Contents
Keratoconjunctivitis sicca
Keratoconjunctivitis sicca also called keratitis sicca or xerophthalmia is a general term for “dry eye syndrome” due to a breakdown in the natural oily layer outside of the tear film that coats the front of the eye and keeps tears from drying up too quickly 1, 2. Normally, the natural oily layer outside of the tear film is a stable homogenous layer that not only provides the cornea and conjunctiva a healthy buffer from damage were it constantly exposed to the air, but this interface between the tear film and the air is also responsible for a significant amount of the focusing power of the eye. When the tear film becomes unhealthy, it breaks down in different places on the cornea and conjunctiva, leading not only to symptoms of irritation, but also to unstable and intermittently changing vision. Keratoconjunctivitis sicca is sometimes caused or worsened by a condition called meibomianitis, which is inflammation of the oil-producing glands or meibomian glands along the edge of your eyelids where the eyelashes are found. There are approximately 100 small meibomian glands that run along the top and bottom of your eyelids. These glands produce an oily liquid that is an important part of the eye’s tears.
Keratoconjunctivitis sicca or dry eye syndrome commonly occurs in people who are otherwise healthy. Dry eye is a common eye condition and it is estimated to affetc 7.4% to 33.7% of the population 3, 4, 5, 6. Keratoconjunctivitis sicca is also more common with older age. This can occur due to hormonal changes that make your eyes produce fewer tears.
