Contents
What is hyphema
Hyphema is accumulation blood in the front area (anterior chamber) of the eye. The blood collects behind the cornea (the clear covering of the eye) and in front of the iris (the colored part of the eye). The blood may cover part or all of the iris and the pupil (the round, dark circle in the middle of your eye). If you have a hyphema, your vision might be partly or totally blocked in that eye.
A hyphema usually happens when an injury causes a tear of the iris or pupil of the eye. Sometimes people mistake a broken blood vessel in the front of the eye for a hyphema. A broken blood vessel in the eye is a common, harmless condition called subconjunctival hemorrhage. A subconjunctival hemorrhage does not hurt. A hyphema, though, is usually painful. A hyphema must be treated properly or it can cause permanent vision problems.
A small amount of blood that is only evident under close microscopic examination is referred to as a microhyphema. A majority of patients present with a history that correlates to the cause. A history of trauma or recent ocular surgery are the most common risk factors. However, a seemingly spontaneous hyphema can result at times from other causes. A comprehensive eye exam is mandatory in every case of hyphema looking for other complications of trauma such as ruptured globe, traumatic optic neuropathy or retinal detachments. Despite the degree or cause, the management of a hyphema and its associated complications can be challenging for any ophthalmologist.
Based on what the ophthalmologist finds, he or she may ask you to:
- wear a special shield over your eye to protect it
- cut back on physical activity, or to rest in bed
- raise the head of your bed to help your eye drain
- see your ophthalmologist often so he or she can check your healing and eye pressure. He or she may prescribe eye drops to decrease the swelling inside your eye and to ease the pain or discomfort.
Your ophthalmologist may tell you not to use aspirin because it can lead to more bleeding. In some cases, your ophthalmologist might tell you to go to the hospital so that your eye can be cared for and checked often. If the hyphema makes your eye pressure rise too high, it can lead to glaucoma or damage your cornea. If this happens, you may need surgery to remove the excess blood or eye drops for treatment.
Figure 1. Eye anatomy
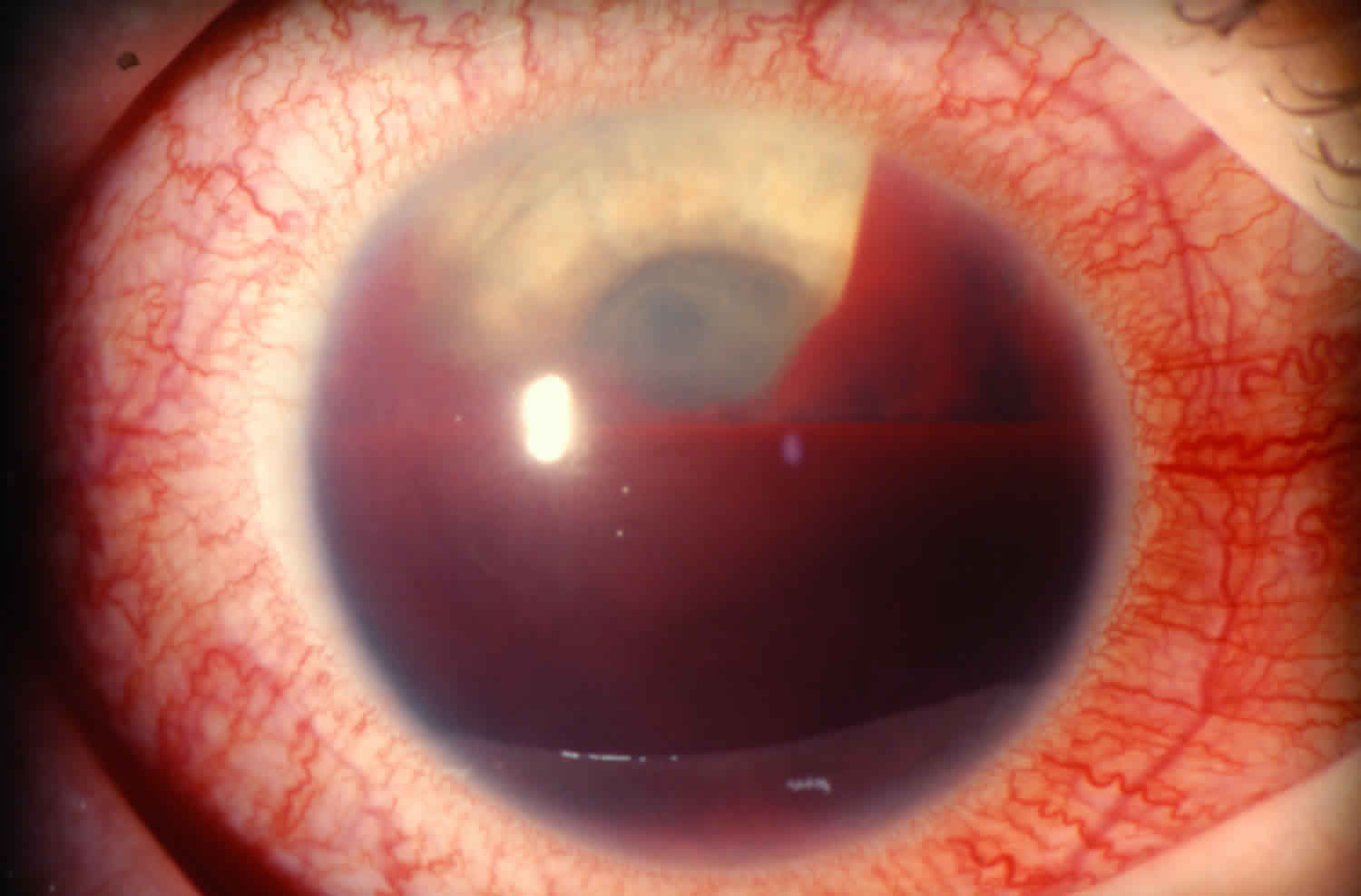
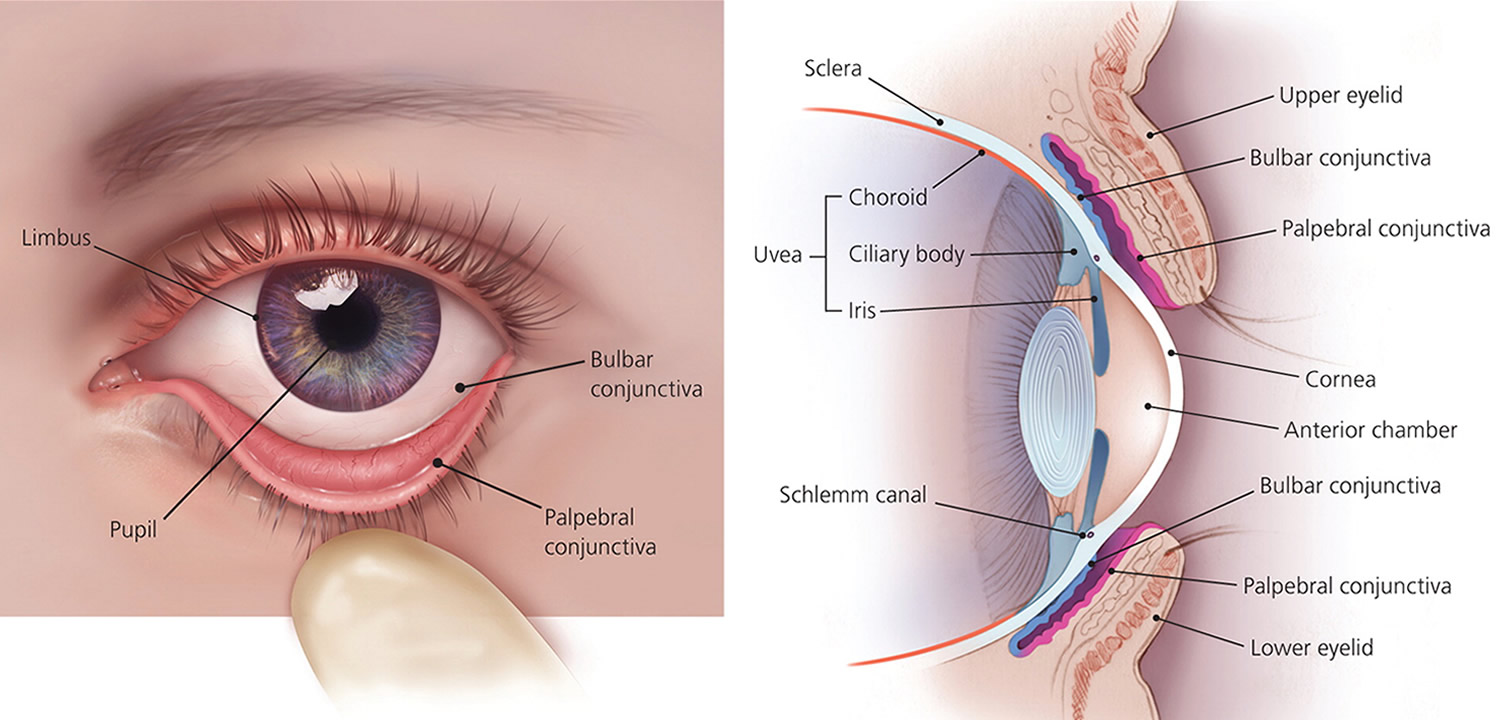 Figure 2. Traumatic hyphema
Figure 2. Traumatic hyphema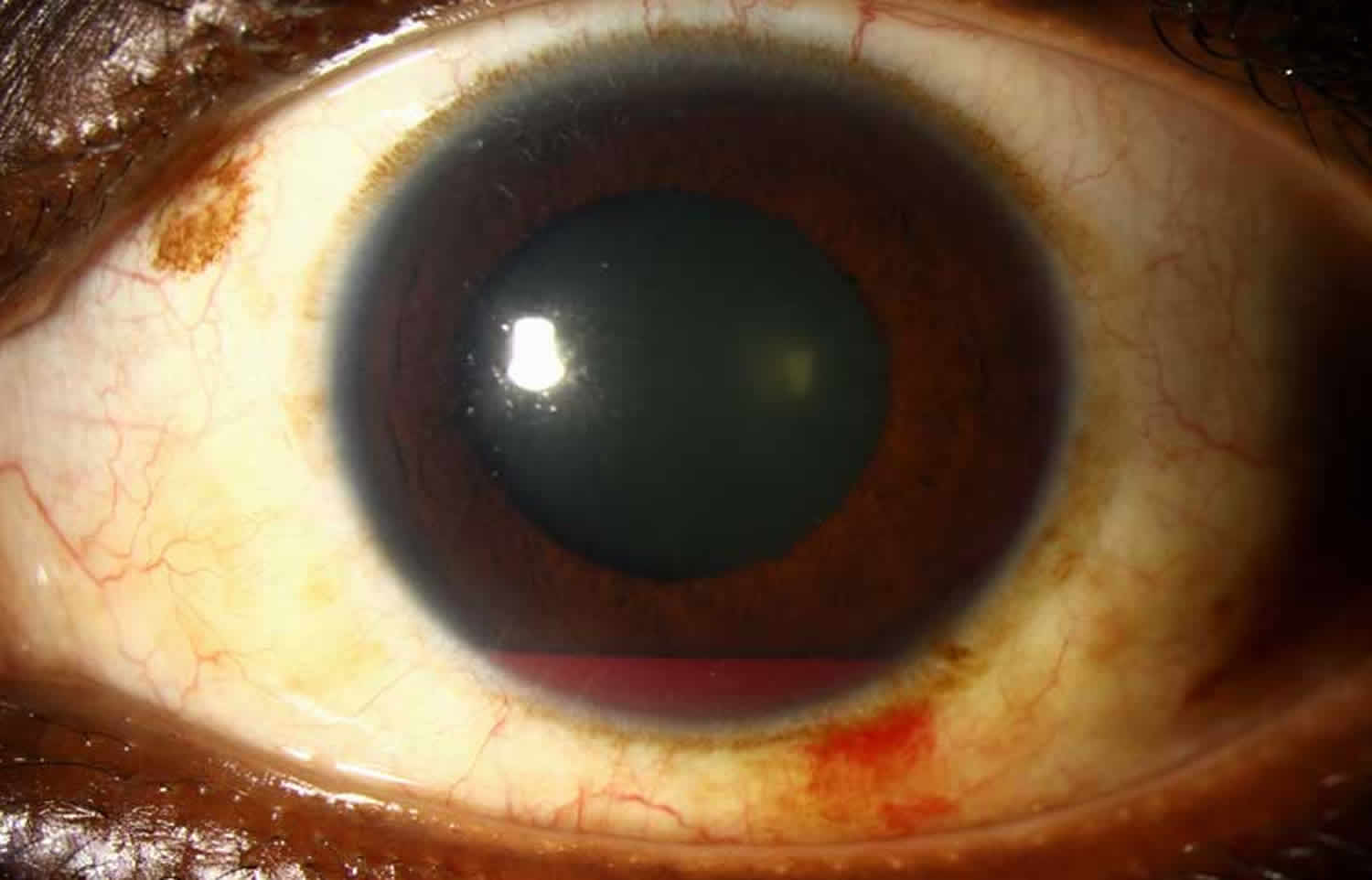
Hyphema grading
The severity of the hyphema can either be measured by the depth of settled red blood cells at the base of the anterior chamber or graded on a scale of zero to four as below 1.
- Grade 0 or “microhyphema”: Rare cells visible within the anterior chamber (microhyphema) only in slit lamp examination, no layering of cells
- Grade 1 Hyphema: Hyphema with cells visible floating in the anterior chamber. Layering of cells at base of anterior chamber, measuring less than one third of the anterior chamber.
