Contents
What is Isaacs Syndrome
Issacs syndrome also known as Isaac syndrome, Isaacs’ syndrome, Isaac-Merten’s syndrome, acquired neuromyotonia, neuromyotonia, peripheral nerve hyperexcitability, continuous muscle fiber activity syndrome or Quantal Squander syndrome, is a rare neuromuscular disorder in which the peripheral nerve cells become overly excited (hyperexcitability) and continuously fire causing muscle fibers to activate 1, 2, 3, 4, 5, 6.
Isaacs syndrome symptoms include:
- Progressive muscle stiffness
- Continuously contracting or twitching muscles (myokymia). This is sometimes described as looking or feeling like worms under your skin.
- Cramping
- Abdominal pain
- Increased sweating (hyperhidrosis)
- Excessive salivation (sialorrhea)
- Delayed muscle relaxation and slow movement
- Piloerection or goosebumps (due to the involuntary contraction of small muscles at the base of hair follicles)
Issacs syndrome patients commonly experience continuously contracting or twitching muscles (myokymia), impaired muscle relaxation, cramps and progressive muscle stiffness 4. Sweating, paresthesias (pins-and-needles sensation), muscle hypertrophy and progressive muscle weakness are other less commonly reported symptoms 5. Some severe cases may involve central nervous system (CNS) impairment resulting in anxiety, memory loss, sleep disturbance and hallucinations 7, 8. Patients with the triad of neuromyotonia (continuously contracting or twitching muscles), encephalopathy and increased sweating (hyperhidrosis) are considered to have Morvan syndrome 9. Some authors identify Isaacs syndrome synonymously with neuromyotonia 4, while others report Isaacs syndrome more specifically as an acquired neuromyotonia 10, 11, 12. Other terms referring to Issacs syndrome include continuous muscle fiber activity syndrome 13, Quantal Squander syndrome, Armadillo syndrome, Mertens’ syndrome, Mertens-Isaacs’ syndrome, neurotonia, myotonia with impaired muscular relaxation and generalized myokymia 4.
Isaacs syndrome symptoms occur even during sleep or when individuals are under spinal or general anesthesia 1, 14. Many people also develop weakened reflexes and muscle pain, but numbness is relatively uncommon. In most people with Issacs syndrome, stiffness is most prominent in limb and chest muscles, although symptoms can be limited to cranial muscles 1. Speech and breathing may be affected if pharyngeal or laryngeal muscles are involved.
Isaacs syndrome signs and symptoms generally develop between ages 15 and 60, with most individuals experiencing symptoms before age 40 1.
The exact underlying cause is unknown, there appear to be hereditary (inherited or passed down from one generation to another) and acquired (non-inherited) forms of Isaacs syndrome. The inherited form of Isaacs syndrome is much less common, and has been associated with point mutations in the KCNA1 gene (potassium voltage-gated channel subfamily A member 1 gene) on chromosome 12 9, 5, which encodes the potassium (K+) channel subunit Kv1.1 15. Mutations of this KCNA1 gene are commonly found in episodic ataxia type 1 which demonstrates an autosomal dominant mode of inheritance 15.
The acquired form of Isaacs syndrome occasionally develops in association with damage to the peripheral nervous system (peripheral neuropathies) or after radiation treatment (also called radiotherapy, a type of cancer treatment that uses high doses of radiation to kill cancer cells and shrink tumors), but a significant proportion of Isaacs syndrome patients (45–50%) is caused by an autoimmune condition 16, 17, 1. The autoimmune condition that cause Isaac syndrome is associated with antibodies produced by your immune system (autoantibodies) that is directed against your own voltage-gated potassium channel (VGKC) complex proteins that include contactin associated protein 2 (CASPR2) and leucine-rich glioma inactivated 1 (LGI1) 18, 19, 2. The antibodies do not directly affect voltage-gated potassium channel (VGKC) kinetics but rather act to decrease channel density on nerve terminals 11. Voltage-gated potassium channels (VGKCs) are important in nerve terminal repolarization after action potential 15.
There is no cure for Isaacs syndrome 1, 16. Treatment is based on the signs and symptoms present in each person. Anticonvulsants or antiepileptics (medications used in the treatment of epileptic seizures) such as phenytoin, carbamazapine, gabapentin, sodium valproate, lamotrigine and acetazolamide usually provide significant relief from the stiffness, muscle spasms, and pain 20, 4, 10, 21, 1. Plasma exchange also called plasmapheresis and intravenous immunoglobulin (IVIG) may provide short-term relief for individuals with some autoimmune forms of the acquired Isaacs syndrome 16, 7, 8. Botulinum toxin type A (Botox) has also been successful in symptom management 20, 22.
Testing for acetylcholine receptor antibodies should be done if thymoma is suspected. The thymus gland should be surgically removed if thymoma is present.
