Contents
What is an ileus
Ileus also called paralytic ileus or pseudo-obstruction, is temporary absence of the normal contractile movements of your intestines. Ileus is a condition in which your bowel does not work correctly, but there is no structural problem causing it. Abdominal surgery and drugs that interfere with the intestine’s movements are a common cause of paralytic ileus. Paralytic ileus is one of the major causes of intestinal obstruction in infants and children.
The most common cause of ileus is:
- Abdominal surgery
Ileus commonly occurs for 24 to 72 hours after abdominal surgery, particularly when the intestines have been manipulated.
Other causes include drugs, especially opioid analgesics and anticholinergic drugs (drugs that block the action of acetylcholine e.g., promethazine, benztropine, cyproheptadine). Ileus may also be caused by an infection inside the abdomen, such as appendicitis or diverticulitis. Disorders outside the intestine, such as kidney failure, an underactive thyroid gland, heart attack, or abnormal levels of blood electrolytes (low potassium levels or high calcium levels, for example), may cause ileus.
Bloating, vomiting, constipation, cramps, and loss of appetite occur.
The diagnosis of paralytic ileus is made by x-ray.
People are given nothing to eat or drink, and sometimes a thin suction tube is passed through the nose into the stomach.
Like an obstruction (blockage) of the intestines, ileus prevents the passage of intestinal contents. Unlike a mechanical obstruction, though, ileus rarely leads to rupture.
What is adynamic ileus
Adynamic ileus is the failure of passage of enteric contents through the small bowel and colon that are not mechanically obstructed. Essentially it is paralytic ileus or the paralysis of intestinal motility.
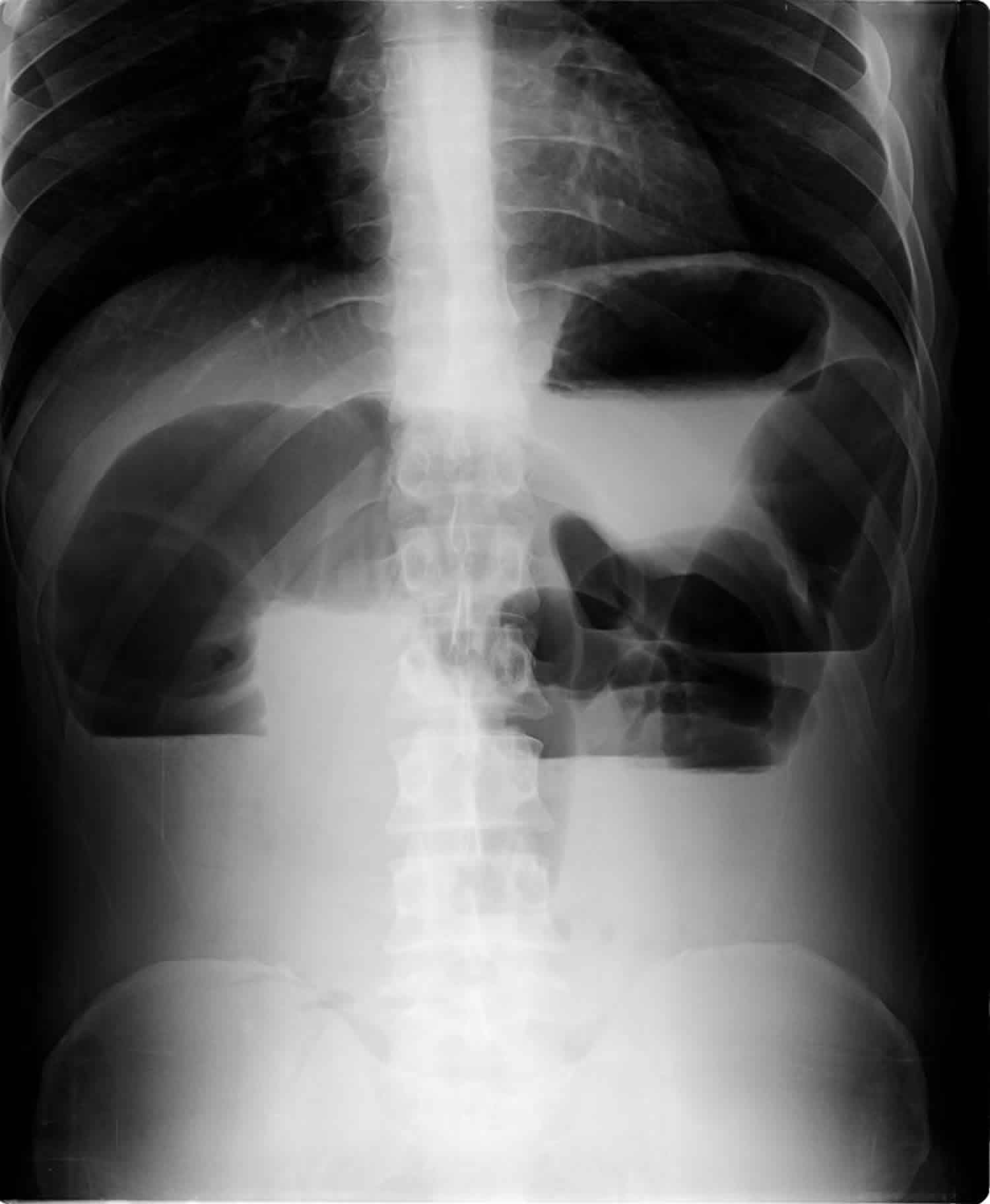
Figure 1. Paralytic ileus

Footnote: Generalized, uniform, gaseous distension of the both large and small bowel loops without frank transitional zone. Involvement of large bowel and lack of a transition point help distinguish it from small bowel obstruction (SBO).
[Source 1 ]What is meconium ileus
Meconium ileus refers to a neonatal bowel obstruction of the distal ileum due to abnormally thick and impacted meconium. Unlike in the meconium plug syndrome, the meconium is abnormal in consistency. Meconium ileus is more common in white populations and affects both sexes almost equally.
Meconium found in the intestine of a neonate consists of succus entericus (bile salts, bile acids, and debris from the intestinal mucosa) and is normally evacuated within 6 hours of birth (or earlier).
Meconium ileus occurs when meconium becomes inspissated and obstructs the distal ileus. It is usually a manifestation of cystic fibrosis. Approximately 20% of infants with cystic fibrosis present with meconium ileus at birth.