Other common causes of dry eyes or keratoconjunctivitis sicca include:
- Dry environment or workplace (wind, air conditioning)
- Sun exposure
- Smoking or second-hand smoke exposure
- Cold or allergy medicines
- Wearing contact lenses
Keratoconjunctivitis sicca can also be caused by:
- Heat or chemical burns
- Previous eye surgery
- Use of eye drops for other eye diseases
- An uncommon autoimmune disorder in which the meibomian glands that produce tears are destroyed (Sjögren syndrome). Sjögren’s syndrome is an autoimmune disease, where the body’s white blood cells attack healthy tissue and organs. With Sjögren’s syndrome, your immune system attacks the lacrimal and salivary glands that keep our eyes and mouth lubricated. This is why dry eyes are very common with Sjögren’s syndrome 7. Nine out of 10 people who have Sjögren syndrome are women between 40 and 60 years old. However, Sjögren syndrome can affect men and women of any age.
Stay away from dry environments and things that irritate your eyes to help prevent dry eye symptoms.
The first step in keratoconjunctivitis sicca treatment is artificial tears. These come as preserved (screw cap bottle) and unpreserved (twist open vial). Preserved tears are more convenient, but some people are sensitive to preservatives. There are many brands available without a prescription.
Start using the artificial tears at least 2 to 4 times per day. If your symptoms are not better after a couple of weeks of regular use:
- Increase use (up to every 2 hours).
- Change to unpreserved drops if you have been using the preserved type.
- Try a different brand.
