Contents
What is Kwashiorkor
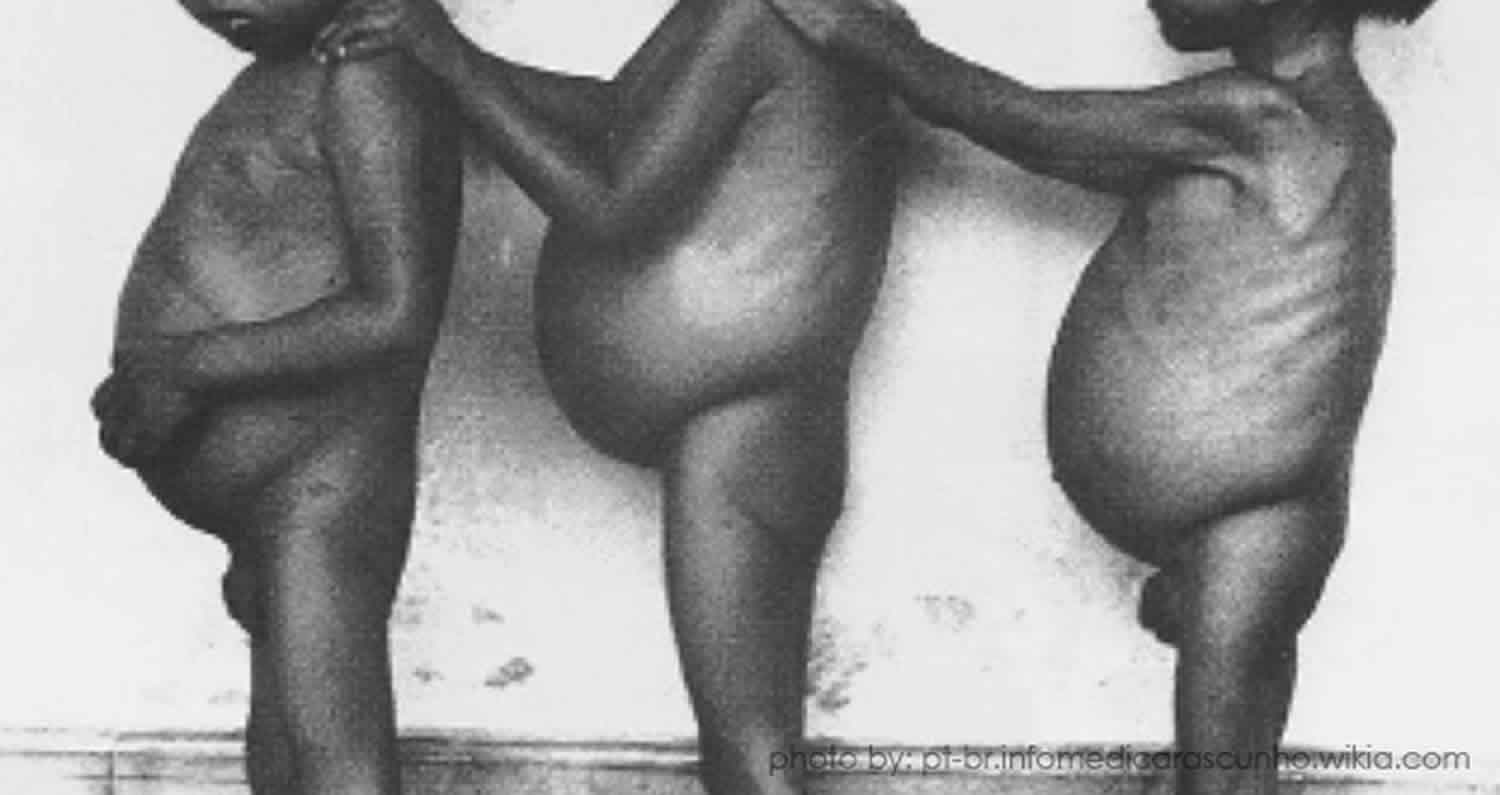
Kwashiorkor is a disease marked by severe protein malnutrition and bilateral extremity swelling 1. Kwashiorkor is most common in some developing regions of the world where babies and children have a diet that lacks protein and other essential nutrients. The main sign of kwashiorkor is too much fluid in the body’s tissues, which causes swelling under the skin (edema). It usually begins in the legs, but can involve the whole body, including the face.