Although it is usually understood as synonymous with cystic fibrosis until proven otherwise, it may also be seen with pancreatic atresia or stenosis of the pancreatic duct.
Only rarely does it occur without cystic fibrosis or pancreatic abnormality, and is thought to be related to gut immaturity (more favorable outcome).
Meconium ileus treatment and prognosis
Water-soluble contrast enema usually clears the impacted meconium, with a success rate of over 60%.
Meconium ileus complications
- ileal atresia or stenosis
- ileal perforation resulting in meconium peritonitis
- volvulus with or without pseudocyst formation
Ileus vs Obstruction
Intestinal obstruction can be a partial or complete blockage of the bowel. An obstruction of the intestine is a blockage that completely stops or seriously impairs the passage of intestinal contents. An obstruction may occur anywhere along the small or large intestine and can be partial or complete. The part of the intestine above the obstruction continues to function. This part of the intestine enlarges as it fills with food, fluid, digestive secretions, and gas. The intestinal lining becomes swollen and inflamed. If the condition is not treated, the intestine can rupture, leaking its contents and causing inflammation and infection of the abdominal cavity (peritonitis).
The classic clinical features of bowel obstruction are:
- colicky abdominal pain
- vomiting
- abdominal distension
- absolute constipation
The order and timescale in which these appear vary depending on whether there is large or small bowel obstruction. Absolute constipation and pain are more prominent early on in large bowel obstruction while vomiting is the predominant early feature for small bowel obstruction.
Additional features depend on the exact underlying pathology.
The most common causes of intestinal obstruction in adults are scar tissue resulting from previous abdominal surgery, hernias, and tumors.
The diagnosis is based on the results of a physical examination and x-rays.
Surgery to remove the obstruction is often needed.
Obstruction of the bowel may be due to:
- A mechanical cause, which means something is in the way
- Ileus
Mechanical causes of intestinal obstruction may include:
- Adhesions or scar tissue that forms after surgery
- Foreign bodies (objects that are swallowed and block the intestines)
- Gallstones (rare)
- Hernias
- Impacted stool
- Intussusception (telescoping of one segment of bowel into another)
- Tumors blocking the intestines
- Volvulus (twisted intestine)
Intestinal obstruction causes
Causes of intestinal obstruction differ depending on the person’s age and the location of the obstruction.