- Talk to your doctor if you cannot find a brand that works for you.
Other treatments for keratoconjunctivitis sicca may include:
- Fish oil 2 to 3 times per day
- Glasses, goggles or contact lenses that keep moisture in the eyes
- Medicines such as cyclosporine (Restasis) or lifitegrast (Xiidra), corticosteroid eye drops, and oral tetracycline and doxycycline
- Tiny plugs placed in the tear drainage ducts to help moisture stay on the surface of the eye longer
Other helpful remedies include:
- DO NOT smoke.
- Avoid second-hand smoke, direct wind, and air conditioning.
- Use a humidifier, particularly in the winter.
- Limit allergy and cold medicines that may dry you out and worsen your symptoms.
- Purposefully blink more often. Rest your eyes once in a while.
- Clean eyelashes regularly and apply warm compresses.
Some dry eye symptoms are due to sleeping with the eyes slightly open. Lubricating ointments work best for this problem. You should use them only in small amounts since they can blur your vision. It is best to use them before sleep.
Surgery may be helpful if your dry eyes are caused by the eyelids being in an abnormal position.
Figure 1. Meibomian glands
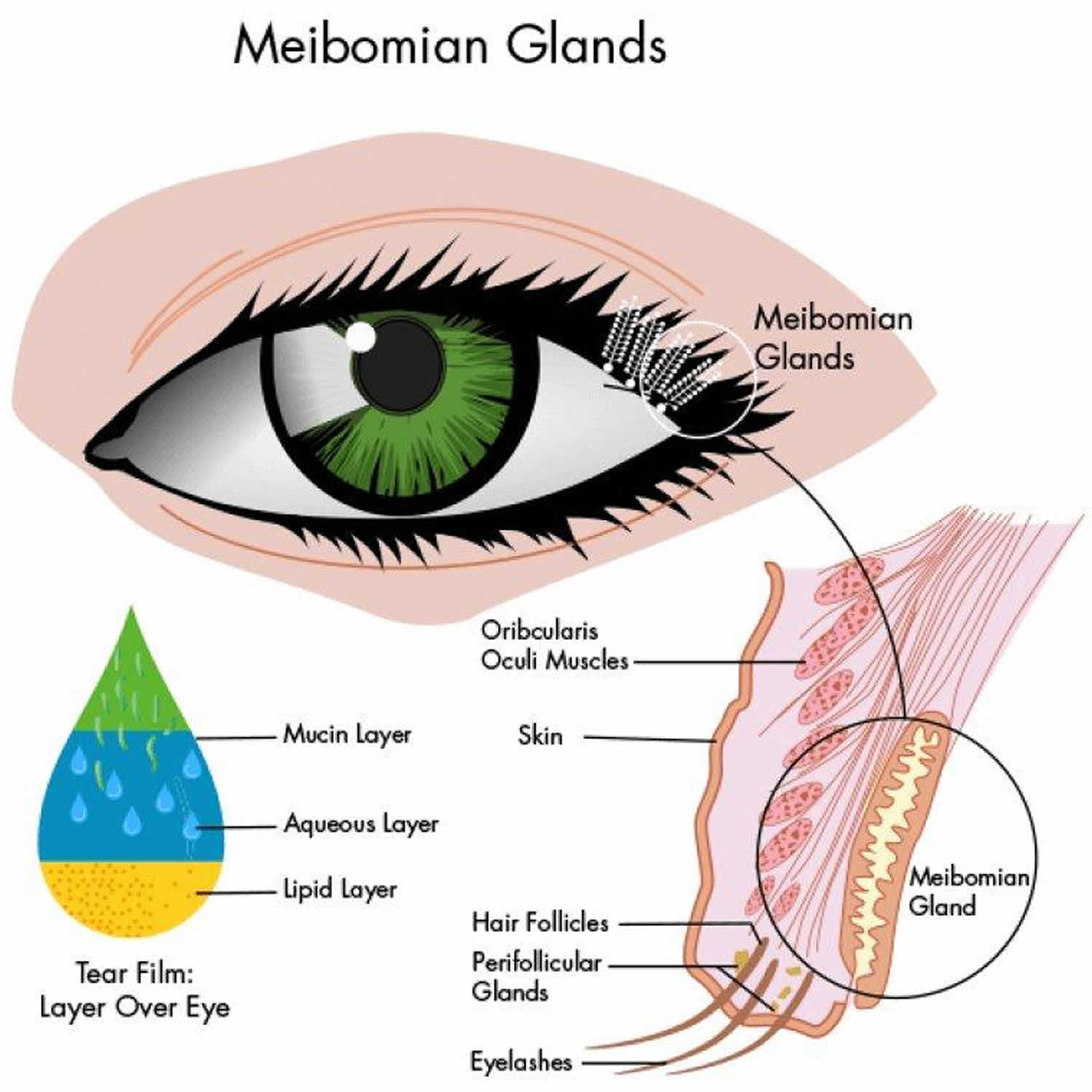
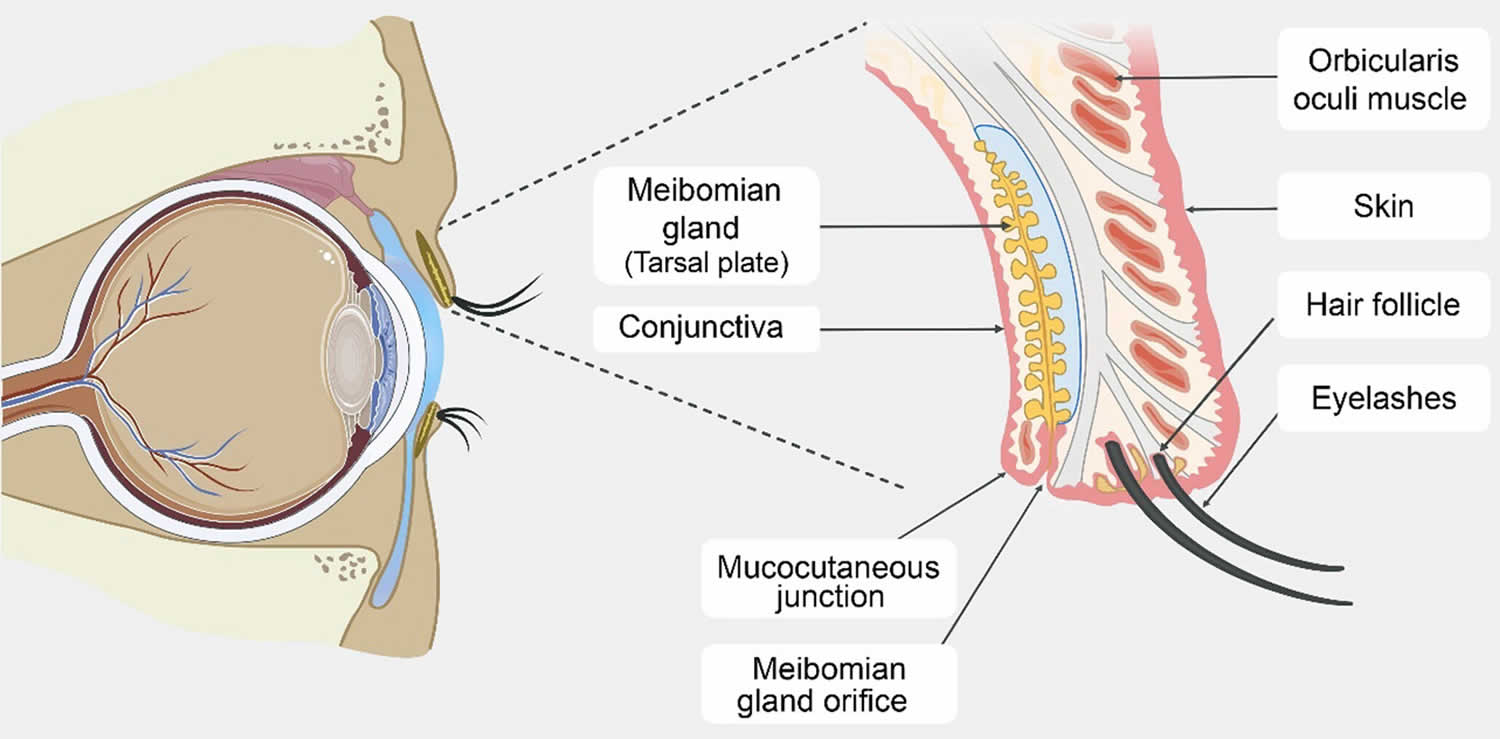
Figure 2. Tear film (structure of the tear film)
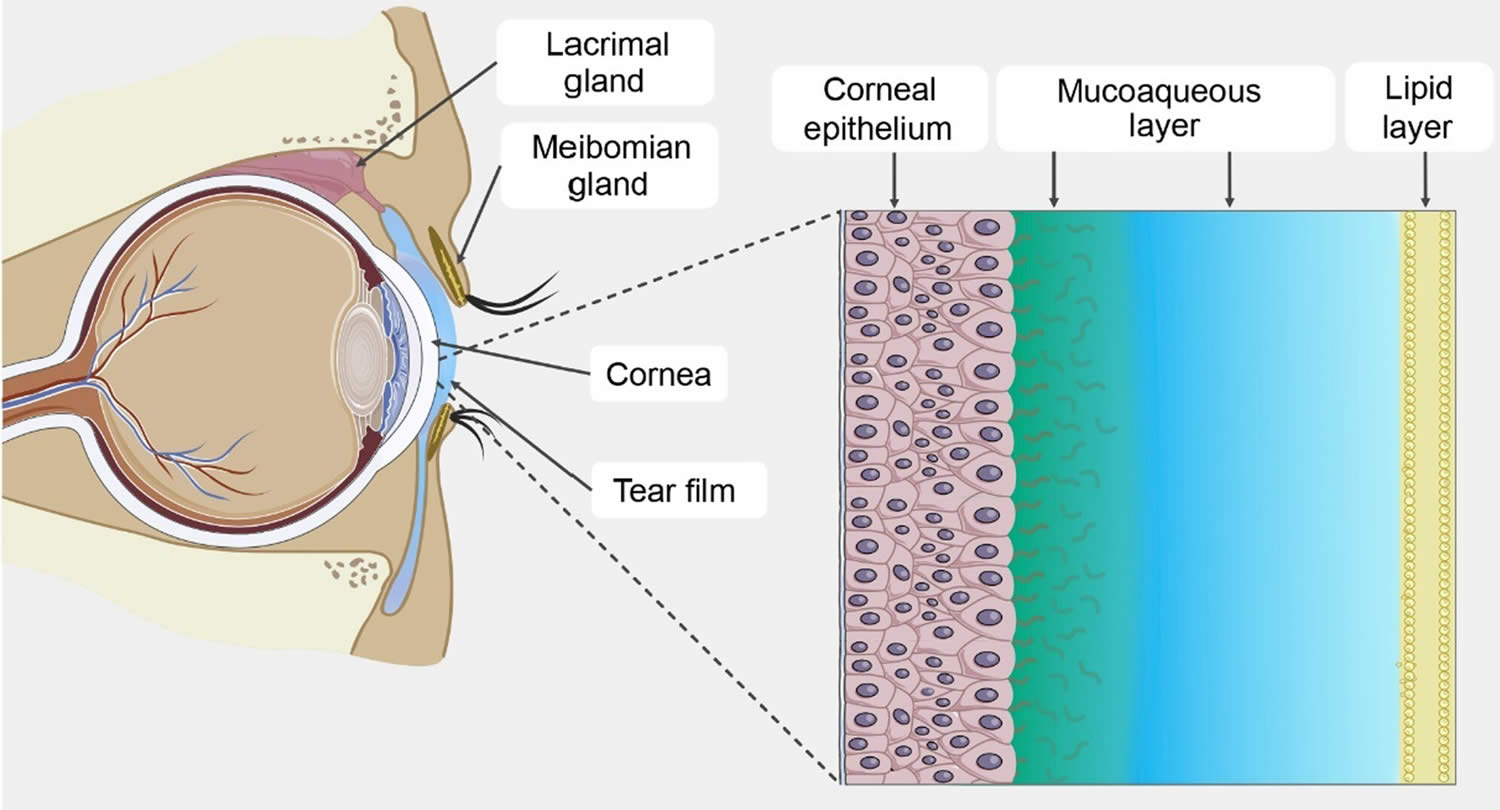
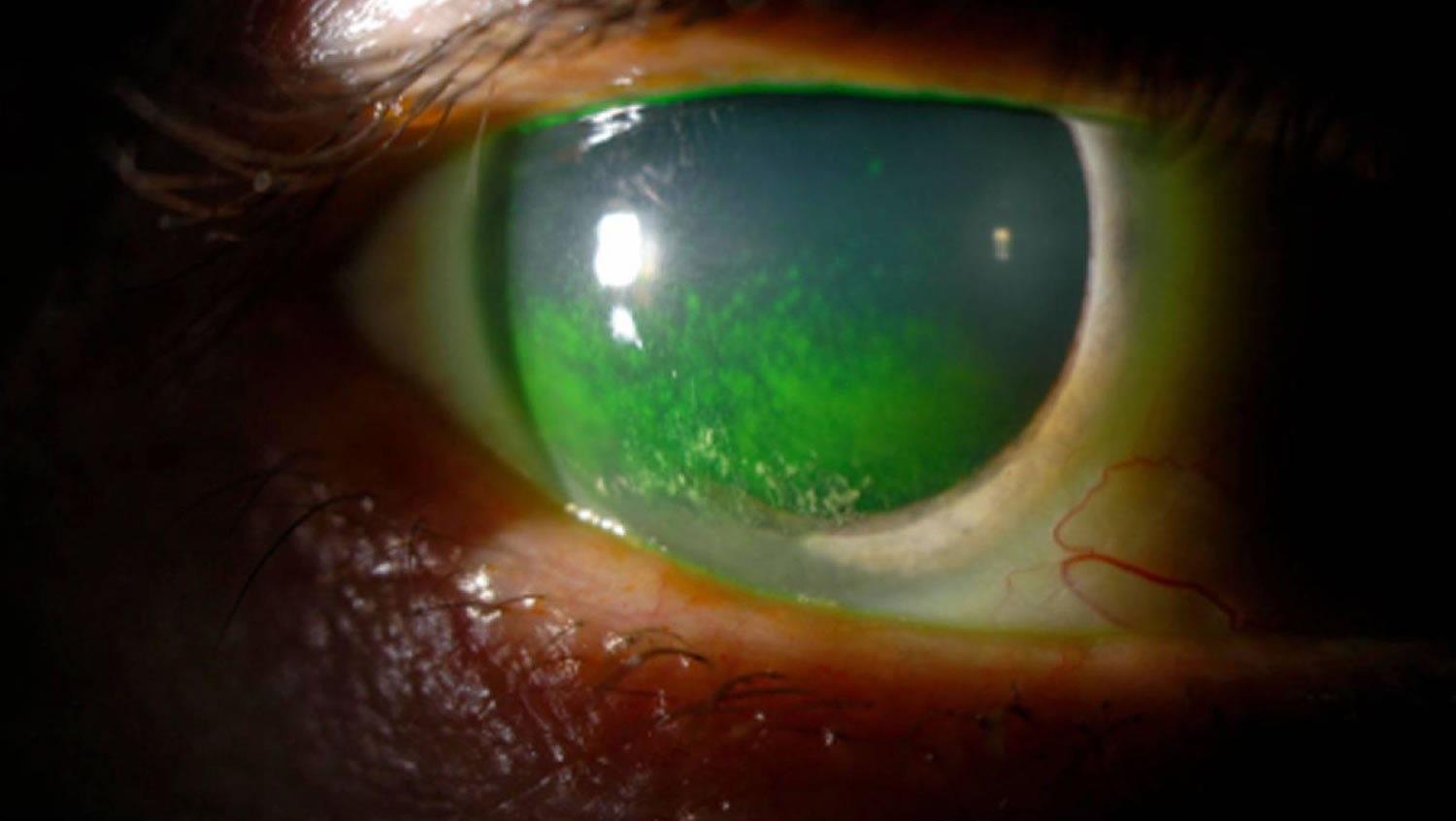
Figure 3. Keratoconjunctivitis sicca
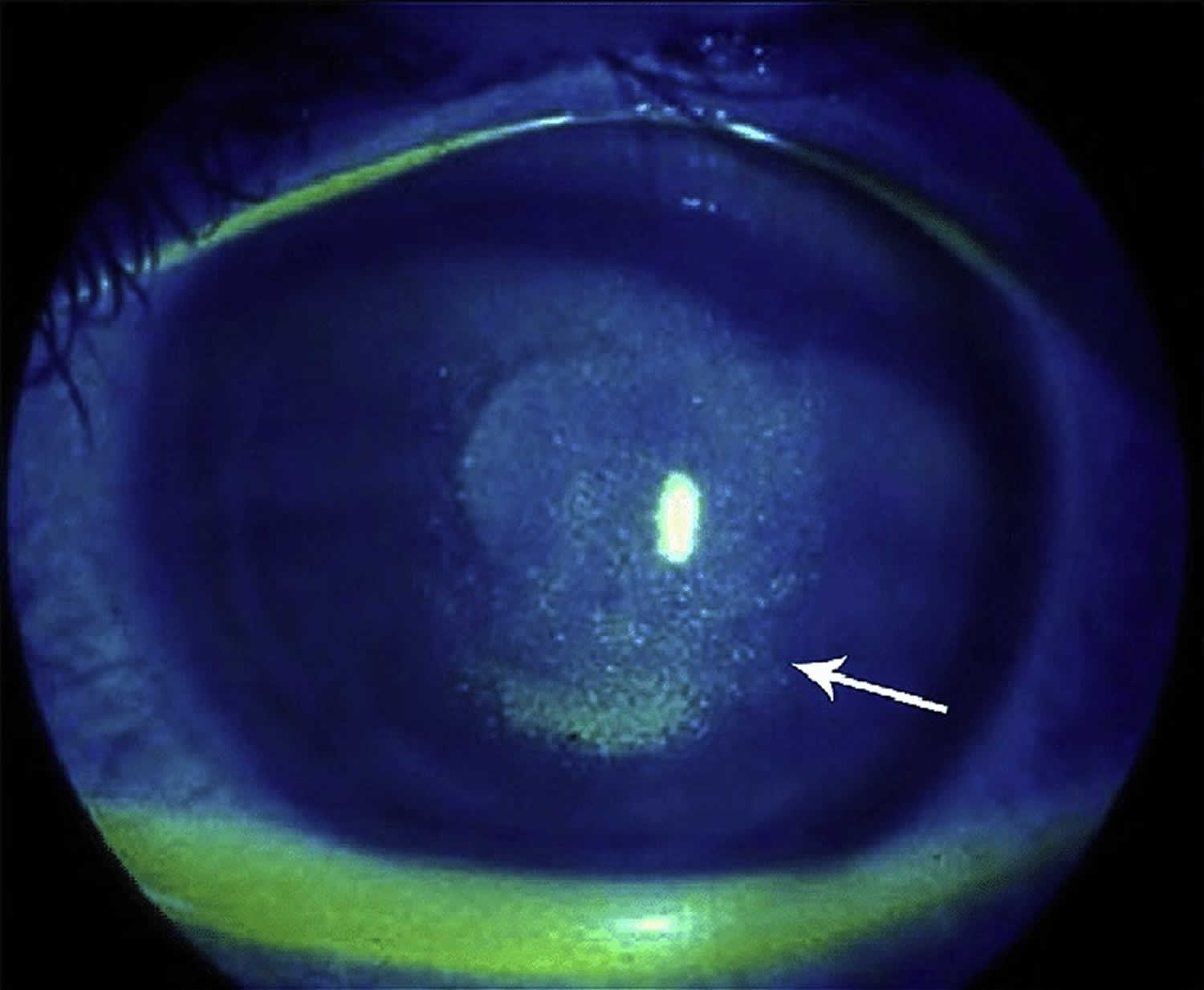
Footnote: Keratoconjunctivitis sicca. Arrow points to punctate epithelial erosion resulting from corneal dessication.
