Contents
What is a hysterosalpingogram
Hysterosalpingogram is an X-ray fluoroscopic examination of the Fallopian tubes and of the uterus (womb), most commonly used in the investigation of infertility or recurrent spontaneous abortions 1. Hysterosalpingogram involves an injection of opaque dye through the cervix into the uterus to outline any structural problems or blockages in your Fallopian tubes. In some cases the hysterosalpingogram procedure may help unblock Fallopian tubes. Blockages can prevent eggs passing down the Fallopian tubes to the womb, and stop pregnancy occurring.
Hysterosalpingogram (HSG) is a fluoroscopic examination of the uterus and the Fallopian tubes, most commonly used in the investigation of infertility or recurrent spontaneous abortions.
Hysterosalpingogram is often used to see if the fallopian tubes are partly or fully blocked. It also can show if the inside of the uterus is of a normal size and shape. All of these problems can lead to infertility and pregnancy problems.
Hysterosalpingogram also is used a few months after some tubal sterilization procedures to make sure that the fallopian tubes have been completely blocked.
Hysterosalpingogram is NOT done if a woman has any of the following conditions:
- Pregnancy
- Pelvic infection
- Heavy uterine bleeding at the time of the procedure
Detectable pathology
Conditions which may be detected with hysterosalpingogram include:
- Uterine
- uterine congenital anomalies
- submucosal uterine fibroids
- uterine malignancy
- adenomyosis