In newborns and infants, intestinal obstruction is commonly caused by a birth defect, a hard mass of intestinal contents (meconium plug syndrome), a twisting of a loop of intestine (volvulus), a narrowing or absence of a portion of the intestines (intestinal atresia), or a telescoping of one segment of intestine into another (intussusception).
In adults, the most common causes overall are bands of internal scar tissue resulting from previous abdominal surgery (adhesions), parts of the intestine bulging through an abnormal opening (hernias), and tumors. The likelihood of a particular cause varies depending on the part of the intestine affected.
An obstruction of the first segment of the small intestine (duodenum) may be caused by cancer of the pancreas, scarring from an ulcer, or Crohn disease. Rarely, a gallstone, a mass of undigested food, or a collection of parasitic worms may block other parts of the small intestine.
An obstruction of the large intestine is commonly caused by cancer, diverticulitis, or a hard lump of stool (fecal impaction). Adhesions and volvulus are less common causes of obstruction of the large intestine.
Strangulation
If an obstruction cuts off the blood supply to the intestine, the condition is called strangulation. Strangulation occurs in nearly 25% of people with obstruction of the small intestine. Usually, strangulation results when part of the intestine becomes trapped in an abnormal opening (strangulated hernia), volvulus, or intussusception. Gangrene can develop in as few as 6 hours. With gangrene, the intestinal wall dies, usually causing rupture, which leads to peritonitis, shock, and, if untreated, death.
Intestinal obstruction symptoms
Symptoms of intestinal obstruction usually include cramping pain in the abdomen, accompanied by bloating and loss of appetite. Pain tends to come in waves and eventually becomes continuous. Vomiting is common with obstruction of the small intestine but is less common and begins later with obstruction of the large intestine.
- Complete obstruction causes severe constipation, whereas partial obstruction may cause diarrhea.
- With strangulation, pain may become severe and steady. A fever is common and is particularly likely if the intestinal wall ruptures.
- With volvulus, pain often begins abruptly. Pain is continuous and may come in waves.
Intestinal obstruction possible complications
Complications may include or may lead to:
- Electrolyte (blood chemical and mineral) imbalances
- Dehydration
- Hole (perforation) in the intestine
- Infection
- Jaundice (yellowing of the skin and eyes)
If the obstruction blocks the blood supply to the intestine, it may cause infection and tissue death (gangrene). Risks for tissue death are related to the cause of the blockage and how long it has been present. Hernias, volvulus, and intussusception carry a higher gangrene risk.
In a newborn, paralytic ileus that destroys the bowel wall (necrotizing enterocolitis) is a life-threatening condition. It may lead to blood and lung infections.
Intestinal obstruction diagnosis
A doctor examines the abdomen for tenderness, swelling, or masses. When an obstruction occurs, the abdomen is almost always swollen. The sounds normally made by a functioning intestine (bowel sounds), which can be heard through a stethoscope, may be much louder and higher pitched, or they may be absent. The abdomen is usually not very tender when the doctor presses on it unless rupture has caused peritonitis.
Doctors usually also do imaging studies of the abdomen, such as x-rays or a CT scan.
X-rays may show dilated loops of intestine that indicate the location of the obstruction. The x-rays also may show air around the intestine or under the layer of muscle that separates the abdomen and the chest (diaphragm). Air normally is not found in those places and thus is a sign of rupture or dead bowel.
Computed tomography (CT) of the abdomen is often used to get a better picture of the intestines and to identify the precise location and cause of the obstruction along the intestines.
Intestinal obstruction treatment
- Suction via nasogastric tube
- Fluids given by vein
- Surgery for strangulation
- Sometimes a colostomy
Anyone suspected of having an intestinal obstruction is hospitalized. Usually, a long, thin tube is passed through the nose and placed in the stomach (called a nasogastric tube) or into the intestine. Suction is applied to the tube to remove the material that has accumulated above the blockage. Fluid and electrolytes (sodium, chloride, and potassium) are given by vein (intravenously) to replace water and salts lost from vomiting or diarrhea.
Sometimes an obstruction resolves without further treatment, especially if caused by scarring or adhesions. Occasionally, an endoscope (a flexible viewing tube), which is inserted through the anus, or a barium enema, which inflates the large intestine, may be used to treat some disorders, such as a twisted intestinal segment in the lower part of the large intestine. Most often, however, surgery is done as soon as possible if doctors are concerned about strangulation.