[Source 9 ]Figure 4. Keratoconjunctivitis sicca in a patient with Sjögren’s syndrome
Keratoconjunctivitis sicca causes
Keratoconjunctivitis sicca causes include 1:
- Allergies
- Aging associated with decreased hormones
- Pregnancy and associated hormonal changes
- Thyroid eye conditions
- Leukemia
- Lymphoma (cancer of the lymph system)
- Eyelid inflammation (blepharitis)
- Medication/supplement use including, but not limited to: psychiatric medicines, OTC cold medicines, anti-histamines, beta-blockers, pain relievers, sleeping pills, diuretics, hormonal replacement, and oral contraceptives
- Sjögren’s syndrome (dry mucus membranes throughout body)
- Other autoimmune disorders including Lupus and/or Rheumatoid Arthritis
- Chemical exposures / injuries to the eyes
- Previous eyelid, eye or facial surgery
- Laser vision correction
- Infrequent blinking, associated with staring at computer or video screens which is becoming a more frequent contributor and Parkinson’s disease
- Environmental (dusty, windy, hot/dry)
- Contact lens use
- Neurologic conditions including: stroke, Bell’s palsy, Parkinson’s, trigeminal nerve dysfunction
- Exposure keratitis, in which the eyelids do not close completely during sleep (i.e. lagophthalmos)
- Corneal ulcers and infections
- Post refractive surgery (LASIK or PRK)- while typically transient can become a chronic issue in some
- Inflammatory eye conditions, including conjunctivitis, uveitis or iritis
- Diabetes
- Infectious Keratitis, including Herpes Simplex and Herpes Zoster Keratitis
- Neurotrophic Keratitis
- Vitamin A deficiency (rare in US except in certain diseases such as Crohn’s disease).
Keratoconjunctivitis sicca symptoms
There are numerous different symptoms one can experience from keratoconjunctivitis sicca or dry eye syndrome, prominent amongst these symptoms is tearing 1. Naturally, a person with keratoconjunctivitis sicca may wonder why their eye(s) can be “dry” despite producing plenty of tears. This is because of the unhealthy tear film and the irritation that comes from it stimulates the brain to produce a wave or reflex of tears to help counteract the irritation. However, this reflex tearing is simply insufficient to correct the overall problem. For this reason, dry eye syndrome could more appropriately be termed “Tear Film Dysfunction”. Other symptoms of dry eye syndrome or tear film dysfunction include 1:
- Burning
- Stinging
- Itching
- Tearing
- Sandy or gritty feeling in the eye
- Scratchy or foreign-body sensation
- Discharge
- Frequent blinking
- Mattering or caking of the eyelashes (usually worse upon waking)
- Redness in the eye
- Blurry or fluctuating vision (made worse when reading, computer, watching television, driving, or playing video games)
- Sensitivity to light or photophobia
- Eye pain and/or headache
- Heavey eye lids
- Eye fatigue.
Keratoconjunctivitis sicca complications
Keratoconjunctivitis sicca complications range from mild to severe. Mild-to-moderate dry eye syndrome causes symptoms detailed above, including eye irritation or visual disturbances. More severe diseases can result in corneal complications, including infectious keratitis, ulceration, and scarring, which may cause subsequent loss of vision 11, 12. Although causation has not been established, several non eye complications exist with dry eye syndrome, including depression, sleep and mood disorders, dyslipidemia, and migraine headaches 13, 14.
Keratoconjunctivitis sicca diagnosis
Currently, there is NO “gold standard” diagnostic procedure for dry eye conditions 1. The debate on the most appropriate dry eye diagnostic tests for clinical practice is ongoing. Most people with dry eye syndrome or keratoconjunctivitis sicca have signs which are not even obvious on a general eye exam. An individual with dry eye syndrome or keratoconjunctivitis sicca may, in fact, have more than one cause acting simultaneously to produce his/her symptoms. This is actually the case for many persons who suffer from dry eye syndrome. For this reason, many persons who undergo casual examination and/or treatment attempts of dry eye syndrome without investigating for and treating all the possible causes can end up becoming frustrated, have persistent symptoms that can worsen, and may jump from doctor to doctor to seek relief.
A thorough history is essential in the workup of dry eye symptoms due to the frequent lack of correlation between symptoms and exam findings 15, 16. Examination should include evaluation of the face and eyelids, blinking patterns, eyelid margins, eyelashes, conjunctiva, cornea, and tear film.
Depending on the particular constellation of signs, symptoms, history and comorbidities, dry eye syndrome or keratoconjunctivitis sicca tests may include Schirmer’s tear test and blood tests to check for systemic disease may be warranted. The phenol red thread test is similar to the Schirmer’s tear test, except that red strips of special thread are used instead of paper strips. Numbing drops are not needed. The test takes 15 seconds.
People with dry eye syndrome or keratoconjunctivitis sicca may have these tests:
- Visual acuity measurement
- Slit lamp exam
- Diagnostic staining of the cornea and tear film
- Measurement of tear film break-up time (TBUT)
- Measurement of rate of tear production (Schirmer’s tear test or phenol red thread test)
- Measurement of concentration of tears (osmolality)
Schirmer’s tear test (Schirmer test)
A Schirmer’s tear test is a diagnostic tool that measures the amount of tears produced by your eyes to determine if they are producing enough to keep your eyes moist 17, 18. It’s often used to diagnose dry eye syndrome, but it can also be used to assess tear overproduction.