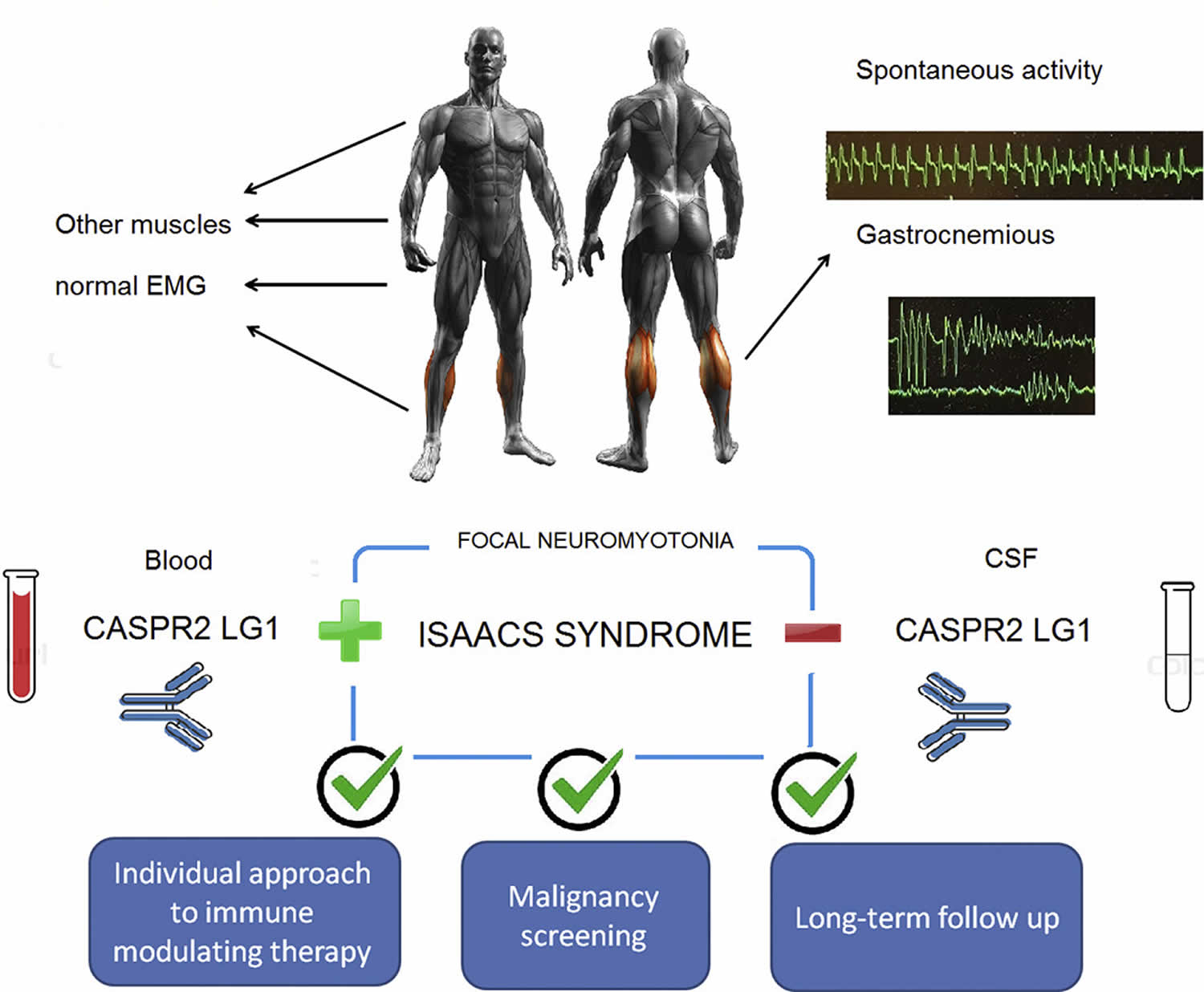
Figure 1. Isaacs syndrome
Who might get Isaacs syndrome?
The signs and symptoms of Isaacs syndrome usually begin between the ages of 15 and 60. But it has been reported in younger people and even infants.
Isaacs syndrome may be associated with other conditions, including:
- Cancer
- Celiac disease
- Chronic inflammatory demyelinating polyneuropathy (CIDP), a neurological disorder.
- Guillain-Barré syndrome
- Hashimoto’s disease
- Lupus
- Myasthenia gravis
- Peripheral neuropathy
- Rheumatoid arthritis
- Thymoma
- Vitamin B12 deficiency.
Isaacs syndrome causes
The exact cause of Isaacs syndrome is unknown, but there appear to be hereditary (inherited or passed down from one generation to another) and acquired (non-inherited) forms of Isaacs syndrome 9, 4, 5.
The inherited form of Isaacs syndrome is much less common, and has been associated with point mutations in the KCNA1 gene (potassium voltage-gated channel subfamily A member 1 gene) on chromosome 12 9, 5, which encodes the potassium (K+) channel subunit Kv1.1 15. Mutations of this KCNA1 gene are commonly found in episodic ataxia type 1 which demonstrates an autosomal dominant mode of inheritance 15.
The acquired form of Isaacs syndrome occasionally develops in association with damage to the peripheral nervous system (peripheral neuropathies) or after radiation treatment (also called radiotherapy, a type of cancer treatment that uses high doses of radiation to kill cancer cells and shrink tumors), but a significant proportion of Isaacs syndrome patients (45–50%) is caused by an autoimmune condition 16, 17, 1. The autoimmune condition that cause Isaac syndrome is associated with antibodies produced by your immune system (autoantibodies) that is directed against your own voltage-gated potassium channel (VGKC) complex proteins that include contactin associated protein 2 (CASPR2) and leucine-rich glioma inactivated 1 (LGI1) 18, 19, 2. The antibodies do not directly affect voltage-gated potassium channel (VGKC) kinetics but rather act to decrease channel density on nerve terminals 11. Voltage-gated potassium channels (VGKCs) are important in nerve terminal repolarization after action potential 15.