- intrauterine adhesions
- uterine (endometrial) polyps
- Tubal
- obliteration of fallopian tubes : usually secondary to previous pelvic inflammation. It must be differentiated from incomplete tubal opacification due to tubal spasm, or underfilling of the uterus with contrast 2
- tubal polyps 3
- tubal malignancy
- hydrosalpinx
- salpingitis isthmica nodosa (SIN) 4
- tubal spasm 3: can be physiological
- salpingectomy
Figure 1. Uterus anatomy (note: Uterine tube = Fallopian tube)
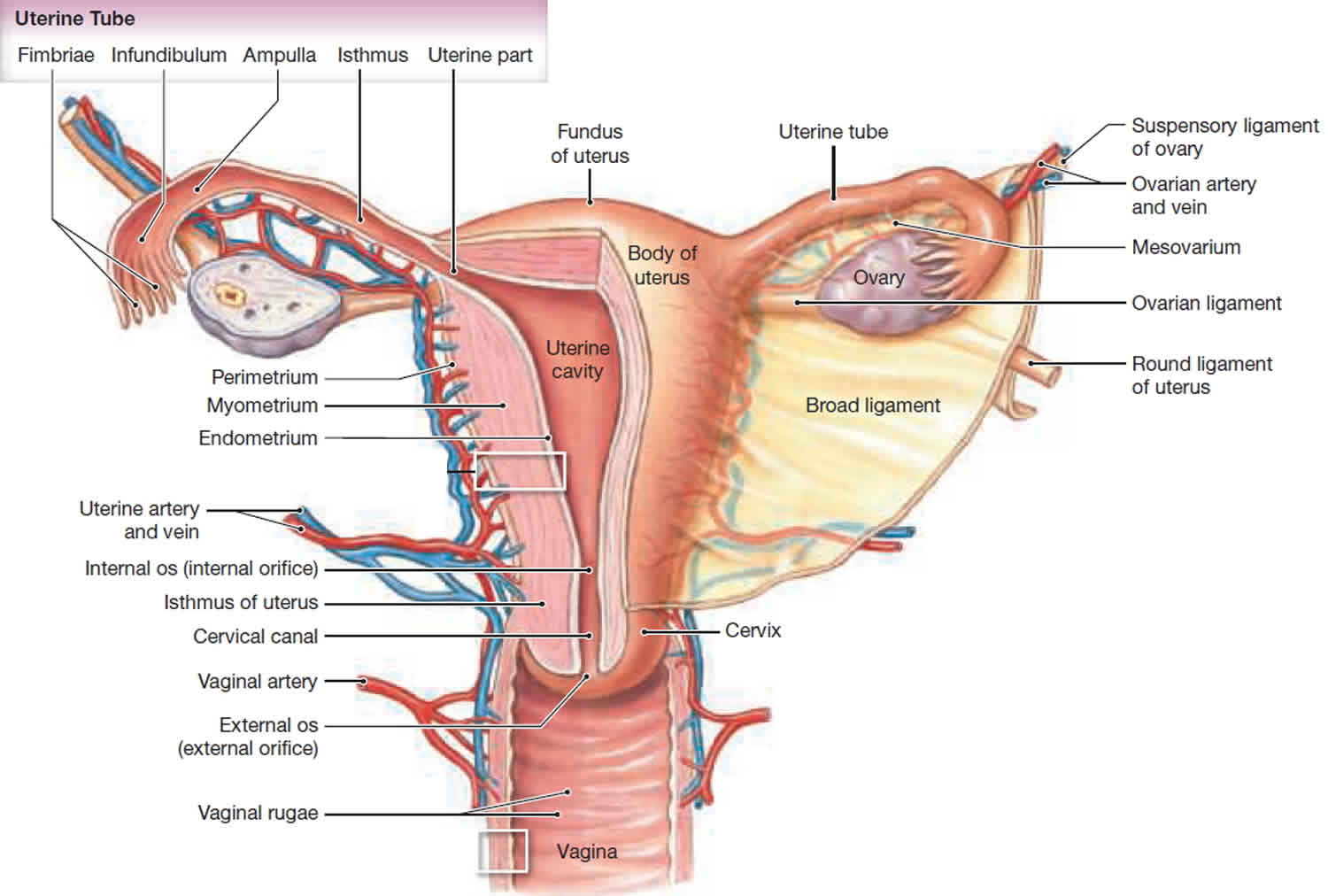
Figure 2. Normal hysterosalpingogram

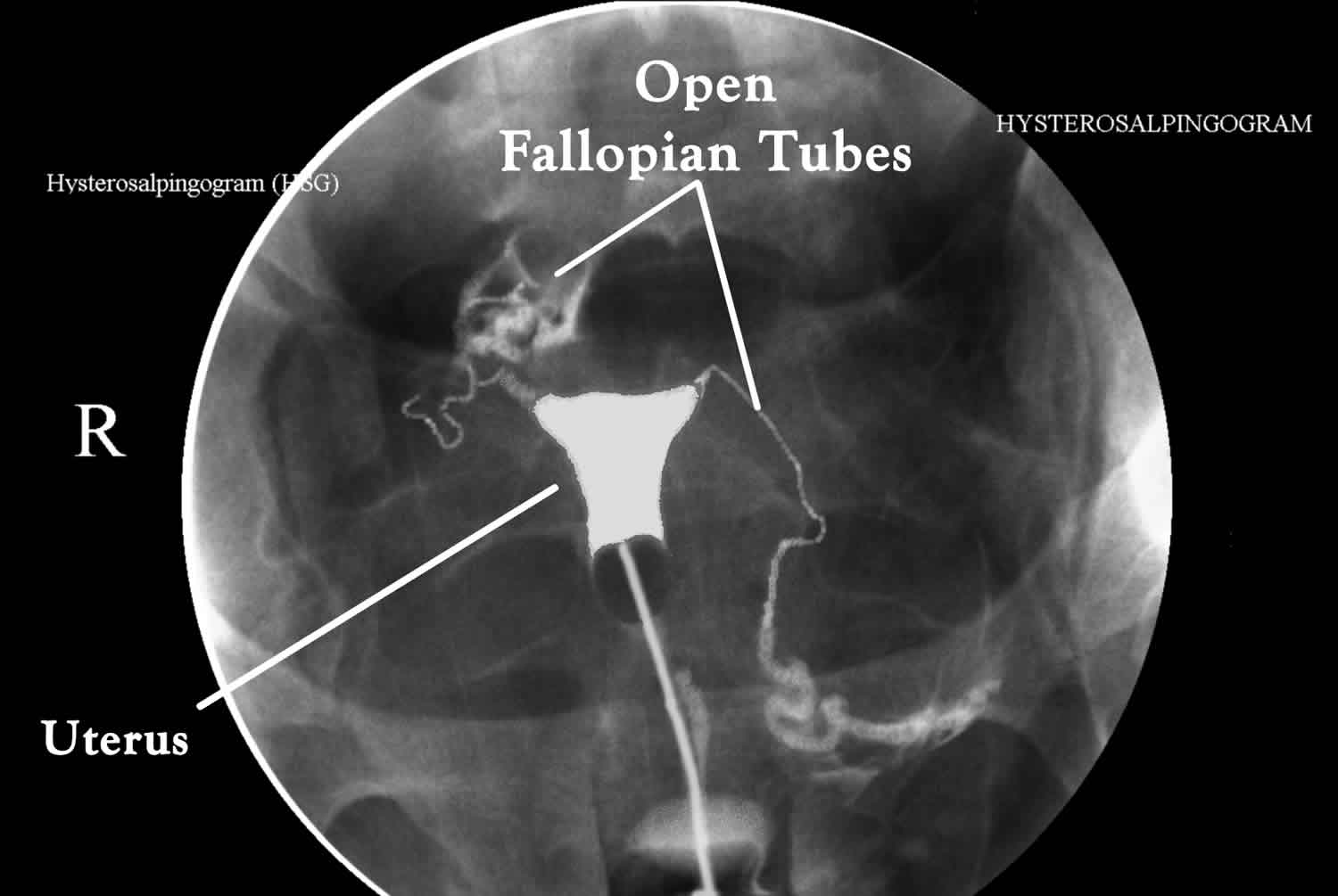
Footnote: Normal hysterosalpingogram (HSG) showing contrast material flowing freely through the fallopian tubes, then spilling out to the peritoneum, i.e. no obstruction. Contrast material seen filling up the uterine cornua and the length of the fallopian tubes, then beginning to spill out to the peritoneal cavity.
[Source 5 ]What are some common uses of hysterosalpingogram procedure?
Hysterosalpingogram is primarily used to examine women who have difficulty becoming pregnant by allowing the radiologist to evaluate the shape and structure of the uterus, the openness of the fallopian tubes, and any scarring within the uterine or peritoneal (abdominal) cavity.
Hysterosalpingogram procedure can be used to investigate repeated miscarriages that result from congenital or acquired abnormalities of the uterus and to determine the presence and severity of these abnormalities, including:
- Tumor masses
- Adhesions
- Uterine fibroids