Here’s how Schirmer’s tear test is performed:
- The patient is given numbing eye drops to prevent your eyes from tearing due to irritation from the paper strips. Sometimes the test is done without numbing drops to test for other types of tear problems.
- The eye doctor will place the end of Schirmer strips or filter paper (Whatman filter paper #41) with dimensions 35 mm and 5 mm inside the lower eyelid of each eye 19
- The patient closes their eyes gently for 5 minutes. Closing the eyes tightly or rubbing the eyes during the test can cause abnormal test results.
- After 5 minutes, the eye doctor removes the paper strips and measures how much they became moistened.
- Do not rub the eyes for at least 30 minutes after the test. Leave contact lenses out for at least 2 hours after the test.
The amount of moisture on the paper strip indicates the level of tear production 17:
- Normal: More than 15 millimeters of moisture on the filter paper after 5 minutes (>10 mm). More than 15 mm of moisture is a sign of normal tear production. Both eyes normally release the same amount of tears
- Possible dry eyes: 10 to 15 millimeters (10 to 15 mm)
- Moderately dry eyes: 5 to 10 millimeters (5 to 10 mm)
- Extremely dry eyes: 0 to 5 millimeters (0 to 5 mm)
The Dry Eye Workshop (DEWS) proposes a Schirmer test cutoff value of 10 mm for 5 minutes as one of the criteria for diagnosing dry eye disease 20. The dry eye disease cutoff value varies in the literature, ranging from 15 mm originally reported by Schirmer, 10 mm by the Dry Eye Workshop (DEWS), 10 mm by Jones, and 5 mm by Sjogren 17. A test result of less than 5 mm indicates a pathologic dry eye, while more than 15 mm is considered normal 17.
Studies have shown that the Schirmer test has acceptable levels of intraexaminer reproducibility and interexaminer repeatability. Topical anesthesia does not seem to affect these parameters 21. Experts recommend that the same examiner conduct the testing during follow-up visits and repeated same-day measures if confirmation of results is needed.
Even though the Schirmer test has been available since 1903, several studies show that it does not properly identify a large group of people with dry eyes. It is most useful in the diagnosis of patients with severe aqueous deficiency, but is relatively insensitive for patients with mild dry eye 22. Newer and better tests are being developed. One test measures a molecule called lactoferrin. People with low tear production and dry eye have low levels of this molecule.
Another test measures tear osmolarity, or how concentrated the tears are. The higher the osmolarity, the more likely it is that you have dry eye.
Tear Osmolarity
Patients with dry eye disease have been found to have elevated tear film osmolarity (TFO) 23, 24. Tear hyperosmolarity can induce tear film instability by modifying the interaction between tear film lipids and proteins, damaging the epithelial cell membranes, triggering inflammation, and stimulating corneal nerves 25, 26.
Tear osmolarity can be determined easily in the office using the point of care TearLab Osmolarity System (TearLab, San Diego, CA), which measures the osmolarity of a 50 nanoliter (50 nL) tear sample. Normal values are considered to be 296±9.8 mOsm/L 23 27. Greater than 308 mOsm/L is considered to indicate at least mild dry eye and has been demonstrated to serve as an early indicator of ocular surface instability 28.
The test is performed by placing the tip of the handheld device at the lateral tear meniscus and then docking the sampler into the reader. The device contains a gold-plated microchip that measures electrical impedance in the sample and displays the osmolarity measurement within seconds.
Tear film osmolarity (TFO) testing is indicated for use in conjunction with other signs and symptoms. Combination of tear film osmolarity (TFO) with at least one other dry eye test will enhance the sensitivity and specificity 29, 30, 31. Schargus et al 28, however, did not find a significant correlation between tear film osmolarity (TFO) and MMP-9 levels or with any other clinical dry eye test.
Matrix metalloproteinase 9 (MMP-9)
Stressed epithelial cells on the eye surface can produce matrix metalloproteinases (MMP) 1. Matrix metalloproteinase 9 (MMP-9) has been shown to be elevated in the tears of patient with dry eye disease, and levels correlate with examination findings in patients with moderate to severe dry eye. The normal range of MMP-9 levels in human tears is 3 to 40 ng/mL 32. MMP-9 levels can be elevated in other inflammatory conditions, such as graft-versus-host disease, Stevens-Johnson syndrome, and following corneal surgery.
InflammaDry (Rapid Pathogen Screening Inc, Sarasota, FL) is a single use, noninvasive, disposable test that detects MMP-9 levels of 40 ng/mL or higher 1.
The InflammaDry test is performed prior to instillation of anesthetic eye drops by dabbing the sample collector at multiple sites along the palpebral conjunctiva. The lid can be released every 2 to 3 dabs to allow blinking. This should be repeated 6 to 8 times, after which the sampling fleece should rest against the conjunctiva for at least 5 seconds or until it is saturated with tears (indicated by a pink or glistening appearance). The sample collector is then snapped onto the test cassette and dipped into the buffer solution for activation. After 10 minutes, the test is read. One blue line and one red line indicate a positive test result, and the intensity of the red line is related to MMP-9 concentration. One blue line only indicates a negative test result.
The InflammaDry test was shown to have a sensitivity of 85% and specificity of 94% 33. In another study by Sambursky et al 34, the test was found to have a total positive and negative agreement of 81% (127/157) and 98% (78/80), respectively, with clinical assessment when Ocular Surface Disease Index (OSDI) was included in the definition of mild dry eye. When Ocular Surface Disease Index (OSDI) was excluded, the InflammaDry demonstrated a positive and negative agreement with clinical assessment of 86% (126/146) and 97% (88/91), respectively. Studies have also demonstrated that elevated MMP-9 levels correlate most with other dry eye tests in advanced disease and is likely a late sign that is rarely present in mild cases 28, 35.
Corneal sensation
Corneal hyperesthesia and/or reduced sensation may be present in severe and chronic dry eye disease 36. Sensory denervation may cause dry eye by reducing the afferent signaling of tear production, reducing the blink rate, and by altering trigeminal nerve influences on eye epithelial health. Decreased corneal sensation can also result from chronic dry eye.
Corneal sensation can be measured using a cotton tip applicator or more precisely with a Cochet-Bonnet esthesiometer 1.
Tear break up time (TBUT)
Tear break up time (TBUT) is an indication of tear film stability 1. The proper method of tear break up time (TBUT) testing is using a fluorescein-impregnated strip wet with non-preserved saline solution (benzalkonium chloride can increase tear break up speed) 1. The dye is distributed by blinking, and the patient is then asked to stare straight ahead without blinking. The tear film is observed under the cobalt blue light of a slit lamp, and the time between the last blink and the appearance of the first dry spot or hole in the tear film is measured and equal to the tear break up time (TBUT).
Tear break up time (TBUT) has been shown to be decreased in keratoconjunctivitis sicca, mucin deficiency, and Meibomian gland disease 1. Normal subjects show variability in tear break up time (TBUT), although 10 seconds is the typical cutoff between normal and abnormal results and has been found to be relatively specific in screening patients for tear film instability 37.
Delayed tear clearance
Following fluorescein placement, the persistence of fluorescein in the tear film at various time points can be determined. This may be more important to rule out nasolacrimal duct issues as a cause of tearing or epiphora.
