Contents
What is immune response
The immune response is the response made by the host to defend itself against a pathogen. The immune system is the name used to describe a complex network of tissues, cells, organs in your body and molecules involved in adaptive immunity, or sometimes the totality of host defense mechanisms. The function of the immune system is to protect the body from foreign invading pathogens. The survival of an organism is highly correlated with the quality of its immune system 1. Your body’s immune system is designed to protect you from, or get rid of, infection. An underactive or overactive immune system can cause health issues. Once the immune system recognizes matter as non-self, it activates multiple chemical and physiological processes to control and eliminate the pathogen 2. These processes are collectively known as immune response. Active immunity functions as an additional immunologic defense to eliminate infective pathogens from your body. The process is more energy-intensive compared to the innate immune response and is therefore reserved for pathogens not effectively removed by the body’s initial defense. Immunity mounted by the active, antigen-specific response provides decades of protection against that antigen.
The immune system comprises:
- skin
- bone marrow
- the thymus, a gland in your upper chest
- white blood cells, which fight infection
- lymph, a milky fluid carrying white blood cells
- the lymphatic system, a network of tiny vessels that carry lymph around the body
- lymph nodes, small lumps in your groin, armpit, around your neck and elsewhere
- the spleen, an organ under your ribs on the left
- mucous membranes, like the lining of the inside of your mouth.
The lymphatic system allows immune cells to travel between tissues and the bloodstream. The lymphatic system contains lymphocytes (white blood cells; mostly T cells and B cells), which try to recognise any bacteria, viruses or other foreign substances in your body and fight them.
Lymph nodes are found in certain areas such as the base of the neck and the armpit. They become swollen or enlarged in response to an infection.
The body’s immune system is crucial in preventing invasion and harm from a variety of microbiological organisms such as bacteria, viruses, fungi, and parasites. Many levels of protection are involved in this process. Physical barriers such as skin, mucous membranes, and the acidic environment of the gastrointestinal (GI) tract provide an initial defense. If these fail, the innate or non-specific immune system is next to respond. Innate immunity involves the release of cytokines, complement, and chemokines as well as neutrophils and macrophages to destroy the invading pathogens. When this is not enough, an antigen-specific or adaptive immune response is initiated, and antibodies, B cells, and T cells enter the battle. The generation of a specific response to an antigen is referred to as active immunity. Active immunity plays an important role in immune responses in the event of re-exposure and our utilization of vaccines 3.
The immune response may operate unregulated, overstimulated, or uncontrolled. This can lead to auto-immune diseases where the immune system targets self-proteins. Alternatively, the immune system can be poorly responsive or unresponsive to infection and disease leading to immunodeficiencies.
The adaptive (active) immune response takes 1 to 2 weeks to reach its full functioning capacity, much longer compared to the twelve hours required to activate the innate immunity completely. With the development of the adaptive immune response, comes a phenomenon called immunologic memory, an immune defense that can last a lifetime to provide a future defense if re-exposed to the same antigen.
Active immunity can be achieved naturally or acquired through vaccines. An example of this is a child who becomes ill with the chickenpox or varicella-zoster infection. During this illness, the child’s immune system will mount a specific response to the virus, and the child will have immunity moving forward. This is a natural, active immune response. An example of acquired immunity against varicella is through vaccination with the live attenuated varicella vaccine. With this method, the individual has never truly been infected by the organism 4.
The body must use the immune response carefully, balancing power with caution.
Ability to recognize abnormal cells:
- if poor, then
- slow response to disease-causing organisms
- cancer (the bodies own cells dividing out of control)
- if too efficient, then
- allergies (immune response to non-dangerous substance) Why are allergies more common in developed nations?
- autoimmune diseases (the immune system attacks cells of the body)
- reproductive failures (sperm and fetal tissue can be recognized by the immune system as non-self;
Relevant terms and definitions
- Immunogen: Protein or carbohydrate that is recognized and sufficiently activates an immune response
- Antigen: A molecule that is recognized by a specific antibody or T-cell receptor (TCR)
- Adjuvant: Prolongs the presence of antigen in tissue and enhances the immune response to an antigen; used in acquired or artificial immunization (vaccinations)
- Dendritic cells (antigen presenting cells): Facilitate activation of an antigen-specific response by the innate system; presents antigens via major histone complexes to activate CD8 and CD4 T cells
- CD4 helper T cells: Facilitate cell-to-cell interactions and cytokine release to activate and control immune and inflammatory responses
- CD8 cytotoxic T cells: Travel throughout the body looking for antigens presented by the MHC I molecules present on all nucleated cells. Activated by TH1-cell cytokine release of IL-2; destroy virally infected cells
- Major histocompatibility complex (MHC) I: Found on all nucleated cells, play a significant role in determining “self.” Responsible for presenting intracellular antigens to CD8 T cells
- MHC II: Found on antigen-presenting cells that interact with CD4 T cells; responsible for presenting exogenous antigens
- TH0: The initial role of activated CD4 T cells, promotes cell immunity by activating dendritic cells and stimulating lymphocyte growth; releases cytokines IL-2, IL-4, and IFN-gamma; can develop into TH1, TH2, TH17, or other TH cells
- TH1: The response stimulated by the release of IL-12 from dendritic cells and macrophages; secretes IL-2, IFN-gamma, and TNF-beta; inhibited by IL-4 and IL-10; provides defense against intracellular infections and fungi
- TH17: The early response to bacterial and fungal infections when IL-23 is released instead of IL-12. Releases IL-17, TNF-alpha, and chemokines
- TH2: The response that occurs in the absence of IL-12 and IFN-gamma; promotes systemic antibody driven response; releases IL-4, IL-5, IL-6, IL-10 cytokines
- Plasma cells: Permanently differentiated B-cells that secrete antibodies
- Memory B cells: Long-lasting B-cells that are responsive to one particular antigen and become activated with re-exposure to the same antigen.