Elevated voltage-gated potassium channel (VGKC) antibodies are seen in peripheral nerve hyperexcitability disorders (acquired neuromyotonia), such as Isaacs syndrome, Morvan syndrome, and cramp-fasciculation syndrome 23, 24, 3, 25, 26, 27.
Studies have shown that 21–25% of patients diagnosed with Isaacs syndrome have some form of underlying neoplasm (an abnormal growth of tissue that can be benign [noncancerous] or malignant [cancerous]), highlighting the need to screen carefully for cancer 16, 17. Isaacs syndrome has been reported to be associated various cancers such as thymoma (thymus cancer), small cell lung cancer (SCLC), Hodgkin lymphoma, plasmacytoma, lymphoblastic lymphoma, hemangioblastoma, ovarian cancer, and bladder cancer 3. In these cancers, thymoma and small cell lung cancer (SCLC) are tumors most commonly seen in patients with Isaacs’ syndrome 28.
Thymomas (thymus cancer) are cited to be present in 20% of patients with a CASPR2 antibody 29, 30, 16. The association with cancer suggests that Isaacs syndrome can develop through paraneoplastic mechanisms, with tumor-associated antigens triggering an autoimmune response via cross-reacting antibodies with nerve related epitopes (the part of an antigen that is recognized by your immune system) 31, 32.
In thymoma patients, Isaacs’ syndrome was the second frequent paraneoplastic neurologic disease (3.5%), secondary to myasthenia gravis (38%) 33. Isaacs syndrome usually coexisted with other autoimmune disorders mostly myasthenia gravis in thymoma patients 34. In literature, thymoma patients associated with Isaacs syndrome without myasthenia gravis or other paraneoplastic syndromes were rare 35.
Isaacs syndrome has also been associated with infection 4, drugs such as penicillamine 9, exposure to toxins 4, pregnancy 36, and with autoimmune disorders such as myasthenia gravis 4, Lambert-Eaton myasthenia syndrome 37, Hashimoto thyroiditis, Addison disease, vitiligo, vitamin B12 deficiency, celiac disease, rheumatoid arthritis 9, 10, 8 and Guillaine-Barre syndrome 5.
There is no specific association of autoantibody type with clinical symptoms, while LGI1 antibodies are primarily associated with limbic encephalitis and central nervous system (CNS) involvement, 31% of patients display peripheral involvement including hyperexcitability or neuropathic pain in >20% 38. Similarly, CASPR2 antibodies are associated with both central nervous system (CNS) and peripheral-predominant clinical presentations 38 and associated with neuromyotonia in <40% of cases 30.
Isaacs syndrome symptoms
Isaacs syndrome signs and symptoms generally develop between ages 15 and 60, with most individuals experiencing symptoms before age 40 1.
Isaacs syndrome symptoms include:
- Progressive muscle stiffness
- Continuously contracting or twitching muscles (myokymia). This is sometimes described as looking or feeling like worms under your skin.
- Muscle cramping, spasms, and weakness that progressively worsen
- Abdominal pain
- Excessive sweating (hyperhidrosis)
- Excessive salivation (sialorrhea)
- Delayed muscle relaxation and slow movement
- Ataxia, trouble coordinating movement
- Trouble speaking or breathing if the muscles of your throat are affected
- Changes in heart rate
- Fatigue and insomnia
- Piloerection or goosebumps (due to the involuntary contraction of small muscles at the base of hair follicles)
The clinical presentation of Isaacs syndrome involves a gradual stiffening of the muscle, with frequent cramping and slow movement. Many people also develop weakened reflexes and muscle pain. In addition to the classical muscle symptoms of Isaacs syndrome, there is a spectrum of autonomic and central nervous system (CNS) involvement that link Isaacs syndrome to other autoimmune disorders. Sensory symptoms including paresthesia (pins-and-needles sensation) and pain and autonomic disturbance including excessive sweating (hyperhidrosis), fast heart rate (tachycardia), excessive salivation (sialorrhea), piloerection (goosebumps), abdominal pain or diarrhea are reported by almost half of patients 16. Central nervous system (CNS) symptoms are also prominently reported including insomnia, personality and mood changes, anxiety and depression 16, 17. Neuropathic pain and numbness is a rare finding in patients with Isaacs syndrome 39. In most people with Issacs syndrome, stiffness is most prominent in limb and chest muscles, although symptoms can be limited to cranial muscles 1. Speech and breathing may be affected if pharyngeal or laryngeal muscles are involved.
Isaacs syndrome symptoms occur even during sleep or when individuals are under spinal or general anesthesia 1, 14. Many people also develop weakened reflexes and muscle pain, but numbness is relatively uncommon. In most people with Issacs syndrome, stiffness is most prominent in limb and chest muscles, although symptoms can be limited to cranial muscles 1. Speech and breathing may be affected if pharyngeal or laryngeal muscles are involved.