- Grade 2 Hyphema: Layering of cells at the base of the anterior chamber, measuring between one third to one half of the anterior chamber.
- Grade 3 Hyphema: Layering of cells at the base of the anterior chamber, measuring greater than one half to less than total of the anterior chamber but not occupying its entirety.
- Grade 4 Hyphema: Total filling of the anterior chamber with blood. If the anterior chamber is completely filled with bright red blood it is called a total hyphema. If the anterior chamber is filled with dark red-black blood it is called a “black ball” or “8-ball” hyphema. The black color is suggestive of impaired aqueous circulation and decreased oxygen concentration. This distinction is important because an eight ball hyphema is more likely to cause pupillary block and secondary angle closure 2.
Grading hyphemas has value because the risk for intraocular pressure elevation increases with larger hyphemas, with the exception being in Sickle cell cases where even a small amount of red blood cells can elevate intraocular pressure. Coles 3, in his series of 235 cases noted that the risk of elevated intraocular pressure went up dramatically for those whose hyphemas filled more than 50% of the anterior chamber or a grade 3 hyphema. Only 13.5% of Grade 1 to 2 hyphemas had an intraocular pressure increase, but 27% of those with Grade 3 hyphemas has an intraocular pressure increase. Grade 4 hyphemas were even more so with 52% experiencing an intraocular pressure increase. Also, cases with rebleeding had a more than 50% chance of having elevated intraocular pressure.