The cause of the obstruction and the appearance of the intestine determine whether the surgeon can relieve the blockage without removing a segment of the intestine. Sometimes adhesions can be cut to release the trapped segment of intestine, but they may re-form and obstruction may recur. In some cases, an ileostomy (a procedure where a cut-off end of the small intestine is permanently attached to a surgical opening in the abdominal wall) or colostomy (a surgically created opening between the large intestine and the abdominal wall—see Figure: Understanding Colostomy) is required to relieve an obstruction.
Ileus vs SBO
SBO or small bowel obstruction, is a common surgical emergency due to a mechanical blockage of the bowel 2. Small bowel obstruction (SBO) accounts for 80% of all mechanical intestinal obstruction, the remaining 20% results from large bowel obstruction. It has a mortality rate of ~5% 3. SBO can be caused by many pathologic processes, but the leading cause in the developed world is intra-abdominal adhesions, accounting for ~75% of obstructions while in developing countries incarcerated hernias are much more common accounting for 80% of obstructions 4. Small bowel obstructions can be partial or complete and can be non-strangulated or strangulated.
Classical presentation is cramping abdominal pain and abdominal distension with nausea and vomiting. Radiographic findings can be evident 6-12 hours before the onset of clinical symptoms 5.
Post-surgical adhesions most commonly cause SBO. Incarcerated hernias are the second most common cause 2. Other common causes include malignancy, inflammatory bowel disease (Crohn), stool impaction, foreign bodies, and volvulus. In the pediatric population, common causes include congenital atresia, pyloric stenosis, other congenital anomalies, and intussusception 6.
It is estimated that more than 300,000 laparotomies are performed each year in the United States for SBO (small bowel obstruction). The small bowel comprises 80% of bowel obstructions. There is a similar incidence of males and females. There is higher incidence with age and number of intra-abdominal procedures.
What causes SBO?
SBO causes can be divided into congenital and acquired. Acquired causes may be extrinsic causing compression, intrinsic, or luminal.
Congenital
- jejunal atresia
- ileal atresia or stenosis
- enteric duplication
- midgut volvulus
- mesenteric cyst
- Meckel diverticulum
Extrinsic causes
- fibrous adhesions
- main cause in developed countries (75% of cases)
- almost all are related to post-operative adhesions with a small percentage secondary to peritonitis
- diagnosis of exclusion as adhesive bands are not seen on CT
- abrupt change in caliber without mass lesion, inflammation or bowel wall thickening at transition point
- abdominal hernia
- 10% of cases in developed countries
- external hernia related to abdominal or pelvic wall defect (congenital weakness or previous surgery)
- internal hernia with protrusion of viscera through peritoneum or mesentery into another abdominal compartment
- endometriosis
- rare cause of SBO
- endometrial implants are typically on anti-mesenteric edge of the bowel
- solid enhancing nodule contiguous with or penetrating the thickened bowel wall
- may infiltrate the submucosa with a hypoattenuating layer between the muscularis and mucosa
- masses
- extrinsic neoplasm
- intra-abdominal abscess
- aneurysm
- hematoma
Intrinsic bowel wall causes
- inflammation, e.g. Crohn, tuberculosis, eosinophilic gastroenteritis
- small bowel obstruction in Crohn disease may relate to:
- acute flare with luminal narrowing secondary to transmural inflammation
- cicatricial stenosis in long-standing disease
- adhesions or incisional hernias from previous surgery
- small bowel obstruction in Crohn disease may relate to:
- tumor (rare)
- primary small bowel neoplasms are rare (<2% all GI malignancy) and usually advanced at the time of SBO.
- GIST, adenocarcinoma, lymphoma
- asymmetric and irregular mural thickening at transition point
- small bowel involvement of metastatic disease is more common
- peritoneal carcinomatosis with extrinsic serosal disease in association with the transition point
caecal malignancy involving ileocecal valve
- peritoneal carcinomatosis with extrinsic serosal disease in association with the transition point
- primary small bowel neoplasms are rare (<2% all GI malignancy) and usually advanced at the time of SBO.