Kwashiorkor usually affects infants and children, most often around the age of weaning through age 5. Kwashiorkor is seen in very severe cases of starvation and poverty-stricken regions worldwide. In the 1950s, it was recognized as a public health crisis by the World Health Organization. However, there was a delay in its recognition, because most cases of childhood death were reported as being from diseases of the digestive system or infectious cause. Since then, various relief efforts were aimed at eradicating kwashiorkor.
As scientists continued to investigate the natural history of kwashiorkor in children, they discovered something very striking. Children who were dying from “digestive system diseases” and presenting with diarrhea, cough, coryza (irritation and swelling of the mucous membrane in the nose) and shortness of breath also were having symptoms of kwashiorkor during this time (pitting edema, anorexia, skin changes, etc.). This finding led to the medical conundrum of whether kwashiorkor was the primary or the secondary cause of death. It was concluded to be the secondary cause of death because many cases of the disease would not have developed without the precipitating stress of diarrhea, dehydration and other infectious diseases such as HIV and measles.
Kwashiorkor is rare in children in the United States. There are only isolated cases. When kwashiorkor does occur in the United States, it is most often a sign of child abuse and severe neglect. However, one government estimate suggests that as many as 50% of elderly people in nursing homes in the United States do not get enough protein in their diet.
Kwashiorkor is most common in areas where there is:
- Famine
- Limited food supply
- Low levels of education (when people do not understand how to eat a proper diet)
Kwashiorkor is more common in very poor countries. It often occurs during a drought or other natural disaster, or during political unrest. These conditions are responsible for a lack of food, which leads to malnutrition. Worldwide, most affected regions include Southeast Asia, Central America, Congo, Puerto Rico, Jamaica, South Africa, and Uganda. Prevalence can vary, but kwashiorkor is seen mostly during times of famine. Rural and farming communities are often affected the hardest.
Kwashiorkor vs Marasmus
While kwashiorkor is a disease of edematous malnutrition, marasmus is similar in appearance. Marasmus is another type of malnutrition that can affect young children in regions of the world where there’s an unstable food supply – a diet that is very low in both protein and calories. Marasmus is also called “balanced starvation” 2. Signs of marasmus include thinness and loss of fat and muscle without any tissue swelling (edema).
Marasmus is known as the wasting syndrome (malnutrition without edema). Children typically have a depletion of body fat stores, low weight for height, and reduced mid-upper arm circumference. Other features of marasmus can include thin, dry skin; a head that appears large relative to the body; an emaciated, weak appearance; bradycardia; hypotension; hypothermia; and thin, shrunken arms, thighs, and buttocks with redundant skin folds.
Like kwashiorkor, marasmus is caused by a lack of the right types of nutrients. This may occur among kids of all ages, but is more common among one- year-olds. If breast-feeding is unsuccessful or the mother has insufficient breast-milk supply and little or no alternative food is given to the infant, the result could be marasmus.
The following characterize marasmus:
- Failure to gain weight followed by loss of weight until emaciation results
- Skin becomes wrinkled and loose
- Face becomes shrunken and the child looks like an old man
- The abdomen is distended or thin
- Muscle wasting (buttocks, thighs, shoulders, and upper arms)
- Loose skin folds in the buttocks
- Growth retardation (body weight is 60 percent or less of expected weight)
- Infant is usually quiet and apathetic
Associated diseases or conditions include dehydration resulting from infectious diarrhea, tuberculosis, and the presence of intestinal parasites.
Tests may need to be carried out to exclude other causes of thinness. The treatment for marasmus is similar to that for kwashiorkor.