Hysterosalpingogram is also used to evaluate the openness of the fallopian tubes, and to monitor the effects of tubal surgery, including:
- Blockage of the fallopian tubes due to infection or scarring
- Tubal ligation
- The closure of the fallopian tubes in a sterilization procedure and a sterilization reversal
- The re-opening of the fallopian tubes following a sterilization or disease-related blockage
What are the benefits vs. risks of hysterosalpingogram test?
Benefits
- Hysterosalpingogram is a minimally invasive procedure with rare complications.
- Hysterosalpingogram is a relatively short procedure that can provide valuable information on a variety of abnormalities that cause infertility or problems carrying a fetus to term.
- Hysterosalpingogram can occasionally open fallopian tubes that are blocked allowing the patient to become pregnant afterwards.
- No radiation remains in a patient’s body after an x-ray examination.
- X-rays usually have no side effects in the typical diagnostic range for this exam.
Risks
- There is always a slight chance of cancer from excessive exposure to radiation. However, the benefit of an accurate diagnosis far outweighs the risk.
- The effective radiation dose for this procedure varies. See the Safety page for more information about radiation dose.
- In the event of a chronic inflammatory condition, pelvic infection or untreated sexually transmitted disease, be certain to notify the physician or technologist before the procedure to avoid worsening of infection.