- radiation enteritis
- produces adhesive and fibrotic changes in the mesentery with luminal narrowing and dysmotility
- may cause obstruction in the late phase (>1 year after therapy)
- intestinal ischemia
- occlusion or stenosis of the mesenteric arterial or vascular supply
- produces small bowel wall thickening and obstruction
- pneumatosis and portal venous gas if advanced
- intramural hematoma
- trauma, iatrogenic, anticoagulant therapy, Henoch-Schonlein purpura
- produces luminal narrowing
- better seen on non-enhanced CT with homogenous, regular and spontaneously hyper-attenuating wall
- intussusception
- rare in adults (<5% of SBO)
- lead point may relate to neoplasm, adhesion or foreign body
- bowel-within-bowel with or without mesenteric fat and mesenteric vessels
- leading mass should be carefully interpreted and differentiated from the soft-tissue pseudotumor that represents the intussusception itself
Intraluminal causes
- swallowed, e.g. foreign body, bezoar
- gallstone ileus
- rare complication of recurrent cholecystitis
- biliary-intestinal fistula with impaction of a gallstone in the small bowel
- meconium ileus (or meconium ileus equivalent, distal intestinal obstruction syndrome)
- migration of gastric balloon
Twisting of the bowel leads to proximal bowel distention and distal bowel decompression. Initially, peristalsis may increase, leading to frequency bowel movements. Distention of the proximal bowel may lead to vomiting. The twisted bowel will first cut off venous blood flow and lead to bowel wall edema and inflammation. The third spacing of fluid often occurs as well. The thickened and inflamed bowel wall is at risk for ischemia and bacterial translocation. Bacterial translocation can cause peritonitis and bacteremia, most commonly from Escherichia coli. As the bowel further twists, the arterial flow will be cut off, leading to bowel ischemia and eventually perforation, peritonitis, and death if untreated 7.
SBO signs and symptoms
History of previous abdominal surgeries, inflammatory bowel disease, malignancy, or a hernia is a critical point to ascertain. Patients often present with complaints of abdominal pain, distention, nausea, and vomiting. Abdominal pain may be progressive or intermittent. Patients may have constipation or obstipation but could also have flatus and even loose bowel movements.
Bowel sounds may be reduced and high pitched. Abdominal tenderness on exam may be diffuse or focal. Distention may be present. Signs of peritonitis such as rebound, guarding, and rigidity are late findings which may be present depending on the time of presentation. Evaluation for hernias, surgical scars, masses including in the rectum and fecal impactions may demonstrate the possible cause. Additionally, patients can present with symptoms and signs of dehydration and sepsis.
SBO complications
- Bowel necrosis and perforation
- Wound dehiscence
- Intra-abdominal abscess
- Aspiration
- Short bowel syndrome
SBO diagnosis
Small bowel obstruction may be diagnosed with physical exam alone, but often further diagnostics are required for surgical evaluation and management. While traditionally a physical exam was used to diagnose small bowel obstruction, the invention of computed tomography has greatly improved the accuracy and characterization of this disease. X-ray is often used as a supplementary imaging modality; however, ultrasound is more sensitive and specific than an x-ray. Additionally, ultrasound does not result in radiation exposure and has the benefit of rapid and serial examinations 8.
Plain radiography has poor sensitivity, ranging from 50% to 80%, and may be an initial screening test for obvious air-fluid levels and free intra-abdominal air but cannot be relied upon to rule out small bowel obstruction. Small bowel diameter of greater than 6 centimeters, large bowel greater than 12 centimeters, and cecum greater than 15 centimeters is worrisome for obstruction.
CT is the gold standard imaging modality in many centers of care. Intravenous contrast should be used if the patient has normal renal function and does not have a contraindication. If the patient has subnormal renal function, a non-contrast study may be obtained, but consultation with the radiologist to determine the optimal study is best. Oral contrast is most often unnecessary in the evaluation of small bowel obstruction as it can lead to delayed diagnosis and complications. Magnetic resonance imaging may be appropriate in specific circumstances such as young patients who have had multiple computed tomography evaluations previously.
Point-of-Care Ultrasound
- With the patient in the supine position, select the transducer of the highest frequency possible that will provide adequate depth for the patient. In pediatric patients, this will often be a linear high-frequency transducer (5 to 10MHz) and for adult patients it may be a curvilinear transducer (3 to 5MHz).
- Begin in the right lower quadrant of the abdomen in the transverse plane. Apply serial compressions every three centimeters along all four quadrants of the abdomen, ending in the left lower quadrant.