Immune system disorders fast facts
- The human body’s immune system is a complex network of cells and proteins located throughout the body, that defend against infections. Immune system disorders include allergic diseases, immunodeficiencies and autoimmune diseases.
- Overactivity of the immune system can take many forms. In allergic diseases the immune system makes an excessive response to proteins in substances (known as allergens). In autoimmune diseases the immune system mounts a response against normal components of the body.
- Allergic diseases are extremely common. These include food, drug or insect allergy, hay fever (allergic rhinitis), sinus disease, asthma, hives (urticaria) and eczema (atopic dermatitis). Anaphylaxis is the most severe type of allergic reaction and is potentially life-threatening.
- Autoimmune diseases range from common to rare. These include multiple sclerosis, autoimmune thyroid disease, type 1 diabetes, systemic lupus erythematosus (lupus), rheumatoid arthritis and vasculitis. For Fast Facts about autoimmune diseases go to www.allergy.org.au/patients/fast-facts/autoimmune-diseases
- Underactivity of the immune system, also called immunodeficiency, can be inherited, acquired as a result of medical treatment or caused by another disease. Immunodeficiency predisposes people to infections ad/or swellings and can be life threatening in severe cases.
- Primary immunodeficiencies are conditions in which the immune system does not function correctly, leading to increased infections or swellings. These are usually inherited and include Common Variable Immune Deficiency (CVID), X-linked Severe Combined Immunodeficiency (SCID) and Hereditary Angioedema (HAE). For Fast Facts about primary immunodeficiencies go to www.allergy.org.au/patients/fast-facts/primary-immunodeficiencies
Acquired immunodeficiencies include HIV/AIDS. - Immunosuppression treatment is most often required for recipients of cancer chemotherapy and transplants (to prevent rejection or graft versus host disease). This can also make people more susceptible to infections.
- Research into the immune system has been active in recent decades. This makes immunology and allergy a dynamic and constantly changing field of medicine.
How does the immune system work?
The skin and mucous membranes are the first line of defence against bacteria, viruses and other foreign substances. They act as a physical barrier, and they also contain immune cells.
When your skin has a cut, microbes can enter and invade your body. The cut triggers certain immune cells in the bloodstream that try to destroy the invaders.
In an infection, white blood cells identify the microbe, produce antibodies to fight the infection, and help other immune responses to occur. They also ‘remember’ the attack.
This is how vaccinations work – vaccines expose your immune system to a dead or weakened microbe or to proteins from a microbe, so that your body is able to recognize and respond very quickly to any future exposure to the same microbe.
- Overactivity of the immune system is related to disorders such as allergies and autoimmune diseases.
- Allergies involve an immune response to something considered harmless in most people, such as pollen or a certain food.
- Autoimmune diseases, such as multiple sclerosis and rheumatoid arthritis, occur when your immune system attacks normal components of the body.
- Underactivity of the immune system, or immunodeficiency, can increase your risk of infection. You may be born with an immunodeficiency, or acquire it due to medical treatment or another disease.
What are Immune cells
Granulocytes include basophils, eosinophils, and neutrophils. Basophils and eosinophils are important for host defense against parasites. They also are involved in allergic reactions. Neutrophils, the most numerous innate immune cell, patrol for problems by circulating in the bloodstream. They can phagocytose, or ingest, bacteria, degrading them inside special compartments called vesicles.
Mast cells also are important for defense against parasites. Mast cells are found in tissues and can mediate allergic reactions by releasing inflammatory chemicals like histamine.
Monocytes, which develop into macrophages, also patrol and respond to problems. They are found in the bloodstream and in tissues. Macrophages, “big eater” in Greek, are named for their ability to ingest and degrade bacteria. Upon activation, monocytes and macrophages coordinate an immune response by notifying other immune cells of the problem. Macrophages also have important non-immune functions, such as recycling dead cells, like red blood cells, and clearing away cellular debris. These “housekeeping” functions occur without activation of an immune response.
Neutrophils accumulate within minutes at sites of local tissue injury. They then communicate with each other using lipid and other secreted mediators to form cellular “swarms.” Their coordinated movement and exchange of signals then instructs other innate immune cells called macrophages and monocytes to surround the neutrophil cluster and form a tight wound seal.
Dendritic cells (DC) are an important antigen-presenting cell (APC), and they also can develop from monocytes. Antigens are molecules from pathogens, host cells, and allergens that may be recognized by adaptive immune cells. Antigen-presenting cells like dendritic cells are responsible for processing large molecules into “readable” fragments (antigens) recognized by adaptive B or T cells. However, antigens alone cannot activate T cells. They must be presented with the appropriate major histocompatiblity complex (MHC) expressed on the antigen-presenting cell. Major histocompatiblity complex (MHC) provides a checkpoint and helps immune cells distinguish between host and foreign cells.
Natural killer (NK) cells have features of both innate and adaptive immunity. They are important for recognizing and killing virus-infected cells or tumor cells. They contain intracellular compartments called granules, which are filled with proteins that can form holes in the target cell and also cause apoptosis, the process for programmed cell death. It is important to distinguish between apoptosis and other forms of cell death like necrosis. Apoptosis, unlike necrosis, does not release danger signals that can lead to greater immune activation and inflammation. Through apoptosis, immune cells can discreetly remove infected cells and limit bystander damage. Recently, researchers have shown in mouse models that natural killer cells, like adaptive cells, can be retained as memory cells and respond to subsequent infections by the same pathogen.
What are Adaptive Cells
B cells (B lymphocytes) have two major functions: They present antigens to T cells, and more importantly, they produce antibodies to neutralize infectious microbes. Antibodies coat the surface of a pathogen and serve three major roles: neutralization, opsonization, and complement activation.