- Women should always inform their physician or x-ray technologist if there is any possibility that they are pregnant. See the Safety page for more information about pregnancy and x-rays.
A word about minimizing radiation exposure
Special care is taken during x-ray examinations to use the lowest radiation dose possible while producing the best images for evaluation 6. National and international radiology protection organizations continually review and update the technique standards used by radiology professionals.
Modern x-ray systems have very controlled x-ray beams and dose control methods to minimize stray (scatter) radiation 6. This ensures that those parts of a patient’s body not being imaged receive minimal radiation exposure.
Are there alternatives to hysterosalpingogram?
There are other procedures that can give your health care provider some of the same information as hysterosalpingogram:
- Laparoscopy — This surgical procedure requires general anesthesia.
- Hysteroscopy — This procedure can give a detailed view of the inside of the uterus. However, it cannot show whether the fallopian tubes are blocked.
- Sonohysterography — This technique uses ultrasound to show the inside of the uterus. Like hysteroscopy, it does not give information about the fallopian tubes.
Hysterosalpingogram contraindications
- pregnancy
- active pelvic infection
- recent uterine or tubal surgery
Hysterosalpingogram procedure
On the night before the procedure, you may be asked to take a laxative or an enema to empty your bowels, so that the uterus and surrounding structures can be seen clearly. Your health care provider may also recommend that you take an over-the-counter pain reliever an hour before your hysterosalpingogram procedure 7. Some physicians prescribe an antibiotic prior to and/or after the procedure. Discuss this decision with your health care provider. In some cases, he or she also may prescribe an antibiotic for you to take before your hysterosalpingogram test. Most people can drive themselves home after having hysterosalpingogram. However, you may not feel well after the procedure, so you may want to make arrangements for someone to drive you home.
You should inform your physician of any medications being taken and if there are any allergies, especially to iodinated contrast materials. Also inform your doctor about recent illnesses or other medical conditions.
Also, tell your doctor if you have any signs of pelvic infection or pelvic inflammatory disease.
Women should always inform their physician and x-ray technologist if there is any possibility that they are pregnant. Many imaging tests are not performed during pregnancy so as not to expose the fetus to radiation. If an x-ray is necessary, precautions will be taken to minimize radiation exposure to the baby.
Hysterosalpingogram procedure should be performed during the proliferative phase of your menstrual cycle (days 6-12), when your endometrium is thinnest, this improves visualization of the uterine cavity and also minimizes the possibility that the patient may be pregnant 3.
If there is any uncertainty about the patient’s pregnancy status, a beta human chorionic gonadotropin (hCG) is warranted prior to commencing.
How hysterosalpingogram is done
Hysterosalpingogram is done in a hospital, clinic, or health care provider’s office. It is best to have hysterosalpingogram done in the first half (days 1–14) of your menstrual cycle. This timing reduces the chance that you may be pregnant.
During hysterosalpingogram, a contrast medium is placed in the uterus and Fallopian tubes. This is a fluid that contains a dye. The dye shows up in contrast to the body structures on an X-ray screen. The dye outlines the inner size and shape of the uterus and Fallopian tubes. It also is possible to see how the dye moves through the body structures.
The procedure is performed as follows:
- You will be asked to lie on your back with your feet placed as for a pelvic exam (the lithotomy position). After an antiseptic cleaning of the external genital area, a vaginal speculum is inserted into your vagina. It holds the walls of the vagina apart to allow the cervix to be viewed. The cervix is cleaned with an aseptic solution.
- The end of the cervix may be injected with local anesthesia (pain relief). You may feel a slight pinch or tug as this is done.
- Catheterization of the cervix is then performed. One of two methods may be used to insert the dye; the type of device used depends on local practice preferences 8:
- In one method, the cervix is grasped with a device to hold it steady. An instrument called a cannula is then inserted into the cervix.