Figure 3. Grade 1 Hyphema
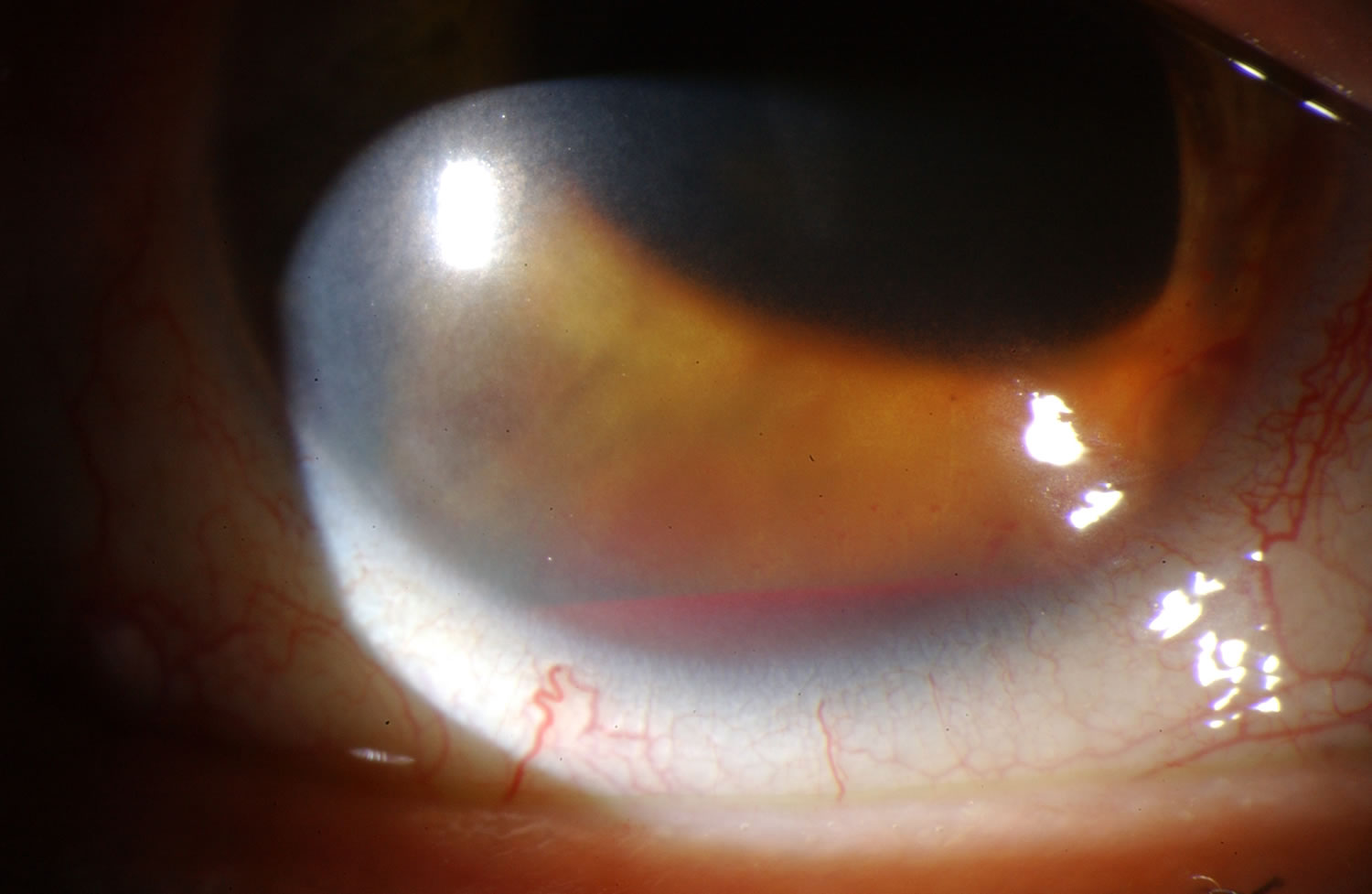
Figure 4. Grade 3 Hyphema

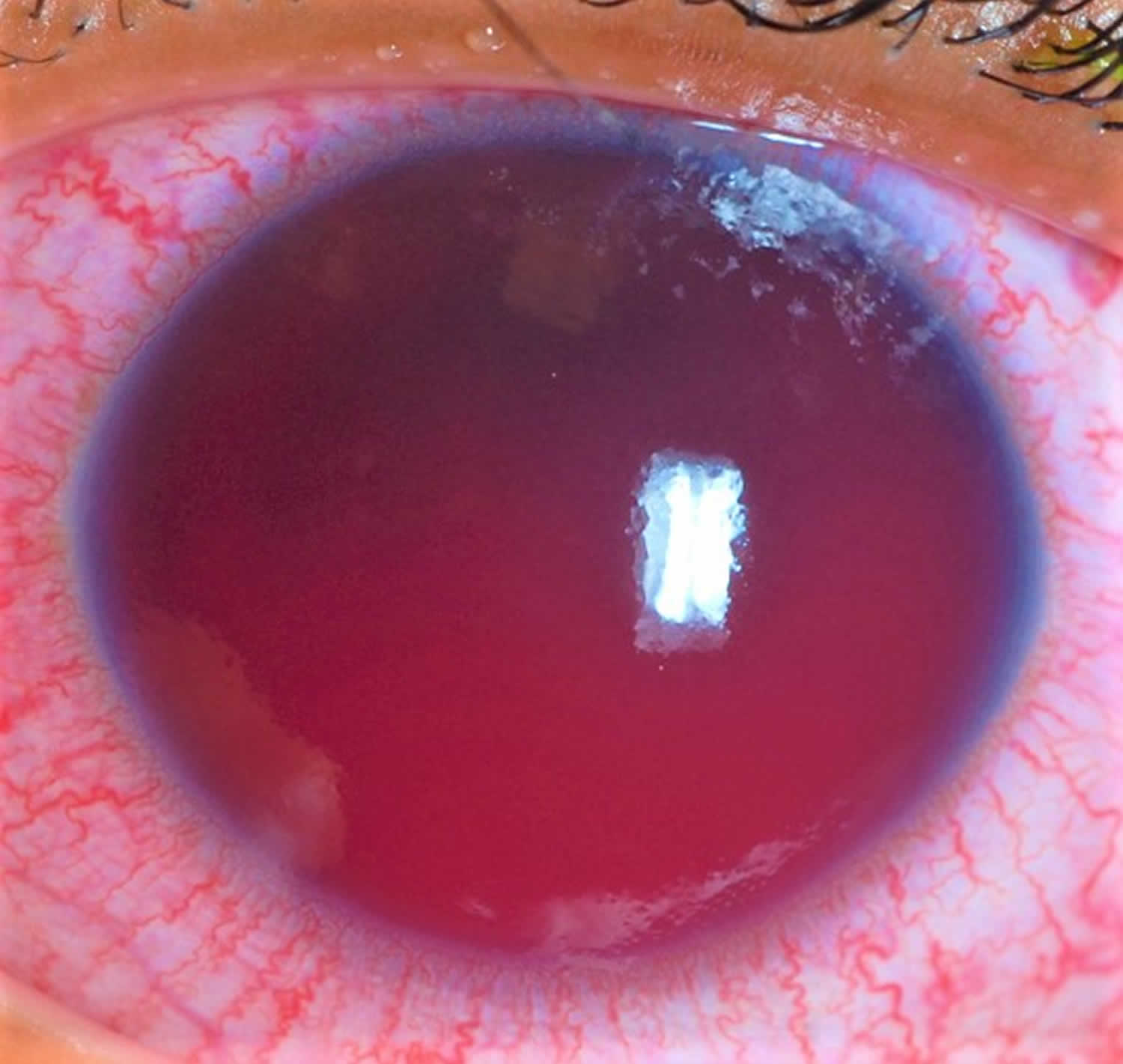
Figure 5. Eight ball hyphema
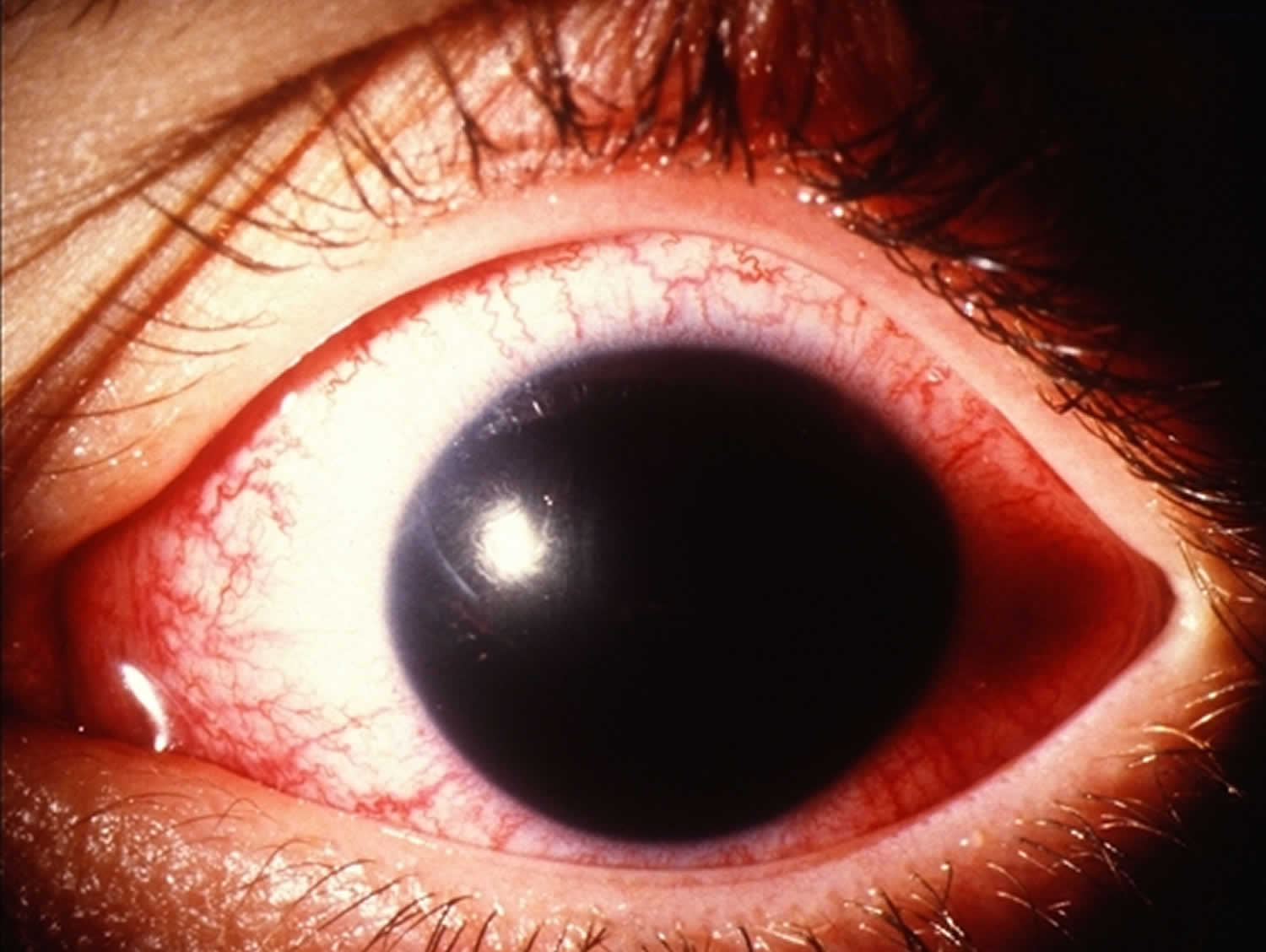
Figure 6. Total hyphema
Hyphema recovery time
A hyphema can take several months to clear completely from the front of the eye. The larger the hyphema, the longer it can take to clear.
A condition known as corneal blood staining can occur where the blood products leave a scar over the pupil. The pupil can also be fixed with dilation in severe cases. If the hyphema does not clear completely, the blood products can be rinsed from the eye with a procedure known as an anterior chamber washout. If blood staining of the cornea occurs, it may require corneal transplant surgery to remove, but the condition should be observed for at least six months before moving forward with surgery. If the pressure in the eye is elevated and blood remains, it is usually a good idea to do the washout.
Hyphema causes
Hyphema is most often caused by blunt or lacerating trauma to the eye from accidents or playing sports. Blunt trauma is the most common cause of a hyphema. Compressive force to the globe can result in injury to the iris, ciliary body, trabecular meshwork, and their associated vasculature. The shearing forces from the injury can tear these vessels and result in the accumulation of red blood cells within the anterior chamber. Because most