Tear meniscus height (meniscometry)
The tear meniscus height can be used to estimate tear volume. A tear meniscus height less than 0.25 mm is suggestive of dry eye.
Tear film interferometry
Interferometry of the lipid layer of the tear film is a noninvasive method of grading tear film quality and estimating the thickness of the lipid layer, which have been shown to be abnormal in evaporative dry eye that is secondary to meibomian gland dysfunction. The LipiView interferometer (TearScience Inc, Morrisville, NC) is a commercially available tool that can measure lipid layer thickness.
Sjö test
Sjögren’s syndrome is an autoimmune disease, where the body’s white blood cells attack healthy tissue and organs 38. With Sjögren’s syndrome, your immune system attacks the lacrimal and salivary glands that keep our eyes and mouth lubricated 38. This is why dry eyes are very common with Sjögren’s syndrome. Traditionally, Sjögren’s syndrome has been diagnosed using the detection of SS-A (anti-Ro) and SS-B (anti-La) autoantibodies in serum. Of these, SS-A (anti-Ro) is probably the most sensitive and specific antibody for Sjogren’s but alone is not diagnostic since it may be present in other autoimmune disorders and may be absent in up to a third of Sjogren cases 38. The most specific single test is a minor salivary gland (lip) biopsy which will demonstrate focal lymphocytic sialadenitis in positive specimens 39, 40, 41.
Recently, additional autoantibodies were identified as diagnostic of Sjogrens syndrome. These include autoantibodies to salivary gland protein 1 (SP-1), carbonic anhydrase 6 (CA6), and parotid secretory protein (PSP). SP-1, CA6, and PSP were found in 45% of patients who met clinical criteria for Sjögren’s syndrome but tested negative for anti-Ro and anti-La. The novel autoantibodies may be present earlier in the disease course. In a study of patients with xerostomia and xerophthalmia for less than two years, 76% had autoantibodies to SP-1 or CA6 compared to 31% who had anti-Ro or anti-La antibodies 42. Currently in clinical practice, SP-1, CA-6, and PSP autoantibody levels can be determined using a commercially available blood test called Sjö (Bausch & Lomb), which also includes SS-A, SS-B, antinuclear antibody (ANA), and rheumatoid factor (RF) levels in its panel.
The test can be administered in the office using a simple finger stick with a lancet. Once a large drop of blood appears, the five dotted circles on the test card are filled. The sample is then allowed to air dry for 30 minutes, after which it can be sealed in a plastic envelope with a dessicating package. The sample along with the patient information is then mailed in. Test results are typically available within one week.
Ocular surface staining
Fluorescein sodium
Fluorescein dye is the most commonly used stain in ophthalmology. Areas in which the corneal or conjunctival surface epithelial cells are loose or desquamated will stain with fluorescein. Fluorescein dye should be instilled as described above. The degree of staining can be graded using various scales 37.
Rose Bengal
Rose Bengal is more sensitive for conjunctival staining, but also more difficult to visualize and less well tolerated compared to fluorescein. Rose Bengal stains devitalized epithelial cells that lack a healthy mucin coating. It is applied using a dye-impregnated paper strip.
Interpretation of staining is based on intensity and location using a grading scale described by van Bijsterveld 43. The nasal and temporal conjunctiva and the cornea are graded on a scale of 0-3 with a maximum possible score of 9.
In aqueous tear deficiency, the interpalpebral conjunctiva is the most common location for Rose Bengal staining 1. The severity of staining has been shown to correlate with the degree of aqueous deficiency, tear film instability, and reduced mucin production by conjunctival goblet and epithelial cells 37.
Lissamine green
Lissamine green has similar staining characteristics but is much better tolerated than Rose Bengal 1. Lissamine green is also available in dye-impregnated paper strips 1.
Keratoconjunctivitis sicca differential diagnosis
Many conditions may evoke symptoms similar to those caused by keratoconjunctivitis sicca 20. Some conditions may also be associated with or lead to keratoconjunctivitis sicca, such as allergic conjunctivitis, cicatricial conjunctivitis, filamentary keratitis, and neurotrophic keratitis 44. Identifying the underlying primary condition in these cases is key to reducing the progression of the disease and worsening of dry eye.
Differential diagnosis for keratoconjunctivitis sicca include 44:
- Conjunctivitis (allergic, viral, bacterial, parasitic/chlamydial)
- Anterior blepharitis
- Demodex blepharitis
- Cicatricial conjunctivitis (Stevens-Johnson Syndrome, mucous membrane pemphigoid)
- Bullous keratopathy
- Contact lens–related keratoconjunctivitis
- Eyelid malposition (entropion, ectropion) or abnormality (trichiasis) leading to ocular surface disease
- Keratitis (interstitial, filamentary, contact lens–related, neurotrophic)
Keratoconjunctivitis sicca treatment
Depending on the causes of keratoconjunctivitis sicca or your dry eyes, there are numerous treatments for dry eye syndrome or tear film dysfunction, but the more common treatment modalities include 1, 44, 45:
- Education about the condition
- Lid hygiene (warm compresses and eyelash and eyelid scrubs)
- Oral essential fatty acid supplements. Oral flaxseed oil or fish oil supplements 2000mg/day has also been found to be useful in alleviating symptoms and decreasing the frequency of topical agents anecdotally. However, the DREAM (Dry Eye Assessment and Management Study) Research Group concluded that patients with dry eye who received 3,000 mg of fish-derived n-3 fatty acids for 12 months had no significantly better outcomes than patients who received an olive oil placebo 46.
- Modification of the environment
- Eliminating direct high airflow or fans
- Reducing screen time
- Taking frequent screen breaks
- Using a humidifier
- Identification and elimination of offending topical and systemic agents
- Topical eye lubricants or artificial tears (preferably ones without a redness-reliever component in them)
- Longer acting agents such as artificial tear gel and ointments and LACRISERT® (hydroxypropyl cellulose ophthalmic insert)
- Tear conserving interventions such as punctal plugs or nighttime masks/goggles
- Prescription medicines such as Restasis (cyclosporine 0.05%) (increase tear-production), Cequa (cyclosporine 0.09%) (increase tear production) or Xiidra (lifitegrast 5%) (mechanism unknown-however is a small molecule integrin antagonist)
- Topical ophthalmic steroids are helpful in controlling the inflammatory aspect of the disease in short bursts.
- Oral antibiotics (macrolide or tetracycline) 47
- TearCare (Automated Meibomian Gland Heating/Manual Expression Procedure)
- LipiFlow (Automated Meibomian Gland Heating and Expression Procedure)
- Intense Pulsed Light (IPL) Therapy.
Additional treatment options include 44:
- Serum eye drops. Autologous serum tears, compounded artificial tears with mixed with the patient’s serum, can be particularly helpful in recalcitrant cases.
- Oral or topical secretagogues
- Therapeutic contact lenses
- Amniotic membrane grafting
- Surgical punctal occlusion
- Tarsorrhaphy.