- In the other method, a thin plastic tube is passed into the cervical opening. The tube has a small balloon at the end that is inflated e.g., 6 Fr Foley catheter with balloon inflation. The balloon keeps the tube in place in the uterus.
- Whatever the device, it should be primed with contrast prior to commencing to avoid the introduction of gas bubbles which may provide a false positive appearance of a filling defect.
- The speculum is removed, and you are placed beneath an X-ray machine.
- Water soluble iodinated contrast is subsequently injected slowly under fluoroscopic guidance.
- Some radiologists use iodinated oil (Lipiodol) as contrast when the indication is for lack of fertility. Some authors report increased fertility after its use: this remains controversial however 9.
- The fluid slowly is placed through the cannula or tube into the uterus and fallopian tubes. The fluid may cause cramping. If the tubes are blocked, the fluid will cause them to stretch.
- X-ray images are made as the contrast medium fills the uterus and tubes. You may be asked to change position. If there is no blockage, the fluid will spill slowly out the far ends of the tubes. After it spills out, the fluid is absorbed by the body.
- A typical hysterosalpingogram test includes a preliminary frontal view of the pelvis, as well as subsequent spot images that demonstrate uterine endometrial contour, filled Fallopian tubes and bilateral intraperitoneal spill of contrast, to establish tubal patency.
- After the images are made, the cannula or tube is removed.
What should I expect after the hysterosalpingogram procedure?
After your hysterosalpingogram test, you can expect to have a sticky vaginal discharge as some of the fluid drains out of the uterus. The fluid may be tinged with blood. A pad can be used for the vaginal discharge. Do not use a tampon. You also may have the following symptoms:
- Slight vaginal bleeding
- Cramps
- Feeling dizzy, faint, or sick to your stomach
Hysterosalpingogram side effects
Severe problems after an hysterosalpingogram are rare. They include an allergic reaction to the dye, injury to the uterus, or pelvic infection.
Common side effects of hysterosalpingogram but self-limiting:
- abdominal cramping
- per vaginal spotting
- venous extravasation
Rare but serious:
- pelvic infection
- contrast reaction
See your health care provider if you have any of these symptoms:
- Foul-smelling vaginal discharge
- Vomiting
- Fainting
- Severe abdominal pain or cramping
- Heavy vaginal bleeding
- Fever or chills
- Hysterosalpingogram. https://radiopaedia.org/articles/hysterosalpingogram?lang=us[↩]
- Chalazonitis A, Tzovara I, Laspas F et-al. Hysterosalpingography: technique and applications. Curr Probl Diagn Radiol. 38 (5): 199-205. doi:10.1067/j.cpradiol.2008.02.003[↩]
- Simpson WL, Beitia LG, Mester J. Hysterosalpingography: a reemerging study. Radiographics. 26 (2): 419-31. doi:10.1148/rg.262055109[↩][↩][↩]
- Creasy JL, Clark RL, Cuttino JT et-al. Salpingitis isthmica nodosa: radiologic and clinical correlates. Radiology. 1985;154 (3): 597-600.[↩]
- Hysterosalpingogram: normal. https://radiopaedia.org/cases/hysterosalpingogram-normal-2?lang=us[↩]
- Hysterosalpingography. https://www.radiologyinfo.org/en/info.cfm?pg=hysterosalp[↩][↩]
- Hysterosalpingography. https://www.acog.org/Patients/FAQs/Hysterosalpingography[↩]
- Tur-kaspa I, Seidman DS, Soriano D et-al. Hysterosalpingography with a balloon catheter versus a metal cannula: a prospective, randomized, blinded comparative study. Hum. Reprod. 1998;13 (1): 75-7. doi:10.1093/humrep/13.1.75[↩]
- Johnson NP, Hadden WE, Chamley LW. Fertility enhancement by hysterosalpingography with oil-soluble contrast media: reality not myth. AJR Am J Roentgenol. 2005;185 (6): 1654. doi:10.2214/AJR.05.51581[↩]





{kind=link}