hyphemas happen because of sports injuries, it is important to wear protective eyewear. Sports injuries, especially with small balls like racquetballs, can cause serious eye problems. Besides hyphema, these injuries can cause cataracts, retinal detachments and glaucoma and lead to blindness. If you hurt your eye, see an ophthalmologist right away.
Hyphema can also occur after intraocular surgery, spontaneously (e.g., in conditions such as rubeosis iridis, juvenile xanthogranuloma, iris melanoma, myotonic dystrophy, keratouveitis (e.g., herpes zoster), leukemia, hemophilia, von Willebrand disease, and in association with the use of substances that alter platelet or thrombin function (e.g., ethanol, aspirin, warfarin) 4.
Hyphemas can also be iatrogenic in nature. Intraoperative or postoperative hyphema is a well known complication to any ocular surgery. Rarely, the placement of an intraocular lens within the anterior chamber can result in chronic inflammation, secondary iris neovascularization, and recurrent hyphemas, known as uveitis-glaucoma-hyphema syndrome 5. This is a direct result of a malpositioned or rotating anterior chamber intraocular lens. This condition has also been reported in posterior chamber, sulcus, and suture-fixated intraocular lenses 6. Additionally, a hyphema resulting from an ocular laser procedure is a possible adverse event. Postlaser hyphema is not uncommon after the use of the Nd:YAG laser for a peripheral iridectomy. Typically the resulting hyphema is minimal and self-limited.