- Then place the transducer in the longitudinal or sagittal orientation and compress the bowel in all four quadrants ending in the right lower quadrant. A dilated small bowel that measures more than three centimeters is suggestive of an obstruction or ileus. Additionally, an edematous bowel wall that measures more than three millimeters is suggestive of an obstruction or other intestinal inflammatory process. The noncompressibility of bowel and free fluid further suggests obstruction. Anterograde-retrograde or back and forth peristalsis is specific for obstruction. Lastly, visualization of a transition point is specific for obstruction. A transition point on ultrasound demonstrates a dilated, thick, noncompressible bowel adjacent to small, decompressed bowel.
A dilated, non-compressible bowel is the hallmark of small bowel obstruction on ultrasound. A small bowel more than three centimeters is dilated. The small bowel wall is thick when it is more than three millimeters. Back and forth peristalsis and visualizing a transition point are specific findings for obstruction on ultrasound. CT scan remains an accurate method to diagnose and characterize a small bowel obstruction.
Ultrasound is not a replacement for CT and should not delay surgical consultation. However, it is useful in the instances when it can facilitate diagnosis, surgical consultation, and rule out other diagnoses.
Typical laboratory studies also need to be sent to evaluate for bowel ischemia, inflammation, extent of dehydration, pre-operative care, and to rule out possible confounding diagnoses. These may include a complete blood count, lactic acid, complete metabolic profile, urine studies, and coagulation studies.
Figure 2. Small bowel obstruction
Footnote: Plain radiograph of the abdomen erect and supine view reveal dilated small bowel loops with typical air/fluid level and absent gas in colon and distal bowel suggestive of small bowel obstruction.
[Source 9 ]SBO treatment
Surgery consultation should be utilized without delay as many SBO patients require surgical management. Initial treatment of SBO involves fluid resuscitation, pain control, antibiotics, and, often, nasogastric decompression. Antibiotics of choice for small bowel obstruction should target gut flora and cover both gram-negative and anaerobic bacteria 10.
Ileus and partial small bowel obstructions often can be treated conservatively with nasogastric decompression. Surgical consultation should still be sought, but surgical intervention may not be required.
Ileus causes
The cause of ileus is thought to be complex and multifactorial, involving bowel inflammation 11, inhibitory neural reflexes 12 and neurohormonal peptides 13.
Causes of paralytic ileus may include:
- Bacteria or viruses that cause intestinal infections (gastroenteritis)
- Chemical, electrolyte, or mineral imbalances (such as decreased potassium [hypokalemia] or sodium level [hyponatremia])
- Abdominal surgery
- Abdominal trauma
- Intra-abdominal inflammation and peritonitis e.g., pancreatitis
- Retroperitoneal hematoma
- Myocardial infarction (heart attack) / congestive heart failure
- Decreased blood supply to the intestines
- Infections inside the abdomen, such as appendicitis
- Kidney or lung disease
- Use of certain medicines, especially narcotic drugs: e.g. opioids
- Parkinson medication
- Sepsis: especially gram-negative bacteria
- Head injury or neurosurgery
- Pelvic and spinal fractures
Postoperative ileus vs. paralytic ileus
Some degree of ileus is a normal and expected finding after abdominal surgery. Conventional recovery times have been reported at 14:
- Small intestine: 0-24 hours
- Stomach: 24-48 hours
- Colon: 48-72 hours
These intervals, however, may be overestimations 15.
Prolonged postoperative ileus (>72 hours) has been termed “paralytic” ileus by some and is concerning for small bowel obstruction, bowel perforation, peritonitis, and intra-abdominal abscess.
Improving postoperative ileus is often determined clinically as much as radiographically, with the resumption of oral intake and flatus.
Ileus symptoms
Patients may be asymptomatic or present with symptoms similar to a mechanical bowel obstruction such as nausea, vomiting, abdominal bloating caused by a buildup of gas and liquids, reduced or absent bowel movements, severe constipation, loss of appetite, and abdominal cramps. Bowel sounds may also be absent. Some people may pass watery stool.
Symptoms of ileus or obstruction may include:
- Abdominal swelling (distention)
- Abdominal fullness, gas
- Abdominal pain and cramping
- Breath odor
- Constipation
- Diarrhea
- Inability to pass gas
- Vomiting
Ileus diagnosis
Your doctor may hear few of the sounds normally made by a functioning intestine (bowel sounds) or none at all through a stethoscope.
During a physical exam, your health care provider may find bloating, tenderness, or hernias in your abdomen.
Tests that show obstruction include:
- Abdominal CT scan
- Abdominal x-ray
- Barium enema
- Upper GI and small bowel series
An x-ray of the abdomen shows bulging loops of intestine.