Neutralization occurs when the pathogen, because it is covered in antibodies, is unable to bind and infect host cells. In opsonization, an antibody-bound pathogen serves as a red flag to alert immune cells like neutrophils and macrophages, to engulf and digest the pathogen. Complement is a process for directly destroying, or lysing, bacteria.
Antibodies are expressed in two ways. The B-cell receptor (BCR), which sits on the surface of a B cell, is actually an antibody. B cells also secrete antibodies to diffuse and bind to pathogens. This dual expression is important because the initial problem, for instance a bacterium, is recognized by a unique B-cell receptor and activates the B cell. The activated B cell responds by secreting antibodies, essentially the B-cell receptor but in soluble form. This ensures that the response is specific against the bacterium that started the whole process.
Every antibody is unique, but they fall under general categories: IgM, IgD, IgG, IgA, and IgE. (Ig is short for immunoglobulin, which is another word for antibody.) While they have overlapping roles, IgM generally is important for complement activation; IgD is involved in activating basophils; IgG is important for neutralization, opsonization, and complement activation; IgA is essential for neutralization in the gastrointestinal tract; and IgE is necessary for activating mast cells in parasitic and allergic responses.
T cells (T lymphocytes) have a variety of roles and are classified by subsets. T cells are divided into two broad categories: CD8+ T cells or CD4+ T cells, based on which protein is present on the cell’s surface. T cells carry out multiple functions, including killing infected cells and activating or recruiting other immune cells.
CD8+ T cells also are called cytotoxic T cells or cytotoxic lymphocytes (CTLs). They are crucial for recognizing and removing virus-infected cells and cancer cells. CTLs have specialized compartments, or granules, containing cytotoxins that cause apoptosis, i.e., programmed cell death. Because of its potency, the release of granules is tightly regulated by the immune system.
The four major CD4+ T-cell subsets are TH1, TH2, TH17, and Treg, with “TH” referring to “T helper cell.” TH1 cells are critical for coordinating immune responses against intracellular microbes, especially bacteria. They produce and secrete molecules that alert and activate other immune cells, like bacteria-ingesting macrophages. TH2 cells are important for coordinating immune responses against extracellular pathogens, like helminths (parasitic worms), by alerting B cells, granulocytes, and mast cells. TH17 cells are named for their ability to produce interleukin 17 (IL-17), a signaling molecule that activates immune and non-immune cells. TH17 cells are important for recruiting neutrophils.
Regulatory T cells (Tregs), as the name suggests, monitor and inhibit the activity of other T cells. They prevent adverse immune activation and maintain tolerance, or the prevention of immune responses against the body’s own cells and antigens.
Immune cells communication
Immune cells communicate in a number of ways, either by cell-to-cell contact or through secreted signaling molecules. Receptors and ligands are fundamental for cellular communication. Receptors are protein structures that may be expressed on the surface of a cell or in intracellular compartments. The molecules that activate receptors are called ligands, which may be free-floating or membrane-bound.
Ligand-receptor interaction leads to a series of events inside the cell involving networks of intracellular molecules that relay the message. By altering the expression and density of various receptors and ligands, immune cells can dispatch specific instructions tailored to the situation at hand.
Cytokines are small proteins with diverse functions. In immunity, there are several categories of cytokines important for immune cell growth, activation, and function.
- Colony-stimulating factors are essential for cell development and differentiation.
- Interferons are necessary for immune-cell activation. Type I interferons mediate antiviral immune responses, and type II interferon is important for antibacterial responses.
- Interleukins, which come in over 30 varieties, provide context-specific instructions, with activating or inhibitory responses.
- Chemokines are made in specific locations of the body or at a site of infection to attract immune cells. Different chemokines will recruit different immune cells to the site needed.
- The tumor necrosis factor (TNF) family of cytokines stimulates immune-cell proliferation and activation. They are critical for activating inflammatory responses, and as such, TNF blockers are used to treat a variety of disorders, including some autoimmune diseases.
Toll-like receptors (TLRs) are expressed on innate immune cells, like macrophages and dendritic cells. They are located on the cell surface or in intracellular compartments because microbes may be found in the body or inside infected cells. Toll-like receptors (TLRs) recognize general microbial patterns, and they are essential for innate immune-cell activation and inflammatory responses.
B-cell receptors (BCRs) and T-cell receptors (TCRs) are expressed on adaptive immune cells. They are both found on the cell surface, but B-cell receptors also are secreted as antibodies to neutralize pathogens. The genes for B-cell receptors and T-cell receptors are randomly rearranged at specific cell-maturation stages, resulting in unique receptors that may potentially recognize anything. Random generation of receptors allows the immune system to respond to unforeseen problems. They also explain why memory B or T cells are highly specific and, upon re-encountering their specific pathogen, can immediately induce a neutralizing immune response.
Major histocompatibility complex (MHC), or human leukocyte antigen (HLA), proteins serve two general roles.
MHC proteins function as carriers to present antigens on cell surfaces. MHC class I proteins are essential for presenting viral antigens and are expressed by nearly all cell types, except red blood cells. Any cell infected by a virus has the ability to signal the problem through MHC class I proteins. In response, CD8+ T cells (also called CTLs) will recognize and kill infected cells. MHC class II proteins are generally only expressed by antigen-presenting cells like dendritic cells and macrophages. MHC class II proteins are important for presenting antigens to CD4+ T cells. MHC class II antigens are varied and include both pathogen- and host-derived molecules.
MHC proteins also signal whether a cell is a host cell or a foreign cell. They are very diverse, and every person has a unique set of MHC proteins inherited from his or her parents. As such, there are similarities in MHC proteins between family members. Immune cells use MHC to determine whether or not a cell is friendly. In organ transplantation, the MHC or HLA proteins of donors and recipients are matched to lower the risk of transplant rejection, which occurs when the recipient’s immune system attacks the donor tissue or organ. In stem cell or bone marrow transplantation, improper MHC or HLA matching can result in graft-versus-host disease, which occurs when the donor cells attack the recipient’s body.