A spontaneous hyphema, commonly confused with a traumatic hyphema, is likely secondary to neovascularization (e.g., diabetes mellitus, ischemia, cicatrix formation), ocular neoplasms (e.g., retinoblastoma), uveitis, or vascular anomalies (e.g., juvenile xanthogranuloma) 7.
Hyphema can be caused by other, less common things, including:
- Abnormal blood vessels on the surface of the iris
- Severe inflammation of the iris
- Post-surgical hyphema: Surgical manipulation of the anterior structures of the eye may result in bleeding.
- Advanced diabetes: blood in the front of the eye could be a result of ruptured friable vessels that grow on the iris and in the angle in response to long-term retinal ischemia from diabetic retinopathy.
- Blood disorders such as sickle cell anemia
- Eye infections caused by a herpes virus – keratouveitis (e.g., herpes zoster)
- Blood clotting problems
- Problems with artificial lenses placed in the eye after cataract surgery
- Very rarely, cancers of the eye
Traumatic hyphema
Blunt trauma to the eye may result in injury to the iris, pupillary sphincter, angle structures, lens, zonules, retina, vitreous, optic nerve, and other intraocular structures. Blunt trauma to the eye is associated with a rapid, marked elevation in intraocular pressure with sudden distortion of intraocular structures.[8] As a result, normal vasculature within the anterior chamber is exposed to shearing forces that are responsible for hyphema formation.
Hyphema secondary to ocular surgery or laser
Hyphema is a risk factor for any intraocular surgery performed; however, rare in routine elective cases. The incidence is higher in patients with a past medical or ocular history that predisposes them to irregular vasculature within the anterior chamber (e.g., ocular ischemia and neovascularization).
Neovascularization
Abnormal blood vessel growth on the iris, ciliary body, or within the angle may lead to the development of a hyphema. Typically, this neovascularization is a direct result of posterior segment ischemia. Retinal microvascular disease in diabetic patients is by far the most common cause. Vascular endothelial growth factor (VEGF) up regulation from ischemic tissue disperses within the eye and allows for anterior segment neovascular growth. Retinal ischemia also can occur subsequently to retinal arterial or venous occlusion. Another cause of the neovascularization is carotid stenosis, which can lead to ocular ischemia (ocular ischemic syndrome) 7.
Neoplastic
Tumor growth is dependent on an extensive vascular supply. Ocular neoplastic disease such as melanoma (iris, ciliary body, and / or choroidal) or pediatric retinoblastoma can predispose patients to the development of a hyphema.
Inflammatory / Infectious
Common intraocular inflammatory conditions that can result in neovascularization and resultant hyphema are herpetic (herpes simplex virus and varicella-zoster virus) uveitis and Fuch’s heterochromic iridocyclitis.
Vascular anomaly
A rather rare disease that is commonly thought of when evaluating pediatric patients with a hyphema is juvenile xanthogranuloma. It is mainly a skin disorder characterized by a typically, raised, orange lesion, occurring either singly or in crops and regresses spontaneously with occasional involvement of the eyes. The most common ocular finding is diffuse or discrete iris nodules, which could be quite vascular and may bleed spontaneously, resulting in hyphema 8.
Hyphema symptoms
Symptoms associated with a hyphema can be variable depending on the cause. Typically patients will complain of associated blurry vision and ocular distortion. In the setting of trauma or secondary intraocular pressure elevation, patients may complain of pain, headahce, and photophobia.
Hyphema symptoms include:
- bleeding in the front of the eye
- sensitivity to light
- pain in the eye
- blurry, clouded or blocked vision
Hyphema complications
Patients with hyphemas may develop sudden jumps in their intraocular pressure putting them at risk for glaucomatous optic nerve damage and significant discomfort. Therefore, intraocular pressure needs to be monitored daily for several days following the injury.
- Obstruction of trabecular meshwork with associated intraocular pressure elevation
- Peripheral anterior synechiae (PAS)
- Posterior synechiae
- Corneal bloodstaining
- Rebleeding: Can occur when the initial clot retracts and lyses allowing for a second episode of bleeding. Rebleeds are generally more severe than the initial bleed, more likely to lead to glaucoma, corneal blood staining, and synechiae formation 2. It has been reported to occur 3.5% to 38% of the time 9 and probably 5-10% overall. It usually occurs within the first 5 days after the injury. Risk factors for rebleeding include hypotony or elevated intraocular pressure 10, 50% or greater hyphema 11, systemic hypertension 12, use of aspirin 13 and Black patients 14.
- Pupillary block
- Amblyopia (pediatric patients)
Hyphema prognosis
Hyphema prognosis is dependent on the cause and whether the patient developed an associated complication from the hyphema. These patients should be monitored closely to ensure adequate resolution of the hyphema without the development of visually debilitating complications. Additionally, patients with a history of ocular trauma require routine follow-up with gonioscopic examination because of the potential for development of angle-recession glaucoma.
Hyphema diagnosis
An ophthalmologists will examine your eye completely to diagnose a hyphema. He or she will check:
- how well you can see
- the pressure in your eye
- the inside of your eye
Diagnosis is made with slit-lamp examination of the anterior chamber. A large hyphema can be noted with pen-light examination alone.
A large hyphema can be noted with pen-light examination alone. The height and color of the hyphema should be documented. Height can be measured in millimeters from the inferior corneal limbus. Color can vary from red to black depending on the time frame of the hyphema. Blood that has clotted will appear darker in appearance (black). It is important to evaluate intraocular pressure.
In some cases, the ophthalmologist may order a CT scan. This scan checks the condition of the bones that form your eye sockets and other parts of your face.