Isaacs syndrome diagnosis
Your healthcare provider will review your symptoms with you and do a physical exam. The diagnosis of acquired neuromyotonia is based on the presence of continuous muscle contractions (myokymia), especially in the face and hands, rhythmic tics or twitches (fasciculations), and muscle cramps. You may also undergo a test called electromyography, which shows how well your muscles are working. Serum investigations include auto-immune serology and specifically testing for the presence of voltage-gated potassium channel (VGKC) antibodies. Testing for acetylcholine receptor antibodies should be done if thymoma is suspected. Because Isaacs syndrome is associated with cancers especially lung cancer and thymoma, your doctor may order X-rays or a CT scan of your chest and lungs.
Neurological examination
Your doctor may check your neurological health by testing:
- Reflexes.
- Muscle strength.
- Muscle tone.
- Senses of touch and sight.
- Coordination.
- Balance.
Blood tests
Complete blood count, chemistry, creatine kinase, thyroid testing group, sedimentation rate, VGKC antibodies level, Venereal Disease Research Laboratory (VDRL) test, and rheumatology screening are the basic laboratory tests for all patients with clinical myokymia. Serum alcohol level and toxic screen are recommended for acute onset of generalized myokymia.
About 40% of patients with Isaacs syndrome have detectable antibodies to VGKC 4. These antibodies are directed against proteins that form a complex with VGKC such as LGI1 and CASPR2 as well as other unknown proteins 10. LGI1 is localised to central nervous system synapses and CASPR2 organizes VGKC’s on both central and peripheral nervous system axons 10, 12.
Electromyography (EMG)
Electromyography (EMG) measures the electrical activity traveling between your brain and your muscle. Electromyography (EMG) involves inserting a fine wire electrode through your skin and into a muscle to test a single muscle fiber.
Electromyography (EMG) examination of Isaacs’ syndrome normally shows an abnormal pattern of motor unit firing which are different from Lambert-Eaton syndrome and myasthenia gravis, consisting of myokymic discharges, doublets and multiplets, neuromyotonic discharges, and fasciculations, which may occur spontaneously or may be activated by voluntary muscle contraction 40. Myokymic discharges fire repeatedly at 50–150 Hz and appear as doublet, triplet or multiplet single unit discharges with a high-intraburst frequency 4, 9, 11. Neuromyotonic discharges fire at 150–300 Hz, begin and end abruptly, and their amplitude often fades 4, 11. Fasciculations and fibrillation potentials are also often present 4. These abnormalities may occur alone or in combination 41.
To differentiate Lambert-Eaton syndrome and myasthenia gravis, repetitive nerve stimulation is a crucial test. Traditionally, an increase of the compound muscle action potential (CMAP) amplitude more than 100% is considered specific for Lambert-Eaton syndrome. Recently, an increase of the compound muscle action potential (CMAP) amplitude more than 60% is considered to have both high sensitivity and specificity for Lambert-Eaton syndrome diagnosis, which is rarely represented in myasthenia gravis 42.
Imaging tests
Imaging tests use x-rays, magnetic fields, or radioactive substances to create pictures of the inside of your body.
Chest x-ray
A chest x-ray may be the first imaging test a doctor orders if they suspect a problem in the middle of the chest or in the lungs. It may be able to show if there is a tumor in the chest. In some cases, a chest x-ray may find tumors when the person is having the x-ray done for another reason. But some thymomas are small or in places that may not show up on a chest x-ray. If your doctor is still suspicious or if a change is seen on the chest x-ray, a CT scan may be ordered.
Computed tomography (CT) scan
A CT scan uses x-rays to make detailed cross-sectional images of your body. Instead of taking 1 or 2 pictures, like a regular x-ray, a CT scanner takes many pictures and a computer then combines them to show a slice of the part of your body being studied. A chest CT with contrast is often used.
A CT scan is more likely to show lung tumors than routine chest x-rays. It can also show the size, shape, and position of any lung tumors and can help find enlarged lymph nodes that might contain cancer that has spread. This test can also be used to look for masses in the adrenal glands, liver, brain, and other organs that might be due to the lung cancer spread.
CT scans can also be used to guide a biopsy needle precisely into a suspected tumor or metastasis. This is called a CT-guided needle biopsy.
Magnetic resonance imaging (MRI) scan
Like CT scans, MRI scans provide detailed images of soft tissues in the body. But MRI scans use radio waves and strong magnets instead of x-rays.
MRI of the chest may be done to look more closely at thymus tumors. They are most often used for people who cannot have a CT scan for medical reasons (like problems with the IV contrast). MRI images are also particularly useful in looking for cancer that may have spread to the brain or spinal cord.
Positron emission tomography (PET) scan
For a PET scan, you are injected with a slightly radioactive form of sugar known as FDG, which collects mainly in cancer cells. A special camera is then used to create a picture of areas of radioactivity in the body. The picture is not detailed like a CT or MRI scan, but a PET scan can look for possible areas of cancer spread in all areas of the body at once.
A PET scan can help give the doctor a better idea of whether a change seen on another imaging test is a tumor or not. If you have already been diagnosed with cancer, your doctor may use this test to see if the cancer has spread to lymph nodes or other parts of the body. A PET scan can also be useful if your doctor thinks the cancer may have spread but doesn’t know where.
Certain machines are able to perform both a PET and CT scan at the same time (PET/CT scan). This lets the doctor compare areas of higher radioactivity on the PET scan with the more detailed pictures of that area on the CT. Combined PET/CT is used more often than PET (alone) in looking at thymomas or lung cancer.