Complement refers to a unique process that clears away pathogens or dying cells and also activates immune cells. Complement consists of a series of proteins found in the blood that form a membrane-attack complex. Complement proteins are only activated by enzymes when a problem, like an infection, occurs. Activated complement proteins stick to a pathogen, recruiting and activating additional complement proteins, which assemble in a specific order to form a round pore or hole. Complement literally punches small holes into the pathogen, creating leaks that lead to cell death. Complement proteins also serve as signaling molecules that alert immune cells and recruit them to the problem area.
Types of immune response
An immune response is generally divided into innate and adaptive immunity. Innate immunity occurs immediately, when circulating innate cells recognize a problem. Adaptive (active) immunity occurs later, as it relies on the coordination and expansion of specific adaptive immune cells. Immune memory follows the adaptive response, when mature adaptive cells, highly specific to the original pathogen, are retained for later use.
The innate immune response is non-specific to the pathogen and does not provide a long lasting immunity. The major components of the innate immune response are 5:
- Physical barriers, such as tears and skin, block the entrance of possible invaders.
- The Complement system is composed of molecules that intensify the effect of other immune functions.
- Macrophages are responsible to phagocytose, digest and present pathogens.
- Natural Killer Cells induce cytotoxic apoptosis (cell death) to infected cells.
A pathogenic invasion occurs once viral or bacterial material pass these first lines of defense. Once they have crossed the innate defense, pathogens tend to migrate to suitable locations for occupation and multiplication. Foreign invasion activates an adaptive immune response (active immune response) that impedes the replication and migration of the pathogen to attempt to free the host from the external threat. The adaptive immune response is specific to each invader and is conducted by two main types of cells 5:
- T-Cells : Lymphocytes maturated in the thymus.
- B-Cells : Lymphocytes maturated in the bone marrow.
T-cells are highly specialized cells that not only coordinate (T-helper) and regulate (T-regulatory) the immune response, but also destroy infected cells (T-cytotoxic). B-cells secrete antibodies and perform pathogen presentation similar to the macrophages. Antibodies are proteins that can mark an infected cell or a pathogen to facilitate its elimination. Additionally, antibodies can stop the replication of the pathogens by impeding their attachment to healthy cells. Both T-cells and B-cells provide immunity against a pathogen by producing memory cells (T-memory and B-memory) during an infection process. Similarly, immunity can be artificially induced by vaccination. Immunity against a pathogen heightens the immune response to prevent future infections.
The efficacy of the immune response is determined by multiple factors. Many of them are associated with the host, including age, physical fitness, gender, and nutrition 6. Various studies report different causes for deterioration of the immune system throughout an individual’s life-time. As the individual ages, limited capacity to defend against invaders is caused by multiple alterations in T-cell and B-cell functionality 7. Likewise, nutrition is a critical factor for the quality of the immune response of an individual. Studies have shown a strong relationship between malnutrition and multiple immune response deficiencies. These may include impairment of the complement system, cell mediated immunity, and phagocyte functionality 8. Obesity 9, high-cholesterol levels 10, and low vitamin and mineral intake 11 are some of the nutrition related causes for those immune response deficiencies.
In addition to access to health care, types and frequency of social interactions, gender drastically affects the competence of the immune response 12. This is primarily attributed to the blood levels of gonadal steroid hormones. Multiple studies have shown androgens as natural immunosuppressors, as well as estrogens as humoral immunity enhancers 13. Moreover, physical fitness of individuals has a unique effect on the immune response. Although positive immuno-stimulatory activity is observed with moderate exercising, both lack of and excessive exercise produce an immuno-suppressive response 14.
Innate immune response
Innate immune cells respond to any cells WITHOUT the set of surface proteins (major histocompatibility or MHC markers) on the cell membrane unique to all cells of the body in each individual. Innate immune cells express genetically encoded receptors, called Toll-like receptors (TLRs), which recognize general danger- or pathogen-associated patterns. These proteins mark cells of the body as SELF, analogous to a military uniform used to identify one’s own countryman. There are over 100 different forms (alleles) of MHC in the human population. Collectively, these receptors can broadly recognize viruses, bacteria, fungi, and even non-infectious problems. However, they cannot distinguish between specific strains of bacteria or viruses.
There are numerous types of innate immune cells with specialized functions. They include neutrophils, eosinophils, basophils, mast cells, monocytes, dendritic cells, and macrophages. Their main feature is the ability to respond quickly and broadly when a problem arises, typically leading to inflammation. Innate immune cells also are important for activating adaptive immunity. Innate cells are critical for host defense, and disorders in innate cell function may cause chronic susceptibility to infection.
Adaptive immune response
Your adaptive immune system is essential for protection against infectious disease. Adaptive immune cells are more specialized, with each adaptive B or T cell bearing unique receptors, B-cell receptors (BCRs) and T-cell receptors (TCRs), that recognize specific signals rather than general patterns. Each receptor recognizes an antigen, which is simply any molecule that may bind to a B-cell receptor or T-cell receptor. Antigens are derived from a variety of sources including pathogens, host cells, and allergens. Antigens are typically processed by innate immune cells and presented to adaptive cells in the lymph nodes.
The genes for B-cell receptors and T-cell receptors are randomly rearranged at specific cell maturation stages, resulting in unique receptors that may potentially recognize anything. Random generation of receptors allows the immune system to respond to new or unforeseen problems. This concept is especially important because environments may frequently change, for instance when seasons change or a person relocates, and pathogens are constantly evolving to survive. Because B-cell receptors and T-cell receptors are so specific, adaptive cells may only recognize one strain of a particular pathogen, unlike innate cells, which recognize broad classes of pathogens. In fact, a group of adaptive cells that recognize the same strain will likely recognize different areas of that pathogen.