Keratoconjunctivitis sicca prognosis
There are minimal published data describing the natural history of treated and untreated dry eye syndrome 48. Dry eye syndrome is often considered chronic, with periods of exacerbation due to intermittent contributing factors. Most people with dry eye syndrome who keep up with their regimen as prescribed by their eye doctor are able to have their symptoms controlled, allowing them to function either symptom-free or with minimal difficulty 1. Because of the nature of the causes of dry eye syndrome, most people do not get “cured” of their problem, but with regular maintenance can function as though they are cured 1. However, even the patient who is well-controlled on maintenance therapy can have break-through episodes and require a visit to their eye doctor, in addition to regularly scheduled visits.
Postsurgical dry eye such as following cataract surgery or refractive surgery often improves with time, possibly related to the regeneration of corneal nerves or reduction of ocular inflammation 49.
- Dry Eye Syndrome. https://eyewiki.org/Dry_Eye_Syndrome[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Dry eye syndrome. https://medlineplus.gov/ency/article/000426.htm[↩]
- Alshamrani AA, Almousa AS, Almulhim AA, Alafaleq AA, Alosaimi MB, Alqahtani AM, Almulhem AM, Alshamrani MA, Alhallafi AH, Alqahtani IZ, Alshehri AA. Prevalence and Risk Factors of Dry Eye Symptoms in a Saudi Arabian Population. Middle East Afr J Ophthalmol. 2017 Apr-Jun;24(2):67-73. doi: 10.4103/meajo.MEAJO_281_16[↩]
- Lin PY, Tsai SY, Cheng CY, Liu JH, Chou P, Hsu WM. Prevalence of dry eye among an elderly Chinese population in Taiwan: The Shihpai Eye Study. Ophthalmology. 2003;110:1096–101. doi: 10.1016/S0161-6420(03)00262-8[↩]
- Lee AJ, Lee J, Saw SM, Gazzard G, Koh D, Widjaja D, et al. Prevalence and risk factors associated with dry eye symptoms: A population based study in Indonesia. Br J Ophthalmol. 2002;86:1347–51. doi: 10.1136/bjo.86.12.1347[↩]
- McCarty CA, Bansal AK, Livingston PM, Stanislavsky YL, Taylor HR. The epidemiology of dry eye in Melbourne, Australia. Ophthalmology. 1998;105:1114–9. doi: 10.1016/S0161-6420(98)96016-X[↩]
- What Is Sjögren’s Syndrome? https://www.aao.org/eye-health/diseases/what-is-sjogren-syndrome[↩]
- Fineide, F., Magnø, M.S., Khan, A.Z., Chen, X., Vehof, J. & Utheim, T.P. (2024) Intense pulsed light treatment in meibomian gland dysfunction: Past, present, and future. Acta Ophthalmologica, 102, e414–e442. Available from: https://doi.org/10.1111/aos.15759[↩][↩]
- Jeganathan VS, Wirth A, MacManus MP. Ocular risks from orbital and periorbital radiation therapy: a critical review. Int J Radiat Oncol Biol Phys. 2011 Mar 1;79(3):650-9. doi: 10.1016/j.ijrobp.2010.09.056[↩]
- Simpson RG, Moshirfar M, Edmonds JN, Christiansen SM, Behunin N. Laser in situ keratomileusis in patients with collagen vascular disease: a review of the literature. Clin Ophthalmol. 2012;6:1827-37. doi: 10.2147/OPTH.S36690[↩]
- Li M, Gong L, Sun X, Chapin WJ. Anxiety and depression in patients with dry eye syndrome. Curr Eye Res. 2011 Jan;36(1):1-7. doi: 10.3109/02713683.2010.519850[↩]
- Ayaki M, Kawashima M, Negishi K, Tsubota K. High prevalence of sleep and mood disorders in dry eye patients: survey of 1,000 eye clinic visitors. Neuropsychiatr Dis Treat. 2015 Mar 31;11:889-94. doi: 10.2147/NDT.S81515[↩]
- Aldaas KM, Ismail OM, Hakim J, Van Buren ED, Lin FC, Hardin JS, Meyer JJ. Association of Dry Eye Disease With Dyslipidemia and Statin Use. Am J Ophthalmol. 2020 Oct;218:54-58. doi: 10.1016/j.ajo.2020.05.007[↩]
- Ismail OM, Poole ZB, Bierly SL, Van Buren ED, Lin FC, Meyer JJ, Davis RM. Association Between Dry Eye Disease and Migraine Headaches in a Large Population-Based Study. JAMA Ophthalmol. 2019 May 1;137(5):532-536. doi: 10.1001/jamaophthalmol.2019.0170[↩]
- The epidemiology of dry eye disease: report of the Epidemiology Subcommittee of the International Dry Eye WorkShop (2007). Ocul Surf. 2007 Apr;5(2):93-107. doi: 10.1016/s1542-0124(12)70082-4[↩]
- Nichols KK, Nichols JJ, Mitchell GL. The lack of association between signs and symptoms in patients with dry eye disease. Cornea. 2004 Nov;23(8):762-70. doi: 10.1097/01.ico.0000133997.07144.9e[↩]
- Brott NR, Zeppieri M, Ronquillo Y. Schirmer Test. [Updated 2024 Feb 24]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK559159[↩][↩][↩][↩]
- Schirmer test. https://medlineplus.gov/ency/article/003501.htm[↩]
- Negrel AD, Lemasson JM. Papier filtre Whatman-41 et prélèvement des sécrétions du cul-de-sac conjonctival [Whatman-41 filter paper and sample of the secretions of the conjunctival cul-de-sac]. Rev Int Trach Pathol Ocul Trop Subtrop. 1979;56(3-4):69-72. French.[↩]
- Wolffsohn JS, Arita R, Chalmers R, Djalilian A, Dogru M, Dumbleton K, Gupta PK, Karpecki P, Lazreg S, Pult H, Sullivan BD, Tomlinson A, Tong L, Villani E, Yoon KC, Jones L, Craig JP. TFOS DEWS II Diagnostic Methodology report. Ocul Surf. 2017 Jul;15(3):539-574. doi: 10.1016/j.jtos.2017.05.001[↩][↩]
- Lee JH, Hyun PM. The reproducibility of the Schirmer test. Korean J Ophthalmol. 1988 Jun;2(1):5-8. doi: 10.3341/kjo.1988.2.1.5[↩]
- Krachmer. (2013). Cornea, 3rd Edition. Elsevier.[↩]
- Versura P, Profazio V, Campos EC. Performance of tear osmolarity compared to previous diagnostic tests for dry eye diseases. Curr Eye Res. 2010 Jul;35(7):553-64. doi: 10.3109/02713683.2010.484557[↩][↩]
- Lemp MA, Bron AJ, Baudouin C, Benítez Del Castillo JM, Geffen D, Tauber J, Foulks GN, Pepose JS, Sullivan BD. Tear osmolarity in the diagnosis and management of dry eye disease. Am J Ophthalmol. 2011 May;151(5):792-798.e1. doi: 10.1016/j.ajo.2010.10.032[↩]