Bone scan
For a bone scan, a small amount of low-level radioactive material is injected into the blood and collects mainly in abnormal areas of bone. A bone scan can help show if a cancer has spread to the bones. But this test isn’t needed very often because PET scans can usually show if cancer has spread to the bones.
Tests to diagnose lung cancer
Symptoms and the results of certain tests may strongly suggest that a person has lung cancer, but the actual diagnosis is made by looking at lung cells in the lab.
The cells can be taken from lung secretions (mucus you cough up from the lungs), fluid removed from the area around the lung (thoracentesis), or from a suspicious area using a needle or surgery (biopsy). The choice of which test(s) to use depends on the situation.
Sputum cytology
A sample of sputum (mucus you cough up from the lungs) is looked at in the lab to see if it has cancer cells. The best way to do this is to get early morning samples 3 days in a row. This test is more likely to help find cancers that start in the major airways of the lung, such as squamous cell lung cancers. It might not be as helpful for finding other types of lung cancer. If your doctor suspects lung cancer, further testing will be done even if no cancer cells are found in the sputum.
Thoracentesis
If fluid has collected around the lungs (called a pleural effusion), doctors can remove some of the fluid to find out if it is caused by cancer spreading to the lining of the lungs (pleura). The buildup might also be caused by other conditions, such as heart failure or an infection.
For a thoracentesis, the skin is numbed and a hollow needle is inserted between the ribs to drain the fluid. The fluid is checked in the lab for cancer cells. Other tests of the fluid are also sometimes useful in telling a malignant (cancerous) pleural effusion from one that is not.
If a malignant pleural effusion has been diagnosed and is causing trouble breathing, a thoracentesis may be repeated to remove more fluid which may help a person breathe better.
Pulmonary function tests
These tests measure whether your condition is affecting your breathing.
Biopsy
Although signs, symptoms, and imaging tests can suggest that a thymic tumor or lung cancer is likely, doctors can’t be certain of the diagnosis without looking at the tumor under a microscope. An advantage of needle biopsies is that they don’t require a surgical incision. The drawback is that they remove only a small amount of tissue and in some cases, the amount of tissue removed might not be enough to both make a diagnosis and to perform more tests on the cancer cells that can help doctors choose anticancer drugs.
For most cancers, taking out a small piece of the tumor known as a biopsy is needed to confirm whether a tumor is present and, if so, to determine its type. For thymomas, this is rarely done because doctors can usually tell that the tumor is very likely a thymoma based on how it looks on imaging tests. Because of this, doctors often remove the entire tumor rather than do a biopsy. This provides tissue for a diagnosis and treats the tumor at the same time. The specimen is sent to the lab after surgery to confirm the diagnosis.
Isaacs syndrome differential diagnosis
Isaacs syndrome differential diagnosis include other autoimmune neuromuscular junction diseases that include Lambert-Eaton syndrome and myasthenia gravis.
- Lambert-Eaton syndrome also known as Lambert-Eaton myasthenic syndrome, is a autoimmune neuromuscular junction disease in which your immune system attacks the voltage-gated calcium channels (VGCC) on the motor nerve membrane at the neuromuscular junction, the areas where your nerves and muscles connect. These voltage-gated calcium channels (VGCC) normally conduct calcium into the nerve resulting in the release of a chemical known as acetylcholine (ACh). Acetylcholine (ACh) helps in the communication between nerve cells and muscles and is one of a group of chemicals known as neurotransmitters, which help to transmit nerve impulses. The autoantibodies attack the VGCC resulting in less acetylcholine release. Because Lambert-Eaton syndrome affects the way your nerves and muscles communicate, making it difficult to move your muscles as you normally would. Lambert-Eaton syndrome is characterized by weakness and fatigue especially of the muscles in your legs and arms. Lambert-Eaton myasthenic syndrome may affect your ability to engage in strenuous exercise and may make such activities as climbing stairs or walking up a steep walkway difficult. Onset is gradual, typically taking place over several weeks to many months. There is often a progression of symptoms whereby the shoulder muscles, muscles of the feet and hands, speech and swallowing muscles and eye muscles are affected in a stepwise fashion. The symptoms progress more quickly when Lambert-Eaton syndrome is associated with cancer. Most Lambert-Eaton syndrome patients also exhibit the following symptoms (sometimes called autonomic symptoms): dry mouth, dry eyes, constipation, impotence and decreased sweating. Lambert-Eaton syndrome patients with or without cancer may also undergo significant weight loss. The tendon reflexes are diminished or absent on examination. In summary, Lambert-Eaton syndrome is often described as a clinical “triad” of proximal muscle weakness, autonomic symptoms and reduced tendon reflexes.