Paralytic ileus treatment
Treatment involves suction via placing a nasogastric tube through the nose into the stomach or intestine (also called nasogastric decompression). This is to help relieve abdominal swelling (distention) and vomiting. Treatment also involve a temporary restriction of food and fluids by mouth. Fluids are given by vein (intravenously).
With restriction of food and fluids by mouth, ileus usually resolves on its own after 1 to 3 days. During this time, fluids and electrolytes (such as sodium, chloride, and potassium) are given by vein (intravenously). Whenever possible, powerful pain relievers called opioid analgesics are stopped or reduced.
Severe vomiting is rare, but if it occurs, the buildup of gas and liquid caused by ileus must be relieved. Usually, a tube is passed through the nose into the stomach or small intestine (nasogastric tube), and suction is applied to relieve pressure and expansion (distention). The person is not allowed to eat or drink anything until normal intestinal function returns. Sometimes, if the problem involves mainly the large intestine, a tube is passed through the anus into the large intestine to relieve the pressure.
Surgery may be needed to relieve the obstruction if the tube does not relieve the symptoms. It may also be needed if there are signs of tissue death.
Ileus recovery time
Conventional recovery times have been reported at 14:
- Small intestine: 0-24 hours
- Stomach: 24-48 hours
- Colon: 48-72 hours
These intervals, however, may be overestimations 15.
- Paralytic ileus. https://radiopaedia.org/cases/paralytic-ileus?lang=us[↩]
- Schick MA, Meseeha M. Bowel, Obstruction Small. [Updated 2018 Nov 14]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2018 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK448079[↩][↩]
- Small bowel obstruction. https://radiopaedia.org/articles/small-bowel-obstruction?lang=us[↩]
- Brant WE, Helms CA. Fundamentals of Diagnostic Radiology. Lippincott Williams & Wilkins. (2007) ISBN:0781761352.[↩]
- Musson RE, Bickle I, Vijay RK. Gas patterns on plain abdominal radiographs: a pictorial review. (2011) Postgraduate medical journal. 87 (1026): 274-87. doi:10.1136/pgmj.2009.082396[↩]
- Bower KL, Lollar DI, Williams SL, Adkins FC, Luyimbazi DT, Bower CE. Small Bowel Obstruction. Surg. Clin. North Am. 2018 Oct;98(5):945-971.[↩]
- Edwards MK, Kuppler CS, Croft CA, Eason-Bates HM. Adhesive Closed-loop Small Bowel Obstruction. Clin Pract Cases Emerg Med. 2018 Feb;2(1):31-34.[↩]
- Linden AF, Raiji MT, Kohler JE, Carlisle EM, Pelayo JC, Feinstein K, Kandel JJ, Mak GZ. Evaluation of a water-soluble contrast protocol for nonoperative management of pediatric adhesive small bowel obstruction. J. Pediatr. Surg. 2018 Oct 05[↩]
- Small bowel obstruction. https://radiopaedia.org/cases/small-bowel-obstruction-8?lang=us[↩]
- Ozturk E, van Iersel M, Stommel MM, Schoon Y, Ten Broek RR, van Goor H. Small bowel obstruction in the elderly: a plea for comprehensive acute geriatric care. World J Emerg Surg. 2018;13:48.[↩]
- Kalff JC, Schraut WH, Simmons RL et-al. Surgical manipulation of the gut elicits an intestinal muscularis inflammatory response resulting in postsurgical ileus. Ann. Surg. 1998;228 (5): 652-63.[↩]
- Barquist E, Bonaz B, Martinez V et-al. Neuronal pathways involved in abdominal surgery-induced gastric ileus in rats. Am. J. Physiol. 1996;270 (4 Pt 2): R888-94.[↩]
- Cullen JJ, Eagon JC, Kelly KA. Gastrointestinal peptide hormones during postoperative ileus. Effect of octreotide. Dig. Dis. Sci. 1994;39 (6): 1179-84.[↩]
- Miedema BW, Johnson JO. Methods for decreasing postoperative gut dysmotility. Lancet Oncol. 2003;4 (6): 365-72. https://www.thelancet.com/journals/lanonc/article/PIIS1470-2045(03)01118-5/fulltext[↩][↩]
- Böhm B, Milsom JW, Fazio VW. Postoperative intestinal motility following conventional and laparoscopic intestinal surgery. Arch Surg. 1995;130 (4): 415-9.[↩][↩]





{kind=link}