10.1007/s00270-006-0153-1[↩]
- Calame P, Weck M, Busse-Cote A, Brumpt E, Richou C, Turco C, Doussot A, Bresson-Hadni S, Delabrousse E. Role of the radiologist in the diagnosis and management of the two forms of hepatic echinococcosis. Insights Imaging. 2022 Apr 8;13(1):68. doi: 10.1186/s13244-022-01190-y[↩]
- Mihmanli M, Tanal M, Bozkurt E, et al. The surgical management of hydatid cyst of the liver: what is new? In: Derbel F, Braiki M. (eds) Overview on echinococcosis. 2020. https://www.intechopen.com/chapters/70728[↩][↩][↩]
- Julien C, Le Treut YP, Bourgouin S, Palen A, Hardwigsen J. Closed Cyst Resection for Liver Hydatid Disease: a New Standard. J Gastrointest Surg. 2021 Feb;25(2):436-446. doi: 10.1007/s11605-019-04509-1[↩][↩]
- Deo KB, Kumar R, Tiwari G, Kumar H, Verma GR, Singh H. Surgical management of hepatic hydatid cysts – conservative versus radical surgery. HPB (Oxford). 2020 Oct;22(10):1457-1462. doi: 10.1016/j.hpb.2020.03.003[↩]
- Illuri HR, Souza CD, Dias EAI, et al. Hydatid disease: a 2 years retrospective study in a tertiary care center in South India. Int Surg J 2018; 5: 602.[↩]
- Vagholkar K, Pawanarkar A, Chougle Q, et al. Surgery for intra-abdominal hydatid disease: a single centre experience. Int J Res Med Sci 2016; 4: 4241–4245.[↩][↩]
- Brunetti E., Kern P., Vuitton D.A. Writing Panel for the WHO-IWGE. Expert consensus for the diagnosis and treatment of cystic and alveolar echinococcosis in humans. Acta Trop. 2010;114:1–16. doi: 10.1016/j.actatropica.2009.11.001[↩]
- Neumayr A, Tamarozzi F, Goblirsch S, Blum J, Brunetti E. Spinal cystic echinococcosis–a systematic analysis and review of the literature: part 2. Treatment, follow-up and outcome. PLoS Negl Trop Dis. 2013 Sep 19;7(9):e2458. doi: 10.1371/journal.pntd.0002458[↩][↩]
- Mansfield BS, Pieton K, Pather S. Spinal Cystic Echinococcosis. Am J Trop Med Hyg. 2019 Jan;100(1):9-10. doi: 10.4269/ajtmh.18-0588[↩]
- Sayek I, Tirnaksiz MB, Dogan R. Cystic hydatid disease: current trends in diagnosis and management. Surg Today. 2004;34(12):987-96. doi: 10.1007/s00595-004-2830-5[↩]
- Dhar P, Chaudhary A, Desai R, Agarwal A, Sachdev A. Current trends in the diagnosis and management of cystic hydatid disease of the liver. J Commun Dis. 1996 Dec;28(4):221-30.[↩]
- Bouraoui H, Trimeche B, Mahdhaoui A, Majdoub A, Zaaraoui J, Hajri Ernez S, Gouider J, Ammar H. Echinococcosis of the heart: clinical and echocardiographic features in 12 patients. Acta Cardiol. 2005 Feb;60(1):39-41. doi: 10.2143/AC.60.1.2005047[↩]





{kind=link}