If a B or T cell has a receptor that recognizes an antigen from a pathogen and also receives cues from innate cells that something is wrong, the B or T cell will activate, divide, and disperse to address the problem. B cells make antibodies, which neutralize pathogens, rendering them harmless. T cells carry out multiple functions, including killing infected cells and activating or recruiting other immune cells. The adaptive response has a system of checks and balances to prevent unnecessary activation that could cause damage to the host. If a B or T cell is autoreactive, meaning its receptor recognizes antigens from the body’s own cells, the cell will be deleted. Also, if a B or T cell does not receive signals from innate cells, it will not be optimally activated.
Immune memory is a feature of the adaptive immune response. After B or T cells are activated, they expand rapidly. As the problem resolves, cells stop dividing and are retained in the body as memory cells. The next time this same pathogen enters the body, a memory cell is already poised to react and can clear away the pathogen before it establishes itself.
Vaccination, or immunization, is a way to train your immune system against a specific pathogen. Mounting of an immune response after vaccination is dependent on active immunity. Vaccination achieves immune memory without an actual infection, so the body is prepared when the virus or bacterium enters. Saving time is important to prevent a pathogen from establishing itself and infecting more cells in the body.
An effective vaccine will optimally activate both the innate and adaptive response. An immunogen is used to activate the adaptive immune response so that specific memory cells are generated. Because B-cell receptors and T-cell receptors are unique, some memory cells are simply better at eliminating the pathogen. The goal of vaccine design is to select immunogens that will generate the most effective and efficient memory response against a particular pathogen. Adjuvants, which are important for activating innate immunity, can be added to vaccines to optimize the immune response. Innate immunity recognizes broad patterns, and without innate responses, adaptive immunity cannot be optimally achieved.
Figure 1. Adaptive immune response
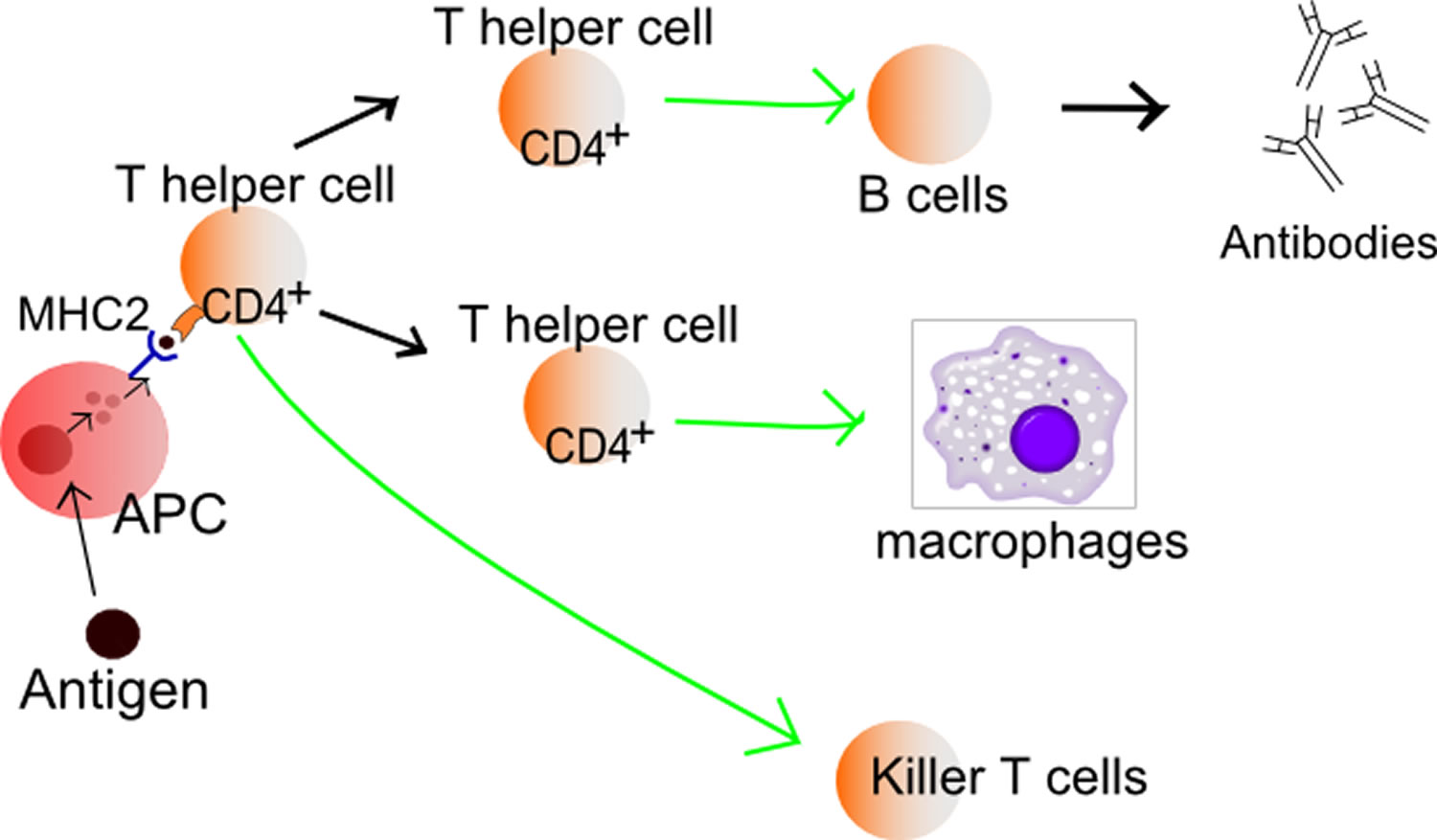 Figure 2. Humoral and cellular immune response (adaptive immune response)
Figure 2. Humoral and cellular immune response (adaptive immune response)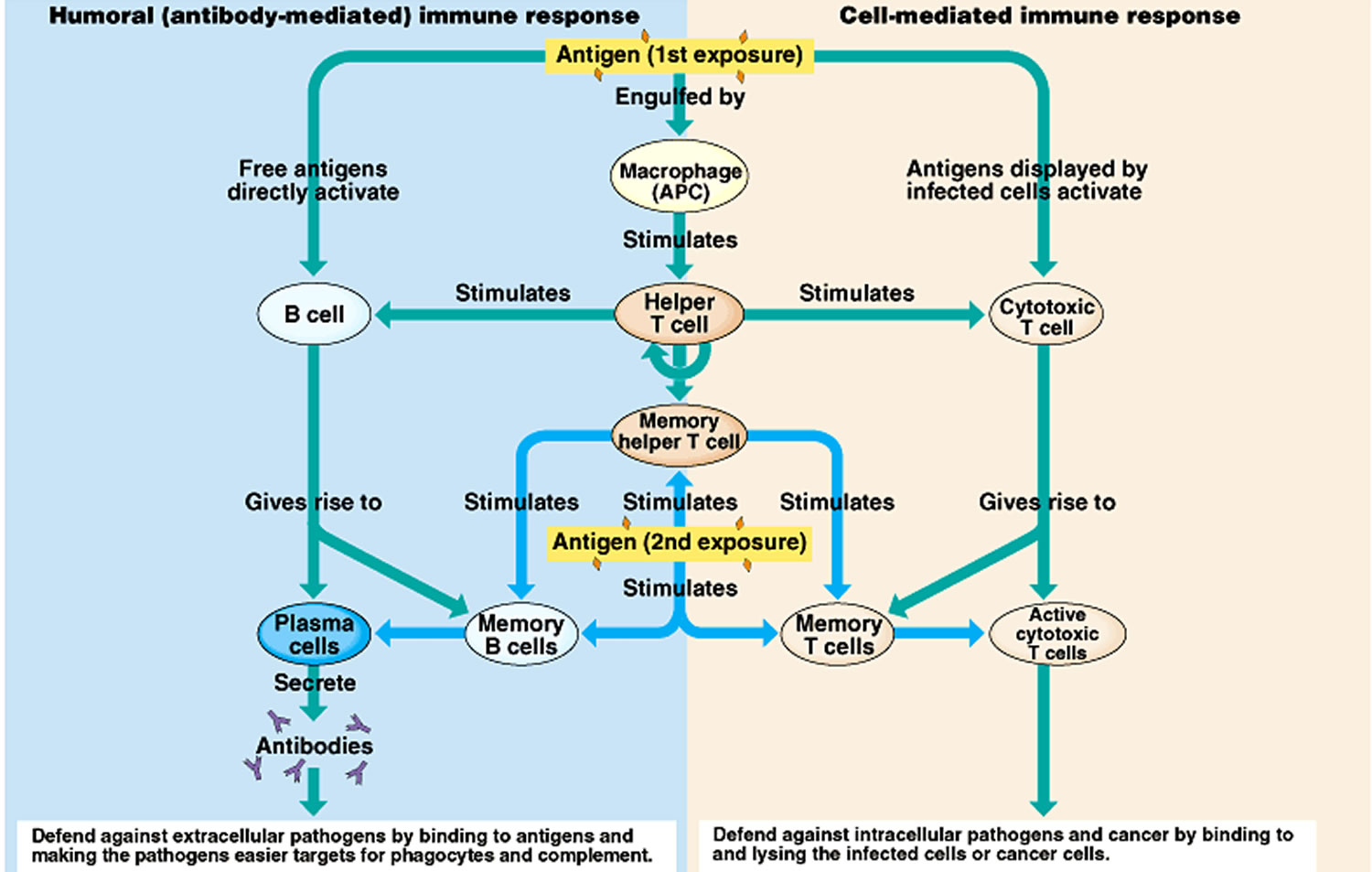
Footnote: A specific antigen (the macromolecule, typically part of the disease-causing organism, that elicits an immune response) can only activate specific B and T cells. Of millions of B and T cells types produced by the body, one type that is specific for destroying a particular type of disease causing organism is rapidly produced in the presence of that specific antigen of the disease-causing organism. The race is on.
The antigen must be exposed to a helper T cell before the specific type of B cell or cytotoxic T cell (both of which must also be exposed to the antigen) can begin to multiple rapidly (i.e. is stimulated). This provides a ‘check’ prior to initiating a major immune response.
There are two general responses: antibody-mediated B cell response and cell-mediated T cell response (see descriptions at bottom of the above diagram).
Memory cells are produced that are specific to that antigen and result in a much faster response to the disease in the event of future infections (i.e. immunity to that disease is conferred).