- Myasthenia gravis. Myasthenia gravis is an autoimmune neuromuscular junction disease where the anti-acetylcholine receptor antibodies (anti-AChR) causes muscles under your voluntary control (skeletal muscles) to feel weak and get tired quickly. In myasthenia gravis, the immune system makes antibodies that block or destroy many of your muscles’ receptor sites for a neurotransmitter called acetylcholine (ACh). With fewer acetylcholine (ACh) receptor sites available, your muscles receive fewer nerve signals. This causes weakness. Muscle weakness caused by myasthenia gravis gets worse when the affected muscle is used. Because symptoms usually get better with rest, muscle weakness can come and go. However, the symptoms tend to progress over time. They usually reach their worst within a few years after the disease begins. Some patients with anti-acetylcholine receptor antibodies (anti-AChR) have antibodies that attack another protein called the muscle-specific receptor tyrosine kinase (MuSK). These anti-MuSK antibodies also lead to a decrease in the number of acetylcholine receptors. Recently, antibodies to lipoprotein-related protein 4 (LRP4) were identified in patients without antibodies to MuSK or AChR. Research studies have found other antibodies and the number of antibodies involved will likely grow over time. In five to eight percent of patients an antibody in the blood cannot be identified but patients have other tests consistent with myasthenia gravis. Myasthenia gravis is not inherited and it is not contagious. A temporary form of myasthenia gravis may develop in the fetus when a woman with myasthenia gravis passes the antibodies to the fetus. Generally, it resolves in 2 to 3 months.
Isaacs syndrome treatment
There is no cure for Isaacs syndrome 1, 16. Treatment is based on the signs and symptoms present in each person. Anticonvulsants or antiepileptics (medications used in the treatment of epileptic seizures) such as phenytoin, carbamazapine, gabapentin, sodium valproate, lamotrigine and acetazolamide usually provide significant relief from the stiffness, muscle spasms, and pain 20, 4, 10, 21, 1. Plasma exchange also called plasmapheresis and intravenous immunoglobulin (IVIG) may provide short-term relief for individuals with some autoimmune forms of the acquired Isaacs syndrome 16, 7, 8. Botulinum toxin type A (Botox) has also been successful in symptom management 20, 22.
- Plasmapheresis (plasma exchange). This procedure uses a filtering process that’s like dialysis. Your blood is put through a machine that removes the antibodies that block transmission of signals from your nerve endings to your muscles. However, the good effects from this procedure usually last only a few weeks. Having several procedures can lead to problems finding veins for the treatment. Risks of plasmapheresis include a drop in blood pressure, bleeding, heart rhythm problems or muscle cramps. Some people have an allergic reaction to the solutions used to replace the plasma.
- Intravenous immunoglobulin (IVIg). This therapy provides your body with typical antibodies, which alters your immune system response. Benefits are usually seen in less than a week and can last 3 to 6 weeks. Side effects, which usually are mild, can include chills, dizziness, headaches and fluid retention.
Some people with Isaacs syndrome have a tumor in the thymus gland (thymoma). Whether or not a thymoma is considered resectable (able to be removed with surgery) is one of the most important factors in determining treatment options 43. The main treatment options for thymoma are: surgery, radiation therapy and chemotherapy. For people with resectable thymoma, surgery to remove the thymus gland called thymectomy offers the best chance for long-term survival. Surgery includes removing the entire thymus and, depending on the extent of the disease, maybe parts of nearby organs or blood vessels, too. The thymectomy can be performed as an open surgery or as a minimally invasive surgery. In open surgery, the surgeon splits the central breastbone (the sternum) to open the chest and remove the thymus gland.
If you have small cell lung cancer (SCLC), your treatment options are based mainly on the stage (extent) of the cancer, but other factors, such as your overall health and lung function are also important 44. Sometimes, more than one of type of treatment is used. If you have small cell lung cancer (SCLC), you will probably get chemotherapy if you are healthy enough. If you have limited stage disease, radiation therapy and – rarely – surgery may be options as well. People with extensive stage disease often receive chemotherapy with or without immunotherapy.
Isaacs syndrome prognosis
Isaacs syndrome prognosis (outlook) varies, depending on the severity of the disorder, the underlying cause, treatment effectiveness and any associated medical conditions (e.g., cancer, autoimmune disorders). Although there’s currently no cure for Isaacs syndrome, the condition isn’t generally fatal. Neuromyotonia symptoms progressively worsen over time. They can significantly limit movement and interfere with daily activities.