History
A majority of patients will have a history consistent with recent ocular trauma or surgery. However, in the setting of a spontaneous hyphema further investigation may be required. It is important to ask the patient if they have a past history of bleeding diathesis or anticoagulation therapy, which can be a rare risk factor in the development of a hyphema. It is also important to discuss factors that may predispose the patient to ocular complications of a hyphema, such as a clotting disorders or sickle cell disease.
Sickle cell anemia is an especially important factor to consider. Red blood cells in this disease process can sickle in the anterior chamber causing them to become rigid and unable to easily escape through the trabecular meshwork. This leads to a much greater likelihood of elevated intraocular pressure 15. In addition, intravascular sickled red blood cells can cause catastrophic vaso-occlusive vents like central retinal artery occlusion and ischemic optic neuropathy even at mildly elevated intraocular pressure that would not otherwise be a threat to most eyes. Sickle cell anemia is much more common in those of African descent, perhaps as high as 10% 2. Even those with sickle trait are at risk, not just those with sickle cell disease.
Physical examination
The examination for a hyphema should consist of a routine ophthalmic work-up (visual acuity, pupillary examination, intraocular pressure, slit-lamp examination) as well as a gonioscopy to evaluate the condition of the angle and trabecular meshwork. This is important especially in the setting of ocular trauma to gain an understanding of the extent of the trauma. This can be delayed until after the critical 5-day, high-risk, re-bleed period, particularly when doing dynamic gonioscopy. Angle abnormalities such as peripheral anterior synechiae and angle recession may commonly be found 7. It is also critical to measure the height of the hyphema from the inferior limbus.
Laboratory test
All African American patients with a hyphema should be screened for sickle cell trait or disease with a sickle cell prep. A greater risk of trabecular meshwork obstruction with red blood cells exists while in the sickled state. Resultant elevated intraocular pressure levels put the patient at greater risk of permanent vision loss from optic nerve damage. Hemoglobin electrophoresis can be used as a confirmatory test for a positive sickle cell prep.
Hyphema treatment
Currently, there is no designated protocol for medical management of hyphemas. Uncomplicated hyphemas should be managed conservatively, with an eye shield, limited activity, and head elevation 5. A patient should be monitored closely during the first few days after injury as this is the highest risk time frame for rebleeding. Maintaining head elevation of at least 45 degrees will allow the hyphema to settle inferiorly within the anterior chamber. This avoids central visual obstruction, as well as limits both corneal endothelial and trabecular meshwork exposure to red blood cells. Most patients can be managed in an outpatient setting with close follow-up to evaluate vision, hyphema regression, and intraocular pressure. However, hospitalization should be considered for noncompliant patients, patients with bleeding diathesis or blood dyscrasia, patients with severe ocular or orbital injuries, and patients with concomitant intraocular pressure elevations with known sickle cell disease 16. Pain control for all patients with a hyphema should not include aspirin-containing products or NSAIDs, as these can increase the risk for further bleeding.
Medical Management
Medical treatment for an isolated hyphema typically is topical. Medicinal eye drops such as corticosteroids (e.g. prednisolone acetate) and cycloplegics (cyclopentolate or atropine) are most commonly used. Fibrinolytics, such as aminocaproic acid and tranexamic acid, have been extensively discussed in the literature, however sensitivity analyses have demonstrated that these medications minimally reduce the risk of secondary bleeding. Therefore, these drugs have fallen out of favor for treating hyphemas. Patients with hyphemas may develop sudden jumps in their intraocular pressure putting them at risk for glaucomatous optic nerve damage and significant discomfort. Therefore, intraocular pressure needs to be monitored daily for several days following the injury.
For cases of elevated intraocular pressure, first-line therapy includes the use of pressure-reducing medications. Of note, carbonic anhydrase inhibitors like dorzolamide are contraindicated in patients with sickle cell disease or trait, due to their effect on lowering pH which can induce sickling 5. Also, systemic hyperosmotic agents may induce a sickle crisis in dehydrated patients with sickle cell disease, and should be avoided in these patients for this reason. All patients should be questioned about their sickle cell status and if there is any possibility the patient could have sickle cell disease, hemoglobin analysis testing should be ordered to ascertain disease status of the patient.
Also, in those with sickle cell disease, adrenergic agonists with significant alpha-1 activity such as iopidine or apraclonidine are a concern as they may promote intravascular sickling by their vasoconstrictive and sugsequent deoxygenating properties 2.
Systemic and topical aminocaproic acid have been recommended in various studies as treatment options to avoid secondary hemorrhage in hyphema patients 17. Aminocaproic acid is a derivative and analog of the amino acid lysine, and competitively inhibits plasmin, an important protein enzyme involved in fibrinolysis. If secondary hemorrhages are the result of lysis and retraction of a clot that has produced an occlusion of the traumatized vessel, then prevention of normally occurring clot lysis for 5-6 days should be advantageous to allow the injured blood vessel to more completely repair its integrity 7. Tranexamic acid is another alternative. It is more potent than aminocaproic acid with fewer side effects 18. Antifibrinolytics such as aminocaproic acid and tranexamic acid are not routinely used in the treatment of hyphemas, but may be beneficial in patients at higher risk for rebleeding or other hyphema associated complications.
Due to the inherent association of hyphema with trauma, inflammation is classically seen in addition to red blood cells. Thus, topical steroids (systemic for severe cases), in addition to cycloplegics, are commonly prescribed to reduce inflammation and the risk of development of iris synechiae (iris scarring to lens or cornea). It is important to keep in mind that once symptoms of inflammation have resolved, topical steroids should be tapered to reduce the risk of steroid-induced glaucoma.