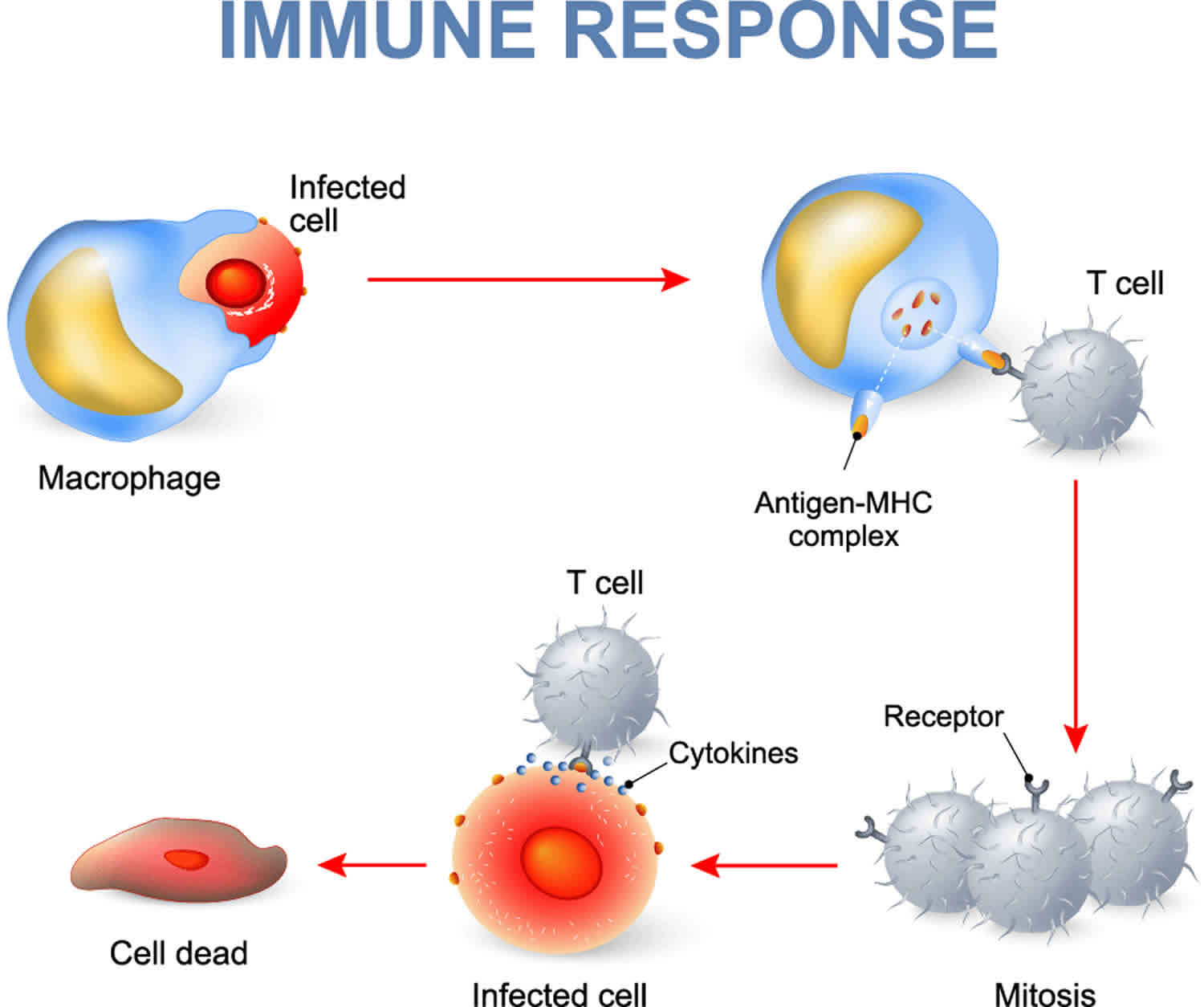
Immune response steps
A 2-step activation process is required to prevent unnecessary or detrimental responses. Step one begins with CD4 helper T-cell interactions with dendritic cells. Dendritic cells will take up an antigen, process it, bind it to an MHC II molecule and present it on its cell surface. The T-cell receptor complex (TCR) on helper T cells recognize these MHC II-antigen complexes, bind, and become activated which allows for the second signal to occur. The second step of activation requires a B7 receptor on the dendritic cell to interact with the CD28 receptor on the helper T cell. This is important to note because B7 receptors are only expressed on activated dendritic cells. If the first signal occurs without the second, the T cell is inappropriately interacting with an unactivated dendritic cell and undergoes apoptosis. Destruction of these defective T cells eliminates self-reactive cells and improves self-tolerance. If all goes correctly and both the MHC-II and B7 receptors are expressed, the T cell is fully activated and ready to migrate out of the lymph node into circulation or to the B cell areas of the lymph node and spleen.
Activated helper T cells begin as TH0 cells and enhance immunity by releasing cytokines such as IL-2, IFN-gamma, and IL-4 to stimulate lymphocyte growth and activate more dendritic cells. If IL-12 is present (released from dendritic cells and macrophages), the TH0 cell will transform into a TH1 cell and releases IL-2, IFN-gamma, and TNF-beta which play roles in both the cellular and antibody responses. The production of TH1 cells is perpetuated by the release of IFN-gamma (also known as macrophage activation factor) which stimulates further synthesis of IL-12. TH1 cells activate macrophages, natural killer cells and CD8 cytotoxic T cells which are important for intracellular infections such as viral illnesses 15.
Cytotoxic T lymphocytes (CTL) develop from CD8 T cells in response to cytokines released from TH1 cells and play a role in destroying virally infected cells and tumor cells. CTLs bind to their target cells via antigen presenting MHC I molecules. They destroy infected cells using perforin proteins which bore holes in the membrane and allow an influx of granzymes into the cell to promote apoptosis. CTLs can also trigger apoptosis through FasL (on T cells) and Fas (target cells) protein binding 16.
If IL-12 and IFN-gamma signals are not present, TH0 cells become TH2 cells. The TH2 cells are activated by dendritic cells presenting MHC II-antigen complexes on their surface. Once activated, TH2 cells release IL-4, IL-5, IL-6 and IL-10 cytokines which stimulate a humoral (antibody) response. These cytokines promote B cell immunoglobulin class switching from IgM and IgD to IgG, IgE, and IgA. Antibodies play a role in eliminating infectious pathogens, preventing hematologic spread and providing future protection if re-exposed.
While the T cells are being activated, antigens also enter the lymphatics traveling to the lymph nodes and spleen where they interact with specific B-cell immunoglobulin receptors. The B cells ingest and process the antigen, bind it to an MHC II molecule and express it on their surface. Now, the activated TH2 cells can bind these B-cell which have a similar antigen receptor. Once bound together, TH2 cells signal the B cells to become plasma cells and produce immunoglobulins. Plasma cells will secrete IgM until cytokines from the TH2 cells prompt an isotype switch. Some of these B cells become memory cells and allow for long-term immunity 15.