What causes kwashiorkor
The cause of Kwashiorkor is fairly unknown, but diets based mainly on maize, cassava, or rice are frequently associated kwashiorkor 1. Kwashiorkor was previously believed to be due to protein deficiency and low levels of antioxidants and aflatoxins. Evidence for these associations exists; however, efforts targeted to replete diets with high-protein and antioxidants have not been successful 1. Aflatoxin, previously thought to be the cause of kwashiorkor, is not always associated with the disease in certain populations. Some factors that are consistently associated with kwashiorkor include recent weaning, recent infection (particularly measles), and disruptions in childhood (parental death, temporary home environment, poverty).
Kwashiorkor is most common in developing countries with a limited food supply, poor hygiene, and a lack of education about the importance of giving babies and children an adequate diet.
Kwashiorkor is rare in developed countries such as the US, but it can occasionally occur as a result of severe neglect, long-term illness, a lack of knowledge about good nutrition, or a very restricted diet.
Although kwashiorkor can affect people of all ages, it’s more common in children than adults.
Kwashiorkor pathophysiology
Kwashiorkor is characterized by peripheral edema in a person suffering from starvation. Edema results from a loss of fluid balance between hydrostatic and oncotic pressures across capillary blood vessel walls. Albumin concentration contributes to the oncotic pressure, allowing the body to keep fluids within the vasculature. Children with kwashiorkor were found to have profoundly low levels of albumin and, as a result, became intravascularly depleted. Subsequently, antidiuretic hormone (ADH) increases in response to the hypovolemia, resulting in edema. Plasma renin also responds aggressively, causing sodium retention. These factors contribute to the edema.
Kwashiorkor is also marked by low glutathione (antioxidant) levels. This is thought to reflect high levels of oxidant stress in the malnourished child. High oxidant levels are commonly seen during starvation and are even seen in cases of chronic inflammation. One measure at reversal would be improved nutritional status and sulfur-containing antioxidants. There is also an experimental theory proposing that alterations in the microbiome/virone contribute to edematous malnutrition, however, further studies are required to understand the mechanism.
Kwashiorkor prevention
To prevent kwashiorkor, make sure the diet has enough carbohydrates, fat (at least 10% of total calories), and protein (12% of total calories).
Kwashiorkor symptoms
As well as peripheral pitting edema that begins in dependent regions and proceeds cranially, symptoms of kwashiorkor can include:
- loss of muscle mass (muscle atrophy)
- an enlarged tummy (“pot belly”) with/without dilated bowel loops and hepatomegaly
- regular infections, or more serious or long-lasting infections than usual
- thin, dry, red or inflamed patches of skin that darken (hyperpigmentation) and peel or split open
- dry, brittle hair that falls out easily or is easily plucked and may lose its color (hypopigmented hair)
- hair changes: lack of luster, “flag sign” (alternating light and dark bands in the hair, indicating alternating periods of protein adequacy and deprivation)
- failure to grow in height (growth retardation)
- tiredness or irritability
- ridged or cracked nails
- round face (prominence of the cheeks, or “moon facies”) due to edema
- hepatomegaly (enlarged liver from fatty liver infiltrates)
- psychic changes (anorexia, apathy)
- skin lesions/dermatitis (perineum, groin, limbs, ears, armpits)
- subcutaneous fat retention with loose inner inguinal skin folds
Kwashiorkor can be fatal if it’s left untreated for too long because children become very vulnerable to infections.
Kwashiorkor complications
Some complications of kwashiorkor include:
- Hepatomegaly (from the fatty liver)
- Cardiovascular system collapse/hypovolemic shock
- Urinary tract infections
- Abnormalities of the gastrointestinal tract including atrophy of the pancreas with subsequent glucose intolerance, atrophy of the mucosa of the small
- intestine, lactase deficiency, ileus, bacterial overgrowth, which can lead to bacterial septicemia and death.
- Loss of immune function, antioxidant function, subsequent infections, septic shock, and death.
- Endocrinopathies where insulin levels are decreased; growth hormone is increased, but insulin-like growth factor levels are reduced. This leads to insulin intolerance
- Metabolic disturbances and hypothermia
- Impaired cellular functions, including endothelial dysfunction
- Electrolyte abnormalities are commonplace
- Coma
- Permanent mental and physical disability
- Shock
Kwashiorkor diagnosis
Kwashiorkor can often be diagnosed based on a child’s physical appearance and questions about their diet and care. Nutritional history, past medical history, vaccination history, and family history are also important to elicit from patients suspected of being malnourished.