In addition to medication, preventative measures such as placing strict activity restrictions, maintaining an elevated position of the head and using an eye shield are highly recommended to encourage settling of red blood cells and to reduce risk of secondary bleeds. Patients with non-resolving clots, corneal blood staining, or uncontrolled elevated intraocular pressures may benefit from surgical evacuation of the clot or blood from the anterior chamber. All hyphema patients are at lifelong risk of glaucoma due to the damage to the trabecular meshwork from the injury and/or blood and need regular intraocular pressure checks for life.
If the intraocular pressure is not adequately controlled with medical management, or the patient develops further ocular complications (corneal blood staining, rebleed), surgical treatment may be necessary.
Surgery
A majority of hyphemas will resolve with medical management alone. Approximately 5 percent of patients with traumatic hyphema require surgery 19. The patient can typically be monitored for the first 4 days with medical treatment alone to allow for spontaneous resolution. After that point, surgical intervention may be indicated in the setting of uncontrolled glaucoma, corneal blood staining, the persistence of a large or total hyphema, and active bleeding in the anterior chamber 20. Uncontrolled intraocular hypertension is defined as greater than or equal to 50 mmHg for more than five days, or more than 25 mmHg for more than 24 hours in patients with sickle hemoglobinopathy despite maximal medical therapy 4. Patients with sickle cell hemoglobinopathies and even those with sickle cell trait require surgical intervention if intraocular pressure is not controlled within 24 hours 7. If a large hyphema results in complete visual obstruction in a pediatric patient, amblyopia could result. In these younger patients, early surgical intervention may be justified to avoid this visual complication.
Options for surgical intervention consist of anterior chamber irrigation and aspiration through a small incision (anterior chamber washout), hyphema evacuation with closed vitrectomy instrumentation, or clot irrigation with a filtering procedure (trabeculectomy). Additionally, an anterior chamber paracentesis can be performed for temporarizing control of elevevated intraocular pressure. If a total hyphema is present, it’s possible that pupillary block could occur, and a peripheral iridectomy may be indicated during the time of surgery. An anterior chamber washout with irrigation and aspiration is commonly performed first 5. If intraocular pressure remains uncontrolled, a trabeculectomy along with repeat anterior chamber washout is indicated. A trabeculectomy is generally not performed for smaller hyphemas, but is used by some clinicians as the initial surgical approach (with concomitant peripheral iridectomy and anterior chamber washout) 7.
Postoperative hyphemas may be seen at the time of surgery or within the first 2-3 days after surgery. If bleeding is identified intraoperatively, it must be identified and coagulated if it does not cease on its own 7.
- Hyphema. http://morancore.utah.edu/basic-ophthalmology-review/hyphema/[↩]
- Bazzaz S, Katz JL, Myers JS. Post-Traumatic Glaucoma. In: Shaarawy T, Sherwwod MB, Hitchings RA, Crowston JG, eds. Glaucoma: Medical Diagnosis and Therapy. Elsevier:2009:431-439.[↩][↩][↩][↩]
- Coles WH. Traumatic hyphema: an analysis of 235 cases. South Med J. 61:813-816. 1968.[↩]
- Walton W, et al. Management of traumatic hyphema. Survey of Ophthalmology. 2002 Jul-Aug; 47(4): 297-334.[↩][↩]
- Basic and Clinical Science Course. Glaucoma. pp 114-116; 2009-10.[↩][↩][↩][↩]
- Condon, Garry P. Single-Piece Syndrome. Glaucoma Today. June 2011.[↩]
- Sheppard, John D. Jr, et al. Hyphema. Medscape Reference. 2009.[↩][↩][↩][↩][↩][↩][↩]
- P Vijayalakshmi, et al. Bilateral spontaneous hyphaema in juvenile xanthogranuloma. Indian Journal of Ophthalmology. 2006. Vol 56 (1): 45-46.[↩]
- Volpe NJ, Larrison WI, Hersh PS, et al. Secondary hemorrhage in traumatic hyphema. Am J Ophthalmol 1991;112:507-513.[↩]
- Howard GM, Hutchinson BT, Frederick AR. Hyphema resulting from blunt trauma. Gonioscopic, tonographic, and ophthalmoscopic observations following resolution of the hemorrhage. Trans Am Acad Ophthalmol Otolaryngol. 69:294-306. 1965.[↩]
- Edwards WC, Layden WF: Traumatic hyphema. A report of 184 consecutive cases. Am J Ophthalmol. 75:110-116. 1973.[↩]
- Fong LP: Secondary hemorrhage in traumatic hyphema. Predictive factors for selective prophylaxis. Ophthalmology. 101:1583-1588. 1994.[↩]
- Ganley JP, Geiger JM, Clement JR, et al.: Aspirin and recurrent hyphema after blunt ocular trauma. Am J Ophthalmol 96:797-801. 1963.[↩]
- Spoor TC, Kwito GM, O’Grady JM, et al.: Traumatic hyphema in an urban population. Am J Ophthalmol. 109:23-27. 1990.[↩]
- Nasrullah A, Kerr NC: Sickle cell as a risk factor for secondary hemorrhage in children with traumatic hyphema. Am J Ophthalmol. 123:783-790. 1997.[↩]
- Ehlers, Justis P. and Shah, Chirag P. The Wills Eye Manual. Office and Emergency Room Diagnosis and Treatment of Eye Disease. 5th Edition. 2008. pp 20-22.[↩]
- Beiran, Itzchak, et al. Characteristics and Functional Outcome of Traumatic Hyphema without Routine Administration of Aminocaproic Acid. IMAJ. Nov 2002. Vol 4(1009-1010).[↩]
- Deans R, Noeel LP, Clarke WN: Oral administration of tranexamic acid in the management of traumatic hyphema in children. Can J Ophthalmol. 27:181-183 1992[↩]
- Andreoli, Christopher M., et al. Traumatic hyphema: Epidemiology, anatomy, and pathophysiology. UpToDate. 2011.[↩]
- Wilson FM. Traumatic hyphema: pathogenesis and management. Ophthalmology. 1980;87:910-919.[↩]





{kind=link}