- Isaacs Syndrome. https://www.ninds.nih.gov/health-information/disorders/isaacs-syndrome[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Al-Chalabi M, DelCimmuto NR, Devarasetty PP, Jeyarajan J, Baumle BN, Pirzada N. Isaac Syndrome with Intractable Neuropathic Pain Features: A Case Report. Case Rep Neurol. 2022 Mar 29;14(1):185-190. doi: 10.1159/000523821[↩][↩][↩]
- Ahmed, A. and Simmons, Z. (2015), Isaacs syndrome: A review. Muscle Nerve, 52: 5-12. https://doi.org/10.1002/mus.24632[↩][↩][↩]
- Maddison P. Neuromyotonia. Clin Neurophysiol. 2006 Oct;117(10):2118-27. doi: 10.1016/j.clinph.2006.03.008[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Myers KA, Baker SK. Late-onset seropositive Isaacs’ syndrome after Guillain-Barré syndrome. Neuromuscul Disord. 2009 Apr;19(4):288-90. doi: 10.1016/j.nmd.2009.01.007[↩][↩][↩][↩][↩][↩]
- Samogalskyi V, Alcalay Y, Gadoth A, Eilam A, Gilad R. Case report: Isolated muscle neuromyotonia, as presenting feature of Isaacs’ syndrome. J Neuroimmunol. 2021 Apr 15;353:577491. https://doi.org/10.1016/j.jneuroim.2021.577491[↩][↩]
- Vernino S. Peripheral nerve hyperexcitability and the neuromuscular junction. Handb Clin Neurol. 2008;91:433-43. doi: 10.1016/S0072-9752(07)01514-X[↩][↩][↩]
- Newsom-Davis J, Mills KR. Immunological associations of acquired neuromyotonia (Isaacs’ syndrome). Report of five cases and literature review. Brain. 1993 Apr;116 ( Pt 2):453-69. doi: 10.1093/brain/116.2.453[↩][↩][↩][↩]
- Rana SS, Ramanathan RS, Small G, Adamovich B. Paraneoplastic Isaacs’ syndrome: a case series and review of the literature. J Clin Neuromuscul Dis. 2012 Jun;13(4):228-33. doi: 10.1097/CND.0b013e318246197d[↩][↩][↩][↩][↩][↩][↩]
- Fleisher J, Richie M, Price R, Scherer S, Dalmau J, Lancaster E. Acquired neuromyotonia heralding recurrent thymoma in myasthenia gravis. JAMA Neurol. 2013 Oct;70(10):1311-4. doi: 10.1001/jamaneurol.2013.2863[↩][↩][↩][↩][↩][↩]
- Arimura K, Sonoda Y, Watanabe O, Nagado T, Kurono A, Tomimitsu H, Otsuka R, Kameyama M, Osame M. Isaacs’ syndrome as a potassium channelopathy of the nerve. Muscle Nerve Suppl. 2002;11:S55-8. doi: 10.1002/mus.10148[↩][↩][↩][↩][↩]
- van Sonderen A, Wirtz PW, Verschuuren JJ, Titulaer MJ. Paraneoplastic syndromes of the neuromuscular junction: therapeutic options in myasthenia gravis, lambert-eaton myasthenic syndrome, and neuromyotonia. Curr Treat Options Neurol. 2013 Apr;15(2):224-39. doi: 10.1007/s11940-012-0213-6[↩][↩]
- Isaacs H. A SYNDROME OF CONTINUOUS MUSCLE-FIBRE ACTIVITY. J Neurol Neurosurg Psychiatry. 1961 Nov;24(4):319-25. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC495392/pdf/jnnpsyc00272-0015.pdf[↩]
- Thompson PD. The stiff-man syndrome and related disorders. Parkinsonism Relat Disord. 2001 Oct;8(2):147-53. doi: 10.1016/s1353-8020(01)00029-3[↩][↩]
- Falace A, Striano P, Manganelli F, Coppola A, Striano S, Minetti C, Zara F. Inherited neuromyotonia: a clinical and genetic study of a family. Neuromuscul Disord. 2007 Jan;17(1):23-7. doi: 10.1016/j.nmd.2006.09.014[↩][↩][↩][↩][↩][↩]
- Vincent A, Pettingill P, Pettingill R, Lang B, Birch R, Waters P, Irani SR, Buckley C, Watanabe O, Arimura K, Kiernan MC. Association of Leucine-Rich Glioma Inactivated Protein 1, Contactin-Associated Protein 2, and Contactin 2 Antibodies With Clinical Features and Patient-Reported Pain in Acquired Neuromyotonia. JAMA Neurol. 2018 Dec 1;75(12):1519-1527. doi: 10.1001/jamaneurol.2018.2681[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Hart IK, Maddison P, Newsom-Davis J, Vincent A, Mills KR. Phenotypic variants of autoimmune peripheral nerve hyperexcitability. Brain. 2002 Aug;125(Pt 8):1887-95. doi: 10.1093/brain/awf178[↩][↩][↩][↩]
- Irani SR, Alexander S, Waters P, Kleopa KA, Pettingill P, Zuliani L, Peles E, Buckley C, Lang B, Vincent A. Antibodies to Kv1 potassium channel-complex proteins leucine-rich, glioma inactivated 1 protein and contactin-associated protein-2 in limbic encephalitis, Morvan’s syndrome and acquired neuromyotonia. Brain. 2010 Sep;133(9):2734-48. doi: 10.1093/brain/awq213[↩][↩]
- Lai M, Huijbers MG, Lancaster E, Graus F, Bataller L, Balice-Gordon R, Cowell JK, Dalmau J. Investigation of LGI1 as the antigen in limbic encephalitis previously attributed to potassium channels: a case series. Lancet Neurol. 2010 Aug;9(8):776-85. doi: 10.1016/S1474-4422(10)70137-X[↩][↩]
- ÖZ O, Yucel M, Akgun H, et al.. Isaacs’ syndrome—clinical and electrophysiological response to Botulinum toxin type A. Noropsikiyatri Arsivi Arch Neuropsychiatry 2012;49:77–9[↩][↩][↩][↩]