- The definition and classification of dry eye disease: report of the Definition and Classification Subcommittee of the International Dry Eye WorkShop (2007). Ocul Surf. 2007 Apr;5(2):75-92. doi: 10.1016/s1542-0124(12)70081-2[↩]
- Baudouin C. The pathology of dry eye. Surv Ophthalmol. 2001 Mar;45 Suppl 2:S211-20. doi: 10.1016/s0039-6257(00)00200-9[↩]
- TearLab® Osmolarity System. https://www.labtician.com/therapeutics/product/tearlab/[↩]
- Schargus M, Ivanova S, Kakkassery V, Dick HB, Joachim S. Correlation of Tear Film Osmolarity and 2 Different MMP-9 Tests With Common Dry Eye Tests in a Cohort of Non-Dry Eye Patients. Cornea. 2015 Jul;34(7):739-44. doi: 10.1097/ICO.0000000000000449[↩][↩][↩]
- Sullivan BD, Crews LA, Sönmez B, de la Paz MF, Comert E, Charoenrook V, de Araujo AL, Pepose JS, Berg MS, Kosheleff VP, Lemp MA. Clinical utility of objective tests for dry eye disease: variability over time and implications for clinical trials and disease management. Cornea. 2012 Sep;31(9):1000-8. doi: 10.1097/ICO.0b013e318242fd60[↩]
- Szalai E, Berta A, Szekanecz Z, Szûcs G, Módis L Jr. Evaluation of tear osmolarity in non-Sjögren and Sjögren syndrome dry eye patients with the TearLab system. Cornea. 2012 Aug;31(8):867-71. doi: 10.1097/ICO.0b013e3182532047[↩]
- Baudouin C, Aragona P, Messmer EM, Tomlinson A, Calonge M, Boboridis KG, Akova YA, Geerling G, Labetoulle M, Rolando M. Role of hyperosmolarity in the pathogenesis and management of dry eye disease: proceedings of the OCEAN group meeting. Ocul Surf. 2013 Oct;11(4):246-58. doi: 10.1016/j.jtos.2013.07.003[↩]
- Sambursky R, O’Brien TP. MMP-9 and the perioperative management of LASIK surgery. Curr Opin Ophthalmol. 2011 Jul;22(4):294-303. doi: 10.1097/ICU.0b013e32834787bb[↩]
- Sambursky R, Davitt WF 3rd, Latkany R, Tauber S, Starr C, Friedberg M, Dirks MS, McDonald M. Sensitivity and specificity of a point-of-care matrix metalloproteinase 9 immunoassay for diagnosing inflammation related to dry eye. JAMA Ophthalmol. 2013 Jan;131(1):24-8. doi: 10.1001/jamaophthalmol.2013.561. Erratum in: JAMA Ophthalmol. 2013 Mar 1;131(3):364.[↩]
- Sambursky R, Davitt WF 3rd, Friedberg M, Tauber S. Prospective, multicenter, clinical evaluation of point-of-care matrix metalloproteinase-9 test for confirming dry eye disease. Cornea. 2014 Aug;33(8):812-8. doi: 10.1097/ICO.0000000000000175[↩]
- Chotikavanich S, de Paiva CS, Li de Q, Chen JJ, Bian F, Farley WJ, Pflugfelder SC. Production and activity of matrix metalloproteinase-9 on the ocular surface increase in dysfunctional tear syndrome. Invest Ophthalmol Vis Sci. 2009 Jul;50(7):3203-9. doi: 10.1167/iovs.08-2476[↩]
- De Paiva CS, Pflugfelder SC. Corneal epitheliopathy of dry eye induces hyperesthesia to mechanical air jet stimulation. Am J Ophthalmol. 2004 Jan;137(1):109-15. doi: 10.1016/s0002-9394(03)00897-3[↩]
- Methodologies to diagnose and monitor dry eye disease: report of the Diagnostic Methodology Subcommittee of the International Dry Eye WorkShop (2007). Ocul Surf. 2007 Apr;5(2):108-52. doi: 10.1016/s1542-0124(12)70083-6[↩][↩][↩]
- Carsons SE, Patel BC. Sjogren Syndrome. [Updated 2023 Jul 31]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK431049[↩][↩][↩]
- De Vita S, Gandolfo S, Zandonella Callegher S, Zabotti A, Quartuccio L. The evaluation of disease activity in Sjögren’s syndrome based on the degree of MALT involvement: glandular swelling and cryoglobulinaemia compared to ESSDAI in a cohort study. Clin Exp Rheumatol. 2018 May-Jun;36 Suppl 112(3):150-156.[↩]
- Martel A, Coiffier G, Bleuzen A, Goasguen J, de Bandt M, Deligny C, Magnant J, Ferreira N, Diot E, Perdriger A, Maillot F. What is the best salivary gland ultrasonography scoring methods for the diagnosis of primary or secondary Sjögren’s syndromes? Joint Bone Spine. 2019 Mar;86(2):211-217. doi: 10.1016/j.jbspin.2018.06.014[↩]
- Baer AN, Walitt B. Update on Sjögren Syndrome and Other Causes of Sicca in Older Adults. Rheum Dis Clin North Am. 2018 Aug;44(3):419-436. doi: 10.1016/j.rdc.2018.03.002[↩]
- Shen L, Suresh L, Lindemann M, Xuan J, Kowal P, Malyavantham K, Ambrus JL Jr. Novel autoantibodies in Sjogren’s syndrome. Clin Immunol. 2012 Dec;145(3):251-5. doi: 10.1016/j.clim.2012.09.013[↩]
- van Bijsterveld OP. Diagnostic tests in the Sicca syndrome. Arch Ophthalmol. 1969 Jul;82(1):10-4. doi: 10.1001/archopht.1969.00990020012003[↩]
- Golden MI, Meyer JJ, Zeppieri M, et al. Dry Eye Syndrome. [Updated 2024 Feb 29]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK470411[↩][↩][↩][↩]
- Morthen MK, Magno MS, Utheim TP, Snieder H, Hammond CJ, Vehof J. The physical and mental burden of dry eye disease: A large population-based study investigating the relationship with health-related quality of life and its determinants. Ocul Surf. 2021 Jul;21:107-117. doi: 10.1016/j.jtos.2021.05.006[↩]
- Dry Eye Assessment and Management Study Research Group; Asbell PA, Maguire MG, Pistilli M, Ying GS, Szczotka-Flynn LB, Hardten DR, Lin MC, Shtein RM. n-3 Fatty Acid Supplementation for the Treatment of Dry Eye Disease. N Engl J Med. 2018 May 3;378(18):1681-1690. doi: 10.1056/NEJMoa1709691[↩]
- Mohamed HB, Abd El-Hamid BN, Fathalla D, Fouad EA. Current trends in pharmaceutical treatment of dry eye disease: A review. Eur J Pharm Sci. 2022 Aug 1;175:106206. doi: 10.1016/j.ejps.2022.106206[↩]
- Stapleton F, Alves M, Bunya VY, Jalbert I, Lekhanont K, Malet F, Na KS, Schaumberg D, Uchino M, Vehof J, Viso E, Vitale S, Jones L. TFOS DEWS II Epidemiology Report. Ocul Surf. 2017 Jul;15(3):334-365. doi: 10.1016/j.jtos.2017.05.003[↩]
- Chao C, Golebiowski B, Stapleton F. The role of corneal innervation in LASIK-induced neuropathic dry eye. Ocul Surf. 2014 Jan;12(1):32-45. doi: 10.1016/j.jtos.2013.09.001[↩]





{kind=link}