Active immunity utilizes cytotoxic T lymphocytes, TH1, TH2 cells, and activated B cells to target infections from multiple angles. Cytotoxic T lymphocytes destroy infected cells and the immunoglobulins produced by B cells target antigens in the bloodstream to bind and prevent them from reaching their target cells.
Summary
Immune responses are mediated by leukocytes, which derive from precursors in the bone marrow. A pluripotent hematopoietic stem cell gives rise to the lymphocytes responsible for adaptive immunity, and also to myeloid lineages that participate in both innate and adaptive immunity. Neutrophils, eosinophils, and basophils are collectively known as granulocytes; they circulate in the blood unless recruited to act as effector cells at sites of infection and inflammation. Macrophages and mast cells complete their differentiation in the tissues where they act as effector cells in the front line of host defense and initiate inflammation. Macrophages phagocytose bacteria, and recruit other phagocytic cells, the neutrophils, from the blood. Mast cells are exocytic and are thought to orchestrate the defense against parasites as well as triggering allergic inflammation; they recruit eosinophils and basophils, which are also exocytic. Dendritic cells enter the tissues as immature phagocytes where they specialize in ingesting antigens. These antigen-presenting cells subsequently migrate into lymphoid tissue. There are two major types of lymphocyte: B lymphocytes, which mature in the bone marrow; and T lymphocytes, which mature in the thymus. The bone marrow and thymus are thus known as the central or primary lymphoid organs. Mature lymphocytes recirculate continually from the bloodstream through the peripheral or secondary lymphoid organs, returning to the bloodstream through the lymphatic vessels. Most adaptive immune responses are triggered when a recirculating T cell recognizes its specific antigen on the surface of a dendritic cell. The three major types of peripheral lymphoid tissue are the spleen, which collects antigens from the blood; the lymph nodes, which collect antigen from sites of infection in the tissues; and the mucosal-associated lymphoid tissues (MALT), which collect antigens from the epithelial surfaces of the body. Adaptive immune responses are initiated in these peripheral lymphoid tissues: T cells that encounter antigen proliferate and differentiate into antigen-specific effector cells, while B cells proliferate and differentiate into antibody-secreting cells.
- Phuphanich S, Rudnick J, Chu R, Mazer M, Wang H, Serrano N, Richardson J, Wheeler C, Black K, Singh M, et al. The 46th Annual Meeting of the American Society of Clinical Oncology vol. 6. Chicago, Illinois, June: Journal of Clinical Oncology 28:155 Alexandria, Virginia; 2010. Immune response correlation with progression-free survival in glioblastoma following dendritic cell immunotherapy, ICT-107[↩]
- Kindt TJ, Goldsby RA, Osborne BA, Kuby J. Kuby Immunology. New York: WH Freeman; 2007[↩]
- Grubbs H, Kahwaji CI. Physiology, Active Immunity. [Updated 2018 Oct 27]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2019 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK513280[↩]
- Baxter D. Active and passive immunity, vaccine types, excipients and licensing. Occup Med (Lond). 2007 Dec;57(8):552-6.[↩]
- Reyes-Silveyra J, Mikler AR. Modeling immune response and its effect on infectious disease outbreak dynamics. Theor Biol Med Model. 2016;13:10. Published 2016 Mar 5. doi:10.1186/s12976-016-0033-6 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4779228/[↩][↩]
- McDade TW. The ecologies of human immune function. Annu Rev Anthropol. 2005;34:495–521. doi: 10.1146/annurev.anthro.34.081804.120348[↩]
- Castle SC. Clinical relevance of age-related immune dysfunction. Clin Infect Dis. 2000;31(2):578–85. doi: 10.1086/313947[↩]
- Chandra RK. Nutrition and the immune system: an introduction. Am J Clin Nutr. 1997;66(2):460.[↩]
- Yang H, Youm YH, Vandanmagsar B, Rood J, Kumar KG, Butler AA, Dixit VD. Obesity accelerates thymic aging. Blood. 2009;114(18):3803. doi: 10.1182/blood-2009-03-213595[↩]
- Blanc M, Hsieh WY, Robertson KA, Watterson S, Shui G, Lacaze P, Khondoker M, Dickinson P, Sing G, Rodríguez-Martín S, et al. Host defense against viral infection involves interferon mediated down-regulation of sterol biosynthesis. PLoS Biol. 2011;9(3):1000598. doi: 10.1371/journal.pbio.1000598[↩]
- Chandra R. Nutrition and the immune system from birth to old age. Eur J Clin Nutr. 2002;56:73. doi: 10.1038/sj.ejcn.1601492[↩]
- Anker M. Addressing sex and gender in epidemic-prone infectious diseases. Geneva: World Health Organization Report; 2007.[↩]
- Cutolo M, Sulli A, Capellino S, Villaggio B, Montagna P, Seriolo B, Straub R. Sex hormones influence on the immune system: basic and clinical aspects in autoimmunity. Lupus. 2004;13(9):635. doi: 10.1191/0961203304lu1094oa[↩]
- Silveira EMS, Rodrigues MF, Krause MS, Vianna DR, Almeida BS, Rossato JS, Oliveira Jr LP, Curi R, de Bittencourt Jr PIH. Acute exercise stimulates macrophage function: possible role of NF- κB pathways. Cell Biochem Funct. 2007;25(1):63–73. doi: 10.1002/cbf.1365[↩]
- McHeyzer-Williams M, McHeyzer-Williams L, Panus J, Pogue-Caley R, Bikah G, Driver D, Eisenbraun M. Helper T-cell-regulated B-cell immunity. Microbes Infect. 2003 Mar;5(3):205-12.[↩][↩]
- Kajino K, Kajino Y, Greene MI. Fas- and perforin-independent mechanism of cytotoxic T lymphocyte. Immunol. Res. 1998;17(1-2):89-93[↩]





{kind=link}