- Morgan PJ. Peripartum management of a patient with Isaacs’ syndrome. Can J Anaesth. 1997 Nov;44(11):1174-7. doi: 10.1007/BF03013340[↩][↩]
- Ginsburg G, Forde R, Martyn JA, Eikermann M. Increased sensitivity to a nondepolarizing muscle relaxant in a patient with acquired neuromyotonia. Muscle Nerve. 2009 Jul;40(1):139-42. doi: 10.1002/mus.21322[↩][↩]
- Shillito P, Molenaar PC, Vincent A, et al.. Acquired neuromyotonia: evidence for autoantibodies directed against K+ channels of peripheral nerves. Ann Neurol. 1995;38(5):714-722. doi: 10.1002/ana.410380505[↩]
- Hart IK, Waters C, Vincent A, et al.. Autoantibodies detected to expressed K+ channels are implicated in neuromyotonia. Ann Neurol. 1997;41(2):238-246. doi: 10.1002/ana.410410215[↩]
- Katirji B. Peripheral nerve hyperexcitability. Handb Clin Neurol. 2019;161:281-290. https://doi.org/10.1016/B978-0-444-64142-7.00054-0[↩]
- Barber PA, Anderson NE, Vincent A. Morvan’s syndrome associated with voltage-gated K+ channel antibodies. Neurology. (2000) 54:771–2. 10.1212/WNL.54.3.771[↩]
- Radja GK, Cavanna AE. Treatment of VGKC complex antibody-associated limbic encephalitis: a systematic review. J Neuropsychiatry Clin Neurosci. (2013) 25:264–71. 10.1176/appi.neuropsych.13020022[↩]
- Huang K, Luo YB, Yang H. Autoimmune Channelopathies at neuromuscular junction. Front Neurol. 2019;10:516. doi: 10.3389/fneur.2019.00516[↩]
- Ratté S, Prescott SA. Afferent hyperexcitability in neuropathic pain and the inconvenient truth about its degeneracy. Curr Opin Neurobiol. 2016 Feb;36:31-7. doi: 10.1016/j.conb.2015.08.007[↩]
- Boyko M, Au KLK, Casault C, de Robles P, Pfeffer G. Systematic review of the clinical spectrum of CASPR2 antibody syndrome. J Neurol. 2020 Apr;267(4):1137-1146. doi: 10.1007/s00415-019-09686-2[↩][↩]
- Binks SNM, Klein CJ, Waters P, Pittock SJ, Irani SR. LGI1, CASPR2 and related antibodies: a molecular evolution of the phenotypes. J Neurol Neurosurg Psychiatry. 2018 May;89(5):526-534. doi: 10.1136/jnnp-2017-315720[↩]
- Toothaker TB, Rubin M. Paraneoplastic neurological syndromes: a review. Neurologist. 2009;15(1):21–33. doi: 10.1097/NRL.0b013e3181870aa2[↩]
- Bernard C, Frih H, Pasquet F, Kerever S, Jamilloux Y, Tronc F, et al. Thymoma associated with autoimmune diseases: 85 cases and literature review. Autoimmun Rev. 2016;15(1):82–92. doi: 10.1016/j.autrev.2015.09.005[↩]
- Gastaldi M, De Rosa A, Maestri M, Zardini E, Scaranzin S, Guida M, et al. Acquired neuromyotonia in thymoma-associated myasthenia gravis: a clinical and serological study. Eur J Neurol. 2019;26(7):992–999. doi: 10.1111/ene.13922[↩]
- Li KC, Liao MF, Wu YR, Lyu RK. Isaacs’ syndrome as the initial presentation of malignant thymoma and associated with double-positive voltage-gated potassium channel complex antibodies, a case report. BMC Neurol. 2022 Mar 4;22(1):74. doi: 10.1186/s12883-022-02584-7[↩]
- Basiri K, Fatehi F, Chitsaz A. Isaac’s syndrome associated with CIDP and pregnancy. Arch Iran Med. 2011 May;14(3):206-8.[↩]
- Sinha S, Newsom-Davis J, Mills K, Byrne N, Lang B, Vincent A. Autoimmune aetiology for acquired neuromyotonia (Isaacs’ syndrome). Lancet. 1991 Jul 13;338(8759):75-7. doi: 10.1016/0140-6736(91)90073-x[↩]
- Gadoth A, Pittock SJ, Dubey D, McKeon A, Britton JW, Schmeling JE, Smith A, Kotsenas AL, Watson RE, Lachance DH, Flanagan EP, Lennon VA, Klein CJ. Expanded phenotypes and outcomes among 256 LGI1/CASPR2-IgG-positive patients. Ann Neurol. 2017 Jul;82(1):79-92. doi: 10.1002/ana.24979[↩][↩]
- Park SB, Thurbon R, Kiernan MC. Isaacs syndrome: the frontier of neurology, psychiatry, immunology and cancer. J Neurol Neurosurg Psychiatry. 2020 Dec;91(12):1243-1244. https://doi.org/10.1136/jnnp-2020-324675[↩]
- Huang K, Luo YB, Yang H. Autoimmune Channelopathies at Neuromuscular Junction. Front Neurol. 2019 May 17;10:516. doi: 10.3389/fneur.2019.00516[↩]
- Auger RG. AAEM minimonograph #44: diseases associated with excess motor unit activity. Muscle Nerve. (1994) 17:1250–63. 10.1002/mus.880171103[↩]
- Liang CL, Han S. Neuromuscular junction disorders. PM R. (2013) 5:S81–8. 10.1016/j.pmrj.2013.03.016[↩]
- Treatment of Thymus Cancers by Extent and Type of Tumor. https://www.cancer.org/cancer/types/thymus-cancer/treating/by-extent.html[↩]
- Treatment Choices for Small Cell Lung Cancer, by Stage. https://www.cancer.org/cancer/types/lung-cancer/treating-small-cell/by-stage.html[↩]





{kind=link}