However, blood and urine tests may be carried out to rule out other conditions. This can include tests to:
- Measure blood sugar and protein levels
- Check how well the liver and kidneys are working by testing the urine and blood for anemia
- Measure the levels of vitamins and minerals in the body
- Arterial blood gas
- Blood urea nitrogen (BUN)
- Complete blood count (CBC)
- Creatinine clearance
- Serum creatinine
- Serum potassium
- Total protein levels
- Urinalysis
Other tests may include growth measurements, calculating body mass index (BMI), measuring body water content, taking a skin biopsy and analysing a hair sample.
The World Health Organization has a classification system for evaluating for malnutrition severity that determines wasting versus kwashiorkor. They use three clinical measures:
- The mid-upper arm circumference (MUAC),
- Weight-for-height/length Z score, and
- Presence of symmetrical pitting edema.
It is generally accepted that mid-upper arm circumference (MUAC) less than 110 mm is highly associated with mortality in infants younger than 6 months old. Criteria for hospital admission is based on reaching defined cutoffs set by the WHO.
Kwashiorkor treatment
If kwashiorkor is identified early it can be treated with either specially formulated milk-based feeds or ready-to-use therapeutic food (RUTF).
Ready-to-use therapeutic food is typically made up of peanut butter, milk powder, sugar, vegetable oil, and added vitamins and minerals.
More intensive treatment in hospital will be needed in severe cases or where there are already complications, such as infections. However, children who have had kwashiorkor will never reach their full potential for height and growth.
The following are ten primary principles used universally for treatment of patients who are admitted for Kwashiorkor 1. These principles are done in different phases from the time the child arrives requiring emergency stabilization through eventual rehabilitation.
- Treating/preventing hypocalcemia,
- Treating/preventing hypothermia
- Treating/preventing dehydration
- Correcting electrolyte imbalance
- Treating/preventing infection
- Correcting micronutrient deficiencies
- Starting cautious feeding
- Achieving catch-up growth
- Providing sensory stimulation and emotional support and
- Preparing for follow up after recovery.
It is important to highlight how critical it is to address the fluid imbalance in kwashiorkor. In the past, there was concern about aggressive rehydration causing acute heart failure. However, this was proven to be exaggerated. At the same time, severe hypovolemia could cause hypovolemic shock and death. So, medical staff had to proceed cautiously. The standard normal saline solution contains too much sodium and too little potassium. However, ReSoMal (Rehydration Solution of Malnutrition) is a customized solution that can be given orally or via nasogastric tubes that contains the exact amount of mineral/electrolytes, sugar, and water that the WHO recommends 1.
Hospital treatment will usually involve:
- treating or preventing low blood glucose
- keeping the person warm – kwashiorkor can make it harder to generate body heat
- treating dehydration with specially formulated rehydration solution
- treating infections with antibiotics – kwashiorkor greatly increases the risk of infections
- treating vitamin and mineral deficiencies – vitamin supplements are usually included in the special milks or ready-to-use therapeutic food
- slowly introducing small amounts of food before gradually increasing the amount of food
The whole process usually takes between two and six weeks to complete.
Recovering from kwashiorkor
How well a person recovers from kwashiorkor depends on how severe their symptoms were when treatment began.
If treatment was started early, the person will usually recover well, although children may never reach their full growth potential and be shorter than their peers.
If treatment was started in the later stages of protein malnutrition, the person may be left with physical and intellectual disabilities.
If kwashiorkor isn’t treated or treatment is significantly delayed, it can lead to death.
- Benjamin O, Lappin SL. Kwashiorkor. [Updated 2018 Oct 27]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2018 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK507876[↩][↩][↩][↩][↩]
- On Malnutrition: What is Kwashiorkor and Marasmus? https://medicalobserverph.com/babyminder-on-malnutrition-what-is-kwashiorkor-and-marasmus/[↩]





{kind=link}